what is copd quality of care program · 2018-08-01 · copd : thai guideline 2560 non-...
TRANSCRIPT
What is COPD quality of care program?
KITTIMA BANGPATTANASIRI, MD.
CENTRAL CHEST INSTITUTE OF THAILAND
COPD : definition
►Chronic Obstructive Pulmonary Disease (COPD) is a
common, preventable and treatable disease that is
characterized by persistent respiratory symptoms and airflow
limitation that is due to airway and/or alveolar abnormalities
usually caused by significant exposure to noxious particles or
gases.
© 2018 Global Initiative for Chronic Obstructive Lung Disease
© 2017 Global Initiative for Chronic Obstructive Lung Disease
► COPD is currently the fourth leading cause of death in the world.1
► COPD is projected to be the 3rd leading cause of death by 2020.2
► More than 3 million people died of COPD in 2012 accounting for 6% of all deaths
globally.
► Globally, the COPD burden is projected to increase in coming decades because of
continued exposure to COPD risk factors and aging of the population.
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;
380(9859): 2095-128.
2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006; 3(11): e442.
COPD : Burden of disease
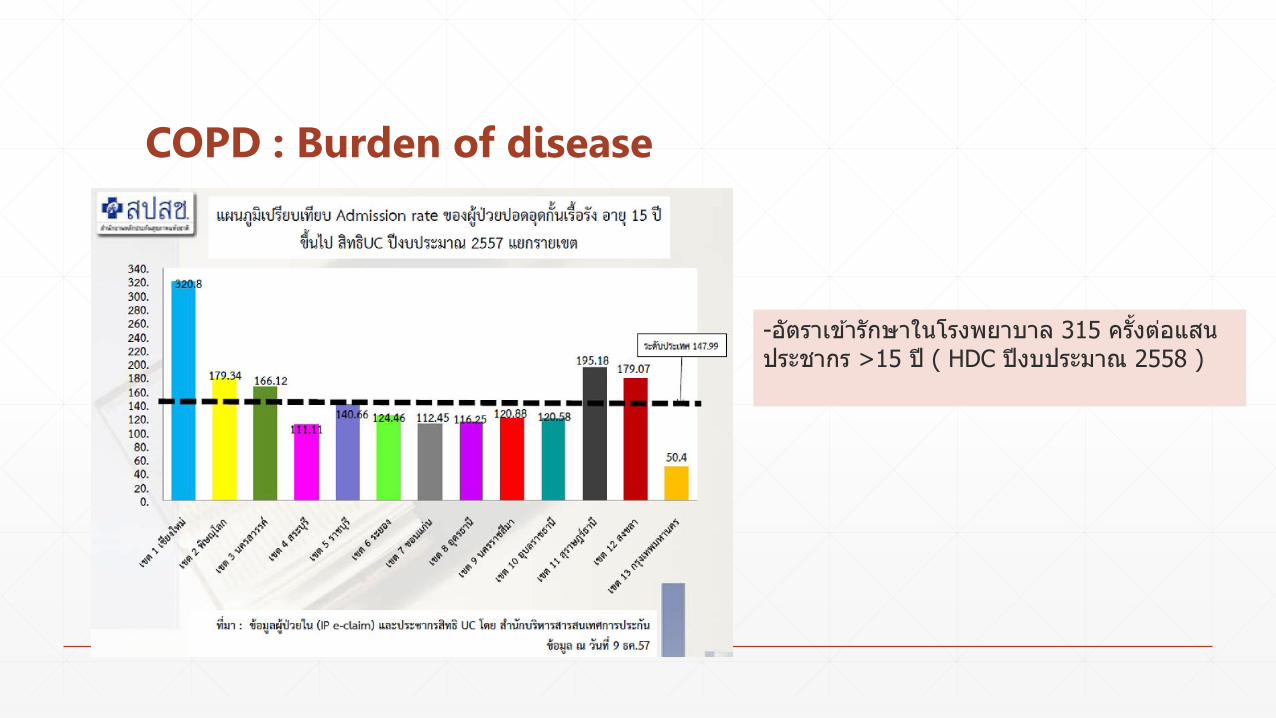
COPD : Burden of disease
-อตราเขารกษาในโรงพยาบาล 315 ครงตอแสนประชากร >15 ป ( HDC ปงบประมาณ 2558 )
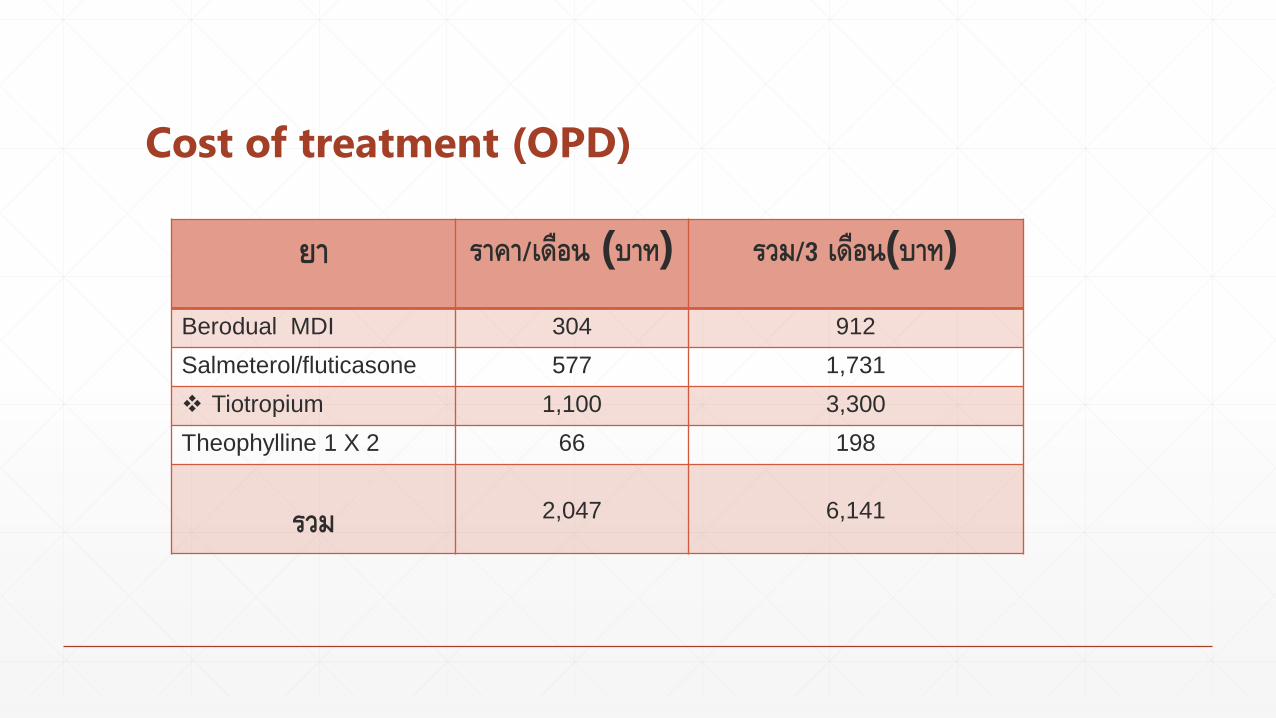
Cost of treatment (OPD)
ยา ราคา/เดอน (บาท) รวม/3 เดอน(บาท)
Berodual MDI 304 912
Salmeterol/fluticasone 577 1,731
Tiotropium 1,100 3,300
Theophylline 1 X 2 66 198
รวม 2,047 6,141
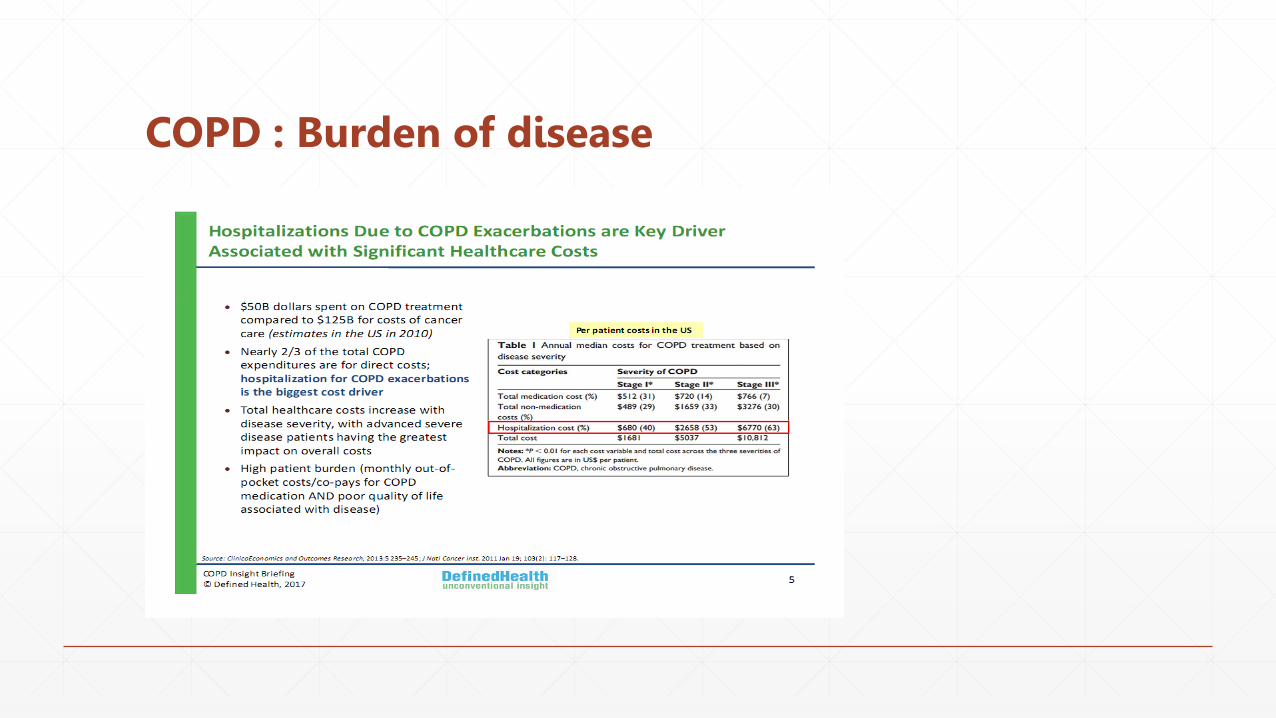
COPD : Burden of disease
