what's hot in diabetes care 2018 -...
TRANSCRIPT

What's Hot in Diabetes Care 2018
Fred Toffel, MD, FACP, FACE

Objectives
• A Taste of Technology
– Updates on Continuous Glucose Monitoring
– Smart Insulin Pumps
– Connected Insulin Pens
• Getting to the Heart of Type 2 Algorithms
– Review of the 2018 AACE Algorithm
– Review of Cardiovascular Outcomes Trials and How these Impact Diabetes Treatment Recommendations

History of Glucose Monitoring
In 1500 BCDiabetes First Described In Writing
Hindu healers wrote that flies and ants were attracted to urine of people with a mysterious disease that caused intense
thirst, enormous urine output, and wasting away of the body

In 1941 Clinitest® effervescent
urine sugar testing tablets
launched by Bayer (formerly
Miles Laboratories)
Methodology: Urinalysis for glucose
Uses alkaline copper
sulphate and Na citrate –
forms colour in re-hydrated
state dependent on glucose
content – ‘non-specific’ test
subject to interference
0% 2%
Red
cuprous oxide
Monitoring Glycaemic Control : Early History

Methodology: Urinalysis for glucose
In 1954 Glucotest /Testape roll
licensed by Eli Lilly to Boehringer
Mannheim)
• In 1964 Combur-Test (BM) for glucose, protein and pH of urine.
• Later range extended to include ketones – Ketostix/Ketodiastix
During 196Os the ‘dipstix’ :
Diastix, Clinistix,
Chemstrip uG available
Monitoring Glycaemic Control : Early History

Early History : Self-Monitoring Blood Glucose (SMBG)
Visual Reading: ‘semi-quantitative’ estimations
Glucose + O2 gluconic acid + H2O2
H2O2 + dye* reduced oxidised dye + H2O
colourless coloured
*chromogen
Glucose oxidase
Peroxidase
In 1964 Earnest C Adams
developed Dextrostix
(Ames – Miles Laboratories)
Patent No 3,092,465
issued 4th April 1963)
Limitations :• Large drop of blood required to cover test zone (30μl)• Reaction time 60 seconds, • Remove blood - wash/blot or wipe, • Read result within 1-2 seconds after washing • Reliance on color matching
1st dry-reagent blood sugar test-
strip using immobilized glucose
oxidase with horse-
radish peroxidase and a
color indicator.
Modifications: covering over
enzymes and dye with water
resistant material on a plastic
support

1968 Haemo-Glukotest
developed (improved
1979). Remains the gold
standard of accuracy for
purely visual blood
glucose determination.
Automated Evaluation : Reflectance Meters (ARM)
(i) photometric (colourimetric) – ‘Desk-Top’
1974 Reflomat1979 Dextrometer
Reflectance
Meters
Bulky
Heavy
Expensive
1st film-based colorimetric test-strip
Early History : Self-Monitoring Blood Glucose (SMBG)

1983 Reflolux / Accu-chek : from Roche diagnostix
1986 Reflolux II / Accu-chek II
1987 Reflolux II M / Accu-chek II M , memory & PC interface
1990 Reflolux S / Accu-chek III
Automated Evaluation : Glucose meters - digital read-out
(1) photometric test strips –Roche (ex Boehringer M)
Early History : Self-Monitoring Blood Glucose (SMBG)

1987 One Touch meter : introduced by LifeScan
Automated digital read-out meter using
photometric test strips
Second Generation Meters - requirements1. Recognise blood sample application and
time the reaction,
2. Eliminate need for blood removal step by
separation of plasma from RBCs, or
correct for blood color in colorimetric
devices or use electrochemical reactions
4. Incorporate checks to identify defects and
user error in procedure
One Touch II
Early History : Self-Monitoring Blood Glucose (SMBG)
Simplify: No timing, wiping, blotting or washing of blood

Today’s Many Choices

The Transformation from Intermittent Self Blood Glucose
Monitoring (SMBG) to Continuous Glucose Monitoring (CGM)

