ventricular thrombosis and systemic embolism in bodybuilders: etiology and management
TRANSCRIPT

that the rate of blood loss via the chest tube [3] as thebasis for urgent thoracotomy can be inaccurate becauseof the formation of clots.
References
1. Hawkins ML, Carraway RP, Ross SE, Johnson RC, Tyndal EC,Laws HL. Pulmonary artery disruption from blunt thoracictrauma. Am Surg 1988;54:148–52.
2. McKeown PP, Rosemurgy A, Conant P. Blunt traumaticrupture of pulmonary vein, left atrium and bronchus. AnnThorac Surg 1991;52:1171–2.
3. Miura H, Taira O, Hiraguri S, et al. Blunt thoracic injury. JpnJ Thorac Cardiovasc Surg 1998;46:556–60.
INVITED COMMENTARY
This case, with its discussion, again emphasizes theimportance of a working familiarity with basic patho-physiology when treating thoracic trauma. Althoughtrauma systems—centers and organized training pro-grams—have increased the salvage rate of severely in-jured patients, the high volume, necessary “check list”approach, and usual absence of thoracic surgeons ininitial management may be deleterious.
This patient survived because the improperly function-ing chest tubes did not allow exsanguination. The bleed-ing raised the intrapleural pressure to above atrial andpulmonary vein pressures, arresting further hemorrhage.When the tubes were blocked by clot or clamps thepatient could be resuscitated and transferred, and surgi-cal repair successfully accomplished.
Two generations ago, observations of many similarcases led to a policy of delaying chest tube insertion fortreatment of hemothorax until the patient was fullyevaluated and definitive treatment could be undertaken.The beneficial factors of low pulmonary vascular andatrial pressures and intrinsic lung clotting factors arenegated with an immediate chest tube, especially withsuction applied. Chest tube insertion for hemothoraxmay occasionally precipitate massive exsanguination in apreviously relatively stable patient. Delay in tube drain-age for an hour or two while the patient is evaluated andan operating room made available is usually wiser. (Se-rious respiratory distress from airway or systemic vascu-lar leaks obviously requires immediate tube decompres-sion of the pleural space.)
Interestingly, this patient did not require endotrachealintubation and artificial ventilation even though his oxy-gen saturation was only 85%, equivalent to a PaO2 ofabout 60 mm Hg, or lower. I wonder what would havehappened in most American trauma centers.
James W. Pate, MD
Department of SurgeryUniversity of Tennessee956 Court AveMemphis, TN 38163
Ventricular Thrombosis andSystemic Embolism in Bodybuilders:Etiology and ManagementKathryn McCarthy, MB, BS, Augustine T. M. Tang,FRCS, Malcolm J. R. Dalrymple-Hay, FRCS, andMarcus P. Haw, FRCS
Department of Cardiac Surgery, Wessex Cardiac & ThoracicUnit, Southampton General Hospital, Southampton, UnitedKingdom
Increased thrombogenicity and acute embolism are well-recognized complications of chronic anabolic steroidabuse. The following cases highlight such dangers insteroid-enhanced bodybuilders who developed intracar-diac thrombosis that subsequently embolized. Systemicanticoagulation and surgical thrombectomy constitutedthe mainstay treatment. This represents the first report ofsuch devastating cardiovascular complications after ana-bolic steroid abuse and their management.
(Ann Thorac Surg 2000;70:658–60)© 2000 by The Society of Thoracic Surgeons
Adverse systemic effects of anabolic steroid abuseincluding arterial thrombosis are well documented.
However, thrombosis in the left ventricle and the pro-pensity for systemic embolism have hitherto not beenrecognized. We describe our experience of this compli-cation in two young bodybuilders who followed differentmanagement strategies.
Case Reports
Patient 1
A 35-year-old competitive bodybuilder presented with a3 day history of central chest pain, back pain, andbreathlessness following a 4 to 6 week flulike illness. Hewas an exsmoker with a family history of coronary arterydisease and had been “cycling” various testosteroneanalogs including nandrolone and nandralone for manyyears. Cycling involves 2 to 3 months of continuousadministration of the drug punctuated by abstinence of 2to 3 weeks. Electrocardiography confirmed sinus rhythm.Myocarditis was initially diagnosed for which angioten-sin-converting enzyme inhibitors and diuretics were in-stituted. The patient was allowed to continue with ana-bolic steroid treatment to avoid withdrawal problems.However, despite treatment he developed pulmonaryedema and transthoracic echocardiography demon-strated dilated cardiomyopathy with severe global left
Accepted for publication Dec 14, 1999.
