successful smoking cessation : learning to swim without ... cessation... · university of catania...
TRANSCRIPT
SuccessfulSuccessful Smoking Smoking CessationCessation ::learninglearning toto swimswim withoutwithout drowningdrowning
Prof. Prof. RiccardoRiccardo PolosaPolosaDirectorDirector
Institute of Internal Medicine and Clinical Immunol ogyInstitute of Internal Medicine and Clinical Immunol ogyUniversity of University of CataniaCatania
[email protected]@unict.it
Symposium Symposium –– AsthmaAsthmaand COPDand COPD

Tobacco dependence shows many features of a
chronic disease, with smokers typically cycling
through multiple periods of relapse and remission
Clinicians must appreciate that relapse is likely
reflecting the chronic nature of dependence, not
their personal failure, nor a failure of their patients
Tobacco DependenceTobacco Dependence
a Chronic Relapsing Diseasea Chronic Relapsing Disease
Diagnosis of Tobacco Dependence: ICD IX-CM 305.1
…an exacerbating factor for variousestablished medical conditions
…a risk factor for several diseases
Tobacco Dependence is alsoTobacco Dependence is also……

Global consumption of cigarette: 15 billion/dayGlobal consumption of cigarette: 15 billion/day
Tobacco use is a global pandemic, affecting anestimated 1.2 billion peopleTobacco use is a global pandemic, affecting anestimated 1.2 billion people
Source: WHO. Tobacco or Health: a Global Status Report, 1997; pp. 1–32. Geneva: World Health Organization.


Approx. 5 million tobacco-related deaths annuallyApprox. 5 million tobacco-related deaths annually
Source: WHO. Tobacco or Health: a Global Status Report, 1997; pp. 1–32. Geneva: World Health Organization.
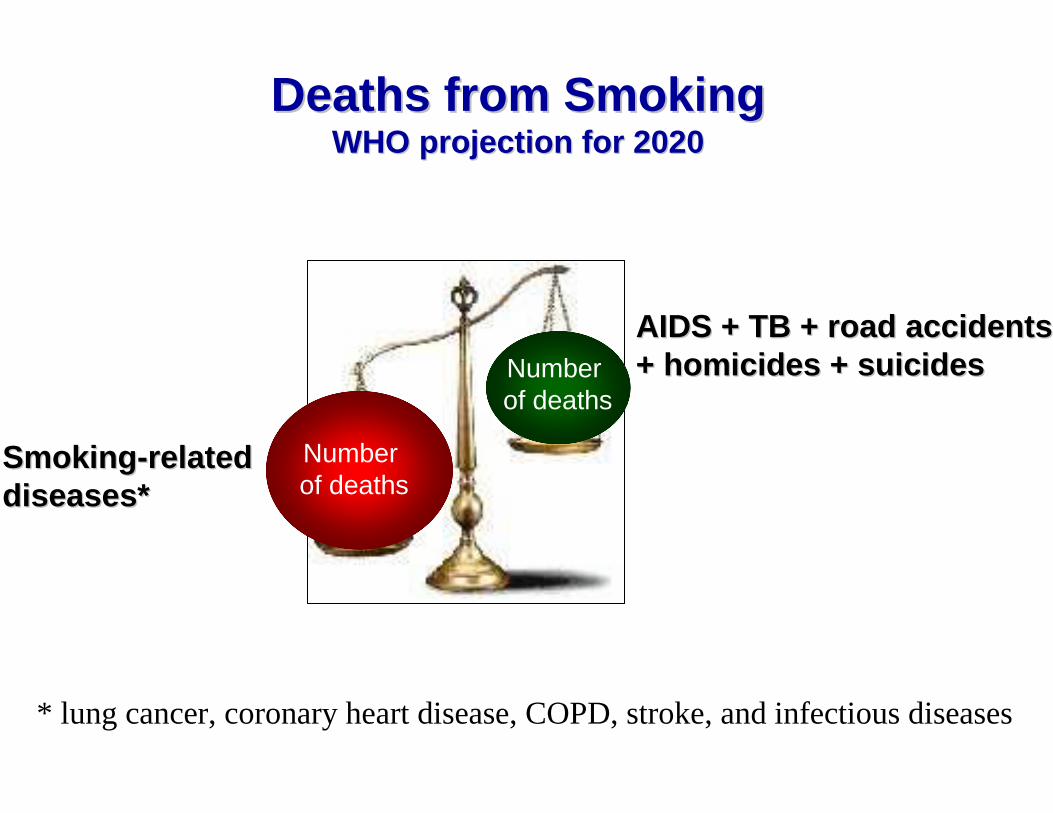
AIDS + TB + road accidents AIDS + TB + road accidents + homicides + suicides+ homicides + suicides
SmokingSmoking --related related diseases*diseases*
Deaths from SmokingDeaths from SmokingWHO projection for 2020WHO projection for 2020
Numberof deaths
Numberof deaths
* lung cancer, coronary heart disease, COPD, stroke, and infectious diseases

THE ADVANTAGE OF QUITTING SMOKING:THE ADVANTAGE OF QUITTING SMOKING:EVIDENCE FROM 50 YRS FOLLOWEVIDENCE FROM 50 YRS FOLLOW --UPUP
OF THE BRITISH MALE DOCTORS STUDYOF THE BRITISH MALE DOCTORS STUDY
DollDoll R. R. etet al.al. MortalityMortality in relation in relation toto smoking: 50 smoking: 50 yearsyears observationsobservations on male on male BritishBritish doctorsdoctorsBMJ 2004; 328: 1519BMJ 2004; 328: 1519--30.30.
•• youyou can live up can live up toto 6 6 yearsyears longerlonger ifif youyou quitquit at the at the ageage of 50of 50
•• youyou can live up can live up toto 9 9 yearsyears longerlonger ifif youyou quitquit at the at the ageage of 40of 40
•• whowho quitsquits byby the the ageage of 35 of 35 hashas the the samesame life life expectancyexpectancy of a long life non of a long life non smokersmoker

•• AsthmaAsthma•• Rheumatoid arthritisRheumatoid arthritis•• CTD (LES)CTD (LES)•• DiabetesDiabetes•• AlzheimerAlzheimer•• LeukemiaLeukemia•• PepticPeptic ulcerulcer•• OsteoporosisOsteoporosis•• PeriodontitisPeriodontitis•• InfertilityInfertility•• Neuropsychiatric conditions (schizophrenia, anxiety , Neuropsychiatric conditions (schizophrenia, anxiety ,
depression)depression)
Excess morbidity from smoking is also Excess morbidity from smoking is also
commonly found in other medical conditionscommonly found in other medical conditions

PREVALENCE RATES IN SMOKERS WITH ASTHMAPREVALENCE RATES IN SMOKERS WITH ASTHMAThe The sizesize of the of the problemproblem
Recent surveys indicate about 20Recent surveys indicate about 20--25% 25% (similar to general population).(similar to general population).AlthuisAlthuis, JA 1999, JA 1999Silverman, Chest 2003,Silverman, Chest 2003,Watson, Watson, FamFam PractPract 2005,2005,YunYun et al et al PrevPrev Med 2006Med 2006
Higher rates in smokers withHigher rates in smokers withasthma presenting to emergency asthma presenting to emergency
departments in USA. departments in USA. Silverman, Chest 2003Silverman, Chest 2003

