work-injury management and return-to-work in the
TRANSCRIPT

Work-injury Management and Return-to-work in the Manufacturing Industry in Selangor, Malaysia
Dr Siew Wei Fern 15 October 2018

In fulfilment of the requirements for the degree of Doctor of Philosophy in Medical and Health Sciences. Supervisors: Prof. Dr. Stephen Periathamby Ambu Associate Dean, IMU Research Lab, B. Med Sc Programme, International Medical University
Prof. Dr. Mak Joon Wah Vice President, Research, International Medical University
Dato’ Sri Dr Mohammed Azman bin Dato’ Aziz Mohammed Chief Executive Officer, Social Security Organisation (SOCSO), Malaysia
This study was funded by the internal research grant of IMU.
This research was aimed to answer the following questions:
Research question (1):
What approaches had SOCSO incorporated to engage the key
stakeholders (nurses, employers and workers with work related injuries) in
its national RTW programme relating to work injury management, return to
work practices and workplace adjustments or modification practice?
3
Research question (2):
What organisational policy and practices were in placed to manage work
injury, return to work practices and workplace adjustments or modification
practices in the manufacturing industry in Selangor, Malaysia?
Research question (3):
How do nurses, employers and workers with work related injuries
perceived their experiences in participating with work-injury
management, return to work practices and workplace adjustments or
modification practices?

Global perspective
Work-related injuries
occurrences have been a global
burden to the developed and
developing countries for many
decades. (Takala et al, 2014)
Employers, workers and the
society are burdened by the
economic cost of work injuries
due to accidents which come in
the form of direct and indirect
costs.
PROBLEM STATEMENT
Organisation’s burden:
staff turnover costs
training costs
loss of output
increased insurance premium
and legal cost
Injured workers’s burden:
net loss of future earnings
(minus compensation)
medical cost and rehabilitation
cost
Society’s burden:
social payout
investigation / inspection
costs
work, safety and health
promotion
loss of human capital and
medical subsidy 4

Figure 1.1 Number of industrial accidents 2004 – 2013
Note. From SOCSO Annual Report 2004 – 2013.
Figure 1.2 Compensation – employment injury 2004 – 2013
Note. From SOCSO Annual Report 2004 – 2013.
In Malaysia, numbers of work-
related injuries due to
industrial accidents have
reduced considerably over
the last ten years, but do not
correspond with SOCSO
compensation pay-out, which
has increased over the years.
5
3
Over last 10 years
Over last 10 years

RTW is a complex issue broad understanding of the
processes is vital. (Shaw, Feuerstein, Miller & Wood, 2002)
Workers have also reported a sense of powerlessness in the
process of recovery and RTW following a workplace injury (Friesen, 2004).
6
Statutory obligations may be in place for workplace rehabilitation
but most employers have adopted a minimalist approach,
introducing workplace rehabilitation solely because “it’s the law”
or rather than as a component of a risk management strategy (Hawkins, 2000)
committed participation by the various key stakeholders in
the management to ensure early return to work of workers
sustaining injuries

Acknowledges that:
workers form the major component of human resources
in the industries
workers are highly in demand for every sector of the
various industries
they are the assets to the organisation
In Malaysia, the Ministry of Human Resources is greatly
concern over the number of occurrences in work injuries
related to industrial accidents as well as the economic
costs resulting from these accidents.
When workers sustained injury while at work which
resulted in time loss at work, they are deemed as a liability
to their organisation. 7
workers were rushed through the recovery and rehabilitation
process by, e.g healthcare professionals and employers, who tend
to not believe that the workers have a legitimate problem
My professional perspective from observations
8
employers have no clues how to accommodate modified duties
when workers are prescribed with light duties by the physician
workers were inadequately counselled on early RTW, pressed
to RTW once they have exhausted their medical leave
entitlement or otherwise face the consequences of having their
wage deducted / terminated
nurses were not empowered to provide holistic counselling to
the injured workers as the role of counselling was done by the
in house or visiting doctors

9
Effective communication
Readiness in managing the process
Policies and practices in place
Present job guaranteed
Injured worker well facilitated through their
recovery and return to sustainable employment
Questions
‹#›