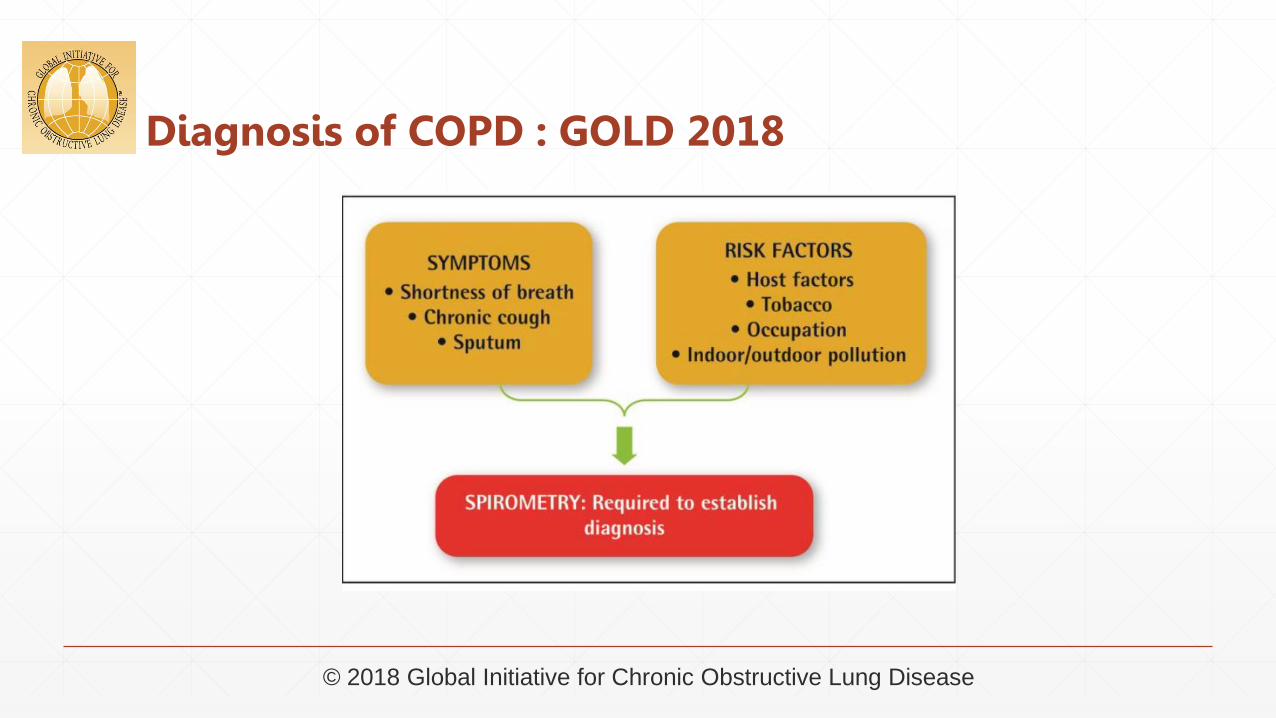
Diagnosis of COPD : GOLD 2018
© 2018 Global Initiative for Chronic Obstructive Lung Disease
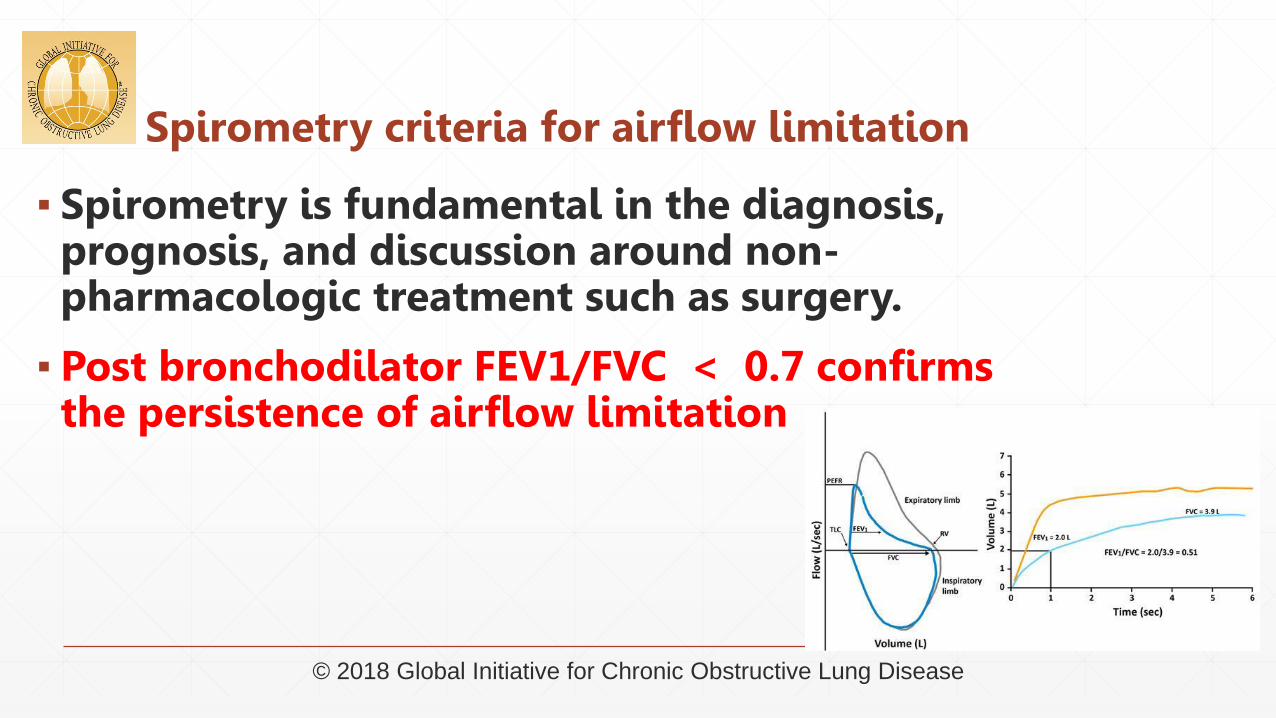
Spirometry criteria for airflow limitation
▪ Spirometry is fundamental in the diagnosis, prognosis, and discussion around non-pharmacologic treatment such as surgery.
▪ Post bronchodilator FEV1/FVC < 0.7 confirms the persistence of airflow limitation
© 2018 Global Initiative for Chronic Obstructive Lung Disease
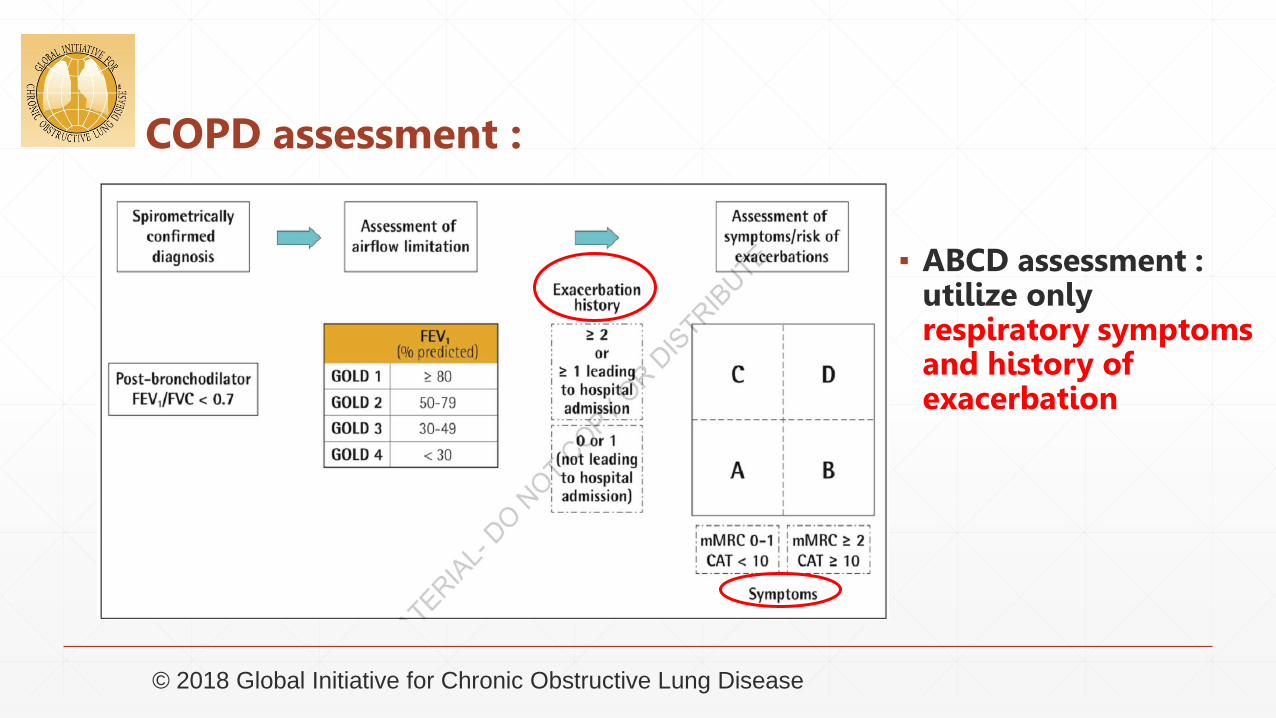
COPD assessment :
▪ ABCD assessment : utilize only respiratory symptoms and history of exacerbation
© 2018 Global Initiative for Chronic Obstructive Lung Disease
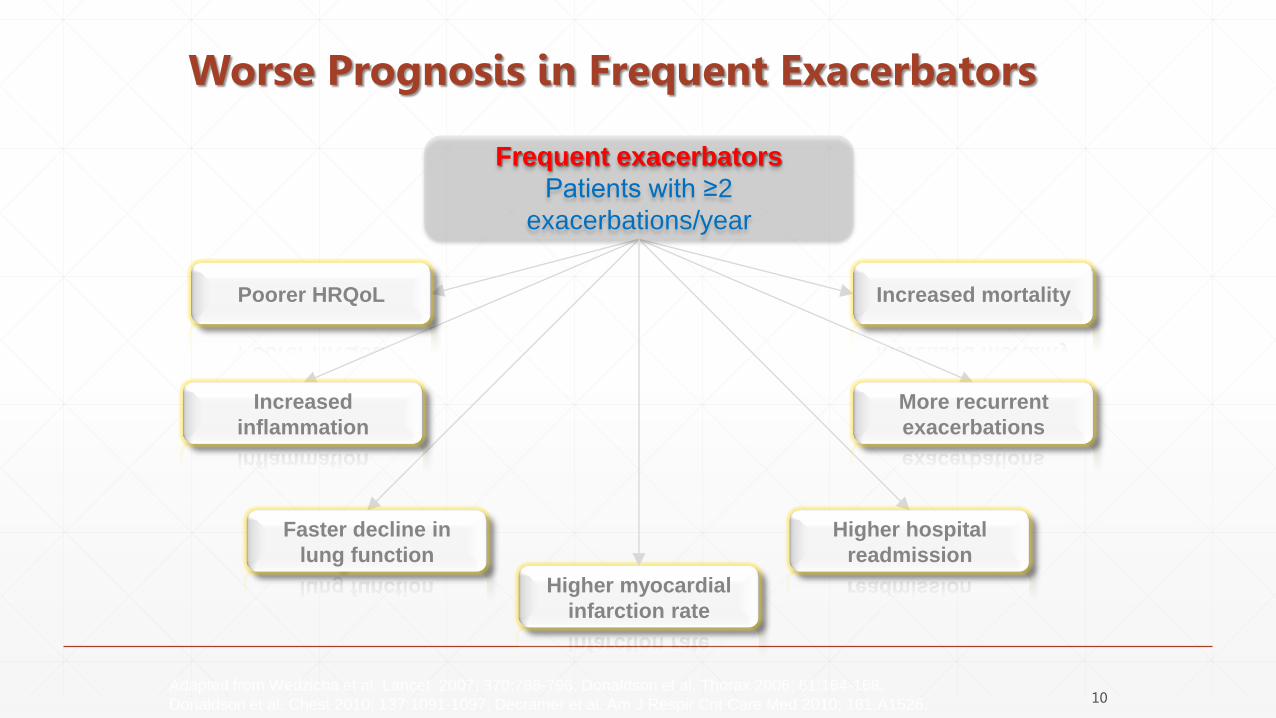
Adapted from Wedzicha et al. Lancet 2007; 370:786-796; Donaldson et al. Thorax 2006; 61:164-168;
Donaldson et al. Chest 2010; 137:1091-1097; Decramer et al. Am J Respir Crit Care Med 2010; 181:A1526.
Poorer HRQoL
Increased
inflammation
Faster decline in
lung function
Higher hospital
readmission
More recurrent
exacerbations
Increased mortality
Frequent exacerbators
Patients with ≥2
exacerbations/year
Higher myocardial
infarction rate
Worse Prognosis in Frequent Exacerbators
10
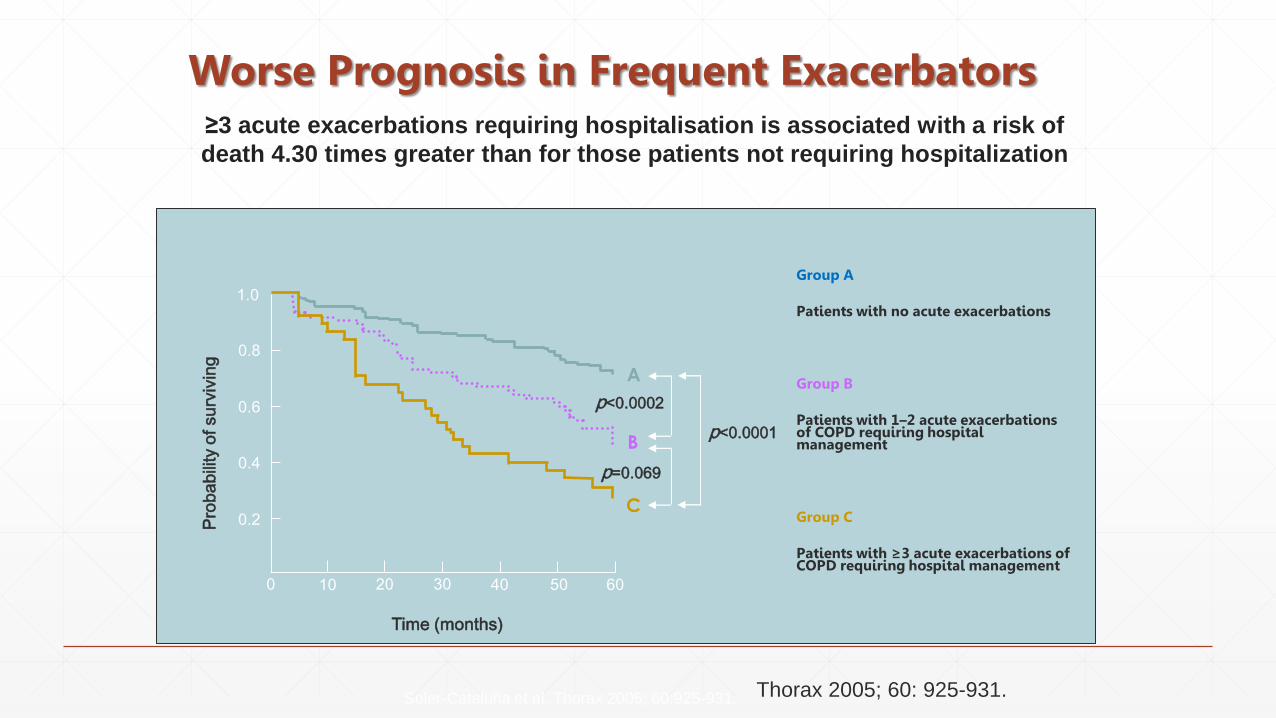
Group A
Patients with no acute exacerbations
Group B
Patients with 1–2 acute exacerbations of COPD requiring hospital management
Group C
Patients with ≥3 acute exacerbations of COPD requiring hospital management
Time (months)
0 10 20 30 40 50 60
0.2
0.4
0.6
0.8
1.0
Pro
babi
lity
of s
urvi
ving
p<0.0001
A
B
C
p=0.069
p<0.0002
Soler-Cataluña et al. Thorax 2005; 60:925-931.
