vitamin a deficiency disorders in children - home - iapb a deficiency disorders in children clare...
TRANSCRIPT
Vitamin A deficiency
disorders in children
Clare Gilbert
Reader in International Eye Health

Vitamin A deficiency disorders
Has been a very important cause of blindness in children: 1999: 350,000 out of 1.4 million (25%)
Poor countries
Declining in many countries
Important cause of child mortality
Common in pregnant and lactating women in developing countries
Other high risk groups: long term prisoners
children in institutions for the multiply handicapped

Vitamin A deficiency - definitions
New terminology: replaces “clinical” and “subclinical” deficiency
reflects the spectrum of deficiency
Vitamin A deficiency (VAD): a state of inadequate vitamin A nutriture
VAD begins when liver stores are below 20g/g
serum levels can often be maintained despite this
serum retinol levels <20g/dL (0.70mol/L) are deficient
Vitamin A deficiency disorders (VADD): physiological disturbances secondary to VAD
subclinical (increased infection; anaemia) and clinical
Xerophthalmia: Ocular signs


Global distribution
Affects poorest communities in poorest countries
Clinically significant public health problem - 39 countries
Serious problem - 11 other countries
Regional or likely problem - 45 countries
At least 140 million preschool age children and >7 million pregnant women suffer from VADD each year
1.2 – 3.0 million children die unnecessarily each year
4.4. million children and 6.2 million women suffer from xerophthalmia
Nearly 50% VAD occurs in South and Southeast Asia.

Prevalence of VADD, West, 2002
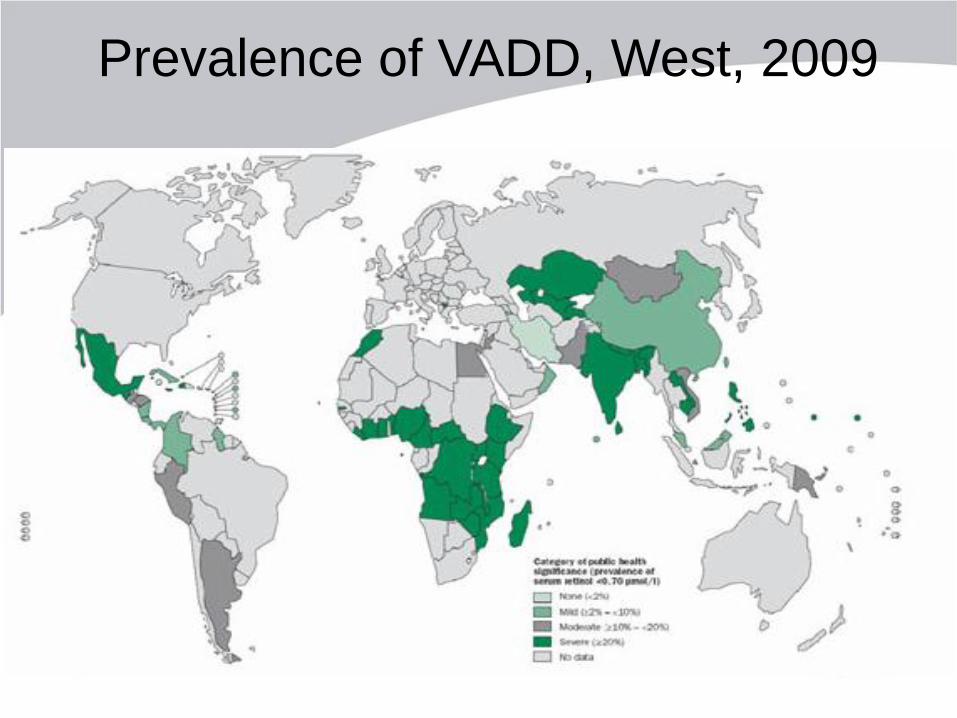
Prevalence of VADD, West, 2009

Vitamin A deficiency disorders:
number of children affected
Children : ~150 - 200 mill
Xerophthalmia :
children ~3 million
pregnant women ~3 million
Blindness : ~500,000/ year
Preventable deaths : ~1 - 2.5 mill/ year

Sources of vitamin A
Vitamin A is fat soluble vitamin
Occurs as retinol in animal sources: Breast milk
Egg yolk
Dairy products
Fish liver
Provitamin A precursors found in plant sources (carotenoids e.g. β-carotene): Yellow, orange and red fruits (e.g. mango, papaya)
Yellow and orange vegetables (e.g. squash, carrots)
Dark green leafy vegetables
Red palm oil (West Africa)
>600 identified, but only 10 have pro-vitamin A activity
C40 skeleton with C5 isoprene units

Sources of vitamin A
Foetus acquires retinol across the
placenta
Retinol more biologically active than
provitamin A precursors
Need oil or fat in the diet for absorption