‹#›

Conceptual Framework of this Study
Figure 1.6 Conceptual framework of the study
Workers
Compensation
SOCSO
Workplace
(manufacturing industry)
Work
Injured
Workers
Nurses servicing
in this industry
Employer
External
Acci
dent
Surg
ery
Acut
e
Inpa
tient
Trea
tmen
t
Pros
thes
is? Physical rehabilitation
Vocational rehabilitation Constant communication
Constant monitoring
GOAL?
Maintain patient-doctor-
employer relations
Safe recovery
RTW
Permeability between the
inner and outer circle for
cohesive work-injury and
RTW management
12
Figure 1.5 Comprehensive Disability Management Model.
Adapted from “A conceptual model for Comprehensive Disability Management," by
H.G. Harder and L.R. Scott, 2003, Journal of the Ontario Occupational Health
Nurses Association, p. 20.
Healthcare
Lawyer
Family
Workers
Compensation
Insurance
Third party
administrator
Safety
Agencies
Advocates
Social
Support
Expectations
Employee
Assistance
Programs
Community
Agencies
Workplace
Work
Worker Union
Co-workers Management
External
Conceptual Framework of this Study Based on CDMModel

Research design: Mixed methods approach
Methodology
Objective (2)
Self-reporting QA
Employers 13
Figure 3.4 Morgan (2014) multipart sequential mixed methods approach applied in this study
Preliminary phase
QUAL
data collection, analysis, results
Second phase
QUANT
data collection,
analysis, results
Follow-up extension
phase
QUAL
data collection,
analysis, results
Interpretation
Triangulate corroborate & converge data
25
Objective (1)
Document review,
Non-participant observation
Objective (3)
FGDs – employers
Semi-structured
interview: workers and
industrial nurses
26
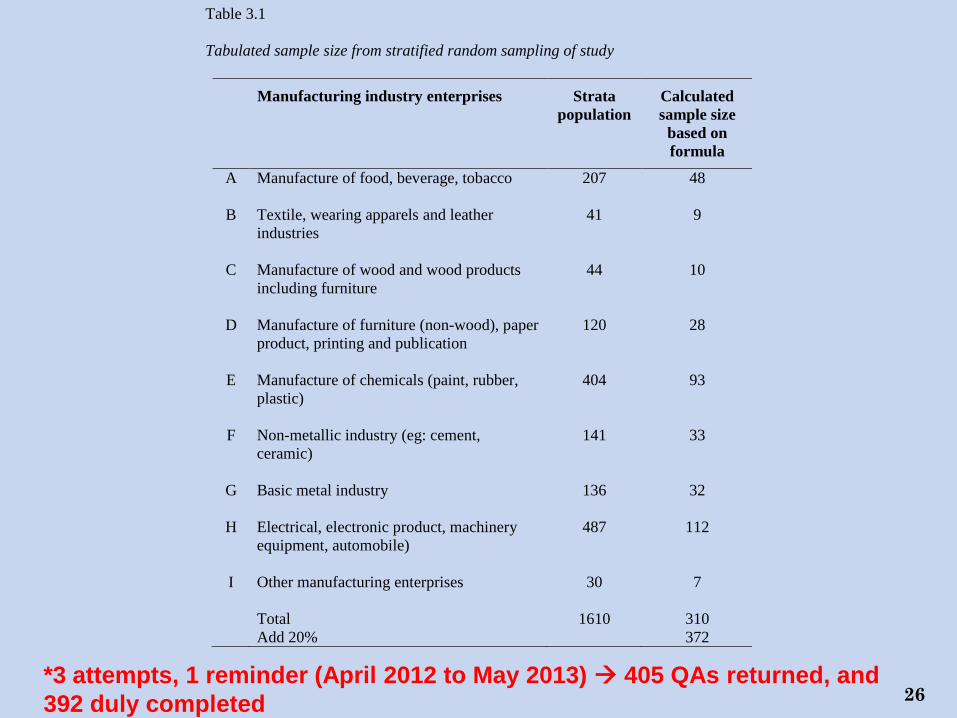
Table 3.1
Tabulated sample size from stratified random sampling of study
Manufacturing industry enterprises Strata
population
Calculated
sample size
based on
formula
A Manufacture of food, beverage, tobacco
207 48
B Textile, wearing apparels and leather
industries
41 9
C Manufacture of wood and wood products
including furniture
44 10
D Manufacture of furniture (non-wood), paper
product, printing and publication
120 28
E Manufacture of chemicals (paint, rubber,
plastic)
404 93
F Non-metallic industry (eg: cement,
ceramic)
141 33
G Basic metal industry
136 32
H Electrical, electronic product, machinery
equipment, automobile)
487 112
I Other manufacturing enterprises
30 7
Total 1610 310
Add 20% 372
*3 attempts, 1 reminder (April 2012 to May 2013) 405 QAs returned, and
392 duly completed