AsthmaAsthma & Smoking: The & Smoking: The EvidenceEvidence
• Accelerated decline in lung function over time is p resent in asthmatic
individuals who smoke (Lange P, et al. N Engl J Med 1998; James AL, et al. Am J
Respir Crit Care Med 2005)
• Adults and older children with asthma who are activ e smokers have
also more severe symptoms and worse asthma-specific quality of life
compared to asthmatic non-smokers (Austin JB, et al. Arch Dis Child 2005;
Eisner MD, et al. Nicotine Tob Res 2007)
• Asthma mortality is greater among asthmatics who sm oke cigarettes
compared to asthmatics who do not smoke (Marquette C, et al. Am Rev Resp
Dis 1992; Ulrik CS, et al. Chest 1995)
• Asthmatic patients who smoke appear to have a reduc ed therapeutic
response to inhaled and oral corticosteroids (Chaudhuri R, et al. Am J Respir
Crit Care Med 2003; Lazarus SC, et al. Am J Respir Crit Car e Med 2007)
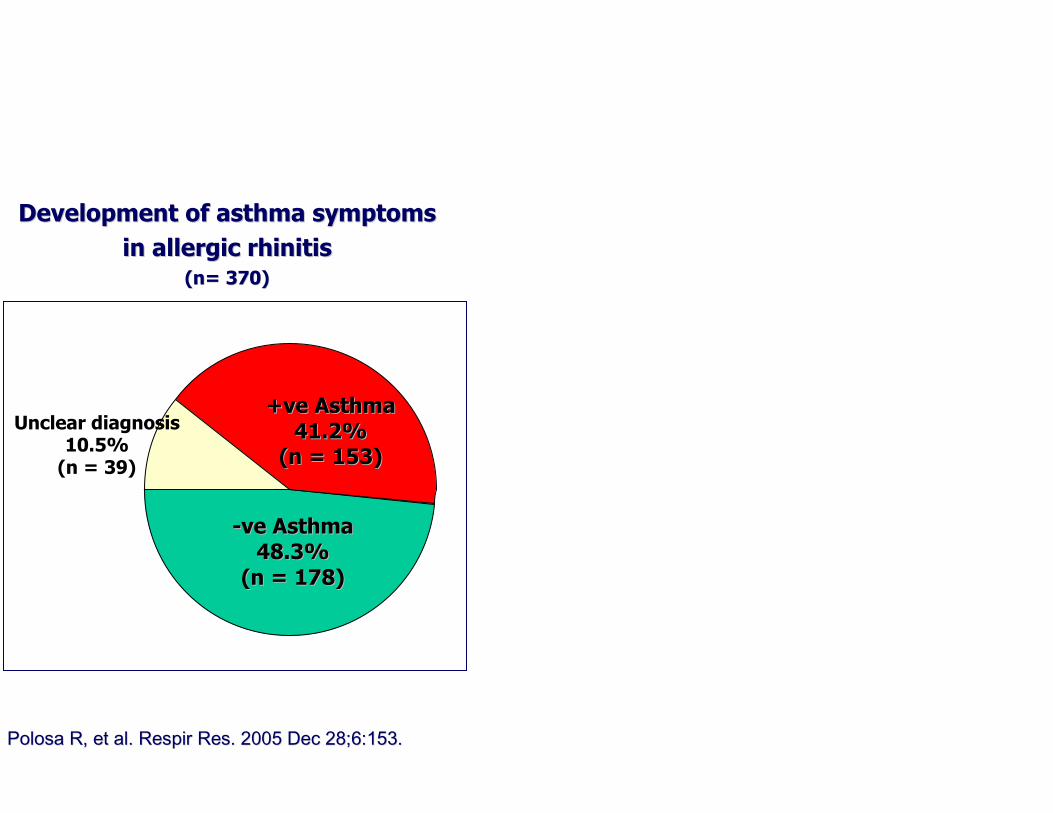
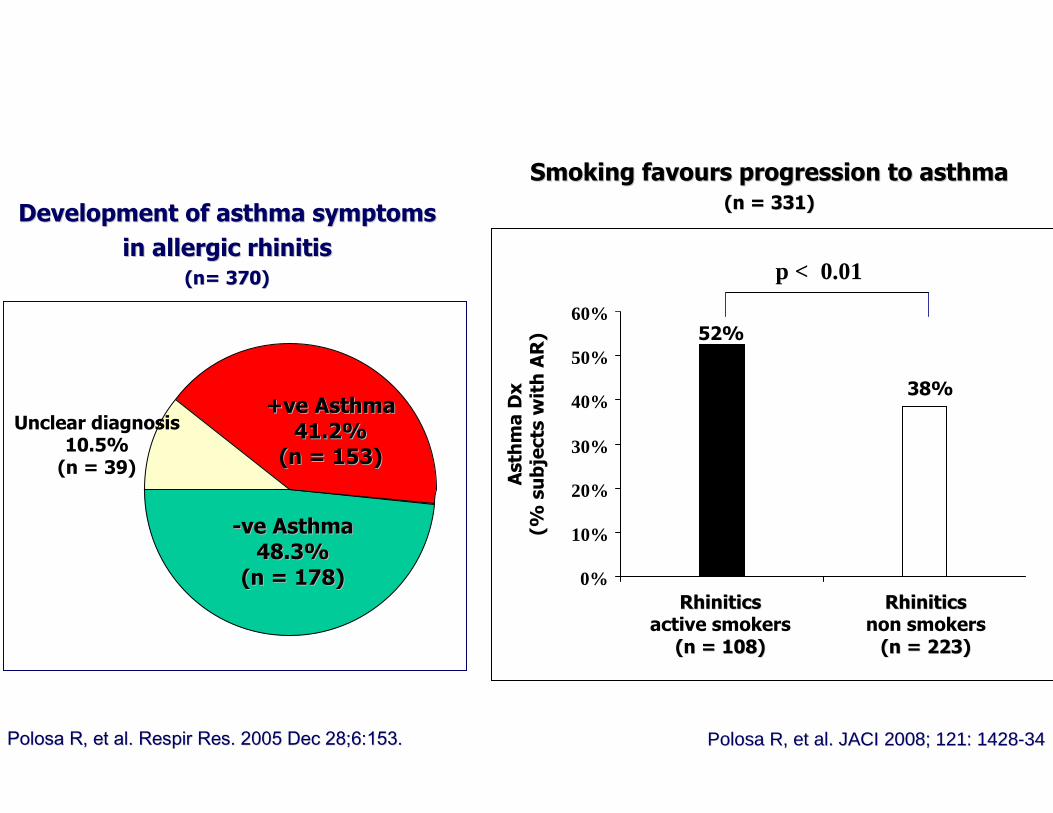
Unclear diagnosis10.5%(n = 39)
Development of asthma symptomsDevelopment of asthma symptoms
in allergic rhinitisin allergic rhinitis
((n=n= 370)370)
--ve ve AsthmaAsthma
48.3%48.3%
(n = 178) (n = 178)
+ve+ve AsthmaAsthma
41.2%41.2%
(n = 153) (n = 153)
PolosaPolosa R, R, etet al.al. RespirRespir Res. 2005 Res. 2005 DecDec 28;6:153.28;6:153.
Development of asthma symptomsDevelopment of asthma symptoms
in allergic rhinitisin allergic rhinitis
((n=n= 370)370)
--ve ve AsthmaAsthma
48.3%48.3%
(n = 178) (n = 178)
Smoking Smoking favoursfavours progression to asthmaprogression to asthma
(n = 331)(n = 331)
AsthmaDx
(% subjectswithAR)
RhiniticsRhiniticsactive smokers
(n = 108)(n = 108)
RhiniticsRhiniticsnon smokers
(n = 223)(n = 223)
p < 0.01
38%
52%
0%
10%
20%
30%
40%
50%
60%
+ve+ve AsthmaAsthma
41.2%41.2%
(n = 153) (n = 153)
PolosaPolosa R, R, etet al.al. JACI 2008; 121: 1428JACI 2008; 121: 1428--3434PolosaPolosa R, R, etet al.al. RespirRespir Res. 2005 Res. 2005 DecDec 28;6:153.28;6:153.
Unclear diagnosis10.5%(n = 39)

