www.pspbc.ca psp child and youth mental health sheraton wall centre vancouver october 4 & 5,...
TRANSCRIPT

www.pspbc.ca
PSP Child and Youth Mental Health
Sheraton Wall Centre VancouverOctober 4 & 5, 2011
AdolescentMajor Depressive Disorder(MDD)
Dr. Stan Kutcher
www.Dreamstime.com 1345216
2

3
Adolescence = puberty to mid-twenties Affects approx. 6-8% of adolescents Most experience 1st episode between 14-24 yrs old Youth onset usually = chronic condition
› Substantial morbidity
› Poor economic/vocational/interpersonal/health outcomes
› Increased mortality Suicide Other long term chronic illness: diabetes, heart disease,
etc.
Fast Facts
Adolescent Depression

4
Early identification & early effective treatment
› Decreases short-term morbidity
› Improves long-term outcomes Decreased mortality
www.freedigitalphotos.net by Zirconicusso
Fast Facts
Adolescent Depression

5
1. Over the past few weeks have you been having difficulties with your feelings, such as feeling sad, blah or down most of the time?› If YES – consider a depressive disorder › Apply the KADS evaluation
Depression Screening Question

6
1. Identification of youth at risk for MDD2. Screening & diagnosis in the clinical setting3. Treatment template4. Suicide assessment5. Contingency planning6. Referral flags
Key Steps for Treatment of MDD in Adolescents
www.dreamstime.com 310430

Step 1: Major Depressive Disorder in Youth
Risk Identification TableWell established andsignificant risk effect
Less well establishedrisk effect
Possible “group”identifiers
(these are not causal for MDD but may
identify factors relatedto adolescent onset
MDD)
1. Family history of MDD
2. Family history of suicide
3. Family history of a mental illness (mood disorder, anxiety disorder, substance abuse disorder)
4. Childhood onset anxiety disorder
1. Childhood onset ADHD
2. Substance abuse
3. Severe and persistentenvironmental stressors(sexual abuse, physical abuse, neglect) in childhood.
4. Head injury (concussion)
1. School failure
2. Gay, lesbian, bisexual,transsexual
3. Bullying (victim and/or perpetrator)
7

8
Educate
› About risk of familial mental disorders Record
› Family history of mental disorder Agree
› On a ‘clinical review’ threshold Urgent and emergency clinical reviews
(re: suicide ideation) Arrange
› A standing ‘mental health checkup’ 15 minutes each 3 – 6 months Use KADS tool during checkups
www.freedigitalphotos.net by Ambro
If Youth is High Risk…

9
Check for patterns
› Declining grades
› Frequent lates or absences
Confidentiality & informed consent
› Both young person and
parents/guardian(s) involved
› Easier for youth to access care
› Easier for parents to know what to expect
www.dfreeigitalphotos.net by Idea Go
If Youth is High Risk…
Kutcher Adolescent Depression Scale (KADS-6)
Methods for Clinical Screening & Diagnosis
Explain purpose of test
& give feedback on
resultswww.dreamstime.com ID:983365
Including contraception
& sexual health
visits
Screen at clinical contacts
10

Distress vs. DisorderDistress Disorder
Associated with a precipitating event May be associated with a precipitating event or may onset spontaneously
Functional impairment is usually mild Functional impairment may range; mild–severe
Transient – will usually ameliorate with change in environment or removal ofstressor
Long lasting or may be chronic, environment may modify but not ameliorate
Professional intervention not usually necessary
External validation (syndromal diagnosis: DSM*/ICD*)
Can be a positive factor in life – person learns new ways to deal with adversity
Professional intervention is usually necessary
Social supports such as usual friendship and family networks help
May increase adversity due to effect on creation of negative life events (e.g.: low mood can lead to relationship loss)
Counseling and other psychological interventions can help
May lead to long term negative outcomes (substance abuse, job loss, etc.)
Medications should not usually be used Medications may be needed. Must use properly
Social supports and specific psychological interventions are helpful
11

12
Who to Screen?
Adolescents with:
• Risk factors
• Persistent low or irritable
mood of recent onset
• Academic
problems/failure
• Substance misuse
• Suicidal ideation
Clinical MDD Screening in Primary Care
Stockxchng ID: 63460_4774
Refer to
Risk Identification Table