Cygnus Glucowatch

MiniMed Guardian Real-TimeMARD=19.7%
(2006)Dexcom STS
MARD=26.0%(2006)
Abbott NavigatorMARD=13%
(2006)
2006 The Year EVERYTHING Changed

The Second Generation
2008 Medtronic Paradigm522/722 System
MARD 19.7%
2008 Dexcom Seven 2009 Dexcom Seven PlusMARD 15.9%

CGMs 2018
Eversense Implanted CGM
Dexcom G6 CGM→(No Calibration)
Guardian Connect CGM →
Freestyle Libre CGM(No Calibration)


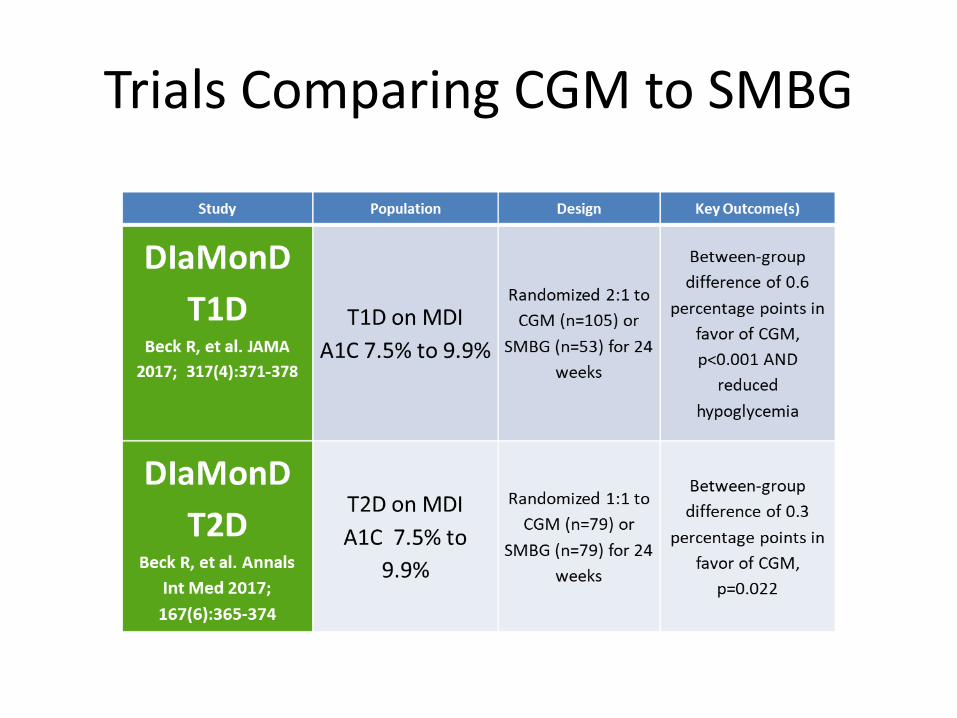
Trials Comparing CGM to SMBG

Study Population Design Key Outcome(s)
GOLDLind M, et al. JAMA
2017; 317(4) :379-387
T1D on MDI
A1C ≥ 7.5%
Randomized
crossover 1:1 to 26
weeks of CGM
before (n=82) or
after (n=79) 26
weeks of usual care
Between-group
difference of 0.43
percentage points in
favor of CGM,
p<0.001 AND less
hypoglycemia
COMISAIRSoupal J, et al.
Diabetes TechTher.
2016 ; 18(9):532-8.
T1D / MDI or CSII
A1C 7.0% to 10%
1 year
Nonrandomized,
controlled: CGM
(n=15 SAP, 12 MDI)
or SMBG (n= 20
using CSII, 18 MDI)
Comparable
reductions in A1C
and hypoglycemia in
CGM/MDI and
CGM/CSII groups
HypoDEHeinemann L, et al.
Lancet 2018; 391:1367-
1377
T1D on MDI
History of
impaired hypo
awareness or
recent severe
hypo
Randomized 1:1 to
CGM (n=75) or
usual care (n=74)
for 26 weeks
Incidence of
hypoglycemic events
fell by 72% for CGM
group, p<0.0001