15
Interviews – Industrial Nurses
Table 4.37
Industrial nurses’ details (Interview).
Nurses Sex Age Types of enterprise
Years of working
experience in industrial
nursing
Year graduated as
Registered Nurse
Clinical experience
prior current job
N 1 F 28 A 3 2011 Fresh graduate
N 2 F 35 E 4 2010 Fresh graduate
N 3 F 36 H 4 2010 Fresh graduate
N 4 F 44 H 8 2006 2 years hospital
experience
N 5 F 33 D 5 2009 3 years hospital
experience
N 6 F 52 E 15 1999 3 years hospital
experience
Note. F=Female; A=Manufacture of food, beverage, tobacco; D=Manufacture of paper product, printing and publication;
E=Manufacture of chemicals (paint, rubber, plastic); H= Metal and machinery equipment (electrical, automobile)
16
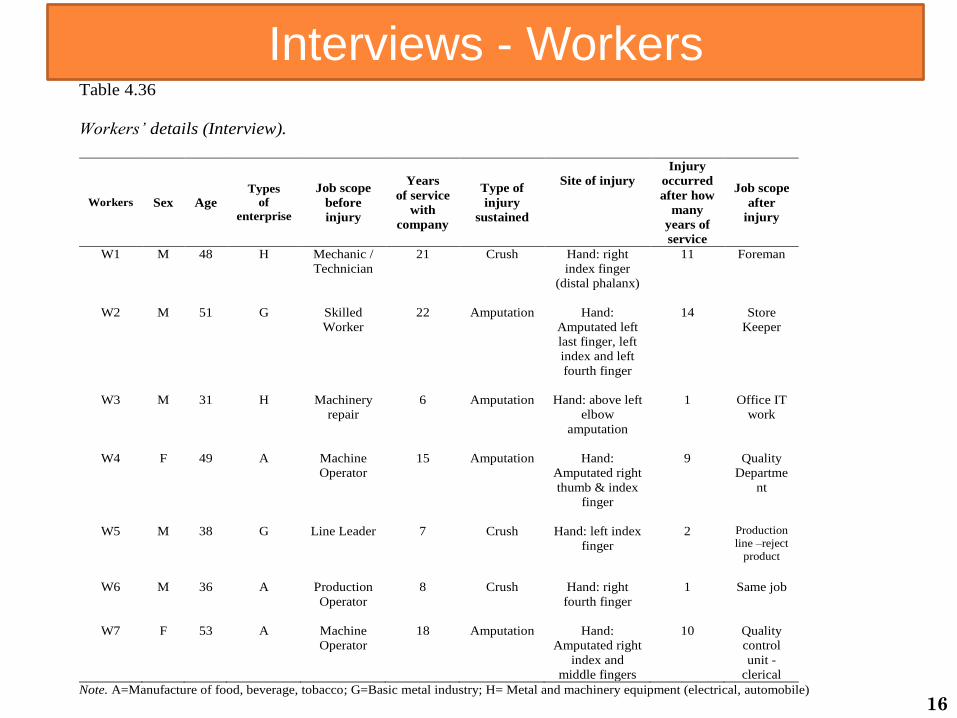
Interviews - Workers Table 4.36
Workers’ details (Interview).
Workers Sex Age
Types
of
enterprise
Job scope
before
injury
Years
of service
with
company
Type of
injury
sustained
Site of injury
Injury
occurred
after how
many
years of
service
Job scope
after
injury
W1 M 48 H Mechanic /
Technician
21 Crush Hand: right
index finger
(distal phalanx)
11 Foreman
W2 M 51 G Skilled
Worker
22 Amputation Hand:
Amputated left
last finger, left
index and left
fourth finger
14 Store
Keeper
W3 M 31 H Machinery
repair
6 Amputation Hand: above left
elbow
amputation
1 Office IT
work
W4 F 49 A Machine
Operator
15 Amputation Hand:
Amputated right
thumb & index
finger
9 Quality
Departme
nt
W5 M 38 G Line Leader 7 Crush Hand: left index
finger
2 Production
line –reject
product
W6 M 36 A Production
Operator
8 Crush Hand: right
fourth finger
1 Same job
W7 F 53 A Machine
Operator
18 Amputation Hand:
Amputated right
index and
middle fingers
10 Quality
control
unit -
clerical
Note. A=Manufacture of food, beverage, tobacco; G=Basic metal industry; H= Metal and machinery equipment (electrical, automobile)

