vol 1 issue 6 eng definitivo
TRANSCRIPT

Nov-Dec 2015 | vol. 1 | issue 6 www.hysteroscopy.info
INSIDE THIS ISSUE
WELCOME 1
Interview of the month 3
My point of view 5
Highlights articles 8
What's your diagnosis? 10
Talking about 11
Devices 14
Hysteroscopy Basic 15
My experience 20
1
The field of Ob/Gyn is rapidly evolving and keeps dividing into an ever-growing number of sub-disciplines. Some are actual new fields and some are based on procedures, operations or tools that are perfected to levels that require an expert who has mastered them to the highest level. Hysteroscopy is such example. Hysteroscopy is a very valuable tool that is being used with increasing frequency for diagnosis and treatment in Ob/Gyn and infertility. Some intrauterine interventions, like treatment of Asherman’s syndrome, intramural fibroids, adenomyosis, and even resection of large polyps, carry a risk of damaging the endometrium, the integrity of which is of prime importance for normal implantation. Hence a high level of competence is required to perform them. The selection of the instrument used to perform the operation can also be crucial for future fertility. For example, using blunt dissection, scissors, or electrocautery to treat intrauterine adhesions can result in different degrees of irreversible damage to the endometrium. Long term follow up is mandatory in order to appreciate the results of such treatment. However, some of the dedicated hysteroscopists never see the patients again after the operation. The patients return to their reproductive specialist who has to deal with the results whether good or bad. To achieve the best results it is clear that the endoscopist should be part of the IVF team and have continuous follow up on the quality of his work and the appropriateness of the mode of operation. On the other hand, the reproductive specialist must not entrust hysteroscopy fully to the expert endoscopist. Some reproductive experts are also very fine endocrinologists and can provide consultation for example on menopause or family planning. Others are skillful surgeons or endoscopists that can treat fibroids, endometriosis, cysts, or re-implantation of ovarian tissue. Equally all reproductive specialists should be trained to at least do diagnostic hysteroscopy. Diagnostic hysteroscopy remains a central tool in preparation for IVF treatment and more so in the evaluation of implantation failure, despite the fact that it has not been proven that routine examination results in better success in IVF, compared to controls. It is within the interest of the patient to be served by physicians who are aware or master a “large toolbox” which promises the right selection of the proper intervention. The reproductive specialist who performs the examination or refers the patient to a more advanced operation should be well trained and familiar with the procedure and its possible complications. The World Congress on Controversies in Obstetrics, Gynecology and infertility - COGI - is a concept congress that was established to serve today’s busy clinicians who are interested in more than one field. COGI serves as an umbrella to all sub-disciplines in our field and brings together world imminent speakers from all sub-disciplines under one roof, to tackle clinical and therapeutic issues. The congress adopted the debate format and deals mainly with unsettled topics that are lacking the required evidence, leaving ample time for discussion between the audience and speakers.
In contrast to the plethora of monothematic congresses, COGI tries to appraise the ObGyn discipline as a whole. The message is that it is within the interest of the physicians to be updated on the major changes that are taking place frequently. This includes not only, infertility, IVF and perinatology but also gynecology, endoscopy, endometriosis, gyne-oncology, uro-gynecology, HPV, infections etc. COGI audiences enjoy being quickly and efficiently updated on the burning issues in the field.
Prof. Zion Ben-Rafael
HYSTEROSCOPY PICTURES
2
TEAM COODINATORSPAIN
L. Alonso
EDITORIAL COMMITTEE
SPAINE. Cayuela
L. Nieto
ITALYG. Gubbini
A. S. Laganà
USAJ. CarugnoL. Bradley
MEXICOJ. Alanis-Fuentes
PORTUGALJ. Metello
ARGENTINA A. M. Gonzalez
VENEZUELAJ. Jimenez
SCIENTIFIC COMMITTEE
A. Tinelli (ITA)A. Úbeda (Spa)A. Arias (Ven)
M. Rodrigo (Spa)A. Di Spiezio Sardo (Ita)
E. de la Blanca (Spa)J. Rios (Spa)
M. Bigozzi (Arg)S. Haimovich (Spa)
R. Lasmar (Bra)A. Garcia (USA)N. Malhotra (Ind)
J. Dotto (Arg)I. Alkatout (Ger)
R. Manchanda (Ind)
All rights reserved. The responsibility of the signed contributions is primarily of the authors and does not necessarily reflect the views of the editorial
or scientific committees.
HYSTEROSCOPY
PICTURES
www.hysteroscopy.info
2
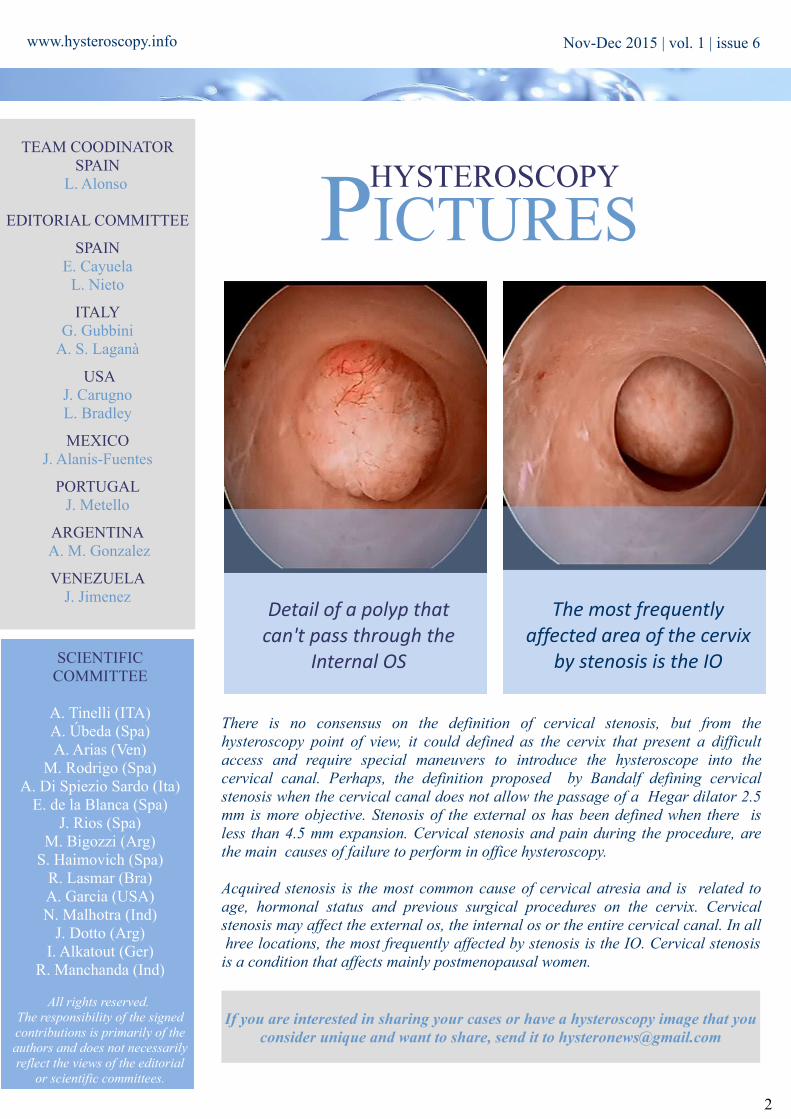
There is no consensus on the definition of cervical stenosis, but from the hysteroscopy point of view, it could defined as the cervix that present a difficult access and require special maneuvers to introduce the hysteroscope into the cervical canal. Perhaps, the definition proposed by Bandalf defining cervical stenosis when the cervical canal does not allow the passage of a Hegar dilator 2.5 mm is more objective. Stenosis of the external os has been defined when there is less than 4.5 mm expansion. Cervical stenosis and pain during the procedure, are the main causes of failure to perform in office hysteroscopy.
Acquired stenosis is the most common cause of cervical atresia and is related to age, hormonal status and previous surgical procedures on the cervix. Cervical stenosis may affect the external os, the internal os or the entire cervical canal. In all hree locations, the most frequently affected by stenosis is the IO. Cervical stenosis is a condition that affects mainly postmenopausal women.
Detail of a polyp that can't pass through the
Internal OS
The most frequently affected area of the cervix
by stenosis is the IO
If you are interested in sharing your cases or have a hysteroscopy image that you consider unique and want to share, send it to [email protected]
Nov-Dec 2015 | vol. 1 | issue 6
3
www.hysteroscopy.info
INTERVIEW WITH... To talk about Dr. I. Mazzon is to talk about innovation in hysteroscopic myomectomy. His “cold loop” technique is something that all ginecologists should know. He is the head of the department of the “Arbor Vitae” endoscopic centre in Rome
Watch this video of a hysteroscopic myomectomy using Mechanical
loops of Mazzon.