Vitamin A conversion factors
1 µg retinol = 0.00349 µmol retinol
1.15 µg retinyl acetate
1.83 µg retinyl palmitate
3.33 IU retinol
10 I.U provitamin carotenoids 1 Retinol Equivalent (RE)
Retinol Activity Equivalent (RAE)
1 µg retinol
12 µg all trans β-carotene
24 µg other provitamin A carotenoids
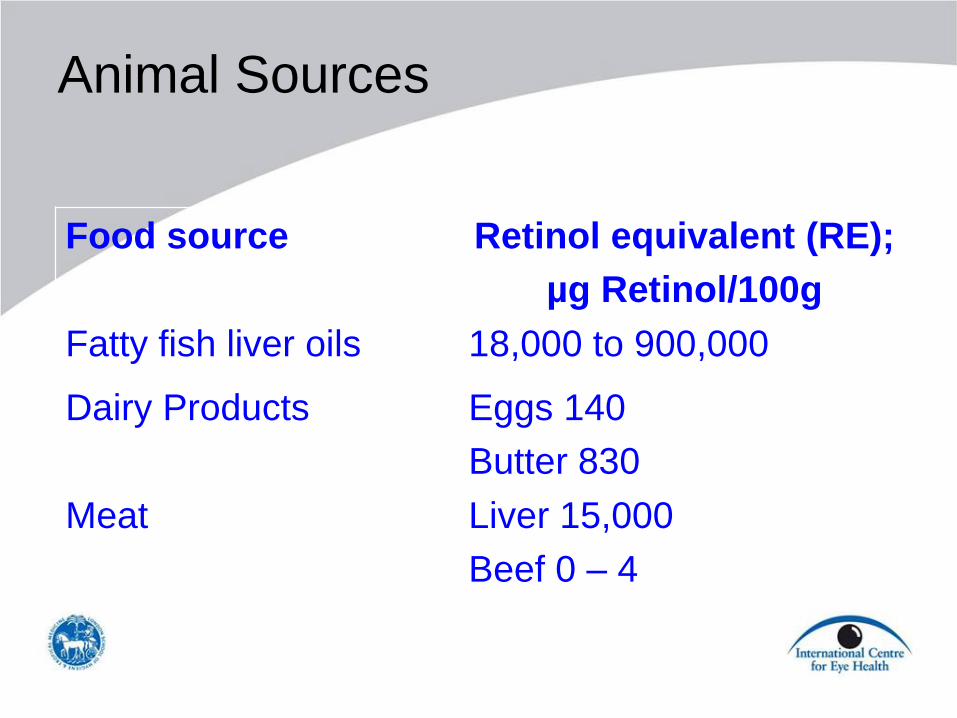
Animal Sources
Food source Retinol equivalent (RE);
µg Retinol/100g
Fatty fish liver oils 18,000 to 900,000
Dairy Products Eggs 140
Butter 830
Meat Liver 15,000
Beef 0 – 4

Plant Food Sources
Food source Retinol equivalent (RE);
µg Retinol/100g
Vegetables Red palm oil 30,000
Carrots 2,000
Dark green leafy veg 685
Fruits Buriti palm 3,000
Mango 307
Other Sources Tablets/capsule
Injections
Fortified foods

Vitamin A rich foods – plant sources

Vitamin A rich foods – animal
sources
Liver

Vitamin A – poor sources
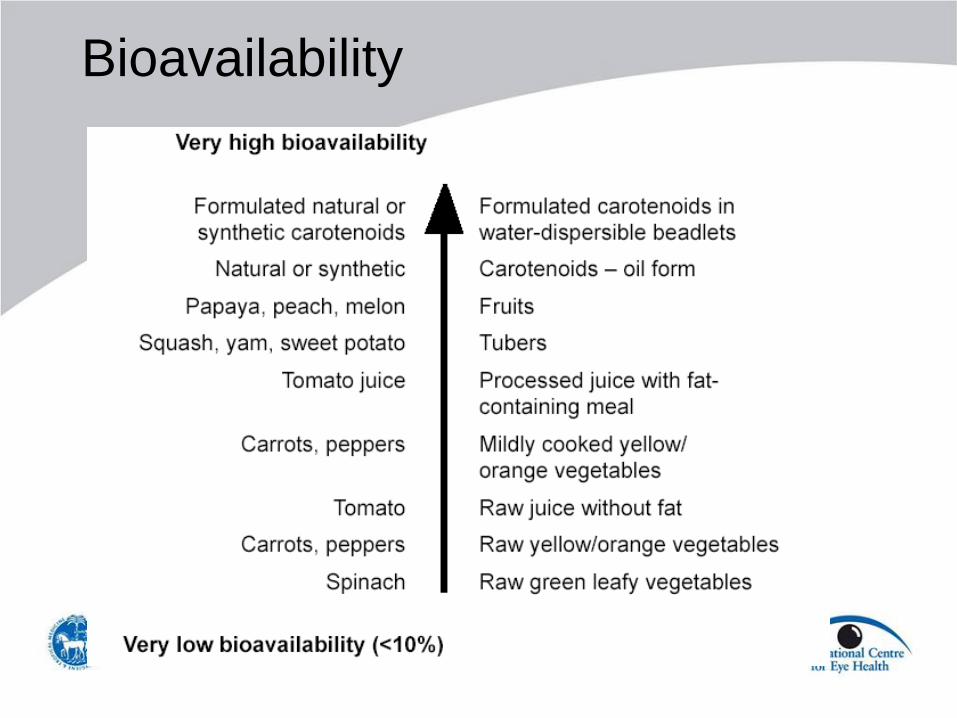
Bioavailability

Dietary equivalence (ug)
Retinol equivalents:
= ratio of non-animal sources : animal
sources which give equivalent intake
1989, NRC, traditional 6:1
2001, IOM, US pop 12:1
West, C 21:1

“Vitamin A” in food supply in
different regions
0
200
400
600
800
1000
1200
1400
Europe Africa S America Asia
FAO / WHO (6:1)* IOM (12:1)* C West (21:1)*
Minimum requirement
* Retinol equivalent used to assess content

Recommended daily intake for children (RE)
Vitamin A g/d
Infants 0-6 months 400
7-12 months 500
Children 1-3 years 300
4-8 years 400
Boys 9-13 years 600
14-18 years 900
Girls 9-13 years 600
14-18 years 700
Safe level needed to sustain health through periods of low intake and stress