Studycenter picture on
slidePopulation Design Key Outcome(s)
ImpactBolinder J, et al.
Lancet 2016; 388:
2254–2263,
T1D on MDI or
CSII
A1C <7.5%
Excluded IAH
Randomized 1:1
to Flash (n=119)
or usual care
(n=120) for 24
weeks
Reduced
hypoglycemia. No
between-group
difference in A1C
change, p=0.9556
ReplaceHaak T, et al. Diabetes
Ther. 2017; 8(1): 55–
73.
T2D on MDI or
CSII
A1C 7.5% to
12.0%
Randomized 2:1
to CGM (n=149)
or usual care
(n=75) for 6
months
No between-group
difference in A1C
change,
p=0.82222.
Reduced
hypoglycemia
I HART
CGMReddy M, et al. Diabet
Med. 2018; 35(4): 483–
490
T1D on MDI
Gold score ≥4 or
recent severe
hypo
Randomized 1:1
to CGM (n=20) or
flash glucose
monitoring
(n=20) for 8
weeks
CGM reduces
hypoglycemia
more effectively
than flash glucose
monitoring



CMS Will Cover Home CGM for Patients Insured by Medicare
• Has a diagnosis of diabetesand
• Currently monitors fingerstick glucose four (4) times dailyand
• Injects insulin three (3) times daily
If the patient:
Currently only Dexcom G5 and Freestyle Libre are Medicare approved

