wilson’s disease – how do i manage dr. ashish bavdekar
TRANSCRIPT

Wilson’s Disease – How do I manage ?
Dr. Ashish BavdekarAssociate Professor
Consultant Ped. GastroenterologistK.E.M. Hospital, [email protected]
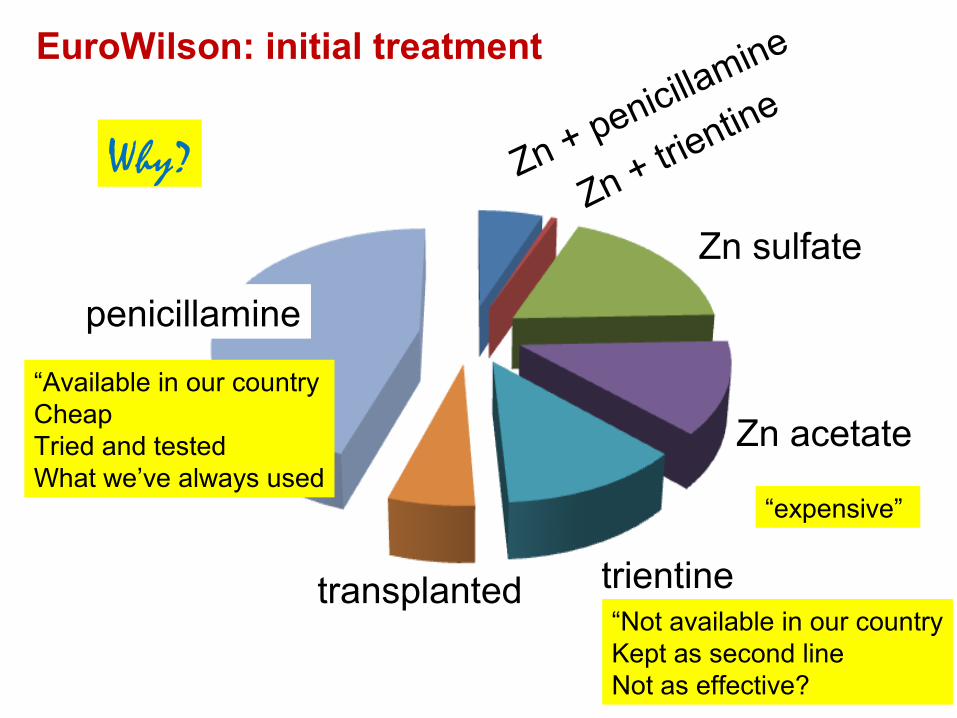
Zn + penicillamine
Zn + trientine
Zn sulfate
Zn acetate
trientine
penicillamine
transplanted
EuroWilson: initial treatment
Why?
“Available in our countryCheapTried and testedWhat we’ve always used
“Not available in our countryKept as second lineNot as effective?
“expensive”

Wilson’s disease – management
- Low copper diet - Serving size (< 0.1mg, 0.1-0.2, > 0.2mg)


Wilson’s disease – management
- Low copper diet - Serving size (< 0.1mg, 0.1-0.2, > 0.2mg)
- Medications - D-Penicillamine
- Trientine
- Zinc
- Ammonium molybdate

Wilson’s Disease - therapy
1) Reduce Cu to sub-toxic threshold - takes 6-12 months - DP, Trientine
2) Maintain slightly negative Cu balance - life long therapy - DP, Trientine, Zn

DP Trientine Zinc
Chelator Chelator Induces MT
Easy availability Patient named basis
Easy availability
Reasonable cost V Expensive Cheap
Side effects Neurological
Minimal SE Gastric discomfort

Treatment: Hepatic cases
acute liver failure with encephalopathy
acute liver failure without encephalopathy
intermediate severity
Asymptomatic transaminitis
Asymptomatic and normal LFTs
Neonate detected by screening
List for TxTrientine + zinc‘bridge’
Modified Kings scoreTx if >11Trientine + zinc

Score Bilirubinmol/Lɥ
INR ASTIU/L
WCCx 109/L
Albuming/L
0 0-100 0-1.29 0-100 0-6.7 >451 101-150 1.3-1.6 101-150 6.8-8.3 34-442 151-200 1.7-1.9 151-300 8.4-10.3 25-333 201-300 2.0-2.4 301-400 10.4-15.3 21-244 >301 >2.5 >401 >15.4 <20
Modified King’s score
A score > 11 = urgent need for transplantationValidated in other centres; better than PELD

Treatment: Hepatic cases
acute liver failure with encephalopathy
acute liver failure without encephalopathy
intermediate severity
Asymptomatic transaminitis
Asymptomatic and normal LFTs
Neonate detected by screening
List for TxTrientine + zinc‘bridge’
Modified Kings scoreTx if >11Trientine + zinc
Zinc
Zinc – when to start?