CIGARETTE SMOKING IS ASSOCIATED WITH A CIGARETTE SMOKING IS ASSOCIATED WITH A GREATER RISK GREATER RISK OF INCIDENT ASTHMA IN ALLERGIC RHINITISOF INCIDENT ASTHMA IN ALLERGIC RHINITIS
Polosa R. et al. J Allergy Clin Immunol 2008
Table 2. Logistic Regression for Developing Asthma; Continuing Smokers, Former Smokers, and Nonsmokers Combined
Univariate Multivariate Variable df χ
2 P OR (CI) χ2 P OR (CI)
Smokers vs. nonsmokers 1 18.4 <0.0001 2.67 (1.70, 4.19) 18.3 <0.0001 2.98 (1.81, 4.92) Current vs. former vs. nonsmokers 2 19.3 <0.0001
Current vs. nonsmokers 2.93 (1.81, 4.74) Former vs. nonsmokers 1.93 (0.91, 4.10)
Age (years) 1 2.3 0.13 1.03 (0.99, 1.07) Sex (male vs. female) 1 21.6 <0.0001 0.34 (0.22, 0.54) 18.2 <0.0001 0.34 (0.20, 0.55) Symptoms: better vs. not better 1 24.5 <0.0001 0.30 (0.19, 0.49) 24.3 <0.0001 0.27 (0.16, 0.45) Symptoms: better vs. unchanged vs. worse 2 25.4 <0.0001
Better vs. worse 0.19 (0.08, 0.46) Unchanged vs. worse 0.54 (0.21, 1.41)
Passive smoke (yes vs. no) 1 2.1 0.15 1.39 (0.89, 2.17) House pet (yes vs. no) 1 9.3 0.002 2.05 (1.29, 3.25) 7.3 0.007 2.04 (1.21, 3.41) Atopic family Hx (yes vs. no) 1 5.6 0.02 1.75 (1.10, 2.78) Immunotherapy (yes vs. no) 1 3.4 0.06 0.66 (0.42, 1.03)
df = degrees of freedom χ
2 = chi-squared statistic (Wald) P = P-value for chi-squared statistic OR = odds ratio CI = 95% confidence interval Only significant (P < 0.01) variables are included in the multivariate analysis

CIGARETTE SMOKING IS ASSOCIATED WITH A CIGARETTE SMOKING IS ASSOCIATED WITH A GREATER RISK GREATER RISK OF INCIDENT ASTHMA IN ALLERGIC RHINITISOF INCIDENT ASTHMA IN ALLERGIC RHINITIS
Polosa R. et al. J Allergy Clin Immunol 2008
Table 3. Logistic Regression for Developing Asthma; Continuing Smokers and Nonsmokers Combined
Univariate Multivariate Variable df χ
2 P OR (CI) χ2 P OR (CI)
Pack years (four categories) 3 20.7 0.0001 20.0 0.0002
1 - 10 vs 0 2.08 (1.07, 4.04) 2.05 (0.99, 4.27) 11 - 20 vs 0 3.87 (1.98, 7.57) 3.71 (1.77, 7.78) 21+ vs 0 3.24 (1.35, 7.76) 5.05 (1.93, 13.2)
Age (years) 1 1.8 0.13 1.03 (0.99, 1.07) Sex (male vs. female) 1 23.3 <0.0001 0.30 (0.19, 0.49) 22.6 <0.0001 0.27 (0.16, 0.46) Symptoms: better vs. not better 1 24.1 <0.0001 0.29 (0.18, 0.47) 27.0 <0.0001 0.23 (0.13, 0.40) Symptoms: better vs. unchanged vs. worse 2 24.9 <0.0001
Better vs. worse 0.17 (0.07, 0.45) Unchanged vs. worse 0.51 (0.19, 1.42)
Passive smoke (yes vs. no) 1 1.5 0.22 1.34 (0.84, 2.15) House pet (yes vs. no) 1 6.4 0.01 1.88 (1.15, 3.05) Atopic family Hx (yes vs. no) 1 4.4 0.03 1.69 (1.04, 2.76) Immunotherapy (yes vs. no) 1 3.5 0.06 0.64 (0.40, 1.02)
df = degrees of freedom χ
2 = chi-squared statistic (Wald) P = P-value for chi-squared statistic OR = odds ratio CI = 95% confidence interval Only significant (P < 0.01) variables are included in the multivariate analysis

“Allergic march”
FROM SNEEZING TO WHEEZINGFROM SNEEZING TO WHEEZING
Smoking is also a key risk factor for new onset ast hma in Smoking is also a key risk factor for new onset ast hma in
allergic individualsallergic individuals
PolosaPolosa R, R, etet al.al. JACI 2008; 121: 1428JACI 2008; 121: 1428--3434

Current Smokersn = 74 (48.7%)
Former Smokersn = 17 (11.2%)
Never Smokersn = 61 (40.1%)
Cases selected for final analysesn = 325
New onset asthma at follow-up (2000)n = 152*
Pack/yrscalculated
Polosa R, et al. Greater Severity Of New Onset Asthma In Allergic
Subjects Who Smoke: A 10-year Longitudinal Study
Submitted for Publication

Current Smokersn = 74 (48.7%)
Former Smokersn = 17 (11.2%)
Never Smokersn = 61 (40.1%)
Cases selected for final analysesn = 325
New onset asthma at follow-up (2000)n = 152*
STEP In = 24
(37.5%)
STEP IIn = 18
(50.0%)
STEP IIIn = 24
(58.5%)
STEP IVn = 8
(72.7%)
STEP In = 8
(12.5%)
STEP IIn = 4
(11.1%)
STEP IIIn = 4
(9.8%)
STEP IVn = 1
(9.1%)
STEP In = 32
(50.0%)
STEP IIn = 14
(38.9%)
STEP IIIn = 13
(31.7%)
STEP IVn = 2
(18.2%)
Controlledn = 19
(27.1%)
PartlyControlled
n = 36(69.2%)
Uncontrolledn = 13
(72.2%)
Controlledn = 10
(14.3%)
PartlyControlled
n = 4(7.7%)
Uncontrolledn = 2
(11.1%)
Controlledn = 41
(58.6%)
PartlyControlled
n = 12(23.1%)
Uncontrolledn = 3
(16.7%)
Pack/yrscalculated
AsthmaAsthmaseverityseverityclassclasscomputedcomputed

