ventilator associated pneumonia: new for 2008 - ucsf … · ventilator associated pneumonia: new...
TRANSCRIPT

Ventilator Associated Pneumonia: New for 2008
Jeanine P. Wiener-Kronish, MDHenry Isaiah Dorr Professor of Research and Teaching in Anaesthetics and AnaesthesiaDepartment of Anesthesia and Critical CareAnesthetist-in-ChiefMassachusetts General Hospital

Objectives for TalkObjectives for Talk
• Endotracheal tubes are a conduit from the mouth to the lung
• What is an infection in a organ filled with bacteria
• Ideas regarding management

TAKE HOME POINTS• We do not have optimal dx tests or gold
standard for VAP• Therefore it should not be used as a
quality measure• Always use gloves and use alcohol based
soaps before and after examining each patient
• Patients should be extubated as quickly as possible--Daily wake-up from sedation-- consider daily weaning trials/ non-invasive ventilation
• Consider quantitative cultures as a method of discontinuing un-necessary tx

VAP-Wrong Benchmark
• No consensus as to clinical dx• CDC criteria is very subjective• Difficult to modify hospital processes and
eliminate VAP• ATS, SCCM, ACCP will be coming out with
letter protesting VAP as a benchmarkKlompas M Ann Intern Med 2007;147:803-5

The Major Issues• Antibiotic treatment of ventilator associated
pneumonia( VAP) has to be early and appropriate to improve patient outcomes
• ~30% of intubated patients develop VAP• Fifty percent of ICU patients receive broad-
spectrum antibiotics, for VAP. This practice has contributed to a crisis of increasing antibiotic resistance in pathogenic bacteria
• Antibiotic resistance is like second-hand smoke in the ICU

Antibiotic Tx• Failure to start appropriate antibiotic treatment-
increased costs, increased healthcare utilization, increased morbidity and mortality
• Unnecessary administration of antibiotics-- increased costs, increased risks for adverse drug reactions, selection of resistant microbial flora, poorer outcomes
• Use of antibiotics alters ecology in ICU--increases cross-colonization and increases infections with resistant pathogens in ICU [Affects study design]
Lisboa Curr Opin Infect Dis 2008;21:174-178Hurley J Antimicrobial Chemotherapy Epub ahead March 8, 2008

Antibiotic Resistance
• Netherlands, Canada, Scandinavia do not have increasing antibiotic resistance.
• Strict isolation and restricted antibiotic administration appears to help control resistance.
Conclusion for Introduction
• What objective data identify the intubated patients that are truly infected?
• Goal should be both to treat people who are infected and not to treat people who do not need antibiotics

Definitions

Infection vs Colonization• Infection -Finding bacteria in a normally
sterile environment;• Defined as a decrease in host fitness;
the patient has sustained some decrement in organ function due to bacterial-induced injury
• Colonization - bacterial present but no decrement in organ function

Evaluation of ET tube Colonization
• Evaluated 10 healthy men (mean age 35) intubated for trauma
• 9/10 colonized within 12h with rapid increase in numbers of bacteria over 24h and peak at 96h
• Organisms in lung come from oropharynx and gut
Feldman- Eur Resp J 1999;13:546-551

Evaluation of ET tube Colonization
• Evaluated 10 healthy men (mean age 35) intubated for trauma
• 9/10 colonized within 12h with rapid increase in numbers of bacteria over 24h and peak at 96h
• Organisms in lung come from oropharynx and gut
Feldman- Eur Resp J 1999;13:546-551
Molecular Characterization of Oral Flora
• Obtained tongue swabs from trauma victims right before bronchoscopy performed
• Compared cultures of tongue swabs and BAL
• Compared molecular characterization of bacteria in mouth and in BAL
Bahrani-Mougeot FK JClin Micro 2007; 45: 1588-1593.

16S rRNA gene
Identical in all bacteria
Differs between bacteria
16S F 16S R
PCR to obtain the 16S rRNA gene from all bacteria in a sample

Findings from Tongues• 88% of bacteria found on tongue swabs
identified using molecular tools --also present in BAL
• Data suggests oral secretions source of bacteria in lungs
• 56% bacteria found with molecular tools not found by microbiology lab
Bahrani-Mougeot FK JClin Micro2007; 45: 1588-1593.
Teeth and Plaque• 25% of nursing home patients(NHP) have
respiratory pathogens in their dental plaques• 11/49 NHP had dentures and were
significantly less colonized (27% vs 66%)• Dental plaque cultures obtained prior to
development of VAP documented the same bacteria (PFGE) in plaque that then appeared in VAP cultures
El-Solh Chest 2004:126:1575-1582