Ivan MazzonHead of the department
Endoscopic Centre “Arbor Vitae”Roma. Italy
You were the first in use the term “cold loop myomectomy” . Do you think that the technique is well known?? At the beginning of nineties, for the first time I presented the “cold loop” hysteroscopic myomectomy at the National Congress of the Italian Society of Gynecologic Endoscopy. In the following years, this technique was spread among Italian endoscopic surgeons and nowadays the majority of Endoscopic Centres in Italy, routinely performing hysteroscopic myomectomy, utilizes “the cold loop technique” for the treatment of G1 and G2 myomas. Until now, outside Italy few Centres in USA, Belgium, Germany, England, South America know and perform such technique. Unfortunately, only in the last years I started to publish data about the cold loop technique in international Journals and probably for this reason the technique is still not utilised in all over the world. Nevertheless, I am noticing an international growing interest on the cold loop hysteroscopic myomectomy.
Can you make a brief resume of the technique and its advantages? The technique is articulated in two phases: 1) Slicing the Intracavitary Component of the Myoma The intracavitary component of myoma is removed using the conventional slicing technique powered by monopolar or bipolar current (in pure cutting mode). When the cleavage plane between the myoma and myometrium is identified, the slicing has to be stopped. In order to identify the correct cleavage plane between myoma and myometrium, it is very important to reach accurately the plane of the endometrial surface: remaining above or falling below of such plane makes it difficult to recognize the correct dissection plane.
2) Enucleation of the Intramural Component of the Myoma The electric cutting loop is subsequently replaced with a not electrified cold loop (mechanical loops of Mazzon; Karl Storz, Tuttlingen, Germany). Usually, it is better to start with the “straight cold loop” (the most atraumatic), which is inserted into the cleavage plane and applied repeatedly along the surface of the myoma. In this way, the connective fibers anchoring the myoma to the pseudocapsule are disconnected by blunt dissection. In case of wide and tough fibro-connectival bridges, it is useful to resort to the “rake-shaped” or to the “knife-shaped” cold loops. In this way, the intramural component of myoma is progressively detached from the myometrium and becomes an endocavitary neoformation, safely removable by slicing. In case of myomas of large volume, it is possible to repeat for more times this phase.
The main objective of the “cold loop hysteroscopic myomectomy” is to avoid the contact of the electrical cutting loop with the myometrium: in this way it is possible to achieve efficacy and safety. a – the tissues are preserved from the thermal injury caused by the electric energy. In this way, the myoma, the myometrium and the cleavage plane between myoma and pseudocapsule are easily distinguishable;
https://www.youtube.com/watch?v=QoCX8aKPAb8
Nov-Dec 2015 | vol. 1 | issue 6
4
www.hysteroscopy.info
b – uterine perforation with the electrical thermal loop is virtually eliminated; c – avoiding the damage of the healthy myometrium, the risk of haemorrhage and post-surgical intrauterine synechiae is reduced. Indeed, haemostatic contraction of the myometrium is maintained and the fibrous reaction caused by the thermal injury is avoided; d – the thickness of the free myometrial margin loses its importance; e – the chance to accomplish the treatment of G1 or G2 myomas in only one surgical step is greatly improved; only the achievement of a critical value limit in absorption of distension media could need the interruption of the procedure and so the scheduling of a new surgical step to complete the treatment.
Which are the limits of the single step hysteroscopic myomectomy? Theoretically, every submucous myoma may be removed hysteroscopically in only onesurgical step. Nevertheless, the limit is determined by the absorption of the distension media and such limit may significantly change according to the surgeon experience. The surgeons should treat only submucous myomas that really are able to remove.
How important are the courses and the “hands on” training in hysteroscopy? Since over 20 years I organize courses in which the “hands on training” has great importance. They are fundamental in order to know correctly the instruments and the surgical gesturing. The courses and the “hands on trainings” should always come first to the learning pathway during the clinical practice.
You have published some books and atlas in DVD. Can hysteroscopy be improved with the use of audiovisual aids? Books, atlas, DVD and all multimedia instruments are important to build the necessary knowledge in hysteroscopy but, as usual, they may be insufficient without an adequate training during courses or in Endoscopic Centres setting with a tutoring carried out by expert surgeons.
Do you have any advice for the young physician that is starting out in the world of gynecologic minimally invasive surgery?" Being a minimally invasive surgery, the great fault, (and in the same time the most frequent) is to consider the hysteroscopic surgery as a procedure extremely easy to accomplish and therefore to believe that it requests a “minimal” training commitment. Unfortunately, a bad use of such surgery may be characterized by serious complications. There are several reports in the scientific literature about it. As for all surgical techniques, it is necessary a correct learning pathway, which allows a real knowledge of the uterus anatomy and the uterine cavity (the diagnostic hysteroscopy has a fundamental role), a suitable comprehension of the instrumentations utilised and an adequate learning curve. I believe that only in this way the hysteroscopic surgery can be performed with efficacy and safety.
“The main objective of the “cold loop hysteroscopic myomectomy”
is to avoid the contact of the electrical cutting loop with the myometrium”
Nov-Dec 2015 | vol. 1 | issue 6
“ .. the great fault, (and in the same time the most frequent) is to consider
the hysteroscopic surgery as a procedure extremely easy to accomplish”
www.hysteroscopy.info
5
Recently the press has echoed the demands made by a group of women who claim had adverse effects after placement of Essure ® devices, demanding the withdrawal of the device off the market.
Currently, the FDA has received a significant increased number of reports of adverse effects, which include: chronic pelvic pain, fatigue, headaches, hair loss, depression and pregnancy. Similarly, there are social networking groups who support these claims, and even the famous activist Erin Brockovich leads a popular campaign against Essure ®.
I am a firm believer of the virtues of Essure ® and the benefits that this device offered to thousands of women who had it inserted without any side effect, gives me no choice but to rethink the current situation and ask the following questions: What is the real extent of the problem?, What is the severity of the complications? And, in my opinion, the most important question: What can we do to avoid or minimize them?
There is a social alarm that objectively quantifies 7000 complaints to the FDA, and others that are yet to be reported to the EMA (European Medicines Agency). Moreover, the MAUDE database registry of complications and unwanted pregnancies also appears inaccurate, because not all existing complications are reported. Conversely, there are complications that seem to be well defined, and have constantly been reported such as headaches, nausea, fatigue, hair loss, chronic pelvic pain, nickel allergy and heavy menstrual bleeding.
To establish a correlation between Essure® insertion and any given side effect, it must be demonstrated that the incidence of the specific symptom is higher in carriers of Essure ® than in the general population. Therefore, if we consider that these devices have been placed in over 800,000 women, it seems obvious that there is no correlation.
Another frequently reported complication is the claim of heavy menstrual bleeding after having Essure® inserted. The first thing to keep in mind is that between 30-50% of the carriers of Essure® were on hormonal contraceptives or had a levonorgestrel IUD before having Essure ®, so their menstrual cycles were medically controlled; translated into absolute numbers, between 240,000 to 400,000 women used hormonal contraception before having Essure ®, many women had decreased menstrual bleeding because of hormonal contraception. There is no scientific evidence to support higher incidence of heavy menstrual bleeding after placement of the devices. Moreover, in a survey conducted by our group in 1, 500 women carrying devices between 1 and 5 years, only 11% reported heavy menstrual bleeding, instead we had 9% of women who reported an improvement in their menstrual cycle. (1)
Regarding chronic pelvic pain, noted that the prevalence of it in the general population of women of reproductive age is 3.5%, which means that approximately 28,000 women who carry the Essure ® should have this type of pain regardless of the device. It has been noted, that in most cases the pain resolves with removal of Essure ®. Our grup (2) reported an incidence of chronic pelvic pain of 0.16% (7 cases), in 4274 women followed for seven years after placing the devices. In our series, the symptoms completely disappeared after the withdrawal of devices.
Essure: My point of viewJ. E. Arjona. Secretary- Treasure Spanish Society Obstetrics and Gybecology. Hospital Universitario Reina Sofía,
L. Nieto. Attending physician. Hospital Universitario Reina Sofía. Córdoba. Spain
Nov-Dec 2015 | vol. 1 | issue 6

www.hysteroscopy.info
6
Undoubtedly we must acknowledge that any foreign body can cause such symptoms, so when a patient reports this complication, the gynecologist should investigate the cause of pelvic pain. If the presence of the Essure ® is the suspected reason of the pain, it must be removed, ideally by hysteroscopy. Essure ® removal can be done by laparoscopy or using a hysteroscopy approach. Our group has reported a case of hysteroscopic Essure ® removal 12 years after insertion. To perform a hysteroscopic removal, there must be a large portion of the Essure ® inside the uterine cavity, that is why we should leave 6 to 8 rings inside the uterine cavity at the time of insertion to facilitate its removal by hysteroscopy if necessary. Another approach would be to offer laparoscopic bilateral salpingectomy to ensure effective permanent sterilization after removal of the devices.
