waste management and public health: the state of the evidence
TRANSCRIPT
South West Public Health Observatory
Waste management and publichealth: the state of the evidence
A review of the epidemiological research into theimpact of waste management activities on health
July 2002
Project team:Dr Derek Pheby
Melanie GreyDr Lorenzo Giusti
Lisa Saffron
Centre for Research in Environmental Systems, Pollution and RemediationUniversity of the West of England, UWE
Waste management and publichealth: the state of the evidence
A review of the epidemiological research on theimpact of waste management activities on health
This report has been prepared by the South WestPublic Health Observatory and the Centre forResearch in Environmental Systems, Pollution andRemediation, University of the West of England, UWE,Bristol.
The South West Public Health Observatory is partof a national network of eight regional public healthobservatories, funded by the Department of Health.These were established in 2000 as outlined in theGovernment White Paper Saving Lives: Our HealthierNation. Key tasks include: monitoring health anddisease trends; identifying gaps in health information;advising on methods for health and health impactassessment; drawing together information fromdifferent sources and carrying out projects onparticular health issues.
The South West Public Health Observatory alsoforms a key part of the developing South WestRegional Observatory. This is a wider regionalintelligence function, currently supported by theDepartment of Health, Government Office for theSouth West, the South West of England RegionalDevelopment Agency, the Regional Assembly and theEnvironment Agency.
Further information about the work of the SouthWest Public Health Observatory can be found atwww.swpho.org.uk.
Addresses for correspondence:
Lisa SaffronUnit of Applied EpidemiologyUniversity of the West of EnglandFrenchay CampusColdharbour LaneBristol BS16 1QY
Email: [email protected]
or
South West Public Health ObservatoryKing Square HouseKing SquareBristol BS2 8EE
Email: [email protected]
© South West Public Health Observatory 2002Published by the South West Public Health ObservatoryISBN 0-9541359-3-8

i
Thanks are due to all the contacts and advisorygroup and the anonymous contributors for their help.Throughout the process, there has been input from avariety of people working in the field. As well as visitsto people working in the Environment Agency andwaste disposal authorities, an advisory group met on15 October 2001 to discuss the report. Feedbackfrom these discussions was influential in determiningthe direction of the project.
The research was funded and supervised bySelena Gray and Helen Cooke of the South WestPublic Health Observatory. Constructive comments
Acknowledgements
and input were made by Alistair Gordon(Environment Agency South West), Emma Hayes,(Environment Agency Bristol), Joyshri Sarangi (AvonHealth Authority), James Longhurst (University of theWest of England), Melanie Grey (University of theWest of England), Rob Quigley (Health DevelopmentAgency, London), Erica Ison, (Oxford), PaulJohnstone (Greenpeace Research Laboratory),Martine Vrijheid (London School of Hygiene andTropical Medicine), and Ronan Lyons (University ofWales Swansea).
ii
Contents
Acknowledgements ...................................................................................... iList of figures .............................................................................................. iiiList of tables ................................................................................................ iiiSummary .................................................................................................... iv
1 Introduction ...................................................................................... 11.1 Background ......................................................................................... 11.2 Aims .................................................................................................... 11.3 Methods ............................................................................................... 1
2 Waste management .......................................................................... 42.1 Background ......................................................................................... 42.2 Managing waste.................................................................................... 52.3 Waste management regulation ............................................................. 112.4 Waste management in the South West .................................................. 11
3 Impact on human health ................................................................ 133.1 Definition of health ............................................................................. 133.2 Case studies ...................................................................................... 133.3 Quantifying factors which may affect health .......................................... 133.4 Exposure routes ................................................................................. 173.5 Assessing exposure ............................................................................ 203.6 Potential impacts on health .................................................................. 21
4 Evidence of an impact on health .................................................... 244.1 Types of study .................................................................................... 244.2 Study limitations and confounding factors ............................................. 254.3 The strength of the association ............................................................ 28
5 Summarising the evidence ............................................................. 305.1 Making a judgement ........................................................................... 305.2 Landfill ............................................................................................... 315.3 Incineration ....................................................................................... 315.4 Composting ....................................................................................... 315.5 Sewage discharges ............................................................................. 315.6 Soil amendments ................................................................................ 325.7 Summary of judgements ..................................................................... 33
6 Protecting the health of the public ................................................ 346.1 National policy .................................................................................... 346.2 Decision making in the face of uncertainty ............................................ 346.3 The role of public health agencies ........................................................ 36
7 Recommendations ........................................................................... 39
8 Conclusions ..................................................................................... 40
9 References ...................................................................................... 41
AppendicesAppendix 1: The literature search................................................................... 48Appendix 2: How judgements were derived or justification for judgements ........ 50Appendix 3: Strategies and local plans in the South West ................................. 56Appendix 4: Summary and appraisal of reviews .............................................. 58
iii
List of tables
Table 1 Judgements about the evidence of thehealth impacts of the main waste management procedures ................. vi
Table 2 Types of waste ................................................................................. 4Table 3 Strategies for waste disposal: advantages and disadvantages ............. 9Table 4 The roles and responsibilities of the authorities involved
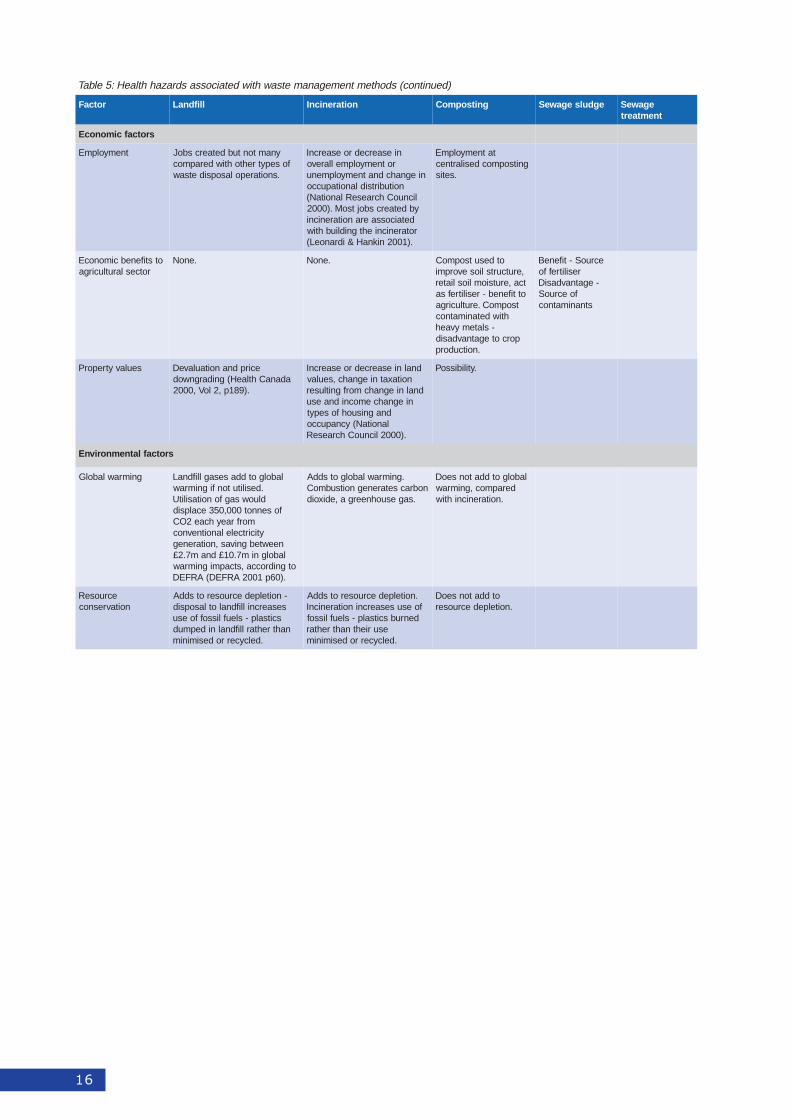
in waste management ...................................................................... 11Table 5 Health hazards associated with waste management methods .............. 14Table 6 Hierarchy of study designs ............................................................... 24Table 7 Relative risk and judgements ........................................................... 28Table 8 Examples of environmental factors where there is
strong and conclusive evidence of an adverse impact on health .......... 29Table 9 Examples from studies on waste management and health .................. 29Table 10 Health outcomes investigated in primary studies of landfill sites .......... 30Table 11 Health outcomes investigated in primary studies of incineration .......... 31Table 12 Health outcomes investigated in primary studies of sewage
discharges ...................................................................................... 32Table 13 Summary of judgements ................................................................. 33
Appendices
Table A Number and types of studies identified .............................................. 49Table B Strategies and local plans in the South West ...................................... 56Table C Reviews on the health impacts of landfill ........................................... 58Table D Reviews on the health impacts of incineration .................................... 60Table E Reviews on the health impacts of sewage discharges ......................... 61
List of figures
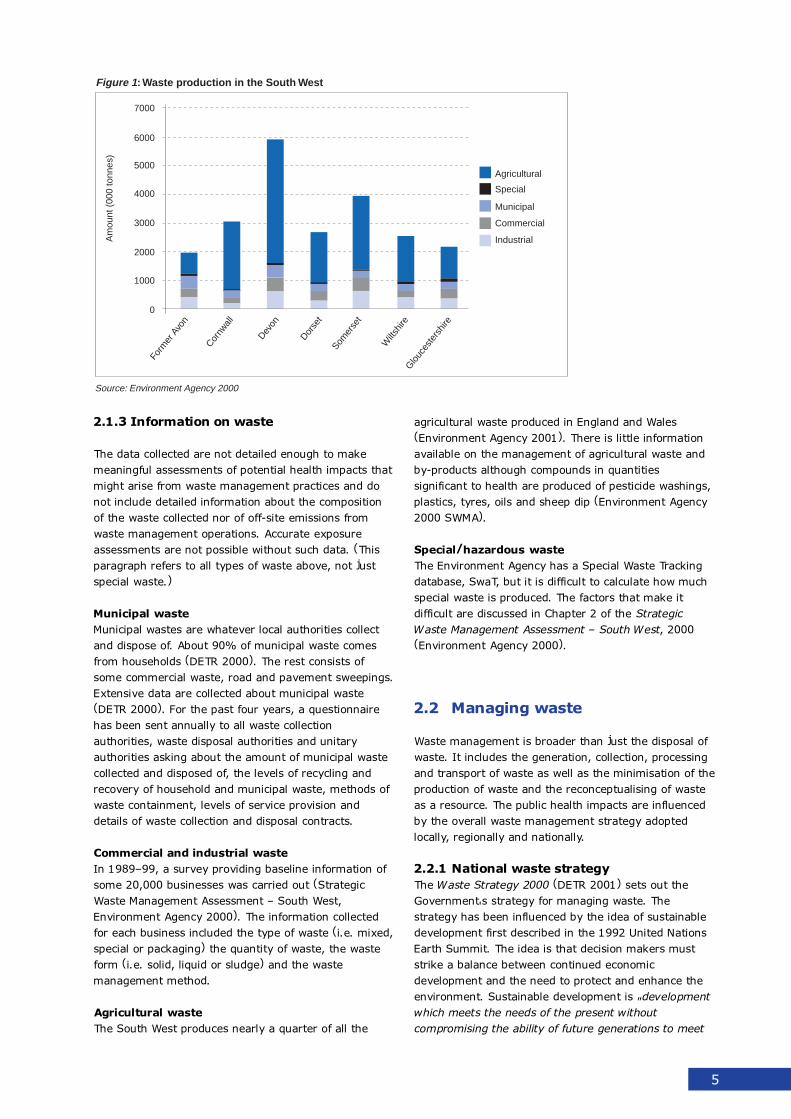
Figure 1 Waste production in the South West ..................................................... 5
Figure 2 The waste hierarchy ........................................................................... 6
Figure 3 Recycling rates by local authority 1998. South West ............................. 12
Figure 4 Waste management facilities in the South West in 1998-99 ................... 12
Figure 5 Exposure pathways from a landfill site ................................................ 19
Figure 6 Hierarchy of exposure data ................................................................ 21
Figure 7 Health impacts .................................................................................. 22
Box 1: Guidelines on assessing exposure to hazards released fromwaste sites: five essential steps .......................................................... 20
Box 2: Questions the public want answered .................................................... 36

iv
Summary
The aim of this project was to provide an overview ofthe health impacts of different methods of wastemanagement methods so as to inform public healthinput into the waste management regulatory system.Public health input into the development of local,regional and national waste strategies has not beenroutinely sought nor offered, while public health inputinto the Integrated Pollution Prevention and Control(IPPC) process has only recently become a statutoryresponsibility. Health authorities and their consultantsare ill prepared for their new role as advisors in thefield of waste management. Those working in wastemanagement lack expertise to interpret andincorporate health information into decision making.There is a need for decision makers and advisors towork together, to develop a shared understanding ofthe issues and to learn a common language.
This report is intended as a resource for publichealth advisors and decision makers in the field ofwaste management. It provides a summary of theepidemiological evidence about the health impacts ofwaste management methods. It can be used asbackground material to supplement the IntegratedPollution Prevention and Control: a Practical GuideFor Health Authorities (Kibble & Saunders 2001) andas a resource pack for use in a Health ImpactAssessment. It is hoped this project will build bridgesbetween those in public health and those in wastemanagement so that waste management decisionsfully take into account the possible health impacts inlight of the scientific evidence.
The questions addressed in this report are:
1. How is waste managed in England and particu-larly in the South West?
2. How might waste management practices impacton human health?
3. How strong is the evidence that current wastemanagement practices have had an impact onhuman health?
4. How can the evidence be used in waste manage-ment strategies and practice to protect the healthof the public?
A summary of the findings of each question isshown below.
Waste management practice
Waste is a complex mixture of different substancesand objects, only some of which are intrinsicallyhazardous to health. However, any type of waste hasthe potential to affect health depending on thecollection system used, the location where waste isgenerated, and the waste management strategyemployed.
Waste management is broader than just thedisposal of waste. It includes the generation,collection, processing and transport of waste as wellas the minimisation of the production of waste andthe reconceptualising of waste as a resource. Thepublic health impacts are influenced by the overallwaste management strategy adopted locally,regionally and nationally. The waste managementoptions chosen by decision makers could have animpact on health both directly and indirectly:
1. Directly, by leading to potential adverse and/orbeneficial health impacts such as increased riskof cancer or decreased quality of life,
2. Indirectly, by the broader environmental impacton the global ecology, such as the contribution toglobal warming, loss of bio-diversity and thedepletion of non-renewable resources.
The National Waste Strategy proposes the conceptof the Best Practicable Environmental Option � i.e."the option that provides the most benefits or theleast damage to the environment as a whole, atacceptable cost, in the long term as well as in theshort term". The Best Practicable EnvironmentalOption is likely to be a mix of different wastemanagement methods. To guide decision makers, theStrategy proposes a "waste hierarchy" whichprioritises reduction, re-use, and recovery abovedisposal.
This holistic approach, if adopted, would go a longway towards reducing the health risks associated withparticular waste management options. An integratedwaste management system requires separation ofwaste as well as restrictions on certain productionpractices that introduce toxic materials into widelydistributed household products. The current systemresults in health risks because it does not includeproduction and consumer use in the materials flowcycle. Many of the risks that arise in the last stage ofthe materials flow cycle, i.e. the disposal stage, resultfrom actions taken at the earlier stages ofproduction, packaging and marketing.

v
The main methods reviewed in this report are:� Recycling/recovery options, i.e. composting and
landspreading sewage sludge.� Waste processing options, i.e. incineration.� Waste disposal options, i.e. discharge of treated
sewage effluent; landfill.
Potential impact of wastemanagement practice on health
Using the World Health Organisation definition ofhealth as a 'state of complete physical, mental andsocial well-being and not merely the absence ofdisease and infirmity' provides a foundation foridentifying factors associated with wastemanagement that might have an impact on health.Factors may be beneficial, damaging or neutral. Theymay be present in the waste or formed during thewaste management process.
With improvements in analytical methods,contaminants can be identified at very lowconcentrations, so low that their implications forhuman health can only be guessed at.
In most cases, a mixture of different contaminantswill be present. The implications of mixtures ofcompounds is unknown. The risks may be additive orsynergistic, i.e. there may be interaction effects thatmake the risks higher or lower than that predicted byanalysing individual contaminants separately. Theremay be no interactions at all, with each compoundacting independently.
It is difficult to determine what relationship any ofthese factors have to health impacts and even moredifficult to quantify their effects. Identifying andmeasuring hazards gives an impression of accuracyand leads to the assumption that the measurablerisks from physical hazards are more substantial andimportant than those from psychosocial hazards. Infact, data about physical hazards are alsoincomplete. Information is lacking about the toxicity,persistence and ability to bio-accumulate of many ofthe hundreds of thousands of chemicals that end upin waste.
Exposure
For physical hazards, the crucial link between ahealth hazard and a health outcome is exposure. Therisk to health depends not only on how much ispresent but also on whether there is a route by whichpeople may be exposed. An exposure pathway hasthree elements:
1. Release from the site � air, water, solids2. Transport through environmental media3. Uptake by people � inhalation, ingestion of food
or drinking water, skin contact, fire and explosionIf there is no exposure, there is no threat to health.
Exposure assessment involves the following:
1. Site characterisation2. Characterisation of receptors3. Characterisation of exposure pathways4. Determination of concentrations of contaminants5. Exposure estimation
In general, high-dose exposure and long-term,low-dose exposure are more likely to result in healthimpacts than short-term, low-dose exposures.However, it is extremely difficult to define exposureand thus observe a dose-response relationship inpeople exposed to contaminants from wastemanagement sites.
Health impacts
Health impacts result from an interaction between thefactors affecting health and the health status ofexposed populations. The health outcomes aredetermined by the contaminant levels and thesusceptibility of individuals, ranging from mortality athigh levels of exposure to body burdens with nodiscernible effects at low levels of exposure.Commonly studied health impacts are reproductiveoutcomes, symptoms, diseases, and biomarkers.
Evidence of impact of wastemanagement practice on health
In a "weight of evidence" approach to evaluating theevidence, greater weight is placed on the conclusionsdrawn from some types of study over others. Thestudy designs at the top of the hierarchy (see Table6) � i.e. studies on people � are those most likely tolead to valid conclusions from which generalisationscan be made. Evidence from studies on people ismore conclusive than extrapolations from studies onanimals. Animal studies carry more weight thanstudies on parts of organisms outside the body or onrelated chemicals. Amongst the different kinds ofstudies on people, the ones higher up the hierarchy,i.e. experimental studies and prospective cohortstudies are useful for testing hypotheses andestablishing whether a causal relationship exists. Thestudy designs further down the hierarchy, i.e.observational studies without controls, are useful forgenerating hypotheses which subsequently needconfirmation from study designs further up thehierarchy.
It is difficult to establish a cause-and-effectrelationship in epidemiological studies in this areabecause of the incompleteness of the data, inherentvariability and confounding by other unrelated factorsthat may explain the results as well as the factorunder investigation. Confounding takes place whenthe exposure is associated with some other factorwhich also increases the risk of the health outcome

vi
studied. This includes other sources of pollutants andother factors which affect health status. Informationmay be incomplete because of lack of exposure data,unreliable health data, or low statistical power.Variability occurs in both the human populationsstudied and the waste procedures. Whilst it istechnically possible to detect the presence of healthhazards in waste sites and health impacts amongpeople working or living nearby, there are manyproblems demonstrating the relationship betweenexposure and the health impacts observed. The mainlimitations of epidemiological investigations are thesmall sample size, lack of exposure information, lackof toxicological data about mixtures of chemicals andthe lack of specificity of indicators of adverse healtheffects.
An association, even if statistically significant, isnot necessarily proof of causation. To determinecausation, the cause must precede the effect and theassociation should be "consistent, unbiased, strong,graded, coherent, repeated, predictive and plausible"(WCRF and AICR, 1997). A useful framework fordescribing the strength of evidence has beendeveloped by WCRF and has been used here (see5.1 for further details). Possible judgements are�convincing�, �probable�, �possible� and �insufficient�evidence of a causal association.
The results of applying this framework to theliterature are shown in Table 1 below.
Protecting the health of the public
This overview of the scientific evidence exposes ahigh degree of uncertainty about the impact of wastemanagement operations on health, which may ormay not ever be resolved by further research.Despite the impressive amount of research and thehigh quality of many of the studies, the state of theevidence is such that, with a few exceptions, nocertain conclusions can be drawn.
Disagreement about the management of apotentially risky activity like incineration arises notonly because of different interpretations of thescientific evidence but because of the differentjudgements people make about how risky theybelieve the activity to be. Individuals as well asregulatory bodies try to avoid or control activitiesthey judge to be too risky and ignore or tolerateothers. Conflict occurs when people form differentjudgements about the riskiness of the activity.Disagreements about risk are inevitable becausethere is no way to define risk that does not includevalues, beliefs and assumptions � especially wheninformation on which to base the judgement isscarce.
Where there is uncertainty, judgements about riskare based on assumptions and mental strategies thathelp decision making and on qualitative aspectsinherent in a hazard. As well as the likelihood of
harm, people consider whether incurring the risk isvoluntary, has potential catastrophic consequences, isunknown and unfamiliar, and is new to society.Judgements about risk are also influenced byindividuals' views of the world and the kind of societythey want.
Precautionary principle
One way to manage the risks associated with wastemanagement is to apply the precautionary principle."Where there are threats of serious or irreversibledamage, lack of full scientific certainty shall not beused as a reason for postponing cost-effectivemeasures to prevent environmental degradation.When in doubt about the impact of a development, itwill be managed according to the worst-case scenarioof its impact on the environment and human health."(UNCED 1992.) The conditions under which theprecautionary principle applies are:
� When health effects are most serious orirreversible
� When the subject is a matter of scientificuncertainty and full evidence is lacking
� When cost-effective measures are possible.
ConclusionsThe data collected about waste are not detailedenough to make meaningful assessments of potentialhealth impacts that might arise from wastemanagement practices. The data do not include
:1elbaT htlaehehtfoecnediveehttuobastnemegduJserudecorptnemeganametsawniamehtfostcapmi
ecnedivE ksirsesaercnI
gnicnivnoC nignihtabdnasmotpmyslanitsertniorsaG.sretawlanoitaercerdetanimatnocegawes
elbaborP ,ehcadaeh,smelborptcartlanitsetniortsaGnignikrowdnasmotpmyssyawriadnaeugitaf
.stnalptnemtaertegawes
elbissoP .ytilicafgnitsopmocdesilartnecatagnikroW
tneiciffusnI lilfdnalraenecnediserdnasemoctuohtlaehynAetis
llifdnalatagnikrowdnasemoctuohtlaehynA.etis
natagnikrowdnasemoctuohtlaehynA.rotarenicni
raenecnediserdnasemoctuohtlaehynA.rotarenicni
raenecnediserdnasemoctuohtlaehynA.ytilicafgnitsopmocdesilartnec
tnemtaertegawesnignikrowdnarecnaC.seitilicaf
egawesgnidaerpsdnaldnasemoctuohtlaehynA.egduls

vii
detailed information about the composition of thewaste collected nor of off-site emissions from wastemanagement operations. Accurate exposureassessments are not possible without such data.
The nature of existing epidemiological research inthis area is such that most studies are useful forgenerating hypotheses but are unable to test thehypotheses or to provide convincing evidence of anassociation between exposure and a health impact.
For most waste management methods, theevidence is insufficient to claim that adverse healthoutcomes will result. The exception is the convincingevidence that bathing in sewage contaminatedrecreational waters increases the risk ofgastrointestinal symptoms, even when the watermeets present guideline levels of faecal coliforms.
Implementation of the current Waste Hierarchyand the Precautionary Principle through the adoptionof an integrated waste management strategy atnational, regional and local level will be the mosteffective way to reduce the health risks from wastemanagement procedures.
1
1 Introduction
1.1 Background
Waste disposal and health was identified as a priority bySouth West Public Health Observatory (SWPHO), in2000. This was because changes to current wastemanagement strategies, e.g. pyrolysis and moreincinerators, may have an impact on public health. Inline with their function to identify gaps in healthinformation and to give early warning of future healthissues, SWPHO wanted to find out what these impactsmight be and to have an input into policy making bywaste planning authorities in the South West.
1.2 Aims
These were clarified in a series of meetings withmembers of the South West Public Health Observatoryand the University of the West of England project team.It was agreed that the following questions would beaddressed:
1. How is waste managed in England and particularly inthe South West?
2. How might waste management practices impact onhuman health?
3. How strong is the evidence that current wastemanagement practices have had an impact on humanhealth?
4. How can the evidence be used in waste managementstrategies and practice to protect the health of thepublic?
1.3 Methods
1.3.1 The literature search
To answer the questions above, a literature search wasundertaken. The first step was a scoping exercise to findout what literature was available. Once key decisionswere made to narrow down the search, a thoroughsearch was carried out. Details of the search strategiesemployed are described in Appendix 1. During theliterature search, a database was kept of the referencesfound and a classification scheme developed (detailsavailable from authors). Throughout the process, therehas been input from a variety of people working in thefield (see Acknowledgements).
1.3.2 Evaluating the reviews
When carrying out a literature review, the second phaseis to check whether adequate reviews already exist
(CRD 2001, WHO Working Group 2000). Guidelines forassessing reviews were applied (Welsh Office 1999,WHO Working Group 2000, CRD 2001) using thefollowing questions:
i) Agreement on question to be dealt withWhat is the review's objective?
ii) Identification of all relevant studiesWhat sources were searched to identify primarystudies? Was there an explicit search strategy, aneffort to include all available studies, searching ofbibliographic databases, inclusion of non-Englishlanguage reports?
iii) Assessment of quality of the studiesWhat were the inclusion criteria and how were theyapplied? What criteria were used to assess thequality of primary studies and how were theyapplied? (study question clear, exposure assessedusing valid and reliable measures, health outcomeassessed using valid and reliable measures, studydesign appropriate, data analysis takes intoconsideration chance, confounding and bias,conclusions consistent with the results of the dataanalysis).
iv) Interpretation of the evidenceHow were the data extracted from the primarystudies and how were the data synthesised? Howwas heterogeneity between studies investigated?How were data combined? Was it reasonable tocombine studies and summary results of review?Do conclusions flow from the evidence reviewed?Use of meta-analysis?
Meta-analysis is an approach which involves theaggregation of results from a number of publishedstudies in order to provide a quantitative assessment ofthe extent to which bias might account for observedresults and of the patterns, and sources ofheterogeneity. A meta-analysis can only be done if thebiases and confounding factors are adequatelyaddressed in the studies and if the studies measured thesame exposures in the same way and compared riskbetween or among similar levels of exposure. For mostepidemiological studies of the health impacts of wastemanagement systems, exposure data are missing andthere is no confounding control. With the exception ofone review (Pruss 1998), none of the reviews attemptedto aggregate results and none carried out meta-analyses.