Recommended daily intake for dults (RE)
Vitamin A g/d
Men 19->70 years 900
Women 19->70 years 700
Pregnancy 14-18 years 750
19-50 years 770
Lactation 14-18 years 1200*
19-50 years 1300*
Safe level needed to sustain health through periods of low intake and stress

Amount of foods required daily Daily requirement (g) Child Woman Males, lactating
women
Mango 130 162 195
Buriti palm 13 17 20
Red palm oil 1 2 2
Carrot 20 25 30
DGLV 58 73 88
Cod liver oil 2.2 2.8 3.3
Eggs 286 357 429
Liver 2.6 3.3 4
Beef, pork 10,000 12,000 15,000

Food intake for daily requirement
Age group
Carrots Sweet
potatoes
DGLV Mango
Children:
0-5 months
6-11 months
1-2 years
2-6 years
Breast milk
1 ½ tablespoon
1 ½ tablespoon
2 tablespoon
Breast milk
1 tablespoon
1 tablespoon
1 ½ tablespoon
Breast milk
1/3 cup
½ cup
½ cup
Breast milk
½
½
2/3
Females:
Non-pregnant
Pregnant
Lactating
¼ cup
¼ cup
¼ cup
2 ½ tablespoon
2 ½ tablespoon
¼ cup
1 cup
1 cup
1 ½ cup
1
1
2/3
DGLV = dark green leafy vegetables

Digestion and absorption of retinol
Released in stomach by proteolysis
Aggregate with lipids and pass to small intestine
Fat and protein in diet stimulate secretion of bile
through cholecystokinin
Emulsifies lipids to micelles for absorption
Bile salts stimulate pancreatic lipase and
esterases hydrolyse retinyl esters in
enterocytes to retinol
70 – 90% Retinol absorbed by mucosal cells

Digestion and absorption provitamin A
e.g. β-carotene
Most pass through intestinal mucosa and into blood and
lymph unchanged
Some undergo cleavage
β-carotene 2 Retinal Retinyl esters

Digestion and absorption of retinol
Cellular Retinol Binding Protein (CRBP) carries the
lipid-soluble retinol to lecithin:retinol acetyltransferase (LRAT)
Retinol esterified
and delivered
to chylomicrons
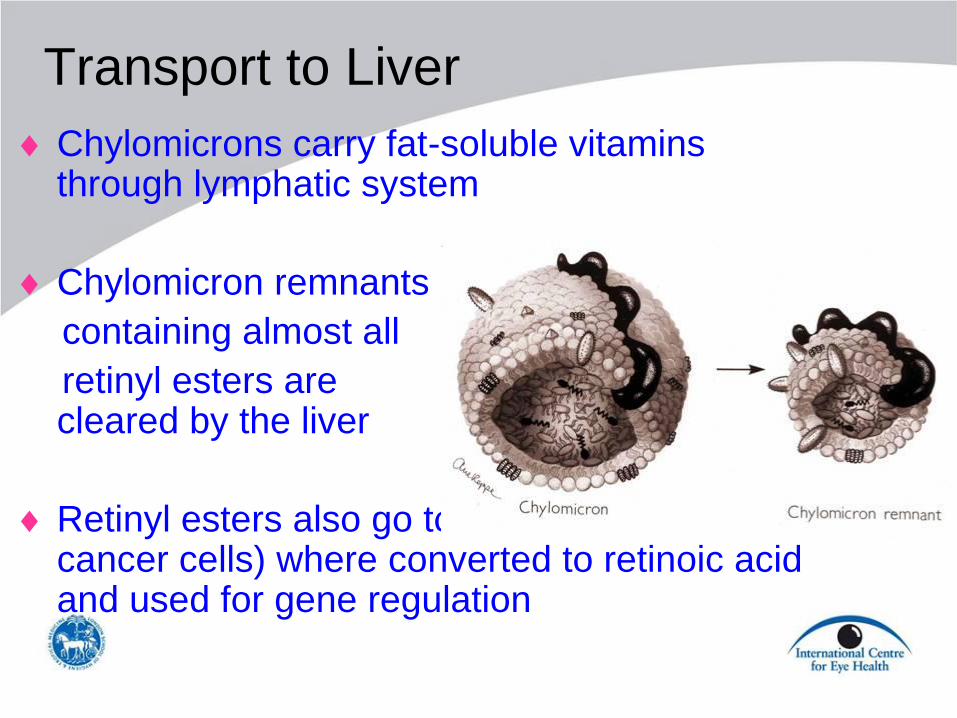
Transport to Liver
Chylomicrons carry fat-soluble vitamins through lymphatic system
Chylomicron remnants
containing almost all
retinyl esters are cleared by the liver
Retinyl esters also go to other tissues (and cancer cells) where converted to retinoic acid and used for gene regulation

Metabolism in Liver
Retinyl esters taken up by hepatocytes
Hydrolysed and processed in endosomes
Retinol to endoplasmic reticulum
Binds to retinol binding protein RBP, enters
Golgi apparatus, and is secreted from the cell
50 – 80% vitamin A (retinyl esters) is in the liver,
in the stellate and parenchymal cells
Other storage sites: adipose cells, RPE

Transport to other cells
Retinol is recycled between plasma, liver and other tissues
In plasma, retinol-RBP complex is bound to transthyretin
[RBG] in adult plasma: 1.9 – 2.4 µmol/l
PEM, infections and parasitic infestations lower the concentration