History of pelvic inflammatory disease (PID), have been linked to an increased incidence of chronic pelvic pain, therefore we must inform patients with such a history that placement of Essure ® could lead to pelvic pain. On the other hand, it is known that the risks and complications of a laparoscopic sterilization procedures are also increased in patients with history of PID, leaving the patient with a complex decision in case of permanent sterilization desire.
Regarding nickel allergy, recent published data described the incidence in asymptomatic females at 15% (3), that is, women who are allergic to nickel and do not know it. Therefore, if the nickel produces an allergic reaction in all patients with hypersensitivity to this metal, this type of allergic reaction would have affected about 120,000 women. By contrast, only a very small number of women so far have been reported with nickel allergy symptoms after Essure ® insertion. Of note, this allergy is often associated with other skin diseases. As a side note of information, one must know that the amount of nickel that is absorbed in the diet is higher than the amount released by the implant.
Perforation at the time of insertion is another workhorse. Interestingly our group, where 99.9% of devices are placed in an office setting without anesthesia, has only had two holes in 7200 cases, which means that this complication occurs only in 0.03% (4). In premarketing studies the incidence of perforation was 1-1.5%. A very difficult and painful insertion suggests the possibility of perforation. In my opinion, sedation may increase the chance of perforation, and eliminates the cardinal symptom of this complication: pain. Therefore, all gynecologists should refine the insertion technique to be carried out without need of anesthesia.
Regarding the safety of the device, a recently (post-approval) 5 years follow-up study (5), revealed no new safety issue or higher incidence of complication from the ones already known and described in the insertion package instructions for use of Essure ®. This study also confirms the effectiveness of the device to prevent pregnancy after 5 years of use is 99.7%. Our group (6) published an absolute rate of 0.25% of pregnancies in 1200 women with a minimum follow-up of 5 years with a Pearl Index of 0.05 after 72 months of follow up.
A recent published paper (7) indicates that the possibility of reoperation in patients who underwent hysteroscopic sterilization is 10 times higher than laparoscopic sterilization. In this study, the characteristics of the patients included several serious comorbidities not equally distributed in both groups, so that the samples may not be comparable. The authors note that in general, patients with pelvic adhesions, or a history of pelvic inflammatory disease, had an increased risk of postoperative complications and traditionally these women were not considered laparoscopy candidates. Also, the term “reoperation” is not well defined, which seems somewhat vague since it does not distinguish between reoperations after hysteroscopic sterilization and a second attempt to place an Essure ® device after a first failed attempt. A common practice is to offer a second attempt after failure during the first insertion procedure. Another possibility is failure of bilateral tubal occlusion so the woman should be offered a laparoscopic tubal occlusion procedure. Finally, if after a confirmatory test, the placement of the devices is unsatisfactory, it requires removal. A laparoscopic tubal ligation should be offered to ensure sterilization.
Nov-Dec 2015 | vol. 1 | issue 6

www.hysteroscopy.info
7
Nov-Dec 2015 | vol. 1 | issue 6
Regardless of this publication (7) it is known that patients undergoing hysteroscopy tend to have more comorbidities than laparoscopy candidates (also statistically significant in their results), the authors of this article make a serious mistake, because the procedure identified as “intervention” (Essure ® insertion), is a minor, in office procedure performed without anesthesia, and the patient goes home immediately. That is, the authors of this paper are comparing a minor in office procedure with an invasive procedure such as laparoscopy, which requires surgical setting and general anesthesia. Based of that, I can affirm that the concept of this paper is wrong, in my opinion, in New York the Essure® has allow to avoid the need of 90% of laparoscopy surgery for permanent sterilization.
Finally, another recent publication (8) which refers to the design of pre-marketing studies Essure ® is also incorrect, but that is another issue to be discussed in future issues of this magazine. Simply a reflection, have you notice that it took them 13 years to realize this ?
Finally, as recommendations to minimize the possible risk I suggest:
- Report in detail and comprehensively to all users of the possible complications in the short and long term as well as the action to take for resolution.- Appropriate patient selection.- Be firm in the recommendation that women should come back for follow up three months after the procedure, as in this query the correct placement of the devices and tubal blockage is confirmed.- Provide a contact number to the patients so they can discuss any concerns or adverse effect after placement of the device.- Establish a network so that in the event of a complication appears, the woman easy access to find an adequate response in the shortest possible time.
References:
1- Velasco Sánchez E, Arjona Berral JE, Povedano Cañizares B. “Satisfaction of hysteroscopic tubal sterilization with Essure mictoinserts”. 18 annualCongress ESGEJ. 2- E. Arjona Berral, B. Rodríguez Jiménez, E. Velasco Sánchez, B. Povedano Cañizares, J. Monserrat Jordan, J. Lorente Gonzalez,C. Castelo-Branco . “Essure and chronic pelvic pain: A population-based cohort" . J Obstet Gynaecol. 2014 Nov;34(8):712-33- T.L. Diepgen, R.F. Ofenloch, M.Bruze, P. Bertuccio, S.Cazzaniga, P-J.Coenraads, P.Elsner, M.Goncalo, A.Svensson and L.Naldi. “Prevalence of contact allergy in the general population in different European regions”. Br J Dermatol. 2015 Sep 154- B Povedano,JE Arjona,E Velasco,JA Monserrat,J Lorente,C Castelo-Branco. “Complications of hysteroscopic Essure sterilisation: report on 4306 procedures performed in a single centre”. BJOG.2012 Jun;119(7):795-9.5- Scott G. Chudnoff, MD, MS, John E. NicholsJr, MD, and Mark Levie, MD.“Hysteroscopic Essure Inserts for Permanent Contraception: Extended Follow-Up Results of a Phase III Multicenter International Study”. J MinimInvasiveGynecol. 2015 Sep-Oct;22(6):951-606- José E. Ríos-Castillo, Esther Velasco, José E. Arjona-Berral, José A. Monserrat Jordán, Balbino Povedano-Cañizares, and Camil Castelo-Branco. “Efficacy of Essure hysteroscopic sterilization – 5 years follow up of 1200 women”. Gynecol Endocrinol.2013 Jun;29(6):580-27- Jialin Mao,SamanthaPfeifer,Peter Schlegel,Art Sedraky. “Safety and efficacy of hysteroscopic sterilization compared with laparoscopic sterilization: an observational cohort study”. BMJ.2015 Oct 13;351:h51628- Sanket S. Dhruva, M.D., Joseph S. Ross, M.D., M.H.S., and Aileen M. Gariepy, M.D., M.P.H.“Revisiting Essure — Toward Safe and Effective Sterilization”. N Engl J Med 2015 Oct8;373(15):e17
www.hysteroscopy.info
8
Comparing the effect of office hysteroscopy with endometrial scratch versus office hysteroscopy on intrauterine insemination outcome: a randomized controlled trial.
El-Khayat W, Elsadek M, Saber W.Eur J Obstet Gynecol Reprod Biol. 2015 Aug 28;194:96-100
Assessment of Abdominal Ultrasound Guidance in Hysteroscopic Metroplasty.Vigoureux S, Fernandez H, Capmas P, Levaillant JM, Legendre G.
J Minim Invasive Gynecol. 2015 Aug 28. pii: S1553-4650(15)01490-9.
Undoubtedly we must acknowledge that any foreign body can cause such symptoms, so when a patient reports this complication, the gynecologist should investigate the cause of pelvic pain. If the presence of the Essure ® is the suspected reason of the pain, it must be removed, ideally by hysteroscopy. Essure ® removal can be done by laparoscopy or using a hysteroscopy approach. Our group has reported a case of hysteroscopic Essure ® removal 12 years after insertion. To perform a hysteroscopic removal, there must be a large portion of the Essure ® inside the uterine cavity, that is why we should leave 6 to 8 rings inside the uterine cavity at the time of insertion to facilitate its removal by hysteroscopy if necessary. Another approach would be to offer laparoscopic bilateral salpingectomy to ensure effective permanent sterilization after removal of the devices.
History of pelvic inflammatory disease (PID), have been linked to an increased incidence of chronic pelvic pain, therefore we must inform patients with such a history that placement of Essure ® could lead to pelvic pain. On the other hand, it is known that the risks and complications of a laparoscopic sterilization procedures are also increased in patients with history of PID, leaving the patient with a complex decision in case of permanent sterilization desire.
Regarding nickel allergy, recent published data described the incidence in asymptomatic females at 15% (3), that is, women who are allergic to nickel and do not know it. Therefore, if the nickel produces an allergic reaction in all patients with hypersensitivity to this metal, this type of allergic reaction would have affected about 120,000 women. By contrast, only a very small number of women so far have been reported with nickel allergy symptoms after Essure ® insertion. Of note, this allergy is often associated with other skin diseases. As a side note of information, one must know that the amount of nickel that is absorbed in the diet is higher than the amount released by the implant.