Current Smokersn = 74 (48.7%)
Former Smokersn = 17 (11.2%)
Never Smokersn = 61 (40.1%)
Cases selected for final analysesn = 325
New onset asthma at follow-up (2000)n = 152*
STEP In = 24
(37.5%)
STEP IIn = 18
(50.0%)
STEP IIIn = 24
(58.5%)
STEP IVn = 8
(72.7%)
STEP In = 8
(12.5%)
STEP IIn = 4
(11.1%)
STEP IIIn = 4
(9.8%)
STEP IVn = 1
(9.1%)
STEP In = 32
(50.0%)
STEP IIn = 14
(38.9%)
STEP IIIn = 13
(31.7%)
STEP IVn = 2
(18.2%)
Controlledn = 19
(27.1%)
PartlyControlled
n = 36(69.2%)
Uncontrolledn = 13
(72.2%)
Controlledn = 10
(14.3%)
PartlyControlled
n = 4(7.7%)
Uncontrolledn = 2
(11.1%)
Controlledn = 41
(58.6%)
PartlyControlled
n = 12(23.1%)
Uncontrolledn = 3
(16.7%)
Pack/yrscalculated
AsthmaAsthmacontrolcontrollevellevelcomputedcomputed
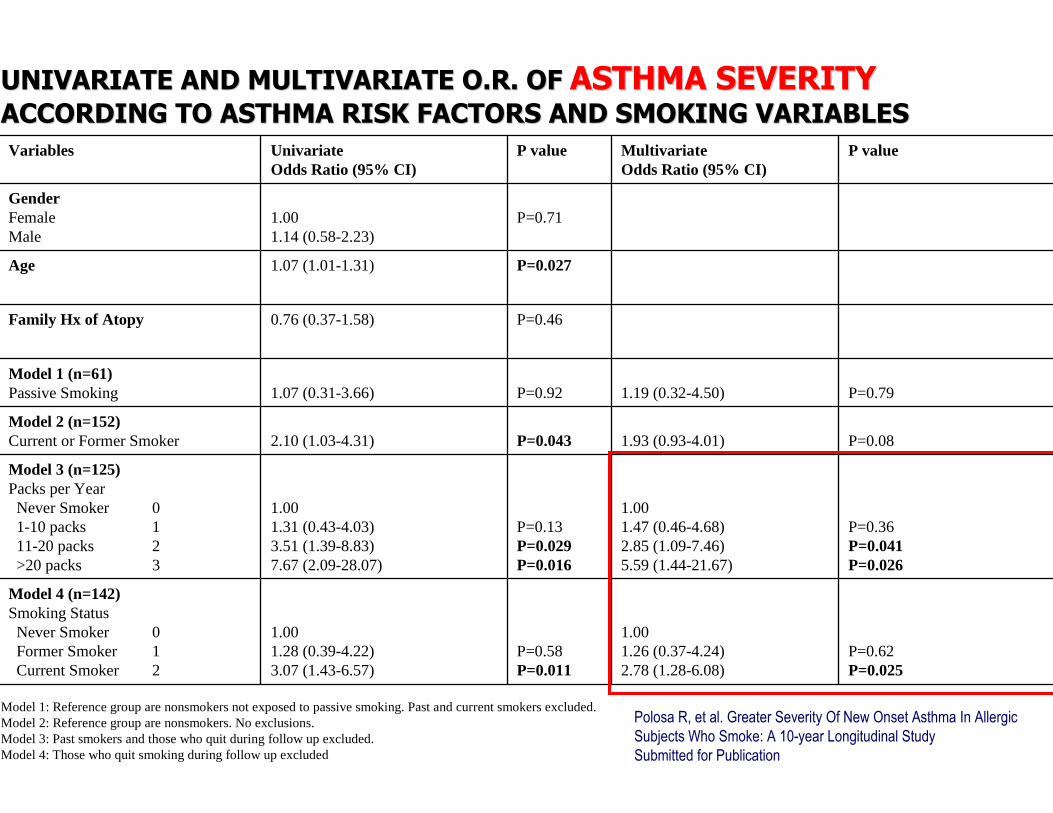
UNIVARIATE AND MULTIVARIATE O.R. OF UNIVARIATE AND MULTIVARIATE O.R. OF ASTHMA SEVERITYASTHMA SEVERITYACCORDING TO ASTHMA RISK FACTORS AND SMOKING VARIABLESACCORDING TO ASTHMA RISK FACTORS AND SMOKING VARIABLES
P=0.62P=0.025
1.001.26 (0.37-4.24)2.78 (1.28-6.08)
P=0.58P=0.011
1.001.28 (0.39-4.22)3.07 (1.43-6.57)
Model 4 (n=142)Smoking StatusNever Smoker 0Former Smoker 1Current Smoker 2
P=0.36P=0.041P=0.026
1.001.47 (0.46-4.68)2.85 (1.09-7.46)5.59 (1.44-21.67)
P=0.13P=0.029P=0.016
1.001.31 (0.43-4.03)3.51 (1.39-8.83)7.67 (2.09-28.07)
Model 3 (n=125)Packs per YearNever Smoker 01-10 packs 111-20 packs 2>20 packs 3
P=0.081.93 (0.93-4.01)P=0.0432.10 (1.03-4.31)Model 2 (n=152)Current or Former Smoker
P=0.791.19 (0.32-4.50)P=0.921.07 (0.31-3.66)Model 1 (n=61)Passive Smoking
P=0.460.76 (0.37-1.58)Family Hx of Atopy
P=0.0271.07 (1.01-1.31)Age
P=0.711.001.14 (0.58-2.23)
GenderFemaleMale
P valueMultivariateOdds Ratio (95% CI)
P valueUnivariateOdds Ratio (95% CI)
Variables
Model 1: Reference group are nonsmokers not exposed to passive smoking. Past and current smokers excluded.Model 2: Reference group are nonsmokers. No exclusions.Model 3: Past smokers and those who quit during follow up excluded.Model 4: Those who quit smoking during follow up excluded
Polosa R, et al. Greater Severity Of New Onset Asthma In Allergic
Subjects Who Smoke: A 10-year Longitudinal Study
Submitted for Publication

UNIVARIATE AND MULTIVARIATE O.R. OF UNIVARIATE AND MULTIVARIATE O.R. OF ASTHMA CONTROLASTHMA CONTROLACCORDING TO ASTHMA RISK FACTORS AND SMOKING VARIABLES ACCORDING TO ASTHMA RISK FACTORS AND SMOKING VARIABLES
P=0.29P <0.0001
1.001.70 (0.52-5.58)9.54 (3.98-22.88)
P=0.26P=<0.0001
1.001.64 (0.51-5.30)9.46 (4.03-22.24)
Model 4 (n=130)Smoking StatusNever Smoker 0Former Smoker 1Current Smoker 2
P=0.01P=0.002
1.005.51 (1.73-17.54)13.38 (4.57-39.19)
P=0.03P=0.0002
1.004.69 (1.55-14.13)15.03 (5.25-43.03)
Model 3 (n=114)Packs per YearNever Smoker 01-10 packs 1>10 packs 2
P<0.00015.16 (2.43-11.02)P<0.00015.18 (2.47-10.90)Model 2 (n=140)Current or Former Smoker
P=0.310.53 (0.16-1.81)P=0.300.53 (0.16-1.78)Model 1 (n=56)Passive Smoking
P=0.061.06 (1.00-1.12)Age
P=0.611.001.19 (0.61-2.32)
GenderFemaleMale
P valueMultivariateOdds Ratio (95% CI)
P valueUnivariateOdds Ratio (95% CI)
Variables
Model 1: Reference group are nonsmokers not exposed to passive smoking. Past and current smokers excluded.Model 2: Reference group are nonsmokers. No exclusions.Model 3: Past smokers and those who quit during follow up excluded.Model 4: Those who quit smoking during follow up excluded Polosa R, et al. Greater Severity Of New Onset Asthma In Allergic
Subjects Who Smoke: A 10-year Longitudinal Study
Submitted for Publication

THE ADVANTAGE OF QUITTING SMOKING:THE ADVANTAGE OF QUITTING SMOKING:EVIDENCE FROM ASTHMA STUDIESEVIDENCE FROM ASTHMA STUDIES

Conclusions :By 12-months after smoking cessation, we observed a significant improvement in BHR to AMP and Mch in quitters: their D–R curves being displaced to the right to a similarextent (1.4 and 1.1 doubling concentrations for AMP and Mch respectively).
Respir Med. 2008 Feb;102(2):256-65.

Nicotine Tob Res 2005; 7:139–148.

Smoking is AddictiveSmoking is Addictive
•• 70% of smokers say 70% of smokers say they would like to they would like to quitquit
•• 30% attempts to quit30% attempts to quit
•• 3% are successful 3% are successful each yeareach year
Self Self mutilationmutilation byby smoking smoking –– thisthis patientpatienthadhad allall fourfour limbslimbs amputatedamputated forfor a a
BuergerBuerger’’s s typetype obliterativeobliterative vascularvasculardiseasedisease
BridgwoodBridgwood et al,et al, General Household Survey 1998.General Household Survey 1998.WestWest,, Getting serious about stopping smokingGetting serious about stopping smoking 1997.1997.ArnstenArnsten,, Prim PsychiatryPrim Psychiatry 1996.1996.