Method of analysis to qualitative components Table 3.10 Stages involved with developing the template.
Identify priori themes
Coded 1st FGD
Cluster codes from
1st FGD
Identify themes and developed the
initial template
Analyse 2nd and 3rd FGDs.
Review and revised the template
Analyse individual worker’s
interviews.
Review and revised the template
Analyse individual industrial
nurse’s interviews.
Review and revised the template
Analyse all the data from all the
FGDs and individual interview.
Develop final template
• not an expert in
counselling for injured
workers
• unable to modify
workplace
• unsure of the options for
light duty
• injured workers unable to
multitask
• lack of awareness and
training on compensation
scheme and return to
work programme
• communication gap
among employers
doctor(s) treating the
injured workers
• unable to cater to injured
worker(s) due to fast
production needs
17

18
Results & Discussion

19
Quantitative analysis
Non- parametric test was used as the dependent variables
failed the assumption of normality distribution:
Table 4.29
Tests of Normality
Shapiro-Wilk
Statistics df p
Work-injury case management subscale 0.921 392 <.001
RTW practices subscale 0.971 392 <.001
Work adjustments or modification practices subscale 0.883 392 <.001
OPP summated scores 0.933 392 <.001
*p < 0.05

20
Qualitative analysis
Themes:
Figure 4.1 Initial Template: priori themes to second template: modified
theme
The initial template
Coded and clustered into priori themes
following 1st FGD
The second template
Coded and clustered following the remaining
2nd, 3rd FGDs and interviews with nurses
Theme 1:
Not an expert to counsel injured
workers
Modified theme 1:
Uncertainties in decision making
Theme 2:
Unable to modify workplace for
injured workers
Theme 3:
Unsure of the options for light
Duty
Modified theme 2:
Commitment to extended roles
Theme 4:
Injured workers are unable to
multitask
Theme 5:
Lack of awareness in
compensation scheme
Modified theme 3:
Deficient knowledge related to process
management of RTW
Theme 6:
Communication gap among
employers and doctor(s) treating the
injured workers
Theme 7:
Unable to cater to injured worker(s)
job relocation need
Modified to Integrative theme:
Effective communication

21
Results
Document analysis findings
Treating doctor’s prescription in RTW to workers following
work-injury:
light duty, no prolonged lifting of weight more than two kilograms,
avoid heavy load of 5 kilograms, avoid operating heavy
machineries for two months and also avoid prolonged standing,
walking and sitting.
Reporting to SOCSO following injury by the Employer: (days)
Median length: 60
Minimum days: 2
Maximum 150

22
Results
N = 142
Types of injuries Frequency (n) Percentage (%)
Fractures 81 57.0
Crushes 31 21.8
Amputations 21 14.8
Sprains 9 6.4
Types of injuries
Document analysis findings

23
Results
N = 142
Site of injuries Frequency (n) Percentage (%)
Upper limbs 83 58.5
Multiple locations 32 22.5
Lower limbs 15 10.6
Back 9 6.4
Site of injuries
Document analysis findings

24
Results
N = 69
Medical leave taken (months) Frequency (n) Percentage (%)
> 1 month to 3 months
29 42.0
> 3 months to 9 months
37 53.6
> 9 months 3 4.4
Medical leave taken
Note. MDN = 67.5
Document analysis findings

25
Results
N = 142
Duration of intervention Frequency (n) Percentage (%)
1 to 3 months 47 33.1
> 3 to 6 months 18 12.7
> 6 to 9 months 20 14.1
> 9 to 12 months 17 12.0
> one year 40 28.1
Intervention duration for RTW programme.
Document analysis findings