Perforation at the time of insertion is another workhorse. Interestingly our group, where 99.9% of devices are placed in an office setting without anesthesia, has only had two holes in 7200 cases, which means that this complication occurs only in 0.03% (4). In premarketing studies the incidence of perforation was 1-1.5%. A very difficult and painful insertion suggests the possibility of perforation. In my opinion, sedation may increase the chance of perforation, and eliminates the cardinal symptom of this complication: pain. Therefore, all gynecologists should refine the insertion technique to be carried out without need of anesthesia.
Regarding the safety of the device, a recently (post-approval) 5 years follow-up study (5), revealed no new safety issue or higher incidence of complication from the ones already known and described in the insertion package instructions for use of Essure ®. This study also confirms the effectiveness of the device to prevent pregnancy after 5 years of use is 99.7%. Our group (6) published an absolute rate of 0.25% of pregnancies in 1200 women with a minimum follow-up of 5 years with a Pearl Index of 0.05 after 72 months of follow up.
A recent published paper (7) indicates that the possibility of reoperation in patients who underwent hysteroscopic sterilization is 10 times higher than laparoscopic sterilization. In this study, the characteristics of the patients included several serious comorbidities not equally distributed in both groups, so that the samples may not be comparable. The authors note that in general, patients with pelvic adhesions, or a history of pelvic inflammatory disease, had an increased risk of postoperative complications and traditionally these women were not considered laparoscopy candidates. Also, the term “reoperation” is not well defined, which seems somewhat vague since it does not distinguish between reoperations after hysteroscopic sterilization and a second attempt to place an Essure ® device after a first failed attempt. A common practice is to offer a second attempt after failure during the first insertion procedure. Another possibility is failure of bilateral tubal occlusion so the woman should be offered a laparoscopic tubal occlusion procedure. Finally, if after a confirmatory test, the placement of the devices is unsatisfactory, it requires removal. A laparoscopic tubal ligation should be offered to ensure sterilization.
OBJECTIVE: To compare the rates of re-intervention, and immediate and later complications associated with abdominal ultrasound-guided versus unguided hysteroscopic metroplasty in the surgical repair of ESHRE/ESGE class II intrauterine septa.DESIGN: We performed a large observational retrospective study (Canadian Task Force Classification II-2) in a selection of patients who underwent metroplasty in a tertiary university center between 2009 and 2013.PATIENTS: A total of 108 patients were included in the study.INTERVENTIONS: Patients were categorized as having abdominal ultrasound-guided metroplasty (n = 46) or unguided metroplasty (n = 62).MEASUREMENTS AND MAIN RESULTS: Data were collected with regard to medical and reproductive histories, diagnosis of septate uterus, surgical procedures, and complications. Using these data, the need for re-intervention and complication rates were compared between groups. Statistical analysis was performed using Fisher's exact test and Student's t-test. The characteristics of the 2 groups were comparable. A persistent septum of >10 mm, defined by 3-dimensional ultrasound hysterosonography, with a need for re-intervention, was found in 16 patients (39.0 %) in the unguided group versus 7 patients (18.4 %) in the ultrasound guidance group (p = .04). Risk of a persistent septum after resection (>10 mm) was reduced with ultrasound guidance (odds ratio = 0.35; 95% confidence interval 0.13-0.99). Two uterine perforations occurred in our series; both were in the unguided group.CONCLUSIONS: A systematic abdominal ultrasound-guided metroplasty by hysteroscopy seems to reduce the rates of re-intervention.
OBJECTIVE: To evaluate the role of endometrial injury in the cycle preceding ovarian stimulation for intrauterine insemination (IUI) cycle on the clinical pregnancy rate.STUDY DESIGN: This was a prospective randomized controlled trial which included three hundred and thirty two infertile women with an indication for IUI. The subjects were randomly divided into two groups. The intervention group (group A) (n=166) subjects underwent office hysteroscopy with endometrial injury using grasping forceps with teeth, while the control group (group B) (n=166) subjects underwent office hysteroscopy alone without endometrial injury. Primary outcome was clinical pregnancy rate.RESULTS: There were no significant differences in baseline or clinical characteristics between the groups. There were no significant differences in clinical pregnancy rate [13.8% (23/166) versus 12% (20/166); RR 1.15 (95% CI 0.66-2.01), p=0.62]. The abortion rate [4.3% (1/23) versus 15% (3/20); RR 0.29 (95% CI 0.03-2.57), p=0.27], the multiple pregnancy rate [13% (3/23) versus 15% (3/20); RR 0.87 (95% CI 0.20-3.83), p=0.85] and the live birth rate [13.6% (22/166) versus 10.4% (17/166); RR 1.28 (95% CI 0.71-2.32), p=0.42].CONCLUSION: There is no evidence of significant difference on the clinical pregnancy rate when endometrial scratching during hysteroscopy is compared to only hysteroscopy in women undergoing IUI.
HIGHLIGHT ARTICLESPublished on different medias
Nov-Dec 2015 | vol. 1 | issue 6

www.hysteroscopy.info
9
DID YOU KNOW...?
Pathogenetic mechanisms that link chronic endometritis with infertility, recurrent pregnancy loss and repeated implantation
failure are still unknown.
Joseph Asherman described the etiology, frequency, andsymptoms of intrauterine adhesions in 1948, it is
known as Asherman's syndrome
Nov-Dec 2015 | vol. 1 | issue 6
www.hysteroscopy.info
10
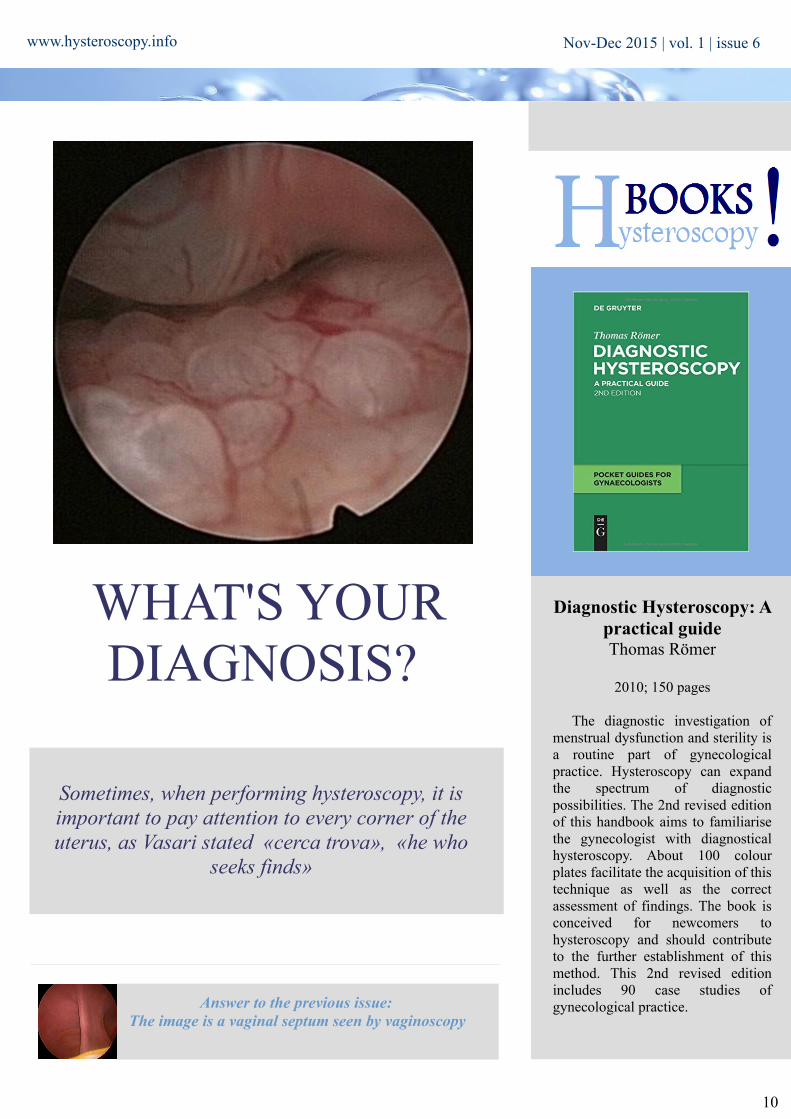
Diagnostic Hysteroscopy: A practical guideThomas Römer
2010; 150 pages
The diagnostic investigation of menstrual dysfunction and sterility is a routine part of gynecological practice. Hysteroscopy can expand the spectrum of diagnostic possibilities. The 2nd revised edition of this handbook aims to familiarise the gynecologist with diagnostical hysteroscopy. About 100 colour plates facilitate the acquisition of this technique as well as the correct assessment of findings. The book is conceived for newcomers to hysteroscopy and should contribute to the further establishment of this method. This 2nd revised edition includes 90 case studies of gynecological practice.
Sometimes, when performing hysteroscopy, it is important to pay attention to every corner of the uterus, as Vasari stated «cerca trova», «he who
seeks finds»
WHAT'S YOUR DIAGNOSIS?