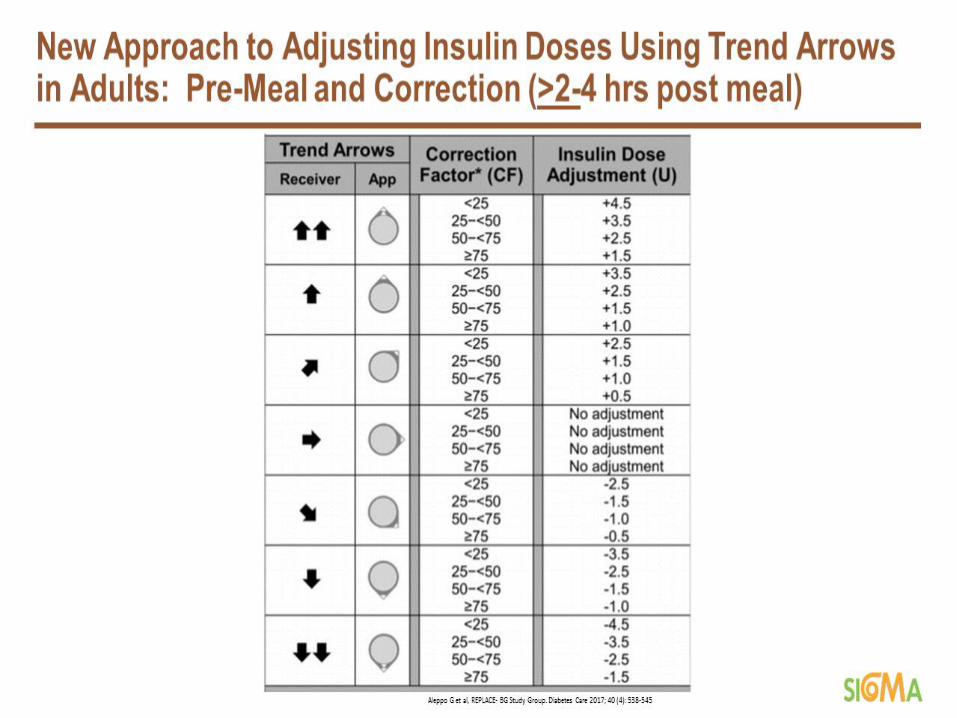
Adding the Other DimensionFollow the Arrow
+ Active Insulin
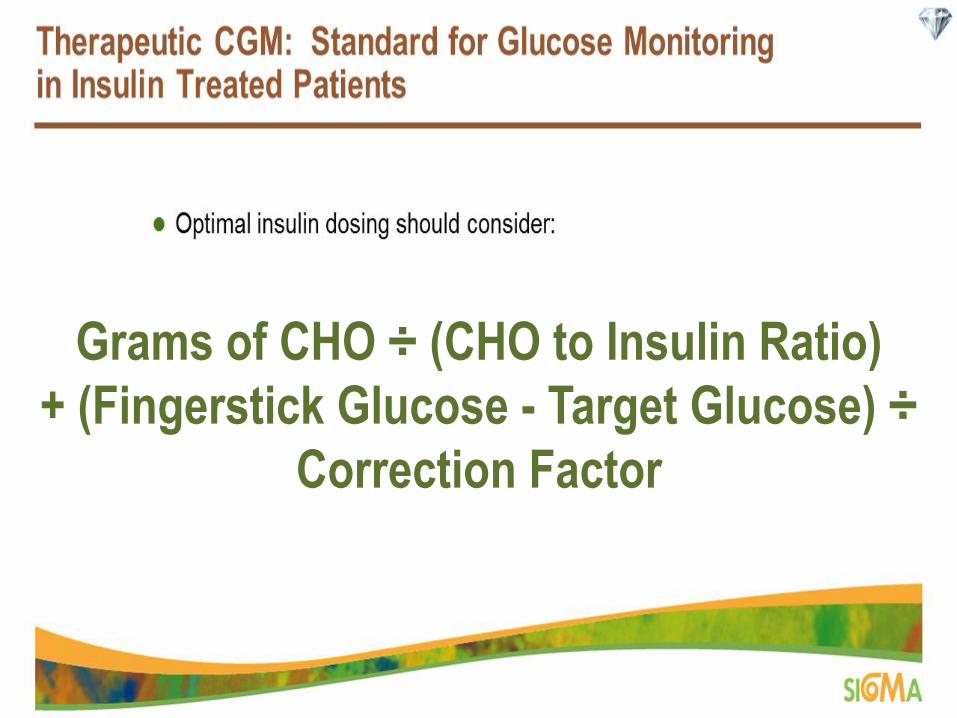
Grams of CHO ÷ (CHO to Insulin Ratio)
+ (Fingerstick Glucose - Target Glucose) ÷
Correction Factor




Freestyle Report

Dexcom Report

Combining CGM with CSII
Bionic Pancreas 1.0

History of BP
• Under Development for more than 50 years
• Described in 1974
– As a “computerized control system …closely simulating the endocrine function of the pancreas.”1
– Intravascular delivery of dextrose and insulin based on instantaneous glucose readings
• Only worked on supervised inpatient conditions
Peyser et al., 2014, Annals of New York Academy of Science, 1311, 102-1231. Albisser et al., 1974, Diabetes, 23, 389-396.

Biostator: The Artificial Pancreas 1977
Clemens, AH. The development of Biostator, a glucose controlled insulin infusion system (GCIIS), Horm Metab Res 1977.

Current Outpatient Conceptual Models
• Closed Loop
– Patient is removed from interaction once the system has been initiated
– Algorithm has total control
• Open Loop (Hybrid Closed Loop)
– Varying Degrees of Interaction
• Meal / Exercise announcement

Hormonal Models
• Uni-Hormonal – Only insulin is used
– Algorithms to reduce risk of hypoglycemia
• Bi-Hormonal – Insulin to lower the blood glucose
– Glucagon to raise the glucose
– Algorithms balance the effects of the two hormones
– Generally doses of glucagon are quite small
Peyser et al., 2014, Annals of New York Academy of Science, 1311, 102-123