≥3 acute exacerbations requiring hospitalisation is associated with a risk of
death 4.30 times greater than for those patients not requiring hospitalization
Worse Prognosis in Frequent Exacerbators
Thorax 2005; 60: 925-931.

Prevention of COPD exacerbations : ERS/ATS
▪ Pharmacological▪ Mucolytics
▪ LABA/LAMA
▪ Roflumilast
▪ macrolide
Prevention of COPD exacerbations : Pharmacological treatment
▪ Mucolytics
▪ Reduce exacerbation , high dose (N-acetylcysteine), moderate – severe COPD
▪ No effect on mortality
Prevention of COPD exacerbations : Pharmacological treatment
▪ LAMAs or LABAs
▪ Tiotropium (LAMA) vs indacaterol (LABA) / Tiotropium vs Salmeterol
(moderate to severe COPD)
▪ Less exacerbations in LAMA ( 30.9% vs 34.6% ; risk ratio 0.89 , 95% CI 0.85-0.94)
▪ Fewer severe adverse effects
▪ No different in mortality
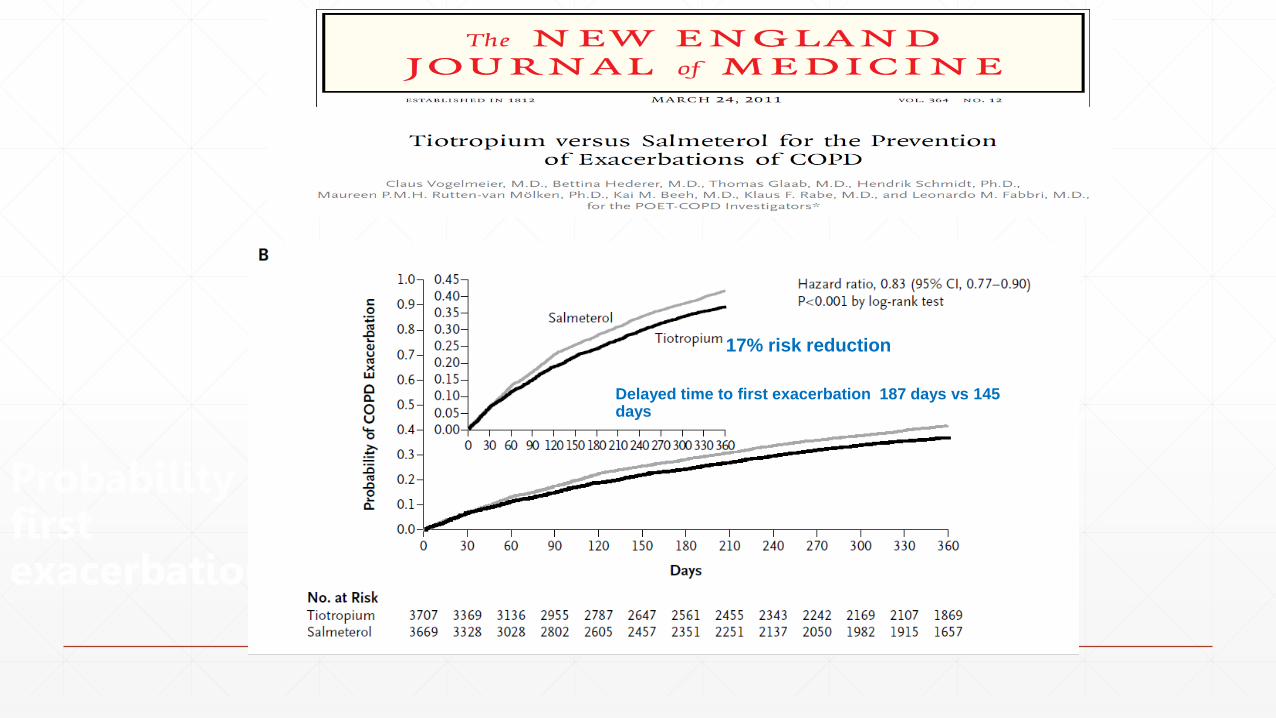
Probability of a first exacerbation
17% risk reduction
Delayed time to first exacerbation 187 days vs 145 days
Prevention of COPD exacerbations : Pharmacological treatment
▪ Roflumilast
▪ Decreased number of moderate to severe exacerbations per patient-year (rate ratio 0.85; 95% CI 0.78-0.91) in moderate –severe COPD with chronic bronchitis
▪ No effect on mortality
▪ Adverse effect : diarrhea, weight loss, nausea, anxiety and depression
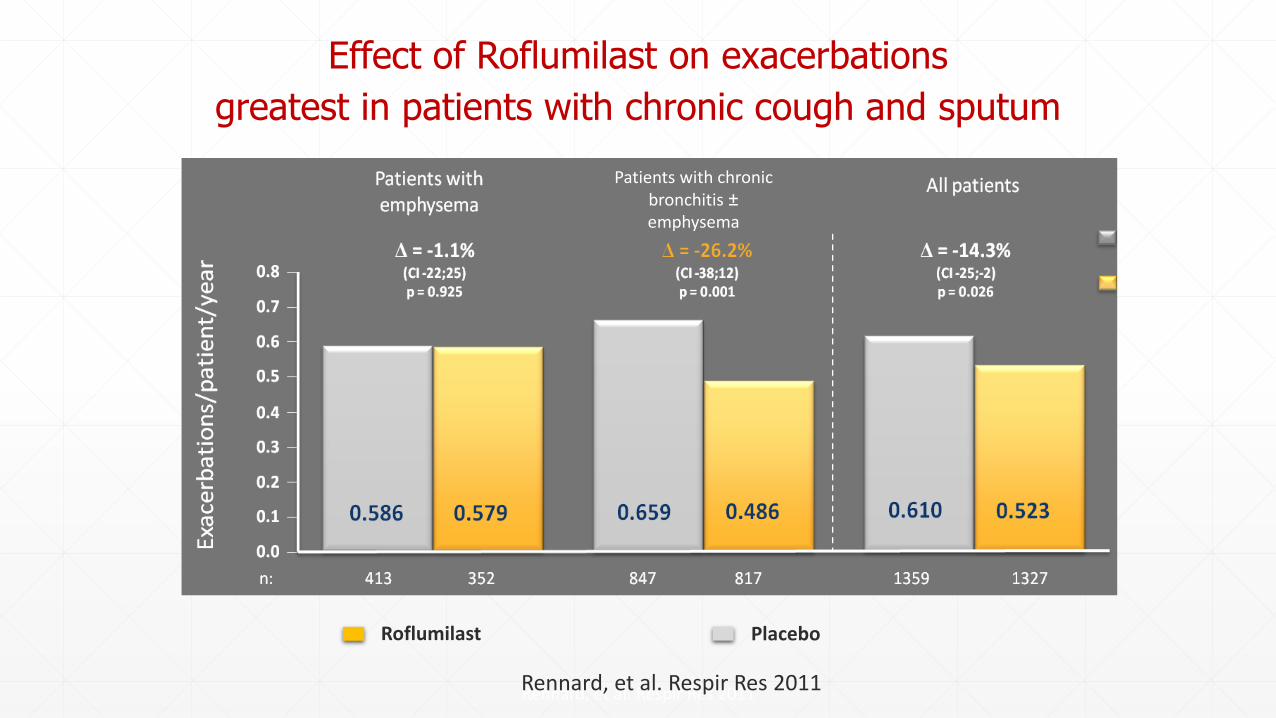
Rennard, et al. Respir Res 2011
Effect of Roflumilast on exacerbations
greatest in patients with chronic cough and sputum
Patients with chronic bronchitis ±emphysema
PlaceboRoflumilast
Rennard, et al. Respir Res 2011
Prevention of COPD exacerbations : Pharmacological treatment
▪ Macrolide
▪ Decreased rate of COPD exacerbations (rate ratio 0.76; 95% CI 0.68-0.86)
▪ Increased time to first exacerbation
▪ Improved quality of life
▪ No effect on mortality
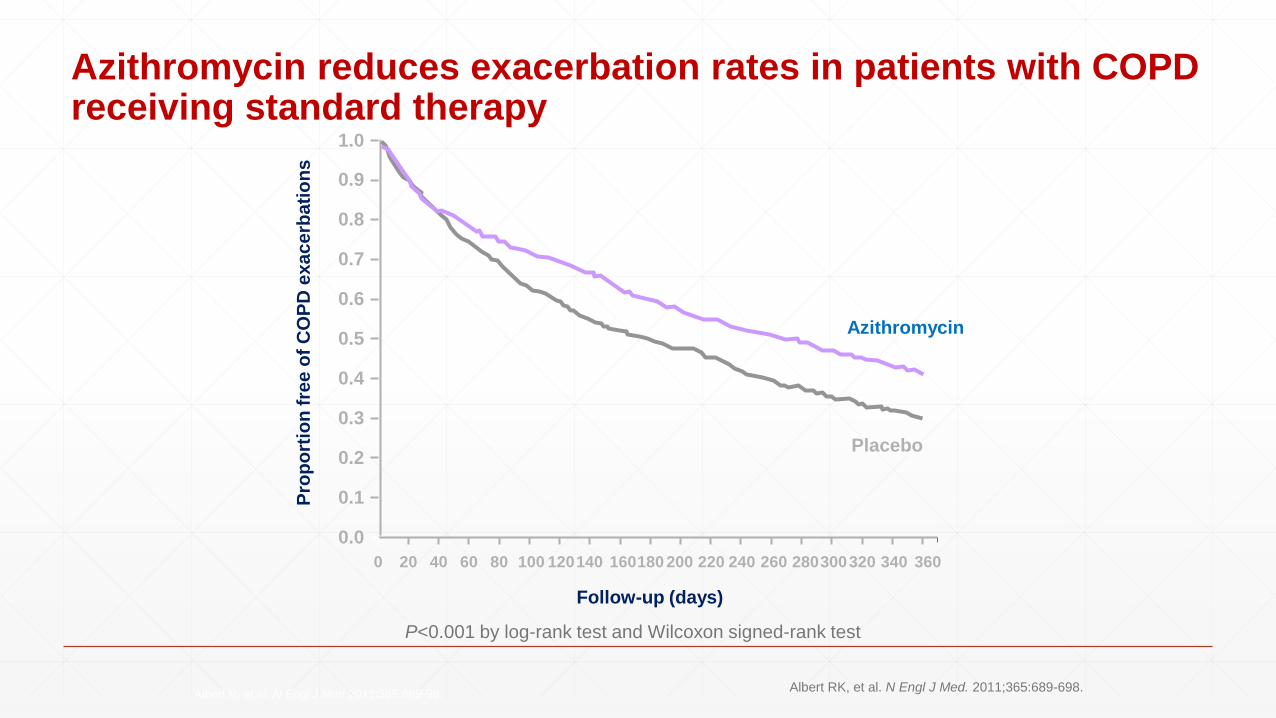
Azithromycin reduces exacerbation rates in patients with COPD receiving standard therapy
Albert R. et al. N Engl J Med 2011;365:689-98.