Transport of vitamin A in tissues
Target cell
ROH = Retinol
RA =Retinoic acid
RBP = Retinol binding prot
CRBP = Cellular retinol BP
CRABP = Cellular retinoic acid BP
RXR, RAR = Nuclear receptors
RBP–ROH
Extracellular
Regulated
gene
transcription
DN
A
Receptor
ROH–CRBP
ROH RA Nucleus
RA–RXR RAR–RA
RA
RA–CRABP
Intracellular
Cell membrane and nuclear membrane receptors

Functions of Vitamin A
Gene expression:
During development
Differentiation (epithelial tissues)
Growth
Immune system:
Barrier function
Humoral and cell mediated immunity
Glycoprotein, glycosaminoglycan synthesis
Reproduction (testosterone production)

Functions of vitamin A
Energy Balance: thermogenesis by mitochondria is under
transcriptional regulation by RA
Regulation of dopaminergic system:
Gap junctional communication:
Haemopoesis
Antioxidant
Vision

Visual cycle
Light

Risk factors for
vitamin A deficiency

Risk factors for vitamin A deficiency
Macro-environment
Household
Person

Macroenvironment:
Ecology
Climate
Political
Infrastructure
Cultural practices and taboos
Structure of society
Inadequate health services
Factors leading to poverty
Risk factors for vitamin A deficiency

Household:
Poor water supply
Inadequate sanitation
Dirty local environment
Lack of female literacy
Large family sizes
Over crowding
Lack of land ownership
Risk factors for vitamin A deficiency

Children:
measles and other febrile illnesses
malabsorption (diarrhoea, infestations)
malnutrition
Adults:
pregnancy and lactation
alcoholism
wars and conflicts (malnutrition)
prisoners
diseases with malabsorption (coeliac disease)
Risk factors for vitamin A deficiency

Children are at higher risk:
Liver stores relatively low at birth
Breast milk supplies adequate retinol for 6 months
High requirement because of growth
High rate of infection and diarrhoea after weaning
Measles infection after the age of 6 months
Totally dependant on adults
Risk factors for vitamin A deficiency

Children can develop VADD even if vitamin A rich foods are available and affordable: Inadequate breast feeding
Complimentary and weaning foods low in vitamin A
Feeding practices and taboos
Food preferences
Over cooking
Inadequate preservation methods
DGLV not mashed
Risk factors for vitamin A deficiency

Pathology in vitamin A deficiency
Dedifferentiation of epithelial cells:
Loss of goblet cells
Low mucin production
Squamous metaplasia
Eye
Respiratory tract
[Skin and hair]
Loss of barrier function

Vicious cycle in vitamin A deficiency
Infection
Vitamin A
deficiency
Loss of barrier function
Reduced immunity
Increased demand
Increased loss
Lower RBP
Acute phase proteins

Manifestation of vitamin A deficiency
Morbidity:
Ocular
Other
Mortality

Xerophthalmia

Relationship between blindness due to
VAD and Human Development Index
0
10
20
30
40
50
60
70
0.25 0.35 0.45 0.55 0.65 0.75 0.85 0.95
Human Development Index
% b
lin
dn
ess d
ue
to
VA
D

Xerophthalmia - classification
Night Blindness XN
Conjunctival Xerosis X1A
Bitot’s Spots X1B
Corneal Xerosis X2
Corneal Ulceration <1/3 X3A
Corneal Ulceration >1/3 X3B
Corneal Scar XS
Xerophthalmic Fundus XF
NB This is not a chronological classification