2
1.3.3 Making judgementsAs most of the reviews were unable to do more thansummarise the literature and its limitations, a differentmodel was sought to make sense of the evidence. Themodel used to appraise the evidence in this paper is theone used by the World Cancer Research Fund toevaluate the role of food and nutrition in the preventionof cancer (WCRF & AICR 1997). The model consists ofguidelines for making judgements about the reliabilityand strength of the evidence and was chosen becausethe judgements are straightforward and easy tocomprehend with relatively clear criteria for inclusion.
tnemegduJ noitaterpretnI airetirC
gnicnivnoC evisulcnocsierehT-esuacafoecnedive
tceffe-dna.noitaicossa
.slacimehcroslaminanoseidutsyrotarobaltsujton,snoitalupopnamuhnoeraseidutsehT.1
,sksirevitalergnortshtiw,seidutsgnitset-sisehtopyhforebmunelbaredisnocaeraerehT.2.02nahteromylbareferp
gniwohsseidutswefhtiw,seidutsehtfotsomnidevresbodnatnetsisnocsinoitaicossaehT.3.etisoppoeht
.rofdellortnocneebevahsrotcafgnidnuofnocelbissoP.4
evitcepsorpgnidulcniylbareferp,sngisedydutsgnitset-sisehtopyhfoegnaraeraerehT.5.seiduts
.spuorgnoitalupoptnereffidnituodeirracneebevahseidutS.6
emitehtotreferdluohsataD.tceffehtlaehehtedecerptsumdrazahehtfoecnaraeppaehT.7.emoctuohtlaehehtfoecnerruccoehtgnidecerp
.pihsnoitalerehtmrifnocdluohsyeht,devresboeraspihsnoitaleresnopser-esodfI.8
.elbisualpyllacigoloibebdluohssnoitaicossaehT.9
rehtohtiwtcilfnoctonodatadehtfonoitaterpretnitceffednaesuaceht-ecnerehoC.01ylgnortsroevitroppusyllaususiecnediveyrotarobaL.emoctuohtlaehehtfoegdelwonk
.evitroppus
foksirehtsesaercednoitpmusnoctiurfdnaelbategevtahtgnicnivnocsiecnediveeht:elpmaxElacigoloce41dnalortnoc-esac691,trohoc73nodesabsitnemegdujsihT.srecnaclareves
tceffeevitcetorptnacifingisyllacitsitatsasawereht,seidutslortnoc-esacehtfo%08nI.seidutseromroenorofmutcerdnasaercnap,sugahpaseo,gnul,ytivaclaro,hcamotsehtfosrecnacrof
.)3.6pahC,7991RCIA&FRCW(seirogetactiurfro/dnaelbategev
elbaborP noitaicossalasuacA.ylekilsi
erehT.noitaicossaehtgnitroppustonemoshtiwseidutsehtgnomaycnetsisnocsselsierehT.evitroppusylgnortsroevitroppusyllaususiecnediveyrotarobaL.seidutsrewefera
eraerehtesuaceB.recnaclatcerolocfoksirehtsesaercniylbaborplohoclA:elpmaxEeht,seidutslortnocesac02nahteromdnaseidutstrohoc11morfstlusertnetsisnocni
ybdemrifnocerastluser,dnertemitatroppusseidutsehtrevewoH.gnicnivnoctonsitnemegduj.)5.5pahC7991RCIA&FRCW(deifitnedineebevahsmsinahcemelbisualpdna,seidutslamina
elbissoP aebyamerehTpihsnoitalerlasuacsiecnediveehttub
othguonegnortston.eruseb
seidutsgnitsixero;seidutsynamyrevebtonyamereht,revewoH.noitaicossanawohsseidutSecnediveevitroppusebtonyamroyamerehT.tnetsisnocnierastluserroytilauqroopfoera
.senilpicsidrehtomorfecnediveevitroppusylgnortssierehttubseidutsyrotarobalmorf
nodesabsitnemegdujsihT.recnacgnulfoksirehtsesaercniylbissoplohoclA:elpmaxEgnidnuofnocerehwseidutslortnocesaclarevesdnaseidutstrohoc6morfstlusertnetsisnocni
)5.5pahC7991RCIA&FRCW(.ylekilerasrotcaf
tneiciffusnI yleremecnediveehTlasuacastseggus
oN.noitaicossaebnactnemegduj
.edam
ehtfoytilauqroopehttubtnetsisnocebyamhcihwseidutsforebmundetimilaeraerehT.mehtmorfnwardsnoisulcnocehtfoytilibailerehttimilseiduts
dooffonoitanimatnocmuimdacneewtebknilehttuobaedamebnactnemegdujoN:elpmaxEoterusopxelanoitapuccotuobastroperlareveseraerehthguohtlA.recnacetatsorpdna
oneraereht,yticinegonicracrofmsinahcemelbisualpadnarecnacetatsorpdnamuimdac.erusopxeyrateidmorfksirdesaercninagniwohsseiduts
Assessment of the strength of the evidence dependson two factors:
1. the scale of the association demonstrated betweenexposures and presumed health outcomes and
2. its statistical significance (i.e. the likelihood thatsuch an association could have arisen by chance.)To determine the strength of an association, the conceptof relative risk is generally used. (See section 4.3 forfurther details). However, an association, even if strongand statistically significant, is not proof of causation. Todetermine causation, we took the following criteria fromthe approach used to evaluate the diet and cancerevidence:
3
From these categories, an algorithm was developedto help to make the judgements about the evidence onthe associations with health outcomes from the differentwaste practices.
Based on the review articles, abstracts and theprimary papers found in the literature search, this
algorithm was used to assign judgements to theevidence about the health impacts of landfill,incineration, sewage treatment, sewage sludgelandspreading and composting.
1 Have studies been done on human populations?
NOClassify as Insufficient
YES
2 Have hazards been identified? Does the appearance of the hazard precede the health outcome? Is the associationbiologically plausible? Is there data on exposure?
NOClassify as Insufficient
YES
3 Are there ANY hypothesis-testing studies?
NOClassify as Insufficient
YES
4 Have any of the hypothesis-testing studies controlled for possible confounding factors?
YES NO
5 Are there more than 20 hypothesis-testing studiesconsistently showing strong or moderate relativerisks? Are there a range of study designs? Havestudies been carried out in different populationgroups? If dose-response relationships are ob-served, do they confirm the association between thehazard and the health outcome?
6 Is the association mostly consistent? Is laboratoryevidence usually or strongly supportive?
YESClassify as
Convincing
NOClassify as Probable
YESClassify as Probable
NOClassify as Possible
4
2 Waste management
This section is a summary of current waste managementpractice in England with particular emphasis on theSouth West and the public health implications.
2.1 Background
2.1.1 Sources of wasteAccording to the Environment Act 1995, waste is definedas "any substance or object which the holder discards orintends or is required to discard." Waste is a complexmixture of different substances and objects, only someof which are intrinsically hazardous to health. However,any type of waste has the potential to affect healthdepending on the collection system used, the locationwhere waste is generated, and the waste managementstrategy employed. For example, a plastic bottle isunlikely to be responsible for any adverse health effectswhen buried in landfill. However, the same plastic bottleburned in a poorly managed incinerator could generatedioxins which could potentially lead to an increased riskof cancer in people working in or living down wind of theincinerator.
Sewage is any type of waste that passes through thesewage treatment process. As well as pathogenic micro-organisms from human excrement, sewage containsmany other hazards to health � heavy metals and toxiccompounds from road run-off waters, toxic andendocrine-disrupting compounds from toiletries,cosmetics, and detergents, pesticides from surfacewater run-off, and natural hormones from human urine.
2.1.2 Quantity of wasteIn the South West, 11 million tonnes of controlled wastewere handled, treated or disposed of in the year 1998/99. This included 5.2 million tonnes of commercial andindustrial waste and 2.5 million tonnes of municipalwaste but does not include sewage sludge. The amountof waste produced in the South West did not exceed12% of the total for England and Wales, which isproportional to the number of people and industriesbased in the South West. In addition, approximately14.5 million tonnes of waste was produced by theagricultural sector, with Cornwall, Devon, and Somersetproducing the most. (See Figure 1.)
Household waste
Special/hazardous waste
Industrial waste
Commercial waste
Agricultural waste
Mining and quarrying waste
Explosive waste
From domestic premises, civic amenity sites, street sweeping, prisons, campsites, household hazardous waste, household clinical waste, school waste.
Controlled waste of any kind that may be dangerous to treat - covered by the Special Waste Regulations 1996.
From hospitals, laboratories, workshops, dredging,noxious waste from certain processes, e.g. drycleaning and paint mixing, waste oils, scrapmetals, waste from ships, aircraft, commercialgarages, premises for animals, nuclear waste.
From offices, hotels, clubs, showrooms, privategarages, markets, government departments,council offices, parks and gardens, courts,corporate bodies.
Manure, slurry, crop residues, animal treatmentdips, packaging.
Controlledwaste
Covered by EPA (EnvironmentalProtection Act1990) andCOPA (Controlof Pollution Act1974).
Uncontrolledwaste
Covered by separatelegislation.
W A
S T
E
Table 2: Types of waste
Sewage sludge When landfilled or incinerated.
Sewage sludge When spread on agricultural land.
5
2.1.3 Information on waste
The data collected are not detailed enough to makemeaningful assessments of potential health impacts thatmight arise from waste management practices and donot include detailed information about the compositionof the waste collected nor of off-site emissions fromwaste management operations. Accurate exposureassessments are not possible without such data. (Thisparagraph refers to all types of waste above, not justspecial waste.)
Municipal wasteMunicipal wastes are whatever local authorities collectand dispose of. About 90% of municipal waste comesfrom households (DETR 2000). The rest consists ofsome commercial waste, road and pavement sweepings.Extensive data are collected about municipal waste(DETR 2000). For the past four years, a questionnairehas been sent annually to all waste collectionauthorities, waste disposal authorities and unitaryauthorities asking about the amount of municipal wastecollected and disposed of, the levels of recycling andrecovery of household and municipal waste, methods ofwaste containment, levels of service provision anddetails of waste collection and disposal contracts.
Commercial and industrial wasteIn 1989�99, a survey providing baseline information ofsome 20,000 businesses was carried out (StrategicWaste Management Assessment � South West,Environment Agency 2000). The information collectedfor each business included the type of waste (i.e. mixed,special or packaging) the quantity of waste, the wasteform (i.e. solid, liquid or sludge) and the wastemanagement method.
Agricultural wasteThe South West produces nearly a quarter of all the
agricultural waste produced in England and Wales(Environment Agency 2001). There is little informationavailable on the management of agricultural waste andby-products although compounds in quantitiessignificant to health are produced of pesticide washings,plastics, tyres, oils and sheep dip (Environment Agency2000 SWMA).
Special/hazardous wasteThe Environment Agency has a Special Waste Trackingdatabase, SwaT, but it is difficult to calculate how muchspecial waste is produced. The factors that make itdifficult are discussed in Chapter 2 of the StrategicWaste Management Assessment � South West, 2000(Environment Agency 2000).
2.2 Managing waste
Waste management is broader than just the disposal ofwaste. It includes the generation, collection, processingand transport of waste as well as the minimisation of theproduction of waste and the reconceptualising of wasteas a resource. The public health impacts are influencedby the overall waste management strategy adoptedlocally, regionally and nationally.
2.2.1 National waste strategyThe Waste Strategy 2000 (DETR 2001) sets out theGovernment's strategy for managing waste. Thestrategy has been influenced by the idea of sustainabledevelopment first described in the 1992 United NationsEarth Summit. The idea is that decision makers muststrike a balance between continued economicdevelopment and the need to protect and enhance theenvironment. Sustainable development is "developmentwhich meets the needs of the present withoutcompromising the ability of future generations to meet
7000
6000
1000
2000
3000
4000
5000
0
Form
er A
von
Cornw
all
Devon
Dorse
t
Somer
set
Wilts
hire
Glo
uces
ters
hire
Am
ount
(00
0 to
nnes
)
Agricultural
Special
Municipal
Commercial
Industrial
Figure 1 : Waste production in the South West
Source: Environment Agency 2000
6
their own needs" (Brundtland Report 1987).In terms of protecting human health, the Waste
Strategy mentions the recently adopted LandfillDirective with its stringent controls and the highstandards expected of new high temperatureincinerators.
Although not explicit in the Waste Strategy, the wastemanagement options chosen by decision makers couldhave an impact on health both directly and indirectly: 1. Directly, by leading to potential adverse and/or
beneficial health impacts such as increased risk ofcancer or decreased quality of life.
2. Indirectly, by the broader environmental impact onthe global ecology, such as the contribution to globalwarming, loss of bio-diversity and the depletion ofnon-renewable resources.
The Strategy explains the concept of the BestPracticable Environmental Option � i.e. "the option thatprovides the most benefits or the least damage to the
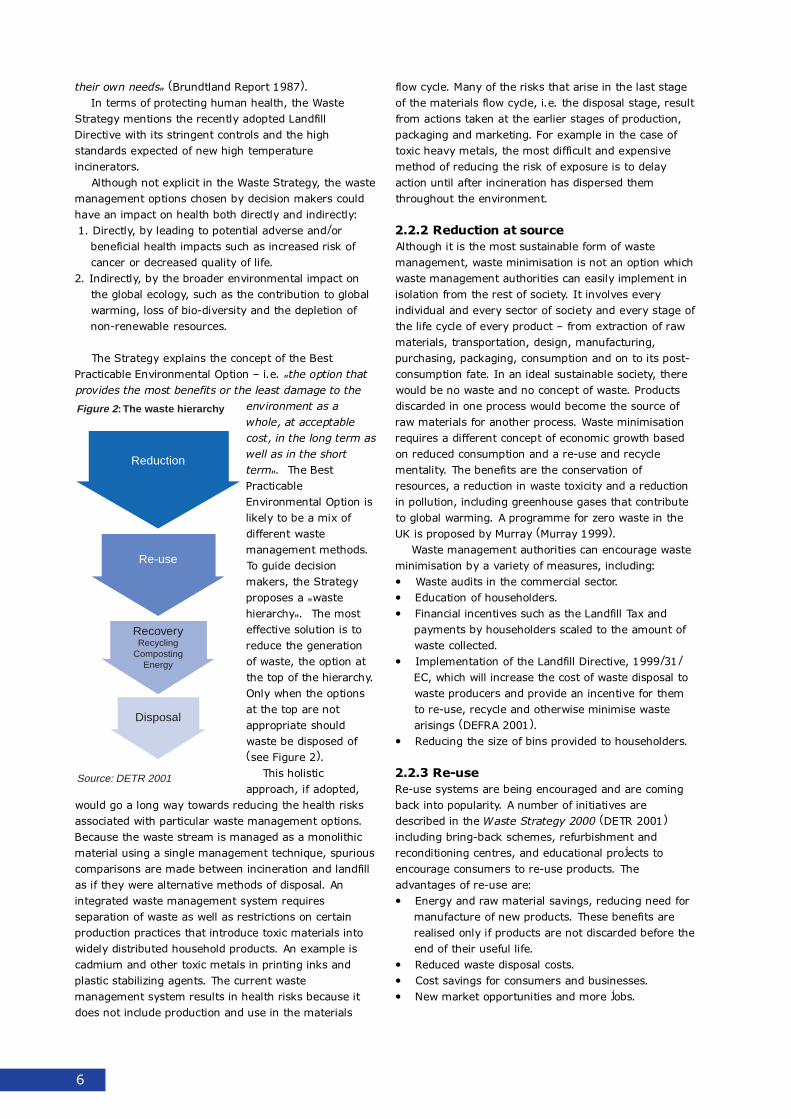
environment as awhole, at acceptablecost, in the long term aswell as in the shortterm". The BestPracticableEnvironmental Option islikely to be a mix ofdifferent wastemanagement methods.To guide decisionmakers, the Strategyproposes a "wastehierarchy". The mosteffective solution is toreduce the generationof waste, the option atthe top of the hierarchy.Only when the optionsat the top are notappropriate shouldwaste be disposed of(see Figure 2).
This holisticapproach, if adopted,
would go a long way towards reducing the health risksassociated with particular waste management options.Because the waste stream is managed as a monolithicmaterial using a single management technique, spuriouscomparisons are made between incineration and landfillas if they were alternative methods of disposal. Anintegrated waste management system requiresseparation of waste as well as restrictions on certainproduction practices that introduce toxic materials intowidely distributed household products. An example iscadmium and other toxic metals in printing inks andplastic stabilizing agents. The current wastemanagement system results in health risks because itdoes not include production and use in the materials
flow cycle. Many of the risks that arise in the last stageof the materials flow cycle, i.e. the disposal stage, resultfrom actions taken at the earlier stages of production,packaging and marketing. For example in the case oftoxic heavy metals, the most difficult and expensivemethod of reducing the risk of exposure is to delayaction until after incineration has dispersed themthroughout the environment.
2.2.2 Reduction at sourceAlthough it is the most sustainable form of wastemanagement, waste minimisation is not an option whichwaste management authorities can easily implement inisolation from the rest of society. It involves everyindividual and every sector of society and every stage ofthe life cycle of every product � from extraction of rawmaterials, transportation, design, manufacturing,purchasing, packaging, consumption and on to its post-consumption fate. In an ideal sustainable society, therewould be no waste and no concept of waste. Productsdiscarded in one process would become the source ofraw materials for another process. Waste minimisationrequires a different concept of economic growth basedon reduced consumption and a re-use and recyclementality. The benefits are the conservation ofresources, a reduction in waste toxicity and a reductionin pollution, including greenhouse gases that contributeto global warming. A programme for zero waste in theUK is proposed by Murray (Murray 1999).
Waste management authorities can encourage wasteminimisation by a variety of measures, including:� Waste audits in the commercial sector.� Education of householders.� Financial incentives such as the Landfill Tax and
payments by householders scaled to the amount ofwaste collected.
� Implementation of the Landfill Directive, 1999/31/EC, which will increase the cost of waste disposal towaste producers and provide an incentive for themto re-use, recycle and otherwise minimise wastearisings (DEFRA 2001).
� Reducing the size of bins provided to householders.
2.2.3 Re-useRe-use systems are being encouraged and are comingback into popularity. A number of initiatives aredescribed in the Waste Strategy 2000 (DETR 2001)including bring-back schemes, refurbishment andreconditioning centres, and educational projects toencourage consumers to re-use products. Theadvantages of re-use are:� Energy and raw material savings, reducing need for
manufacture of new products. These benefits arerealised only if products are not discarded before theend of their useful life.
� Reduced waste disposal costs.� Cost savings for consumers and businesses.� New market opportunities and more jobs.
Reduction
Re-use
RecoveryRecycling
CompostingEnergy
Disposal
Figure 2 : The waste hierarchy
Source: DETR 2001
7
Sewage treatment can be categorised as a systemfor the re-use of water. It is described in section 2.2.5as a waste processing system.
2.2.4 Recovery
RecyclingRecycling is the recovery of materials from productsafter they have been used by consumers. The benefitsof recycling are:� Conservation of resources.� Energy savings.� Supply of raw materials to industry.� Reduction in emissions to air and water in the
production process.� Job creation.� Development of greener technologies.� Reduction in the need for new landfills and
incinerators as there is less waste to dispose.
The disadvantages are:� Emissions from transport of material to be recycled.� In some cases, more energy may be used for
processing than for original manufacture.� Dust, bio-aerosols, odours and vermin at processing
sites.
CompostingComposting is a process for the recovery of valuablematerial from biodegradable organic matter in the wastestream. It is an aerobic, biological process ofdegradation that produces material that can be used asa soil-amendment. Centralised composting is a largescale composting process whereby organic wastes fromlocal authority parks and civic amenity sites are broughtto one centralised location. Composting is also done athome and in allotments. The advantages of compostingare:� Reduction in the volume of waste disposed of to
landfill. Organic biodegradable matter makes up to60% of municipal solid waste which can be removedby composting.
� Recovery of useful organic matter for use asfertiliser in gardening, agriculture and landscape.
� Reduction in amount of landfill gas and leachateproduced and the need for new landfill sites.
The disadvantages of composting are:� Emissions from transport.� Dust, spores, odours and possibly vermin.
Soil amendmentsValuable material from sewage can be recovered for useas a soil amendment on agricultural land, either bylandspreading sewage sludge or by irrigating the landwith wastewater. Sewage sludge consists of the solidsthat have settled out during primary and secondarysewage treatment (see Sewage treatment below). Theraw sludge is further treated to reduce its water contentand the concentration of pathogenic micro-organisms. In
the past, raw sewage wastewater was applied to landand the sludge dumped at sea but this has now beenbanned in the UK. The Landfill Directive restricts theamount of sewage sludge that can be dumped in landfilland most sewage sludge is sent to agricultural land(Environment Agency 2000).
Energy recoveryEnergy can be recovered from:� Incineration of waste � old style incinerators do not
recover energy but modern incinerators are designedas waste-to-energy plants. Mixed waste incineratorscapture only 20% of the energy generated (Murray1999 p26).
� Refuse derived fuel � waste is used as a fuelsubstitute.
� Collection of methane-rich gas from landfill sites.� Anaerobic digestion of organic wastes with energy
released as a by-product of the process.
New and emerging energy recovery technologies arelisted in the Waste Strategy 2000 (DETR 2001 Chapter5).
2.2.5 Waste processing
Sewage treatmentSewage is the waste which is discharged through thedrains and processed at sewage treatment works.Sewage consists of foul domestic and industrialwastewater as well as storm water. Raw sewage is99.9% water with 0.1% suspended and dissolved solids.The treatment process results in a liquid effluent and asemi-solid sludge. There are two objectives of sewagetreatment:1. To produce an effluent which is suitable for abstrac-
tion for treatment to produce a supply of drinkingwater.
2. To make the sludge easier and cheaper to dispose ofwhile minimising adverse effects on the environment.
During sewage treatment, pathogenic micro-organisms may be destroyed or concentrated in thesludge. Toxic and offensive materials may beconcentrated in the sludge or biodegraded. The treatedeffluent is discharged to rivers or the sea while thesewage sludge is disposed of in landfill, used as a soilamendment on agricultural or horticultural land, dumpedat sea or incinerated. Dumping at sea is no longerpermitted in the UK.
IncinerationIncineration is a waste processing option which convertswaste to energy and reduces the volume of waste goingto disposal. It is an interim waste processing functionand not the final stage of waste management.Incineration produces combustion products which arereleased into the atmosphere as gases and ash which isdisposed to landfill or used in construction. Modern
8
incinerators are designed to produce nearly completecombustion and to release negligible amounts of airpollutants from the stacks. However, pollutants are notdestroyed by the process of incineration. Instead, theyare released from the incinerator as solid residues ratherthan as gases. There is a direct link between airemissions and the nature and amounts of solid residueproduced � as more effective pollution control devicesare fitted to incinerator stacks, the concentration andleachability of toxic metals in the fly ash increase. Mostof the studies of health effects are of old incineratorswith less efficient pollution control technologies, buteven incinerators operating to current emissionstandards may have off-normal emission incidents. Theprocess of incineration does not eliminate health hazardsfrom waste. It transfers the risks to another wastemanagement method, usually landfill.
The benefits of incineration are:� Reduces weight and volume of waste � about 30%
of weight is left as ash (Farmer & Hjerp 2001).� Reduces potential infectivity of clinical waste.� Can use bottom ash for materials recovery.� Produces energy which can be recovered partially for
electricity generation.
The disadvantages of incineration are:� Produces hazardous waste that must be disposed of.� Enhances mobility and bio-availability of toxic metals
present in waste (Denison & Silbergeld, 1988).� Discharges contaminated wastewater.� Emits toxic air pollutants.� Produces carbon dioxide, a greenhouse gas.� Causes emissions from transport of waste to and
from incinerator.� Does not alter the process of waste collection and
transfer.
2.2.6 Waste disposal
Discharge to rivers and seaThe liquid effluent from sewage treatment works isdisposed of by discharge into rivers and the sea. Waterquality is inevitably affected by the level of sewagetreatment. In the South West, water companies areinvesting in sewage treatment improvementprogrammes to ensure compliance with the minimumstandard of sewage treatment stipulated by EUlegislation. However, some of the improvement schemesare behind schedule (Environment Agency 2001). Thereis concern in the South West about the quality ofbathing waters, river water, and shellfish waters as aresult of sewage discharges. The hazards of concern arethe faecal pathogens which could pose a health risk to
recreational users of surface waters, to consumers ofshellfish and to drinking water supplies.
LandfillLandfill is the dumping of waste on the land. The termlandfill includes a wide spectrum of sites ranging frommanaged, engineered, regulated sites to illegal,uncontrolled dumps.
Currently, in a typical UK municipal landfill, waste isdeposited in a pre-constructed cell in an engineered site.The base is impermeable clay or is lined with a plastic,rubber or composite layer covered by earth. At the endof each day, the waste is covered with an inert materialsuch as soil. When the cell is full, it is covered over witha layer of inert material. During operation, a fence isbuilt around the site to prevent the wind from blowingmaterial off site. A drainage system is built to collectwater runoff and leachate. An energy recovery system isconstructed to collect gas which can either be used togenerate electricity or is flared (Tubb & Iwugo 2000b).
The Landfill Directive (99/31/EEC) regulates theoperation of landfill sites in the UK. To protect humanhealth, the Directive bans the disposal of all liquids,infectious clinical wastes, and tyres to landfill. It requirestreatment prior to landfilling except for inert wastes andrequires aftercare of closed landfills. In sites receivingbiodegradable waste, landfill gas must be used or flared.Co-disposal of hazardous waste with municipal waste isno longer allowed.
The benefits of landfill are:� It has been a cheap way to dispose of waste by
dumping it in disused quarries and abandonedindustrial sites.
� Waste is used to backfill quarry before reclamation.� Landfill gas contributes to renewable energy supply.
In the South West, about two thirds of the region'srenewable energy supply is from landfill gas(Environment Agency South West 2001).
The disadvantages of landfill are:� Water pollution from leachate and runoff.� Air pollution from the anaerobic decomposition of
organic matter producing methane, carbon dioxide,nitrogen, gases, sulphur, and volatile organiccompounds.
� It is not a sustainable option. The South West hasless than seven years of licensed landfill capacity forbiodegradable waste (Environment Agency SouthWest 2001).
A summary of the potential advantages anddisadvantages of different elements of the wastehierarchy is shown below in Table 3.

9
:3elbaT segatnavdasiddnasegatgnavda:lasopsidetsawrofseigetartS
ygetartsetsaW segatnavdA segatnavdasiD
etsaWnoitasiminim
.secruoserfonoitavresnoC
.noitullopdnayticixotetsawninoitcudeR
.sesagesuohneergninoitcudeR
lacigolohcyspdnalaicos,cimonocerojamseriuqeR.slaudividniybdnayteicosnisegnahc
decudorpetsawhtiwlaedotdedeennoitcaetaidemmI.won
esu-eR rofdeengnicuder,sgnivaslairetamwardnaygrenEerastifenebesehT.stcudorpwenfoerutcafunam
ehterofebdedracsidtonerastcudorpfiylnodesilaer.efillufesuriehtfodne
.stsoclasopsidetsawdecudeR
.sessenisubdnasremusnocrofsgnivastsoC
.sbojeromdnaseitinutroppotekramweN
gnilyceR .secruoserfonoitavresnoC
.sgnivasygrenE
.yrtsudniotslairetamwarfoylppuS
ehtniretawdnariaotsnoissimeninoitcudeR.ssecorpnoitcudorp
.noitaercboJ
.seigolonhcetreneergfotnempoleveD
dnasllifdnalwenrofdeenehtninoitcudeR.esopsidotetsawsselsierehtsasrotarenicni
.delcycerebotlairetamfotropsnartmorfsnoissimE
rofdesuygreneeromebyamereht,sesacemosnI.erutcafunamlanigirorofnahtgnissecorp
gnissecorptanimrevdnasruodo,slosorea-oib,tsuD.setis
gnitsopmoC otfodesopsidetsawfoemulovehtninoitcudeRebnacetsawdiloslapicinumfo%06otpU.llifdnal
devomerebnachcihwrettamelbadargedoibcinagro.gnitsopmocyb
liossaesurofrettamcinagrolufesufoyrevoceR.erutlucirgadnaepacsdnal,gninedragnitnemdnema
etahcaeldnasagllifdnalfotnuomaninoitcudeR.setisllifdnalwenrofdeenehtnidnadecudorp
gnitsopmocgnisilartnectaseitilibissoptnemyolpmE.seitilicaf
.gnitsopmocemohmorferusaelpdnanoitcafsitaS
ecruoserotrognimrawlabolgotetubirtnoctonseoD.noitelped
.tropsnartmorfsnoissimE
.ecnasiunnimrevylbissopdnaesion,sruodO
lagnufroairetcabgniniatnoctsudcinagro-slosorea-oiB.serops
.sdnuopmoccinagroelitalovstimE
cixotyllaitnetopfopu-dliubmretgnolelbissoPseodhcihwtsopmochtiwdednemasliosnisecnatsbus
.stnemeriuqerdnasenilediugytilauqtcirtsteemton
.sdrazahlanoitapuccO
gnidaerpsdnaLegdulsegawes
niresilitrefsaesurofstneirtunfoyrevoceR.erutlucitrohdnaerutlucirga
sdnuopmoccinagrohtiwegdulsfonoitanimatnoC
.slatemyvaehhtiwnoitanimatnoC
rostsycmrow,seropslaozotorphtiwnoitanimatnoC.ignufroairetcabciretne,sesurivoretne,sgge
.efilfoytilauqgnitceffaecnasiuN
.srekrowotsdrazahlanoitapuccO
tnemtaertegaweS ecnelitsepsdiova-etsawnamuhfolasopsidefaS,ylppuselbatopfosecruosstcetorp,ecnasiundnaottnemtaertrofelbatiustneulffeegawessecudorp
.ylppuselbatopecudorp
sdnuopmoccinagroniatnocyamsegrahcsidegaweS.sdnuopmocgnitpursidenircodnedna
.slatemyvaehniatnocyamsegrahcsidegaweS
-orcimcinegohtapniatnocyamsegrahcsidegaweS.smsinagro
.erusopxeediflusnegordyH
.ecnasiunrettildnaruodO
.srekrowotsdrazahlanoitapuccO
10
)deunitnoC(segatnavdasiddnasegatnavda:lasopsidetsawrofseigetartS3elbaT
ygetartsetsaW segatnavdA segatnavdasiD
noitarenicnI fo%03tuoba,etsawfoemulovdnathgiewsecudeR.hsasatfelsithgiew
.etsawlacinilcfoytivitcefnilaitnetopsecudeR
.yrevocerslairetamrofhsamottobesunaC
rofyllaitrapderevocerebnachcihwygrenesecudorPfognidliubgnirudnoitaercboJ.noitarenegyticirtcele
.rotarenicniwen
desopsidebtsumtahtetsawdilossuodrazahsecudorP.fo
slatemcixotfoytilibaliava-oibdnaytilibomsecnahnE.etsawnitneserp
.retawetsawdetanimatnocsegrahcsiD
.stnatullopriacixotstimE
morfdnaotetsawfotropsnartmorfsnoissimesesuaC.rotarenicni
dnanoitcellocetsawfossecorpehtretlatonseoD.refsnart
yvaeh)snixoid.g.e(sdnuopmoccinagrocixotstimE.slosoreacidicadnasesagcidica,setalucitrap,slatem
.ksireriF
.drazahciffartdaoR
.sdrazahlaicosohcysP
.sdrazahlanoitapuccO
.seulavytreporpniporD
otsetubirtnocdnaedixoidnobracsetarenegnoitsubmoC.gnimrawlabolg
.noitelpedecruoserotsddA
rehtardenrubscitsalp.g.e(sleuflissoffoesusesaercnI.)delcycerrodesiminimesuriehtnaht
llifdnaL ybetsawfoesopsidotyawpaehcaneebsaHdenodnabadnaseirrauqdesusidnitignipmud
.setislairtsudni
.demialcererofebyrrauqllifkcabotdesuetsaW
.ylppusygreneelbawenerotsetubirtnocsagllifdnaL
.ffonurdnaetahcaelmorfnoitullopretaW
cinagrofonoitisopmocedciboreanamorfnoitullopriA,negortin,edixoidnobrac,enahtemgnicudorprettam
.sdnuopmoccinagroelitalovdna,ruhplus
ygrenerofnoitpoelbaniatsusmretgnolatoN.noitareneg
laiborcim,slatemyvaeh,slacimehccixotstimE.snegohtap
.setisneporaennimreV
.sdrazahciffartdaoR
.sksirnoisolpxednaeriF
,ecnasiun-efilfoytilauqgnitceffasdrazahlaicosohcysP.yrrowdnaraef,sserts
.sdrazahlanoitapuccO
.seulavytreporpniporD
.desilitutonfignimrawlabolgotddasesagllifdnaL
.noitelpedecruoserotsddA
.sleuflissoffoesusesaercnillifdnalotlasopsiD
11
2.3 Waste management regulation
2.3.1 Roles and responsibilitiesThe roles and responsibilities of different authorities withrespect to risk management is shown in Table 4.
2.3.2 Strategies and Plans
Waste Local PlanThis is a guide to the land use planning aspects of wastemanagement. It is prepared by the county councils as astatutory requirement of the Town and Country PlanningAct 1990. Together with the Minerals Local Plan and theDistrict Local Plans, it makes up the county�s statutoryStructure Plan, i.e. the overall development plan for thecounty. The statutory consultation procedure is laiddown in the Town and Country Planning Act.
Waste Management StrategyThis is a non-statutory document, providing guidance for
improving waste management practice and priorities inthe county. It is the overall framework from which themore detailed Waste Local Plan is prepared. There is nostatutory consultation procedure.
Progress with Waste Strategies and Local Plans in theSouth West are presented in Appendix 3.
2.4 Waste management in the SouthWest
Most waste (approximately 85%) is dumped in landfill.Of the 6 million tonnes sent to landfill, approximately3.5 million was biodegradable and over 2 million tonneswas inert or construction and demolition waste.Recycling rates vary across the region (EnvironmentAgency 2000, data for 1998/99) and are shown inFigure 3.
A summary of waste management facilities in theSouth West is shown in Figure 4.
4elbaT : tnemeganametsawnidevlovniseitirohtuatnereffidfoseitilibisnopserdnaseloR
noitcnuF ydobelbisnopseR ydobyrosivdA
yciloP
ygetartSetsaWlanoitaN lacoL,tropsnarTroftnemtrapeD-dnalgnEsnoigeRehtdnatnemnrevoG
ycnegAtnemnorivnE
dehsilbupebot,selaWrofylbmessAlanoitaN-selaWygetartSetsaWecalperlliwtinehw2002gnirpSni
selaWdnadnalgnE0002
noitatlusnoccilbuP
ygetartSetsaWlanoigeR ylbmessAlanoigeR noitatlusnoccilbuP
nalPerutcurtSytnuoCrofyciloPetsaWcigetartS ytirohtuAgninnalPetsaWsalicnuoCytnuoC noitatlusnoccilbuP
ytnuoCrofnalPlacoLetsaW ytirohtuAgninnalPetsaWsalicnuoCytnuoC noitatlusnoccilbuP
ygetartSetsaWlapicinuM ytirohtuAlasopsiDetsaWsalicnuoCytnuoC noitatlusnoccilbuP
snalpgnilcyceR seitirohtuAnoitcelloCetsaWsalicnuoCtcirtsiD noitatlusnoccilbuP
tnemeganaM
otnoitcudorpmorfetsawfotnemeganamsetalugeR)noitalugerCPPI(,metsysgnisnecilahguorhtlasopsid
sessecorpnoitullop)1(Aeludehcsregralfo
ytirohtuAnoitalugeRetsaWsaycnegAtnemnorivnE
srevirgnivorpmidnagnitcetorprofytilibisnopsersaHretawdnuorgdna
ytirohtuAnoitalugeRetsaWsaycnegAtnemnorivnE
senimreted-lortnoCtnempoleveDtuoseirraCgninnalpsecrofnednasrotinom,snoitacilppagninnalp
slortnoc
ytirohtuAgninnalPetsaWsalicnuoCytnuoC ycnegAtnemnorivnEseitirohtuAhtlaeHdna
seetlusnocyrotutats-
etsawfotnemeganamehtrofstcartnocseldnaHseitirohtuAnoitcelloCetsaWybdetcelloc
ytirohtuAgninnalPetsaWsalicnuoCytnuoC
dlohesuohyklubfotnemeganamrofseitilicafsedivorPgnilcycerdnaetsaw
ytirohtuAgninnalPetsaWsalicnuoCytnuoC
setisroftnemeganam'etiSdesolC'sekatrednUlicnuoCytnuoCehtybdetarepoylsuoiverp
ytirohtuAlasopsiDetsaWsalicnuoCytnuoC
etsawottropsnartdnaetsawdlohesuohtcelloCseitilicaftnemeganam
seitirohtuAnoitcelloCetsaWsalicnuoCtcirtsiD
seitilicafgnilcycernuR seitirohtuAnoitcelloCetsaWsalicnuoCtcirtsiD
etsawlaicremmocdnassenisubtcelloC seitirohtuAnoitcelloCetsaWsalicnuoCtcirtsiD
noitamrofnI
sgnisiraetsawnoatadsedivorP ytirohtuAnoitalugeRetsaWsaycnegAtnemnorivnE
2p,1002nalPlacoLetsaWlicnuoCytnuoCerihsretsecuolG:ecruoS
12
48%
39%
13%
93
75
26
66
282
Treatment facilities, including composting sites
Landfills accepting only inert waste
Landfills accepting household, industrial and commercial waste
Landfills accepting special waste
Total landfill sites100%
Transfer stations, including civic amenity sites
Total landfill sites = 194
Figure 4 : Waste management facilities in the South West in 1998-99
Source: Environment Agency 2000
TOTAL = 542
Below average (<7%)
Below average (7 to 13.9%)
Above average, below target (14 to 24.9%)
Above 2005 target (25 to 29.9%)
Above 2010 target (30 to 32.9%)
Above 2015 target (33%+)
No data
Isles of Scilly
miles
0 3015
Produced by South West Public Health Observatory. 4 January 2002 Adapted from Environment Agency© Crown Copyright. All rights reserved. Licence number HA 10003534
Figure 3 : Recycling rates by local authority 1998.South West

13
How might waste management practices impact onhuman health?
3.1 Definition of health
An often-quoted definition of health is one provided bythe World Health Organisation � health is a 'state ofcomplete physical, mental and social well-being and notmerely the absence of disease and infirmity'. BetterHealth, Better Wales (Welsh Office 1998) added to thisby saying that sustainable health is achieved 'whenpeople and communities can take control of their livesand are able to live their lives to the full.'
3.2 Case studies
Two case studies illustrate the issues involved in findingevidence of the effects of waste management operationson health. The background to each case is presented inthis section and the relevant findings in the sectionswhich follow.
3.2.1 Nant-y-Gwyddon, WalesIn 1988, the Nant-y-Gwyddon landfill site was opened todispose of household, commercial and industrial waste.In the same area, there were up to seven otheroperating and closed landfill sites (Roberts et al 2000).There had also been a municipal waste incineratorlocated in a steep north westerly valley running throughthe area. The incinerator operated between 1974 and1987 and had been closed because of local complaints,poor performance and air pollution (Roberts et al 2000).In 1996, residents complained about the odoursemanating from the Nant-y-Gwyddon landfill site. Theyformed an action group called RANT � Residents AgainstNant-y-Gwyddon tip and asked the health authority toinvestigate the effects on their health. The healthauthority met with the residents and identified a list ofhealth concerns (Fielder et al 2000). These weremortality, hospital admissions, and various reproductivehealth outcomes. No exposure data were available andthere was no community monitoring during the peak ofthe problem. The exposed population was defined asresidents living in the five electoral wards within 3 km ofthe site, a population of 20,000 people. The comparisongroup was the population living in 22 other electoralwards in the same local authority, matched fordeprivation by the Townsend score.
The odour was identified as hydrogen sulfide butmonitoring of the site in 1997 revealed higher thannormal levels of potentially toxic chemicals such asstyrene, dimethyl styrene, ethyl benzene and C4 alkylbenzenes. Hydrogen sulfide is not known to cause
congenital abnormalities but is likely to causeheadaches, eye irritation and sore throats.
3.2.2 Love Canal, United StatesA canal in Niagara Falls, New York state, was used as alandfill site by the Hooker Chemical Company. Between1942 and 1953, the company disposed of 19,000 tonnesof organic chemical wastes which were produced duringthe manufacture of pesticides. In 1953 when the canalwas full, it was covered with a clay cap and sold to theNiagara Board of Education for $1.00. A school andplayground were built on the canal and housing builtadjacent to it. The integrity of the clay cap wasbreached in the process with the result that rain seepedin and eventually caused the chemicals to overflow thecanal. The residents and city officials were aware of"black sludges bleeding through basement walls, smellslike a chemical factory, rancid liquids of yellow andorchid and blue" oozing out of yards, etc (Brown 1980).However, there was no concern about the health effectsof such exposure until the late 1970s. In 1978, the NewYork State Department of Health evacuated the 235families in the ring of homes closest to the canal. Twoyears later, the federal government evacuated 800 morefamilies in the next ring of homes. The public alarm overthe incident was instrumental in bringing aboutSuperfund legislation.
At Love Canal, records from Hooker ChemicalCompany revealed that the waste consisted of lindaneand other chlorinated hydrocarbon by-products.Investigations of the canal led to the identification of248 chemicals by 1980. These included lindane,benzene, toluene, chloroform, trichloroethylene,tetrachlorethylene, hexane, xylenes, trichlorophenol,hexachlorcyclopentadiene and dioxin isomers (Paigen etal 1987). Toxicology data were available on fewer thanhalf of these chemicals and much of the available datawere incomplete. For those contaminants wheretoxicological data were available, the implications forhuman health were not reassuring. Benzene was one ofthe volatile organic chemicals identified in the canal.From toxicological and occupational studies, benzene isknown to cause leukaemia, aplastic anaemia, bonemarrow depression, central nervous system depressionand skin irritation. It is suspected of embryotoxicity,teratogenesis and of leading to female infertility andlymphoma (Buffler et al 1985).
3.3 Quantifying factors which mayaffect health
The definitions of health in 3.1 provide a foundation foridentifying factors associated with waste managementwhich might have an impact on health. These may be
3 Impact on human health