26
Results
Permanent disability percentage
n = 31
Median percentage awarded: 9.5%,
Minimum: 2%
Maximum: 80% (amputated arm above the elbow)
Document analysis findings

27
Results
N = 118
RTW hierarchy Frequency (n) Percentage (%)
Same employer same job 15
12.7
Same employer similar job 36 30.5
Same employer different job 48
40.7
Different employer same job 2 1.7
Different employer similar job 1 0.8
Different employer different job 10 8.5
Self-employed 6
5.1
RTW hierarchy
Document analysis findings
28
Results
Non participant observations findings
The SOCSO rehabilitation service providers for the RTW programme:
12 centres
Klang valley; Seremban; Ipoh; Melaka; Pulau Pinang
SOCSO engages the employers and workers in its RTW programme
through various strategies. Its strategies are comprehensive and
commendable with an upstream system approach.

29
Results
Non participant observations findings
Emerging topics over the four conferences were:
• strategies of RTW / disability management at workplace;
• early interventions for RTW;
• addressing disability at work with policies and actions;
• challenges in rehabilitation;
• stakeholders influencing RTW and breaking the barriers
• interchangeable topics on light duties, modifications at work and the
importance of early transitional work options for the injured workers.
There were still barriers ahead in the disability management system
among the organisational practices.

30
Results
Non participant observations findings
SOCSO assured its case managers will work closely with the employers
and workers in RTW aspects.
SOCSO officers coordinate to provide information on job vacancies for the
disabled insured persons and assist in preparations for job application.
SOCSO - authorised organisation which is licensed to handle training,
organising the examination and the certification process of Certified
Return to Work Coordinator (CRTWC) and Certified Disability
Management Professional (CDMP) by International Disability Management
Standards Council (IDMSC)
31
Results
Information on safety and health practices: (N = 392)
81.4% (n = 319) of the employers responded that they were
familiar with OSHA 1994.
Some 12% (n = 49) of the employers still do not have a safety and
health committee established.
An alarming 100 % of employers having their teams not trained in
managing RTW.
84.7% (n = 322) utilised the workers’ injury data to help them in
solving problems related to safety and health.
Employers Survey

32
Results
Worker’s compensation awareness
100% employers aware of the roles played by SOCSO.
More than 70% (n = 285) of the employers were still unsure that
SOCSO offers two types of compensation schemes.
51.8% (n = 203) aware the reporting of accident to SOCSO within
is 48 hours of occurrence and yet 48.2% (n = 189) did not answer
this aspect correctly.
Small percentage, 15.3% (n=60) of the employers were still
unaware that SOCSO offers RTW programme to its insured
workers.
Employers Survey
33
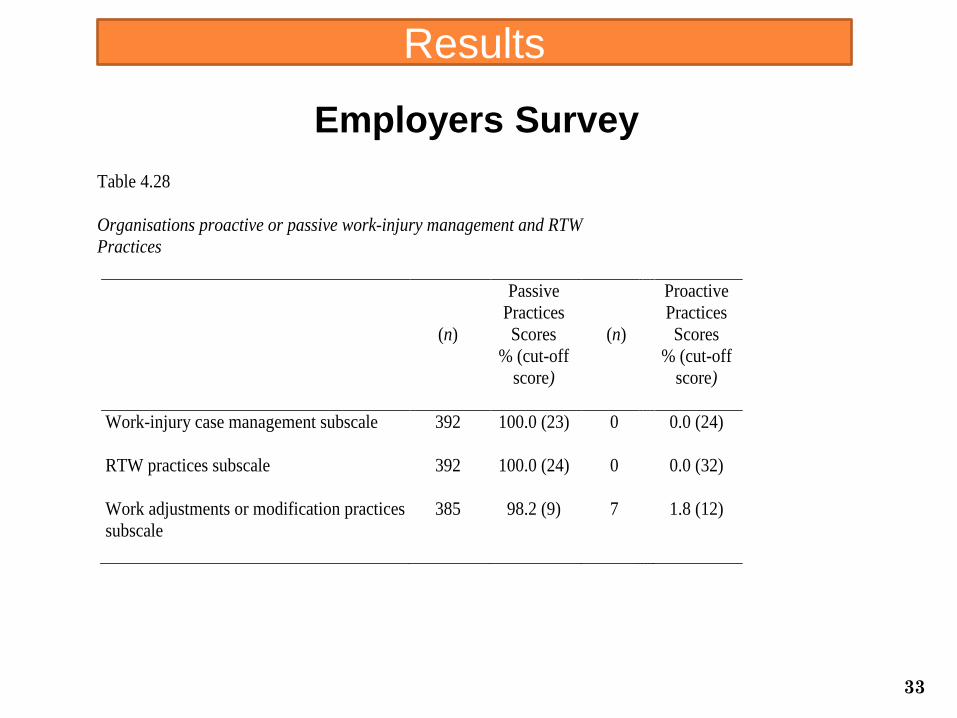
Results
Table 4.28
Organisations proactive or passive work-injury management and RTW
Practices
(n)
Passive
Practices
Scores
% (cut-off
score)
(n)
Proactive
Practices
Scores
% (cut-off
score)
Work-injury case management subscale 392 100.0 (23) 0 0.0 (24)
RTW practices subscale 392 100.0 (24) 0 0.0 (32)
Work adjustments or modification practices
subscale
385 98.2 (9) 7 1.8 (12)
Employers Survey