Courtesy A Sommer
Night blindness (XN)
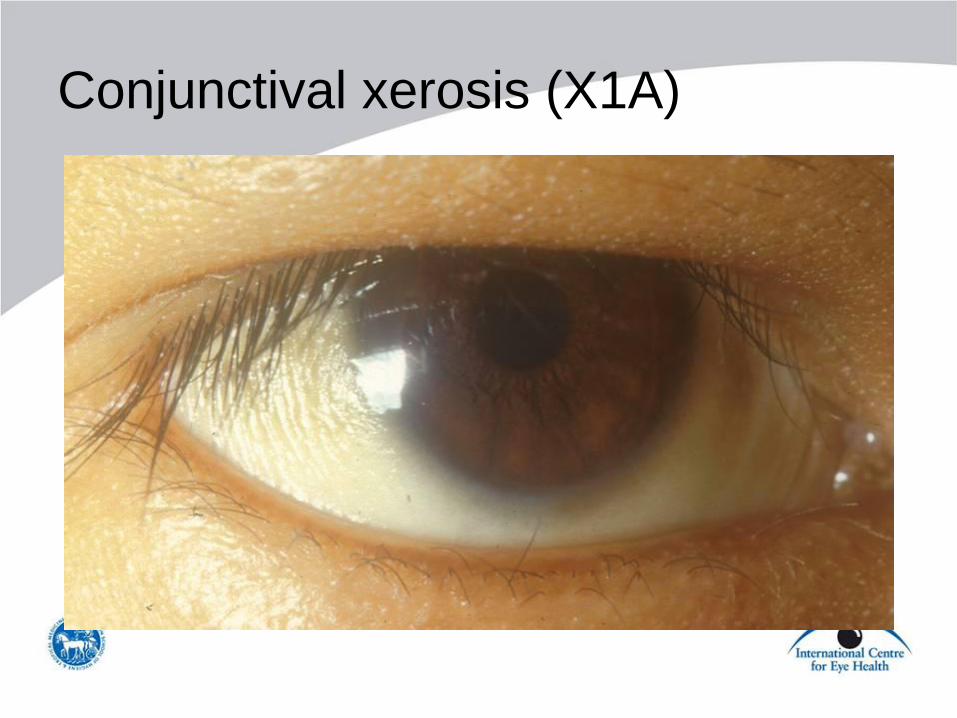
Conjunctival xerosis (X1A)
Difficult sign to elicit C Gilbert
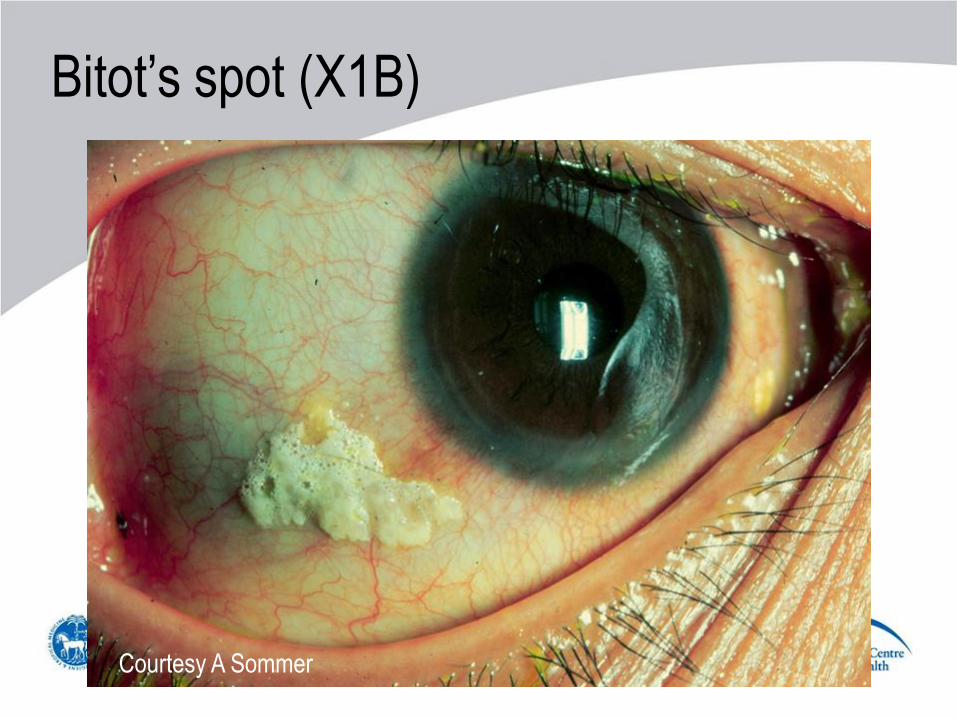
Bitot’s spot (X1B)
Courtesy A Sommer

Bitots spot (X1B)
Pathognomonic of vitamin A deficiency
Accumulations of keratin, acted on by bacteria. Can be wiped off.
Disappear when vitamin A status improves C Gilbert

Corneal (and conjunctival) xerosis (X2)
Courtesy A Sommer

Keritinsation, xerosis and scarring
C Gilbert

Corneal ulcer <1/3 cornea (X3A)

Corneal ulcer <1/3 cornea (X3A)
A Foster

Courtesy A Sommer
Before….
.. and after
treatment

Corneal ulcer >1/3 cornea (X3B)
L Gordillo

Keratomalacia

Courtesy A Sommer

Corneal scarring
C Gilbert

Peak age for different eye signs
Grade of xerophthalmia Peak age group affected
XN Night blindness 2-6 yrs, women
X1A Conjunctival xerosis 3-6 years
X1B Bitot’s spot 3-6 years
X2 Corneal xerosis 1-4 years
X3A C ulcer/keratomalacia <1/3 cornea 1-4 years
X3B C ulcer/keratomalacia 1/3 cornea 1-4 years
XS Corneal scarring (from X3) 1-4 years +
XF Xerophthalmic fundus Adults

Management of xerophthalmia
Optical iridectomy [corneal grating]
C Gilbert
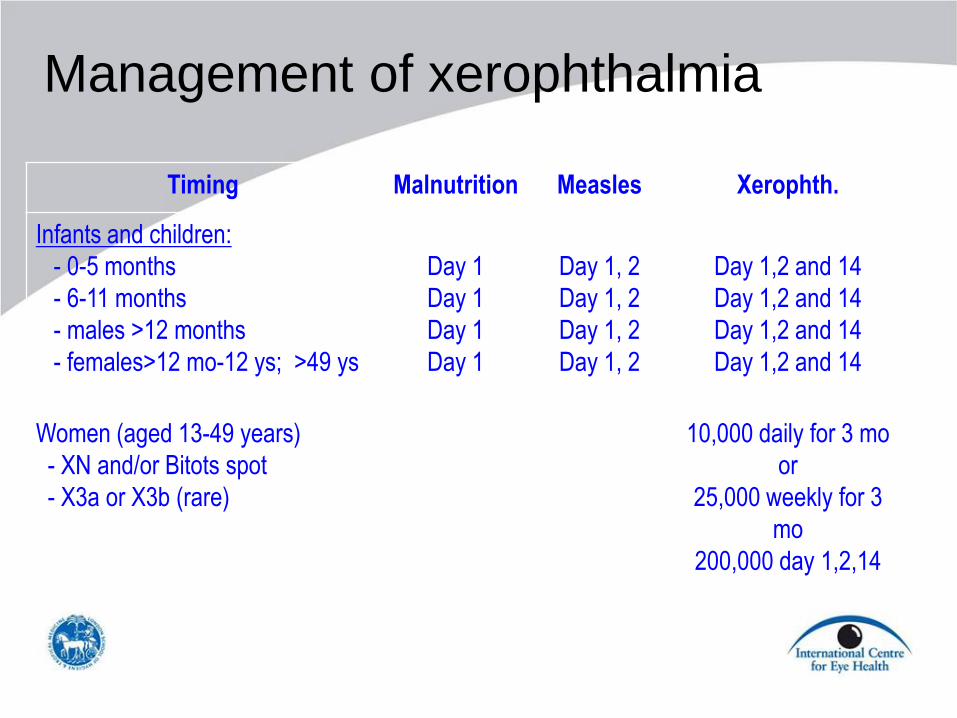
Management of xerophthalmia
Timing Malnutrition Measles Xerophth.
Infants and children:
- 0-5 months
- 6-11 months
- males >12 months
- females>12 mo-12 ys; >49 ys
Day 1
Day 1
Day 1
Day 1
Day 1, 2
Day 1, 2
Day 1, 2
Day 1, 2
Day 1,2 and 14
Day 1,2 and 14
Day 1,2 and 14
Day 1,2 and 14
Women (aged 13-49 years)
- XN and/or Bitots spot
- X3a or X3b (rare)
10,000 daily for 3 mo
or
25,000 weekly for 3
mo
200,000 day 1,2,14