13
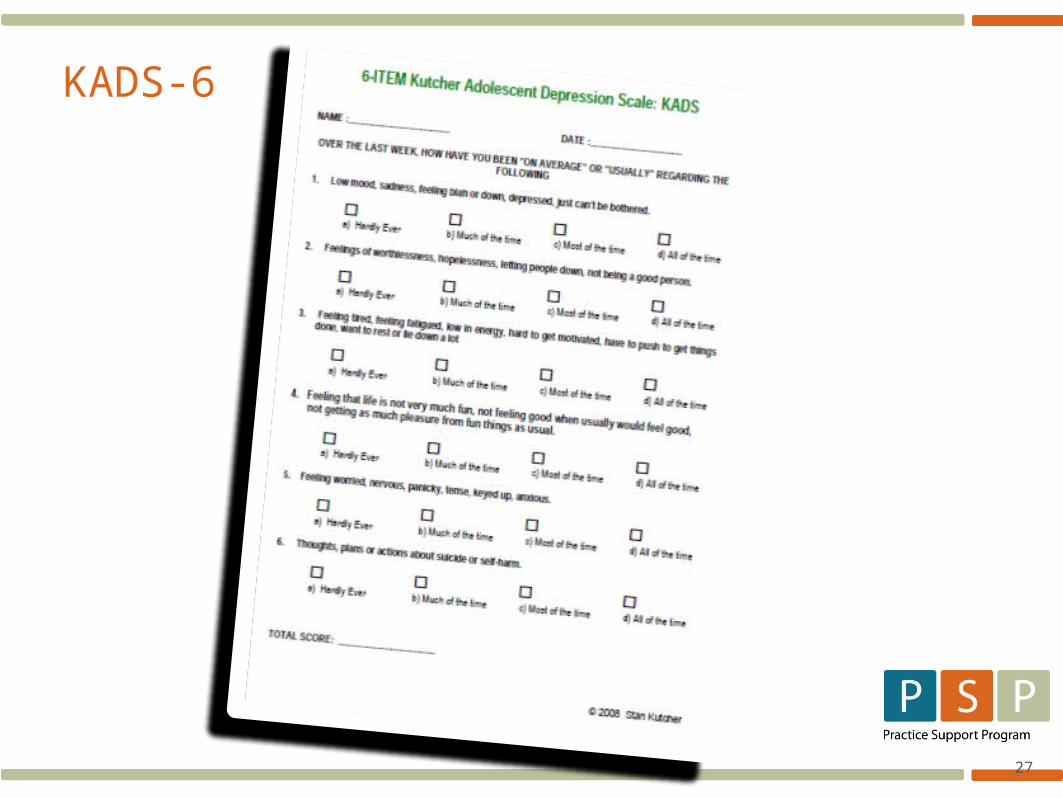
Kutcher Adolescent Depression Scale
(KADS) Self-reporting instrument
› For diagnosis and monitoring
› Scoring information included
› KADS score 6+ = clinical depression suspected
Suggests a possible diagnosis
Use as a guide for further evaluation
Assessment Tool

14
1st appointment Discuss issues in youth’s life & environment
› Use TeFA – Teen Functional Activities Assessment Assists in determining impact of depression
Problem solving assistance› “Supportive rapport”
Use PST – Psychotherapeutic Support for Teens as a guide
KADS Score of 6+
Exercise
Regulated Sleep
Positive Social
Activities
Regulated Eating
Strongly encourage and prescribe:
15
1st appointment (continued) Screen for suicide risk
› Use TASR – Tool for Assessment of Suicide Risk
› ‘Check-in’ 3 days following initial appointment
Via telephone (3 – 5 mins.), text message or e-mail
If problems continue, book appointment ASAP
KADS Score of 6+
www.freedigitalphotos.net by Zirconicusso

16
2nd appointment Mental health checkup
› 15 – 20 minutes› 1 week from first visit› Include: KADS, TeFA, PST› Monitor suicide risk
3rd appointment Mental health checkup
› 15 – 20 minutes › 1 week from 2nd mental health checkup› Include: KADS & TeFA› Monitor suicide risk
KADS Score of 6+
www.freedigitalphotos.net by Nutdanai Apikhomboonwaroot

17
Use the tools
Address important issues
Three -15 minute office visits
Use KADS routinely
Suicide intent/plan/attempt
= Emergency
Mental Health Assessment
Don’t Get Overwhelmed!!
Dreamstimefree 836493