Answer to the previous issue: The image is a vaginal septum seen by vaginoscopy
Nov-Dec 2015 | vol. 1 | issue 6
www.hysteroscopy.info
11
TALKING ABOUTRetained products of conception
L. Alonso. Centro Gutenberg. Málaga. Spain
The term retained products of conception refers to placental or fetal tissue that remains in the uterus after abortion, miscarriage or parturition. The estimated incidence is around 1% after term delivery and it is probably higher in cases of miscarriage and preterm delivery
There are two teories to explain why this happens, the one by Eastman and Hellman, in which they think that the RPOC probably represent a type of placental accreta and the one by Ranney who thinks that can be related to differences in the thickness and the contractility in different areas of myometrium. Maybe both of them are right
Clinical symptoms include bleeding, usually heavier than normal or prolongued than normal, abdominal pain and uterine tenderness. The diagnosis is based in clinical hystory and clinical symptoms, gynecological exam, ultrasound and hysteroscopy. The laboratory results have a limited value in this entity
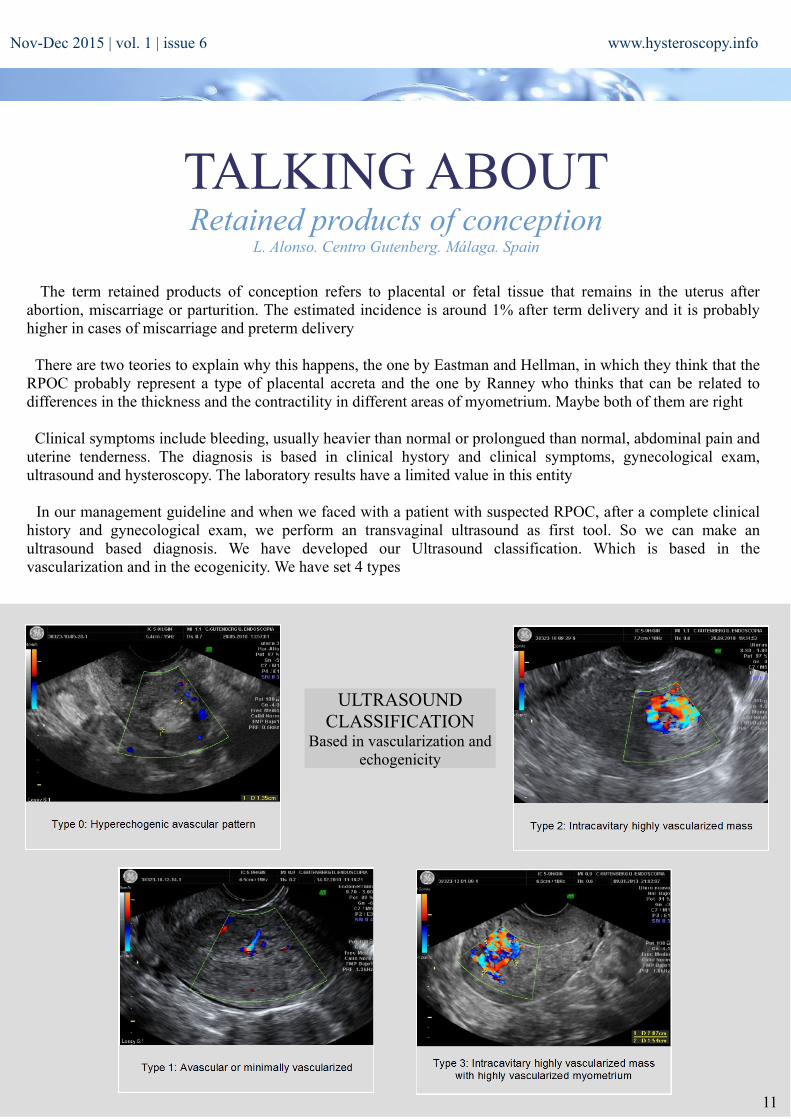
In our management guideline and when we faced with a patient with suspected RPOC, after a complete clinical history and gynecological exam, we perform an transvaginal ultrasound as first tool. So we can make an ultrasound based diagnosis. We have developed our Ultrasound classification. Which is based in the vascularization and in the ecogenicity. We have set 4 types
Nov-Dec 2015 | vol. 1 | issue 6
ULTRASOUND CLASSIFICATION
Based in vascularization and echogenicity
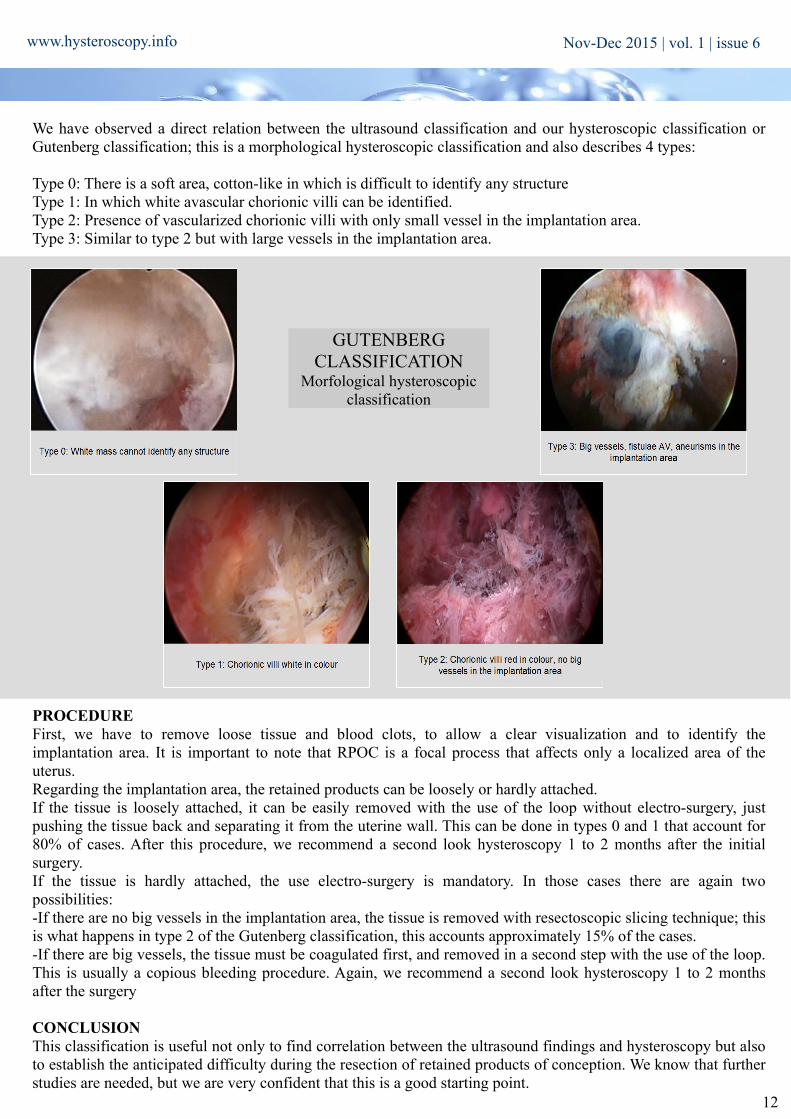
We have observed a direct relation between the ultrasound classification and our hysteroscopic classification or Gutenberg classification; this is a morphological hysteroscopic classification and also describes 4 types:
Type 0: There is a soft area, cotton-like in which is difficult to identify any structureType 1: In which white avascular chorionic villi can be identified.Type 2: Presence of vascularized chorionic villi with only small vessel in the implantation area.Type 3: Similar to type 2 but with large vessels in the implantation area.
PROCEDUREFirst, we have to remove loose tissue and blood clots, to allow a clear visualization and to identify the implantation area. It is important to note that RPOC is a focal process that affects only a localized area of the uterus.Regarding the implantation area, the retained products can be loosely or hardly attached.If the tissue is loosely attached, it can be easily removed with the use of the loop without electro-surgery, just pushing the tissue back and separating it from the uterine wall. This can be done in types 0 and 1 that account for 80% of cases. After this procedure, we recommend a second look hysteroscopy 1 to 2 months after the initial surgery.If the tissue is hardly attached, the use electro-surgery is mandatory. In those cases there are again two possibilities:-If there are no big vessels in the implantation area, the tissue is removed with resectoscopic slicing technique; this is what happens in type 2 of the Gutenberg classification, this accounts approximately 15% of the cases.-If there are big vessels, the tissue must be coagulated first, and removed in a second step with the use of the loop. This is usually a copious bleeding procedure. Again, we recommend a second look hysteroscopy 1 to 2 months after the surgery
CONCLUSIONThis classification is useful not only to find correlation between the ultrasound findings and hysteroscopy but also to establish the anticipated difficulty during the resection of retained products of conception. We know that further studies are needed, but we are very confident that this is a good starting point.