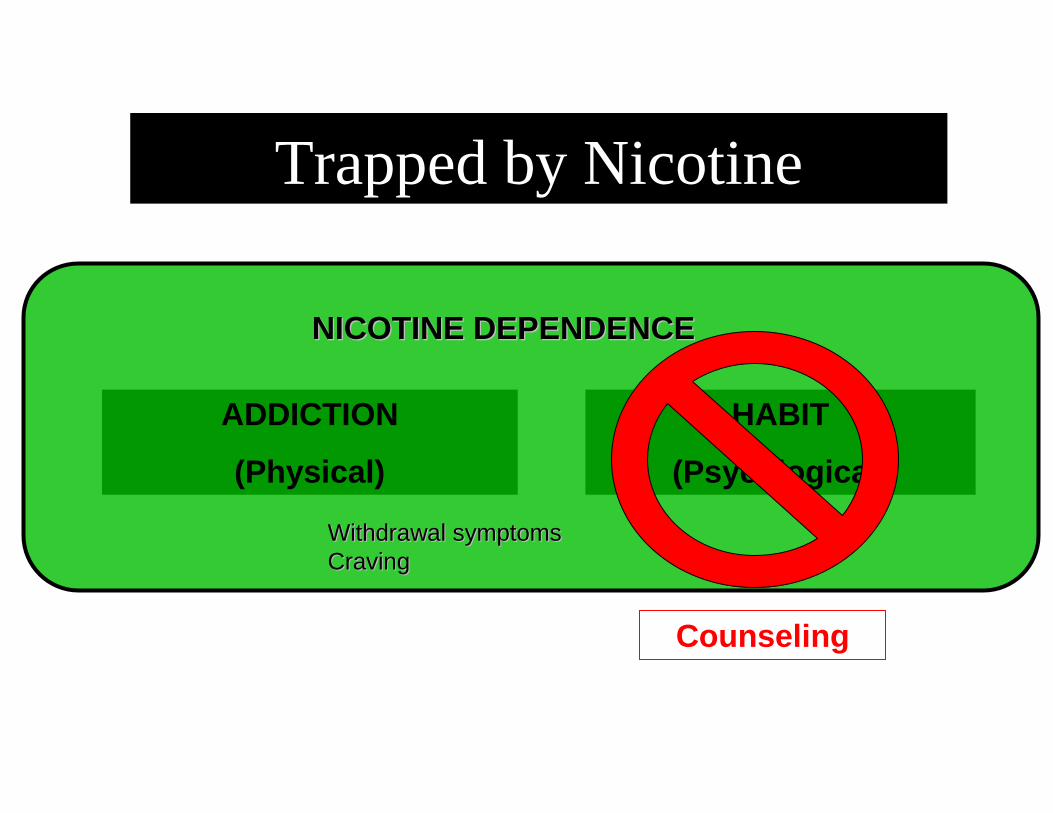
Trapped by Nicotine
ADDICTION
(Physical)
HABIT
(Psycological)
NICOTINE DEPENDENCENICOTINE DEPENDENCE

Smoking CessationSmoking Cessation’’ s ABCs ABC
AAsk at every visit: Do you smoke?sk at every visit: Do you smoke?
BBrief advicerief advice
CCessation supportessation support
McRobbieMcRobbie H, et al. H, et al. N Z Med J.N Z Med J. 2008;121:572008;121:57--70.70. 28
1.1. ““Are you a smoker?Are you a smoker?””
2.2. ““Can I ask if you smoke at all?Can I ask if you smoke at all?””
3.3. ““How much do you smoke per day?How much do you smoke per day?””
4.4. ““How long have you been smoking?How long have you been smoking?””
5.5. ““How are you getting on with your smoking?How are you getting on with your smoking?””
6.6. ““When was the last time you had a cigarette?When was the last time you had a cigarette?””
7.7. ““Have you smoked in the past week or even in the past 6 Have you smoked in the past week or even in the past 6 months?months?””
How Would You How Would You AskAsk About SmokingAbout Smokingin Your Clinical Practice?in Your Clinical Practice?

•• Determining smoking history, including: Determining smoking history, including:
–– Number and methods of previous quit attemptsNumber and methods of previous quit attempts
–– Previous lengths of abstinence achievedPrevious lengths of abstinence achieved
–– Whether smokers who quit recently are calling Whether smokers who quit recently are calling themselves themselves ““nonsmokersnonsmokers””
•• Usually patients visit for another health problem Usually patients visit for another health problem
–– So, a link might be made between smoking and other So, a link might be made between smoking and other health problemshealth problems
–– But But …… be careful not to accuse or alienatebe careful not to accuse or alienate
Outcomes of Asking About SmokingOutcomes of Asking About Smoking

• Personally relevant to the patient’s situation• Unambiguous• Non-judgmental• Empathic
Brief Advice to Quit Smoking Should Be:

• Personally relevant to the patient’s situation
Advice to Quit Smoking Should Be:

HeavyHeavy smokersmoker (60 (60 cigcig /day) 41 /day) 41 yrsyrs referredreferredfromfrom the the ChestChest Clinic Clinic wherewhere hehe hashas beenbeen seenseen
forfor frequentfrequent asthmaasthma exacerbationsexacerbations
““ ByBy quittingquitting youyou willwill notnot onlyonly improveimprove youryourgeneralgeneral healthhealth status, status, butbut alsoalso youryour asthmaasthma
symptomssymptoms .....did.did youyou knowknow thatthat ??””

• Personally relevant to the patient’s situation• Unambiguous
Advice to Quit Smoking Should Be:

““QuittingQuitting isis veryvery goodgood forfor youyou, , butbut itit isis notnot easy. easy. ItItrequiresrequires a a solidsolid plan and plan and committmentcommittment toto a a quitquit
date. date. QuittingQuitting maymay cause some cause some sufferingsufferingparticularlyparticularly in the first in the first couplecouple of of weeksweeks of of
abstinenceabstinence fromfrom tobaccotobacco””
““WeWe are are herehere toto help and help and toto givegive allall the the supportsupportyouyou needneed toto bebe successfulsuccessful””
• Personally relevant to the patient’s situation• Unambiguous• Non-judgmental
Advice to Quit Smoking Should Be:
HeartHeart surgeonsurgeon 40 40 yrsyrs . . HeHe isis embarassedembarassedbecausebecause , , despitedespite hishis knowledgeknowledge of the of the
damagedamage causedcaused byby smoking, smoking, hehe repeatedlyrepeatedlyfailedfailed toto quitquit
““ QuittingQuitting isis notnot easy easy forfor anybodyanybody . And . And thisthisincludesincludes manymany doctorsdoctors likelike you.you. WeWe can can offerofferdifferentdifferent strategiesstrategies toto help help youyou quitquit . I . I amam suresure
togethertogether wewe can can findfind the the rightright one one forfor youyou ””
• Personally relevant to the patient’s situation• Unambiguous• Non-judgmental• Empathic
Advice to Quit Smoking Should Be:

HousewifeHousewife 44 44 yrsyrs , , sheshe hashas relapsedrelapsed after 14 after 14 monthsmonths of of abstinenceabstinence fromfrom tobaccotobacco . . SheShe feelsfeels
a total a total failurefailure and and fearsfears toto relapserelapse againagain ..
I I understandunderstand howhow youyou feelfeel …… butbut relapserelapse isisalwaysalways a a possibilitypossibility in a in a chronicchronic diseasedisease likelikenicotine nicotine addictionaddiction . . HoweverHowever , , pleaseplease considerconsider
the positive the positive aspectsaspects : : youyou havehave beenbeen a non a non smokersmoker forfor more more thanthan a a yearyear and and thisthis relapserelapse
isis a a keykey learninglearning opportunityopportunity forfor youyou . . NextNexttime time willwill bebe muchmuch easiereasier notnot toto relapserelapse ””

• Give a reason to quit
• Acknowledge quitting can be difficult (may take many attempts)
• Motivate the smoker by offering assistance
Strong Advice to Stop Smoking:Strong Advice to Stop Smoking:Examples of What You Can SayExamples of What You Can Say ……
“Stopping smoking is the single best thing that you can do to improve your
current and future health”
“Tobacco is very addictive, so it can be very difficult to give up, and many people have to try several times before they succeed”
“The important thing is to keep trying”
“If you would like to give up smoking, I can help you succeed with support and proven effective medication”
“If you are interested in stopping smoking, there are services and medications which can help you in your quit attempt”
RB1