Address reprint requests to Dr Tang, Department of Cardiac Surgery,Wessex Cardiac & Thoracic Unit, Southampton General Hospital, Tre-mona Rd, Southampton SO16 6YD, United Kingdom; e-mail: [email protected].
658 CASE REPORT McCARTHY ET AL Ann Thorac SurgANABOLIC STEROID AND VENTRICULAR THROMBECTOMY 2000;70:658–60
© 2000 by The Society of Thoracic Surgeons 0003-4975/00/$20.00Published by Elsevier Science Inc PII S0003-4975(00)01572-1
ventricular dysfunction. Steroid-induced cardiomyopa-thy was suspected, which led to the immediate cessationof the drug. Echocardiograhy repeated 5 days later dem-onstrated a large pedunculated thrombus in the leftventricle. After systemic anticoagulation the thrombusdisappeared between the seventh and eighth day oftreatment and echocardiography showed return of nor-mal left ventricular function. However, 4 days later hecomplained of sudden pain in both feet. Clinical assess-ment suggested acute embolic occlusion of the tibialarteries, most probably from the ventricular thrombus,although critical ischemia was absent in either leg. Thesymptoms completely resolved with expectant treatmentand continued systemic anticoagulation before discharge.At 6 months’ follow-up the patient staged a full recovery.
Patient 2A 31-year-old casual bodybuilder presented with bilat-eral acute ischemic legs after harboring a 6-month his-tory of recurrent leg pain initially managed by his familyphysician as tendinitis. Clinical assessment revealed nolimb pulses distal to the right groin and the left poplitealfossa. The patient was a nonsmoker with no familyhistory of arteriosclerosis and had been cycling variousanabolic steroids—testovarin, sustanon, and dianabol—for 8 years. The only abnormal blood test was an in-creased C-reactive protein level of 53.1. Angiographyshowed normal aortic arch, ascending and thoracic aorta,but total occlusion of the right superficial femoral artery(Fig 1) with no distal filling and occluded left poplitealartery with collateral distal filling. Transthoracic echocar-diography revealed the embolic source to be a largepedunculated thrombus in the left ventricle and mildglobal ventricular dysfunction (Fig 2). Urgent operation
was undertaken to prevent further embolization andrevascularize the limb. After median sternotomy andinstitution of cardiopulmonary bypass, an aortotomy wasmade under cardioplegic arrest to allow the ventricularthrombus (2 by 3 cm) to be retrieved across the aorticvalve. After saline lavage of the ventricle, intraoperativetransesophageal echocardiography demonstrated no re-sidual thrombus. This was confirmed by transthoracicechocardiography on the following day. Right femoralembolectomy was performed under the same anesthetic.The patient made an uneventful postoperative recoverywith satisfactory limb perfusion, normal left ventricularfunction, and adequate systemic anticoagulation beforedischarge.
Comment
Anabolic steroid abuse is an increasing problem, partic-ularly among athletes and bodybuilders striving for ex-cellence. Ready access through local outlets and theInternet undoubtedly contributed to the recent surge insteroid usage. However, little or no warning of poten-tially fatal adverse effects is usually given.