34
Results
A Mann-Whitney U test indicates that Organisational Policies and
Practices (OPP) scores is significantly higher for employers:
who employ more than 500 workers (U = 11046, p = 0.039, r =.10)
are familiar with the Occupational Safety and Health Act 1994
(U = 7478, p < .001, r =.24)
have a safety and health committee (U = 4744, p < .001, r =.25)
use workers’ injury data to problem solve RTW (U = 6509,
p < .001, r =.20)
aware that SOCSO offers RTW programme (U = 6079, p < .001, r
=.24).
Employers Survey
35
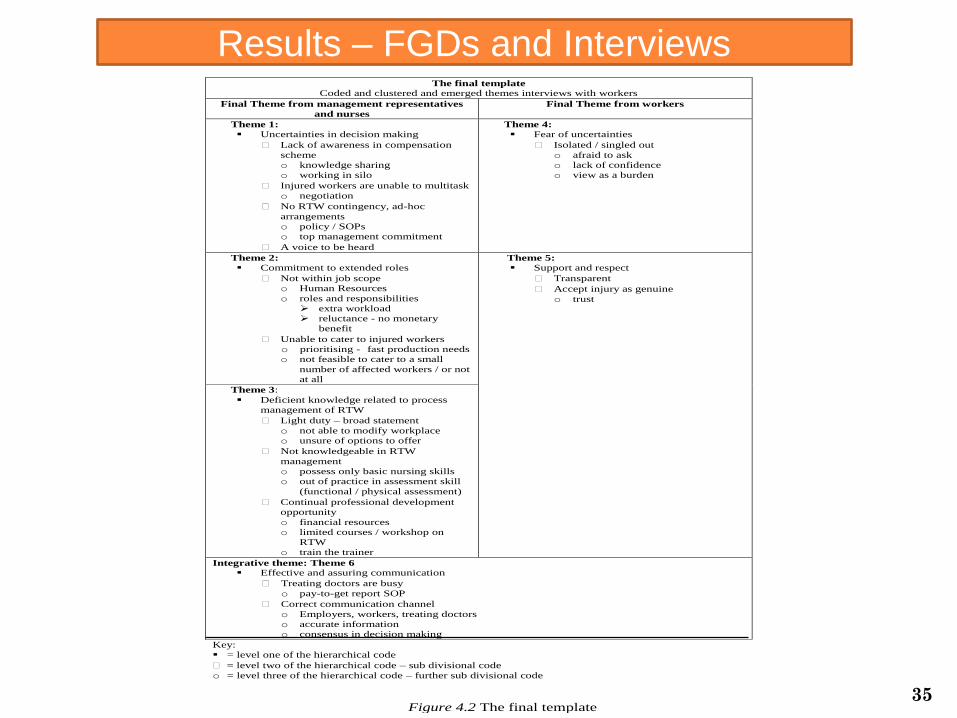
Figure 4.2 The final template
The final template
Coded and clustered and emerged themes interviews with workers
Final Theme from management representatives
and nurses
Final Theme from workers
Theme 1:
Uncertainties in decision making
Lack of awareness in compensation
scheme
o knowledge sharing
o working in silo
Injured workers are unable to multitask
o negotiation
No RTW contingency, ad-hoc
arrangements
o policy / SOPs
o top management commitment
A voice to be heard
Theme 4:
Fear of uncertainties
Isolated / singled out
o afraid to ask
o lack of confidence
o view as a burden
Theme 2:
Commitment to extended roles
Not within job scope
o Human Resources
o roles and responsibilities
extra workload
reluctance - no monetary
benefit
Unable to cater to injured workers
o prioritising - fast production needs
o not feasible to cater to a small
number of affected workers / or not
at all
Theme 5:
Support and respect
Transparent
Accept injury as genuine
o trust
Theme 3:
Deficient knowledge related to process
management of RTW
Light duty – broad statement
o not able to modify workplace
o unsure of options to offer
Not knowledgeable in RTW
management
o possess only basic nursing skills
o out of practice in assessment skill
(functional / physical assessment)
Continual professional development
opportunity
o financial resources
o limited courses / workshop on
RTW
o train the trainer
Integrative theme: Theme 6
Effective and assuring communication
Treating doctors are busy
o pay-to-get report SOP
Correct communication channel
o Employers, workers, treating doctors
o accurate information
o consensus in decision making
Key:
= level one of the hierarchical code
= level two of the hierarchical code – sub divisional code
o = level three of the hierarchical code – further sub divisional code
Results – FGDs and Interviews