www.hysteroscopy.info
12
Nov-Dec 2015 | vol. 1 | issue 6
GUTENBERG CLASSIFICATION
Morfological hysteroscopic classification

www.hysteroscopy.info
13
Pelvic anatomy and gynecologic surgery Las Vegas, USA |Dec 10-12|2015
66 Congreso Mexicano de Ginecologia y Obstetricia Acapulco, Mexico |Nov 1-5|2015
CongresSINTERNATIONAL
44th AAGL Global Congress of Minimally Invasive Gynecology Las Vegas, Nevada |nov 15-19|2015
16th APAGE Annual Congress Beijing, China |Nov 5-8|2015
56 Congresso brasileiro de Ginecologia e obstetriciaBrasilia, Brasil |Nov 12-15|2015
World Congress on recurrent pregnancy lossCannes, Francia |Jan 14-17|2016
Middle East Fertility Society 22nd annual scientific meeting Sharm El Sheikh, Egypt |Nov 5-7|2015
The 23rd World Congress on Controversies in Obstetrics, Gynecology & Infertility Melbourne, Australia |Mar 21-23|2016
59th All India Congress of Obstetrics & GynaecologyAgra, India |Jan 13-17|2016
Nov-Dec 2015 | vol. 1 | issue 6
RCOG world congress 2016 Birmingham, UK |Jun 20-22|2016
14th ESC Congress / 2nd Global ESC ConferenceBasel, Switzerland |May 4-7|2016
4th International Congress of Gynaecology and ObstetricsBarcelona,Spain |May 28-30|2016

14
www.hysteroscopy.info
HYSTEROSCOPY
DEVICESEndosee Dr. P. Indman
The Endosee Hysteroscope with the Disposable Diagnostic (Dx) Cannula is intended for use in viewing the cervical canal and uterine cavity for the purpose of performing diagnostic procedures in an outpatient or in an office setting. Hysteroscopy can be
used for the evaluation of the uterine cavity for pathology such as submucous myomas, endometrial polyps, malignancyand other conditions.
The Endosee Hysteroscope is a lightweight, handheld, battery operated portable system. It is used with a sterile, single-use Disposable Diagnostic (Dx) Cannula with a camera and light source at the distal end to illuminate the area for visualization and
image and video capture. The video signal is electronically transferred to the main body of the hysteroscope via an electrical connector. An LCD touch screen display monitor on the hysteroscope is used for viewing.
Experience with EndoSee: A Novel Hand-Held Digital Hysteroscope for Use in Diagnostic Office Hysteroscopy Harris MS. Women’s Health Research, Phoenix, Arizona
Journal of Minimally Invasive Gynecology, Vol. 20, Issue 6, S67–S68
Study Objective: To perform diagnostic hysteroscopy and capture digital images and video, without the need for separate video processing equipment, in a hand-held portable design.Patients: 25 Women Aged 33-70 presenting to undergo evaluation for Abnormal Uterine Bleeding. Twenty-two procedures were performed in an office setting, 3 in an operating room under general anesthesia prior to another planned procedure.Intervention: Diagnostic hysteroscopy under paracervical block or general anesthesia, using normal saline as the distending medium. Endometrial biopsy or D & C was performed if thought appropriate.Measurements and Main Results: EndoSee is a semi-rigid hysteroscope with disposable curved canula measuring 4.5mm in diameter. Images are captured from a digital processing chip at the tip and transferred to a 3.5inch (diagonal dimension) digital screen at the base of the reusable and rechargeable hand-piece, eliminating a separate tethered digital monitor or power source. An inflow port fits a syringe or IV tubing. Digital video or images may be immediately reviewed on the instrument screen, anddownloaded via USB for storage if desired.Conclusion: EndoSee allows in-office or portable hysteroscopy without the need for other components or complicated instrument processing. Quality digital images are immediately available or easily archived.
Nov-Dec 2015 | vol. 1 | issue 6
15
HYSTEROSCOPYBASIC
ENDOMETRIAL POLYPS
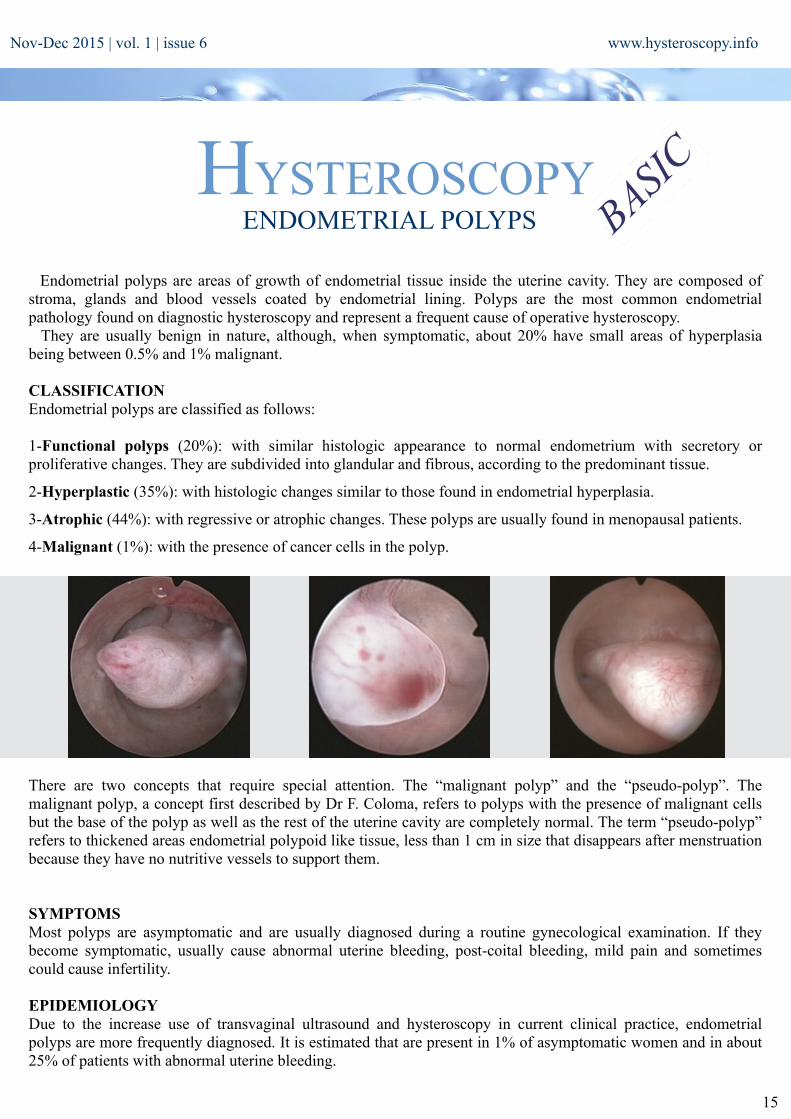
Endometrial polyps are areas of growth of endometrial tissue inside the uterine cavity. They are composed of stroma, glands and blood vessels coated by endometrial lining. Polyps are the most common endometrial pathology found on diagnostic hysteroscopy and represent a frequent cause of operative hysteroscopy. They are usually benign in nature, although, when symptomatic, about 20% have small areas of hyperplasia being between 0.5% and 1% malignant.
CLASSIFICATIONEndometrial polyps are classified as follows:
1-Functional polyps (20%): with similar histologic appearance to normal endometrium with secretory or proliferative changes. They are subdivided into glandular and fibrous, according to the predominant tissue.
2-Hyperplastic (35%): with histologic changes similar to those found in endometrial hyperplasia.
3-Atrophic (44%): with regressive or atrophic changes. These polyps are usually found in menopausal patients.
4-Malignant (1%): with the presence of cancer cells in the polyp.
There are two concepts that require special attention. The “malignant polyp” and the “pseudo-polyp”. The malignant polyp, a concept first described by Dr F. Coloma, refers to polyps with the presence of malignant cells but the base of the polyp as well as the rest of the uterine cavity are completely normal. The term “pseudo-polyp” refers to thickened areas endometrial polypoid like tissue, less than 1 cm in size that disappears after menstruation because they have no nutritive vessels to support them.
SYMPTOMSMost polyps are asymptomatic and are usually diagnosed during a routine gynecological examination. If they become symptomatic, usually cause abnormal uterine bleeding, post-coital bleeding, mild pain and sometimes could cause infertility.
EPIDEMIOLOGYDue to the increase use of transvaginal ultrasound and hysteroscopy in current clinical practice, endometrial polyps are more frequently diagnosed. It is estimated that are present in 1% of asymptomatic women and in about 25% of patients with abnormal uterine bleeding.
www.hysteroscopy.infoNov-Dec 2015 | vol. 1 | issue 6
www.hysteroscopy.info
16
DIAGNOSISOnce the presence of endometrial polyps is suspected, imaging studies are the most sensitive in the diagnosis of intrauterine pathology. Ultrasound is a commonly used imaging modality for the diagnosis of endometrial polyps by direct visualization of the polyp, color Doppler is often used for better visualization of its vascular supply. Often, endometrial polyps are suspected by the presence of increased endometrial thickening. Other techniques that may help in diagnosis are hysterosalpingogram and sonohysterogram. The completion of blind curettage can miss the presence of endometrial polyps in up to 10% of the cases.