Treatment: Hepatic cases
acute liver failure with encephalopathy
acute liver failure without encephalopathy
intermediate severity
Asymptomatic transaminitis
Asymptomatic and normal LFTs
Neonate detected by screening
List for TxTrientine + zinc‘bridge’
Modified Kings scoreTx if >11Trientine + zinc
Zinc
Zinc – when to start?
Trials needed

DP Trientine Zinc
Chelator Chelator Induces MT
Easy availability Patient named basis
Easy availability
Reasonable cost V Expensive Cheap
Side effects Neurological
Minimal SE Gastric discomfort
Initial therapy Initial therapy Initial Rx / co-RxMaintenance Rx
All except Severe t-peniaDP intoleranceNeurological
Initial co-RxMaintenance RxPresympt. cases

Treatment of WD in pregnancy
• Treatment should not be stopped
• DP, Trientine, Zn allowed
• Zinc preferable, no dosage change
• DP, Trientine reduce dose to 25-50% esp in last trimester

Monitoring in WD ?
• To determine clinical and biochemical improvement/deterioration
• Ensure compliance
• To identify adverse effects of medications
• To review diagnosis if necessary

Monitoring plan (chelators)
• Clinical– Liver status, neuro-psychiatric worsening– KF ring annually
• Biochemical (USG)– CBC, LFTs, Urine– 3, 6, 9, 12 days initially– Weekly, biweekly, 1 mo, 3 mo, 6mo
• Urinary Cu, Serum free copper– Initially 4 times per year– Later 1-2 times

DP Trientine ZincEarlyFever, RashBM suppression, Proteinuria, LNpathy
Avoid iron + TRashesHaem. GastritisSideroblastic ALoss of taste
GastritisLeucopeniaIncreased lipase and amylase
LateNephrotoxicityLupus like SEPSLoss of tasteV LateMyasthenia, PolymyositisRetinitis
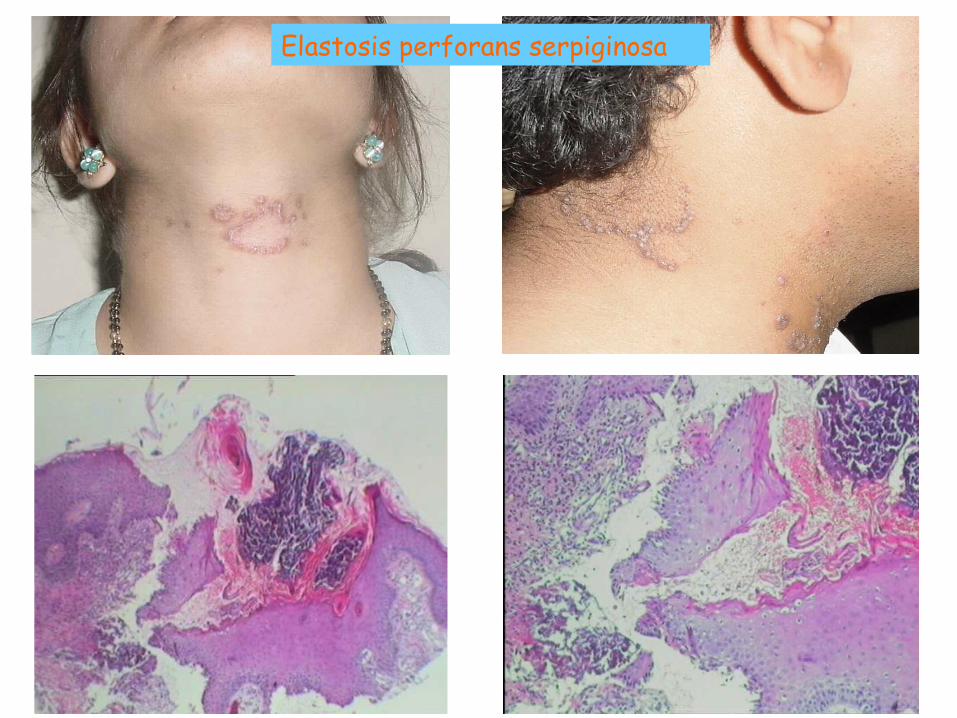
Elastosis perforans serpiginosa

Zinc DP / Trientine
Initial Rx U Cu 100-500 ug/dS free Cu > 25 ug/dL
U Cu > 500ug/dS free Cu > 25 ug/dL
Good control U Cu < 75ug/dS free Cu < 15 ug/dL
U Cu 200-500 ug/dS free Cu < 15ug/dL
Non-compliance/Inadequate dose
U Zn < 2mg/d U Cu < 200 ug/dU Cu > 200 ug/dS free Cu > 15ug/dL
Over-treatment U Cu < 25 ug/d S. free Cu < 5 ug/dLAnemia, leucopeniaIncreased ferritin
U Cu < 200 ug/dS. free Cu < 5 ug/dLAnemia, leucopeniaIncreased ferritin
Urinary copper in Wilson’s disease

Zinc DP / Trientine
Initial Rx U Cu 100-500 ug/dS free Cu > 25 ug/dL
U Cu > 500ug/dS free Cu > 25 ug/dL
Good control U Cu < 100ug/dS free Cu < 15 ug/dL
U Cu 200-500 ug/dS free Cu < 15ug/dL
Non-compliance/Inadequate dose
U Zn < 2mg/d U Cu < 200 ug/dU Cu > 200 ug/dS free Cu > 15ug/dL
Over-treatment U Cu < 25 ug/d S. free Cu < 5 ug/dLAnemia, leucopeniaIncreased ferritin
U Cu < 200 ug/dS. free Cu < 5 ug/dLAnemia, leucopeniaIncreased ferritin
Urinary copper in Wilson’s disease

Summary
• Chelators are mainstay of treatment
• Diet has adjunct role
• Zinc has role in long-term Rx
• Monitoring is crucial
• Interpretation of UCu important