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
0 20 40 60 80 100 120140 160180 200 220 240 260 280300320 340 360
Follow-up (days)
Pro
po
rtio
n f
ree
of
CO
PD
ex
ac
erb
ati
on
s
P<0.001 by log-rank test and Wilcoxon signed-rank test
Azithromycin
Placebo
Albert RK, et al. N Engl J Med. 2011;365:689-698.
Prevention of COPD exacerbations : Non -pharmacological treatment
▪ Smoking cessation
▪ Pulmonary rehabilitation
▪ reduce symptoms, improve functional capacity and increase patient participation Studies indicate that it also may reduce the frequency and duration of subsequent exacerbations
▪ Rehabilitation delivered in the post-acute recovery stage may also reduce the risk of readmissions and even mortality
▪ Influenza vaccine
▪ rate of hospitalizations due to influenza and pneumonia was significantly reduced (adjusted risk ratio 0.48, p=0.008), as was risk of death (adjusted odds ratio 0.30, p<0.001)
▪ up to 50% of exacerbations are related to viral infections,
ERJ Open Research 2015 1: 00011-2015
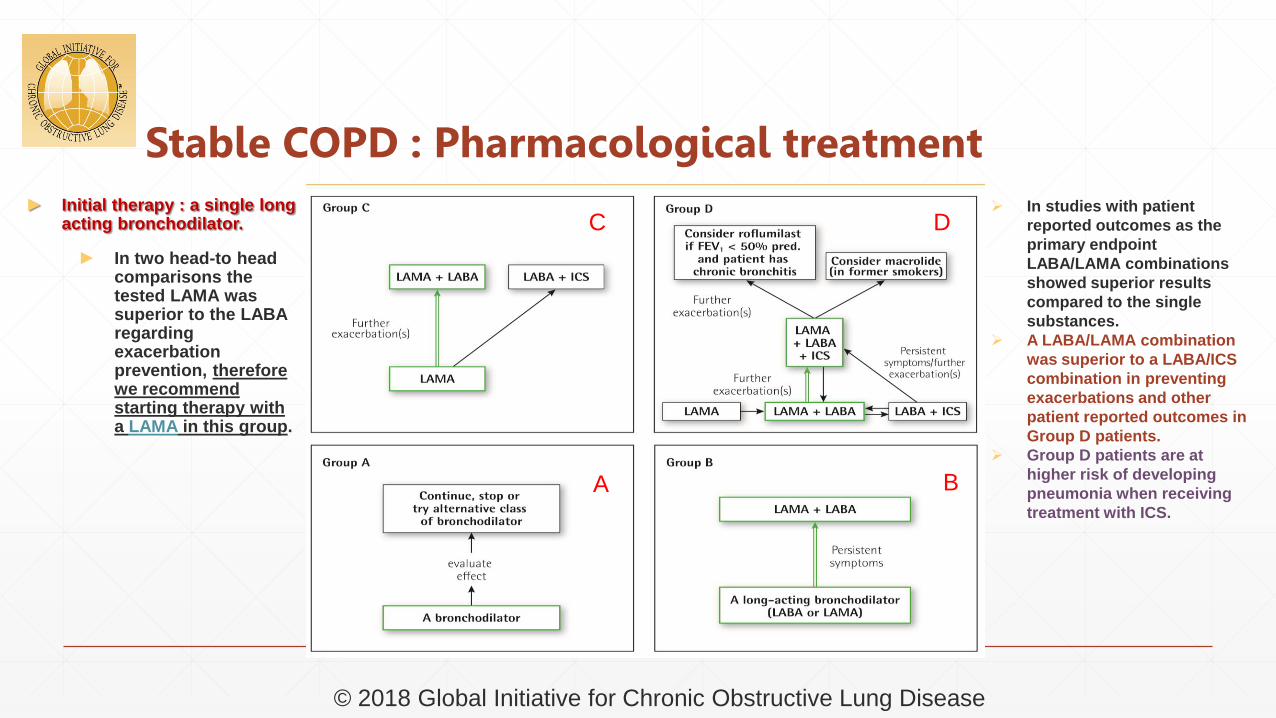
Stable COPD : Pharmacological treatment
© 2018 Global Initiative for Chronic Obstructive Lung Disease
► Initial therapy : a single long acting bronchodilator.
► In two head-to head comparisons the tested LAMA was superior to the LABA regarding exacerbation prevention, therefore we recommend starting therapy with a LAMA in this group.
In studies with patient
reported outcomes as the
primary endpoint
LABA/LAMA combinations
showed superior results
compared to the single
substances.
A LABA/LAMA combination
was superior to a LABA/ICS
combination in preventing
exacerbations and other
patient reported outcomes in
Group D patients.
Group D patients are at
higher risk of developing
pneumonia when receiving
treatment with ICS.
A B
C D
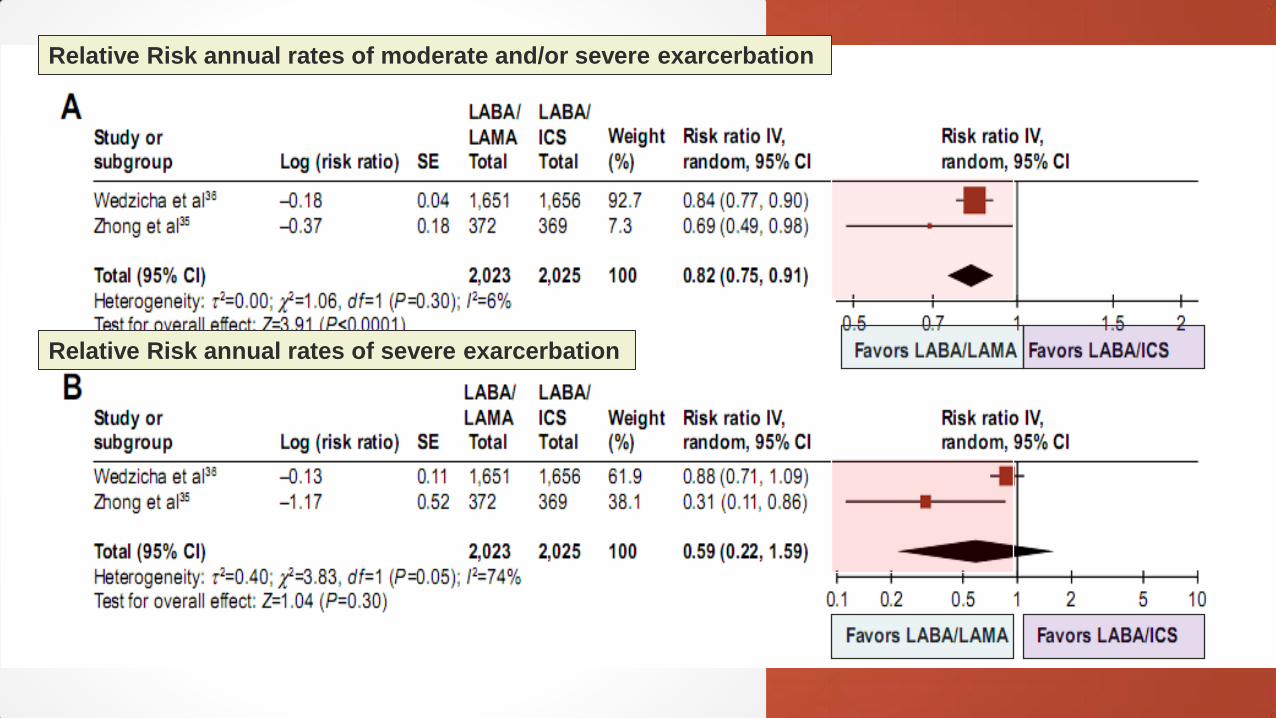
Relative Risk annual rates of moderate and/or severe exarcerbation
Relative Risk annual rates of severe exarcerbation
Stable COPD : non-pharmacological treatment ►Education and self-management
►Physical activity
►Pulmonary rehabilitation programs
►Exercise training
►Self-management education
►End of life and palliative care
►Nutritional support
►Vaccination
►Oxygen therapy
© 2018 Global Initiative for Chronic Obstructive Lung Disease
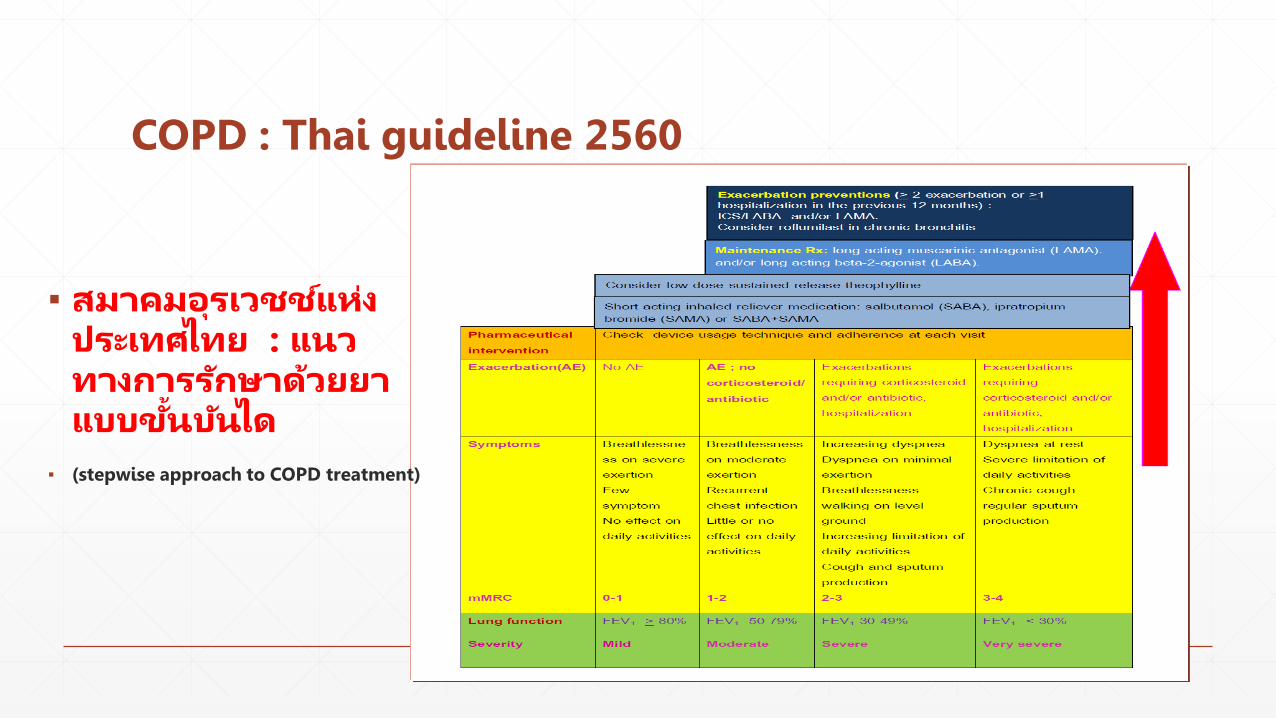
COPD : Thai guideline 2560
▪ สมาคมอรเวชชแหงประเทศไทย : แนวทางการรกษาดวยยาแบบข นบนได
▪ (stepwise approach to COPD treatment)
COPD : Thai guideline 2560non- pharmacological treatment
▪ Smoking cessation
▪ ใหผปวยรบวคซนปองกนไขหวดใหญ (influenza vaccine) ปละ 1 ครง และแนะน าประโยชนของการรบวคซนปองกนปอดอกเสบ (pneumococcal vaccine)
▪ เรมโปรแกรมฟนฟสมรรถภาพปอด (pulmonary rehabilitation) ในผปวยกลมอาการปานกลาง(moderate)ขนไป
▪ ในผปวยกลมอาการรนแรง (severe) ขนไป
- long term oxygen therapy
- แนะน าทางเลอกในการรกษาโดยการผาตด (lung volume reduction surgery – LVRS) ในผปวยทมขอบงช
- End of life care
Thai thoracic society
COPD : monitoring and follow up ▪ Monitoring disease progression and development of complications and/or
comorbidities
► Measurements. Decline in FEV1 can be tracked by spirometry performed at least once a year.