Corneal grafting
Indications: – To maintain integrity of the eye
– To restore visual function, but very
challenging in children, particularly
those blind from VADD: • very poor families
• very poor follow up
• failure to use medication
• early onset visual loss, so amblyopia
• rejection
• astigmatism

Other morbidity

Other morbidity
More difficult to assess
Fewer studies
Conflicting results

Childhood mortality in vitamin A
deficiency

Mortality in children with xerophthalmia
Ocular status Child
intervals
Deaths Mortality
rate
per 1,000
Relative
risk
No xerophthalmia 19,889 108 5.4 1.0
Night blindness only 547 8 14.6 2.7
Bitots spot only 269 6 35.5 6.6
Night blindness + B spot 215 10 46.5 8.6
Clinical trials – childhood mortality
Community based trials:
– 8 randomised, double masked trials in Africa and Asia
– different doses and schedules
– different baseline levels of xerophthalmia
– 6 showed vitamin A supplementation significantly
reduces all cause child mortality
Meta analysis:
– 23% reduction in all trials
– 34% reduction in Asian trials

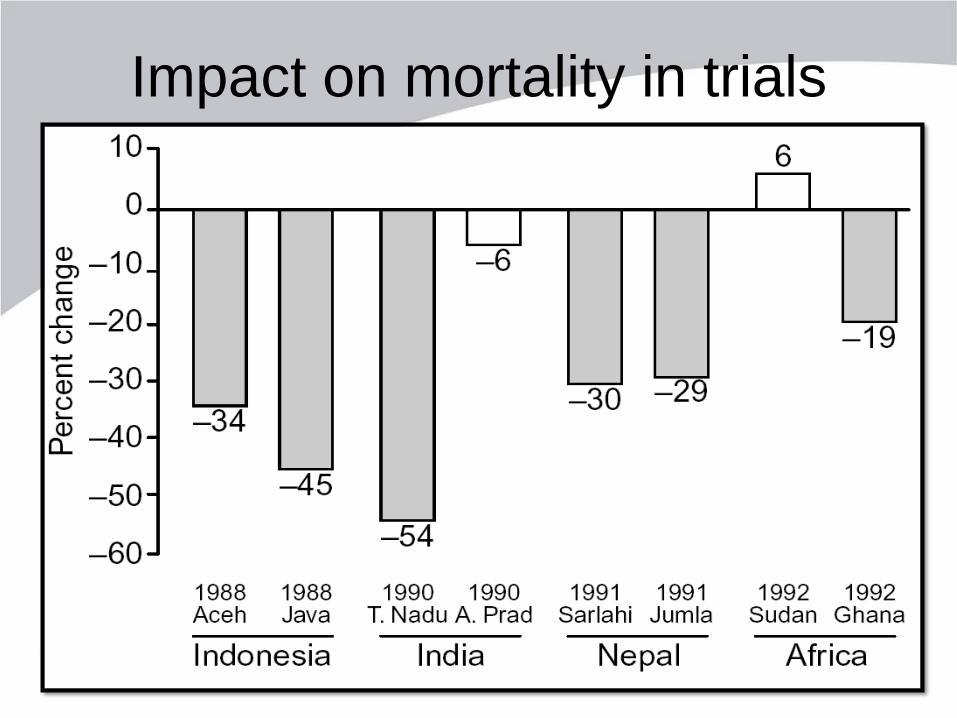
Mortality prevention trails
Study (Year) Country Vit. A Supplement Mortality
reduction
Relative Risk
(95% CI)
Aceh 1986 Indonesia Large dose 6 monly 34% 0.74 (0.54-0.99)
Bogor 1988 Indonesia Vit.A fortified MSG 45% 0.69 (0.57-0.84)
NNIPS 1991 Nepal Large dose 4 mly 30% 0.70 (0.56-0.88)
Jumla 1992 Nepal One and 5 monly 29% 0.55 (0.99)0.74)
Tamil Nadu 1990 India Small Weekly doses 54% 0.46 (0.29-0.71)
Hyderabad 1990 India Large doses 6 monly 6%(NS) 1.00 (0.64-1.55)
Khartoum 1992 Sudan Large doses 6 monly 6%(NS) 1.06 (0.82(-1.37)
VAST1993 Ghana Large doses 4 monly 19% 0.80 (0.29-0.98)
Cochrane Systematic Reviews Vitamin A supplementation for the prevention of morbidity and mortality in
infants six months of age or less. Gogia S, Sachdev HS.
Cochrane Database Syst Rev. 2011 Oct 5;(10):CD007480. Review.
Neonatal vitamin A supplementation for the prevention of mortality and
morbidity in term neonates in developing countries. Haider BA, Bhutta ZA.
Cochrane Database Syst Rev. 2011 Oct 5;(10):CD006980. Review.
Vitamin A supplements for preventing mortality, illness, and blindness in
children aged under 5: systematic review and meta-analysis. Mayo-Wilson E,
Imdad A, Herzer K, Yakoob MY, Bhutta ZA.
BMJ. 2011 Aug 25;343:d5094. doi: 10.1136/bmj.d5094. Review.
Routine vitamin A supplementation for the prevention of blindness due to
measles infection in children. Bello S, Meremikwu MM, Ejemot-Nwadiaro RI,
Oduwole O. Cochrane Database Syst Rev. 2011 Apr 13;(4):CD007719. Review.