36
Discussion
It is evidenced by past research that RTW is effective when interventions
for the workers following an injury at work starts from the day of accident
itself.
Australia - average days taken for submitting a claim with the employer
from an initial injury was slightly more than a month (38 days)
[Mdn 3 months] (Australia Government Comcare, 2005).
Kucera, et.al (2009) study - highlighted that workers with back injuries
were more likely to take 90 days or longer to RTW following a delay of 30
days or longer in the work-injury management
Besen, Harrell and Pransky (2016) study concluded that the predicted
length of disability reduced closed to 40 days less if work disability lag
time was zero days as compared with having a lag time of 30 days or
longer.

37
Discussion
Besen, Harrell and Pransky (2016) reasoned that the findings suggest
possibility of differences types of injury sustained and their study focused
specifically on low back injury, while the other study included all work-
related injuries. [fractures and crushes]
The extend of injuries unable to present the report immediately
because of their injury alongside with prolonged medical leave of absence
and extended periods of treatment. [medical leave in median length of
medical leave taken by these was 67.5 days, with minimum of 34
days and maximum of 478 days].
Hoffmann, 2015; Johnson, 2015; Jafri Mohd Rohani et al, 2015;
Barnett et al., 2010; Worksafe, n.d.; Perry et al., 2005; Silverstein & Clark 2004; Fan, McLeod &
Koehoorn, 2010)

38
Discussion
Vocational rehabilitation yields positive outcome when intervention is
immediate as recovery time for body stressing injuries takes no more
than six weeks in many cases and no more than 12 weeks in severe soft
tissue injuries. (Vandenbroeck, Verjans, Lambreghts & Godderis, 2016; Australian Government Comcare,
2006).
[shortest duration between one to three months, to the longest
duration of more than a year. ]
SOCSO RTW programme – 2007 – limited case managers
SOCSO Ministerial KPI - 116.09 (improved from tremendously from
more than 700 days) *international benchmark of 59.4 days (Olivier et al., 2012).

39
Discussion
Lack of clear RTW policies:
Concur with results from past research - that lack of clear local policies
being the backbone to the proactive early management of RTW may
possibly result in employers directing to solutions based on expense
avoidance instead of aiming at rehabilitation for workers as the focus of
importance is on own business and production revenues rather than a
long term of return of investment.
[the organisations are likely to comply with the provision of self-
regulation of OSHA 1994, with a duty of due diligence to safety and
health in order to ensure so far as is practicable, to protect their
workers at work. ]
Australia Government Comcare, 2016; Snell & Hart, 2009; Foreman, Murphy & Swerissen,
2006; Mills, 2012; Berecki-Gisolf et al., 2012; Nielsen et al., 2012; He et al., 2010; Lee &
Kielhofner 2010; Blank et al., 2008; Foreman, et al., 2006; SOCSO, 2007.