► Symptoms. At each visit, information on symptoms since the last visit should be collected, including cough and sputum, breathlessness, fatigue, activity limitation, and sleep disturbances.
► Exacerbations. The frequency, severity, type and likely causes of all exacerbations should be monitored.
► Imaging. If there is a clear worsening of symptoms, imaging may be indicated.
► Smoking status. At each visit, the current smoking status and smoke exposure should be determined followed by appropriate action.
© 2018 Global Initiative for Chronic Obstructive Lung Disease

COPD : monitoring and follow up
▪ Pharmacotherapy and other medical treatment
▪ In order to adjust therapy appropriately as the disease progresses, each follow-up visit should include a discussion of the current therapeutic regimen.
▪ Monitoring should focus on:
► Dosages of prescribed medications.
► Adherence to the regimen.
► Inhaler technique.
► Effectiveness of the current regimen.
► Side effects.
© 2018 Global Initiative for Chronic Obstructive Lung Disease
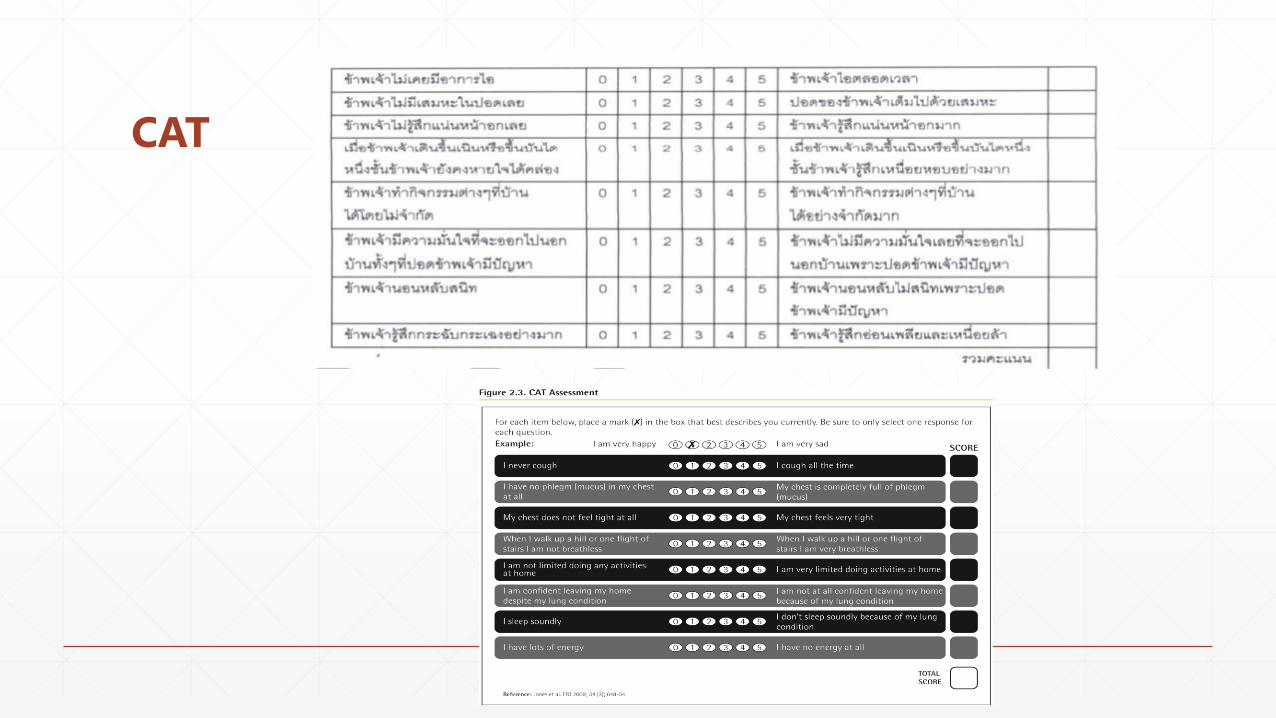
CAT

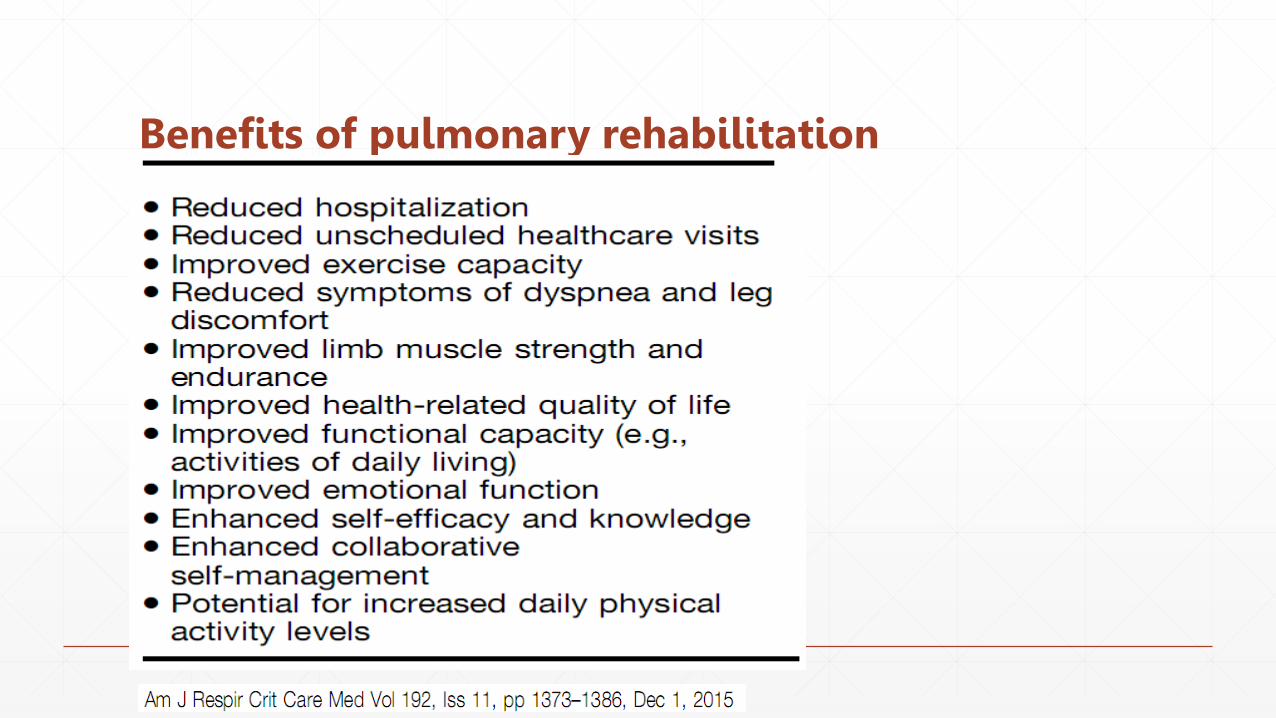
Benefits of pulmonary rehabilitation
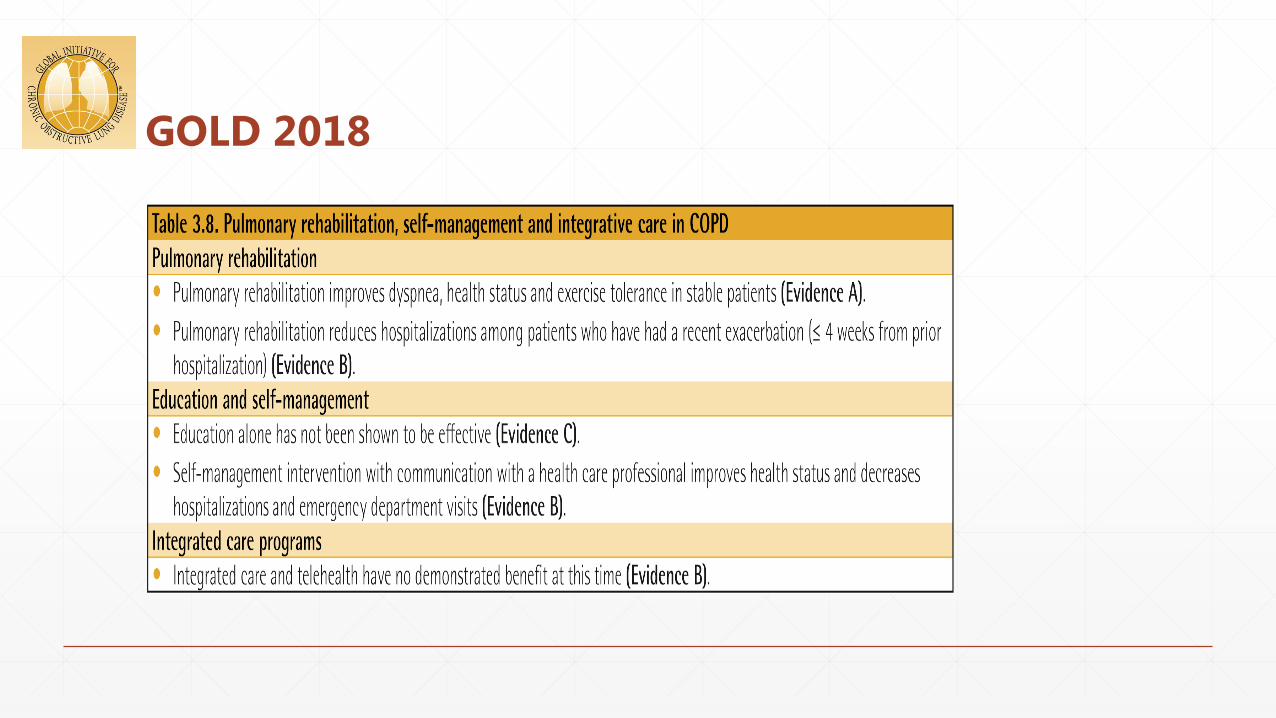
GOLD 2018
GOLD 2018
▪ High risk patients : GOLD B, C, and D
▪ Time point to refer for pulmonary rehabilitation
▪ 1. at diagnosis
▪ 2. at discharge from hospital due to AE
▪ 3. deteriorated symptoms
GOLD 2018
▪ Program 6-8 weeks for optimum benefit
▪ Supervised exercise training twice weekly is recommended
▪ Regimen include endurance training, interval training, and resistance/strength training (upper and lower limbs exercise)
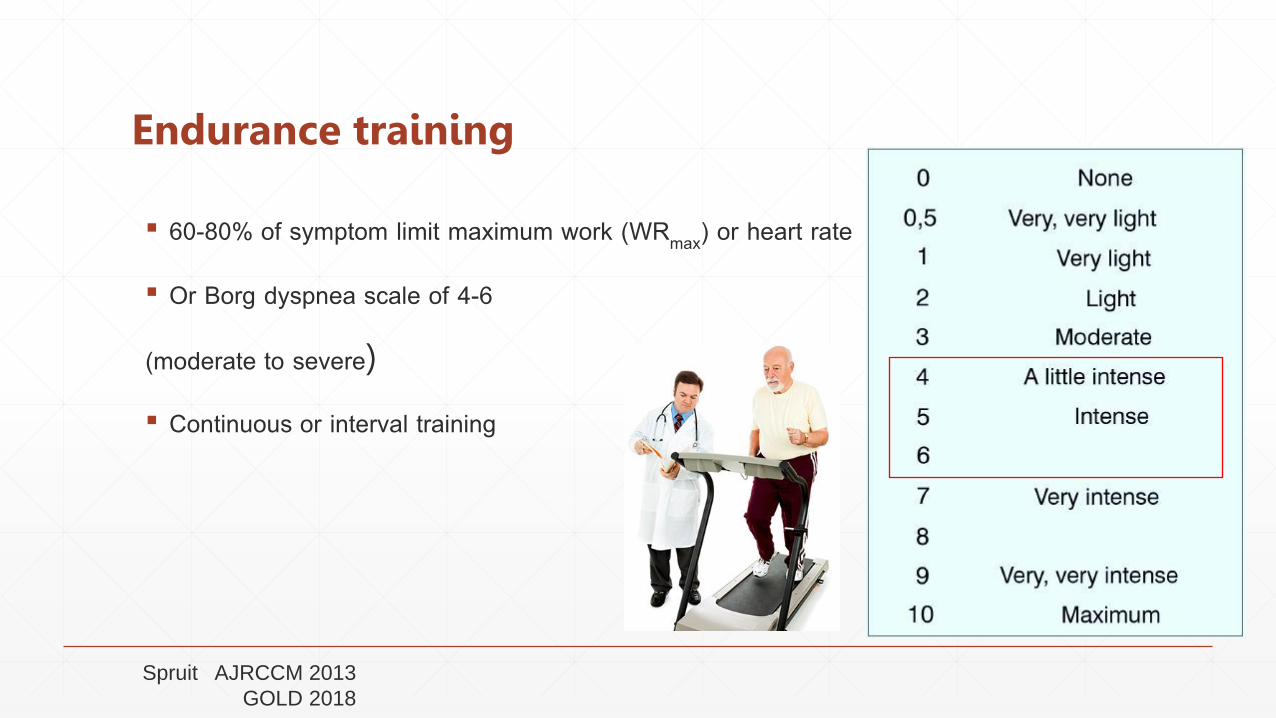
Endurance training
▪ 60-80% of symptom limit maximum work (WRmax) or heart rate
▪ Or Borg dyspnea scale of 4-6
(moderate to severe)
▪ Continuous or interval training
Spruit AJRCCM 2013
GOLD 2018

Endurance training: lower limb ▪ Walking training intensity: It is recommended that for walking
training a starting intensity should be 80% of the average 6MWT speed
▪ To calculate an appropriate intensity for walking laps: 80% ([6MWD ÷ 6] x prescribed duration)
▪ Six-minute walk distance (6MWD) ÷ 6 = Distance in one minute
▪ For distance in 30 minutes = one minute distance x 30
▪ For distance in 20 minutes = one minute distance x 20
▪ For distance in 10 minutes = one minute distance x 10 etc…
Example:
If the patient walked 220 m in six minutes:
One minute distance = 220 ÷ 6 = 36.7 m.