The preferred modality for the diagnosis of endometrial polyps is hysteroscopy, in addition to the direct visualization of the polyp; it allows biopsy and even excision at the time of diagnosis.
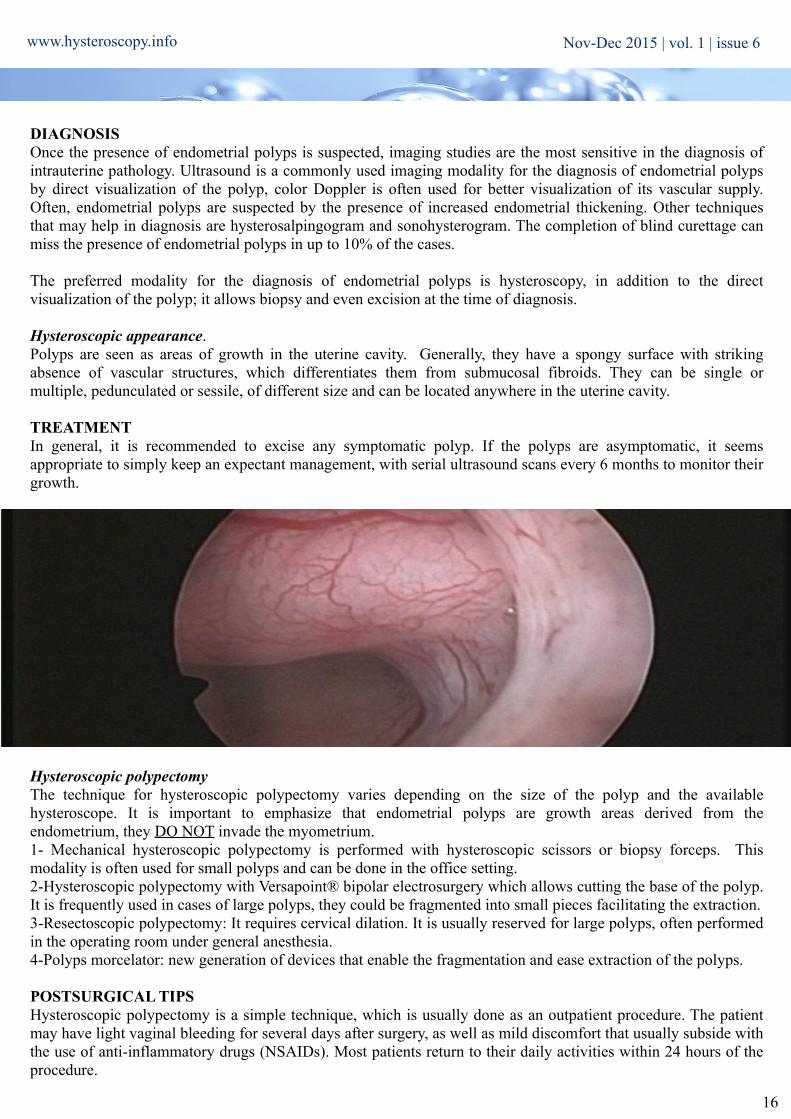
Hysteroscopic appearance.Polyps are seen as areas of growth in the uterine cavity. Generally, they have a spongy surface with striking absence of vascular structures, which differentiates them from submucosal fibroids. They can be single or multiple, pedunculated or sessile, of different size and can be located anywhere in the uterine cavity.
TREATMENTIn general, it is recommended to excise any symptomatic polyp. If the polyps are asymptomatic, it seems appropriate to simply keep an expectant management, with serial ultrasound scans every 6 months to monitor their growth.
Hysteroscopic polypectomyThe technique for hysteroscopic polypectomy varies depending on the size of the polyp and the available hysteroscope. It is important to emphasize that endometrial polyps are growth areas derived from the endometrium, they DO NOT invade the myometrium.1- Mechanical hysteroscopic polypectomy is performed with hysteroscopic scissors or biopsy forceps. This modality is often used for small polyps and can be done in the office setting.2-Hysteroscopic polypectomy with Versapoint® bipolar electrosurgery which allows cutting the base of the polyp. It is frequently used in cases of large polyps, they could be fragmented into small pieces facilitating the extraction.3-Resectoscopic polypectomy: It requires cervical dilation. It is usually reserved for large polyps, often performed in the operating room under general anesthesia.4-Polyps morcelator: new generation of devices that enable the fragmentation and ease extraction of the polyps.
POSTSURGICAL TIPSHysteroscopic polypectomy is a simple technique, which is usually done as an outpatient procedure. The patient may have light vaginal bleeding for several days after surgery, as well as mild discomfort that usually subside with the use of anti-inflammatory drugs (NSAIDs). Most patients return to their daily activities within 24 hours of the procedure.
Nov-Dec 2015 | vol. 1 | issue 6

www.twitter.com/hysteronews
HYSTEROscopy group
Hysteroscopy newsletter
Hysteroscopy newsletter
www.facebook.com/hysteronews
ProjectsHY
ST
ER
O
17
www.hysteroscopy.infoNov-Dec 2015 | vol. 1 | issue 6
Epidemiological evaluation of intrauterine adhesions (IUAs) after hysteroscopic surgery
Coordinator: Dr. S. Haimovich
Design:Dr. A. S. Laganá
Aim of the study:To evaluate the prevalence of
intrauterine adhesions (IUAs) after
hysteroscopic surgery.
Type of the study:Multicenter, cohort
study.
OutcomesThe risk of IUAs after hysteroscopic surgery
will be evaluated according to the
different analyzed variables (age, BMI, parity, use of medical
therapy for endometrial preparation and type of endouterine disease).
Contact:If you are interested in participate in this study,
please contact with [email protected]
Patients and MethodsThe patients will be consecutively selected from a population with suspected endouterine disease with high risk of post surgical IUA and that will probably require a resectoscopy (fibroids/septum), resulting from 2D transvaginal ultrasound screening. Subsequently, they will undergo diagnostic hysteroscopy which will confirm the presence of endouterine disease (if the endouterine disease will be not confirmed, the patient will be not enrolled for the current study). This test will be always performed by the same physician for each center, during the early proliferation phase of the menstrual cycle (seventh or eighth day).We will exclude from the enrollment patients with adnexal or uterine diseases (including oncologic ones) for which hysteroscopy does not represent the gold standard management; and/or cardiovascular, hepatic or renal dysfunctions and any other medical condition which could increase the risk during surgery. For all the patients, we will record age, BMI, parity, use of medical therapy for endometrial preparation and type of endouterine disease.All the patients will undergo hysteroscopic surgery (T0), performed by the same physician for each center using Mono or Bipolar Resectoscope (describe the type of hysteroscope that you want to use).After 3 months all the enrolled patients will undergo diagnostic hysteroscopy (T1) as described before, performed always by the same physician for each center (different from who performed hysteroscopic surgery in the first phase of the study), to check whether IUAs occurred.The presence of IUAs will be defined and classified according to the European Society for Hysteroscopy (Grade I-IV), as reported by the AAGL (American Association of Gynecologic Laparoscopists).
Interested :
Jose Metelo (Portugal)
Alejandro Gonzalez (Argentina)
Mercedes Sobreviela (España)
Suneeta Mittal (India)
Artur Chelmicki (Polonia)
Luigi Nappi (Italia)
S Angioni (Italia)
Narendra Malhotra (India)
This study will start on january the 1st. If you are interested, deadline is november the 30th
18
www.hysteroscopy.info
Hysteroscopy ConundrumsDysmorphic Uterus
VIDEO: Hysteroscopic metroplasty to expand dysmorphic uterus with resectoscope.Watch our last video; Hysteroscopic metroplasty to expand dysmorphic uterus with resectoscope using monopolar collin's.Enjoy our YouTube channelhttps://www.youtube.com/watch?v=yhKiT8Rk-K0
Loo
k fo
r us
: hys
tero
scop
y gr
oup
in L
inke
d In
Nov-Dec 2015 | vol. 1 | issue 6

19
www.hysteroscopy.infoNov-Dec 2015 | vol. 1 | issue 6
TIPS and TRICKS... 4U
Some things just can’t be learned from books. Some things can only be learned through experience. In this section the best hysteroscopists will share their tricks with you.
Hysteroscopic surgery is the treatment of choice for intrauterine adhesions. It allows to perform lysis of adhesions under direct vision and magnification. After the surgery, the adhesions recurrence rate is between 3,1 to 23,5% being the high recurrence rate one of the main problems of this entity. This recurrence rate is higher in severe cases. According to AAGL guidelines, the use of postoperative estrogen hormone therapy to promote endometrial overgrowth and a regrowth of the uterine lining may reduce recurrence of intrauterine adhesions (grade B).