14
beneficial, damaging or neutral. They may be present inwaste or formed during the waste management process.Table 5 illustrates the factors which may impact onhealth and have been studied in relation to methods ofwaste management.
The references listed in Table 5 are examples of
studies found in the literature which have investigatedan association between the factor mentioned and thewaste management method. This table is not acomprehensive listing of all the studies found in theliterature nor is it evidence of a causal association.
5elbaT : sdohtemtnemeganametsawhtiwdetaicossasdrazahhtlaeH
rotcaF llifdnaL noitarenicnI gnitsopmoC egdulsegaweS tnemtaertegaweS
sdrazahlacisyhP
cinagrOlacimehc
:eradnuofsenoniamehT
snobracordyhcitamoracilcycyloP.)5991latehtrowkliS(
,enecarhtna)a(ozneb,enezneB,enesyrhc,eneryp)a(oznebdetanirolhcylop,rolhcatpeh
,enelyhteorolhcartet,slynehpib,enahteorolhcirtlynehpidorolhcid
latelayaD(enelyhteorolhcirt.)5991
sdnuopmoccinagroelitaloV.)4991lateuorimZ(
dnasedicitsepenirolhconagrOtdnrA(sdnuopmoccinagroelitalov
.)9991latesrewE(snarufdnasnixoidF/DDCP
.)4991late.)8891lateneerG-rhetS(sBCP
dnadetarutasdetanirolhc,senaklAtneruaL(snobracordyhdetarutasnu
.)3991late
,snarufdnasnixoiDdetanirolhc,sBCP
,senezneb,slonehpdetanegolah
detanirolhcylop,senehpoihtoznebid
cinagroelitalov,sHAPpposllA(sdnuopmoclanoitaN,1002late
licnuoChcraeseR.)3991ytraM,0002
cinagroelitaloVsdnuopmoc
tnemnorivnE(.)1002ycnegA
citamoracilcycyloP,snobracordyh
,sedicitsepdetanegolah
citahpila,sBCP,sdnuopmoc
,seneznebrolhccinagroelitalov
,sdnuopmoc,snixoid,slonehpsetalathp,snaruf
adanaChtlaeH(-ituecamrahP.)0002
slacimehclac.)6991sregoR(
ssenloH&ttocrehteN(BCP,sdnuopmocosortiN-N.)8891
cixotoneg,senimacitamoranessumsaR&etihW(,sHAPnorutorposiedicibreH.)8991
relssuhcS&,ekhcstiN(gnitpursidenircodnE.)8991
,snixoid,sBCP-sdnuopmoc,TDDsahcussedicitsep
,enadrolhc,HCH,rolhcyxohtemhcussedicibreh,nirdleid,xerim
,enizamis,enizartasa,nilozolcnivsahcussedicignuf
sahcussenomrohcitehtnyslarutan,llipevitpecartnoc
niloidartseosahcussenomrohlonehplykla,eniru
setalahthp,setalyxohteylop.)5991HEI(PHEDsahcus
slatemyvaeH ,6991lateneedeW(muimorhC.)0002latenorraCcM
,muimorhc,muimdac,cinesrAlateinolacceB(daeldnayrucrem
)0002.)3991latefieR(yrucreM
,dael,yrucreM,cinesra,muimdac
lanoitaN(muimorhclicnuoChcraeseRlatepposllA,0002,3991ytraM,1002
dlegrebliS&nosineD.)8891
latemyvaeHninoitalumucca
fosporcdnaslioshtiwdetaertdnal
tereztiE(tsopmocsetropeD,7991la
.)5991late
,esenagnaM,muimdac,reppoc
,dael,yrucrem,lekcin,muimorhc
htlaeH(cniz)0002adanaC
maglamalatned-yrucreMlateewoR,7991latenaF(
)6991
tsuD .)8891lategnilretS(tsuddaeLetisetsawsuodrazahmorftsuD
.)1991lateartueN(
rettametalucitraPhcraeseRlanoitaN(
.)0002licnuoC
tsuDtnemnorivnE(
.)1002ycnegA
laiborciMsnegohtap
zitrO(CepytmunilutobmuidirtsolC.)4991htimS&
ebotylekilnUhtiwdetaicossa
.noitarenicni
.e.islosoreaoiB,tsudcinagro
gniniatnocsahcusairetcab
muidirtsolCmunilutob dna
-cudorp-nixotodnemarGgni
airetcabevitagenlagnufro/dna
sahcusseropssulligrepsA
sutagimuf ,lateregnuB(
,0002tnemnorivnE
,1002ycnegAebuL&lenhoB
.)0002
-aozotorP,eabeoma
,iidnogamsalpoxoT,ailbmalaidraiGmuidiropsotpyrC
rostsyc-shtnimleHsiracsAfosgge
,ppssiruhcirT,pps-sesuriVppsaineaT
hcussesurivoretne,AsititapeHsa
,sesurivoneda,sesurivator
,sesurivanorocciretne-airetcaBsahcusairetcaboslA,allenomlaS
,succocotpertS,muidirtsolC
,muiretcabocyM-ignuF,airetsiL
sulligrepsAadidnaC,sutagimuf
,snaciblasuccocotpryC
htlaeH(snamrofoen,0002adanaC
)3991latebuartS
egawesmorfstifenebhtlaeHfolasopsidefas-tnemtaert
sdiova,etsawnamuh,ecnasiundnaecnelitsep
elbatopfosecruosstcetorpegawessecudorp,ylppus
tnemtaertrofelbatiustneulffeylppuselbatopecudorpot
egaweSnonoissimmoClayoR(htlaeH.)5191-8981lasopsiD
egawesmorfsdrazahcinegohtaP-tnemtaert
tetetnomuD(smsinagroorcimydenneK&snilloC,1002la
ciretnE:airetcaB.)2991iccocotpertslaceaf/airetcab
)8991ssurP,9991naklA(latedaarneoK(retcabolypmaC
tnatsisercitoibitnA.)7991egaweslatipsohniairetcab
:sesuriV.)9891anilloC&araF(lateuoditinavrA(BsititapeHsolcneseD(Asititapeh.)8991
surivklawroN.)1991late.)0891latennamhorG(
.)6991lateabreG(surivatoR
nimreV woltubesaesidgnidaerpsfoksiRhtlaeH(ecnerruccofoytilibaborp
.)0002adanaCtuobastnialpmoclaitnediseR
llifdnalraensdribdnaseilf,stnedor.)0002latenraefdeR(snoitarepo
ebotylekilnUhtiwdetaicossa
.noitarenicni
.ytilibissoP nimrev,stcesnIadanaChtlaeH(
)0002
15
)deunitnoc(sdohtemtnemeganametsawhtiwdetaicossasdrazahhtlaeH:5elbaT
rotcaF llifdnaL noitarenicnI gnitsopmoC egdulsegaweS egaweStnemtaert
)d'tnoc(sdrazahlacisyhP
sedilcunoidaR )1002,lateocsoB(muidaR erehwynadenoitnemtoN ebotylekilnUhtiwdetaicossa
gnitsopmoc
etsawlacinilC
sdnuopmoccinagronI lateredleiF(ediflusnegordyH)0002
dnalCH,2OS-sesagcidicAhtiwslosoreacidicA.3ONHhcraeseRlanoitaN(4OS2H
)0002licnuoC
ebotylekilnUhtiwdetaicossa
gnitsopmoc
,setirtin,setartiNainomma,negortin
,muissatop,muiclac
muisengamadanaChtlaeH(
)0002
negordyHedihplus
lateredienhcS()8991
ciffartdaoR sksirnoitatropsnarTliosgnivomerhtiwdetaicossa
fonoitaidemergnirudteraM(etisetsawsuodrazah
laitnediseR)3991lallifdnaltuobastnialpmoc
latenraefdeR(snoitarepo)0002
ytilibissoP ytilibissoP
noisolpxednaeriF ,eocsoLninoisolpxE1991AMB(erihsybreD
-7691ASUnisesac13.)611p.)0002adanaChtlaeH(7891
rotarenicnieednuDtaeriF)0002SDNE(
ebotylekilnUhtiwdetaicossa
gnitsopmoc
srotcaflaicosohcysP
efilfoytilauQ raeyllasllemsdab-secnasiuNstnedisergnitneverp,dnuor
gniogroswodniwgninepomorfnihsibburnwolbdniw,sklawrof
niseilffosderdnuh,snedragdnasllugaesfoskcolf,sesuoh
gnihsawnognitacefedsworc.)1002nosniboR(edistuotfeltuobastnialpmoclaitnediseR
,dum,sruoh,esion,rettil,ruodollifdnalraenciffart,tsud
latenraefdeR(snoitarepo.)0002
enihcamdnaciffartmorfesioNotdaelyam-noitarepo
stratskrowfipeelsdebrutsid.gninromylrae
fonoitpecreptnediseRytilauqdoohruobhgien)5991lategrebneerG(,noisehocfonoitpursiD,egnahcdoohruobhgien
niesaercedroesaercniytinummocfokcal,noitalupop
hcraeseRlanoitaN(lortnoc.)0002licnuoC
ruododnaesioNtnemnorivnE(ecnasiun
.)1002ycnegA
htlaeH(ecnasiuN)0002adanaC
ruodOnamretsuhS(
norettiL.)2991morfsehcaebKU
egawessegrahcsid
lateppilihP(.)7991
srotcaflacigolohcysP ybyrrow,sserts,snrecnoCsuodrazahraengnivilstnediser
latehturraC(setisetsaw,5991latenametihW,7991
namretsuhS,2991lateregnU,1991lateartueN,1991late
.)9891oknafetS&ztiworoH
fotsurtsid,snrecnoccilbuPcifitneicsdnatnemnrevog
,sserts,yteixna,snoitutitsnissensselrewopfosgnileefniesaercni,noitaneiladna
laicosdnameetseflesoteudnoitcennoc
ytinummocnitnemevlovnilanoitaN(etistsniagamsivitca
,0002licnuoChcraeseR.)1002ACSN
htiwhtlaehottifeneB-gnitsopmocemoh
.nuf,noitcafsitas
srotcaflanoitapuccO
ytefasdnahtlaeHsnoituacerp
svsrekrowllifdnalkroYweNnoitatinaskroYweNrehto.)7991grebleG(srekrow
nistceffehtlaehesrevdAlaterednellaC(srekrow
.)5991lateykztibrW,7991
esrevdaelbissoPfohtlaehnostceffe
tnemnorivnE(srekrow.)1002ycnegA
dnalagnuFseropslairetcab
rianisesurivdnaotksiresopohwsrekrow
roegdulsylppadetaertnokrow
htlaeH(etis)0002adanaC
gnomahtlaeHegaweslapicinum
retawdnasrekrowtnemtaertteznarK-ttelracS(
)7891la
16
)deunitnoc(sdohtemtnemeganametsawhtiwdetaicossasdrazahhtlaeH:5elbaT
rotcaF llifdnaL noitarenicnI gnitsopmoC egdulsegaweS egaweStnemtaert
srotcafcimonocE
tnemyolpmE ynamtontubdetaercsboJfosepytrehtohtiwderapmoc
.snoitarepolasopsidetsaw
niesaercedroesaercnIrotnemyolpmellarevo
niegnahcdnatnemyolpmenunoitubirtsidlanoitapucco
licnuoChcraeseRlanoitaN(ybdetaercsbojtsoM.)0002
detaicossaeranoitarenicnirotarenicniehtgnidliubhtiw
.)1002niknaH&idranoeL(
tatnemyolpmEgnitsopmocdesilartnec
.setis
otstifenebcimonocErotceslarutlucirga
.enoN .enoN otdesutsopmoC,erutcurtsliosevorpmitca,erutsiomliosliater
ottifeneb-resilitrefsatsopmoC.erutlucirga
htiwdetanimatnoc-slatemyvaeh
porcotegatnavdasid.noitcudorp
ecruoS-tifeneBresilitreffo
-egatnavdasiDfoecruoS
stnanimatnoc
seulavytreporP ecirpdnanoitaulaveDadanaChtlaeH(gnidargnwod
.)981p,2loV,0002
dnalniesaercedroesaercnInoitaxatniegnahc,seulav
dnalniegnahcmorfgnitluserniegnahcemocnidnaesu
dnagnisuohfosepytlanoitaN(ycnapucco
.)0002licnuoChcraeseR
.ytilibissoP
srotcaflatnemnorivnE
gnimrawlabolG labolgotddasesagllifdnaL.desilitutonfignimrawdluowsagfonoitasilitU
fosennot000,053ecalpsidmorfraeyhcae2OC
yticirtcelelanoitnevnocneewtebgnivas,noitareneglabolgnim7.01£dnam7.2£
otgnidrocca,stcapmignimraw.)06p1002ARFED(ARFED
.gnimrawlabolgotsddAnobracsetarenegnoitsubmoC
.sagesuohneerga,edixoid
labolgotddatonseoDderapmoc,gnimraw
.noitarenicnihtiw
ecruoseRnoitavresnoc
-noitelpedecruoserotsddAsesaercnillifdnalotlasopsid
scitsalp-sleuflissoffoesunahtrehtarllifdnalnidepmud
.delcycerrodesiminim
.noitelpedecruoserotsddAfoesusesaercninoitarenicnI
denrubscitsalp-sleuflissofesuriehtnahtrehtar
.delcycerrodesiminim
otddatonseoD.noitelpedecruoser

17
3.3.1 Quantifying factors which may impacton healthHealth hazards can be measured or estimated withvarying degrees of accuracy. The number of jobs lost orcreated by a waste management policy can be counted.Community involvement can be measured by assessingthe extent of activity in community recycling schemes.Physical hazards can be identified by measuringconcentrations in:� Waste � i.e. in emissions, incinerator ash, sewage
sludge, etc.� The environment around the waste management site
� i.e. in the soil, air, plants, animals, water,groundwater.
� People � i.e. the body burden.
With improvements in analytical methods,contaminants can be identified at very lowconcentrations, so small that their implications forhuman health is a matter for conjecture.
Identifying and measuring hazards gives animpression of accuracy and can lead to the assumptionthat the measurable risks from physical hazards aremore substantial and important than those frompsychosocial hazards. In fact, data about physicalhazards are also incomplete. Information is lackingabout the toxicity, persistence and ability tobioaccumulate of many of the hundreds of thousands ofchemicals that end up in waste. Out of some 100,000chemicals notified before 1981, the so-called ExistingChemicals, most have not been assessed. Of some2,000 chemicals notified since 1981, the so-called NewChemicals, many assessments are not complete(Santillo, 1999).
3.3.2 Measuring toxicityMost information on toxicity is derived from animalexperiments. Toxicity is usually defined in terms ofLD50, the dose in mg/kg body weight required to killhalf of the animals tested. This value is specific to thespecies tested as well as to the conditions under which itwas tested. It is hard to know what order of magnitudeto use to extrapolate from animals to humans as thereare vast differences between species. Extrapolation tohumans is usually based on the most sensitive animalsspecies tested.
Chronic toxicity is more relevant than acute toxicityto the type of exposure from hazardous waste sites butis even harder to determine for humans. Someknowledge is derived from occupational exposure butmost is extrapolations from short term high doses inanimals to long term low doses in humans. This can leadto under or over estimations of toxicity. Some chemicalssuch as cyanide may be hazardous at high doses butharmless at low doses while others, such as PCBs, donot cause acute toxicity at high doses but arecarcinogenic or teratogenic at chronic low doses.
The toxicity of heavy metals is well known fromclinical and epidemiological studies and is not dependenton extrapolations from animal studies (Denison and
Silbergeld 1988). Heavy metals, i.e. lead, mercury,cadmium, accumulate both in the environment andwithin the human body. Long term low level releasesfrom waste management operations have the potentialto lead to substantial levels in the environment and thebody. Given that there are other environmental sourcesof metals and that every person carries measurablelevels in their bodies, a small increase in exposure fromincineration could theoretically raise levels in peopleenough to cause overt toxicity. In some populations,existing levels of exposure and body burdens arealready in a range associated with detectable adverseimpacts. Exposure to persistent chemicals cannot beconsidered in isolation from other sources.
3.3.3 Combination of chemicalsIn most waste, a mixture of different contaminants willbe present. Little is known about the toxicity ofcombinations of contaminants, or whether theirinteraction is to increase toxicity or to modify it.Assessment of the potential health hazard of mixtures isa challenging task for toxicology. The risks may beadditive or there may be interaction effects that makethe risks higher or lower than that predicted byanalysing individual contaminants separately. There maybe no interaction at all, with each compound actingindependently. Nor is there an adequate understandingof the effects on toxicity of the changes which occurwhen chemicals migrate through soil or water. Unlikelaboratory conditions where animals are exposed to onechemical at known doses, people's exposure to wastesites is typically complex with many agents and multiplepathways (Hansen et al 1998, Carpenter et al 1998).
3.3.4 Comparing hazards from differentwaste management optionsBoth incinerators and landfill sites result in the emissionof toxic pollutants, including dioxins. While most peopleassume that the greatest risk to health from airbornepollutants arises from incinerators, a generic comparisonusing modelling techniques came to the oppositeconclusion (Bridges et al 2000). The comparison wasbased on worst case off-site exposures and concludedthat landfills without gas collection pose a potentiallyhigher risk than municipal solid waste incineratorsperforming to UK standards. It must also be understoodthat incineration and landfill disposal are inextricablylinked. Improvements in air quality controls reduce thetoxicity of emissions from incinerators but increase thetoxicity of fly ash and bottom ash disposed of in landfill.This practice of risk transfer must be considered whenevaluating the health risks from waste managementmethods.
3.4 Exposure routes
For physical hazards, the crucial link between a healthhazard and a health outcome is exposure. The risk tohealth depends not only on how much is present but
18
also on whether there is a route by which people maybe exposed. "Indeed, in the absence of exposure, eventhe most toxic compound carries less risk than aninnocuous one." (Kipen 1996 p221.) A completeexposure pathway is a pathway which starts at thesource of contamination and travels throughenvironmental media to the point of exposure and bysome route of exposure to an exposed population (WHOEuropean Centre for Environment and Health 2000). Anexposure pathway has three elements:� release from the site� transport through environmental media� uptake by people.If any of these elements are missing, there is no threatto health.
3.4.1 ReleasePollutants are released from waste operations as gases,liquids and solids:
Gases� Gases exit from incinerator stacks and migrate off
landfill sites.� Organic chemicals volatilise into the atmosphere.
This is a problem where the soils are very heavilycontaminated or where there are open pools of purechemicals in a concentrated aqueous solution(Eduljee 1992).
Liquids� Leachate is carried out of the contaminated area by
percolating water into groundwater. Leachate is acombination of liquid waste arriving in the site andwater added due to rainwater ingress orgroundwater infiltration. Leachate is formed by:� dissolution of soluble matter� bacterial degradation of organic matter � oxidative
decomposition by acetogenesis and anaerobicdecomposition by methanogenesis.
� solubilisation � chemical degradation whereinsoluble inorganics become soluble.
� Leachate is carried off-site by surface runoff.� Wastewater from incinerator cleaning equipment.� Treated sewage effluent.
Solids� Dust emissions resulting from unloading solid waste,
loading temporary landfill cover material, liftconstruction, vehicle traffic to the site, wind erosionfrom site if large areas are left exposed.
� Incinerator ash includes bottom ash (i.e. the solidresidue at the bottom on the grates, the ashremaining after combustible material has beenburnt) and fly ash (i.e the solids collected by particletrapping devices beyond the combustion chamber).Ash contains highly concentrated and bioavailabletoxic heavy metals and dioxins.
Amounts releasedThe quantities released are crucial to an assessment ofexposure. In landfill operations, levels of pollutants varygreatly according to the nature of the wastes depositedand the time period since they were dumped. The typesof chemicals found in landfill gas change during thechemical and microbial decomposition of the waste.Even after the landfill site is closed, there will beemissions for many years, perhaps up to 50 years. (Fordiscussion of the different chemicals produced duringthe stages of landfill degradation, see Bridges et al2000.) Some pollutants, such as metals, are present inincinerator emissions because the combustion processdoes not destroy them while others are formed duringthe cooling of the gas stream (Bridges et al 2000).
3.4.2 Transport of pollutantsPollutants are transferred into and out of variousenvironmental media. Rates of transfer are affected bybiodegradation, partitioning, bio-concentration, dilution,and other physical, chemical and biological processes(National Research Council 2000).
The ground level concentrations of pollutants from anincinerator are affected by the height of the stack, thegas cleaning technology in operation, prevailing windand other weather conditions and the local topography.Metals are neither created nor destroyed by incinerationbut are transported from their embedded, inert phase inthe waste to a highly mobile particle. Some particlescondense on the surface of the fly ash and areeventually sent to landfill where certain conditionsenhance their leachability in water. Many of theseparticles are of respirable size, less than 10micrometers, and can travel long distances through theair. Metals are also released from incinerators as fumes.
3.4.3 UptakePollutants may be released from the waste site and mayremain toxic after passing through variousenvironmental media but will only pose a risk to health ifthey are taken up by people in sufficient quantities andover a sufficient length of time. Potentially exposedpopulations are waste site workers, constructionworkers involved in development of operational orclosed site, on-site trespassers, neighbouring residentsand those using the site and surrounding area forrecreation. The main routes by which people maybecome exposed to pollutants from waste sites areshown below.
InhalationPollutants released into the air from incinerators,composting facilities, and landfill sites may be inhaled bypeople living in the vicinity or working at the sites. Manyparticles from incinerator fumes and fly ash are ofrespirable size and can be directly inhaled. Volatileorganic chemicals may evaporate into the atmospherefrom landfill sites and be inhaled. Measurements made
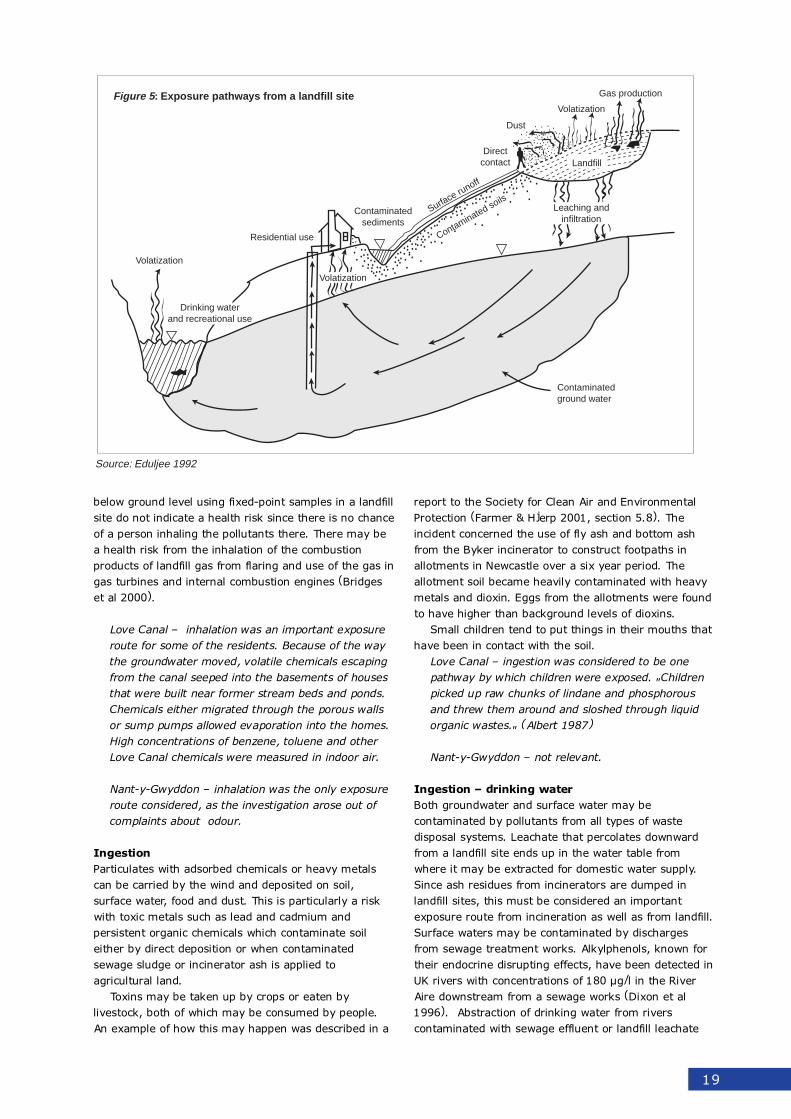
19
below ground level using fixed-point samples in a landfillsite do not indicate a health risk since there is no chanceof a person inhaling the pollutants there. There may bea health risk from the inhalation of the combustionproducts of landfill gas from flaring and use of the gas ingas turbines and internal combustion engines (Bridgeset al 2000).
Love Canal � inhalation was an important exposureroute for some of the residents. Because of the waythe groundwater moved, volatile chemicals escapingfrom the canal seeped into the basements of housesthat were built near former stream beds and ponds.Chemicals either migrated through the porous wallsor sump pumps allowed evaporation into the homes.High concentrations of benzene, toluene and otherLove Canal chemicals were measured in indoor air.
Nant-y-Gwyddon � inhalation was the only exposureroute considered, as the investigation arose out ofcomplaints about odour.
IngestionParticulates with adsorbed chemicals or heavy metalscan be carried by the wind and deposited on soil,surface water, food and dust. This is particularly a riskwith toxic metals such as lead and cadmium andpersistent organic chemicals which contaminate soileither by direct deposition or when contaminatedsewage sludge or incinerator ash is applied toagricultural land.
Toxins may be taken up by crops or eaten bylivestock, both of which may be consumed by people.An example of how this may happen was described in a
report to the Society for Clean Air and EnvironmentalProtection (Farmer & Hjerp 2001, section 5.8). Theincident concerned the use of fly ash and bottom ashfrom the Byker incinerator to construct footpaths inallotments in Newcastle over a six year period. Theallotment soil became heavily contaminated with heavymetals and dioxin. Eggs from the allotments were foundto have higher than background levels of dioxins.
Small children tend to put things in their mouths thathave been in contact with the soil.
Love Canal � ingestion was considered to be onepathway by which children were exposed. "Childrenpicked up raw chunks of lindane and phosphorousand threw them around and sloshed through liquidorganic wastes." (Albert 1987)
Nant-y-Gwyddon � not relevant.
Ingestion � drinking waterBoth groundwater and surface water may becontaminated by pollutants from all types of wastedisposal systems. Leachate that percolates downwardfrom a landfill site ends up in the water table fromwhere it may be extracted for domestic water supply.Since ash residues from incinerators are dumped inlandfill sites, this must be considered an importantexposure route from incineration as well as from landfill.Surface waters may be contaminated by dischargesfrom sewage treatment works. Alkylphenols, known fortheir endocrine disrupting effects, have been detected inUK rivers with concentrations of 180 µg/l in the RiverAire downstream from a sewage works (Dixon et al1996). Abstraction of drinking water from riverscontaminated with sewage effluent or landfill leachate
Volatization
Residential use
Contaminatedsediments
Gas production
Volatization
Directcontact
Surface runoff
Contaminated soils
Dust
Contaminated ground water
Drinking waterand recreational use
Volatization
Leaching andinfiltration
Landfill
Figure 5 : Exposure pathways from a landfill site
Source: Eduljee 1992
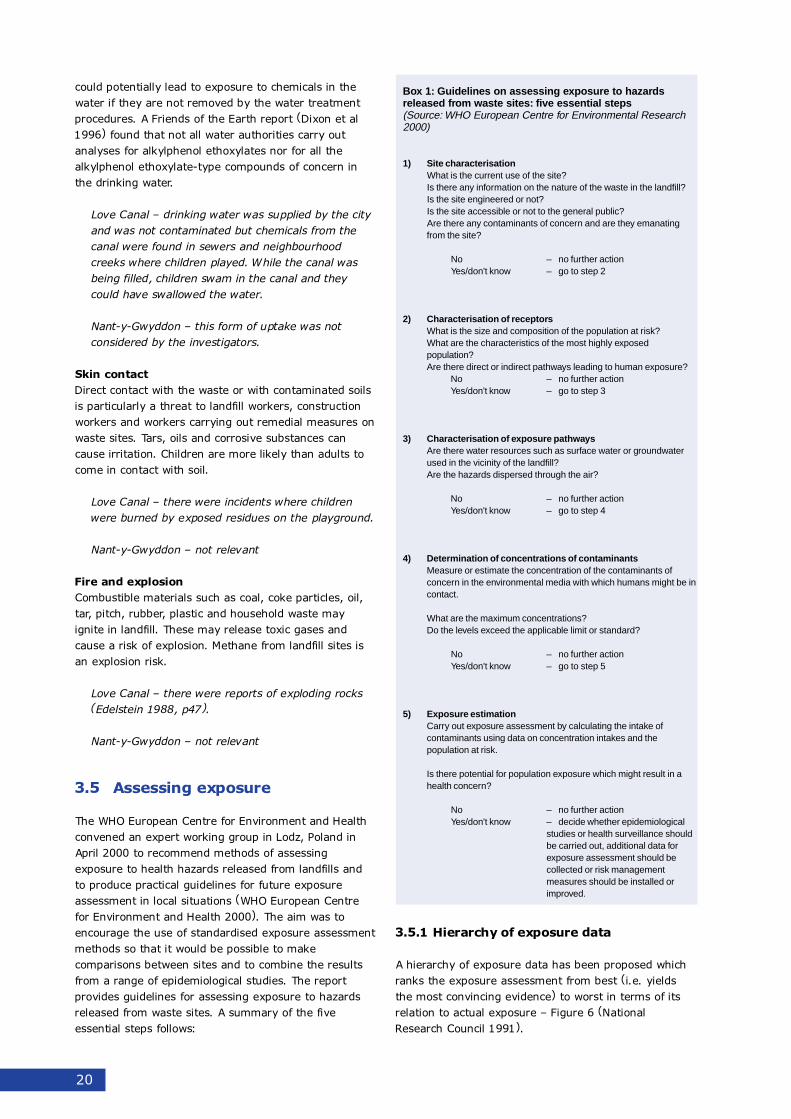
20
could potentially lead to exposure to chemicals in thewater if they are not removed by the water treatmentprocedures. A Friends of the Earth report (Dixon et al1996) found that not all water authorities carry outanalyses for alkylphenol ethoxylates nor for all thealkylphenol ethoxylate-type compounds of concern inthe drinking water.
Love Canal � drinking water was supplied by the cityand was not contaminated but chemicals from thecanal were found in sewers and neighbourhoodcreeks where children played. While the canal wasbeing filled, children swam in the canal and theycould have swallowed the water.
Nant-y-Gwyddon � this form of uptake was notconsidered by the investigators.
Skin contactDirect contact with the waste or with contaminated soilsis particularly a threat to landfill workers, constructionworkers and workers carrying out remedial measures onwaste sites. Tars, oils and corrosive substances cancause irritation. Children are more likely than adults tocome in contact with soil.
Love Canal � there were incidents where childrenwere burned by exposed residues on the playground.
Nant-y-Gwyddon � not relevant
Fire and explosionCombustible materials such as coal, coke particles, oil,tar, pitch, rubber, plastic and household waste mayignite in landfill. These may release toxic gases andcause a risk of explosion. Methane from landfill sites isan explosion risk.
Love Canal � there were reports of exploding rocks(Edelstein 1988, p47).
Nant-y-Gwyddon � not relevant
3.5 Assessing exposure
The WHO European Centre for Environment and Healthconvened an expert working group in Lodz, Poland inApril 2000 to recommend methods of assessingexposure to health hazards released from landfills andto produce practical guidelines for future exposureassessment in local situations (WHO European Centrefor Environment and Health 2000). The aim was toencourage the use of standardised exposure assessmentmethods so that it would be possible to makecomparisons between sites and to combine the resultsfrom a range of epidemiological studies. The reportprovides guidelines for assessing exposure to hazardsreleased from waste sites. A summary of the fiveessential steps follows:
3.5.1 Hierarchy of exposure data
A hierarchy of exposure data has been proposed whichranks the exposure assessment from best (i.e. yieldsthe most convincing evidence) to worst in terms of itsrelation to actual exposure � Figure 6 (NationalResearch Council 1991).
Box 1: Guidelines on assessing exposure to hazardsreleased from waste sites: five essential steps(Source: WHO European Centre for Environmental Research2000)
1) Site characterisationWhat is the current use of the site?Is there any information on the nature of the waste in the landfill?Is the site engineered or not?Is the site accessible or not to the general public?Are there any contaminants of concern and are they emanatingfrom the site?
No – no further actionYes/don't know – go to step 2
2) Characterisation of receptorsWhat is the size and composition of the population at risk?What are the characteristics of the most highly exposedpopulation?Are there direct or indirect pathways leading to human exposure?
No – no further actionYes/don't know – go to step 3
3) Characterisation of exposure pathwaysAre there water resources such as surface water or groundwaterused in the vicinity of the landfill?Are the hazards dispersed through the air?
No – no further actionYes/don't know – go to step 4
4) Determination of concentrations of contaminantsMeasure or estimate the concentration of the contaminants ofconcern in the environmental media with which humans might be incontact.
What are the maximum concentrations?Do the levels exceed the applicable limit or standard?
No – no further actionYes/don't know – go to step 5
5) Exposure estimationCarry out exposure assessment by calculating the intake ofcontaminants using data on concentration intakes and thepopulation at risk.
Is there potential for population exposure which might result in ahealth concern?
No – no further actionYes/don't know – decide whether epidemiological
studies or health surveillance shouldbe carried out, additional data forexposure assessment should becollected or risk managementmeasures should be installed orimproved.