Basal Suspend
Medtronic 630G Tandem T:Slim X2 with Basal IQ Software

Currently Available Hybrid Closed Loop PumpMedtronic 670G

670G Data Download

Dual Hormone Bionic Pancreas at Camp

A Camper’s Thoughts
• I was never hypoglycemic• I never felt hypoglycemic• I was never worrying about
hypoglycemia• I was never recovering from
hypoglycemia• That’s already enough of a game
changer for me. But there was more…
• If I started veering low, my bionic pancreas figured it out and gave me the perfect amount of glucagon to make sure that hypoglycemia didn’t occur
• I always felt safe during the week – at no time did I feel threatened or scared
• My glucoses were being watched and stayed perfectly in range overnight, every night. Wow.
• I counted zero carbs• I never “corrected”• I never thought about insulin
sensitivity and how I couldn’t figure that out
• I never thought about insulin to carb ratios
• I never bolused• I was a nicer and kinder person the
entire week with the bionic pancreas

Results:There were 328 patients, caregivers, and care partners who generated 3347 tweets. One overarching theme, OpenAPS changes lives, and five subthemes emerged from the data: (1) OpenAPS use suggests self-reported A1C and glucose variability improvement, (2) OpenAPS improves sense of diabetes burden and quality of life, (3) OpenAPS is perceived as safe, (4) patient/caregiver–provider interaction related to OpenAPS, and (5) technology adaptation for user needs.
Conclusions:As users of a patient-driven technology, OpenAPS users are self-reporting improved A1C, day-to-day glucose levels, and quality of life. Safety features important to individuals with diabetes are perceived to be embedded into OpenAPS technology. Twitter analysis provides insight on a patient population driving an innovative solution to improve their quality of diabetes care.
Twitter Analysis of #OpenAPS DIY Artificial Pancreas Technology Use Suggests Improved A1C and Quality of Life
Article first published online: September 10, 2018 https://doi.org/10.1177/1932296818795705
Background:Patient-driven innovation in diabetes management has resulted in a group of people with type 1 diabetes who choose to build and share knowledge around a do-it-yourself (DIY) open source artificial pancreas systems (OpenAPS). The purpose of this study was to examine Twitter data to understand how patients, caregivers, and care partners perceive OpenAPS, the personal and emotional ramifications of using OpenAPS, and the influence of OpenAPS on daily life.
Methods:Qualitative netnography was used to analyze #OpenAPS on Twitter over a two-year period.

Not Interested in Wearing a Pump?

Connected Insulin Pens

Pen Based Decision Support Merging Insulin Pen, CGM and Activity data
Can provide dosing decision support, hypoglycemia predictions, proactive alerts, exercise advice
Cloud Based Computing

What Does the Future Hold?
1. Bi-Hormonal systems in a single unit.2. Apps for smart phones to combine CGM, Smart Pen, Smart Watch
exercise data and maybe even to estimate nutrient content from food picture to suggest bolus dose.
3. Implantable systems with glucose sensing and insulin delivery to the portal system.
4. In hospital CGM and automated insulin delivery.5. ????
However we need to remember……

The Dumbest Beta Cells are Still Smarter than Endocrinologists and
their Technologies