Some physical barriers such as intrauterine device (IUD), Foley catheter, intrauterine balloon and hyaluronic acid gel are used as adjuvant therapy. In a retrospective study by Lin in 107 patients with intrauterine adhesions, they found that the intrauterine balloon was more effective in preventing intrauterine adhesion reformation than the use of IUD or hyaluronic acid gel.
A Foley catheter after hysteroscopic surgery for intrauterine adhesions was one of the first devices used to prevent the recurrence of adhesions. A Foley catheter (10-16 Fr) with 3`5 to 5 ml of fluid is used to separate the uterine walls. This catheter is left inside the cavity
for 7-10 days.
Recently, a new triangular shape catheter balloon has been available (Cook medical Inc). This device, due to its more anatomic shape, fits better into the uterine cavity than the classical Foley catheter. This uterine balloon is filled with 5 ml of fluid and maintains
separation of the lateral walls of the uterine cavity which is the area where the recurrence of adhesions is more frequent.
20
www.hysteroscopy.info Nov-Dec 2015 | vol. 1 | issue 6
IMAGE 4
Uterine leiomyomas are frequent, have an impact on reproductive function and on women quality of life.They are classified according to their location in the uterus, and submucosal fibroids would be most related to the uterine bleeding.
When they are symptomatic, should be removed by surgery and the approach for myomectomy depends on their classification. In open and laparoscopic myomectomy after to incise the serosa and the myometrium, we start the blunt dissection in the plane between the myoma and its pseudocapsules. The uterine myomapseudocapsule is a fibrous structure surrounding the neurovascular leiomyoma, separating it from the normal peripheral myometrium.
The fibroid pseudocapsule is composed of a rich neurovascular network in neurofibers similar to the neurovascular bundle surrounding the prostate [1]. In the larger fibroids, after being withdrawn completely from the uterine wall, they are morcellated. In the surgical technique of abdominal myomectomy the myoma is not fragmented before removed from the uterine wall, it is always taken whole, mobilizing the nodule through the pseudocapsule. In this two surgical techniques, the myoma is fragmented after myomectomy, only to be retired of pelvis cavity.
In 1978, Neuwirth held the first hysteroscopic myomectomy using urological resectoscope with applying surgical technique similar to the resection of the prostate, with a resectoscope and "U" loop, slicing the fibroid and, sometimes, damaging the adjacent myometrium [2]. The slicing technique fibroid, gold standard technique, leads to severe exposure lump vessels, causing greater blood loss, through strain absorption and sometimes myometrium damage with consequences for reproduction.
Some authors already make hysteroscopic myomectomy using the pseudocapsule. Litta et al, make the release after the resection of the intracavitary portion of the myoma [3], while Mazzon releases the intramural portion of the fibroid with cold loop [4]. The technique published in Brazil in 2002 by our group uses the pseudocapsule in a similar form of the laparotomy or laparoscopic myomectomy, without partial resection of this, mobilizing the whole fibroid, believing that the integrity of pseudocapsule facilitates surgery [5].
This technique, with the resectoscope with "L" loop (Collins), initiates with the incision of the myoma bed, surrounding it completely. From there, we enter the fibroid plan / pseudocapsule and releasing the fibrous bands, with occasional clotting of the vessels found. The vascular network generally surrounds the myoma, detachment of the myoma occurring inside the pseudocapsule should cause less bleeding and maintain the integrity myometrial, Allowing the facilitation of uterine healing and is of benefit for future reproductive outcome [6]. The first incision should always be done through the posterior portion, completely surrounding the endometrium until you reach the pseudocapsule. When reaching pseudocapsule starts the mobilizations of the nodule, with blunt dissection of the myomapseudocapsule from adjacent myometrium, without cutting the nodule.
My experienceRicardo Lasmar (1) and Bernardo Lasmar (2)
1- Professor of Gynecology of Federal Fluminense University – Rio de Janeiro – Brazil. 2 –Professor of Gynecology of Estacio de Sá University - – Rio de Janeiro – Brazil
email: [email protected]
Why use pseudocapsules of myoma in hysteroscopic myomectomy?

Only after the complete withdrawal of it we make sliced in the longitudinal direction and then, taken from the uterine cavity with grasping. In some larger fibroids, we make the myoma fragmentation before the complete liberation of the myometrium, because there is not enough space to mobilize the nodule in the uterine cavity.
The direct mobilization technique myoma prevents damage to adjacent myometrial and minimizes the risk of overload of the procedure. Moreover, during the mobilization of the fibroid, more intramural portion of the nodule is pushed by the myometrium to the uterine cavity, increasing the myometrium thickness and the distance of the fibroid to serosa, allowing the approach of fibroids with distances smaller than 5 mm to serosa safely. [7,8]
The direct mobilization of the myoma is possible at the ambulatory surgery, doing the same movement with scissor around de pseudocapsule.
References:1: Tinelli A, Malvasi A, Hurst BS, Tsin DA, Davila F, Dominguez G, Dell'edera D, Cavallotti C, Negro R, Gustapane S, Teigland CM, Mettler L. Surgical managementof neurovascular bundle in uterine fibroid pseudocapsule.JSLS. 2012. Jan-Mar;16(1):119-29. 2. Neuwirth RS. A new technique and additional experience with hysteroscopic resection of submucous fibroids.Am J obstetGynecol 1978; 131:91-4.3. Litta P, Vasile C, Merlin F, Pozzan C, Sacco G, Gravila P, Stelia C. A new technique of hysteroscopic myomectomy with enucleation in toto. J Am Assoc GynecolLaparosc. 2003 May;10(2):263-70. 4. Mazzon I. Nuova tecnica per la miomectomia isteroscopica: enucleazione con ansa freda. In: Cittadini E, Perino A, Angiolillio M, Minelli L (eds). Testo-Atlante di Chirugia Endoscopica Ginecologica. Palermo. Italia. COFESE Ed. 1995, cap XXXIIIb5. Lasmar R, Barrozo P. Histeroscopia: uma abordagem prática. 1a ed. Rio de Janeiro: Medsi; 2002.6 Tinelli A, Malvasi A, Rahimi S, Negro R, Cavallotti C, Vergara D, Vittori G,Mettler L. Myomapseudocapsule: a distinct endocrino-anatomical entity ingynecological surgery. GynecolEndocrinol. 2009 Oct;25(10):661-7. 7. RB Lasmar, PRM Barrozo, DB Da Rosa, BP Lasmar, WP Modotte, R Dias. Hysteroscopic myomectomy in a submucous fibroid near from tubal ostia and 5 mm from the serosa: A case report from the Endoscopy Service of Ginendo-RJ. Gynecological Surgery, v. 6, n. 3, p. 283-286, 20098. Hysteroscopic myomectomy in a submucous fibroid 3 mm from the serosa: a case report RB Lasmar, PRM Barrozo, DB Da Rosa, R Dias. Gynecological Surgery 4 (2), 149-152
Nov-Dec 2015 | vol. 1 | issue 6 www.hysteroscopy.info
https://drive.google.com/file/d/0B9_0fZ2JnKsONVBrS08zdTRHYmc/view?usp=sharing
21
https://drive.google.com/file/d/0B9_0fZ2JnKsORVlpY0REQ1BLSE0/view?usp=sharing

Hysteroscopy newsletter
HYSTEROscopy group
Hysteroscopy newsletter
www.twitter.com/hysteronews
FIND US ON www.facebook.com/hysteronews
Hysteroscopy Newsletter is an opened forum to all professionals who
want to contribute with their knowledge and
even share their doubts with a word-wide
gynecological community
At the end of the first year of this ambitious project is time for reflection and analysis. All started as an idea, with the aim to provide a platform and a showcase for all gynecologist dedicated to hysteroscopy where we could express ourselves and contribute to the formation of our colleagues, having a needed place for innovation.
And what happened after a year? Judging by the increased in readers after each new publication, starting with 800 and reaching over 2250 downloads of the latest issue, we can say that this newsletter is a great success!. Another parameter that reinforces our success is the active participation of a large group of experts around the world. We have managed to involve and interview top world leaders experts in the field such as A. Tinelli, L. Bradley, R. Labastida, A. Garcia and A. Di Spiezio Sardo.
Where should we go from now? We will keep growing. To start, the "Japan Society of Gynecologic and Obstetric endoscopy and Minimally Invasive Therapy" with its 3,000 members agreed to receive the newsletter, and we are sure that very soon other international societies will also join. We will continue to be opened to your suggestions and ideas, without them this project would loose its characteristic quality. We will maintain a high level of quality content trying to keep improving every day.
What do we ask from you? Please, continue to participate, this project belongs to every one of us. Your experience, your ideas, your work are essential for the newsletter and is the force that move us forward to improve in what we love so much, hysteroscopy.
Dr Sergio HaimovichHead of the hysteroscopy unit
Hospital del Mar. Barcelona. Spain
www.hysteroscopy.info Nov-Dec 2015 | vol. 1 | issue 6
22
Editorial teaMHYSTEROSCOPY