21
The majority of the epidemiological studiesinvestigating links between waste management andhealth outcomes rely on the worst type of evidence �that of residence or employment near the site. A tinyminority of studies are based on quantified ambient orpersonal measurements of pollutants taken at the timeof potential exposure. In most studies, the wastemanagement facility is like a black box, assumed to beemitting toxic compounds but with no actualmeasurements to use in the exposure assessment.
3.5.2 Risk assessmentA risk assessment methodology to characterise andevaluate the health effects arising from exposure tolandfill sites is described by Eduljee who tested it out onthree landfill sites in England (Eduljee 1992, Departmentof the Environment 1994). The risk assessment involvessimplifications of the exposure scenarios, of off-sitetransport of pollutants and of uptake at the point ofexposure. He claims that it is still possible to develop acredible estimate of the health risks to exposedpopulations even with these simplifications. However, inthe UK, the data needed even for simplified riskassessments are not routinely collected. In particular,there is rarely an adequate characterisation of the wastewithin the landfill nor are there data about flowcharacteristics. Risk assessments cannot be carried outfor the majority of landfills in the UK.
Love Canal � in the health impact studies carried outon Love Canal residents, no exposure measurementswere possible as many of the chemicals were notpersistent. Tests were done by the EnvironmentalProtection Agency for chemicals in the blood of 36Love Canal residents but these did not show higherthan expected levels (Heath 1987). Exposure in otherLove Canal studies was estimated on the basis ofdistance of residence from the canal (Vianna andPolan 1984). Paigen and Goldman (1987) explained
how their study proving an effect on birthweight,children's growth and indigenous wildlife was limitedby the lack of "certainty whether those classified asexposed really had exposure, or whether thoseclassified as unexposed really were unexposed."
Nant-y-Gwyddon � No exposure data were availableand there was no community monitoring during thepeak of the problem.
The procedures for assessing the health risks andcalculating a lifetime excess risk are not discussed inthis report. (For a detailed analysis of the risk to healthposed by contaminated soil, see Hawley 1985). Hawleydescribes the assumptions and calculations used toderive annual average intake values, absorption rates,toxicity and excess lifetime cancer risk for youngchildren, older children and adults exposed tocontaminants in soil from indoor and outdoor activities.
In general, high-dose exposure and long-term, low-dose exposure are more likely to result in health impactsthan short-term, low-dose exposures (Buffler et al1985). Since it is extremely difficult to define exposureand thus observe a dose-response relationship in peopleexposed to contaminants from waste management sites,it is very difficult to prove that the health impactsobserved are caused by the exposure.
3.6 Potential impacts on health
Health impacts result from an interaction between thefactors affecting health and the health status of exposedpopulations. In any population, there will be unexplainedhealth problems. The types of health impactsexperienced by people exposed to contaminants fromwaste management sites and those experienced byunexposed people are primarily the same. Health effectsare non-specific � the human body has only a limitednumber of responses to a wide range of internal andexternal assaults. The responses are determined by thecontaminant levels and the susceptibility of individualsalong the range shown in Figure 7 (Hansen et al 1998).
The types of health impacts that have beeninvestigated is very wide. Ideally, the selection ofpossible health outcomes for study should arise from themeasurements of hazardous compounds at the site andthe likely toxic effects of such compounds. However, asdescribed earlier, such exposure data are often missing.In practice, the selection of health outcomes depends onthe availability of data, the level of effort planned, thefrequency of the outcomes and biological plausibility.The literature includes studies of a wide range of healthoutcomes but the most promising are believed to beadverse reproductive outcomes, chromosomal damageand neurotoxic effects (Marsh & Caplan 1987).
The following categories represent the main healthoutcomes found in the literature; other categories havebeen presented (BMA 1998, Marsh & Caplan 1987 p17).The examples given are from studies on the database.
B E S T
W O R S T
Quantified personal measurements
Quantified area or ambient measurements in thevicinity of the residence or other sites of activity
Quantified surrogates of exposure such as estimatesof drinking water use
Distance from site and duration of residence
Residence or employment in reasonable proximityto site where exposure can be assumed
Distance or duration of residence
Residence or employment in defined geographicalarea of the site
Figure 6 : Hierarchy of exposure data
Source: National Research Council 1991

22
3.6.1 Reproductive outcomesReproductive outcomes include early fetal loss, perinataldeath, low birth weight, prematurity, congenitalabnormalities, chromosome abnormalities detected infetuses, sperm abnormalities, altered sex ratio, multiplebirths, decreased fertility, sexual dysfunction, childhoodmorbidity, and age at menopause (list from Marsh &Caplan 1987 p20). The most commonly studiedoutcomes in the literature on waste management arecongenital abnormalities, low birth weight, spermabnormalities, miscarriage and infertility. The usefulnessof selecting these outcomes to investigate causality isdiscussed in the review by Marsh and Caplan (1987).
It is reasonable to look for increased rates of adversereproductive outcomes because in any waste stream,there will be many agents with known or suspectedreproductive toxicity (see Kipen 1996 for examples).Although only five non-infectious agents have beenshown in epidemiological studies to cause adversereproductive outcomes through environmental exposure,rather than through occupational or pharmacologicalexposure, there are hundreds more agents which testpositive in animal studies or in mutagenicity assays(Kipen 1996).
Field and laboratory studies on a range of wildanimals have demonstrated adverse reproductiveoutcomes from xeno-oestrogens, natural and syntheticsubstances with oestrogenic or anti-oestrogenicproperties (IEH 1995). These compounds (listed in Table5) occur in sewage discharges and have been associatedwith endocrine disruption in wildlife, including "thyroiddysfunction in birds and fish, decreased fertility in birds,fish, shellfish and mammals, gross birth deformities inbirds, fish and turtles, metabolic abnormalities in birds,fish and mammals, behavioural abnormalities in birds,demasculinisation and feminisation of female fish and
birds, and compromised immune systems in birds andmammals" (Colborn & Clement 1992 quoted in IEH1995). The relevance of these studies to human healthis not clear but there is concern about the fall in quantityand/or quality of sperm in recent decades (IEH 1995,Colborn et al 1997).
Love Canal � Low birth weight, prematurity and birthdefects in children living near the hazardous wastesite (Goldman et al 1985).Nant-y-Gwyddon � congenital malformations,spontaneous abortions, stillbirths (Fielder et al 2000).
3.6.2 Non-communicable diseasesAccording to the chair of the US Committee onEnvironmental Epidemiology, the main health outcomesfrom exposure to hazardous waste sites that should beconsidered are a range of diseases, including asthma,adult-onset respiratory hypersensitivity, disturbance oflung function and growth, degenerative neurologicdiseases, immunologic and endocrine diseases such asdiabetes and cancer, including leukaemia (Miller 1996).
Love Canal � cancer incidence in the Love Canal area(Janerich et al 1981).Nant-y-Gwyddon � rates of hospital admissions forgeneral medical and geriatric, all respiratory diseaseand asthma (Fielder et al 2000).
3.6.3 SymptomsSymptoms are either self reported or inferred fromconsumption of over-the-counter drugs or prescribedmedications.
Love Canal � complaints by residents of chloracne,skin irritation, eye irritation, ulcers, pains, and widerange of unexplained health problems. Those whobelieved in the chemical risks suffered from"unpredictably recurring, debilitating anddiagnostically elusive illnesses" (Edelstein 1988).
Nant-y-Gwyddon � residents complained of stress,fatigue, headaches, eye infections, coughs, stuffynose, dry throat, nausea (Fielder et al 2000).
3.6.4 Injuries and poisoningThese are more likely to be associated with occupationalhealth problems than with residence near a site.
Death, disabling and non-disabling injury associatedwith the removal of contaminated soils (Mar et al1993).Heat stress in hazardous waste workers (Favata et al1990).
H I G H L E V E L E X P O S U R E
L O W L E V E L E X P O S U R E
Mortality
Morbidity
Pathophysiologic changes, e.g. organ function impairment
Physiologic changes of uncertain significance, e.g. biochemical and subcellular changes
Body burdens of pollutants with nodiscernable effect on health
Figure 7 : Health impacts
Source: Hansen et al 1998
23
3.6.5 Microbial diseasesThese include viral, bacterial, fungal and parasiticdiseases.
Health risks associated with bathing in sewage-contaminated sea water (Balarajan et al 1991).Risk of infection associated with a wastewater sprayirrigation system used for farming (Linnemann et al1984).
3.6.6 MortalityLove Canal � cause specific mortality (Stark 2000).Nant-y-Gwyddon � assessed whether there wasdifference in age standardised rates of death, allcause, respiratory and cancers (Fielder et al 2000).
3.6.7 Psychosocial impactsLove Canal � stress, stigma, lack of support,community spirit, health preoccupation, dread, fear,well-being, depression, dissatisfied with life, loss ofpersonal control, increase in stress relatedbehaviours such as smoking, increased irritability(Edelstein 1988).Nant-y-Gwyddon � only physical health problemswere reported (Fielder et al 2000).
3.6.8 Economic impactsLove Canal � declaration of a health emergency bystate department of health led to evacuation ofpregnant women, then relocation of some residentswith economic costs.
Nant-y-Gwyddon � not described.
Other example:Social and economic consequences of health effectsto incineration workers � workers' compensationbenefits, loss of home, loss of car, loss ofemployment (Callender et al 1997).
3.6.9 Subclinical abnormalities � biomarkersSome of the biomarkers studied are:� Tests for organ function � e.g. liver function tests.� Immunological abnormalities � e.g. lymphocyte
tests.� Cytogenetic effects � chromosome aberrations,
assays of sister chromatid exchanges.� Neurotoxic effects � nerve conduction abnormalities,
evoked-potential studies.
The significance of these, as they have littlediscernible clinical effect, is difficult to assess. Theadvantages and limitations of using biomarkers isdescribed by Marsh and Caplan (Marsh & Caplan 1987).
Love Canal � Cytogenetic findings in persons livingnear the Love Canal (Heath et al 1984).Nant-y-Gwyddon � no biomarkers investigated.
3.6.10 Broad environmental factorsGlobal warming can contribute to health indirectly bydisturbing crop production, and affecting the spread andtransmission of contagious and vector-born diseasessuch as cholera and malaria.
24
How strong is the evidence that current wastemanagement practices have had an impact on humanhealth?
4.1 Types of study
In a �weight of evidence� approach to evaluatingevidence, greater weight is placed on the conclusionsdrawn from some types of study over others. Studydesigns at the top of the hierarchy (see Table 6) are theones most likely to lead to valid conclusions from whichgeneralisations can be made (CRD 2001, WHO WorkingGroup 2000). Evidence from studies on people is moreconclusive than extrapolations from studies on animals,while animal studies carry more weight than studies onparts of organisms outside the body or on relatedchemicals. Amongst the different kinds of studies on
people, the ones higher up the hierarchy, i.e.experimental studies and prospective cohort studies, areuseful for testing hypotheses and establishing whether acausal relationship exists. The study designs furtherdown the hierarchy, e.g. observational studies withoutcontrols, are useful for generating hypotheses whichsubsequently need confirmation from study designsfurther up the hierarchy.
From some study designs it is possible to inferwhether the intention was that the study be ahypothesis-testing or a hypothesis-generating study. Forthe most part, cross sectional studies are abouthypothesis generation whereas cohort and case controlstudies are concerned with hypothesis testing. Howeverin many cases, the actual execution of the study isflawed in ways that make hypothesis testingproblematic. Studies which purport to be hypothesistesting cannot be seriously regarded in that light unless
4 Evidence of an impact on health
:6elbaT sngisedydutsfoyhcrareiH
ydutsfoepyT tnemeganametsawnoerutaretilehtmorfselpmaxeevitartsullI
ELPOEPNOSEIDUTS
seidutslatnemirepxE .g.edelaecnochtiwlairtdellortnocdesimodnaR
.noitacolla
lairterusopxedesimodnarmorfstluser:gnihtabaesmorfsitiretneortsagfodoohilekiLsitiretneortsaggnitluserrofgnikcehcdnaretawaesnistcejbusfonoisremmignivlovni
.)4991lateyaK(
seidutslatnemirepxe-isauQ .g.e.noitasimodnartuohtiwydutslatnemirepxE
seidutslanoitavresbodellortnoC .g.e-.seidutstrohocevitcepsorP
.seidutstrohocevitcepsorterlacirotsiH.seidutslortnocesaC
evitcepsortera:emoRnisrotarenicnietsawlapicinumtasrekrowgnomaytilatroM.)7991lateitipaR(ydutstrohoc
taerewcebeuQnietisllifdnaletsawdiloslapicinumaraendevilohwnemrehtehW.snoitacoletomereromtadevilohwslaudividninahtrecnacgnipolevedrofksirrehgih
recnac,weivretni,desab-noitalupopdetelpmocylsuoiverpamorfdetcelesstcejbuS8292=n(recnacfosetisneetrihT.laertnoMnidevilohwnemfoydutslortnoc-esac
tegrebdloG(dezylanaerew)714=n(puorglortnocdesab-noitalupopadna)stcejbus.)9991la
seidutslacigolocE - seidutslanoitavresbospuorglortnoctuohtiw
sanwonkosla(seidutsnoitalerroC.)seidutsnosirapmoclacihpargoeg
.syevruslanoitces-ssorC.sisylanaretsulC
sisylanaretsulCerewtopedetsawsuodrazaharaenaeraehtniytilatromdnaecnedicnirecnaC
tceridniehtgnisuailartsuA,selaWhtuoSweNnitahtotderapmocdnadetaluclacselamnirecnacniarb,doirepraey-81narevO.noitasidradnatsxesdnaegafodohtem
yltnacifingissawaeraydutsehtniecnedicnierehwrecnacylnoehtsaw)sesac6(.)8991nidulalaJ&smailliW(detcepxenahtrehgih
yevrusytidibromevitcepsorpgnitareneg-sisehtopyHlapicinumhtiwderapmocerewetisllifdnalatasrekrowfosmelborphtlaehdetroperfleS
sesaercnidevresbO.noitamrofnierusopxeoN.snoitapuccoroodtuorehtoniseeyolpmefohtgnerts,ytilibisualplacigoloibotgnidroccaytilibidercrofdedargerewytidibromni
,sitihcnorbcinorhC.erusopxefoytisnetnifotneidargksirdna,retsulcemit,noitaicossaylhgiherewsredrosiddoomdnasmotpmyscitocran,yrotaripserdenibmoc,hguocyliad
.)7891latenamztreH(etisllifdnalehthtiwnoitaicossanafoelbiderc
seidutsesaC ohwetistsopmocfaellapicinumafodoohruobhgienehtnignivilnamafotroperesaC.)9891lateremarK(sisolligrepsayranomlupohcnorbcigrellamorfdereffus
,ygoloisyhpohtapnodesabnoinipotrepxE.susnesnocrohcraeserhcneb
SLAMINANOSEIDUTS
-seidutslacigolocixotlaminA ovivni ,syassafotnempoleved,tnegaotesnopsercixot
.slaminadesopxeniesaesid
dnacitapeh:stnanimatnocretawdnuorg52foerutximlacimehcafoseidutsygolocixoTfoecneulfnidna,egnellahcedirolhcartetnobracotesnopser,tnemssessalaner
.)4991latesnommiS(noitcirtserretawdecudni-tnemtaert
SMSINAGROFOSTRAPNOSEIDUTS
ortivnI llec,syassamret-trohs,syassa.syassalairetcab,serutluc
lateenahS(rotarenicnilapicinummorfhsaylffoyassayticinegatumlairetcabsemA.)3991
SLACIMEHCNOSEIDUTS
.erutcurtslacimehcmorfsnoitciderP
25
there is evidence in the report that:a. there is an adequate control groupb. there is adequate exposure datac. there is clear evidence of an hypothesis to be tested.Some studies described as cross sectional studies maybe better described as cohort studies because theyinclude evidence of a temporal relationship. Forexample, occupational exposures are necessarilyretrospective in nature.
(For a useful description of epidemiological studydesigns, see Marsh & Caplan 1987, WHO EuropeanCentre for Environment and Health 2000 Annex A4.1.)
4.2 Study limitations andconfounding factors
It is difficult to establish a cause-and-effect relationshipin epidemiological studies in the field of wastemanagement. Particular challenges concern confoundingby other unrelated factors that may explain the resultsas well as the factor under investigation, incompletenessof data, and variability.
4.2.1 ConfoundingConfounding takes place when the exposure isassociated with some other factor which also increasesthe risk of the health outcome studied. For example, apositive correlation between breast cancer and pesticideexposure may be confounded by factors such as highersocio-economic status and delayed child-bearing whichalso apply to the sample under study. It may be possibleto adjust for the effects of potential confounding factorsif enough detailed data are collected.
Factors which affect exposureOther sources of pollutants could be a confoundingfactor, undermining the conclusion linking a particularwaste management site to the health outcomesobserved in a study. There are few areas where there isonly one source of pollutants to which a population isexposed. As well as other environmental pollutants fromindustrial and traffic pollution, there is usuallyconcurrent exposure to occupational hazards, indoor airpollutants, tobacco smoke, alcohol, prescription drugsand recreational drugs.
Where there are several sources of pollutants, theremay well be interactions between the exposures. In theabsence of exposure data, models and epidemiologicalmethods cannot clarify what these interactions may be.Exposure to one source of pollutants may potentiate ormay suppress the relationship between the otherexposure and the health outcome (Marsh & Caplan1987).
Nant-y-Gwyddon � the conclusion that the landfill sitein Nant-y-Gwyddon may have been responsible foran increased rate of congenital abnormalities inresidents near the site (Fielder et al 2000) has been
challenged by researchers who pointed out that amunicipal incinerator operated in the same area justbefore the landfill site opened (Roberts & Redfearn2000). There was no direct evidence that the landfill,rather than the poorly performing and heavilypolluting incinerator, was the cause of the adversehealth outcomes.
Factors which affect healthMatching � Where there is a control group or referencepopulation, an attempt can be made to adjust for theother factors which may have a significant effect on thehealth outcome being studied, i.e. age, social class,occupation, race, gender. To adjust for social class,researchers use measures of deprivation such as theCarstairs deprivation index which is based on socialclass, unemployment, access to a car, and overcrowding(used by Elliott et al 2001). McNamee and Dolk(McNamee & Dolk 2001) point out that the Carstairsindex may not be an adequate proxy measure for allrelevant risk factors and that failure to account forimportant risk factors could substantially distort therelative risks, especially if the relative risks are small asthey were in the SAHSU study (Elliott et al 2001).
Symptoms � Many studies are of self-reportedsymptoms but these studies do not clarify the cause ofthe higher symptom rates. Miller points out that theremay be several explanations for higher symptom ratesin communities near waste management facilities otherthan toxicological or immunological reactions topollutants (Miller 1996). The increased rate may be dueto psychosomatic reactions to the stress brought on bythe presence of a nearby facility, mass psychogenicillness as a reaction to publicity relating to the site,recall bias and confounding factors that have not beenidentified or considered in the analysis.
Biomarkers are becoming more popular as a way ofindicating exposure and as predictors of outcome.However, there is uncertainty about the interpretation ofpositive biomarker results and lack of knowledge abouthow long the abnormalities persist after exposure. Forsome biomarkers, exposure must be current or veryrecent to be detectable. In the case of chromosomaldamage, exposure to pollutants may cause DNAdamage, leading to DNA repair problems. This can bedetected in cytogenetic challenge studies. Theassumption is that individuals with an abnormalcytogenetic response are defective in DNA repair andthus have an increased risk for cancer. However, there isno proof of this association. Many other ubiquitousagents such as sunlight and X-rays cause DNA damage,the rate of DNA repair is not known and laboratoryconditions can affect the amount of damage. (For auseful discussion of the use of biomarkers in studies ofwaste sites see WHO European Centre for Environmentand Health 2000 Annex 5.)

26
4.2.2 Incompleteness of data
Exposure dataMost studies have no exposure data whatsoever, usingresidence near the site based on postcodes or censustracts as a surrogate for actual exposure measurements.Residence, however, is an inadequate and crudesubstitute. Misclassification can occur if people moveinto or out of the area during the time they were meantto be exposed. Leachate from a landfill site maycontaminate groundwater or surface water and affect amuch wider population living further away. People livingupwind may be minimally exposed to air pollutantscompared to those living downwind. In some studies,residence selection is refined slightly to account for this.Where exposure data are absent, the reliability of anyconclusions drawn is substantially weakened.
Love Canal � residence in a Love Canal census tractwas used as a surrogate measurement of exposure inmost Love Canal studies (Janerich et al 1981, Vianna& Polan 1984, Goldman et al 1985, Paigen et al1985, Paigen et al 1987). There was one study whichused actual measurements of chemicals likely to havearisen from the canal (Heath et al 1984). This studyreported no differences in chromosome aberrations in46 people who lived in houses where chemicals weredetected compared with people who lived in anadjacent census tract. However, the exposure datawere limited as there were no data on how long andsustained the exposure was.
Nant-y-Gwyddon � residence within five electoralwards within 3 km of the landfill site was used as asurrogate measurement of exposure (Fielder et al2000).
Defining the exposed population is fraught withdifficulties but is necessary to establish the denominatorfrom which an incidence rate can be calculated. Ifgroundwater is contaminated, communities far from thewaste site may be drinking the water and the exposedpopulation may in fact be greater than those livingwithin 2 km of the site. However, the concentration ofcontaminants in groundwater far from the site will bevery small and thus it will be even harder to pick uphealth effects. In many studies, there are large gapsbetween exposure and the start of the study. Immediatehealth problems can be missed and people move out ofthe area making it hard to trace them.
Studies without a control group can prove very littleas health is strongly affected by characteristics such asrace, social class, smoking, alcohol use, age, sex, dietand occupation which have little to do with exposure tocontaminants from waste management sites. It isdifficult to find an appropriate control group matched forall confounding risk factors. Most important, the controlgroup should not be exposed to hazards either from thewaste management site being studied or other ones inthe area.
Love Canal � a study by the New York StateDepartment of Health found no evidence for highercancer rates in Love Canal residents than in the stateof New York as a whole or in the city of Niagara Fallsof which Love Canal is a part (Janerich et al 1981).The study was done by examining data from astandardised reporting system, the New York CancerRegistry, whose completeness and accuracy couldnot be guaranteed. The exposed population was notwell defined as the study was based on census tractswhich did not correspond exactly to proximity to LoveCanal nor did it include people who had left the area.The US Environmental Protection Agencycommissioned a cytogenetic study of Love Canalresidents which showed an increase in chromosomedamage (Picciano 1980). The study was subsequentlydiscredited as having virtually no scientific validitybecause the control group was not matched withLove Canal residents and because they were nottested simultaneously (Kolata 1980). A later studywith proper controls showed no difference inchromosome damage between exposed people andthe control group (Heath et al 1984).
Nant-y-Gwyddon � the control group was thepopulation in 22 wards in the same authoritymatched for Townsend deprivation score. Theexposed population was slightly less deprived by thissocioeconomic measure than the comparison group(Fielder et al 2000).
Health outcome dataUnreliability � Data about health outcomes may beincomplete or unreliable for a number of reasons withmajor implications for the conclusions reached in theepidemiological studies. Data on congenitalmalformations and stillbirths are highly dependent onthe motivation by health authorities to notify to theregister, to changes in reporting criteria and todefinitions used. When discussing the issues limiting thereliability of the conclusions from the SAHSU study(Elliott et al 2001), the authors mention over-reportingof anomalies in Scotland, under-reporting of anomaliesin England and Wales and changes in the rules aboutwhich malformations were notifiable.
Recall bias inevitably leads to over-reporting incommunities where people are worried about the healtheffects of a waste site. People are already aware of andlooking out for health problems. Recall bias is especiallyimportant for symptoms but less so for other conditionswith more objective measurements such as low birthweight. The limitations of using health outcome databased on recall is described in a study of 22 peopleexposed to fumes from ruptured drums containing nitricacid during a hazardous waste site clean-up operation(Hopwood & Guidott 1988). The people wereinterviewed immediately after the incident byemergency room staff, the next morning by aresearcher and six months later. There was a low level

27
of agreement between the symptoms reported sixmonths after the incident and those reported at thetime. The trend was not random. Subjects consistentlyrecalled more symptoms in the later interview.
Love Canal � from informal surveys carried out bythe residents of Love Canal, a long list of healthimpacts was produced. On the list were birth defects,deafness, rashes, headaches, cancer, epilepsy-likeseizures, nervous disorders, miscarriage, asthma,liver damage, the death of a child from kidney failureand a case of nausea, thick perspiration and sores(Brown 1980).
Latency periods � Studies of illnesses such as cancerwhich have a long latency period can lead to falsenegatives if not followed for a sufficient period of time.Latency periods may be in the order of one year forchildhood leukaemia, several years for adult leukaemiaand longer for solid tumours (Elliott et al 2001). For fetalexposure to hormone-disrupting chemicals, the latencyperiod may be even longer.
Colborn argues that fetal exposure may "deraildevelopment in a variety of ways that will becomeevident at different times, e.g. a boy exposed may haveundescended testicles at birth, low sperm count atpuberty or testicular cancer in middle age." (Colborn etal 1997)
Love Canal � A limitation of the Janerich study(1981) was that exposure from chemicals leakingfrom Love Canal was greatest during the 1970s.Cancers appearing 10 to 15 years later would nothave appeared in that study which used data only upuntil 1977. In a study of chromosomal aberrations(Heath 1987), measurements of the chemicals weremade in 1978 but the chromosome tests were notcarried out until 1980. It is not clear how long afterexposure cytogenetic damage persists and can bedetected.
Sample size and statistical powerThe population affected by a particular waste site isusually small. This limits the range of health effects andthe number of cases that can be observed. The rarer thedisease, the larger the exposed and control group needto be in order to detect a significant increase among theexposed. To design an epidemiological study looking fora doubling in reproductive effects with a probability ofless than 0.05 (p<0.05), the size of the exposed andcontrol groups need to be:
Miscarriage � 15% recognised pregnancies160 pregnancies
Minor birth defects � 10% live births266 live births
Major birth defects � 2% live births1525 live births
Club foot � 0.6% live births5199 live births
(Zielhuis 1985)
In a review of published public health investigationsat 16 hazardous waste sites in the United States, onlytwo studies included more than 1000 people while therest had fewer than 500 people (Levine and Chitwood1985).
Love Canal � a statistically significant excess of lowbirth weight was found in babies living along theswales by Love Canal from 1940 to 1953 when thelandfill was active. From 1954 to 1978, there was nodifference in birth weight between babies born in theLove Canal area and the rest of upstate New York.Included in the study were 383 women who had a totalof 617 children and who lived in the study area fromJanuary 1940 through June 1978 (Vianna and Polan1984).
Single site studies are limited in their statistical power todetect excess risks for rare health outcomes. Multi-sitestudies increase statistical power but have otherproblems. They may dilute out adverse healthoutcomes, obscuring a few highly polluting sitesamongst the statistical average. Even in a study with animpressively large sample size, the observed increase inrisks could be due to study bias. The recent British studyof reproductive outcomes among women living within 2km of landfill sites included about 8 million pregnanciesand 9,565 landfill sites (Elliott et al 2001). Statisticallysignificant excess risks of congenital abnormalities werefound. However, the excess risks were so small, i.e. lessthan 10%, that they could be explained by other biasesin the data (McNamee & Dolk 2001).
4.2.3 VariabilityVariability is defined as the "individual-to-individualdifferences in quantities associated with the predictedrisk" (National Research Council 2000).
Variability in human populationsUnlike laboratory animals which are bred forhomogeneity, the exposed human population isheterogeneous. Children, fetuses, women of child-bearing age and the elderly are particularly sensitive.Children are not just small adults but differ in bodycomposition and maturity of biochemical andphysiological functions (Hansen et al 1998). The fetus isparticularly vulnerable. Many chemicals cross theplacenta and can affect development without obviouseffects on the mother. Young children exposed to lead insoil are more at risk than adults because of theirbehaviour which leads to ingestion of lead from dirtyhands and toys. Adults over 40 years are moresusceptible to carbon monoxide exposure because asmall proportion have decreased cardiovascularcapacity.
As well as differences across age-groups, inter-individual variation affects an individual's predispositionto health outcomes. The interaction between genes andthe environment affects people's resistance or sensitivity
28
to a range of chemical and physical insults and mayexplain why some families living near a waste site areaffected while others are not and why within thesefamilies, some individuals are affected while others arenot.
Variability of waste proceduresUnlike a health care intervention, waste managementmethods are not controlled processes but broadcategories with large variations between individualfacilities and large gaps in the information available.Waste management sites vary from facility to facility andfrom country to country with regard to:
� What goes inThe composition and feed rate of wastes treated.
� How the waste is treatedOperating practices, age of facility, waste disposaltechnology used, frequency of off-normal emissionevents, gas and leachate control systems.
� What comes outThe type and amount of pollutants emitted, climateaffecting atmospheric dispersion, landscape dataaffecting migration through soil and water, facilitydata, pollution-control technologies in use.
� How the emissions reach people � the exposurerouteTransfers by deposition and partitioning to exposuremedia � extent to which groundwater is extractedfor drinking water, human activities which bringpeople into contact with pollutants � consumption oflocally grown food, consumption of drinking water,contact with soil, construction of homes close to thesite, occupational exposure, etc., proximity to othersources of pollutants.
4.2.4 ConclusionWhilst it is technically possible to detect the presence ofhealth hazards in waste sites and health impacts amongpeople working or living nearby, there are manyproblems demonstrating the relationship betweenexposure and the health impacts observed. The mainlimitations of epidemiological investigations are the smallsample size, lack of exposure information, lack oftoxicological data about mixtures of chemicals and thelack of specificity of indicators of adverse health effects.
Even in the case of Love Canal, where contaminationwas undisputed and great efforts were made to studypossible health effects, the studies did not show analarming increase in ill health.
Given these limitations, there will always be a high levelof uncertainty about the health risks to people exposedto hazards from waste management sites.
4.3 The strength of the association
An association, even if statistically significant, is not
proof of causation. To determine causation, the causemust precede the effect and the association should be"consistent, unbiased, strong, graded, coherent,repeated, predictive and plausible" (WCRF & AICR,1997). The strength of the association is an importantpart of assessing causality, but other factors must betaken into account: consistency of the observedassociation, speciality of association, temporal sequenceof events, dose-response relationship, biologicalplausibility of the observed association and experimentalevidence (Lilienfield 1994).
4.3.1 Relative riskRelative risk, RR, is a measure of the strength of therelationship between two variables, usually the proposedcause and effect. For example, it is the ratio of the riskor incidence of a disease among people with a particularcharacteristic (say, residents living near an incinerator)to that among people without that characteristic (say,residents living far from the incinerator).� A relative risk of less than 1 implies a protective
effect.� A relative risk of more than 1 implies an increased
risk. For example, a RR of 2 indicates a doubling ofthe risk. A RR of 1.1 indicates a 10% increase.
� A relative risk of 1 implies no effect.
Small relative risk values, those less than two, maybe important when the number of affected people islarge or the disease is very common and whenconfirmed in several large, well-designed studies.Because observational studies are plagued by biases,uncertainties and confounding factors, manyepidemiologists believe that epidemiological studies maybe inherently incapable of accurately discerning weakassociations. As Michael Thun, the director of analyticepidemiology for the American Cancer Society, puts it,"With epidemiology you can tell a little thing from a bigthing. What's very hard to do is to tell a little thing fromnothing at all." (Quoted in Taubes 1995.)
The odds ratio, OR, is another way of expressing thesize of the effect. It is the ratio of the odds of an effectin the exposed group compared to the odds in thecontrol group. When the rates are very low or very high,the odds ratio is very similar to the relative risk (CRD2001).
:7elbaT stnemegdujdnaksirevitaleR
tnemegduJ ?noitaicossaehtsignortswoH
gnortS yllacitsitatssidna5.0<ro2>siROroRRtnacifingis
etaredoM yllacitsitatstontub5.0<ro2>ROroRRrotnacifingis
dna57.0-5.0ro0.2-5.1neewtebsiROroRRtnacifingisyllacitsitats
kaeW tontub57.0-5.0ro0.2-5.1neewtebsiROroRRtnacifingisyllacitsitats
oNnoitaicossa
yllacitsitatstondna5.1dna78.0neewtebsiRRtnacifingis
7991RCIAdnaFRCW:ecruoS
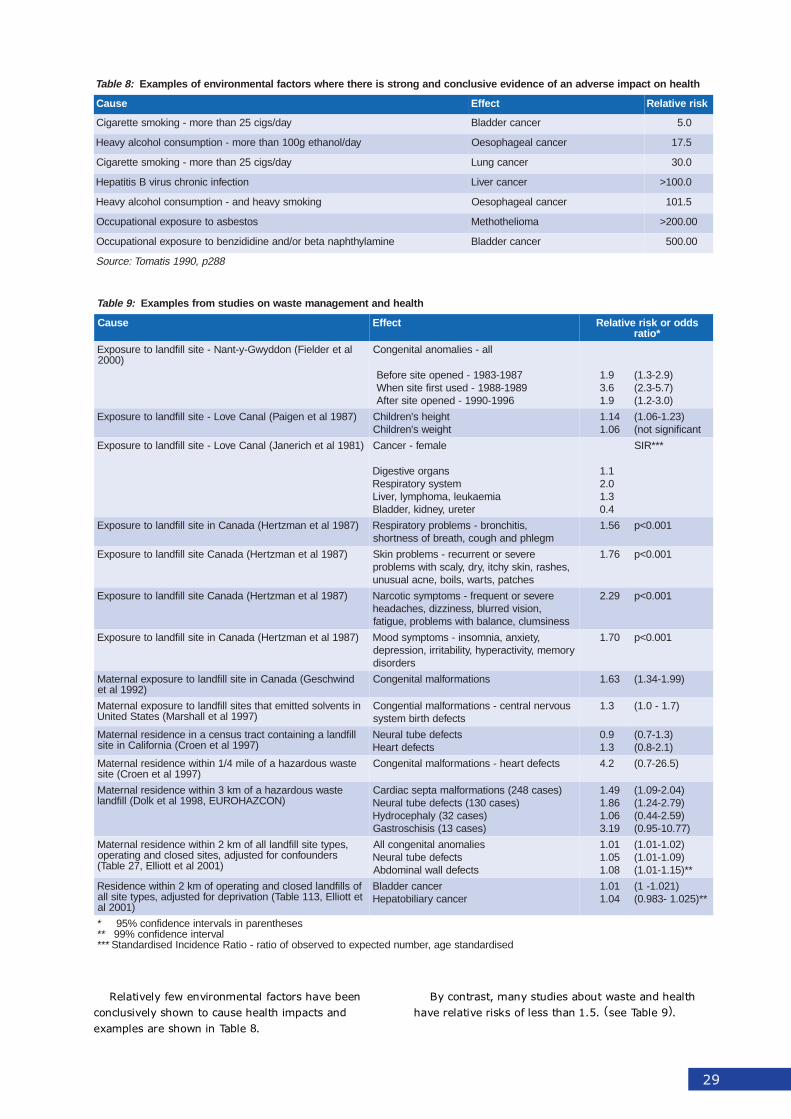
29
:9elbaT htlaehdnatnemeganametsawnoseidutsmorfselpmaxE
esuaC tceffE sddoroksirevitaleR*oitar
lateredleiF(noddywG-y-tnaN-etisllifdnaloterusopxE)0002
lla-seilamonalatinegnoC
7891-3891-denepoetiserofeB9891-8891-desutsrifetisnehW
6991-0991-denepoetisretfA
9.16.39.1
)9.2-3.1()7.5-3.2()0.3-2.1(
)7891latenegiaP(lanaCevoL-etisllifdnaloterusopxE thgiehs'nerdlihCthgiews'nerdlihC
41.160.1
)32.1-60.1(tnacifingiston(
)1891latehcirenaJ(lanaCevoL-etisllifdnaloterusopxE elamef-recnaC
snagroevitsegiDmetsysyrotaripseR
aimeakuel,amohpmyl,reviLreteru,yendik,reddalB
1.10.23.14.0
***RIS
)7891latenamztreH(adanaCnietisllifdnaloterusopxE ,sitihcnorb-smelborpyrotaripseRmgelhpdnahguoc,htaerbfossentrohs
65.1 100.0<p
)7891latenamztreH(adanaCetisllifdnaloterusopxE erevesrotnerrucer-smelborpnikS,sehsar,niksyhcti,yrd,ylacshtiwsmelborp
sehctap,straw,sliob,encalausunu
67.1 100.0<p
)7891latenamztreH(adanaCetisllifdnaloterusopxE erevesrotneuqerf-smotpmyscitocraN,noisivderrulb,ssenizzid,sehcadaeh
ssenismulc,ecnalabhtiwsmelborp,eugitaf
92.2 100.0<p
)7891latenamztreH(adanaCnietisllifdnaloterusopxE ,yteixna,ainmosni-smotpmysdooMyromem,ytivitcarepyh,ytilibatirri,noisserped
sredrosid
07.1 100.0<p
dniwhcseG(adanaCnietisllifdnaloterusopxelanretaM)2991late
snoitamroflamlatinegnoC 36.1 )99.1-43.1(
nistnevlosdettimetahtsetisllifdnaloterusopxelanretaM)7991latellahsraM(setatSdetinU
suovrenlartnec-snoitamroflamlaitnegnoCstcefedhtribmetsys
3.1 )7.1-0.1(
llifdnalagniniatnoctcartsusnecaniecnediserlanretaM)7991lateneorC(ainrofilaCnietis
stcefedebutlarueNstcefedtraeH
9.03.1
)3.1-7.0()1.2-8.0(
etsawsuodrazahafoelim4/1nihtiwecnediserlanretaM)7991lateneorC(etis
stcefedtraeh-snoitamroflamlatinegnoC 2.4 )5.62-7.0(
etsawsuodrazahafomk3nihtiwecnediserlanretaM)NOCZAHORUE,8991latekloD(llifdnal
)sesac842(snoitamroflamatpescaidraC)sesac031(stcefedebutlarueN
)sesac23(ylahpecordyH)sesac31(sisihcsortsaG
94.168.160.191.3
)40.2-90.1()97.2-42.1()95.2-44.0()77.01-59.0(
,sepytetisllifdnalllafomk2nihtiwecnediserlanretaMsrednuofnocrofdetsujda,setisdesolcdnagnitarepo
)1002latettoillE,72elbaT(
seilamonalatinegnocllAstcefedebutlarueN
stcefedllawlanimodbA
10.150.180.1
)20.1-10.1()90.1-10.1(
**)51.1-10.1(
fosllifdnaldesolcdnagnitarepofomk2nihtiwecnediseRtettoillE,311elbaT(noitavirpedrofdetsujda,sepytetislla
)1002la
recnacreddalBrecnacyrailibotapeH
10.140.1
)120.1-1(**)520.1-389.0(
* sesehtnerapnislavretniecnedifnoc%59** lavretniecnedifnoc%99*** desidradnatsega,rebmundetcepxeotdevresbofooitar-oitaRecnedicnIdesidradnatS
:8elbaT htlaehnotcapmiesrevdanafoecnediveevisulcnocdnagnortssierehterehwsrotcaflatnemnorivnefoselpmaxE
esuaC tceffE ksirevitaleR
yad/sgic52nahterom-gnikomsetteragiC recnacreddalB 0.5
yad/lonahteg001nahterom-noitpmusnoclohoclayvaeH recnaclaegahposeO 5.71
yad/sgic52nahterom-gnikomsetteragiC recnacgnuL 0.03
noitcefnicinorhcsurivBsititapeH recnacreviL 0.001>
gnikomsyvaehdna-noitpmusnoclohoclayvaeH recnaclaegahposeO 5.101
sotsebsaoterusopxelanoitapuccO amoilehtohteM 00.002>
enimalyhthpanatebro/dnaenididizneboterusopxelanoitapuccO recnacreddalB 00.005
882p,0991sitamoT:ecruoS
Relatively few environmental factors have beenconclusively shown to cause health impacts andexamples are shown in Table 8.
By contrast, many studies about waste and healthhave relative risks of less than 1.5. (see Table 9).
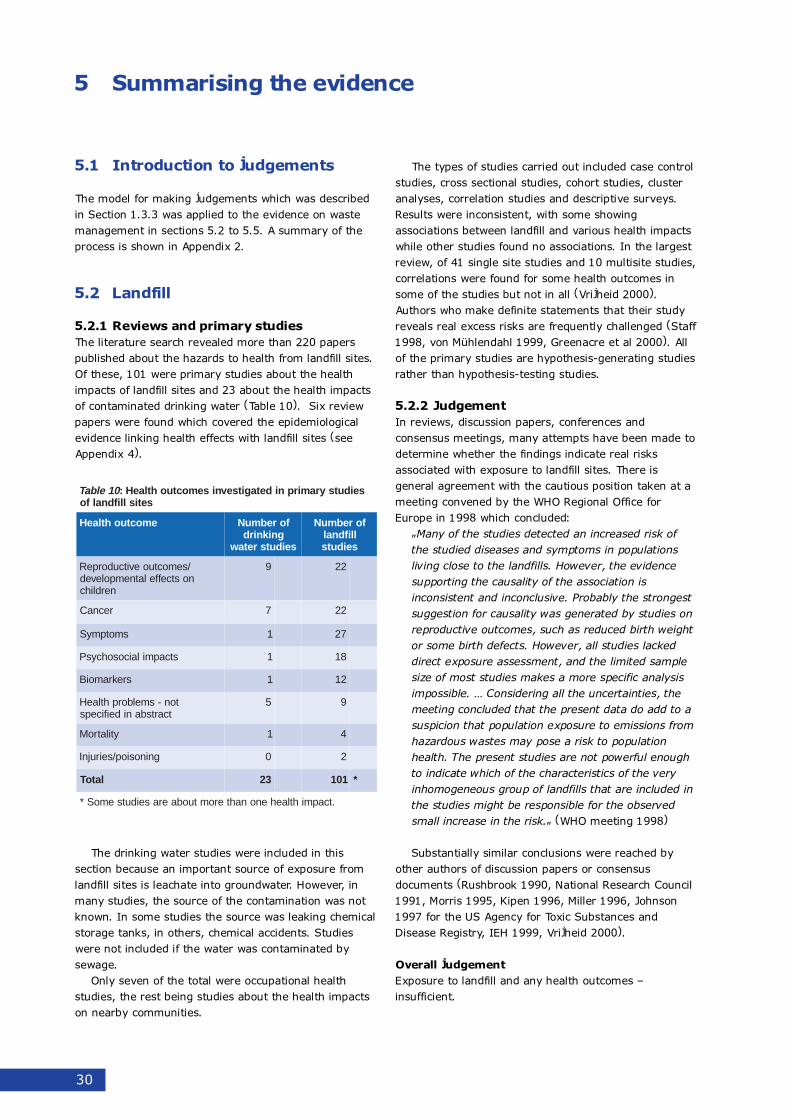
30
5.1 Introduction to judgements
The model for making judgements which was describedin Section 1.3.3 was applied to the evidence on wastemanagement in sections 5.2 to 5.5. A summary of theprocess is shown in Appendix 2.
5.2 Landfill
5.2.1 Reviews and primary studiesThe literature search revealed more than 220 paperspublished about the hazards to health from landfill sites.Of these, 101 were primary studies about the healthimpacts of landfill sites and 23 about the health impactsof contaminated drinking water (Table 10). Six reviewpapers were found which covered the epidemiologicalevidence linking health effects with landfill sites (seeAppendix 4).
The drinking water studies were included in thissection because an important source of exposure fromlandfill sites is leachate into groundwater. However, inmany studies, the source of the contamination was notknown. In some studies the source was leaking chemicalstorage tanks, in others, chemical accidents. Studieswere not included if the water was contaminated bysewage.
Only seven of the total were occupational healthstudies, the rest being studies about the health impactson nearby communities.
5 Summarising the evidence
The types of studies carried out included case controlstudies, cross sectional studies, cohort studies, clusteranalyses, correlation studies and descriptive surveys.Results were inconsistent, with some showingassociations between landfill and various health impactswhile other studies found no associations. In the largestreview, of 41 single site studies and 10 multisite studies,correlations were found for some health outcomes insome of the studies but not in all (Vrijheid 2000).Authors who make definite statements that their studyreveals real excess risks are frequently challenged (Staff1998, von Mühlendahl 1999, Greenacre et al 2000). Allof the primary studies are hypothesis-generating studiesrather than hypothesis-testing studies.
5.2.2 JudgementIn reviews, discussion papers, conferences andconsensus meetings, many attempts have been made todetermine whether the findings indicate real risksassociated with exposure to landfill sites. There isgeneral agreement with the cautious position taken at ameeting convened by the WHO Regional Office forEurope in 1998 which concluded:
"Many of the studies detected an increased risk ofthe studied diseases and symptoms in populationsliving close to the landfills. However, the evidencesupporting the causality of the association isinconsistent and inconclusive. Probably the strongestsuggestion for causality was generated by studies onreproductive outcomes, such as reduced birth weightor some birth defects. However, all studies lackeddirect exposure assessment, and the limited samplesize of most studies makes a more specific analysisimpossible. � Considering all the uncertainties, themeeting concluded that the present data do add to asuspicion that population exposure to emissions fromhazardous wastes may pose a risk to populationhealth. The present studies are not powerful enoughto indicate which of the characteristics of the veryinhomogeneous group of landfills that are included inthe studies might be responsible for the observedsmall increase in the risk." (WHO meeting 1998)
Substantially similar conclusions were reached byother authors of discussion papers or consensusdocuments (Rushbrook 1990, National Research Council1991, Morris 1995, Kipen 1996, Miller 1996, Johnson1997 for the US Agency for Toxic Substances andDisease Registry, IEH 1999, Vrijheid 2000).
Overall judgementExposure to landfill and any health outcomes �insufficient.
01elbaT seidutsyramirpnidetagitsevnisemoctuohtlaeH:setisllifdnalfo
emoctuohtlaeH forebmuNgniknird
seidutsretaw
forebmuNllifdnalseiduts
/semoctuoevitcudorpeRnostceffelatnempoleved
nerdlihc
9 22
recnaC 7 22
smotpmyS 1 72
stcapmilaicosohcysP 1 81
srekramoiB 1 21
ton-smelborphtlaeHtcartsbanideificeps
5 9
ytilatroM 1 4
gninosiop/seirujnI 0 2
latoT 32 101 *
.tcapmihtlaehenonahteromtuobaeraseidutsemoS*
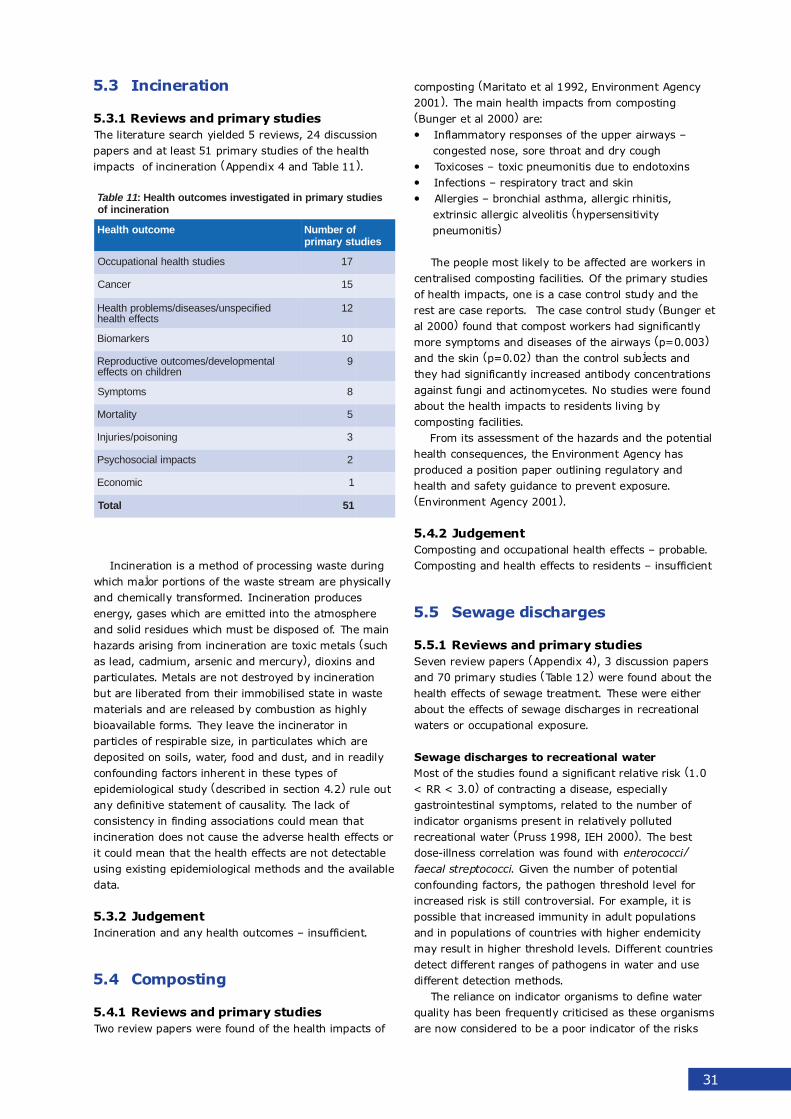
31
5.3 Incineration
5.3.1 Reviews and primary studiesThe literature search yielded 5 reviews, 24 discussionpapers and at least 51 primary studies of the healthimpacts of incineration (Appendix 4 and Table 11).
Incineration is a method of processing waste duringwhich major portions of the waste stream are physicallyand chemically transformed. Incineration producesenergy, gases which are emitted into the atmosphereand solid residues which must be disposed of. The mainhazards arising from incineration are toxic metals (suchas lead, cadmium, arsenic and mercury), dioxins andparticulates. Metals are not destroyed by incinerationbut are liberated from their immobilised state in wastematerials and are released by combustion as highlybioavailable forms. They leave the incinerator inparticles of respirable size, in particulates which aredeposited on soils, water, food and dust, and in readilyconfounding factors inherent in these types ofepidemiological study (described in section 4.2) rule outany definitive statement of causality. The lack ofconsistency in finding associations could mean thatincineration does not cause the adverse health effects orit could mean that the health effects are not detectableusing existing epidemiological methods and the availabledata.
5.3.2 JudgementIncineration and any health outcomes � insufficient.
5.4 Composting
5.4.1 Reviews and primary studiesTwo review papers were found of the health impacts of
composting (Maritato et al 1992, Environment Agency2001). The main health impacts from composting(Bunger et al 2000) are:� Inflammatory responses of the upper airways �
congested nose, sore throat and dry cough� Toxicoses � toxic pneumonitis due to endotoxins� Infections � respiratory tract and skin� Allergies � bronchial asthma, allergic rhinitis,
extrinsic allergic alveolitis (hypersensitivitypneumonitis)
The people most likely to be affected are workers incentralised composting facilities. Of the primary studiesof health impacts, one is a case control study and therest are case reports. The case control study (Bunger etal 2000) found that compost workers had significantlymore symptoms and diseases of the airways (p=0.003)and the skin (p=0.02) than the control subjects andthey had significantly increased antibody concentrationsagainst fungi and actinomycetes. No studies were foundabout the health impacts to residents living bycomposting facilities.
From its assessment of the hazards and the potentialhealth consequences, the Environment Agency hasproduced a position paper outlining regulatory andhealth and safety guidance to prevent exposure.(Environment Agency 2001).
5.4.2 JudgementComposting and occupational health effects � probable.Composting and health effects to residents � insufficient
5.5 Sewage discharges
5.5.1 Reviews and primary studiesSeven review papers (Appendix 4), 3 discussion papersand 70 primary studies (Table 12) were found about thehealth effects of sewage treatment. These were eitherabout the effects of sewage discharges in recreationalwaters or occupational exposure.
Sewage discharges to recreational waterMost of the studies found a significant relative risk (1.0< RR < 3.0) of contracting a disease, especiallygastrointestinal symptoms, related to the number ofindicator organisms present in relatively pollutedrecreational water (Pruss 1998, IEH 2000). The bestdose-illness correlation was found with enterococci/faecal streptococci. Given the number of potentialconfounding factors, the pathogen threshold level forincreased risk is still controversial. For example, it ispossible that increased immunity in adult populationsand in populations of countries with higher endemicitymay result in higher threshold levels. Different countriesdetect different ranges of pathogens in water and usedifferent detection methods.
The reliance on indicator organisms to define waterquality has been frequently criticised as these organismsare now considered to be a poor indicator of the risks
11elbaT seidutsyramirpnidetagitsevnisemoctuohtlaeH:noitarenicnifo
emoctuohtlaeH forebmuNseidutsyramirp
seidutshtlaehlanoitapuccO 71
recnaC 51
deificepsnu/sesaesid/smelborphtlaeHstceffehtlaeh
21
srekramoiB 01
latnempoleved/semoctuoevitcudorpeRnerdlihcnostceffe
9
smotpmyS 8
ytilatroM 5
gninosiop/seirujnI 3
stcapmilaicosohcysP 2
cimonocE 1
latoT 15