Type 2 Diabetes Treatment Algorithm Changes from Results of CVOTs



ADA Glycemic Control Algorithm

Timings represent estimated completion dates as per ClinicalTrials.gov
1. Johansen OE. 20152. White WB et al. 20133. Scirica BM et al. 2013 4. Green JB et al. 20155. Pfeffer MA et al. 2015
6. ORIGIN. 20127. Zinman B et al. 20158. Marso SP et al. 20169. Marso SP et al. 201610. NCT01455896
11. Marso SP et al. 201712. Neal B et al. 201713. NCT0114433814. NCT0189753215. NCT02465515
16. NCT0206579117. Gerstein HC et al. 201718. NCT02692716 19. NCT0247939920. NCT00700856
21. NCT0124342422. NCT0173053423. NCT01394952 24. NCT01986881
Overview of CVOTs of Glucose-lowering Drugs1 (1 of 2)
Copyright © 2017 Eli Lilly and Company
PIONEER 618
(n=~3176)3P-MACE
TOSCA IT20
(n=~3371)4P-MACE
ORIGIN6
(n=12,537)3P-MACE
2013 2015 2016 2017 2018 2019 2020
SAVOR-TIMI 533
(n=16,492)1222 3P-MACE
EXAMINE2
(n=5380)621 3P-MACE
TECOS4
(n=14,671)≥1300 4P-MACE
LEADER8
(n=9341)≥611 3P-MACE
DECLARE-TIMI 5822
(n=~17,150)≥1390 3P-MACE
EMPA-REG OUTCOME7
(n=7028)≥691 3P-MACE
CREDENCE23
(n=~4200)Renal + 5P-MACE
CAROLINA21
(n=~6041)≥631 4P-MACE
FREEDOM CVO10
(n=4156)4P-MACE
VERTIS CV Study24
(n=~8000)3P-MACE
CARMELINA14
(n=~7053)4P-MACE + renal
REWIND16,17
(n=9901)≥1200 3P-MACE
ELIXA5
(n=6068)≥805 4P-MACE
STELLA-LONG TERM19
(n=~11,412)3P-MACE + Tumors
HARMONY Outcomes15
(n=~9400) 3P-MACE
DPP-4i
SGLT-2i
GLP1 RA
Insulin
TZD
Oral GLP1 RA
DEVOTE11
(n=7637)3P-MACE
CANVAS-R12
(n=5812)Albuminuria
CANVAS12
(n=4330)≥420 3P-MACE
EXSCEL13
(n=>14,000)≥1591 3P-MACE
SUSTAIN-69
(n=3297)3P-MACE

Timings represent estimated completion dates as per ClinicalTrials.gov
1. Johansen OE. 20152. White WB et al. 20133. Scirica BM et al. 2013 4. Green JB et al. 20155. Pfeffer MA et al. 2015
6. ORIGIN. 20127. Zinman B et al. 20158. Marso SP et al. 20169. Marso SP et al. 201610. NCT01455896
11. Marso SP et al. 201712. Neal B et al. 201713. NCT0114433814. NCT0189753215. NCT02465515
16. Gerstein HC et al. 201717. NCT01394952 18. NCT02692716 19. NCT0247939920. NCT00700856
21. NCT0124342422. NCT0173053423. NCT0206579124. NCT01986881
Overview of CVOTs of Glucose-lowering Drugs1 (2 of 2)
Copyright © 2017 Eli Lilly and Company
VERTIS CV Study24
(n=~8000)3P-MACE
REWIND16,17
(n=9901)≥1200 3P-MACE
STELLA-LONG TERM19
(n=~11,412)3P-MACE + Tumors
DPP-4i
SGLT-2i
GLP1 RA
Study not yet completed
Insulin
PIONEER 618
(n=~3176)3P-MACE
TOSCA IT20
(n=~3371)4P-MACE
ORIGIN6
(n=12,537)3P-MACE
2013 2015 2016 2017 2018 2019 2020
SAVOR-TIMI 533
(n=16,492)1222 3P-MACE
EXAMINE2
(n=5380)621 3P-MACE
TECOS4
(n=14,671)≥1300 4P-MACE
LEADER8
(n=9341)≥611 3P-MACE
DECLARE-TIMI 5822
(n=~17,150)≥1390 3P-MACE
EMPA-REG OUTCOME7
(n=7028)≥691 3P-MACE
CREDENCE23
(n=~4200)Renal + 5P-MACE
CAROLINA21
(n=~6041)≥631 4P-MACE
FREEDOM CVO10
(n=4156)4P-MACE
CARMELINA14
(n=~8300)4P-MACE + renal
ELIXA5
(n=6068)≥805 4P-MACE
HARMONY Outcomes15
(n=~9400) 3P-MACE
DEVOTE11
(n=7637)3P-MACE
CANVAS-R12
(n=5812)Albuminuria
CANVAS12
(n=4330)≥420 3P-MACE
SUSTAIN-69
(n=3297)3P-MACE
EXSCEL13
(n=>14,000)≥1591 3P-MACE