• Vitamin A supplementation for preventing morbidity and mortality in
children from 6 months to 5 years of age. Imdad A, Herzer K, Mayo-
Wilson E, Yakoob MY, Bhutta ZA. Cochrane Database Syst Rev.
2010 Dec 8;(12):CD008524. Review.
• Vitamin A supplementation during pregnancy for maternal and
newborn outcomes. Van an den Broek N, Dou L, Othman M, Neilson
JP, Gates S, Gülmezoglu AM. Cochrane Database Syst Rev. 2010
Nov 10;(11):CD008666. Review.
• Vitamin A supplementation for postpartum women. Oliveira-
Menegozzo JM, Bergamaschi DP, Middleton P, East CE. Cochrane
Database Syst Rev. 2010 Oct 6;(10):CD005944. Review.
• Vitamin A for preventing acute lower respiratory tract infections in
children up to seven years of age. Chen H, Zhuo Q, Yuan W, Wang
J, Wu T. Cochrane Database Syst Rev. 2008 Jan 23;(1):CD006090.
Review.
Cochrane Systematic Reviews
Impact on mortality in trials

Different age groups of children
Mortality and/or morbidity
Impact on infants of supplementing
mothers
Maternal deaths
More trials on-going....
Clinical trials have studied:

Assessing vitamin A deficiency
in the community

Hidden iceberg of VADD in the
community
Xerophthalmia
VADD i.e. deficient but no eye signs
Higher risk of mortality
Increased risk of infection
Blind, or at high risk
At very high risk of dying
Measles
Malabsorption
Malnutrition

Prevalence of VAD of public health
significance
Criterion Prevalence (%)
Clinical in children aged 2-5 years:
Night blindness XN
Bitot’s spot XB
C ulcers/keratomalacia X2, X3A & B
Xerophthalmia related corneal scars XS
Clinical in women of child bearing age:
Night blindness during a recent pregnancy XN
Biochemical:
Serum retinol < 0.7 mol/L (20g/dL)
>1.0
>0.5
>0.01
>0.05
>5.0
>15.0
Assessing vitamin A deficiency as
a public health problem
Recently simplified (Annency Accords):
Uses under 5 mortality rates:
>50 / 1,000 = highly likely
20 – 50/1,000 = focal; needs confirming
<20/1,000 = unlikely

Distribution of VADD 2009

Under 5 mortality rates in 2007

Control of vitamin A deficiency

Control of vitamin A deficiency
Short term:
– Intermittent supplementation with high dose vitamin A
Medium term:
– Dietary diversification / food supplementation programmes
– Food fortification
Long term:
– Address underlying causes
– Change eating and food preparation behaviours

Courtesy A Sommer
Supplementation with high dose
retinal palmitate

Seasonality of xerophthalmia in India children
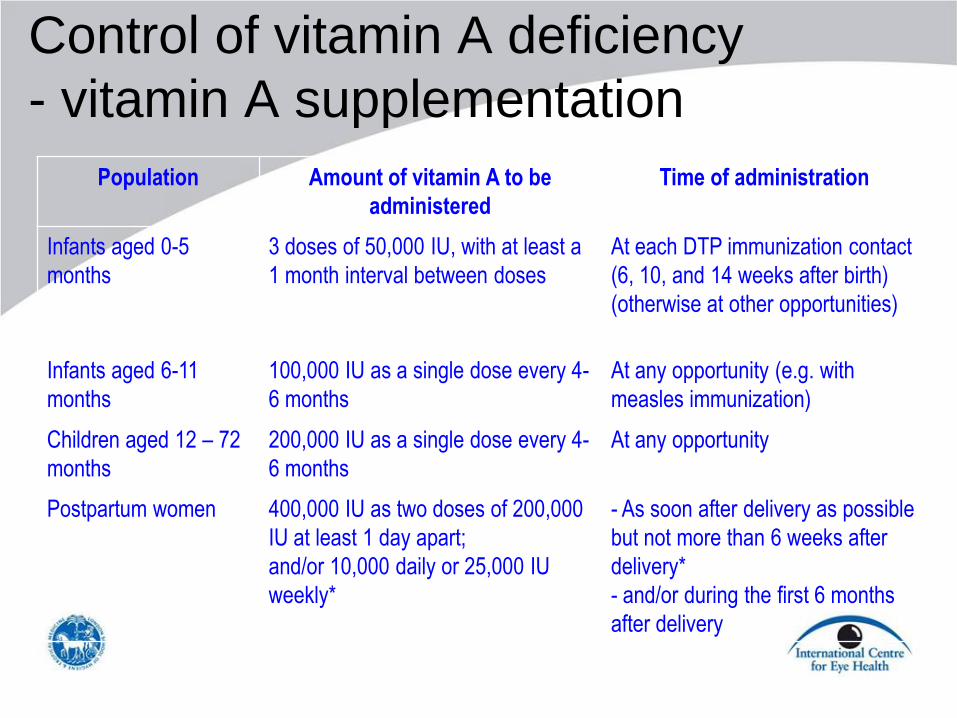
Control of vitamin A deficiency
- vitamin A supplementation
Population Amount of vitamin A to be
administered
Time of administration
Infants aged 0-5
months
3 doses of 50,000 IU, with at least a
1 month interval between doses
At each DTP immunization contact
(6, 10, and 14 weeks after birth)
(otherwise at other opportunities)
Infants aged 6-11
months
100,000 IU as a single dose every 4-
6 months
At any opportunity (e.g. with
measles immunization)
Children aged 12 – 72
months
200,000 IU as a single dose every 4-
6 months
At any opportunity
Postpartum women 400,000 IU as two doses of 200,000
IU at least 1 day apart;
and/or 10,000 daily or 25,000 IU
weekly*
- As soon after delivery as possible
but not more than 6 weeks after
delivery*
- and/or during the first 6 months
after delivery
* as high dose vitamin A is teratogenic vitamin A should not be given during pregnancy, or when a pregnancy is possible