32
associated with viruses, protozoa and even bacteria. Ithas been shown (e.g. Deuter et al 1991) that there is apoor correlation between waterborne human viruses andfaecal coliforms in marine water. Many pathogenssurvive longer than faecal indicator bacteria. Infectivedoses of viruses and protozoa are still present after99.9% removal from raw sewage by secondarytreatment methods (Ashbolt 1996). Pathogensundetectable by conventional methods can remain viablein marine water. Also, pathogens may accumulate insediments and plankton and can be released andbecome infective in suitable conditions (e.g. Henricksonet al 2001). New molecular cell culture techniques arenow available for a more accurate detection of waterquality (e.g. Josephson et al 1991).
Occupational diseases of sewage treatmentworkersCompared with workers in other occupations, workers atsewage treatment plants suffered from moregastrointestinal tract symptoms, airways symptoms,fatigue and headache. No dose response relationshipwas found between cancer and exposure to agentscommonly found in sewage treatment plants.
5.5.2 Judgement
5.6 Soil amendments
5.6.1 Reviews and policy studies
As wastewater irrigation is banned in the UK, the onlysoil amendment discussed here is landspreading ofsewage sludge.
A total of 43 documents were found about the healthimpacts of landspreading sewage sludge. Ninedocuments published since 1990 were reviews ordiscussion papers about the health hazards from sewagesludge. There were 21 primary studies about healthhazards and one primary study of the health impacts.The latter was about the effects of Gram-negativebacteria on the health of workers at wastewater sludgefacilities between 1979 and 1981 (Clark et al 1984).
A discussion paper (Health Canada 2000, Vol 2)described the risks to human health as minimalbecause:� pathogens have a short lifespan and their persistent
forms remain in the soil,� metals are not usually metabolised by soil
microorganisms and will persist in the soil,� most pollutants bind to soil components,� most organic compounds, i.e. dioxins, are broken
down by soil microorganisms,� most organic compounds do not migrate into surface
or ground waters because they adhere to soilcomponents,
� volatile organic compounds evaporate within 48hours of landspreading.
However, there is a lack of understanding of thepotential for transfer of toxic compounds to food andabout the degradability and persistence of some toxiccontaminants (Rogers 1996).
5.6.2 Judgement
Sewage sludge landspreading and health impacts �insufficient.
gnicnivnoC nignihtabdnasmotpmyslanitsetniortsaG.sretawlanoitaercerdetanimitnocegawes
elbaborP eugitaf,ehcadaeh,smelborptcartlanitsetniortsaGegawesnignikrowdnasmotpmyssyawriadna
stnalptnemtaert .
tneiciffusnI tnemtaertegawesnignikrowdnarecnaCseitilicaf
21elbaT seidutsyramirpnidetagitsevnisemoctuohtlaeH:segrahcsidegawesfo
emoctuohtlaeH forebmuNseidutsyramirp
deificepsnu/sesaesid/smelborphtlaeHstceffehtlaeh
44
seidutshtlaehlanoitapuccO 63
smotpmyS 42
nwonknU 4
ytilatroM 4
recnaC 3
gninosiop/seirujnI 2
stcapmilaicosohcysP 2
latnempoleved/semoctuoevitcudorpeRnerdlihcnostceffe
1
srekramoiB 0
cimonocE 0
latoT 76

33
5.7 Summary of judgements
An overall assessment of the evidence linking wastedisposal to an impact on health is shown in Table 13.
31elbaT stnemegdujfoyrammuS:
ecnedivE ksirdesaercnI
gnicnivnoC nignihtabdnasmotpmyslanitsetniortsaG.sretawlanoitaercerdetanimatnocegawes
elbaborP ,ehcadaeh,smelborptcartlanitsetniortsaGnignikrowdnasmotpmyssyawriadnaeugitaf
.stnalptnemtaertegawes
elbissoP desilartnecatagnikrowdnasmotpmyssyawriA.ytilicafgnitsopmoc
tneiciffusnI llifdnalraenecnediserdnasemoctuohtlaehynA.etis
llifdnalatagnikrowdnasemoctuohtlaehynA.etis
natagnikrowdnasemoctuohtlaehynA.rotarenicni
raenecnediserdnasemoctuohtlaehynA.rotarenicni
raenecnediserdnasemoctuohtlaehynA.ytilicafgnitsopmocdesilartnec
tnemtaertegawesnignikrowdnarecnaCseitilicaf
gnidaerpcsdnaldnasemoctuohtlaehynA.egdulsegawes
34
How can the epidemiological evidence be used in wastemanagement strategies and practice to protect publichealth?
6.1 National policy
In its Waste Strategy, the government has stated thatthe protection of human health is one of the importantobjectives of its waste management strategy (DETR2001): "We have long sought to protect the localenvironment and human health from the adverse effectsof waste management through a comprehensive systemof planning and pollution control legislation" (Section 3.5DETR 2001). A key feature of the Framework Directiveon Waste, 91/156/EEC, and the licensing system is "theobjective of ensuring that waste is recovered ordisposed of without endangering human health andwithout using processes or methods which could harmthe environment" (Waste Strategy 2000 Section 3.36DETR 2001).
The government issues guidance on how localauthorities and the Environment Agency are toimplement its policies. The Planning Policy GuidanceNote 10 (DETR 1999) sets out the national planningframework for waste and states that the Governmentwishes to see decisions based on four key principles �the Best Practicable Environmental Option, regional selfsufficiency, proximity principle, and the waste hierarchy.
6.2 Decision making in the face ofuncertainty
6.2.1 Uncertainty"The major problem in marrying policy and thescience which informs it is that the timescales of thetwo never match. This is true almost by definition,since if there were sufficient science in place, thenthe problem of characterizing the scientific essentialsof an issue is solved and policy formulation is thendetermined by consideration of other issues such asthe social, economic and political aspects of theproblem. Unfortunately, life is generally not thissimple, and one often finds that there is insufficientscientific information compared with what ideallywould be required." (Maynard & Howard 2000)
This overview of the scientific evidence exposes ahigh degree of uncertainty about the impact of wastemanagement operations on health, which may or maynot ever be resolved by further research. Despite theimpressive amount of research and the high quality ofmany of the studies, the state of the evidence is suchthat, with a few exceptions (see section 5.7), no certain
conclusions can be drawn.
6.2.2 Interpretations of the evidenceIn the meantime, waste management decisions have tobe made and the health of the public has to beprotected. In theory, decision making should be basedon a rigorous assessment of the scientific evidence. Inreality, waste management decision making takes placein a highly charged political environment, with differentinterest groups driven by conflicting values and beliefsystems as well as by contrary interpretations of thesame scientific evidence.
Decision makers have to proceed despite theuncertainty. The following case illustrates the dilemmasthey face:
Wrexham County Borough Council initially grantedShanks Waste Services permission to install anelectricity generating plant on its landfill site in 1994but refused planning permission in 1999 when thecompany applied to change details of its plan. In theintervening years, local residents had raised concernsabout possible health risks. The Council's planningcommittee was persuaded that there was not enoughindependent scientific evidence to show that fearsabout health risks were unfounded. Shanks appealedand at the subsequent inquiry, the Inspector over-ruled the planning committee's decision and grantedthe company permission to install the plant. TheInspector said that the Council should base theirdecisions on objective assessments, not onunfounded fears. As the emissions from theelectricity generating plant would not exceed NationalAir Quality Standards and World Health Organisationlevels, he could find no evidence to justify concernsabout health impacts (Described in NSCA 2001). Inother inquiries, fear of adverse health effects hasbeen allowed as a material consideration but theweight given to it has varied. (Brian Cook, personalcommunication, September 2001.)
Both of the decisions in this case were based onreasonable interpretations of the same scientificevidence. Neither decision was more objective nor morecorrect than the other. Valid arguments could be madein defence of both the Council's decision and theInspector's. Depending on the interpretation, differentcourses of action will result.
Informed debate has polarised into two plausiblepositions:
Position oneThere is no evidence of significant harm to humanhealth from waste management operations. No humanactivity is completely safe but compared to other
6 Protecting the health of the public
35
environmental health hazards (e.g. vehicle traffic) orcompared to other causes of ill health (e.g, poor diet,diseases), waste management operations are not amajor public health concern.
An example of this position is taken by The NationalSociety for Clean Air and Environmental Protection in itsrecent report on incineration. It concludes, "While wecannot discount effects resulting from the smallquantities of some pollutants emitted by MSW (MunicipalSolid Waste) incinerators where impacts may occur atbackground levels (e.g. dioxins) or where currentstandards (limit values) may be exceeded (e.g. nitrogendioxide) the large number of other important sources ofsuch pollutants suggest that these deserve a greateremphasis on regulatory control." (Farmer & Hjerp 2001)
Position twoLack of evidence is not the same as evidence of lack ofhealth impacts. Waste management methods may havea major impact on health but the limitations of theresearch make it impossible to determine whether this isthe case.
An example of this position comes from theGreenpeace incineration report. It concludes, "With thelimited data available, it is, therefore, impossible topredict health effects of incinerators, either new orupdated installations� There is an urgent need for thecomplete phase out of incineration and theimplementation of sound waste management policiesbased on waste prevention, re-use and recycling."(Allsopp et al 2001)
6.2.3 Judgements about riskDisagreement about the management of a potentiallyrisky activity like incineration arises not only because ofdifferent interpretations of scientific evidence butbecause of the different judgements people make abouthow risky they believe the activity to be. Individuals aswell as regulatory bodies try to avoid or control activitiesthey judge to be too risky and ignore or tolerate others.Conflict occurs when people form different judgementsabout the riskiness of the activity. Disagreements aboutrisk are inevitable because there is no way to define riskthat does not include values, beliefs and assumptions �especially when information on which to base thejudgement is scarce.
Where there is uncertainty, judgements about riskare based on assumptions and mental strategies thathelp decision making and on qualitative aspects inherentin a hazard. As well as the likelihood of harm, peopleconsider whether incurring the risk is voluntary, hascatastrophic consequences, is unknown and unfamiliar,and is new to society. Judgements about risk are alsoinfluenced by individuals' views of the world and thekind of society they want. A summary of currentthinking about risk perception can be found in Saffron(1993).
When scientists make judgements about risk, theprocess is described as risk assessment. Riskassessment is perceived as an objective exercise and is
expressed in terms of probabilities � the likelihood thatsomething bad will happen. If the probability is low,then they perceive the risk to be low; a high probabilitydescribes a high risk. This one-dimensional view of riskenables scientists to consider the risks of eating 40tablespoons of peanut butter in a year, drinking 30 cansof diet soda in a year and cycling ten miles in a year asequivalent because each increases an individual's chanceof death by one in a million. The assumptions, valuesand lack of actual data in risk assessment are rarelymade explicit, contributing to an impression of scientificvalidity. An example of a fact-free, assumption-implicitrisk assessment is given by Hens (Hens 2000) for anorganic chemical that accumulates in the body. The riskassessment takes account of the maximal concentrationof the chemical in the plume using a terrain dispersionmodel to estimate ground level concentrations. Atheoretical amount of the chemical which an adult mightexpect to assimilate is then calculated. The assumptionshidden in this kind of risk assessment are that thehypothetical adult is free from any pollutant in theirbody and will not be exposed to chemicals or otherhazards from other sources. This type of riskassessment is unlikely to lead to emission standards oracceptable daily intakes that would protect humanhealth. Hens likens risk assessment to a "captured spy �if you torture it enough, it will tell you anything youwant to know."
When members of the public make judgements aboutrisk, the process is described as risk perception.Opposition to an incinerator, for example, may becondemned as irrational and ignorant but in fact,scientists make use of the same mental strategies,known as heuristics, as the non-scientifically trainedpublic. The commonly used heuristics are:� Availability � overestimate frequency of rare,
unusual, memorable causes of death (e.g. accidents)and underestimate more common ones (e.g.diseases).
� Overconfidence � unwarranted certainty in thecorrectness of their estimates.
� Trustworthiness of public institutions and officials �recognition that human errors, organisational failingsand patterns of management can affect real lifeoperation of technological systems.
� Framing effect � attitudes to risk influenced by theway choices are presented, e.g. a half empty glassseems worse than one that is half full.
� Optimistic bias � impression that the individual isless vulnerable and more knowledgeable about ahazard than other people.
� Dose response � belief that chemicals are either safeor dangerous.
When there is little knowledge and much uncertainty,experts are as prone to the use of these heuristics asthe public. Scientists may underestimate risks oftechnologies they are familiar with, may suffer fromoverconfidence in their judgements and may beinsensitive to wrong assumptions in their work. They are
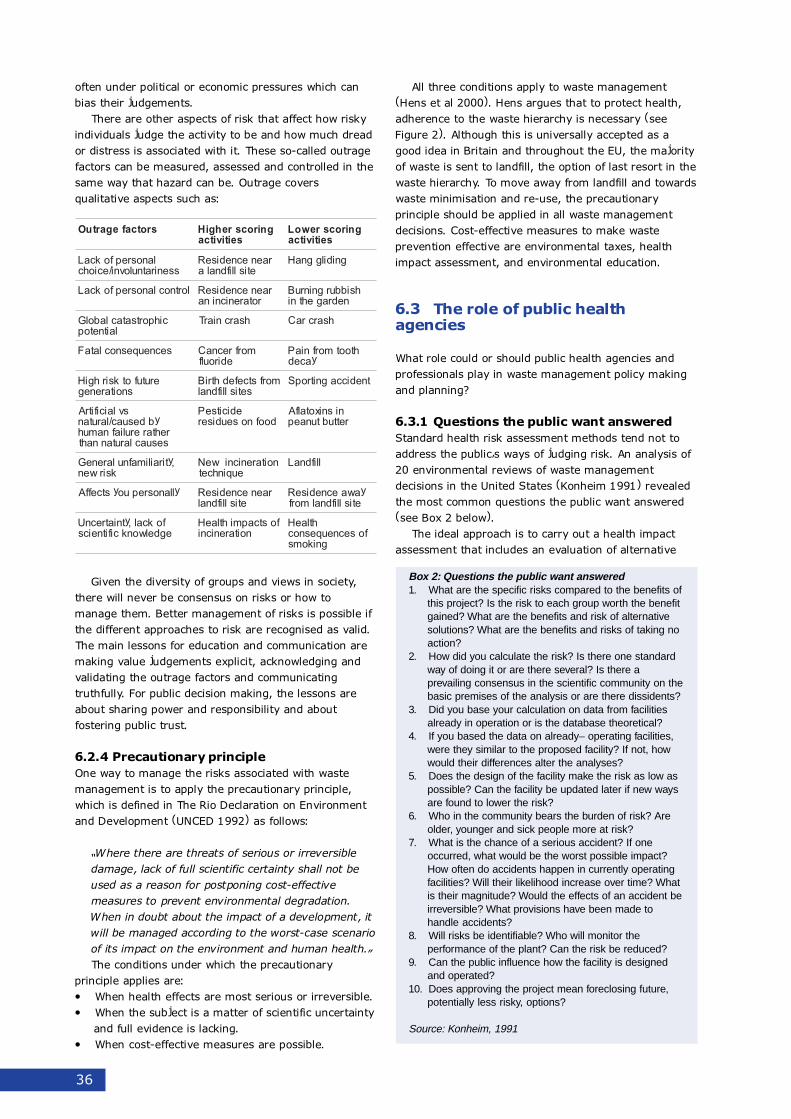
36
Box 2: Questions the public want answered1. What are the specific risks compared to the benefits of
this project? Is the risk to each group worth the benefitgained? What are the benefits and risk of alternativesolutions? What are the benefits and risks of taking noaction?
2. How did you calculate the risk? Is there one standardway of doing it or are there several? Is there aprevailing consensus in the scientific community on thebasic premises of the analysis or are there dissidents?
3. Did you base your calculation on data from facilitiesalready in operation or is the database theoretical?
4. If you based the data on already– operating facilities,were they similar to the proposed facility? If not, howwould their differences alter the analyses?
5. Does the design of the facility make the risk as low aspossible? Can the facility be updated later if new waysare found to lower the risk?
6. Who in the community bears the burden of risk? Areolder, younger and sick people more at risk?
7. What is the chance of a serious accident? If oneoccurred, what would be the worst possible impact?How often do accidents happen in currently operatingfacilities? Will their likelihood increase over time? Whatis their magnitude? Would the effects of an accident beirreversible? What provisions have been made tohandle accidents?
8. Will risks be identifiable? Who will monitor theperformance of the plant? Can the risk be reduced?
9. Can the public influence how the facility is designedand operated?
10. Does approving the project mean foreclosing future,potentially less risky, options?
Source: Konheim, 1991
often under political or economic pressures which canbias their judgements.
There are other aspects of risk that affect how riskyindividuals judge the activity to be and how much dreador distress is associated with it. These so-called outragefactors can be measured, assessed and controlled in thesame way that hazard can be. Outrage coversqualitative aspects such as:
Given the diversity of groups and views in society,there will never be consensus on risks or how tomanage them. Better management of risks is possible ifthe different approaches to risk are recognised as valid.The main lessons for education and communication aremaking value judgements explicit, acknowledging andvalidating the outrage factors and communicatingtruthfully. For public decision making, the lessons areabout sharing power and responsibility and aboutfostering public trust.
6.2.4 Precautionary principleOne way to manage the risks associated with wastemanagement is to apply the precautionary principle,which is defined in The Rio Declaration on Environmentand Development (UNCED 1992) as follows:
�Where there are threats of serious or irreversibledamage, lack of full scientific certainty shall not beused as a reason for postponing cost-effectivemeasures to prevent environmental degradation.When in doubt about the impact of a development, itwill be managed according to the worst-case scenarioof its impact on the environment and human health.�The conditions under which the precautionary
principle applies are:� When health effects are most serious or irreversible.� When the subject is a matter of scientific uncertainty
and full evidence is lacking.� When cost-effective measures are possible.
All three conditions apply to waste management(Hens et al 2000). Hens argues that to protect health,adherence to the waste hierarchy is necessary (seeFigure 2). Although this is universally accepted as agood idea in Britain and throughout the EU, the majorityof waste is sent to landfill, the option of last resort in thewaste hierarchy. To move away from landfill and towardswaste minimisation and re-use, the precautionaryprinciple should be applied in all waste managementdecisions. Cost-effective measures to make wasteprevention effective are environmental taxes, healthimpact assessment, and environmental education.
6.3 The role of public healthagencies
What role could or should public health agencies andprofessionals play in waste management policy makingand planning?
6.3.1 Questions the public want answeredStandard health risk assessment methods tend not toaddress the public�s ways of judging risk. An analysis of20 environmental reviews of waste managementdecisions in the United States (Konheim 1991) revealedthe most common questions the public want answered(see Box 2 below).
The ideal approach is to carry out a health impactassessment that includes an evaluation of alternative
srotcafegartuO gnirocsrehgiHseitivitca
gnirocsrewoLseitivitca
lanosrepfokcaLsseniratnulovni/eciohc
raenecnediseRetisllifdnala
gnidilggnaH
lortnoclanosrepfokcaL raenecnediseRrotarenicnina
hsibburgninruBnedragehtni
cihportsataclabolGlaitnetop
hsarcniarT hsarcraC
secneuqesnoclataF morfrecnaCediroulf
htootmorfniaPyaced
erutufotksirhgiHsnoitareneg
morfstcefedhtriBsetisllifdnal
tnediccagnitropS
svlaicifitrAybdesuac/larutan
rehtareruliafnamuhsesuaclarutannaht
edicitsePdoofnoseudiser
nisnixotalfArettubtunaep
,ytirailimafnulareneGksirwen
noitarenicniweNeuqinhcet
llifdnaL
yllanosrepuoystceffA raenecnediseRetisllifdnal
yawaecnediseRetisllifdnalmorf
fokcal,ytniatrecnUegdelwonkcifitneics
fostcapmihtlaeHnoitarenicni
htlaeHfosecneuqesnoc
gnikoms

37
risks and courses of action, the potential for catastrophicincidents and ways for people affected to control therisks in a meaningful way.
6.3.2 IPPC applicationsSince new regulations came out in 2000, healthauthorities (now devolved to primary care trusts) arestatutory consultees in the IPPC (Integrated PollutionPrevention Control) application process and have beenasked to comment on the health impacts of plans topermit new waste disposal processes. It is not yet clearwhere this responsibility will rest with the abolition ofhealth authorities; CCDCs (consultants in communicabledisease control) may be asked to lead, but are notusually trained in environmental epidemiology and maynot feel prepared to comment.
CIRS, the Chemical Incident Response Service, ispreparing a toolkit for use by CCDCs when they areconsulted about an IPPC application. The toolkit is in theform of a database plus navigation document. Itprovides a series of questions CCDCs can use to checkwhether the applicant has taken health impacts intoaccount in their application. The questions cover sitecharacterisation, monitoring systems, the method usedby the applicant to determine the impact on the localpopulation, modelling data, chemicals on site, emissionsto the atmosphere, presence of action plans, and thepossibilities of noise and odour pollution as well ascompleteness of the application and information aboutthe type of permit. The toolkit is in the pilot stage andshould be available by the end of 2002. For moreinformation, contact Graham Robertson, CIRS, [email protected]
The official Department of Health IPPC contact isProfessor Rod Griffiths, Regional Director of PublicHealth for the West Midlands Region. A checklistguidance document for CCDCs has been produced onhow to respond to IPPC applications that come their way(Kibble 2001).
6.3.3 Local authority waste strategies andwaste local plansLocal authorities carry out extensive consultationexercises in the formation of their plans. Theconsultation process is laid down by statute and theviews of interested parties are sought. Comments fromhealth authorities are welcomed but there is nostatutory obligation to seek out the views of publichealth professionals. Nor is there a statutoryrequirement to carry out a formal health impactassessment when preparing waste local plans andstructure plans. The plans set out general policies andprinciples which guide policy making. To assess bestpracticable environmental option, key criteria are listedincluding an environmental statement and life cycleanalysis. Under Environmental constraints and issues,policies are laid out for nature conservation, landscape,archaeology and the historic environment, agriculture,and water. Health is not specifically mentioned. It isassumed that health impacts are adequately covered in
the existing environmental impact assessment. Giventhe uncertainties in the epidemiological data, it may bethe case that the current risk assessment methodsbased on emission standards are as accurate as can beachieved.
6.3.4 Regional waste strategyThe Regional Assembly for the South West has begunthe process of producing a regional waste strategy andwelcomes public health input (Joe Field and Brian Cook,personal communication).
6.3.5 Health impact assessmentThe White Paper Saving Lives, Our Healthier Nationstates that there is a need for health impact assessmentof policies, plans and projects at national, local andregional level. The Government has made acommitment to consider health in all aspects of policymaking, not just in relation to the health services but toany policy which affects people�s well being and qualityof life. The Department of Health has explained HIA as:
A prospective assessment of a proposed new policyto identify its likely impacts on health. This aims toprovide assessment of policy options and their differingpotential health benefits and disbenefits in order tomaximise health outcomes;
orA retrospective assessment or evaluation of a policy
following implementation. This aims to monitor how apolicy is affecting or has affected health. The results ofsuch a process can then be used to fine tune the futuredirection of policy implementation. (Department ofHealth 1999)
The Welsh Assembly has produced guidelines onchoosing formats for HIA (The National Assembly forWales 1999, p28). They stress that the HIA methodswhich are appropriate for assessing projects are likely tobe different from methods for assessing a policy. Whenchoosing a method, decision makers should be guidedby the need to make it add value to the decision makingprocess. A HIA must do more than point out that a newdevelopment may create noise and air pollution.Methods should be chosen which provide information onthe size and nature of the health impact while, at thesame time, not ignoring those impacts which areimpossible to quantify.
Although there is no standard methodology forcarrying out an HIA, there is considerable experiencewith the process in other countries and within the UK.The following procedures are from the MerseysideGuidelines:
1. Screening � procedure whereby policies are selectedfor assessment. The idea is to see if the project or policyis likely to have significant impacts on health and if it isworth subjecting it to a HIA. A checklist from the BritishColumbia Health Impact Assessment Toolkit can befound in Developing Health Impact Assessment in Wales

38
(The National Assembly for Wales 1999 p19).
2. Scoping � a multidisciplinary steering group isestablished to agree the Terms of Reference. Steeringgroup should include commissioners of HIA, assessors,policy proponents, affected communities and otherstakeholders.
3. Conducting the risk assessment � characterising thenature and magnitude of the harmful and beneficialfactors, how many and which people will be affected bythem and how they will be affected.
A. Policy analysisB. Profiling of affected communitiesC. Interview stakeholders and key informantsD. Identify health determinantsE. Collect evidence from other reports and assess
evidenceF. Establish priority impactsG. Recommend and justify options for action
4. Appraise the assessment
5. Decision making
6. Monitoring and evaluation
The use of an integrated environmental and healthimpact assessment is described by Fehr (Fehr 1999) forthe planned extension of a non-toxic waste disposal sitein Lower Saxony. A ten-step environmental healthimpact assessment model was applied and its useassessed. Fehr argues that such an assessment shouldbe used more often as a tool for health protection andpromotion but that a consensus is needed on theconcept and further development of the tool.
A HIA is an iterative and an interactive process,based on principles of participation, equity, democracy,and a broad definition of health. The aim is toincorporate a public health perspective into the wasteplanning process. This requires intersectoralcollaboration. If policy makers from local authoritieswere involved from the beginning of the HIA process,they would have a sense of ownership and interest inthe process which would make them more likely toconsider health impacts when they prepare their WasteLocal Plans and Waste Strategies. If public healthofficials were involved in the waste planning processfrom its beginning, they would have more impact than ifthey were commenting on an already prepared andaccepted plan.