30 minute distance = 36.7 x 30 = 1100 m.
80% of 1100 = 880 m in 30 minutes.
2016 Lung Foundation Australia

Problems
▪ Diagnosis : under and over diagnosis
▪ Spirometry : บคลากร
: equipment
▪ Data base
▪ Treatment and prevention : guideline
▪ Pharmacological and non-pharmacological treatment
▪ Monitoring
▪ Smoking cessation
▪ Immunization

Service plan NCD : COPD
สภาพปญหา- เปนสาเหตการตายทส าคญของคนไทย- เปนผปวยทรบไวรกษามากเปนอนดบตนๆ โดยเฉพาะใน รพช.- คนไทยยงสบบหรเปนประจ า เกอบ 10 ลานคน-มอตราปวยแตกตางกนระหวางเขต (มากทเขตภาคเหนอ /ภาคใต )- อตราเขารกษาในโรงพยาบาล 315 ครงตอแสนประชากร >15 ป ( HDC ปงบประมาณ 2558 )
1. Service DeliveryCOPD clinic
- บรการ วนจฉย รกษา ฟนฟสภาพ โดยสหวชาชพ- ปฏบตตามมาตรฐานแนวปฏบตการรกษาโรคปอดอดกนเรอรง ป 2553- มระบบขนทะเบยน และตดตามการรกษาตอเนอง-บรการตรวจสมรรถภาพปอด ดวยเครอง Spirometry- มระบบเยยมบาน และ long term careบรการเพอการเลกบหร
เปาหมาย : ลดอตราการรบไวรกษาในโรงพยาบาล < 130
ตอแสนประชากร อาย > 15 ป
(baseline data 146.6 ตอแสนประชากร อาย > 15 ป สทธ UC ป 2556)
2.ขอมลการขนทะเบยนผปวย และผลการประเมนการรกษา3. บคลากรสหสาขาวชาชพ- แพทย พยาบาล เภสชกร นกกายภาพบ าบด4.งบประมาณ สนบสนน สถานทเครองมอ การอบรมเจาหนาท5. ยา/วคซน/เทคโนโลย- ยาขยายหลอดลมชนดออกฤทธยาว- วคซนไขหวดใหญตามฤดกาล- เครอง Spirometry (ควรมถงระดบ F1)6.การก ากบดแล ระดบเขต ระดบจงหวด และระดบ CUP7. การดแลผปวยในชมชน : long term care ใชออกซเจนระยะยาวทบาน
Six building blocks plusการตรวจราชการกระทรวงสาธารณสขคณะท 2 service plan ป 2559สาขา NCD (DM - HT - COPD)
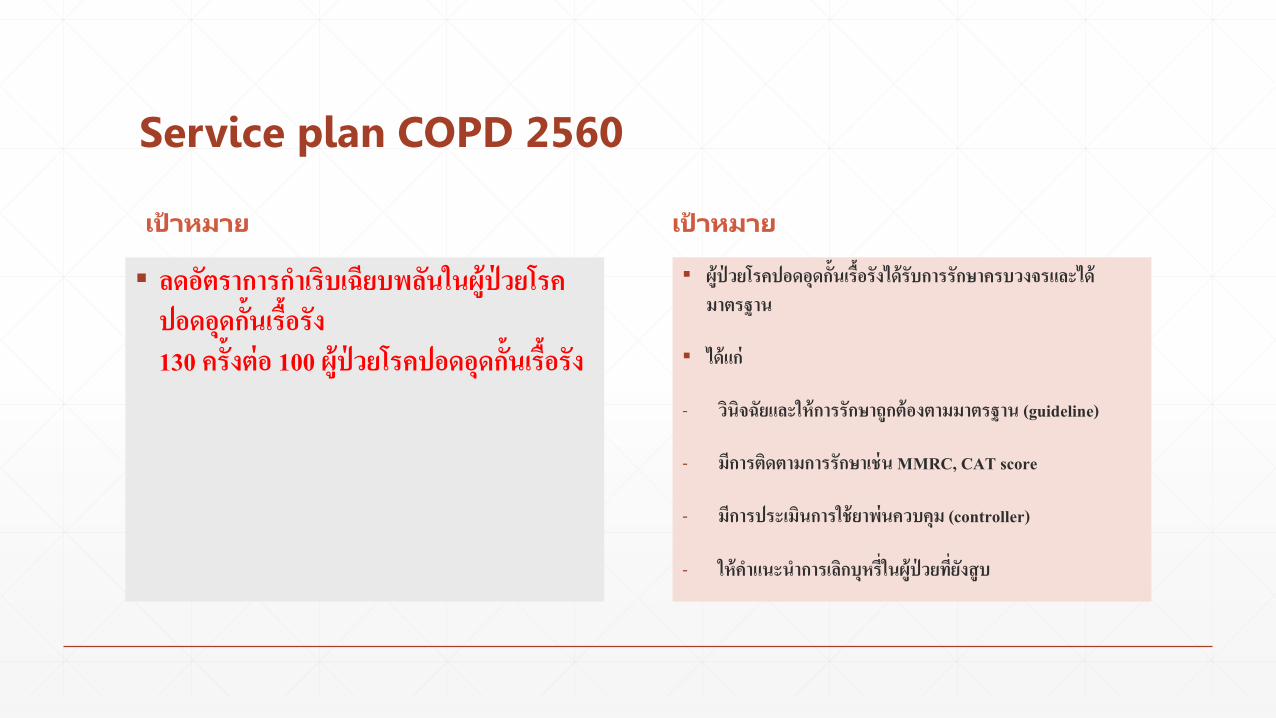
Service plan COPD 2560
เปาหมาย เปาหมาย
▪ ลดอตราการก าเรบเฉยบพลนในผปวยโรคปอดอดกนเรอรง 130 ครงตอ 100 ผปวยโรคปอดอดกนเรอรง
▪ ผปวยโรคปอดอดกนเรอรงไดรบการรกษาครบวงจรและไดมาตรฐาน
▪ ไดแก
- วนจฉยและใหการรกษาถกตองตามมาตรฐาน (guideline)
- มการตดตามการรกษาเชน MMRC, CAT score
- มการประเมนการใชยาพนควบคม (controller)
- ใหค าแนะน าการเลกบหรในผปวยทยงสบ
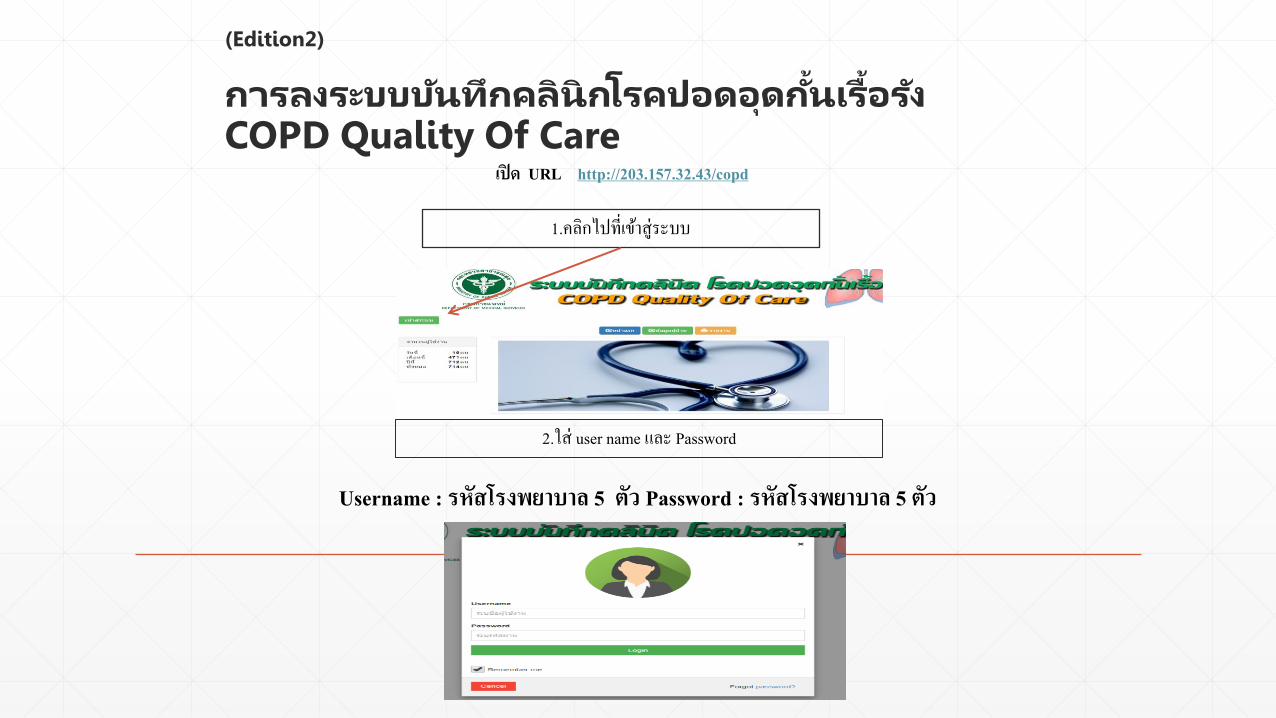
(Edition2)