Cycling involves administering one or more steroids,typically in doses 10 to 100 times greater than those usedtherapeutically for more than 6 to 12 weeks with intervalsof steroid-free “holidays.” This regime is believed tomaximize end-organ effects, prevent gradual loss of ben-efits with chronic usage, and avoid detection on drugtesting. When received in large doses, often by body-builders, the pituitary–testicular axis frequently becomessuppressed resulting in testicular atrophy and azoosper-mia [1]. Other common problems include gynecomastia,hot flushes, and fluid retention [1]. Premature closure ofepiphyseal plates has also been reported in teenageanabolic steroid users resulting in stunted growth. Seri-ous cardiovascular complications reported include sys-temic arterial thrombosis leading to acute ischemic legs[2], brain injury [3], myocardial infarction, ventriculararrhythmia, and congestive heart failure [4]. The inci-dence of intracardiac thrombosis was once recognized in
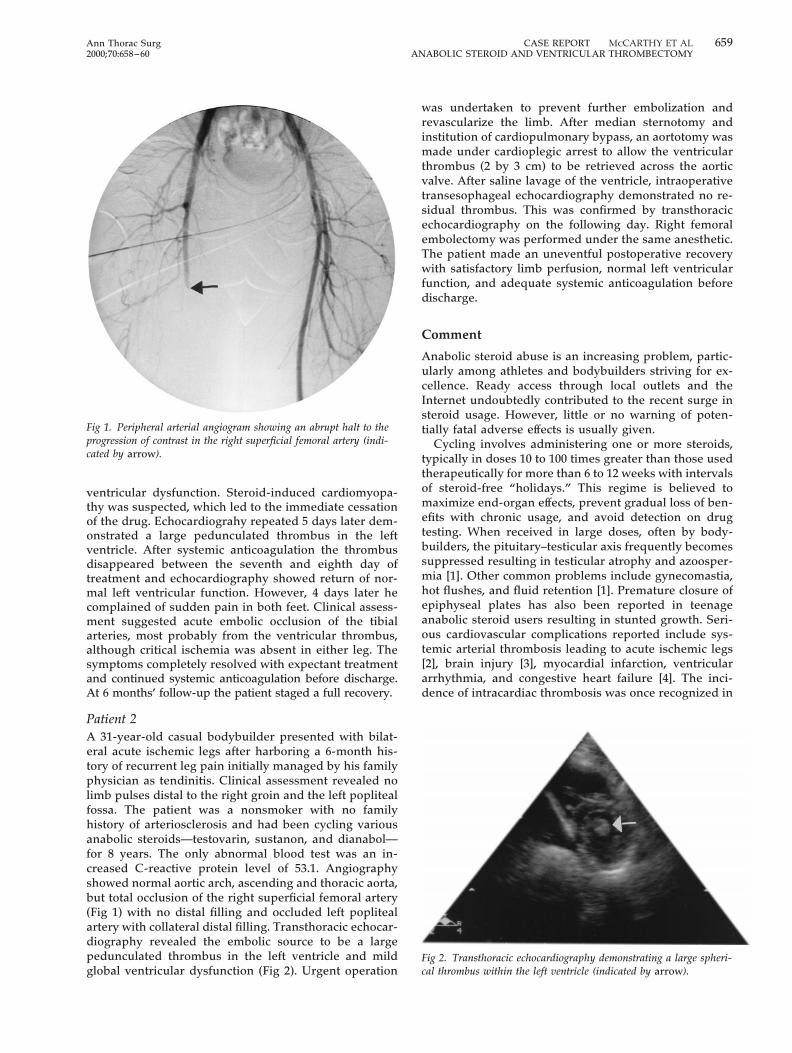
Fig 2. Transthoracic echocardiography demonstrating a large spheri-cal thrombus within the left ventricle (indicated by arrow).
Fig 1. Peripheral arterial angiogram showing an abrupt halt to theprogression of contrast in the right superficial femoral artery (indi-cated by arrow).
659Ann Thorac Surg CASE REPORT McCARTHY ET AL2000;70:658–60 ANABOLIC STEROID AND VENTRICULAR THROMBECTOMY

association with anabolic steroid usage, although afternonintervention, the patient was lost to follow-up [4]. Thepedunculated nature of these thrombi, as opposed toplatelike mural thrombus commonly encountered, maypartly explain their propensity for embolization. Thesepatients represent reports of successful intervention forventricular thrombosis and systemic embolization asso-ciated with chronic abuse of anabolic steroid.
In summary, having adopted a conservative approachin the first patient, he was fortunate to escape neurologicsequelae. We would now recommend early surgical in-tervention to avoid potentially lethal thromboemboliccomplications.
References
1. Marshall E. The drug of champions. Science 1988;242:183–4.2. Falkenberg M, Karlsson J, Ortenwall P. Peripheral arterial
thrombosis in two young men using anabolic steroids. Eur JEndovasc Surg 1997;13:223–6.
3. Laroche GP. Steroid anabolic drugs and arterial complica-tions in an athlete: a case history. Angiology 1990;41:964–9.
4. Nieminen MS, Ramo M, Vitasalo M, et al. Serious cardiovas-cular side effects of large doses of anabolic steroids in weightlifters. Eur Heart J 1996;17:1576–83.