39
7 Recommendations
In his review of epidemiological studies on the healtheffects of hazardous wastes, Miller (Miller 1996) pointsout that we ��face a stark choice. We can largelydepend on analogy, as many have done in the past. Thisinvolves acknowledging that evidence exists of adverseeffects � using the large body of data available on thetoxicity and carcinogenicity of substances identified inhazardous waste sites, relating this knowledge to thatknown on human exposure, inferring a problem, andfinally acting. This basis for risk assessment may berefined a little by epidemiology, but we must recognisethat the majority of studies from the past � published orremaining unpublished � are inconclusive. Alternatively,we can refine our methodology and make valiant effortsto increase the knowledge base.�
Recommendations and research programmes toincrease the epidemiological knowledge base are madeby many agencies, including the Department of Health(Environmental Chemical Unit 1999), the Department ofthe Environment (DOE 1994), the Environment Agency'sWaste Regulation and Management Research
Programme and the World Health Organisation (WHOEuropean Centre for Environment and Health 2000,WHO Meeting 1998). Recommendations focus on:� refining exposure assessment and modelling;� improving health outcome datasets, including GIS,
geographical information systems;� determining the teratogenicity of substances
emanating from waste disposal sites.
This report acknowledges the importance ofincreasing and strengthening the evidence base butrecognises the inevitable uncertainty of epidemiologicalevidence in this field. It recognises also the pressingneed to make public policy decisions when the evidenceremains inconclusive. This report recommends thedevelopment of democratic, health-protective decisionmaking techniques which incorporate theepidemiological evidence base as well as public valuesand concerns.

40
8 Conclusions
The data collected about waste are not detailed enoughto make meaningful assessments of potential healthimpacts that might arise from waste managementpractices. The data do not include detailed informationabout the composition of the waste collected nor of off-site emissions from waste management operations.Accurate exposure assessments are not possible withoutsuch data.
The nature of existing epidemiological research inthis area is such that most studies are useful forgenerating hypotheses but are unable to test thehypotheses or to provide convincing evidence of anassociation between exposure and a health impact.
For most waste management methods, the evidenceis insufficient to claim that adverse health outcomes willresult. The exception is the convincing evidence thatbathing in sewage contaminated recreational watersincreases the risk of gastrointestinal symptoms, evenwhen the water meets present guideline levels of faecalcoliforms.
Implementation of the current Waste Hierarchy andthe Precautionary Principle through the adoption of anintegrated waste management strategy at national,regional and local level will be the most effective way toreduce the health risks from waste managementprocedures.
41
9 References
Albert RE. Health risks of concern. In: Andelman JB; Underhill DW. Health effects from hazardous waste sites.Chelsea, Michigan, USA: Lewis Publishers; 1987. pp. 143�7.
Alkan K. The fate of enteric bacteria in relation to suspended particles in sea water. JCIWEM 1999;13.Allsopp M; Costner P; Johnston P. Incineration and human health � state of knowledge of the impacts of waste
incinerators on human health. UK: Greenpeace; 2001.Arndt V, Vine MF, Weigle K, Environmental Chemical Exposures and Risk of Herpes Zoster. Environmental Health
Perspectives 1999;107(10):835�41.Arvanitidou M, Constantinidis TC, Doutsos J, Mandraveli K, Katsouyannopoulos V. Occupational hepatitis B virus
infection in sewage workers. Med Lav 1998;89(5):437�44.Ashbolt NJ. Human health risk from micro-organisms in the Australian marine environment. In: Zann LP; Sutton DC,
eds. The State of the Marine Environment Report for Australia. Technical Annex 2 � Pollution. Collingwood,Australia: Ocean Rescue 2000, Department of the Environment, Sport and Territories, Canberra, CSIROPublishing;1996.pp.31�40.
ATSDR Agency for Toxic Substances and Disease Registry. Study of symptom and disease prevalence, CaldwellSystems, Inc. Hazardous waste incinerator, Caldwell County, North Carolina. Final Report ed. Atlanta, GA,USA: US Department of Health and Human Services, Agency for Toxic Substances and Disease Registry; 1993.Report No. ATSDR/HS�93/29.
Baker EL, Landrigan PJ, Glueck ZJ, Zack MM, Liddle JA, Burse VW, Housworth WJ, Needham LL. Metabolicconsequences of exposure to polychlorinated biphyenyls PCB in sewage sludge. Am J Epidemiol1980;112:553-63.
Balarajan R, Soni Raleigh V, Yuen P, Wheeler D, Machin D, Cartwright R. Health risks associated with bathing in seawater. BMJ 1991;303(6815):1444�5.
Barrell RA, Hunter PR, Nichols G. Microbiological standards for water and their relationship to health risk.Communicable Disease & Public Health 2000;3(1):8�13.
Beccaloni E, Borrello P, Musmeci L, Stacul E. Arsenic and heavy metals in leachate from a real landfill and alaboratory landfill. Annali Di Chimica 2000;90(11�12):629�36.
BMA British Medical Association. Hazardous waste and human health, Oxford; Oxford University Press, 1991.BMA British M. A. Health and environmental impact assessment � an integrated approach. London: Earthscan
Publications Ltd; 1998.Bohnel H, Lube K. Clostridium botulinum and bio-compost. A contribution to the analysis of potential health hazards
caused by bio-waste recycling. Zentralbl Veterinarmed [B] 2000;47(10):785�95.Bosco ME, Cunha II, Saito RT. Radium migration through clay liners at waste disposal sites. Sci Total Environ
2001;266(1�3):259�64.Bridges O, Bridges J, Potter J. A generic comparison of the airborne risks to human health from landfill and
incinerator disposal of municipal solid waste. Environmentalist 2000;20(4):325�34.Brown M. Laying waste: the poisoning of America by toxic chemicals. New York: Pantheon Books; 1980.Bresnitz EA, Roseman J, Becker D, Gracely E. Morbidity among municipal waste incinerator workers. Am J Ind Med
1992;22(3):363�78.Buffler PA, Crane M, Key MM. Possibilities of detecting health effects by studies of populations exposed to chemicals
from waste disposal sites. Environmental Health Perspectives 1985 Oct;62:423�56.Bunger J, Antlauf-Lammers M, Schulz TG, Westphal GA, Muller MM, Ruhnau P, Hallier E. Health complaints and
immunological markers of exposure to bioaerosols among biowaste collectors and compost workers.Occupational & Environmental Medicine 2000;57(7):458�64.
Callender TJ, Ristovv M, Guerra M, Ruttenberg R. Social and economic impact of neurotoxicity in hazardous wasteworkers in Lenoir, North Carolina. Environ Res 1997;73(1�2):166�74.
Cantor KP. Drinking water and cancer. Cancer Causes & Control 1997;8(3):292�308Carpenter DO, Arcaro KF, Bush B, Niemi WD, Shaokun Pang, Vakharia DD. Human health and chemical mixtures: an
overview. Environmental Health Perspectives 1998;106,Supp 5:1263�1270.Carruth AK, Gilbert K, Lewis B. Environmental health hazards: the impact on a southern community. Public Health
Nurs 1997 Oct;14(5):259�67.Clark CS, Bjornson HS, Schwartz-Fulton J, Holland JW, Gartside PS. Biological health risks associated with the
composting of wastewater treatment plant sludge. Journal of the Water Pollution Control Federation.1984;56(12):1269�76.
Colborn T; Myers JP; Dumanoski D. Our stolen future � are we threatening our fertility, intelligence and survival � ascientific detective story. London: Abacus, 1997.
42
Collins CH, Kennedy DA. The microbiological hazards of municipal and clinical wastes. J Appl Bacteriol 1992Jul;73(1):1�6.
CRD, Centre for Research and Dissemination. Undertaking systematic reviews of research on effectiveness � CRD'sguidance for those carrying out or commissioning reviews. 2nd edition ed. York, Yorkshire: CRD, Centre forResearch and Dissemination; 2001 Mar. CRD Report Number 4.
Croen LA, Shaw GM, Sanbonmatsu L, Selvin S, Buffler PA. Maternal residential proximity to hazardous waste sitesand risk for selected congenital malformations. Epidemiology 1997;8(4):347�54.
Dayal H, Gupta S, Trieff N, Maierson D, Reich D. Symptom clusters in a community with chronic exposure tochemicals in two Superfund sites. Archives of Environmental Health 1995;50(2):108�11.
DEFRA. Implementation of Council Directive 1999/31/EC on the landfill of waste � second consultation paper andregulatory impact assessment. London: Department for Environment, Food and Rural Affairs; 2001 Aug.
Denison RA, Silbergeld EK. Risks of municipal solid waste incineration: an environmental perspective. Risk Anal1988;8(3):343�55.
Department of the Environment. Health effects from hazardous waste landfill sites. The technical aspects ofcontrolled waste management. London, Department of the Environment, Rpt no CSM/057/92, 1994,
Department of Health. Health impact assessment. Report of a methodological seminar. London: Department ofHealth; 1999.
Deportes I, Benoit Guyod JL, Zmirou D. Hazard to man and the environment posed by the use of urban wastecompost: a review. The Science of the Total Environment 172 (2�3) 197�22, 1995.
Desenclos JCA, Klontz KC, Wilder MH, Nainan OV, Mergolis HS, Gunn RA. A multi-state outbreak of hepatitis Acaused by the consumption of raw oysters. Am J Public Health 1991;81:1268�72.
DETR. Waste Strategy 2000 for England and Wales Part 1 and 2. Norwich: Department of the Environment, Tradeand the Regions; 2001.
DETR. Municipal waste management bulletin 1998/99. Department of the Environment, Transport and the RegionsDETR; 2000.
DETR. Planning Policy Guidance Note 10: Planning and Waste Management. Department of the Environment,Transport and the Regions DETR; 1999.
Deuter A, Cale P, Irving TE et al. Viruses in surface waters � occurrence and environmental control. Marlow, UK:Foundation for Water Research/WRc, 1991. Report No. FR 0213.
Dixon R; Humphreys L; Warhurst M. Hormone disrupting compounds. Edinburgh, Scotland: Friends of the EarthScotland;1996 Jun.
Dolk H, Busby A, Armstrong BG, Walls PH. Geographical variation in anophthalmia and microphthalmia in England,1988�94. BMJ 1998;317:905�10.
Dolk H, Vrijheid M, Armstrong B, Abramsky L, Bianchi F, Garne E, et al. Risk of congenital anomalies near hazardous-waste landfill sites in Europe: the EUROHAZCON study. Lancet 1998;352:423�7.
Dumontet S, Scopa A, Kerje S, Krovacek. The importance of pathogenic organisms in sewage and sewage sludge.Journal Of The Air & Waste Management Association 2001;51(6):848�60.
Edelstein M. Contaminated communities: the social and psychological impacts of residential toxic exposure. BoulderCO, USA: Westview Press; 1988.
Eduljee G. Assessing the risks of landfill activities, Harwell Waste Management Symposium � new developments inlandfill proceedings1992; Harwell, Didcot, Oxfordshire, UK. Oxfordshire, UK: AEA Environment and Energy;1992.
Eitzer BD, Iannucci-Berger WA, Mark G, Zito C. Fate of toxic compounds during composting. Bulletin ofEnvironmental Contamination & Toxicology 58(6)953�60, 1997.
Elliott P et al. Risk of adverse birth outcomes in populations living near landfill sites. BMJ 2001;323:363�8.ENDS. Fire at Dundee incinerator hits efforts to rebuild public confidence. Ends Report 2000;308:15�6.Environment Agency South West. A report on the state of the environment in the South West of England. Exeter,
Devon: Environment Agency, South West Region; 2001.Environment Agency. Agency position on composting and health effects. Environment Agency; 2001 Aug.Environment Agency. Health effects of composting � a study of three composting sites and review of past data. UK:
AEAT; 2001 Nov.Environment Agency. Strategic Waste Management Assessment SWMA. Environment Agency; 2000.Environmental Chemical Unit, Department of Health. Research programme on the impacts of health of landfill sites,
Number 928, Department of Health, 1999.Ewers U, Wittsiepe J, Schrey P, Exner M, Selenka F, Hofbauer M, Schmeer D, Holwitt L, Eck R. [Digoxin content in
blood lipids of children, athletes, sports ground attendants and residents after content with dioxin-containingsurface slag (kieselrot)]. Gesundheitswesen 1994 Jan;56(1):14�20.
Fan PL, Arenholt-Bindslev D, Schmalz G, Halbach S, Berendsen. Environmental issues in dentistry � mercury. FDICommission. Int Dent J.1997 Apr;47(2):105�9.
Fara GM, Collina D. Liquid hospital waste. Ann Ig 1989 Jan�1989 Apr 30;1(1�2):51�5.
43
Farmer A; Hjerp P. Municipal solid waste incineration: health effects and public communication. A report to theNational Society for Clean Air & Environmental Protection. Institute for European Environmental Policy (IEEP);2001 May.
Fattal B, Wax Y, Davies M, Shuval HI. Health risks associated with wastewater irrigation: an epidemiological study.Am J Public Health 1986;76(8):977�9.
Favata EA, Buckler G, Gochfeld M. Heat stress in hazardous waste workers: evaluation and prevention. Occup Med1990;5(1):79�91.
Fehr R. Environmental Health Impact Assessment: evaluation of a ten-step model. Epidemiology 1999;10(5):618�625.
Fielder HMP, C M Poon-King, S R Palmer, N Moss, G Coleman. Assessment of impact on health of residents living nearthe Nant-y-Gwyddon landfill site: retrospective analysis. BMJ 2000 Jan;320:19�23.
Gelberg KH. Health study of New York City department of sanitation landfill employees. Journal of Occupational &Environmental Medicine 1997;39(11):1103�10.
Gerba CP, Rose JB, Haas CN, Crabtree KD. Waterborne rotavirus: a risk assessment. Water Research,1996;30(12):2929�40.
Geschwind SA, Stolwijk JA, Bracken M, Fitzgerald E, Stark A, Olsen C, Melius J. Risk of congenital malformationsassociated with proximity to hazardous waste sites. Am J Epidemiol 1992 Jun 1;135(11):1197-207.
Gloucestershire County Council. Gloucestershire Waste Local Plan � 2002�2012 � Revised Deposit Draft. Gloucester:Gloucestershire County Council; 2001 Apr.
Goldberg MS, Siemiatyck J, DeWar R, Desy M, Riberdy H. Risks of developing cancer relative to living near amunicipal solid waste landfill site in Montreal, Quebec, Canada. Archives of Environmental Health1999;54(4):291�6.
Goldman LR, Paigen B, Magnant MM, Highland JH. Low birth weight, prematurity and birth defects in children livingnear the hazardous waste site, Love Canal. Haz Waste Haz Mat 1985;2(2):209�23.
Gray EJ, Peat JK, Mellis CM, Harrington J, Woolcock AJ. Asthma severity and morbidity in a population sample ofSydney school children: part I � prevalence and effect of air pollutants in coastal regions. Aust NZ J Med1994;24:168�75.
Greenacre J, Morgan M, Tucker D. Health effects of landfill sites: analyses require high quality data.[Letter]. BMJ2000 Jun 3;320(7248):1541.
Greenberg MD, Schneider D, Parry J. Brown fields, a regional incinerator and resident perception of neighborhoodquality. Risk Health Safety Environm 1995;6(3):241�59.
Greim H. Toxicological evaluation of emissions from modern municipal waste incinerators, Chemosphere 1990;20(3�4):317�31.
Grohmann GS, Greenberg HB, Welch BM, Murphy AM. Oyster-associated gastroenteritis in Australia: the detection ofNorwalk virus and its antibody by immune electron microscopy and radioimmunoassay. J Med Virol1980;6:11�9.
Hansen H, De Rosa CT, Pohl H, Fay M, Mumtaz MM. Public health challenges posed by chemical mixtures.Environmental Health Perspectives 1998 Dec;106(Suppl 6):1271�80.
Hawley. Assessment of Health Risk from exposure to contaminated soil. Risk Anal 1985;5(4).Health Canada. The Canadian Handbook on Health Impact Assessment. Canada: Office of Environmental Health
Assessment, Health Canada; 2000.Heath CW. Assessment of health risks at Love Canal. In: Andelman JB, Underhill DW. Health Effects from Hazardous
Waste Sites USA. Lewis Publishers; 1987.Heath, Nadel, Zack, Chen, Bender, Preston. Cytogenetic findings in persons living near the Love Canal. Journal of the
American Medical Association 1984;251:1437�40.Henrickson SE, Wong T, Allen P, Ford T, Epstein PR. Marine swimming-related illness: implications for monitoring and
environmental policy. Environmental Health Perspectives 2001 Jul;109(7):645�50.Hens L et al. Towards a precautionary approach for waste management supported by education and information
technology. In: Nicolopoulou-Stamati P et al. Health impacts of waste management policy, Kluwer AcademicPublisher, The Netherlands, 2000. p 283�310
Hertzman C, Hayes M, Singer J, Highland J. Upper Ottawa Street landfill site health study. Environmental HealthPerspectives 1987;75:173�95.
Hopwood DG & Guidott TL. Recall bias in exposed subjects following a toxic exposure incident. Archives ofEnvironmental Health, 1988;43(3):234�7.
Horowitz J, Stefanko M. Toxic waste: behavioral effects of an environmental stressor. Behav Med 1989Spring;15(1):23�8.
Hu SW, Shy CM. Health effects of waste incineration: a review of epidemiologic studies. Journal of the Air & WasteManagement Association 2001;51(7):1100�9.
IEH Seminar 1999 Jan 26; Institute for Environment and Health. www.doh.gov.uk/landh.htm: Department of Health;1999.
44
IEH. Environmental oestrogens � consequences to human health and wildlife. Leicester, UK: Institute forEnvironment and Health, University of Leicester, 1995.
IEH; written by Mugglestone MA; Stutt ED, et al. A review of the health effects of sea bathing water. Leicester, UK:Institute for Environment and Health; 2000(vol. Web Report W2).
Janerich DT, Burnett WS, Feck G, Hoff M, Nasca P, Polednak AP, Greenwald P, Vianna N. Cancer incidence in the LoveCanal area. Science 1981;212(4501):1404�7.
Johnson BL, DeRosa C. The toxicologic hazard of Superfund hazardous-waste sites. Rev Environ Health;12(4):235�51.
Johnson BL. Hazardous waste: human health effects. Toxicology & Industrial Health 1997 ;13(2�3):121�43.Johnson BL. A review of the effects of hazardous waste on reproductive health. American Journal of Obstetrics &
Gynaecology 1999;181(1):S12�6.Josephson KL, Pillai SD, Way J, Gerba CP, Pepper IL. Fecal coliforms in soil detected by polymerise chain reaction and
DNA�DNA hybridisations. Journal of the Soil Science Society of America 1992;55:1326�32.Kay D, Fleisher JM, Salmon RL, Jones F, Wyer MD, Godfree AF, Zelenauch-Jacquotte Z, Shore R, Predicting likelihood
of gastroenteritis from sea bathing: results from randomised exposure. Lancet 1994 Oct 1;344(8927):905�9.Kibble AJ; Saunders P. Integrated pollution, prevention and control � a practical guide for health authorities. Version
1 ed. Birmingham, West Midlands, UK: University of Birmingham, 2001 Aug.Kindzierski WB, Gabos S. Health effects associated with wastewater treatment, disposal and reuse. Water
Environment Research 1996;68(4):818�26.Kipen HM. Assessment of reproductive health effects of hazardous waste. Toxicology & Industrial Health
1996;12(2):211�24.Koenraad PMFJ, Rombouts FM, Notermans SHW. Epidemiological aspects of thermophilic campylobacter in water-
related environments: a review. Water Environment Research 1997;69(1):52�63.Kolata GB. Love Canal: false alarm caused by botched study. Science 1980;208:1239�42.Kramer MN, Kurup VP, Fink JN. Allergic bronchopulmonary aspergillosis from a contaminated dump site. American
Review of Respiratory Diseases 1989;140:1086�8.Konheim CS. Useful communication of risks to decision makers. Chapter 20. In: Hattemer-Frey HA & Travis C,
editors, Health effects of municipal waste incineration, CRC Press, Boston, 1991.Kuo W, Bhattacharya A, Succop P, Linz D. Postural stability assessment in sewer workers. J Occup Environ Med
1996;38:27�34.Laurent C, Lakhanisky T, Jadot P, Joris I, Ottogali M, Planard C, Bazzoni D, Foidart JM, Ros Y. Increased sister
chromatid exchange frequencies observed in a cohort of inhabitants of a village located at the boundary of anindustrial dumping ground: phase I. Cancer Epidemiology, Biomarkers & Prevention 1993 Jul�1993 Aug31;2(4):355�62.
Lee JT, Shy CM. Respiratory function as measured by peak expiratory flow rate and PM10: six communities study.Journal of Exposure Analysis & Environmental Epidemiology 1999 Jul-1999 Aug 31;9(4):293-9.
Leonardi G; Hankin C. A rapid review to inform the Mayor of London's municipal waste strategy. London: LondonHealth Commission; 2001 Sep.
Levine R, Chitwood DD. Public health investigations of hazardous organic chemical waste disposal in the UnitedStates. Environmental Health Perspectives 1985 Oct;62:415�22.
Lilienfield D, Stolley P. Foundations of epidemiology Oxford University Press 1994Linnemann CC Jr, Jaffa R, Gartside PS, Scarpino PV, Clark CS. Risk of infection associated with a wastewater spray
irrigation system used for farming. J Occup Med 1984 Jan;26(1):41�4.Lundholm M, Rylander R. Work-related symptoms among sewage workers. Br J Ind Med 1983;40:325�29.Mar T, Frost F, Tollestrup K. Physical injury risk versus risk from hazardous waste remediation: a case history.
Regulatory Toxicology & Pharmacology 1993 Apr;17(2 Pt 1):130�5.Maritato MC, Algeo ER, Keenan RE. Potential human health concerns from composting. BioCycle, 1992
Dec;33(12):70.Marsh G; Caplan R. Evaluating Health Effects of Exposure at Hazardous waste sites: a review of the state-of-the-art,
with recommendations for future research. Andelman JB; Underhill DW. Health Effects from Hazardous WasteSites. USA: Lewis Publishers; 1987.
Marshall EG, Gensburg LJ, Deres DA, Geary NS, Cayo MR. Maternal residential exposure to hazardous wastes andrisk of central nervous system and musculoskeletal birth defects. Archives of Environmental Health 1997 Nov�1997 Dec 31;52(6):416�25.
Marty MA. Hazardous combustion products from municipal waste incineration. Occup Med 1993 Jul�1993 Sep30;8(3):603�20.
Maynard RL, Howard CV. Particulate Matter: Properties and Effects upon Health. BIOS Scientific Publisher, Oxford,2000.
McCarron P, Harvey I, Brogan R, Peters TJ. Self reported health of people in an area contaminated by chromiumwaste: interview study. BMJ 2000 Jan 1;320(7226):11�5.

45
McNamee R, Dolk H. Does exposure to landfill waste harm the fetus? BMJ 2001;323:351�2.Melbostad E, Eduard W, Skogstad A, Sandven P, Lassen J, Sostrand P, Heldal K. Exposure to bacterial aerosols and
work-related symptoms in sewage workers. Am J Ind Med 1994;25:59�63.Miller AB. Review of extant community-based epidemiologic studies on health effects of hazardous wastes.
Toxicology & Industrial Health 1996;12(2):225�33.Melbostad E, Eduard W, Skogstad A, Sandven P, Lassen J, Sostrand P, Heldal K. Exposure to bacterial aerosols and
work-related symptoms in sewage workers. Am J Ind Med 1994;25:59�63.Morris RD. Drinking water and cancer. Environmental Health Perspectives 1995 Nov;103(Suppl 8):225�31.Murray R. Creating wealth from waste. London: Demos and Ecologika; 1999.National Research Council. Environmental Epidemiology. Vol 1: Public Health and Hazardous Wastes. Washington,
DC: USA, National Academy Press; 1991.National Research Council. Waste incineration and public health. Washington DC USA: National Academy Press;
2000.Nethercott JR, Holness DL Health status of a group of sewage treatment workers in Toronto, Canada. Am Ind Hyg
Assoc J 1988;49(7):346�50.Neutra R, Lipscomb J, Satin K, Shusterman D. Hypotheses to explain the higher symptom rates observed around
hazardous waste sites. Environmental Health Perspectives 1991;94:31�8.Nitschke L, Schussler W, Surface water pollution by herbicides from effluents of waste water treatment plants.
Chemosphere 1998;36(1):35�41.NSCA. The public acceptability of incineration. Brighton, UK: National Society for Clean Air and Environmental
Protection; 2001.Olver WM Jr. Aspergillus fumigatus problem. Compost Science and Utilization 1994;2(1):27�31.Ortiz NE, Smith GR. Landfill sites, botulism and gulls. Epidemiology & Infection 1994;112(2):385�91.Paigen B, Goldman LR, Highland JH, Magnant NM, Steegman AT. Prevalence of health problems in children living
near Love Canal. Haz Waset Haz Mat 1985;2:23�43.Paigen, Goldman, Magnant, Highland, Steegmann. Growth of children living near the hazardous waste site, Love
Canal. Hum Biol 1987;59(3):489�508.Paigen; Goldman. Lessons from Love Canal � the role of the public and the use of birth weight, growth and
indigenous wildlife to evaluate health risk. In: Andelman JB, Underhill DW. Health effects from hazardouswaste sites. USA: Lewis Publishers; 1987.
Philipp R, Pond K, Rees G, Research and the problems of litter and medical wastes on the UK coastline. Br J ClinPract 1997;51(3):164�8.
Picciano D. Pilot cytogenetic study of the residents living near Love Canal. Mammalian Chromosome Newsletter1980;21:86�93.
Pruss A. Review of epidemiological studies on health effects from exposure to recreational water. Int J Epidemiol1998 Feb;27(1):1�9.
Rapiti E, Sperati A, Fano V, Dell'Orco V, Forastiere F. Mortality among workers at municipal waste incinerators inRome: a retrospective cohort study. Am J Ind Med 1997;31(5):659�61.
Redfearn A et al. Assessment of health effects associated with landfills. IWM Scientific and Technical Review 2000Apr;14�28.
Redfearn A et al. Can landfills be good neighbours? IWM Scientific & Technical Review 2000 Apr;9�13.Reif JS, Tsongas TA, Anger WK, Mitchell J, Metzger L, Keefe TJ, Tessari JD, Amler R. Two-stage evaluation of
exposure to mercury and biomarkers of neurotoxicity at a hazardous waste site. Journal of Toxicology &Environmental Health 1993;40(2�3):413�22.
Richardson DB. Respiratory effects of chronic hydrogen sulfide exposure. Am J Ind Med 1995;28:99�108.Roberts D, Redfearn A, Dockerty J. Health effects of landfill sites: whether results are assertions or evidence is
unclear.[Letter]. BMJ 2000 Jun 3;320(7248):1541.Robinson C. Toxic emissions from landfill � extracts from Claire Robinson's evidence to the appeal inquiry. http://
www.gn.apc.org/pmhp/arrow/toxics.htm GreenNet; July 1998.Rogers HR. Sources, behaviour and fate of organic contaminants during sewage treatment and in sewage sludges.
Sci Total Environ 1996;185(1�3):3�26.Romanenko NA, Fedianina LV, Khizhniak NI, Ustinova SN, Pronina AV, Melnik OV, Novosiltsev GI. [Environmental
protection and the population's health status with reutilization of sewage in foreign countries]. Gig Sanit 1993Aug;(8):27�30.
Rowat SC. Incinerator toxic emissions: a brief summary of human health effects with a note on regulatory control.Med Hypotheses 1999 May;52(5):389�96.
Rowe NH, Sidhu KS, Chadzynski L, Babcock RF. Potential public health risks related to mercury/amalgam dischargefrom dental offices. Journal of Michigan Dental Association 1996;78(2):32�6.
Rushbrook P. Risks to man and the environment from the landfill disposal of wastes. Waste Management Today1990;3(2):26�31.
46
Rylander R. Health effects among workers in sewage treatment plants. Journal of Occupational EnvironmentalMedicine 1999;56:354�7.
Sadovski AY, Fattal B, Goldberg D, Katzenelson E, Shuval HI. High levels of microbial contamination of vegetablesirrigated with wastewater by the drip method. Applied & Environmental Microbiology 1978;36(6):824�30.
Saffron L. The consumer's perception of risk. Consumer Policy Review, 1993 Oct;3(4):213�221.Santillo D, Johnston P, Singhofen A. The way forward � out of the chemicals crisis. The Netherlands: Greenpeace
International; 1999.Scarlett-Kranz JM, Babish JG, Strickland D, Lisk DJ. Health among municipal sewage and water treatment workers.
Toxicology & Industrial Health 1987;3(3):311�9.Schneider JS, Tobe EH, Mozley PD, Barniskis L, Lidsky TI. Persistent cognitive and motor deficits following acute
hydrogen sulphide poisoning. Occup Med (Oxf) 1998 May;48(4):255�60.Sever LE. Environmental contamination and health effects: what is the evidence? Toxicology & Industrial Health
1997 Mar�Jun 30;13(2-3):145�61.Shane BS, Gutenmann W, Lisk DJ. Variability over time in the mutagenicity of ashes from municipal solid-waste
incinerators. Mutat Res 1993;301(1):39�43.Shusterman D, Lipscomb J, Neutra R, Satin K. Symptom prevalence and odor-worry interaction near hazardous
waste sites. Environmental Health Perspectives 1991;94:25�30.Shy CM, Degnan D, Fox DL, Mukerjee S, Hazucha MJ, Boehlecke BA, Rothenbacher D, Briggs PM, Devlin RB, Wallace
DD Do waste incinerators induce adverse respiratory effects? An air quality and epidemiological study of sixcommunities. Environ Health Perspect 1995 Jul-1995 Aug 31;103(7-8):714�24.
Silkworth JB, Lipinskas T, Stoner CR. Immunosuppressive potential of several polycyclic aromatic hydrocarbons(PAHs) found at a superfund site: new model used to evaluate additive interactions between benzo[a]pyreneand tcdd. Toxicology 1995;105(2�3):375�86.
Simmons JERS, Yang DJ, Svendsgaard MB, Thompson JC, Seely A, McDonald. Toxicology studies of a chemicalmixture of 25 groundwater contaminants: hepatic and renal assessment, response to carbon tetrachloridechallenge, and influence of treatment-induced water restriction. Journal of Toxicology & Environmental Health1994;43(3):305�25.
Staff MG. Landfill sites and congenital abnormalities. [Letter; comment]. Lancet 1998 Nov 21;352(9141):1705.Stark AD. A community investigation from a state health department perspective: the Love Canal. Environmental
Epidemiology and Toxicology 2000;2(2�3):151�65.Stehr-Green PA, Welty E, Burse VW. Human exposure to polychlorinated biphenyls at toxic waste sites: investigations
in the United States. Archives of Environmental Health 1988 Nov�1988 Dec 31;43(6):420�4.Sterling DA, Johnson DL, Murgueytio AM, Evans RG. Source contribution of lead in house dust from a lead mining
waste superfund site. Journal of Exposure Analysis & Environmental Epidemiology 1998 Jul-1998 Sep30;8(3):359�73.
Straub TM, Pepper IL, Gerba CP. Hazards from pathogenic microorganisms in land-disposed sewage sludge. Reviewsof Environmental Contamination & Toxicology 1993;132:55�91.
Taubes G. Epidemiology faces its limits. Science 1995 Jul 14;269:164�9.The National Assembly for Wales. Developing health impact assessment in Wales. Cardiff, Wales: the National
Assembly for Wales; 1999.Thorn J, Kerekes E. Health effects among employees in sewage treatment plants: a literature survey. Am J Ind Med
2001;40 (2):170�9.Tomatis L. Cancer: causes, occurrence and control. France: International Agency for Research on Cancer; 1990.Tubb A, Iwugo K. Landfill technology. Bristol: University of the West of England; 2000.Tubb A, Iwugo K. Organisation of municipal solid waste management system. Bristol: University of the West of
England; 2000.UNCED. Rio Declaration on Environmental and Development, made at UNCED, 1992. ISBN 9 21 100509 4Unger DG, Wandersman A, Hallman W. Living near a hazardous waste facility: coping with individual and family
distress. Am J Orthopsychiatry 1992;62(1):55�70.Vianna NJ, Polan AK. Incidence of low birth weight among Love Canal residents. Science 1984;226:1217�9.von Muhlendahl KE. Uncontrolled replication: hazardous landfill sites and congenital anomalies. Eur J Pediatr
1999;158(11):950�1.Vrijheid M. Health effects of residence near hazardous waste landfill sites: a review of epidemiologic literature.
Environmental Health Perspectives 2000 Mar;108(Supplement 1):101�12.WCRF & AICR, World Cancer Research Foundation and American Institute for Cancer Research. Food, Nutrition and
the prevention of cancer: a global perspective. Washington DC, USA: American Institute for Cancer Research;1997.
Wedeen RP, Haque S, Udasin I, D'Haese PC, Elseviers M, De Broe ME. Absence of tubular proteinuria followingenvironmental exposure to chromium. Archives of Environmental Health 1996;51(4):321�3.
Welsh Office, Health Evidence Bulletins � Wales: Healthy Environments. Cardiff: Welsh Office; 1999.