18
KADS scores remain at 6+› For over 2 weeks› At each of the three assessment points
Suicidal thoughts or self harm behaviors School, family or interpersonal functioning
declines› Assess using TeFA
If above occurs, on 3rd visit review DSM-V criteria› Five or more items + = diagnosis of MDD› Initiate treatment plan
MDD Highly Probable if…
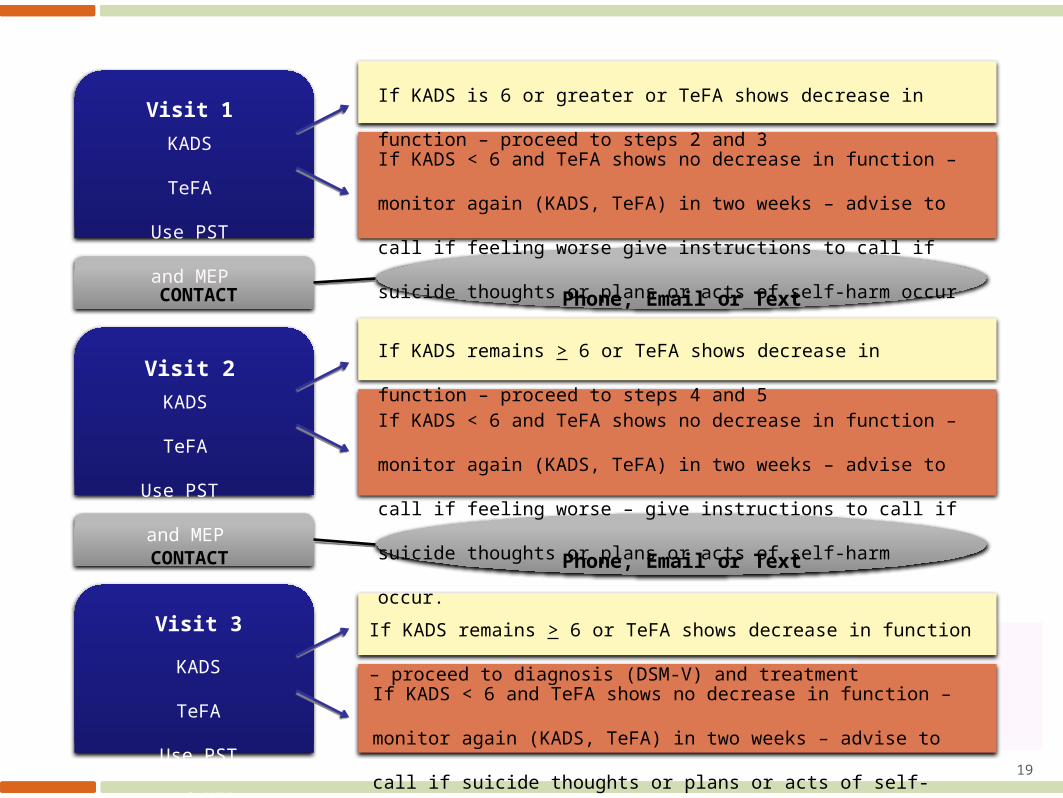
Visit 1
CONTACT
Visit 2
Visit 3
CONTACT
Phone, Email or Text
If KADS is 6 or greater or TeFA shows decrease in function – proceed
to steps 2 and 3If KADS < 6 and TeFA shows no decrease in function – monitor again
(KADS, TeFA) in two weeks – advise to call if feeling worse give
instructions to call if suicide thoughts or plans or acts of self-harm occur
KADS
TeFA
Use PST
and MEP
Phone, Email or Text
KADS
TeFA
Use PST
and MEP
If KADS remains > 6 or TeFA shows decrease in function – proceed to
steps 4 and 5If KADS < 6 and TeFA shows no decrease in function – monitor again
(KADS, TeFA) in two weeks – advise to call if feeling worse – give
instructions to call if suicide thoughts or plans or acts of self-harm
occur.
KADS
TeFA
Use PST
and MEP
If KADS remains > 6 or TeFA shows decrease in function – proceed to
diagnosis (DSM-V) and treatmentIf KADS < 6 and TeFA shows no decrease in function – monitor again
(KADS, TeFA) in two weeks – advise to call if suicide thoughts or plans
or acts of self-harm occur 19

20
1. Determine what is known already
2. Identify areas of misinformation
3. Identify gaps in knowledge & provide information
4. Be knowledgeable, realistic, clear & helpful
5. Provide written materials /websites for self study
› Many think taking meds will lead to addiction
6. Discuss anticipated duration of medication use
› First episode = 6 – 9 months after they get well
7. Discuss how meds will impact lifestyle
› Light alcohol use is usually ok; can drive with SSRI
Provide Information
21
Compassionate & non-judgmental attitude
Active listening
› Eye contact, verbal/non-verbal cues Clarification
› “Help me understand”… Emotional identification
› “It seems you are feeling frustrated”...
Do not jump to conclusions
› You are likely to be wrong ASK, if you don’t understand If you don’t know the answer – admit &
find out
Creating a Supportive Environment
www.freedigitalphotos.net by Idea Go

22
Monitoring CGI TeFA TASR-A KADS (6 item)
Interventions (these do not replace medications or psychotherapies)
PST MEP
Monitoring and Intervention Tools: Depression

23
Risk Factors: History of suicide attempt or self harm
Presence of Depression
› Hopelessness
Family history of suicide
Family history of a mental disorder
› Especially mood disorders
If one or more are identified use
Tool for Assessment of Suicide Risk in Adolescents (TASR-A)
Screening for Suicide Risk
www.freedigitalphotos.net Risk Blocks by jscreationzs

24
CBIS Depression CBT/IPT tools
› Evidence based psychotherapies available (CBIS)
› Application recommended – manual provided
› Can be implemented at any time during the process
› Education about medications should be added
Additional Psychosocial Interventions
www.freedigitalphotos.net by Idea Go

Dealing with Depression
25

26
A tool like KAD-6 is tangible and helps us and the young person in front of us streamline the conversation to an
extent (perhaps relieves some anxiety for us too)
27
KADS-6
28
How can these tools fit into GP practice workflow? What about applicability to school or other practice environments? (for example screening tools)
How can other team members use the information from these tools? How can information from other environments be used to complete them?
How can team members in non-providers roles contribute to administration and completion of these tools?
Table Discussion