Slide 40
RB1 Changed the quotes to a series of animated word bubblesbeckr, 8/25/2009
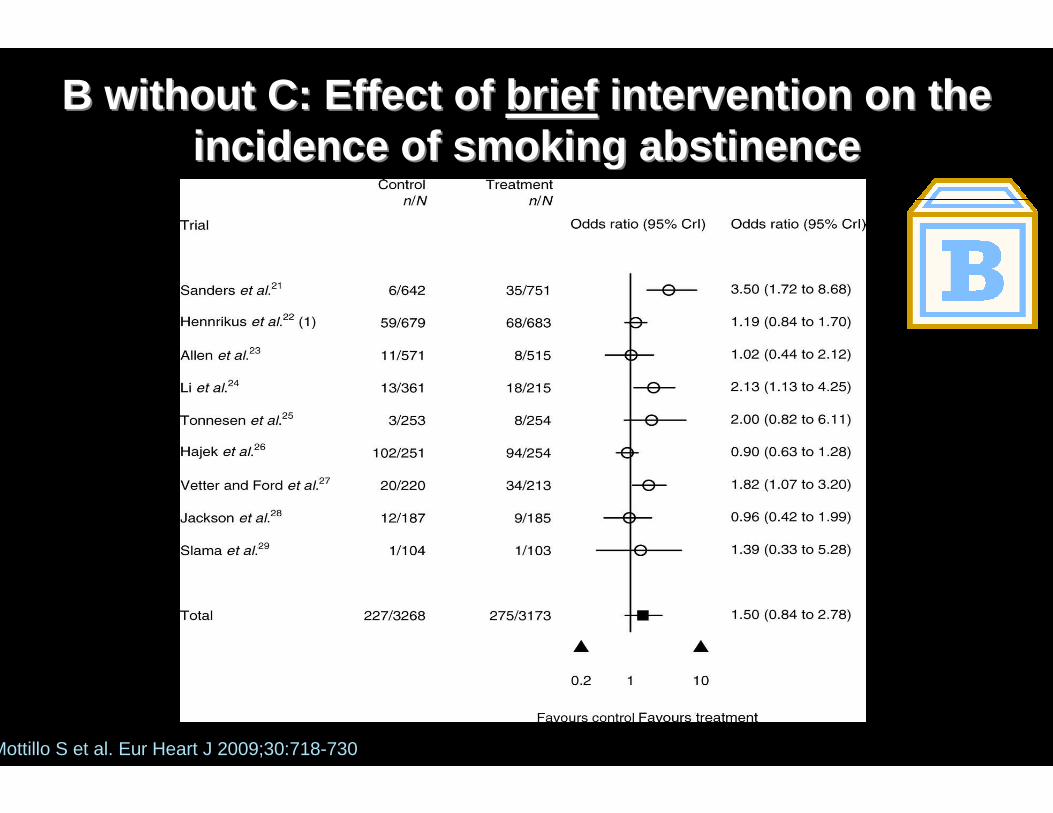
B without C: Effect of B without C: Effect of briefbrief intervention on the intervention on the incidence of smoking abstinenceincidence of smoking abstinence
Mottillo S et al. Eur Heart J 2009;30:718-730
Ask and ActAsk and Act
42

Quitting smokingQuitting smoking……is a process and not an eventis a process and not an event
……therefore longtherefore long--term or longitudinal term or longitudinal approaches work bestapproaches work best
Quitting smokingQuitting smoking……is a process and not an eventis a process and not an event
……therefore longtherefore long--term or longitudinal term or longitudinal approaches work bestapproaches work best
Cessation Support:Cessation Support:

Varenicline
Standard Standard approachapproach toto smoking smoking cessationcessationCentro Universitario per la Prevenzione e Cura del Tabagismo (CPCentro Universitario per la Prevenzione e Cura del Tabagismo (CPCT)CT)
University of CataniaUniversity of Catania
Preparation/planning
Quit Day
follow-up
NRT
Bupropion
Counselling
time
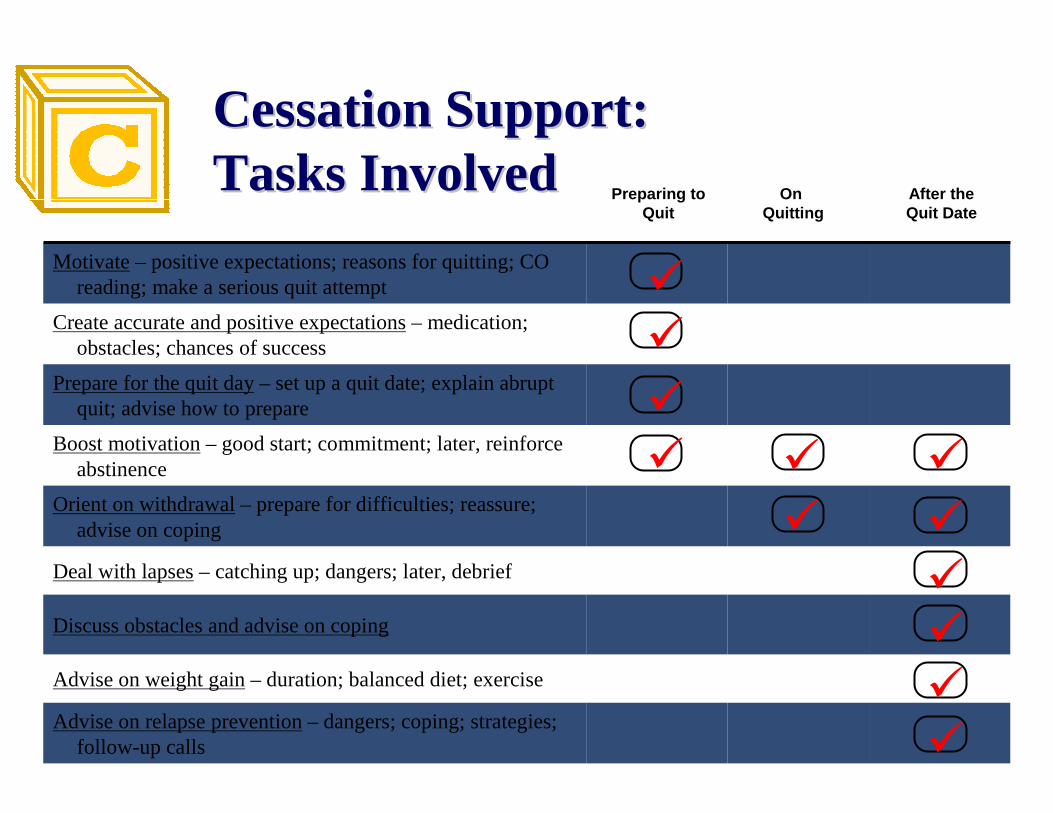
Preparing to Quit
On
Quitting
After the Quit Date
Motivate– positive expectations; reasons for quitting; CO reading; make a serious quit attempt
Create accurate and positive expectations– medication; obstacles; chances of success
Prepare for the quit day– set up a quit date; explain abrupt quit; advise how to prepare
Boost motivation– good start; commitment; later, reinforce abstinence
Orient on withdrawal– prepare for difficulties; reassure; advise on coping
Deal with lapses– catching up; dangers; later, debrief
Discuss obstacles and advise on coping
Advise on weight gain– duration; balanced diet; exercise
Advise on relapse prevention– dangers; coping; strategies; follow-up calls
�
�
�
� ��
� �
�
�
�
�
Preparing toQuit
On Quitting
After theQuit Date
Cessation Support:Cessation Support:Tasks InvolvedTasks Involved

Ramadan - August 2011
JumeirahJumeirah MosqueMosque in in DubaiDubai, (UAE), (UAE)