47
White PA, Rasmussen JB. The genotoxic hazards of domestic wastes in surface waters. Mutat Res 1998Jun;410(3):223�36.
Whiteman DC, Dunne MP, Burnett PC. Psychological and social correlates of attrition in a longitudinal study ofhazardous waste exposure. Archives of Environmental Health 1995;50(4):281�6.
WHO European Centre for Environment and Health. Methods of assessing risk to health from exposure to hazardsreleased from waste landfills.2000 Apr 10�2000 Apr 12; Lodz, Poland. WHO Regional Office for Europe; 2000.
WHO Meeting. Health effects from landfills: impact of the latest research � report on a WHO meeting1998 Oct 22;Bilthoven, Netherlands. Copenhagen, Denmark: WHO Regional Office for Europe; 1998.
WHO Working Group. Evaluation and Use of Epidemiological Evidence for Environmental Health Risk Assessment:WHO Guideline Document. Environmental Health Perspectives 2000;108(10):997�1002.
Williams A, Jalaludin B. Cancer incidence and mortality around a hazardous waste depot. Australian & New ZealandJournal of Public Health 1998;22(3 Suppl):342�6.
Wolfinger TF. Screening-level assessment of airborne carcinogen risks from uncontrolled waste sites. Japca 1989Apr;39(4):461�8.
Wrbitzky R, Goen T, Letzel S, Frank F, Angerer J. Internal exposure of waste incineration workers to organic andinorganic substances. International Archives of Occupational & Environmental Health 1995;68(1):13-21.
Zielhuis R. Strategy of assessment of health risks in environmental and occupational health. In: Castellani A, editor.Epidemiology and quantitation of environmental risk in humans from radiation and other agents. New York:Plenum Press; 1985. pp. 17�31.
Zmirou D, Deloraine A, Saviuc P, Tillier C, Boucharlat A, Maury N. Short-term health effects of an industrial toxicwaste landfill: a retrospective follow-up study in Montchanin, France. Archives of Environmental Health1994;49(4):228�38.
48
A1.1Scoping exercise
An initial scoping exercise was carried out to discoverwhat has been written on the subject of waste andhealth. Searches were conducted of online databasesand references in published papers (Appendix 2). Thesearch revealed thousands of documents about themany health hazards and health impacts associated withwaste and about a number of different types of wastemanagement. It raised questions about the focus of thetopic under consideration. At this stage, any referenceabout waste and health was kept. As a result of thescoping exercise, decisions were needed about how tofocus the search to what was considered relevant forthis project.
A1.2 Decisions
Decision 1: to focus on review papersSince the project brief was to carry out a systematicliterature review, the first decision was to find out whatreviews had been published. To avoid unnecessaryduplication of effort, the CRD protocol recommends athorough search for review papers before searching forprimary studies. The project management team madethe decision to narrow the search to reviews and not tosystematically search for all the primary studies carriedout.
Decision 2: to define health broadlyThe decision was taken not to define health too narrowlybut to use the WHO definition of health as a �state ofcomplete physical, mental and social well-being and notmerely the absence of disease and infirmity�.
Decision 3: to focus on health impactsinstead of health hazardsA health hazard is anything that can potentially causeharm. (For examples see Table 5, Factors AffectingHealth.)
A health impact is any change in health risk that isreasonably attributable to a project, programme orpolicy. (Definitions from BMA 1998, p53.)
The decision was made to search for documentsabout the health impacts associated with waste disposaland not to systematically search for documents aboutthe health hazards. This decision was made in order tofocus the project on those research studies that providethe strongest evidence of a link between the wastedisposal method and human health.
Decision 4: to focus on particular wastedisposal methodsThe initial brief was to focus primarily on the health
impacts of landfill, incineration, sewage treatment, andsoil amendments such as sewage sludge. The advisorygroup suggested that composting and recycling beincluded. Disposal of radioactive waste was not includedalthough a few papers discovered during searching wereretrieved and added to the database.
Decision 5: to focus on studies of directrelevance to waste disposalThe decision was made to prioritise papers directlyrelevant to waste disposal methods, rather than topapers that are only indirectly related. The hazardsidentified are not unique to waste disposal methods.They also originate from other sources such as industrialprocesses, power generation and natural sources.Examples:� Tetrachloroethylene may contaminate drinking water
when it leaches from a landfill site or when it leachesfrom the vinyl lining of drinking-water distributionpipes.
� The source of dioxins is any combustion process inwhich chlorinated organic chemicals are burned.
� Metals processing is the major source of leademissions to the atmosphere.
� Volcanic activity and soil degassing during naturalfires are important contributors to global emissionsof mercury (National Research Council 2000).
A study demonstrating an association between ahealth impact and a hazard arising from a non-wastesource is an important indication of the harmful natureof that hazard. However, the focus of this report is onwaste disposal.
Decision 6: to focus on recent papersThe decision was made not to search thoroughly forpapers written before 1982 partly because of thedifficulties in obtaining papers from before this time butmainly because of changes in waste managementpractices over the years. Only reviews written since1992 were included.
Decision 7: to focus on developed countriesNo consistent decision was made about includingreferences from other countries. Priority was given topapers about the South West of England and the UK.However, studies from other developed countries intemperate zones were included as there are likely to bemany similarities with the UK in waste production andmanagement. There was a bias towards continentalEurope, the United States, Australia and New Zealand.Papers about the health impacts of waste disposal intropical, developing countries were generally notincluded.
Appendix 1: The literature search
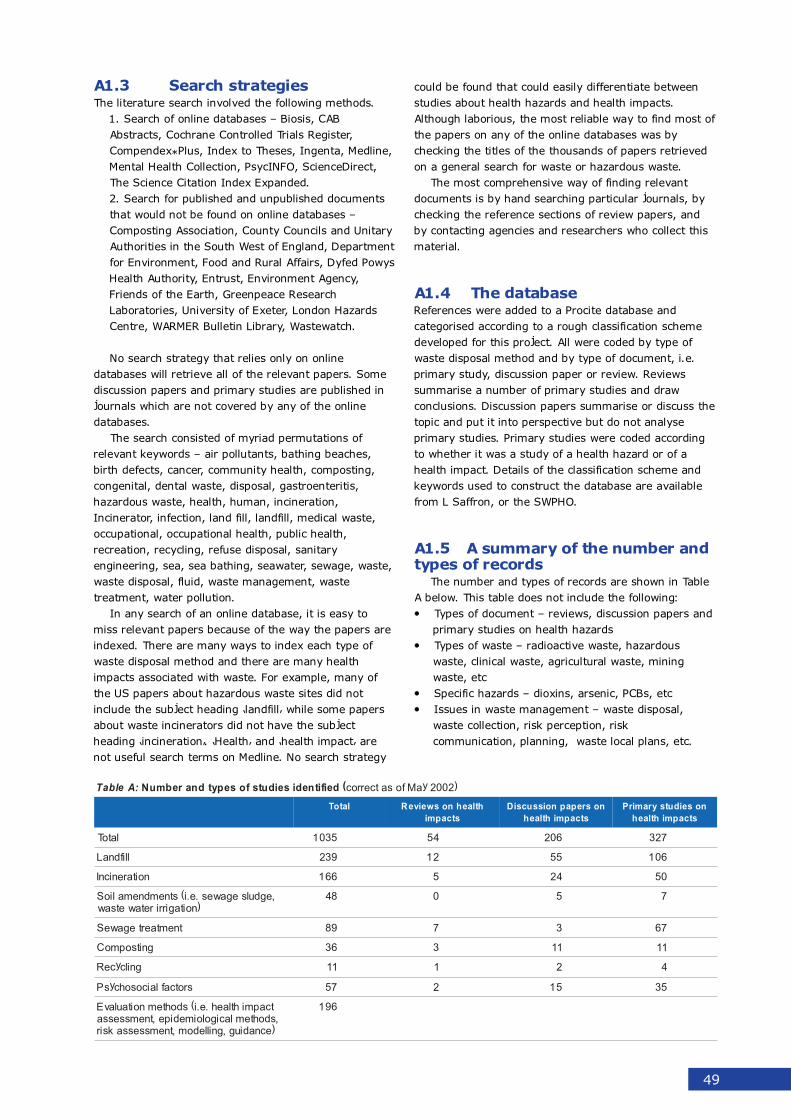
49
A1.3 Search strategiesThe literature search involved the following methods.
1. Search of online databases � Biosis, CABAbstracts, Cochrane Controlled Trials Register,Compendex*Plus, Index to Theses, Ingenta, Medline,Mental Health Collection, PsycINFO, ScienceDirect,The Science Citation Index Expanded.2. Search for published and unpublished documentsthat would not be found on online databases �Composting Association, County Councils and UnitaryAuthorities in the South West of England, Departmentfor Environment, Food and Rural Affairs, Dyfed PowysHealth Authority, Entrust, Environment Agency,Friends of the Earth, Greenpeace ResearchLaboratories, University of Exeter, London HazardsCentre, WARMER Bulletin Library, Wastewatch.
No search strategy that relies only on onlinedatabases will retrieve all of the relevant papers. Somediscussion papers and primary studies are published injournals which are not covered by any of the onlinedatabases.
The search consisted of myriad permutations ofrelevant keywords � air pollutants, bathing beaches,birth defects, cancer, community health, composting,congenital, dental waste, disposal, gastroenteritis,hazardous waste, health, human, incineration,Incinerator, infection, land fill, landfill, medical waste,occupational, occupational health, public health,recreation, recycling, refuse disposal, sanitaryengineering, sea, sea bathing, seawater, sewage, waste,waste disposal, fluid, waste management, wastetreatment, water pollution.
In any search of an online database, it is easy tomiss relevant papers because of the way the papers areindexed. There are many ways to index each type ofwaste disposal method and there are many healthimpacts associated with waste. For example, many ofthe US papers about hazardous waste sites did notinclude the subject heading �landfill� while some papersabout waste incinerators did not have the subjectheading �incineration�. �Health� and �health impact� arenot useful search terms on Medline. No search strategy
could be found that could easily differentiate betweenstudies about health hazards and health impacts.Although laborious, the most reliable way to find most ofthe papers on any of the online databases was bychecking the titles of the thousands of papers retrievedon a general search for waste or hazardous waste.
The most comprehensive way of finding relevantdocuments is by hand searching particular journals, bychecking the reference sections of review papers, andby contacting agencies and researchers who collect thismaterial.
A1.4 The databaseReferences were added to a Procite database andcategorised according to a rough classification schemedeveloped for this project. All were coded by type ofwaste disposal method and by type of document, i.e.primary study, discussion paper or review. Reviewssummarise a number of primary studies and drawconclusions. Discussion papers summarise or discuss thetopic and put it into perspective but do not analyseprimary studies. Primary studies were coded accordingto whether it was a study of a health hazard or of ahealth impact. Details of the classification scheme andkeywords used to construct the database are availablefrom L Saffron, or the SWPHO.
A1.5 A summary of the number andtypes of records
The number and types of records are shown in TableA below. This table does not include the following:� Types of document � reviews, discussion papers and
primary studies on health hazards� Types of waste � radioactive waste, hazardous
waste, clinical waste, agricultural waste, miningwaste, etc
� Specific hazards � dioxins, arsenic, PCBs, etc� Issues in waste management � waste disposal,
waste collection, risk perception, riskcommunication, planning, waste local plans, etc.
:AelbaT (deifitnediseidutsfosepytdnarebmuN )2002yaMfosatcerroc
latoT htlaehnosweiveRstcapmi
nosrepapnoissucsiDstcapmihtlaeh
noseidutsyramirPstcapmihtlaeh
latoT 5301 45 602 723
llifdnaL 932 21 55 601
noitarenicnI 661 5 42 05
,egdulsegawes.e.i(stnemdnemalioS)noitagirriretawetsaw
84 0 5 7
tnemtaertegaweS 98 7 3 76
gnitsopmoC 63 3 11 11
gnilcyceR 11 1 2 4
srotcaflaicosohcysP 75 2 51 53
tcapmihtlaeh.e.i(sdohtemnoitaulavE,sdohtemlacigoloimedipe,tnemssessa
)ecnadiug,gnilledom,tnemssessaksir
691
50
The results of applying the algorithm to deliver ajudgement (1.3.3) to the literature is shown below.
A2.1 Landfill
1. Have studies been done on humanpopulations?
Yes.The literature search revealed more than 220 paperspublished about the hazards to health from landfillsites. Of these, 101 are primary studies about thehealth impacts of landfill sites and 23 about thehealth impacts of contaminated drinking water. Sixreview papers were found which covered theepidemiological evidence linking health effects withlandfill sites (Cantor, 1997, Johnson, 1997, Johnson,1999, Miller, 1996, Sever, 1997, Vrijheid, 2000). Thedrinking water studies were included in this sectionbecause an important source of exposure fromlandfill sites is leachate into groundwater. However, inmany studies, the source of the contamination wasnot known. In some studies the source was leakingchemical storage tanks, in others, chemical accidents.Studies were not included if the water wascontaminated by sewage (see section on sewagebelow). Only seven of the total are occupationalhealth studies, the rest being studies about thehealth impacts on nearby communities.
The studies looked for links between the landfillsites and the following health outcomes:Reproductive outcomes/ developmental effects onchildren (31 studies), Cancer (29), Symptoms (28),Psychosocial impacts (19), Biomarkers (13), Healthproblems - not specified in abstract (14), Mortality(5), Injuries/poisoning (2)
2. Have hazards been identified? Does theappearance of the hazard precede the healthoutcome? Is the association biologicallyplausible? Is there data on exposure?
No.The main weakness of the studies about landfillhealth effects is the complete lack of exposure data.All use residence near the site as a proxy measure ofexposure � i.e. data based on census tract, postcode, or residence within 2 or 3 km of the site. Afew studies provided more detailed exposure data.For example, in a French study (Zmirou et al, 1994)individual exposure was estimated for one point intime, using a dispersion model of volatile airpollutants and the daily activity patterns of each
individual within the area under investigation. Thelandfill site had been in operation for the previous 9years. In this study, there were no statisticallysignificant differences in consumption of prescriptiondrugs.
Where the hazards from landfill sites have beenidentified, as is the case in the National Priorities Listsites in the United States, it is possible to estimateexposure using the EPA Human Exposure Model(Wolfinger, 1989). The model is based onassumptions about the rate and toxicity of siteemissions and can be used to estimate cancer risksfrom inhalation for each site in terms of risk to themaximally exposed individual (MEI risk), to theaverage individual (AEI risk), and to the population.The results of this type of analysis are uncertain andare based on risky assumptions. These remainestimates, not data. However, there is somebiological plausibility in the association of congenitalabnormalities and landfill sites due to the sensitvityof the fetus.
3. Are there ANY hypothesis-testing studies?
No.Because of the lack of exposure data, the studies arehypothesis-generating studies rather thanhypothesis-testing studies.
4. Have any of the hypothesis-testing studiescontrolled for possible confounding factors?
No.With ecological studies of this type, it is impossible tocontrol for other sources of pollutants. For example,the conclusion that the landfill site in Nant-y-Gwyddon may have been responsible for anincreased rate of congenital abnormalities inresidents near the site (Fielder et al, 2000) has beenchallenged by researchers who pointed out that amunicipal incinerator operated in the same area justbefore the landfill site opened (Roberts et al, 2000).There was no direct evidence that the landfill, ratherthan the poorly performing and heavily pollutingincinerator, was the cause of the adverse healthoutcomes. As well as other environmental pollutantsfrom industrial and traffic pollution, there is usuallyconcurrent exposure to occupational hazards, indoorair pollutants, tobacco smoke, alcohol, prescriptiondrugs and recreational drugs.
Appendix 2: How judgements were derived orjustification for judgements
51
5. Are there more than 20 hypothesis-testingstudies consistently showing strong ormoderate relative risks?
No.There are more than 20 hypothesis-generatingstudies but the results were inconsistent, with someshowing associations between landfill and varioushealth impacts while other studies found noassociations. Relative risks ranged from noassociation to strong.
In reviews, discussion papers, conferences andconsensus meetings, many attempts have beenmade to determine whether the findings indicate realrisks associated with exposure to landfill sites. Thereis general agreement with the cautious position takenat a meeting convened by the WHO Regional Officefor Europe in 1998 which concluded:
�Many of the studies detected an increased risk ofthe studied diseases and symptoms in populationsliving close to the landfills. However, the evidencesupporting the causality of the association isinconsistent and inconclusive. Probably the strongestsuggestion for causality was generated by studies onreproductive outcomes, such as reduced birth weightor some birth defects. However, all studies lackeddirect exposure assessment, and the limited samplesize of most studies makes a more specific analysisimpossible. � Considering all the uncertainties, themeeting concluded that the present data do add to asuspicion that population exposure to emissions fromhazardous wastes may pose a risk to populationhealth. The present studies are not powerful enoughto indicate which of the characteristics of the veryinhomogeneous group of landfills that are included inthe studies might be responsible for the observedsmall increase in the risk.� (WHO meeting, 1998)
Judgement - insufficient
A2.2 Incineration
1. Have studies been done on humanpopulations?
Yes.The literature search yielded 50 primary studies andthree reviews (Allsopp et al, 2001, Hu and Shy, 2001,National Research Council, 2000). The majority werestudies on communities but there were 14occupational health studies.
All types of health outcomes were investigated,including: Cancer (15 studies), Health problems/diseases/unspecified health effects (12 studies),Biomarkers (10 studies), Reproductive outcomes/developmental effects on children (9 studies),Symptoms (8 studies), Mortality (5 studies), Injuries/poisoning (3 studies), Psychosocial impacts (2studies), Economic (1 study).
2. Have hazards been identified? Does theappearance of the hazard precede the healthoutcome? Is the association biologicallyplausible? Is there data on exposure?
Yes.Among the occupational health studies, there were 3studies where exposure was presumed fromoccupation in the incinerator; two studies withquantified ambient measurements of PM10(particulates) or metals; and 7 studies providingquantified personal measurements (of blood levels oflead or of urinary mutagens). There was not enoughinformation about the remaining two studies tocategorise the exposure data.
Among the studies of communities living near toincinerators, 4 used quantified ambientmeasurements, 2 used quantified estimates and 27studies used residence as a proxy measure ofexposure.
3. Are there ANY hypothesis-testing studies?
Yes.The following were hypothesis-testing studies:1. An occupational health study of a cohort ofincinerator workers with high, medium and lowexposure to toxic compounds such as metals(Bresnitz et al, 1992),2. A study simultaneously measuring air quality andrespiratory function and symptoms in populationsliving in the neighborhood of waste incineratorscompared with three matched-comparisoncommunities. (Shy et al, 1995)3. A study of six communities in southwestern NorthCarolina investigating the respiratory health status ofresidents whose households are located near anincinerator. This diary study estimated the dailyvariation of pulmonary function measured as peakexpiratory flow rate (PEFR) related to 24-h meanPM10 levels, which were observed at each monitoringstation placed in the six study communities, as asurrogate exposure measure of outdoor air pollution.This study did not show any difference in respiratoryhealth between subjects of an incinerator communityand those of its comparison community. (Lee andShy, 1999)4. Study of 713 children in 2 regions near 2 sludgeburning incinerators in Sydney. Controls were 626children in a region with no incinerator. Exposureassessment by air monitoring and region ofresidence. Outcomes - prevalence of respiratoryillness, airway hyperresponsiveness, atopy, FEV1.Results - no significant differences in baseline FEV1and prevalence of current asthma, atopy, symptomfrequency or severity of asthma illness betweenstudy and control regions. (Gray et al, 1994)
52
4. Have any of the hypothesis-testing studiescontrolled for possible confounding factors?
Yes.For example, the study by Lee & Shy (1999)analyzed how health outcomes varied according tothe degree of exposure to ambient pollutants as wellas to other cofactors including, sex, age, respiratoryhypersensitivity, hours spent outdoors within the areaof the selected community, and surrogate measuresfor indoor air pollution exposure (vacuum use andexperience of air irritants at work).
5. Are there more than 20 hypothesis-testingstudies consistently showing strong ormoderate relative risks?
No.The 4 hypothesis-testing studies consistently showedno association between the hazards from incinerationand any health outcomes. Even among thehypothesis-generating studies, the results wereinconsistent. Roughly half the primary studies foundan increase in the incidence of a health problem andhalf did not.
Using the algorithm above, we judged theevidence linking incineration with any healthoutcomes as insufficient.
A2.3 Composting
1. Have studies been done on humanpopulations?
Yes.Two review papers were found (Maritato et al, 1992,Environment Agency, 2001) and 11 primary studies.
2. Have hazards been identified? Does theappearance of the hazard precede the healthoutcome? Is the association biologicallyplausible? Is there data on exposure?
Yes.The main hazards identified from composting arebioaerosols containing bacteria such as Clostridiumbotulinum and endotoxin-producing Gram negativebacteria and/or fungal spores such as Aspergillusfumigatus. The main health impacts from composting(Bunger et al, 2000) are:� Inflammatory responses of the upper airways �
congested nose, sore throat and dry cough� Toxicoses � toxic pneumonitis due to endotoxins� Infections � respiratory tract and skin� Allergies - bronchial asthma, allergic rhinitis,
extrinsic allergic alveolitis (hypersensitivitypneumonitis)
The association between bioaerosols and these healthoutcomes is biologically plausible. The route ofexposure is inhalation. The data on exposure ismeasurements of specific IgG antibodies to fungi andbacteria as immunological markers of exposure tobioaerosols.
3. Are there ANY hypothesis-testing studies?
Yes.There is a case control study (Bunger et al, 2000)which found that the compost workers hadsignificantly more symptoms and diseases of theairways (p=0.003) and the skin (p=0.02) than thecontrol subjects. They had significantly increasedantibody concentrations against fungi andactinomycetes. No studies were found about thehealth impacts to residents living by compostingfacilities.
4. Have any of the hypothesis-testing studiescontrolled for possible confounding factors?
YesThe participants were interviewed for work relatedsymptoms, conditions of exposure to bioaerosols attheir workplaces, exposure to bioaerosols from othersources, atopic diseases, and smoking habits.
5. Are there more than 20 hypothesis-testingstudies consistently showing strong ormoderate relative risks?
No.Only one case-control study was found. The restwere case reports or hypothesis-generating studies.Regarding occupational exposure, it is possible thatcomposting causes health problems. But the evidenceis insufficient regarding residence near compostingfacilities.
A2.4 Sewage
Bathing in sewage contaminated recreationalwaters and gastrointestinal symptomsBecause only a few studies investigated skin, eye, earand respiratory illnesses associated with recreational useof contaminated water, this judgement is limited to theassociation with gastrointestinal symptoms. Thejudgement is based on a review paper by Prussevaluating the health risks caused by poormicrobiological quality of recreational natural water(Pruss, 1998). Water quality was measured by indicator-bacteria of faecal origin assumed to be resulting fromsewage discharge. It is possible but unlikely that thecontamination could be due to other bathers.
53
1. Have studies been done on humanpopulations?
Yes.Six review papers (Ashbolt, 1996, Barrell et al, 2000,IEH, 2000, Kindzierski and Gabos, 1996, Pruss,1998) and 37 primary studies were found about thehealth effects of recreational bathing in sewagecontaminated waters.
2. Have hazards been identified? Does theappearance of the hazard precede the healthoutcome? Is the association biologicallyplausible? Is there data on exposure?
Yes.The hazards are microbial pathogens known to causegastrointestinal symptoms. The exposure dataconsists of measurements of viral, bacterial andfungal pathogens and faecal indicator organismstypically found in sewage discharges.
3. Are there ANY hypothesis-testing studies?
Yes.In the review by Pruss, there were 22 hypothesis-testing studies meeting strict criteria for inclusion(Pruss, 1998 p2)
4. Have any of the hypothesis-testing studiescontrolled for possible confounding factors?