การลงระบบบนทกคลนกโรคปอดอดก นเรอรงCOPD Quality Of Care เปด URL http://203.157.32.43/copd
1.คลกไปทเขาสระบบ
2.ใส user name และ Password
Username : รหสโรงพยาบาล 5 ตว Password : รหสโรงพยาบาล 5 ตว
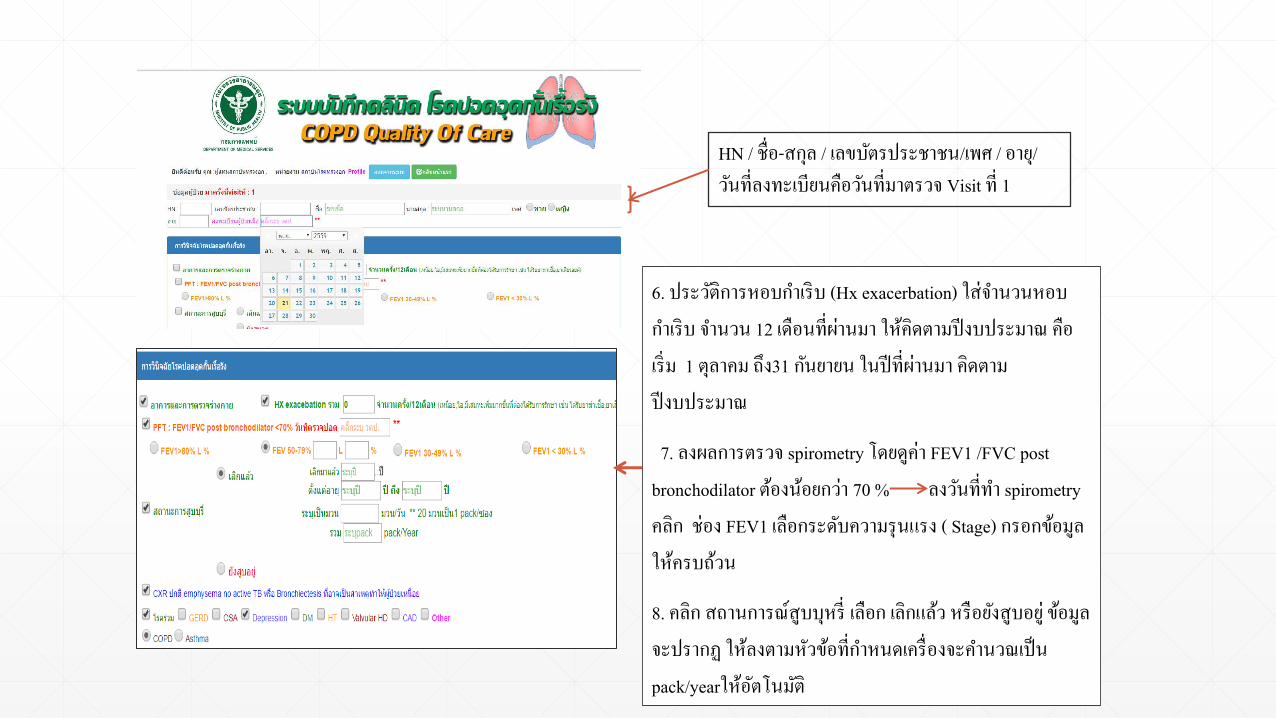
6. ประวตการหอบก าเรบ (Hx exacerbation) ใสจ านวนหอบก าเรบ จ านวน 12 เดอนทผานมา ใหคดตามปงบประมาณ คอเรม 1 ตลาคม ถง31 กนยายน ในปทผานมา คดตามปงบประมาณ
7. ลงผลการตรวจ spirometry โดยดคา FEV1 /FVC post bronchodilator ตองนอยกวา 70 % ลงวนทท า spirometryคลก ชอง FEV1 เลอกระดบความรนแรง ( Stage) กรอกขอมลใหครบถวน
8. คลก สถานการณสบบหร เลอก เลกแลว หรอยงสบอย ขอมลจะปรากฏ ใหลงตามหวขอทก าหนดเครองจะค านวณเปน pack/yearใหอตโนมต
HN / ชอ-สกล / เลขบตรประชาชน/เพศ / อาย/วนทลงทะเบยนคอวนทมาตรวจ Visit ท 1

9. คลก ตรงชองเอกซเรย (ผลปกต)10. คลก โรครวมในรายทมโรครวม11 . คลก ชอง COPD12 . คลก Dx COPD Type โดยใหเลอกเปนชนดไหน emphysema , chronic bronchitis หรอ mixed13. ใสคาน าหนก(BW) หนวยเปนกโลกรม สวนสง (Height) เปน เซนตเมตร เครองจะค านวณเปนคา BMI ใหอตโนมต14. ใสระยะทางการเดน 6 นาท ( 6MWT) ผปวยทลงทะเบยนครงแรกควรสง เดน 6MWT ในวนทลงทะเบยนคอวนทมาตรวจของวนนน
15. ลงแบบประเมนสมรรถนะ ประกอบดวย - Oxygen Saturation
- CAT score ประเมนแตละหวขอ จนครบ เครองจะรวมคะแนนใหอตโนมต
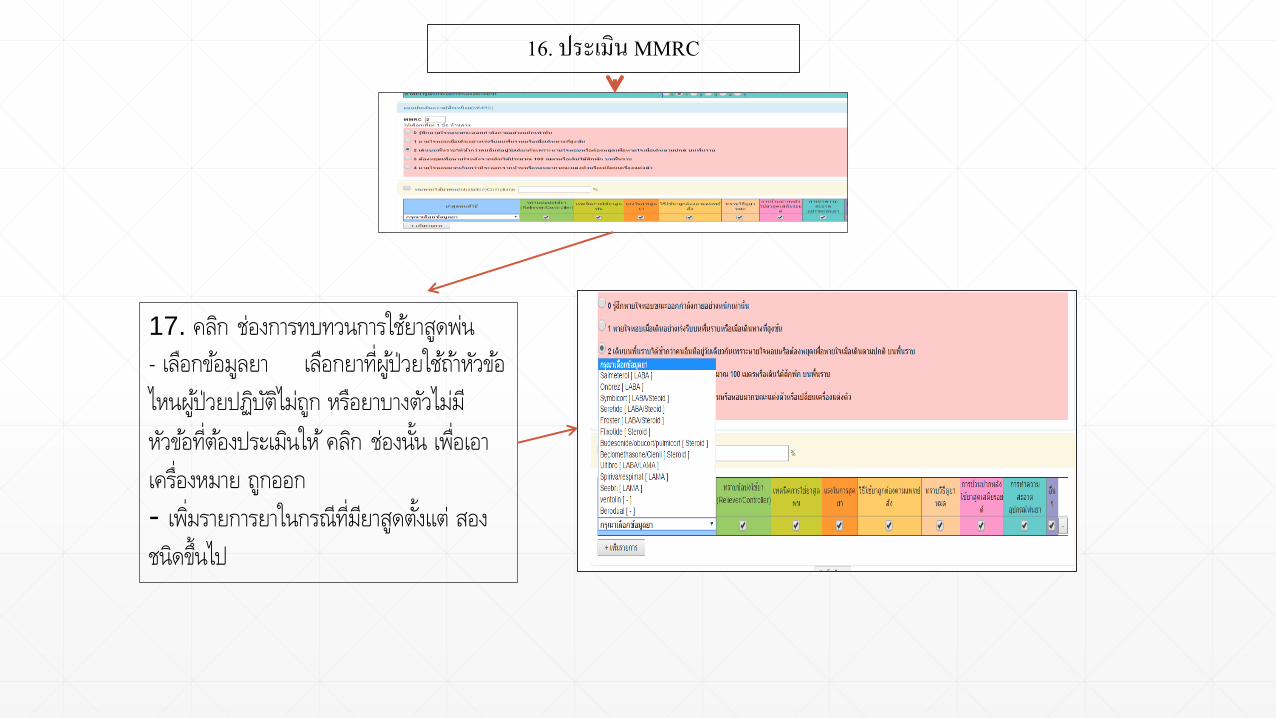
16. ประเมน MMRC
17. คลก ชองการทบทวนการใชยาสดพน
- เลอกขอมลยา เลอกยาทผปวยใชถาหวขอ
ไหนผปวยปฏบตไมถก หรอยาบางตวไมม
หวขอทตองประเมนให คลก ชองนน เพอเอา
เครองหมาย ถกออก
- เพมรายการยาในกรณทมยาสดตงแต สอง
ชนดขนไป
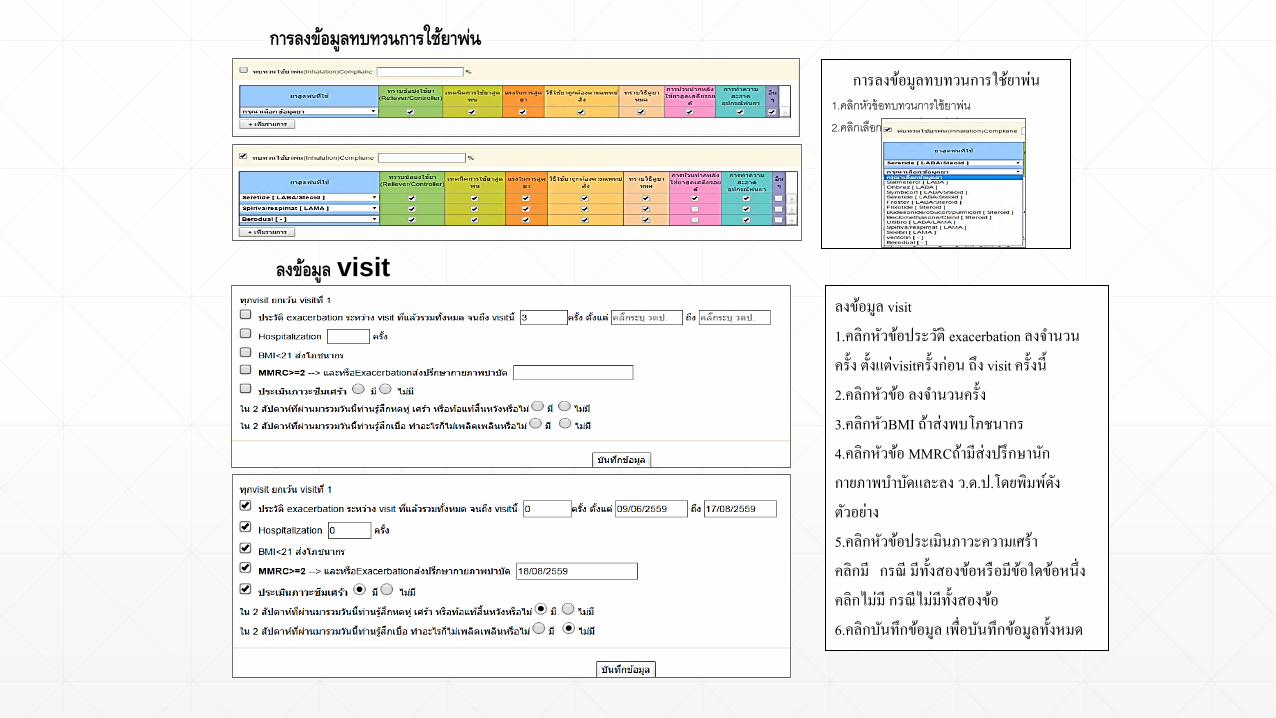
การลงขอมลทบทวนการใชยาพน1.คลกหวขอทบทวนการใชยาพน2.คลกเลอกยาและเพมยาทเพมรายการ
ลงขอมล visit1.คลกหวขอประวต exacerbation ลงจ านวนครง ตงแตvisitครงกอน ถง visit ครงน 2.คลกหวขอ ลงจ านวนครง3.คลกหวBMI ถาสงพบโภชนากร4.คลกหวขอ MMRCถามสงปรกษานกกายภาพบ าบดและลง ว.ด.ป.โดยพมพดงตวอยาง5.คลกหวขอประเมนภาวะความเศราคลกม กรณ มทงสองขอหรอมขอใดขอหนงคลกไมม กรณไมมทงสองขอ6.คลกบนทกขอมล เพอบนทกขอมลทงหมด
การลงขอมลทบทวนการใชยาพน
ลงขอมล visit
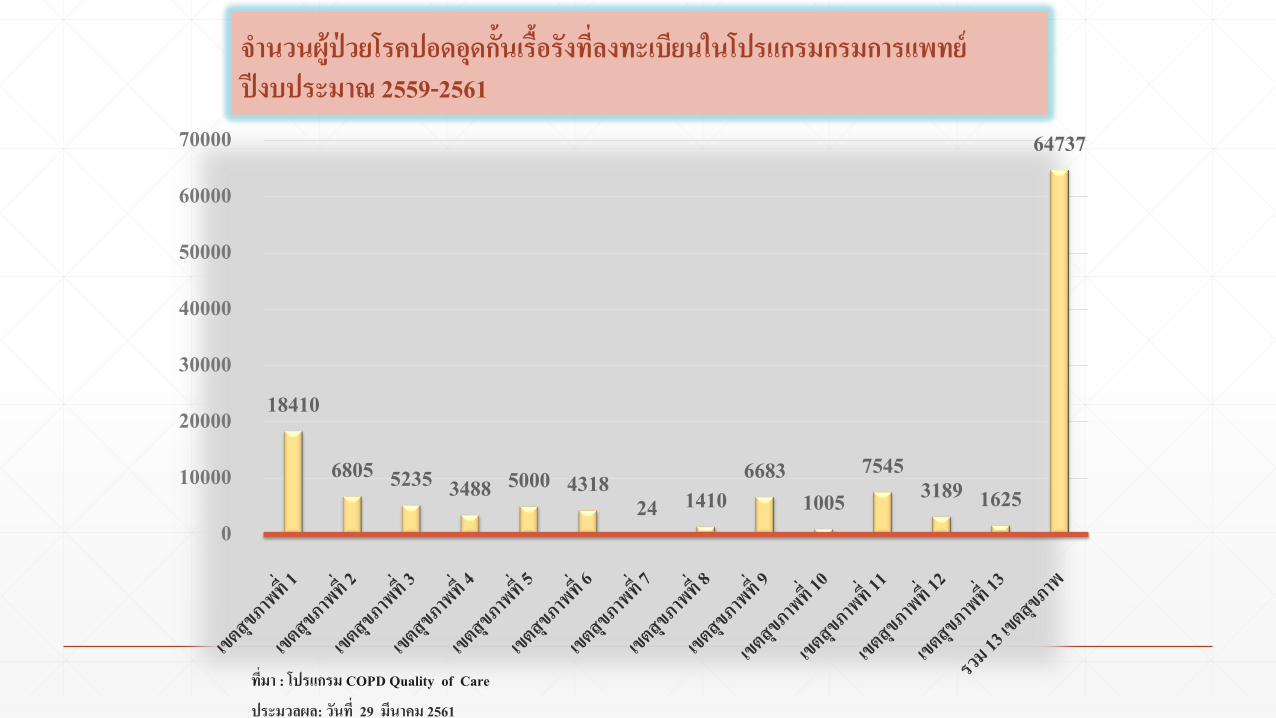