aTwo-sided tests for superiority were conducted (statistical significance was indicated if p≤.0498); bIntegrated analysis of CANVAS and CANVAS-R studiescEstimated study completion per clinicaltrials.govClick on the study title to view additional details regarding each study
Study Identifier No. of Patients Study DesignPrimary
EndpointResults
HR (95% CI)
EMPA-REG OUTCOME1
CVD; HbA1c ≥7.0-10.0%7028
EmpagliflozinPlacebo
3P-MACE0.86 (0.74, 0.99)
p=.04a (superiority)
CANVAS2
High risk/history of CV eventHbA1c 7.0-10.5%
4330Canagliflozin 100 mgCanagliflozin 300 mgPlacebo
3P-MACE
0.86 (0.75-0.97)b
p=.02 (superiority)CANVAS-R2
High risk/history of CV eventHbA1c ≥7.0-≤10.5%
5812Canagliflozin (100 or 300 mg)Placebo
Progression of albuminuria
STELLA LONGTERM3
First ipragliflozin use (July 2014-July 2015)
~11,412Ipragliflozin(Observational study)
CV AEs and malignant tumors
2018c
DECLARE-TIMI 584
CVD~17,150
DapagliflozinPlacebo
3P-MACE 2019c
CREDENCE5
CKD; HbA1c 6.5-12.0%~4200
CanagliflozinPlacebo
ESRD, doubling of sCR,or renal/CV death
2019c
VERTIS CV Study6
Vascular diseaseHbA1c 7.0-10.5%
~8000Ertugliflozin 5 mgErtugliflozin 15 mgPlacebo
3P-MACE 2019c
1. Zinman B et al. N Engl J Med 2015;373:2117-282. Neal B et al. N Engl J Med 2017;Ahead of print3. https://clinicaltrials.gov/ct2/show/NCT02479399
4. https://clinicaltrials.gov/ct2/show/NCT017305345. https://clinicaltrials.gov/ct2/show/NCT020657916. https://clinicaltrials.gov/ct2/show/NCT01986881
Cardiovascular Outcome Trials for SGLT-2 Inhibitors
Copyright © 2017 Eli Lilly and Company
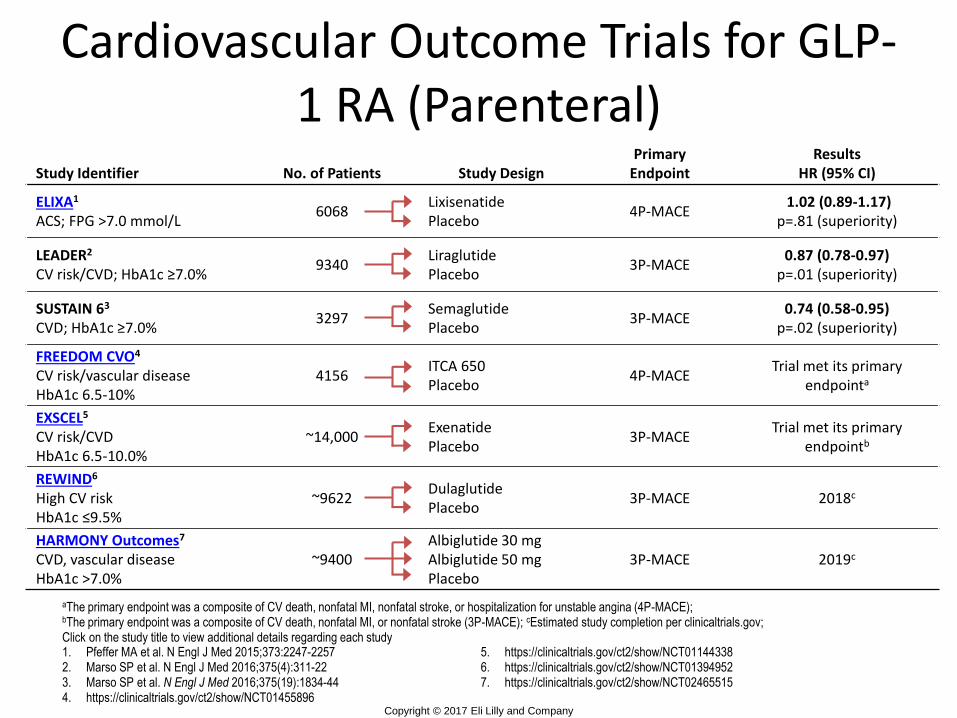
Study Identifier No. of Patients Study DesignPrimary
EndpointResults
HR (95% CI)
ELIXA1
ACS; FPG >7.0 mmol/L6068
LixisenatidePlacebo
4P-MACE1.02 (0.89-1.17)
p=.81 (superiority)
LEADER2
CV risk/CVD; HbA1c ≥7.0%9340
LiraglutidePlacebo
3P-MACE0.87 (0.78-0.97)
p=.01 (superiority)
SUSTAIN 63
CVD; HbA1c ≥7.0%3297
SemaglutidePlacebo
3P-MACE0.74 (0.58-0.95)
p=.02 (superiority)
FREEDOM CVO4
CV risk/vascular diseaseHbA1c 6.5-10%
4156ITCA 650Placebo
4P-MACETrial met its primary
endpointa
EXSCEL5
CV risk/CVDHbA1c 6.5-10.0%
~14,000ExenatidePlacebo
3P-MACETrial met its primary
endpointb