Radiation-Induced GastrointestinalStromal Sarcoma of the EsophagusPreston R. Miller, MD, Stephanie L. Jackson, MD,Benoit C. Pineau, MD, and Edward A. Levine, MD
Departments of Surgery and Pathology, Sections ofGastroenterology and Surgical Oncology, Wake Forest UniversitySchool of Medicine, Winston-Salem, North Carolina
Esophageal sarcoma is an uncommon tumor, sporadicallyreported in the literature. Radiation therapy is frequentlyemployed in the treatment of carcinoma of the esopha-gus, and the increased risk of development of sarcomaarising in irradiated fields is well known. However, to ourknowledge, the occurrence of radiation-associated sarcomaof the esophagus after radiation therapy for carcinoma ofthe esophagus has not been reported. We therefore reportthe case of a 43-year-old female who developed a gastroin-testinal stroma sarcoma 9 years following radiation ther-apy for esophageal squamous cell carcinoma. The patientunderwent resection of her gastrointestinal stromal sar-coma by transhiatal esophagectomy with cervical anasto-mosis and is doing well 18 months later. The increasinguse of radiation therapy for esophageal carcinoma sug-gests that radiation-associated sarcoma of the esophagusmay be seen more frequently in the future.
(Ann Thorac Surg 2000;70:660–2)© 2000 by The Society of Thoracic Surgeons
Esophageal sarcoma is an unusual lesion of the esoph-agus. Its incidence is far overshadowed by the more
common squamous cell carcinoma and adenocarcinoma.Reviews of large tumor registries over nearly 50 yearsshow that esophageal sarcoma comprised less than 0.5%of esophageal malignancy [1]. The precise etiology ofsarcoma is likely multifactorial, with the majority ofpatients having no risk factors. However, there is a clearassociation between the development of sarcoma andprior exposure to radiation. This association was firstreported in animals just after the turn of the century andclinically in 1922 [2]. The patients at greatest risk forradiation-associated sarcoma (RAS) undergo radiationtherapy (RT) for primary malignancies associated withgood survival rates. The reported incidence of RAS islow, ranging from 0.03% to 2.6% of patients treated withtherapeutic radiation [3].
The patient, a 43-year-old white female, was diagnosedwith squamous cell carcinoma of the esophagus in 1990.This initial lesion was in her midesophagus on bariumswallow and esophagoscopy. Computed tomographyshowed regional adenopathy with no evidence of distantmetastatic disease. The patient refused any attempt atsurgical therapy. Consequently, she received RT with atotal dose of 60 Gray to her entire esophagus in anattempt to treat both her primary lesion and her supra-clavicular adenopathy. She had a complete response, andfor 9 years had no clinical evidence of disease ordysphagia.
Nine years later, the patient developed dysphagiainitially for solids and eventually for liquids associatedwith a 5 lb weight loss over several months. Esophagos-copy revealed a mass in the distal esophagus. Biopsy atthis time confirmed a malignancy. An esophagram ancomputed tomography showed a mass in the distalesophagus with no evidence of metastasis. She subse-quently underwent a transhiatal esophagectomy withcervical anastomosis and pyloromyotomy, which shetolerated well. On postoperative day 5, a water solublecontrast swallow was obtained which showed no stenosisor leak. She was discharged home on postoperative day 9and is currently doing well 12 months after surgery.
A review of the patient’s previous biopsy material from1990 revealed invasive, moderately differentiated squa-mous cell carcinoma (Fig 1). The esophagectomy (1998)specimen demonstrated a 6.5 3 4 3 2.5 cm exophytic,ulcerated tan mass in the distal esophagus, several cen-timeters distal to the area of the original tumor from 1990.Examination of the tissue from the area of the previouslytreated squamous cell carcinoma revealed no histologicabnormalities. There was no evidence of in situ carci-noma on detailed examination of the mucosa. Micro-scopic examination of the tumor revealed a submucosalproliferation of plump spindle-shaped cells with scat-tered pleomorphic mono- and multinucleate tumor cellsbeneath an intact, unremarkable squamous mucosa (Fig2). Numerous atypical mitoses were present. Immuno-peroxidase studies revealed the tumor to be negative forcytokeratins (AE1/AE3, CAM5.2, MNF, and 903), S100
Accepted for publication Dec 16, 1999.
Address reprint requests to Dr Levine, Section of Surgical Oncology,Wake Forest University School of Medicine, Medical Center Blvd, Win-ston-Salem, NC 27157; e-mail: [email protected].
660 CASE REPORT MILLER ET AL Ann Thorac SurgRADIATION-INDUCED ESOPHAGEAL SARCOMA 2000;70:660–2
© 2000 by The Society of Thoracic Surgeons 0003-4975/00/$20.00Published by Elsevier Science Inc PII S0003-4975(00)01305-9