Q: Q: WhyWhy prescribingprescribing drugsdrugs forfor smoking smoking cessationcessation ??A: A: DrugsDrugs willwill increaseincrease up up toto 33--fold the chance of success!fold the chance of success!
CasellaCasella G, G, CaponnettoCaponnetto P, P, PolosaPolosa R. Therapeutic advances in the treatment of nicotin e addiction:R. Therapeutic advances in the treatment of nicotin e addiction:presentpresent and future. and future. TherTher AdvAdv ChronicChronic DisDis 2010; 1(3): 952010; 1(3): 95 --106.106.
OddsOdds Ratio of Ratio of abstinenceabstinence withwith first linefirst line smoking smoking cessationcessation therapytherapy
Offer Treatment to Aid the Quit AttemptOffer Treatment to Aid the Quit Attempt

Trapped by Nicotine
ADDICTION
(Physical)
HABIT
(Psycological)
NICOTINE DEPENDENCENICOTINE DEPENDENCE
Drugs forNicotine
Dependence
WithdrawalWithdrawal symptomssymptomsCravingCraving
Trapped by Nicotine
ADDICTION
(Physical)
HABIT
(Psycological)
NICOTINE DEPENDENCENICOTINE DEPENDENCE
Counseling
WithdrawalWithdrawal symptomssymptomsCravingCraving
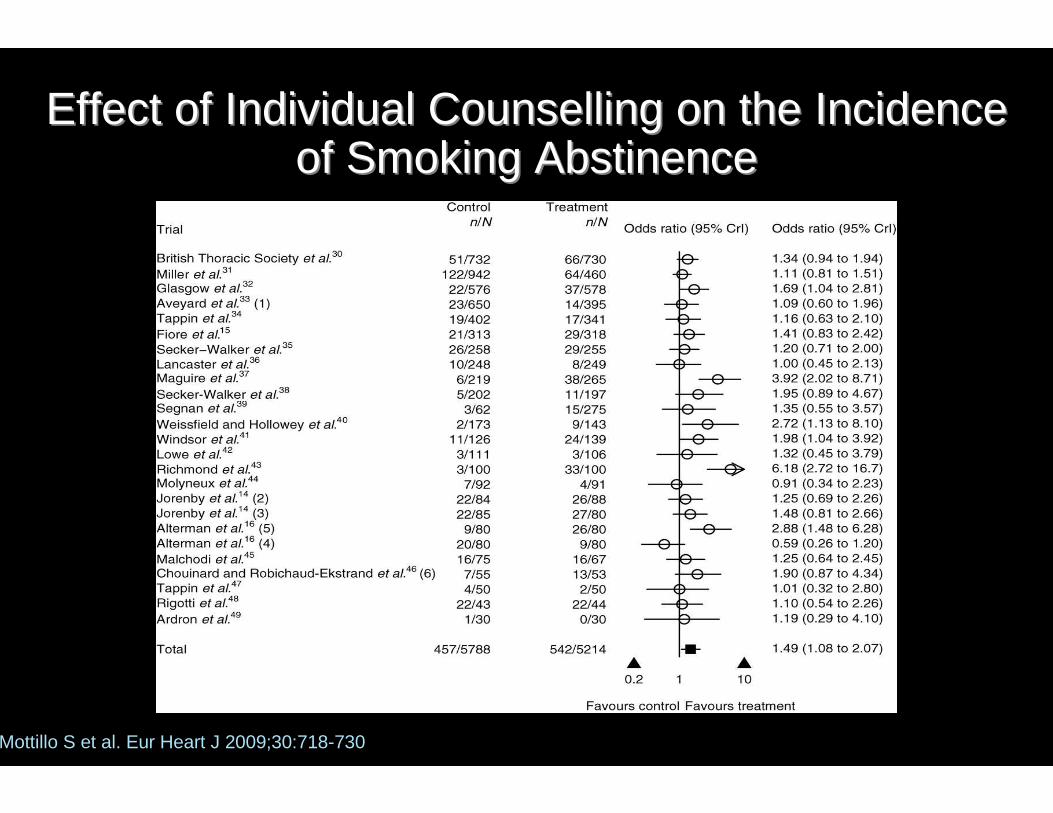
Effect of Individual Counselling on the Incidence Effect of Individual Counselling on the Incidence of Smoking Abstinenceof Smoking Abstinence
Mottillo S et al. Eur Heart J 2009;30:718-730

Combining Counseling and Medication Improves OutcomeCombining Counseling and Medication Improves Outcome
Trapped by Nicotine
ADDICTION
(Physical)
HABIT
(Psycological)
NICOTINE DEPENDENCENICOTINE DEPENDENCE
Counseling
WithdrawalWithdrawal symptomssymptomsCravingCraving

Plastic devices that are intended to provide a coping mechanism Plastic devices that are intended to provide a coping mechanism for for conditioned smoking cues by replacing some of the rituals associconditioned smoking cues by replacing some of the rituals associated ated
with smoking gestures (e.g. handwith smoking gestures (e.g. hand--toto--mouth action of smoking).mouth action of smoking).
Nicotine free inhalatorsNicotine free inhalators

OverallOverall QuitQuit Rate at 24 Rate at 24 wkwk
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PAIPO group Reference group
33.3%28.3%
Caponnetto P, et al. EFFECT OF A NICOTINE FREE INHALATOR AS PART OF A SMOKING CESSATION PROGRAM.Submitted 2010.
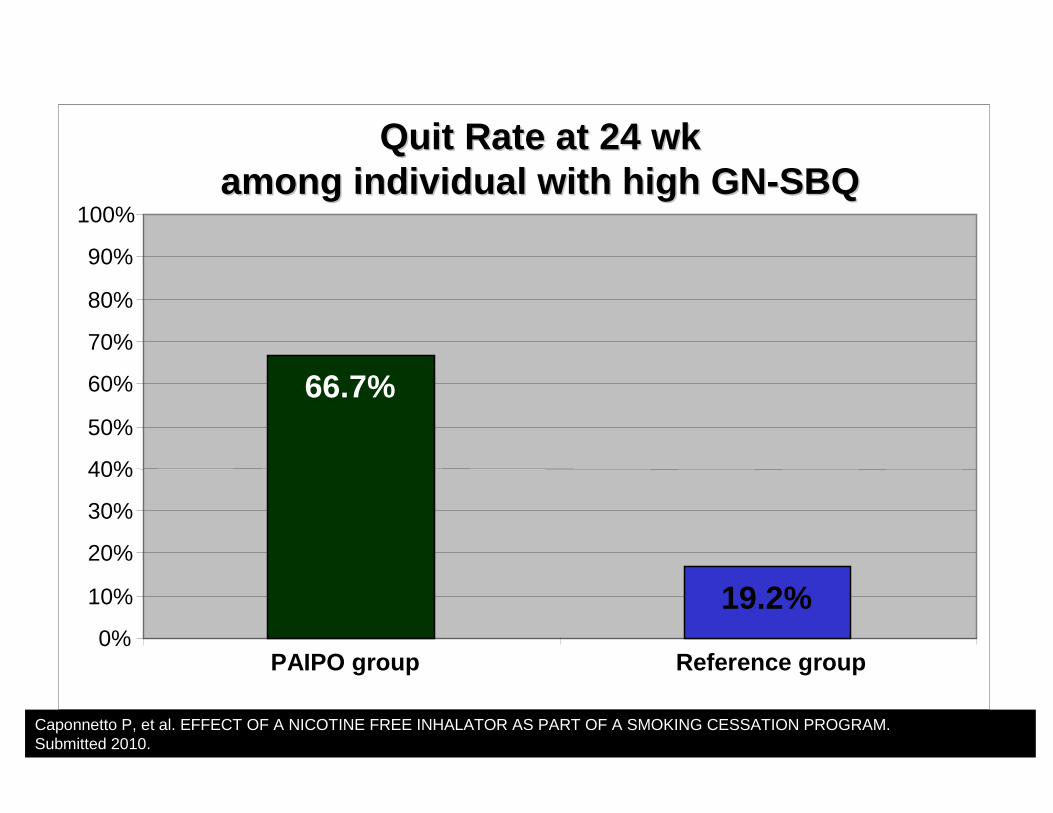
QuitQuit Rate at 24 Rate at 24 wkwkamongamong individualindividual withwith high GNhigh GN --SBQSBQ
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
PAIPO group Reference group
66.7%
19.2%
Caponnetto P, et al. EFFECT OF A NICOTINE FREE INHALATOR AS PART OF A SMOKING CESSATION PROGRAM.Submitted 2010.