ทมา : โปรแกรม COPD Quality of Care
ประมวลผล: วนท 29 มนาคม 2561
18410
6805 5235 3488 5000 431824 1410
66831005
75453189 1625
64737
0
10000
20000
30000
40000
50000
60000
70000
จ านวนผปวยโรคปอดอดกนเรอรงทลงทะเบยนในโปรแกรมกรมการแพทยปงบประมาณ 2559-2561

ทมา : โปรแกรม COPD Quality of Care
ประมวลผล: วนท 29 มนาคม 2561
23991382 979 577 878 524 21
12182471
4631223 626 245
13006
0
2000
4000
6000
8000
10000
12000
14000
จ านวนผปวยโรคปอดอดกนเรอรงทลงทะเบยนในโปรแกรมกรมการแพทยปงบประมาณ 2561 (รอบ 6 เดอน)
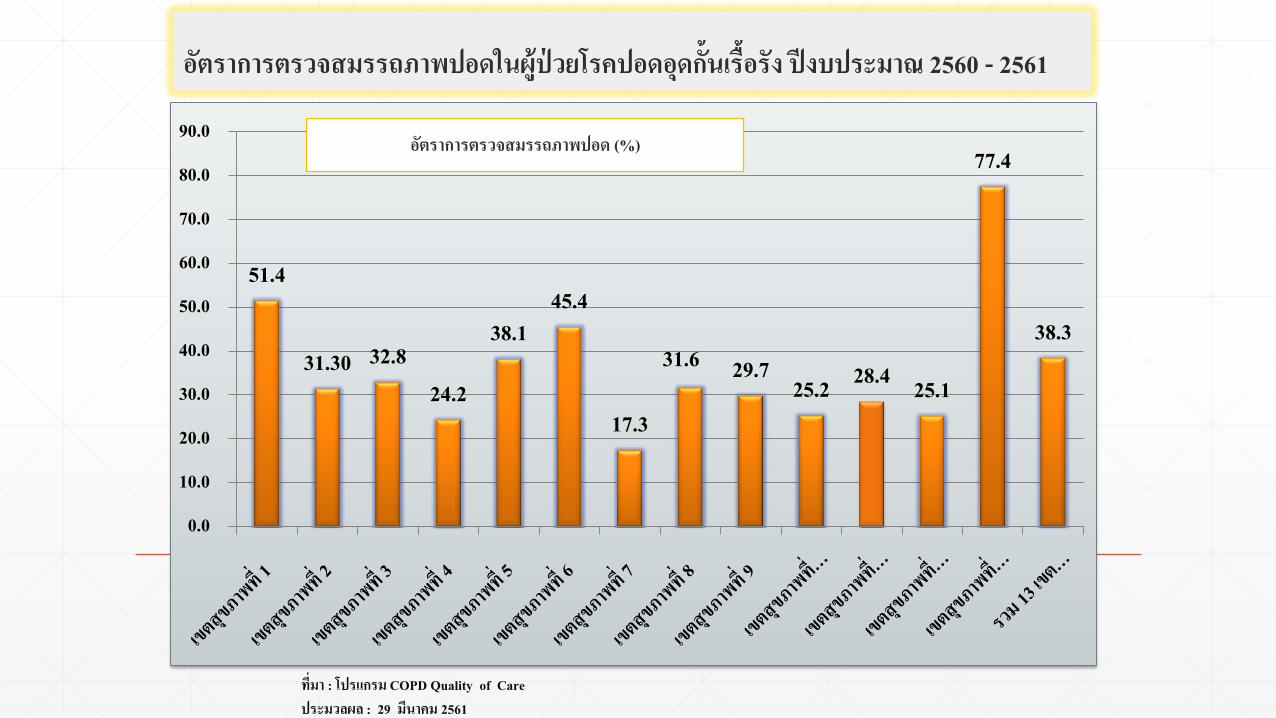
อตราการตรวจสมรรถภาพปอดในผปวยโรคปอดอดกนเรอรง ปงบประมาณ 2560 - 2561
51.4
31.30 32.824.2
38.145.4
17.3
31.6 29.725.2 28.4 25.1
77.4
38.3
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
ทมา : โปรแกรม COPD Quality of Care ประมวลผล : 29 มนาคม 2561
อตราการตรวจสมรรถภาพปอด (%)
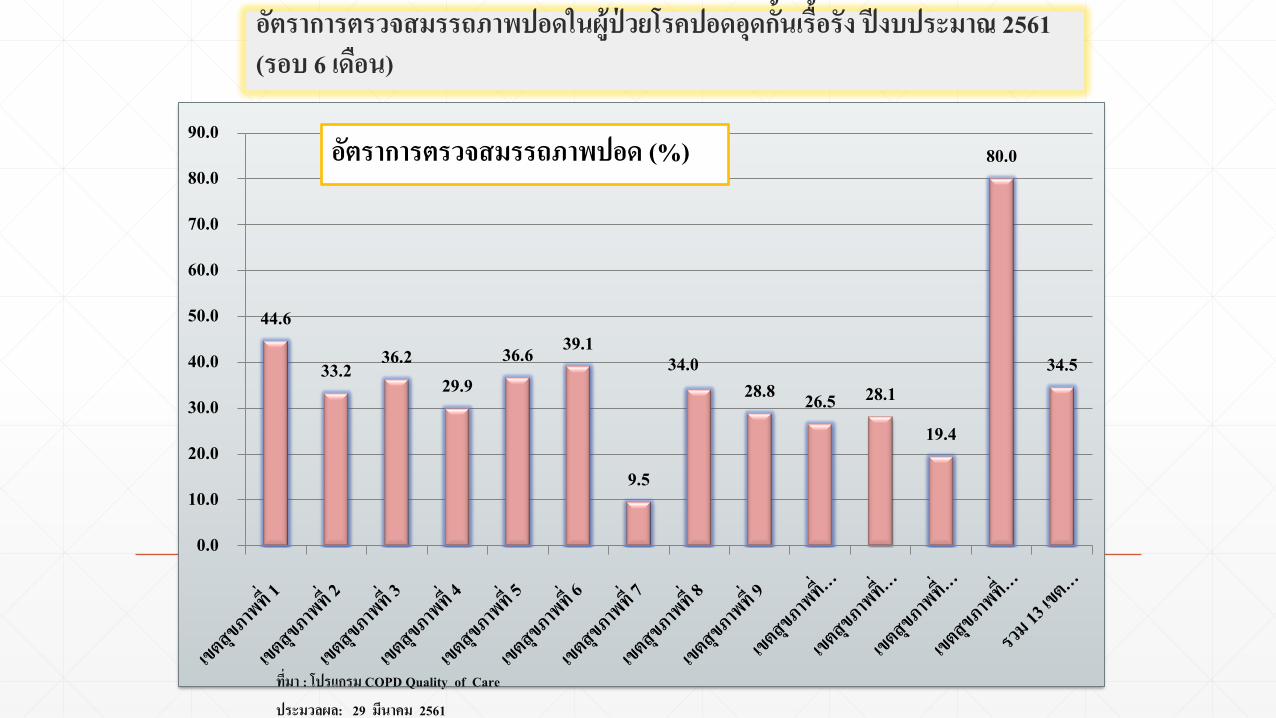
อตราการตรวจสมรรถภาพปอดในผปวยโรคปอดอดกนเรอรง ปงบประมาณ 2561 (รอบ 6 เดอน)
44.6
33.2 36.229.9
36.6 39.1
9.5
34.028.8 26.5 28.1
19.4
80.0
34.5
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0อตราการตรวจสมรรถภาพปอด (%)
ทมา : โปรแกรม COPD Quality of Care
ประมวลผล: 29 มนาคม 2561
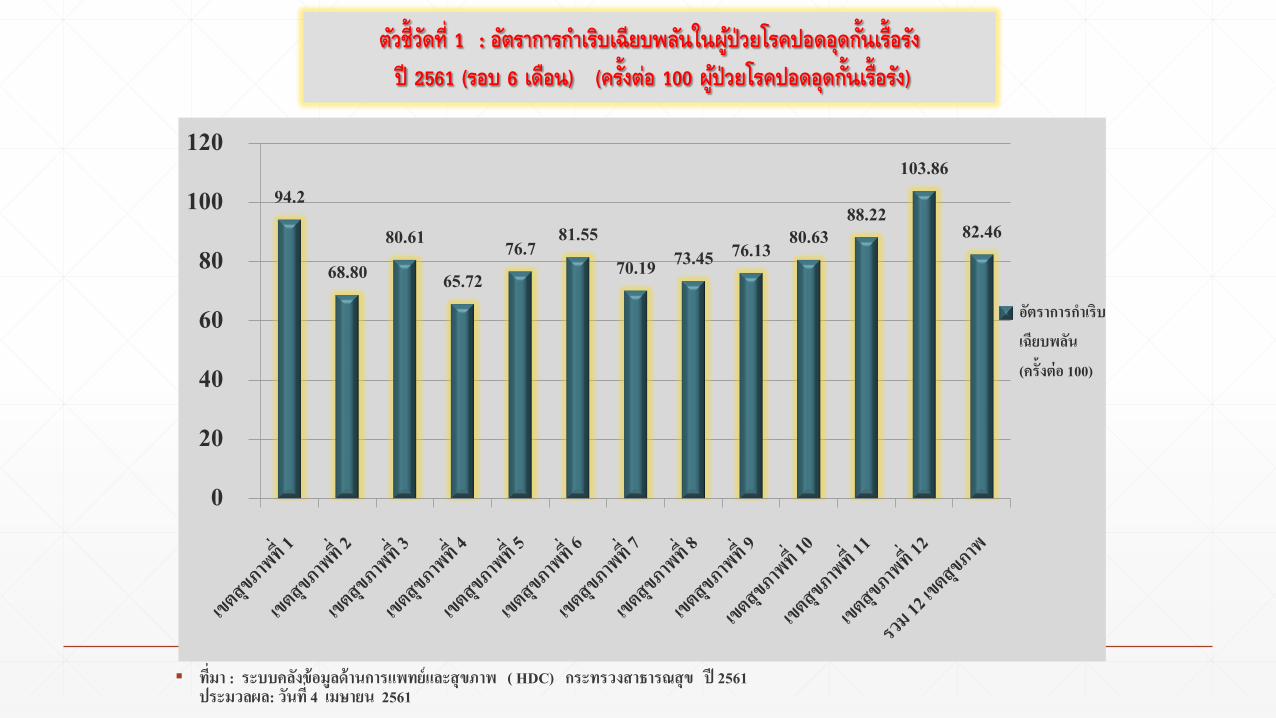
▪ ทมา : ระบบคลงขอมลดานการแพทยและสขภาพ ( HDC) กระทรวงสาธารณสข ป 2561 ประมวลผล: วนท 4 เมษายน 2561
ตวชวดท 1 : อตราการก าเรบเฉยบพลนในผปวยโรคปอดอดก นเรอรง ป 2561 (รอบ 6 เดอน) (คร งตอ 100 ผปวยโรคปอดอดก นเรอรง)
94.2
68.8080.61
65.7276.7 81.55
70.19 73.45 76.13 80.6388.22
103.86
82.46
0
20
40
60
80
100
120
อตราการก าเรบเฉยบพลน (ครงตอ 100)

Conclusion : COPD quality of care program
▪ An integrated program approach to the management of COPD patients that go along with standard guideline by multidisciplinary team
▪ Aims to improved outcome of COPD patients and consequently reduce the financial burden of COPD care
▪ May improved confidence in managing COPD patients for primary care setting, and increased patient satisfactory
Thank you