Yes.The confounding factors controlled for included foodand drink intake, age, sex, history of certaindiseases, drug use, personal contact, additionalbathing, sun, and socioeconomic factors. 12/22studies controlled for less than 3 of the previousfactors. 4/22 studies took into account 3-4 factors. 6/22 studies accounted for 7 or more studies. Giventhe number of potential confounding factors, thepathogen threshold level for increased risk is stillcontroversial. For example, it is possible thatincreased immunity in adult populations and inpopulations of countries with higher endemicity mayresult in higher threshold levels. Different countriesdetect different ranges of pathogens in water and usedifferent detection methods.
5. Are there more than 20 hypothesis-testingstudies consistently showing strong ormoderate relative risks?
Yes.Of the 22 studies in the Pruss review, 19 showed
significant relationship of gastrointestinal symptomsto faecal indicator bacteria or bacterial pathogens. In3 studies, there were no significant relationships.The relative risks included strong and moderatelystrong associations:17 correlations where RR >2 (strong),13 correlations where RR 1.5-2 (moderate)18 corrrelations where RR <1.5 (weak)
6. Are there a range of study designs?
Yes.There were 2 randomised controlled trials, 18prospective cohort, 2 retrospective cohort studies.
7. Have studies been carried out in differentpopulation groups?
Yes.Studies were carried out in the UK, USA, NewZealand, Hong Kong, Australia, Egypt, South Africa,Israel, Spain, France, Canada.
8. If dose-response relationships are observed,do they confirm the association between thehazard and the health outcome?
Yes.Most of the studies showed significant dose-responserelationship. The best dose-illness correlation wasfound with enterococci or faecal streptococci.
Occupational diseases of sewage treatmentworkers
1. Have studies been done on humanpopulations?
Yes.There was one review (Thorn and Kerekes, 2001))and 38 primary studies. The health effectsinvestigated were symptoms (17 studies), infections,i.e. hepatitis A, hepatitis C, legionella, leptospirosis,gastroenteritis (16 studies), mortality (3 studies),reproductive outcomes (1 study), biomarkers (3studies) and cancer (5 studies).
2. Have hazards been identified?
Yes.From the mortality and cancer studies, no hazardswere identified. From studies on symptoms andinfections, the following hazards were identified -bacteria, bacterial endotoxins, hydrogen sulphide,and organic solvents.
54
3. Does the appearance of the hazard precedethe health outcome? Is the associationbiologically plausible?
Yes.For symptoms, it is plausible that pathogenic micro-organisms, bacterial endotoxins, organic solvents andhydrogen sulfide could be related to the symptomsobserved.
No.For cancer, none of the agents commonly found insewage treatment plants have been related to anincreased risk of stomach cancer. The spread of theother cancers over a multitude of organs does notsupport a hypothesis of causality with agentscommonly found in sewage treatment plants.
4. Is there data on exposure?
Yes.Detailed exposure measurements were included insome of the studies on symptoms and infections butin most of the studies, the exposure was inferred bythe subjects� occupation as a sewage treatmentworker. The exposure route was inhalation.Measurements were given of airborne viable bacteria(Lundholm and Rylander, 1983), (Melbostad et al,1994), airborne endotoxin levels (Rylander,1999),(Melbostad et al, 1994), hydrogen sulphide(Richardson, 1995), airborne organic solvents (Kuo etal, 1996), and amount of specific antibodies in theblood. For the mortality and cancer studies, noexposure data was provided.
5. Are there ANY hypothesis-testing studies?
Yes.There were 29 hypothesis-testing studies. Anexample is a retrospective cohort study from theUnited States in which 28 sewage treatment workerswere compared with data from a pooled non-exposedpopulation (Kuo et al, 1996). The health outcomewas central nervous system effects, determined bypostural stability assessment. Exposure assessmentwas by measurement of organic solvents in thesewage treatment plant. In this, there was astatistically significant correlation between posturalsway and organic solvent exposure and sewageworkers had an increased postural sway comparedwith controls.
6. Have any of the hypothesis-testing studiescontrolled for possible confounding factors?
Yes.Of the 29 studies, there were 16 which adjusted forpersonal factors such as smoking, alcohol use, age,educational level and gender.
7. Are there more than 20 hypothesis-testingstudies consistently showing strong ormoderate relative risks?
No.There were 10 studies showing strong or moderatelystrong odds ratios (although there were no ORs in 4of the studies).
8. Are there a range of study designs?
Yes.Uncontrolled cohort, cross-sectional, case-control,case reports, and retrospective cohort studies.
9. Have studies been carried out in differentpopulation groups?
Yes.Studies on sewage treatment workers in Germany,USA, Sweden, Denmark, Norway, UK, Canada,Greece, France, Israel, and Italy.
10. If dose-response relationships areobserved, do they confirm the associationbetween the hazard and the health outcome?
Not observed.
Judgement � probable.
Sewage discharges and reproductiveoutcomes
1. Have studies been done on humanpopulations?
No.Field and laboratory studies on a range of wildanimals have demonstrated adverse reproductiveoutcomes from xeno-oestrogens, natural andsynthetic substances with oestrogenic or anti-oestrogenic properties ((IEH, 1995)). Thesecompounds occur in sewage discharges and havebeen associated with endocrine disruption in wildlife,including �thyroid dysfunction in birds and fish,decreased fertility in birds, fish, shellfish andmammals, gross birth deformities in birds, fish andturtles, metabolic abnormalities in birds, fish andmammals, behavioural abnormalities in birds,demasculinisation and feminisation of female fish andbirds, and compromised immune systems in birdsand mammals� (quoted in (IEH, 1995)). Therelevance of these studies to human health is notclear but there is concern about the fall in quantity
55
and/or quality of sperm in recent decades ((IEH,1995; Colborn et al, 1997)).
Judgement � insufficient.
A2.5 Landspreading of sewagesludge
1. Have studies been done on humanpopulations?
No.There were no studies about the health impacts oflandspreading sewage sludge although there weretwo studies about the health impacts of working infacilities which prepare sewage sludge forlandspreading ((Clark et al, 1984),(Baker et al,1980). These were included in the section onoccupational hazards of sewage treatment workers.
2. Have hazards been identified? Does theappearance of the hazard precede the healthoutcome? Is the association biologicallyplausible? Are there data on exposure?
No.Hazardous substances have been identified in sewagesludge (e.g. (Dumontet et al 2001), (Rogers, 1996),(Ross et al, 1992; Straub et al, 1993) but there areno studies linking those hazards to human healtheffects. The Canadian Handbook on Health ImpactAssessment ((Anon, 2000.)Vol 2) evaluated the risksto human health as minimal because:� Pathogens have a short lifespan and their
persistent forms remain in the soil� Metals are not usually metabolised by soil micro-
organisms and will persist in the soil� Most pollutants bind to soil components� Most organic compounds, i.e. dioxins, are broken
down by soil micro-organisms� Most organic compounds don�t migrate into
surface or ground waters because they adhere tosoil components
� Volatile organic compounds evaporate within 48hours of landspreading.
However, there is a lack of understanding of thepotential for transfer of toxic compounds to food andabout the degradability and persistence of some toxiccontaminants ((Rogers, 1996)).
3. Are there ANY hypothesis-testing studies?
No.
Judgement � insufficient.
56
Appendix 3: Strategies and local plans in the SouthWest
The Government produced guidance on the format of the Waste Strategies in December 2001. The new guidance isbeing used to ensure that all waste management authorities present their strategies in the same format. (Source:Letter from MJ Wood, Contract and Waste Manager, Wiltshire County Council, 19 December 2001.)
BelbaT tseWhtuoSehtnisnalplacoldnaseigetartS: )1002rebmeceDfosatcerroc(
lasopsidetsaWytirohtua
ygetartstnemeganametsaW nalPlacoLetsaW
htaB-SENABtsaEhtroNdna
yratinUtesremoSytirohtuA
dlehnoitatlusnoccilbuP-licnuoCybdetpodasnoituloserdnastegraT
7991rebmevoN-yllaunnaygetartSetsaWweiverotdevloserlicnuoC
8991hcraMdeviecer-srepooCesuohretaWecirPybtropeR
1002rebotcOlicnuocottnewtfarD2002yraunaJdetcepxe-tisopedtfarD
yratinUlotsirBytirohtuA
ot7991rebmetpeS-esicrexenoitatlusnoccilbuP8991yraunaJ
8991hcraMdesiver-yciloptnemeganametsaW,gnitsopmoc,sisylanaesufernotuodeirracseidutS
etsawfosdohtemtnereffidfotcapmilatnemnorivnetnemssessAelcyCefiLgnisulasopsid
ybnoitacificepstcartnocerofebnoitatlusnoccilbuP0002lirpA
yciloptnemeganametsawdetpodalicnuoC0002yaM-stnemetats
snrecnochtlaehgnitagitsevnitcejorpdenoissimmoC?2002eudtroper-stnalpetsaWmorFygrenEfo
2002remmusdetcepxe-tisopedtfarD
ytnuoCllawnroClicnuoC
2002fodnenoitpodafoetaddetcepxE 8991detpoda-noisrevdr3htlaehcilbuplacoldetlusnoc,noitatlusnoccilbuP
s'ALnotnemnrevogmorfecivdalagelkoot,tnatlusnoc1002enuJdedulcnoc-htlaehsdrawotytilibisnopser
1002enuJ-tfardtisopeddesiveR2002yraurbeF-yriuqnicilbuP
ytnuoCnoveDlicnuoC
6991-desilanifreven-tfarDwonnettirwergniebtfarD
3002lirpA-detpodaebotdetcepxenoisrevlaniF
8991rebotcO-tfardnoitatlusnoC1002nmutuA-tisopednonalptfarD
4002-noitpodA
ytnuoCtesroDlicnuoC
roftuognioG.ycilopriehtgniraperpyltnerruCnoitatlusnoc
1002hcraM-noitatlusnoctisoped-erP2002hcraM/beF-tfardtisopedtsriF3002beF/naJ-tfardtisopeddnoceS
3002voN/tcO-yriuqnicilbuplacoL4002tpeS/guA-snoitacifidoM
5002yaM/lirpA-noitpodA
erihsretsecuolGlicnuoCytnuoC
7991dehsilbupygetartstsaL
2002naJ-noitatlusnoC
2002yaMdetelpmocebottcepxE
9991nmutuA-noitatlusnoctisoped-erP1002lirpA-slasoporpdesiverfotisopeD
-tropersrotcepsnI1002nmutua-yriuqnilacolcilbuP1002/1002retniw
2002gnirps-slasoporpfonoitacifidoM2002gnirps-noitpodA
tesremoShtroNytirohtuAyratinU
.tnemucodnoitatlusnocon,gnitlusnocyltnerruC.3002detelpmocebottcepxE
,tnemucodnoitatlusnocontub,wongniognonoitatlusnoC.3002enodeblliw
ytnuoCtesremoSlicnuoC
eulaVtseBnognikrowyltnerruc-ygetartsdesiveR,nettirweblliwygetartshcihwfotuossecorp
2002remmusemitemos
fonoitcudorpniegatstsrif-troper"tratSagnikaM".0002-nalPlacoLetsaW
noitatlusnoclamroftsrif(nalptfardtisopedtsriF1002retniw-)tnemucod
;2002-nalptfardtisopeddnoceS30002ylrae/2002etal-yriuqnicilbuP
4002-noitpodanalP
htuoSerihsretsecuolG
ytirohtuAyratinU
swolloftubtnemucodetarapesasatsixet'nseoDtcartnocehtnideidobmesidnaygetartslanoitaneht
SWUhtiw
9991nmutua-nalptisopedtsriF0002remmusetal-nalptisopeddnoceS
1002hcraM-yriuqnilacolcilbuP1002remmus-tropers'rotcepsnI
1002nmutua-snoitacifidoM2002gnirps-noitpodA
ytnuoCerihstliWlicnuoC
detelpmoceblliW.1002yluJeettimmocotgnioG2002hcraMnidehsilbupdna
9991voN-tnemucodnoitatlusnoC0002rebmevoN-tfardtisopedtsrifgniraperpwoN
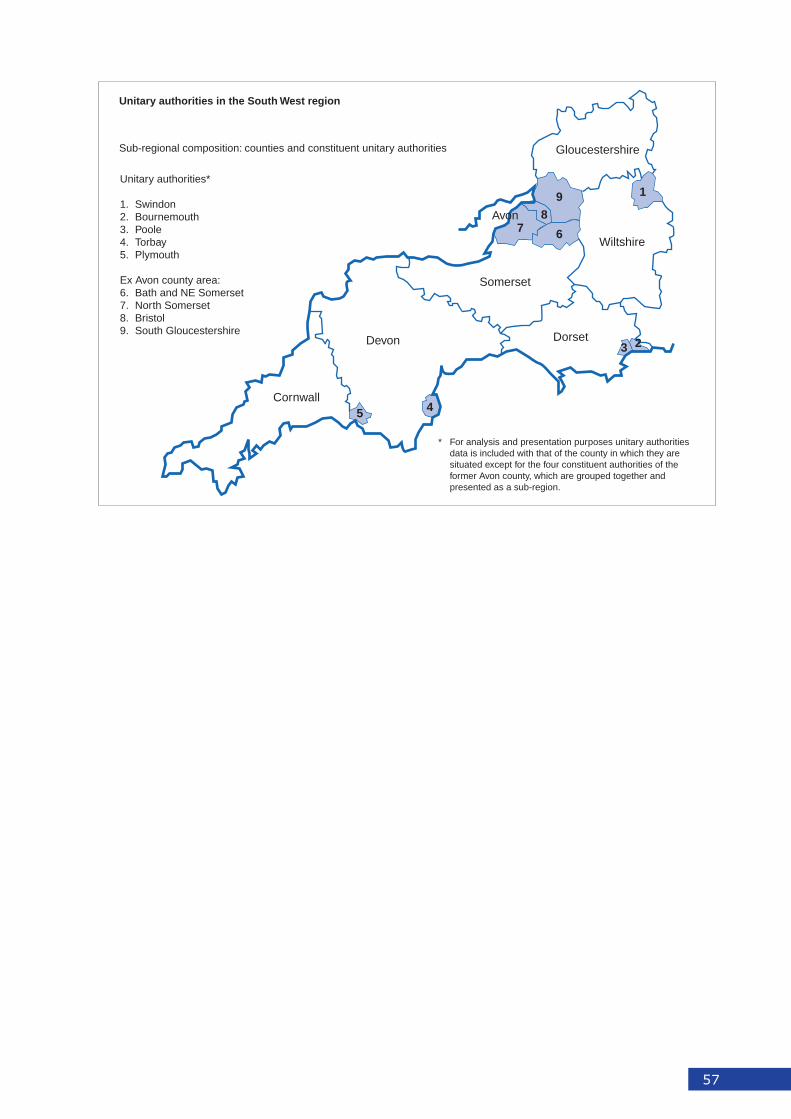
57
Unitary authorities in the South West region
Sub-regional composition: counties and constituent unitary authorities
Unitary authorities*
1. Swindon2. Bournemouth3. Poole4. Torbay5. Plymouth
Ex Avon county area:6. Bath and NE Somerset7. North Somerset8. Bristol9. South Gloucestershire
* For analysis and presentation purposes unitary authorities data is included with that of the county in which they are situated except for the four constituent authorities of the former Avon county, which are grouped together andpresented as a sub-region.
1
23
45
678
9
Cornwall
Devon
Somerset
Dorset
Wiltshire
Gloucestershire
Avon
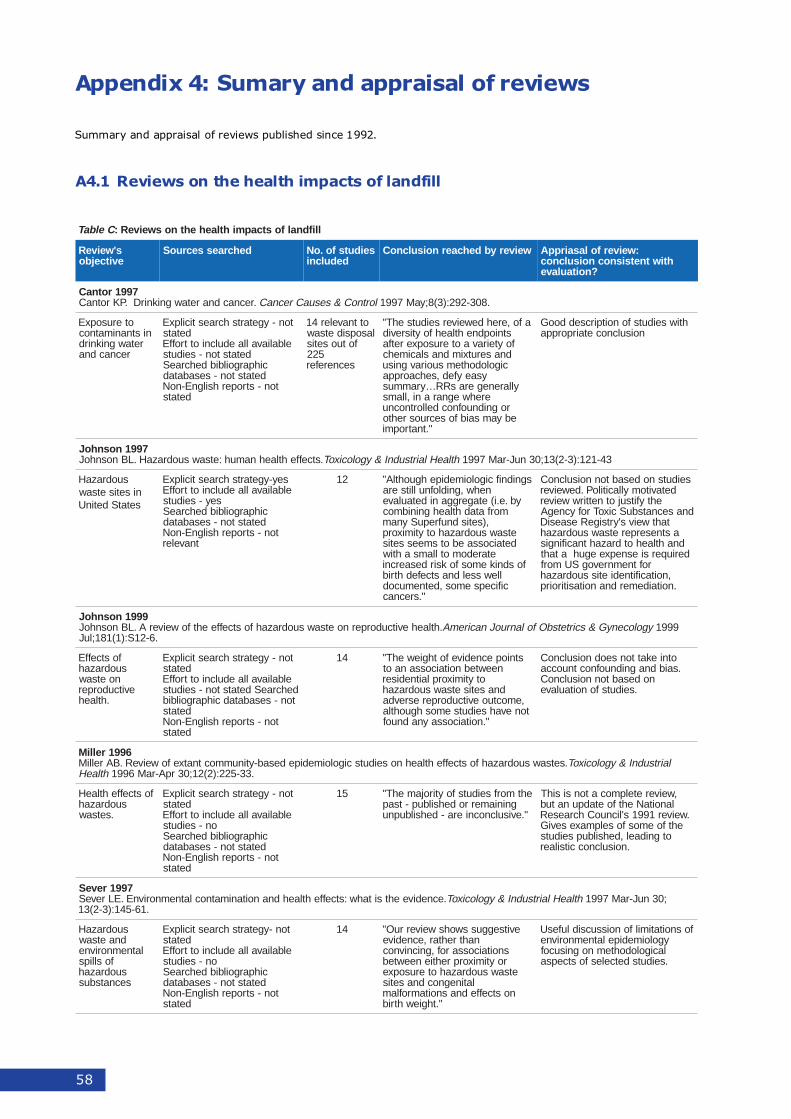
58
Appendix 4: Sumary and appraisal of reviews
Summary and appraisal of reviews published since 1992.
A4.1 Reviews on the health impacts of landfill
CelbaT llifdnalfostcapmihtlaehehtnosweiveR:
s'weiveRevitcejbo
dehcraessecruoS seidutsfo.oNdedulcni
weiverybdehcaernoisulcnoC :weiverfolasairppAhtiwtnetsisnocnoisulcnoc
?noitaulave
7991rotnaC.recnacdnaretawgniknirD.PKrotnaC lortnoC&sesuaCrecnaC .803-292:)3(8;yaM7991
oterusopxEnistnanimatnoc
retawgniknirdrecnacdna
ton-ygetartshcraesticilpxEdetats
elbaliavallaedulcniottroffEdetatston-seiduts
cihpargoilbibdehcraeSdetatston-sesabatad
ton-stroperhsilgnE-noNdetats
ottnaveler41lasopsidetsaw
fotuosetis522
secnerefer
afo,erehdeweiverseidutsehT"stniopdnehtlaehfoytisrevidfoyteiravaoterusopxeretfa
dnaserutximdnaslacimehccigolodohtemsuoiravgnisu
ysaeyfed,sehcaorppayllarenegerasRR…yrammus
erehwegnarani,llamsrognidnuofnocdellortnocnuebyamsaibfosecruosrehto
".tnatropmi
htiwseidutsfonoitpircseddooGnoisulcnocetairporppa
7991nosnhoJ.stceffehtlaehnamuh:etsawsuodrazaH.LBnosnhoJ htlaeHlairtsudnI&ygolocixoT 34-121:)3-2(31;03nuJ-raM7991
suodrazaHnisetisetsawsetatSdetinU
sey-ygetartshcraesticilpxEelbaliavallaedulcniottroffE
sey-seidutscihpargoilbibdehcraeSdetatston-sesabatad
ton-stroperhsilgnE-noNtnaveler
21 sgnidnifcigoloimedipehguohtlA"nehw,gnidlofnullitsera
yb.e.i(etagergganidetaulavemorfatadhtlaehgninibmoc
,)setisdnufrepuSynametsawsuodrazahotytimixorpdetaicossaebotsmeessetis
etaredomotllamsahtiwfosdnikemosfoksirdesaercni
llewsseldnastcefedhtribcificepsemos,detnemucod
".srecnac
seidutsnodesabtonnoisulcnoCdetavitomyllacitiloP.deweiver
ehtyfitsujotnettirwweiverdnasecnatsbuScixoTrofycnegA
tahtweivs'yrtsigeResaesiDastneserperetsawsuodrazahdnahtlaehotdrazahtnacifingisderiuqersiesnepxeeguhataht
roftnemnrevogSUmorf,noitacifitnedietissuodrazah.noitaidemerdnanoitasitiroirp
9991nosnhoJ.htlaehevitcudorpernoetsawsuodrazahfostceffeehtfoweiverA.LBnosnhoJ ygolocenyG&scirtetsbOfolanruoJnaciremA 9991
.6-21S:)1(181;luJ
fostceffEsuodrazah
noetsawevitcudorper
.htlaeh
ton-ygetartshcraesticilpxEdetats
elbaliavallaedulcniottroffEdehcraeSdetatston-seidutston-sesabatadcihpargoilbib
detatston-stroperhsilgnE-noN
detats
41 stniopecnedivefothgiewehT"neewtebnoitaicossanaot
otytimixorplaitnediserdnasetisetsawsuodrazah
,emoctuoevitcudorperesrevdatonevahseidutsemoshguohtla
".noitaicossaynadnuof
otniekattonseodnoisulcnoC.saibdnagnidnuofnoctnuocca
nodesabtonnoisulcnoC.seidutsfonoitaulave
6991relliM.setsawsuodrazahfostceffehtlaehnoseidutscigoloimedipedesab-ytinummoctnatxefoweiveR.BArelliM lairtsudnI&ygolocixoT
htlaeH .33-522:)2(21;03rpA-raM6991
fostceffehtlaeHsuodrazah
.setsaw
ton-ygetartshcraesticilpxEdetats
elbaliavallaedulcniottroffEon-seiduts
cihpargoilbibdehcraeSdetatston-sesabatad
ton-stroperhsilgnE-noNdetats
51 ehtmorfseidutsfoytirojamehT"gniniamerrodehsilbup-tsap
".evisulcnocniera-dehsilbupnu
,weiveretelpmocatonsisihTlanoitaNehtfoetadpunatub
.weiver1991s'licnuoChcraeseRehtfoemosfoselpmaxeseviG
otgnidael,dehsilbupseiduts.noisulcnoccitsilaer
7991reveS.ecnediveehtsitahw:stceffehtlaehdnanoitanimatnoclatnemnorivnE.ELreveS htlaeHlairtsudnI&ygolocixoT ;03nuJ-raM7991
.16-541:)3-2(31
suodrazaHdnaetsaw
latnemnorivnefosllips
suodrazahsecnatsbus
ton-ygetartshcraesticilpxEdetats
elbaliavallaedulcniottroffEon-seiduts
cihpargoilbibdehcraeSdetatston-sesabatad
ton-stroperhsilgnE-noNdetats
41 evitseggusswohsweiverruO"nahtrehtar,ecnedive
snoitaicossarof,gnicnivnocroytimixorprehtieneewteb
etsawsuodrazahoterusopxelatinegnocdnasetis
nostceffednasnoitamroflam".thgiewhtrib
fosnoitatimilfonoissucsidlufesUygoloimedipelatnemnorivnelacigolodohtemnognisucof.seidutsdetcelesfostcepsa
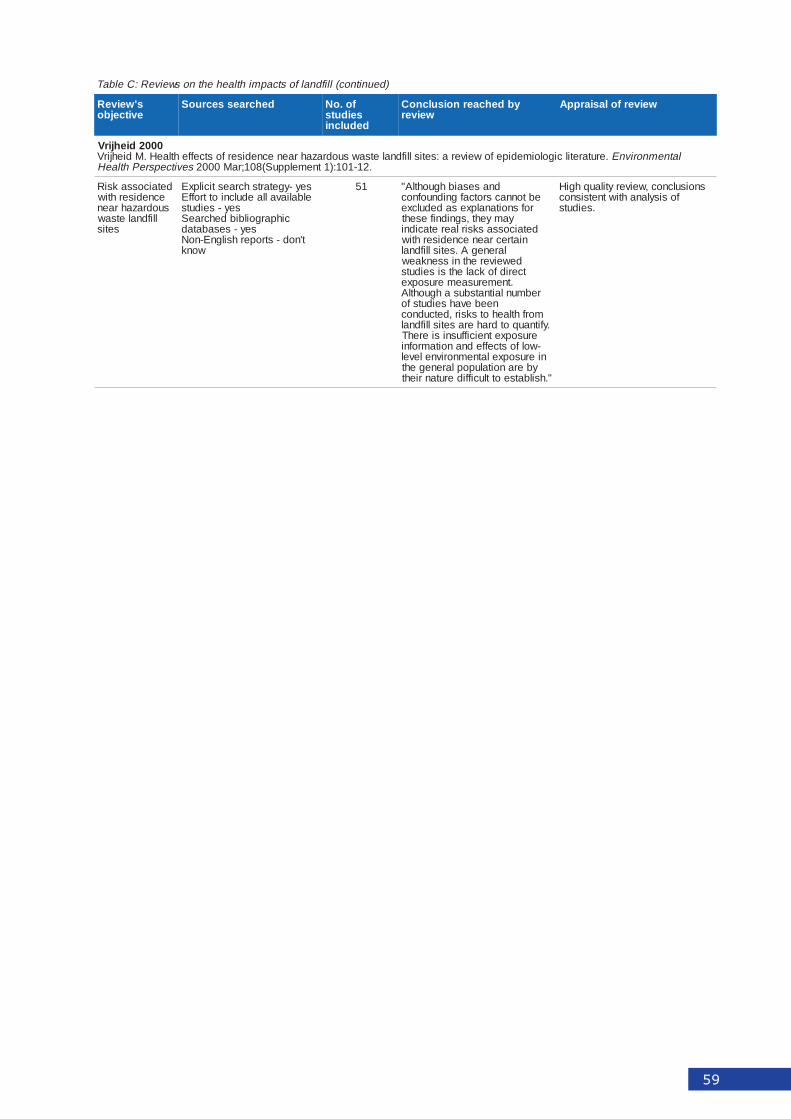
59
)deunitnoc(llifdnalfostcapmihtlaehehtnosweiveR:CelbaT
s'weiveRevitcejbo
dehcraessecruoS fo.oNseiduts
dedulcni
ybdehcaernoisulcnoCweiver
weiverfolasiarppA
0002diehjirV.erutaretilcigoloimedipefoweivera:setisllifdnaletsawsuodrazahraenecnediserfostceffehtlaeH.MdiehjirV latnemnorivnE
sevitcepsrePhtlaeH .21-101:)1tnemelppuS(801;raM0002
detaicossaksiRecnediserhtiwsuodrazahraen
llifdnaletsawsetis
sey-ygetartshcraesticilpxEelbaliavallaedulcniottroffE
sey-seidutscihpargoilbibdehcraeS
sey-sesabatadt'nod-stroperhsilgnE-noN
wonk
15 dnasesaibhguohtlA"ebtonnacsrotcafgnidnuofnoc
rofsnoitanalpxesadedulcxeyamyeht,sgnidnifeseht
detaicossasksirlaeretacidniniatrecraenecnediserhtiw
larenegA.setisllifdnaldeweiverehtnissenkaew
tceridfokcalehtsiseiduts.tnemerusaemerusopxe
rebmunlaitnatsbusahguohtlAneebevahseidutsfo
morfhtlaehotsksir,detcudnoc.yfitnauqotdraherasetisllifdnal
erusopxetneiciffusnisierehT-wolfostceffednanoitamrofninierusopxelatnemnorivnelevel
yberanoitalupoplarenegeht".hsilbatseottluciffiderutanrieht
snoisulcnoc,weiverytilauqhgiHfosisylanahtiwtnetsisnoc
.seiduts
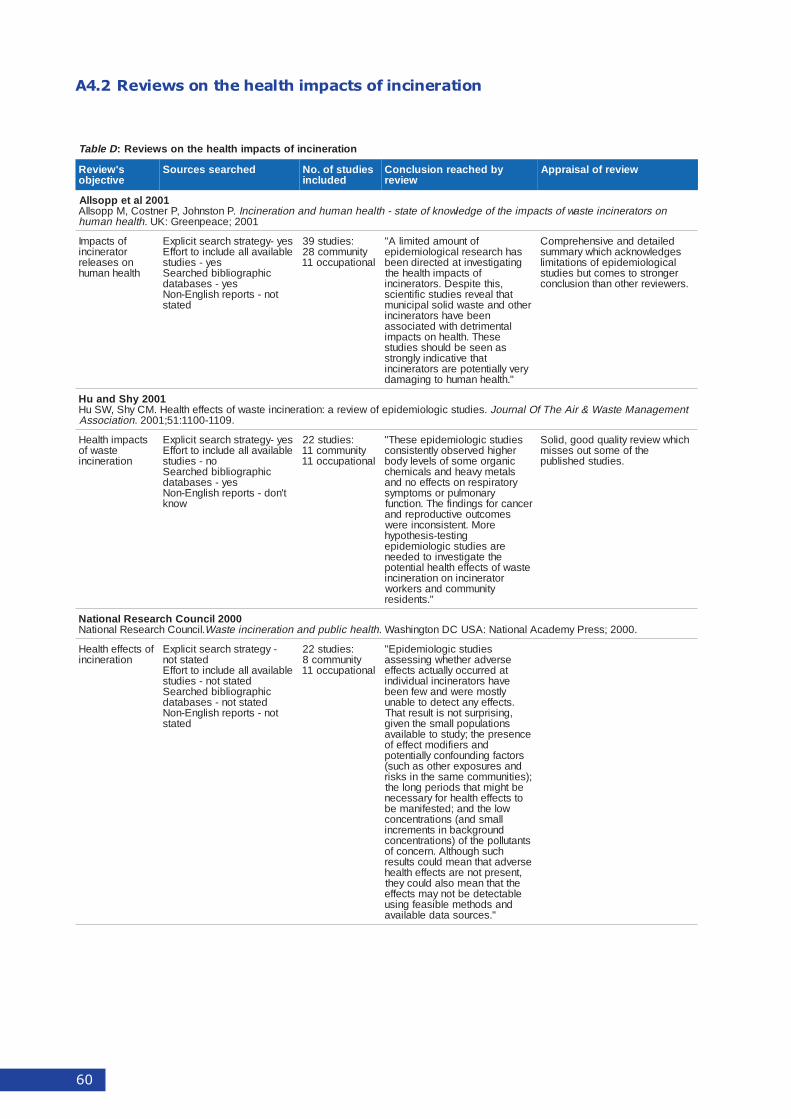
60
A4.2 Reviews on the health impacts of incineration
DelbaT noitarenicnifostcapmihtlaehehtnosweiveR:
s'weiveRevitcejbo
dehcraessecruoS seidutsfo.oNdedulcni
ybdehcaernoisulcnoCweiver
weiverfolasiarppA
1002latepposllA.PnotsnhoJ,PrentsoC,MpposllA nosrotarenicnietsawfostcapmiehtfoegdelwonkfoetats-htlaehnamuhdnanoitarenicnI
.htlaehnamuh 1002;ecaepneerG:KU
fostcapmIrotarenicninosesaeler
htlaehnamuh
sey-ygetartshcraesticilpxEelbaliavallaedulcniottroffE
sey-seidutscihpargoilbibdehcraeS
sey-sesabatadton-stroperhsilgnE-noN
detats
:seiduts93ytinummoc82
lanoitapucco11
fotnuomadetimilA"sahhcraeserlacigoloimedipegnitagitsevnitadetceridneeb
fostcapmihtlaeheht,sihtetipseD.srotarenicni
tahtlaeverseidutscifitneicsrehtodnaetsawdiloslapicinum
neebevahsrotarenicnilatnemirtedhtiwdetaicossa
esehT.htlaehnostcapmisaneesebdluohsseiduts
tahtevitacidniylgnortsyrevyllaitnetoperasrotarenicni
".htlaehnamuhotgnigamad
deliateddnaevisneherpmoCsegdelwonkcahcihwyrammuslacigoloimedipefosnoitatimilregnortsotsemoctubseiduts
.sreweiverrehtonahtnoisulcnoc
1002yhSdnauH.seidutscigoloimedipefoweivera:noitarenicnietsawfostceffehtlaeH.MCyhS,WSuH tnemeganaMetsaW&riAehTfOlanruoJ
noitaicossA .9011-0011:15;1002.
stcapmihtlaeHetsawfo
noitarenicni
sey-ygetartshcraesticilpxEelbaliavallaedulcniottroffE
on-seidutscihpargoilbibdehcraeS
sey-sesabatadt'nod-stroperhsilgnE-noN
wonk
:seiduts22ytinummoc11
lanoitapucco11
seidutscigoloimedipeesehT"rehgihdevresboyltnetsisnoccinagroemosfoslevelydobslatemyvaehdnaslacimehcyrotaripsernostceffeondna
yranomluprosmotpmysrecnacrofsgnidnifehT.noitcnuf
semoctuoevitcudorperdnaeroM.tnetsisnocnierew
gnitset-sisehtopyheraseidutscigoloimedipe
ehtetagitsevniotdedeenetsawfostceffehtlaehlaitnetop
rotarenicninonoitarenicniytinummocdnasrekrow
".stnediser
hcihwweiverytilauqdoog,diloSehtfoemostuosessim
.seidutsdehsilbup
0002licnuoChcraeseRlanoitaN.licnuoChcraeseRlanoitaN htlaehcilbupdnanoitarenicnietsaW .0002;sserPymedacAlanoitaN:ASUCDnotgnihsaW.
fostceffehtlaeHnoitarenicni
-ygetartshcraesticilpxEdetatston
elbaliavallaedulcniottroffEdetatston-seiduts
cihpargoilbibdehcraeSdetatston-sesabatad
ton-stroperhsilgnE-noNdetats
:seiduts22ytinummoc8
lanoitapucco11
seidutscigoloimedipE"esrevdarehtehwgnissessataderruccoyllautcastceffeevahsrotarenicnilaudividni
yltsomerewdnawefneeb.stceffeynatcetedotelbanu,gnisirprustonsitlusertahT
snoitalupopllamsehtnevigecneserpeht;ydutsotelbaliava
dnasreifidomtceffefosrotcafgnidnuofnocyllaitnetopdnaserusopxerehtosahcus(
;)seitinummocemasehtnisksirebthgimtahtsdoirepgnolehtotstceffehtlaehrofyrassecen
wolehtdna;detsefinamebllamsdna(snoitartnecnocdnuorgkcabnistnemercni
stnatullopehtfo)snoitartnecnochcushguohtlA.nrecnocfo
esrevdatahtnaemdluocstluser,tneserptonerastceffehtlaeh
ehttahtnaemosladluocyehtelbatcetedebtonyamstceffe
dnasdohtemelbisaefgnisu".secruosatadelbaliava
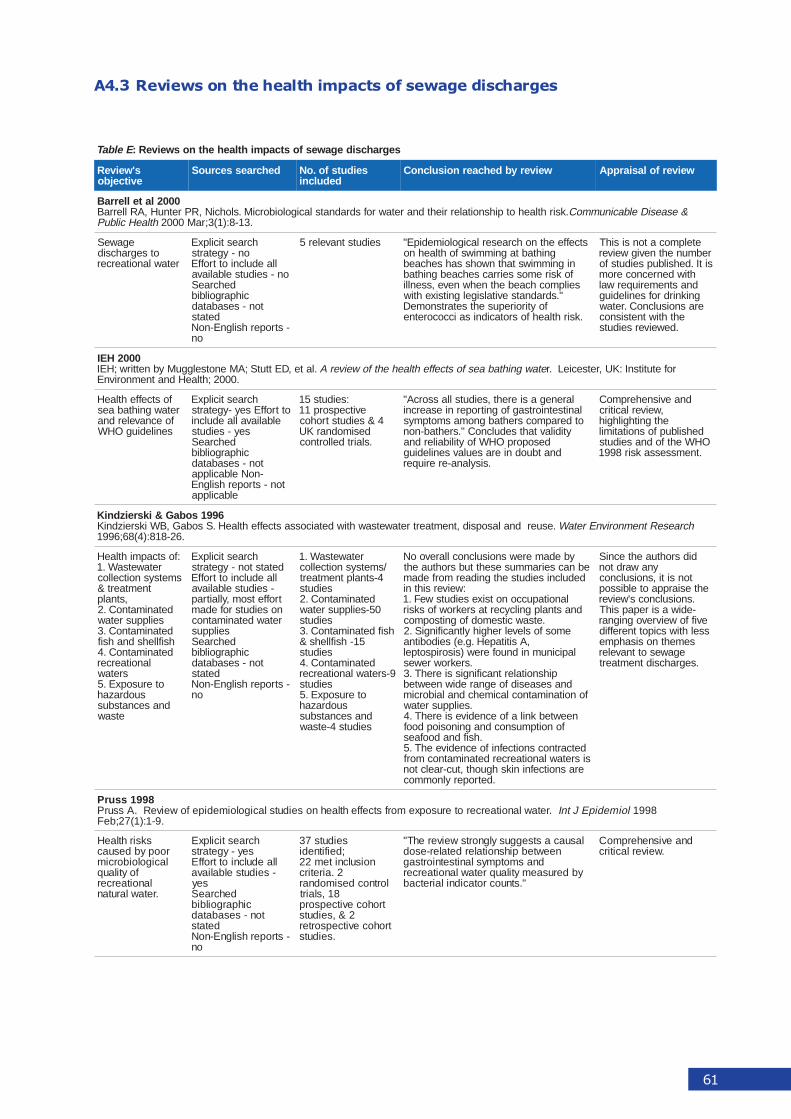
61
A4.3 Reviews on the health impacts of sewage discharges
EelbaT segrahcsidegawesfostcapmihtlaehehtnosweiveR:
s'weiveRevitcejbo
dehcraessecruoS seidutsfo.oNdedulcni
weiverybdehcaernoisulcnoC weiverfolasiarppA
0002latellerraB.ksirhtlaehotpihsnoitalerriehtdnaretawrofsdradnatslacigoloiborciM.slohciN,RPretnuH,ARllerraB &esaesiDelbacinummoC
htlaeHcilbuP .31-8:)1(3;raM0002
egaweSotsegrahcsid
retawlanoitaercer
hcraesticilpxEon-ygetarts
llaedulcniottroffEon-seidutselbaliava
dehcraeScihpargoilbib
ton-sesabataddetats
-stroperhsilgnE-noNon
seidutstnaveler5 stceffeehtnohcraeserlacigoloimedipE"gnihtabtagnimmiwsfohtlaehno
nignimmiwstahtnwohssahsehcaebfoksiremosseirracsehcaebgnihtabseilpmochcaebehtnehwneve,ssenlli
".sdradnatsevitalsigelgnitsixehtiwfoytiroirepusehtsetartsnomeD
.ksirhtlaehfosrotacidnisaiccocoretne
etelpmocatonsisihTrebmunehtnevigweiversitI.dehsilbupseidutsfo
htiwdenrecnoceromdnastnemeriuqerwalgniknirdrofsenilediugerasnoisulcnoC.retaw
ehthtiwtnetsisnoc.deweiverseiduts
0002HEI.late,DEttutS;AMenotselgguMybnettirw;HEI etawgnihtabaesfostceffehtlaehehtfoweiverA rofetutitsnI:KU,retsecieL.r
.0002;htlaeHdnatnemnorivnE
fostceffehtlaeHretawgnihtabaes
foecnavelerdnasenilediugOHW
hcraesticilpxEottroffEsey-ygetarts
elbaliavallaedulcnisey-seiduts
dehcraeScihpargoilbib
ton-sesabatad-noNelbacilppa
ton-stroperhsilgnEelbacilppa
:seiduts51evitcepsorp11
4&seidutstrohocdesimodnarKU.slairtdellortnoc
larenegasiereht,seidutsllassorcA"lanitsetniortsagfognitroperniesaercniotderapmocsrehtabgnomasmotpmys
ytidilavtahtsedulcnoC".srehtab-nondesoporpOHWfoytilibailerdna
dnatbuodnieraseulavsenilediug.sisylana-ereriuqer
dnaevisneherpmoC,weiverlacitircehtgnithgilhgih
dehsilbupfosnoitatimilOHWehtfodnaseiduts.tnemssessaksir8991
6991sobaG&iksreizdniK.esuerdnalasopsid,tnemtaertretawetsawhtiwdetaicossastceffehtlaeH.SsobaG,BWiksreizdniK hcraeseRtnemnorivnEretaW
.62-818:)4(86;6991
:fostcapmihtlaeHretawetsaW.1
smetsysnoitcelloctnemtaert&
,stnalpdetanimatnoC.2
seilppusretawdetanimatnoC.3hsifllehsdnahsifdetanimatnoC.4
lanoitaercersretaw
oterusopxE.5suodrazah
dnasecnatsbusetsaw
hcraesticilpxEdetatston-ygetarts
llaedulcniottroffE-seidutselbaliava
troffetsom,yllaitrapnoseidutsrofedamretawdetanimatnoc
seilppusdehcraeS
cihpargoilbibton-sesabatad
detats-stroperhsilgnE-noN
on
retawetsaW.1/smetsysnoitcelloc
4-stnalptnemtaertseiduts
detanimatnoC.205-seilppusretaw
seidutshsifdetanimatnoC.3
51-hsifllehs&seiduts
detanimatnoC.49-sretawlanoitaercer
seidutsoterusopxE.5
suodrazahdnasecnatsbusseiduts4-etsaw
ybedamerewsnoisulcnocllarevooNebnacseirammusesehttubsrohtuaeht
dedulcniseidutsehtgnidaermorfedam:weiversihtni
lanoitapucconotsixeseidutsweF.1dnastnalpgnilcycertasrekrowfosksir
.etsawcitsemodfognitsopmocemosfoslevelrehgihyltnacifingiS.2
,AsititapeH.g.e(seidobitnalapicinumnidnuoferew)sisoripsotpel
.srekrowrewespihsnoitalertnacifingissierehT.3
dnasesaesidfoegnarediwneewtebfonoitanimatnoclacimehcdnalaiborcim
.seilppusretawneewtebknilafoecnedivesierehT.4
fonoitpmusnocdnagninosiopdoof.hsifdnadoofaes
detcartnocsnoitcefnifoecnediveehT.5sisretawlanoitaercerdetanimatnocmorf
erasnoitcefninikshguoht,tuc-raelcton.detroperylnommoc
didsrohtuaehtecniSynawardton
tonsiti,snoisulcnocehtesiarppaotelbissop
.snoisulcnocs'weiver-ediwasirepapsihT
eviffoweivrevognignarsselhtiwscipottnereffid
semehtnosisahpmeegawesottnaveler
.segrahcsidtnemtaert
8991ssurP.retawlanoitaerceroterusopxemorfstceffehtlaehnoseidutslacigoloimedipefoweiveR.AssurP loimedipEJtnI 8991
.9-1:)1(72;beF
sksirhtlaeHroopybdesuaclacigoloiborcim
foytilauqlanoitaercer.retawlarutan
hcraesticilpxEsey-ygetarts
llaedulcniottroffE-seidutselbaliava
seydehcraeS
cihpargoilbibton-sesabatad
detats-stroperhsilgnE-noN
on
seiduts73;deifitnedi
noisulcnitem222.airetirc
lortnocdesimodnar81,slairt
trohocevitcepsorp2&,seiduts
trohocevitcepsorter.seiduts
lasuacastseggusylgnortsweiverehT"neewtebpihsnoitalerdetaler-esod
dnasmotpmyslanitsetniortsagybderusaemytilauqretawlanoitaercer
".stnuocrotacidnilairetcab
dnaevisneherpmoC.weiverlacitirc
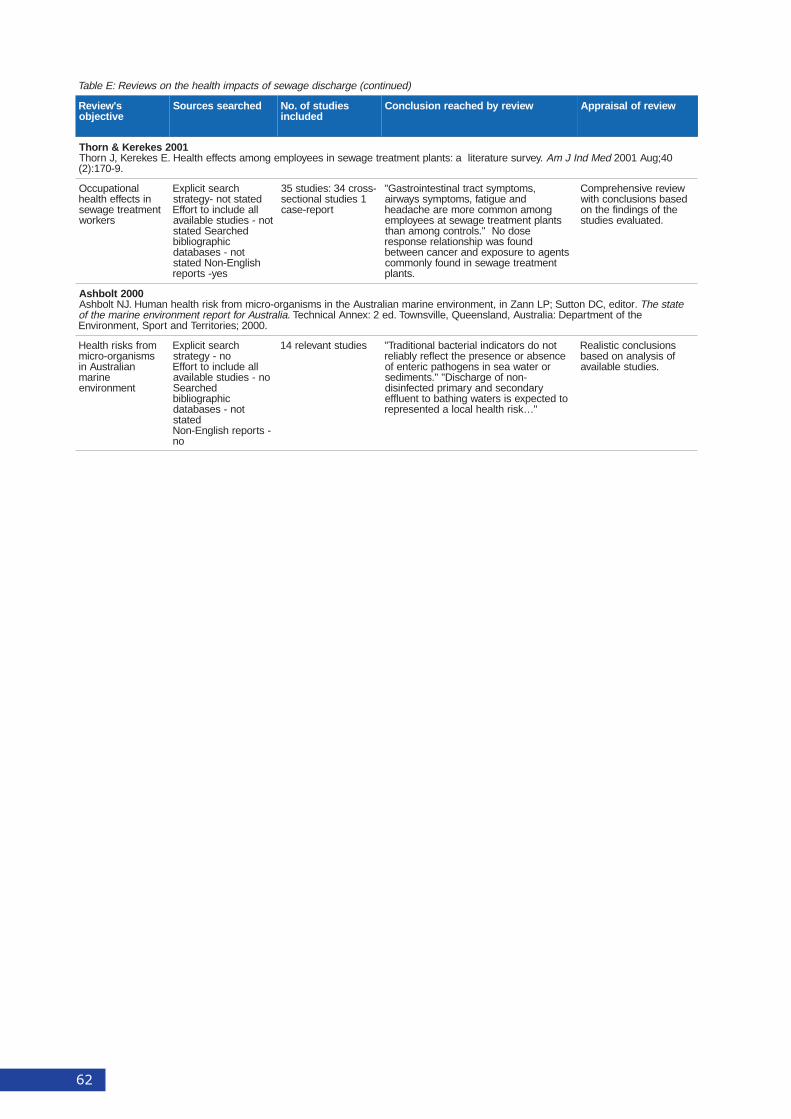
62
)deunitnoc(egrahcsidegawesfostcapmihtlaehehtnosweiveR:EelbaT
s'weiveRevitcejbo
dehcraessecruoS seidutsfo.oNdedulcni
weiverybdehcaernoisulcnoC weiverfolasiarppA
1002sekereK&nrohT.yevruserutaretila:stnalptnemtaertegawesniseeyolpmegnomastceffehtlaeH.EsekereK,JnrohT deMdnIJmA 04;guA1002
.9-071:)2(
lanoitapuccOnistceffehtlaeh
tnemtaertegawessrekrow
hcraesticilpxEdetatston-ygetartsllaedulcniottroffE
ton-seidutselbaliavadehcraeSdetats
cihpargoilbibton-sesabatad
hsilgnE-noNdetatssey-stroper
-ssorc43:seiduts531seidutslanoitces
troper-esac
,smotpmystcartlanitsetniortsaG"dnaeugitaf,smotpmyssyawria
gnomanommoceromeraehcadaehstnalptnemtaertegawestaseeyolpme
esodoN".slortnocgnomanahtdnuofsawpihsnoitaleresnopser
stnegaoterusopxednarecnacneewtebtnemtaertegawesnidnuofylnommoc
.stnalp
weiverevisneherpmoCdesabsnoisulcnochtiw
ehtfosgnidnifehtno.detaulaveseiduts
0002tlobhsArotide,CDnottuS;PLnnaZni,tnemnorivneeniramnailartsuAehtnismsinagro-orcimmorfksirhtlaehnamuH.JNtlobhsA etatsehT.
ailartsuAroftropertnemnorivneeniramehtfo ehtfotnemtrapeD:ailartsuA,dnalsneeuQ,ellivsnwoT.de2:xennAlacinhceT..0002;seirotirreTdnatropS,tnemnorivnE
morfsksirhtlaeHsmsinagro-orcim
nailartsuAnieniram
tnemnorivne
hcraesticilpxEon-ygetarts
llaedulcniottroffEon-seidutselbaliava
dehcraeScihpargoilbib
ton-sesabataddetats
-stroperhsilgnE-noNon
seidutstnaveler41 tonodsrotacidnilairetcablanoitidarT"ecnesbaroecneserpehttcelferylbailer
roretawaesnisnegohtapciretnefo-nonfoegrahcsiD"".stnemides
yradnocesdnayramirpdetcefnisidotdetcepxesisretawgnihtabottneulffe
"…ksirhtlaehlacoladetneserper
snoisulcnoccitsilaeRfosisylananodesab
.seidutselbaliava