Control of vitamin A deficiency
- short term
Intermittent supplementation with high
dose vitamin A:
targeted
vertical programme
integrated programme – with MCH; EPI
43 countries combining vitamin A
supplementation with immunization

Control of vitamin A deficiency
- medium term
Food supplementation: Preferred strategy in India through Anganwadi
(kindergarten programme)
Food fortification: Artificially increases the vitamin A content of foods
Must not alter the colour, taste, shelf life, cost
Must be consumed in small amounts on a regular basis by the target population
Examples: rice, cooking oil, monosodium glutamate
Challenges
Genetic modification – “golden rice”

Fortified foods
“Golden rice” Fortified sugar

Biofortification: cross breeding

Biofortification: cross breeding

Control of vitamin A deficiency
- long term
Address underlying causes:
– Alleviation of poverty
– Improved water and sanitation
– Improve environmental hygiene
– Female education
– Home gardening
– Health education
– Nutrition education
– Improve primary health care, and health services

Control of vitamin A deficiency
- long term
Change foods eaten:
– Availability
– Cost
– Cultural factors
– Beliefs and taboos
Change food preparation:
– Solar drying out of UV light
– Reduce cooking

Control of vitamin A deficiency
- preferred strategies
Vitamin A supplementation
Food diversification
Food fortification

Impact of control of vitamin A
deficiency
Marked decline in xerophthalmia in many
developing countries
Anecdotal evidence of fewer children with
bilateral corneal ulceration
Decline in scarring as a cause of blindness in
some countries (Uganda)
Lower rates of corneal blindness in younger
children than in older children

Change in the prevalence of clinical vitamin
A deficiency in children aged <6years
0
0.5
1
1.5
2
2.5
3
3.5
Phillipines Niger India Bhutan Sri Lanka Indonesia Ethiopia Nepal
Pre
va
len
ce
(%
)
Baseline
After 10 yrs
UN ACC/SCN 1997

Change in VAD in Asian and African
children (% change / 10 years)
UN ACC/SCN 1997 -100
-80
-60
-40
-20
0
20
40
60
80
Phillip
ines
Sri L
anka
Indon
esia
India
Bhuta
n
Eth
iopia
Nep
al
Nig
er
Ch
an
ge
in p
rev
ale
nce
/ 1
0 y
ears
(%
)

Estimated change in number of children
with clinical VAD 1985-1995 (million)
1985 1995
South Asia 2.67 1.58
East Asia/Pacific 0.66 0.40
L America/Caribbean 0.17 0.12
East/S Africa 0.69 0.53
West/Central Africa 0.53 0.45
Middle East/N Africa 0.24 0.12
Total: 5.00 3.30
UN ACC/SCN 1997

VADD in Sub-Saharan Africa • Data from 11 surveys between 1997 and 2003, and the measured effects of
vitamin A deficiency on child mortality were combined to estimate the prevalence
of children at risk for vitamin A deficiency in sub-Saharan Africa and the potential
child-survival benefits of effective and sustained policies and programs for the
control of vitamin A deficiency in this region.
• In the absence of effective and sustained policies and programs for the control
of vitamin A deficiency, an estimated 42.4% of children 0 to 59 months of age in
sub-Saharan Africa (43.2 million children) are at risk for vitamin A deficiency.
Such effective and sustained policy and program action for the control of vitamin
A deficiency can bring about a potential 25% reduction in mortality in children 0
to 59 months with respect to 1995 mortality levels (i.e., before the onset of large-
scale vitamin A supplementation programs in sub-Saharan Africa
Vitamin A deficiency and child survival in sub-Saharan Africa: A reappraisal of
challenges and opportunities Victor M. Aguayo and Shawn K. Baker. Food and
Nutrition Bulletin, 2005 26 348-355.

The State of the Worlds Children (2008)
• >40 countries in Africa have under 5 mortality
rates (U5MR) above the level used to indicate
that VADD is a public health problem (i.e.
>50/1,000 live births),
• 37 countries have U5MRs >100/1,000
• Coverage with supplements:
o poor data in many countries
o probably not as good as anticipated
o much more to be done
VADD in Sub-Saharan Africa