REWIND6
High CV riskHbA1c ≤9.5%
~9622DulaglutidePlacebo
3P-MACE 2018c
HARMONY Outcomes7
CVD, vascular diseaseHbA1c >7.0%
~9400Albiglutide 30 mgAlbiglutide 50 mgPlacebo
3P-MACE 2019c
aThe primary endpoint was a composite of CV death, nonfatal MI, nonfatal stroke, or hospitalization for unstable angina (4P-MACE);bThe primary endpoint was a composite of CV death, nonfatal MI, or nonfatal stroke (3P-MACE); cEstimated study completion per clinicaltrials.gov; Click on the study title to view additional details regarding each study1. Pfeffer MA et al. N Engl J Med 2015;373:2247-22572. Marso SP et al. N Engl J Med 2016;375(4):311-223. Marso SP et al. N Engl J Med 2016;375(19):1834-444. https://clinicaltrials.gov/ct2/show/NCT01455896
5. https://clinicaltrials.gov/ct2/show/NCT011443386. https://clinicaltrials.gov/ct2/show/NCT013949527. https://clinicaltrials.gov/ct2/show/NCT02465515
Cardiovascular Outcome Trials for GLP-1 RA (Parenteral)
Copyright © 2017 Eli Lilly and Company

ORLANDO — The treatment approach to type 2 diabetes should begin with an assessment of cardiovascular disease (CVD) status, other comorbidities, and patient preferences, according to a draft of the upcoming 2018 joint consensus statement from the American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD).
The final version of the 2018 update to the current 2015 ADA/EASD Management of Hyperglycemia in Type 2 Diabetes statement (Diabetes Care. 2015;38:140-149) will be presented on October 5, 2018 at the EASD annual meeting in Berlin and will be published in Diabetes Care and Diabetologia.
The statement will aim to help clinicians navigate the increasingly complex options for management of hyperglycemia in type 2 diabetes, with particular emphasis on data published since 2014, including those suggesting cardiovascular benefit for the sodium-glucose cotransport-2 (SGLT2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists.
ADA/EASD Consensus Statement

ADA Updated Glycemic Control Algorithm


andEmpower Our Patients to Control Their
Diabetes and Not Let Diabetes Control Them
Thank You!
Questions?
Remember as Physicians we need to……
Combine High Tech with High Touch!