40
Discussion
Past research conducted which showed that larger companies exercise
formal RTW programme and are able to offer extensive range of
assistance to workers (Adya, et.al, 2012; Ossman et al., 2005; Johnson & Fry, 2002; Australia Institute for
Primary Care, 2006; Kenny, 1998).
[OPP scores were significantly higher for employers who employ
more than 500 workers, other than the possible practice of due
diligence in safety and health by the organisations, it is more likely
that large organisations have greater financial capital and thus
have more resources to be able to support their RTW programme
internally].
Effective work transition exercise is impracticable when information on
worker’s capabilities and physical demands of the required job are
vague and not clearly specified, as it will not yield effective outcomes
[operationalised challenges]
(Gonser & Archibald, 2010; Tugman et. al, 2010).

41
Discussion
Training and communication is vital because those assigned to
manage the cases of injured workers returning to work would not be
familiar with the processes as the programme itself must be
individualised, where it is tailored to meet the specific needs of the
workers. Johnson & Fry, 2002, p. 17; Vandenbroeck, et.al, 2016
[However, managers and nurses have very little contact time
with the injured workers and therefore this is a crucial aspect
which need to be improved – knowledge deficient play as
evidenced]

RECOMMENDATIONS
1. Timely need for the Ministry of Human Resources Malaysia to review the Occupational Safety and Health Act 1994 to supplement a regulation mandating a written RTW policy to ensure commitment from the top management of large companies with more than 500 employees in compliance with the Part IV - General Duties of Employers and Self-Employed Persons: Section 15. General duties of employers and self-employed persons to their employees.
2. As for the smaller companies, SOCSO consultation shall be sought for the RTW related matters, nevertheless best practices are recommended.
3. The employers are recommended to seek consultation from SOCSO to assist in the practical implementation and application of the RTW programme at organisation level. This is when the RTW strategies of assessment, planning, implementation, evaluation and follow-up can be maximised. Through these strategies effective and assuring two-way communication between management and workers can be achieved.
4. Meanwhile, the management should start monitoring if the RTW programme generates a return on investment for the company for cases managed.
42
RECOMMENDATIONS 5. Digital resources can be used by employers to link worker’s compensation and RTW information to all the staff via an internet portal, or through staff bulletin board where information should be constantly updated.
This link can be customised to allow uploads of SOCSO Accident Reporting form 21 from the managers / supervisors /safety and health officers directly to the Human Resources. This could assist the Human Resources personnel to report the accident to SOCSO within the stipulated time of 48 hours.
6. The management should consider its best practice to encourage staff career development programme relating to disability management in order to create best workers who are knowledgeable and competent in this field. This can drive job satisfaction and improve motivation towards work as well for these workers.
7. Make courses related to disability management / rehabilitation affordable to all. As this encourages the generation of a pool of competent RTW coordinators. A home-grown curriculum is recommended.
8. Managements should consider setting up a mini place of exercise within the organisation,
as this will enhance wellness not only for the healthy employers and employees, but also provide a space and basic equipment for workers with disability to exercise (range of motion, isometrics) during their transition to work duties. They can be supervised by the nurses and ensure continuity of physiotherapy when time and transport are not in favour to them to attend the physiotherapy at the designated SOCSO rehabilitation centre.
43

Nurses, employers, workers with work related injuries and
SOCSO’s real involvement are depicted in their participating
efforts and strategies in work-injury and RTW management in
the manufacturing industry in Selangor, Malaysia.
It presents actual needs for developing an effective work
injury management with RTW programme within
manufacturing industry.
Nurses, employers, workers must play an active role here
and possess knowledge, skills, abilities and aptitudes in
collaborative work injury management.
Summary
44

This study can provide perspective to the human resources on
formulating organisational policy and SOPs for workplace injury
and RTW management to support and facilitate injured workers
returning to their occupation in optimum health and work
functionality.
As an academic, provide me with the opportunity to initiate work
with the various healthcare professionals / health ministry in
relating to nursing practice for nurses servicing the manufacturing
industry in Malaysia to enable them to advance and upgrade
themselves in the field of work rehabilitation.
The findings from this study could serve as a source of information
and reference for future studies to other countries who are
interested in work injury management and RTW.
Summary
45

THANK YOU
46