Trapped by Nicotine
ADDICTION
(Physical)
HABIT
(Psycological)
NICOTINE DEPENDENCENICOTINE DEPENDENCE
Counseling
WithdrawalWithdrawal symptomssymptomsCravingCraving
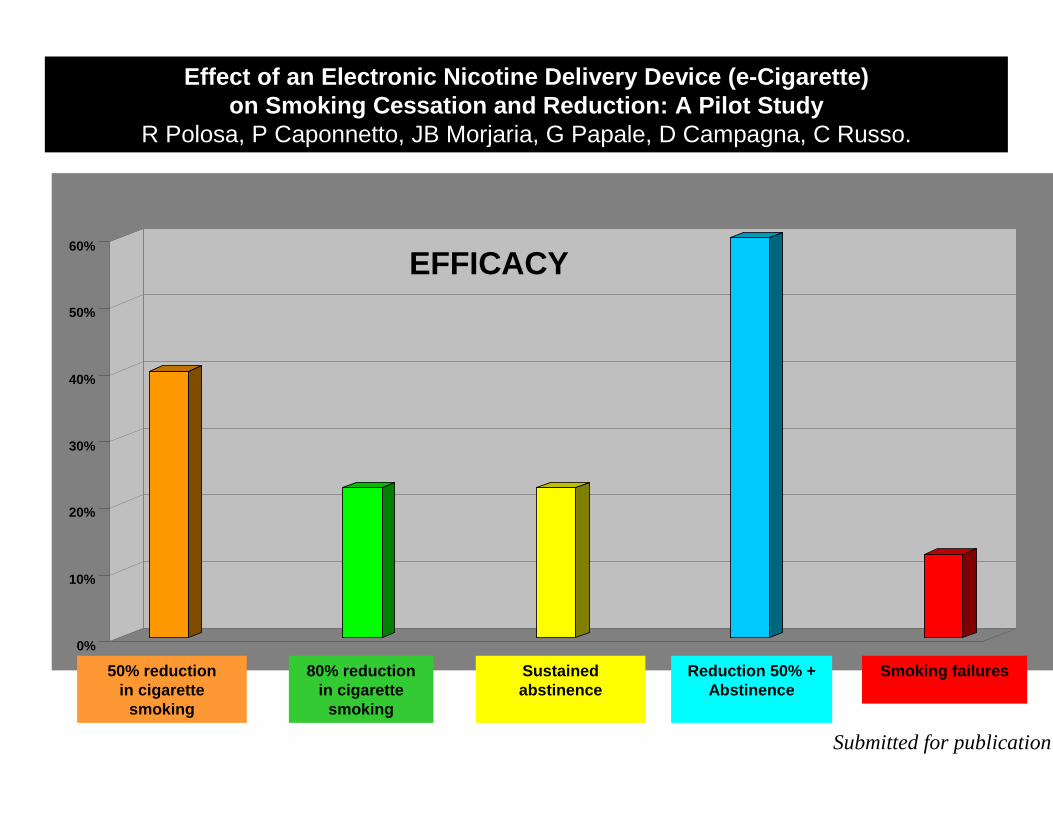
Effect of an Electronic Nicotine Delivery Device ( e-Cigarette)on Smoking Cessation and Reduction: A Pilot Study
R Polosa, P Caponnetto, JB Morjaria, G Papale, D Campagna, C Russo.
EFFICACYEFFICACY
0%
10%
20%
30%
40%
50%
60%
EFFICACYEFFICACY
50% reductionin cigarette
smoking
80% reductionin cigarette
smoking
Sustained abstinence
Reduction 50% + Abstinence
Smoking failures
Submitted for publication
4-week (% )
8-week (% )
12-week (% )
0,00%
5,00%
10,00%
15,00%
20,00%
25,00%
30,00%
35,00%
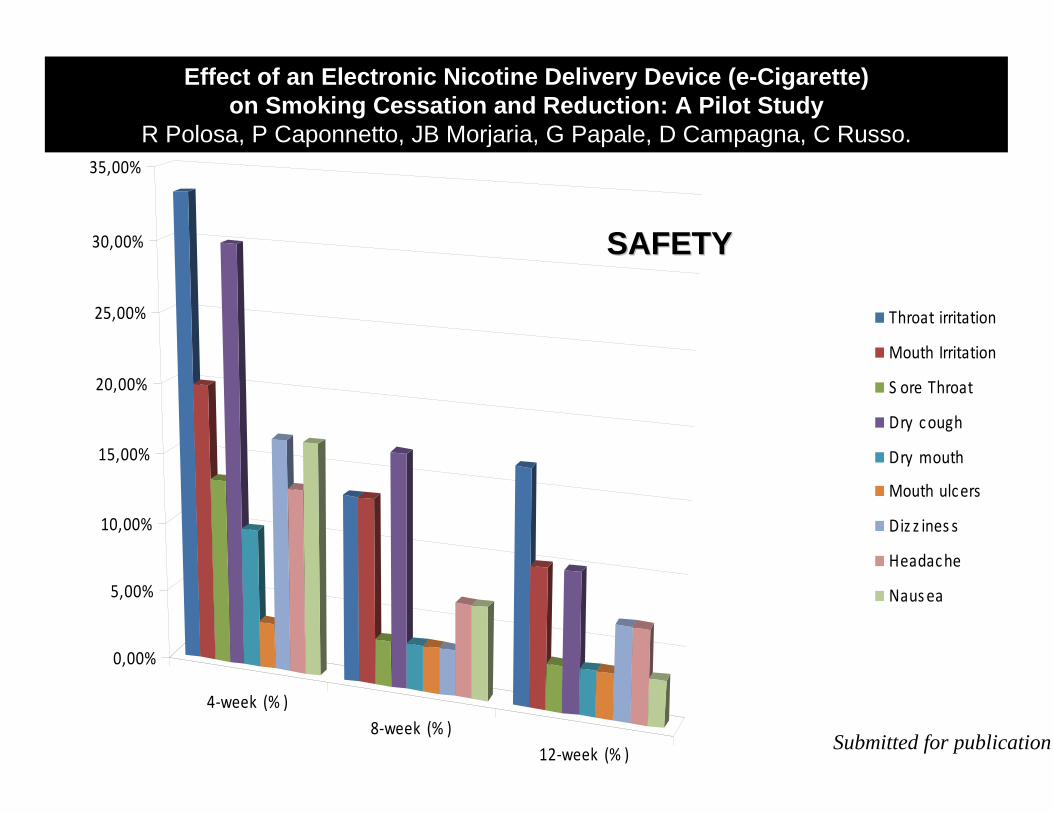
Throat irritation
Mouth Irritation
S ore Throat
Dry c ough
Dry mouth
Mouth ulc ers
Diz z ines s
Headac he
Naus ea
Effect of an Electronic Nicotine Delivery Device ( e-Cigarette)on Smoking Cessation and Reduction: A Pilot Study
R Polosa, P Caponnetto, JB Morjaria, G Papale, D Campagna, C Russo.
SAFETYSAFETY
Submitted for publication

Compared to the past, more and more smokers are try ing to quitCompared to the past, more and more smokers are try ing to quit ……
……we have the obligation to offer them the best possi ble support.we have the obligation to offer them the best possi ble support.

Comunicato ufficiale Ministero della salute arabo su sigarette elettroniche:http://www.moh.gov.ae/en/NewsDetails617.aspx
Al seguente link trovi una breve rassegna di notizie sul fumo riguardanti Dubai.http://www.no-smoke.org/goingsmokefree.php?id=637