Bacteria in Mouthwash• Report of administration of alcohol-free
mouthwash that was contaminated with Burkholderia cenocepacia
• Ventilated patients died of respiratory infections with this bacteria; others had respiratory illness with this bacteria
• Documents aspiration of oral flora and importance of oral flora
• Consider using alcohol-containing mouthwash, esp. chlorhexidine
Kutty Chest 2007; epub ahead of print

Conclusions RE: Colonization
• Oropharyngeal colonization, which may be due to dental plaque and/or placement of ET (or NG) tubes, appears to be the major source of bacteria for bacterial-induced VAP
• Bacteria form biofilms on tubes within hours of placement
• How do we know when patients are just colonized or when they have become infected??
Gorman Eur J Clin Microbiol Infect Dis 1993;12:9-17

Diagnosis

Diagnosis of VAP• 48 Hours of Hospitalization- Patients develop2 of 3 of the following:• Fever > 38.5oC or hypothermia; • Leukocytosis >10,000 or leukopenia <4000• Purulent secretions and new and persistent/progressive infiltrate on
chest radiograph (except ARDS)

Diagnosis of VAP• Criteria have high sensitivity but very low
specificity• Will overtreat if use only these criteria--
only 50% of patients diagnosed with VAP using the clinical criteria have lung infections
• How to confirm the dx?Lisboa Curr Op Infect Dis 2008;21:174-178

Postmortem vs clinical dx VAP
• 25 patients had autopsy evidence of VAP• CXR-13/25 had localized infiltrates;7 had
diffuse;5 had no chest radiograph findings• WBC-15/25 had increased-- 10 did not• Purulent secretions-16/25 had some-9 did not
Fabregas N Thorax 1999;54:867-873
How to tell if there is VAP??• CRP and Procalcitonin--no adequate cut-off for definitive dx• CRP does go down with adequate
antibiotic tx• Combining biomarkers with clinical
signs may be valuableLisboa Curr Op Infect Dis 2008;21:174-178

Thresholds for Quantitative Cultures

Bacterial Thresholds for “Infections”
• Obtained BALs and Protected brush specimens in patients who had just died- samples within 1 hour of death
• Did thoracotomies and took lung out that had been sampled
• Cultured lungs--infected lungs grew 104cfu/gram of lung
Chastre J Am Rev Respir Dis 1984;130:924-9

Sensitivities/Specificities of Tests
• Bronchoscopic BAL at 104cfu/ml- 91% sensitive and 78% specific
• Chastre J Am Rev Respir Dis 1984;130:924-9
• Blind Mini-BAL at 103 cfu/mL was 78% sensitive and 86% specific --used 20ml and retrieved 2ml
Bregeon F.Eur Respir J 2000;16:969-975

Comparisons to Bronchoscopic BAL
• Perform repeated BALs-75% reproducibility
• Quantitative Cultures of endotracheal aspirates- if use threshold of 106cfu/ml has a sensitivity of 68% and specificity of 84%
Jourdain B Am J Respir Crit Care Med 1995;152:241-6

Threshold in VAP in Trauma Patients
• Performed fiberoptic bronchoscopy and BAL- 100 mL on 526 patients
• Stopped antibiotics if BAL cultures were less than 105cfu/ml
• Followed patients, if became febrile again then had another BAL--if then had a culture with 105cfu/ml first BAL called a false- negative study
Croce MA J Trauma 2004;56:931-936
Outcomes of Trauma Patients
• Highest mortality in patients with 105cfu/ml-- 17% vs 15% for 104 cfu/ml and 13% for 103
cfu/ml or less; not statistically different• 43/1372 BALs considered false negative as
next BAL[within 7 days] over threshold;36 had 104cfu/ml and 8 had fewer than 1000 cfu/ml
• They suggest they accept 104cfu/ml for Pseudomonas and Acinteobacter
Croce MA J Trauma 2004;56:931-936

Chronic Ventilator Patients• 14 patients in chronic ventilator facility; all
have tracheostomies and had been on for > 5 months
• All 14 had > 104 cfu/mL in distal airways without fever, white count or chest radiograph findings
• After tracheostomies and on chronic ventilation see high bacterial burdens constantly
Baram D Chest 2005;127:1353-1357

Use Test Data • Heyland compared invasive, quantitative cultures of
BAL to noninvasive, nonquantitative culture of tracheal aspirate
• No differences in antibiotic administration or outcomes --excluded MRSA and P.aeruginosa
• No de-escalation of antibiotics even when cultures were negative! Did not use data from tests
Canadian Critical Care Trials Group N Engl J Med 2006;355:2619-2630

Conclusions on Thresholds• Quantitative Cultures may allow you to
discontinue antibiotics--and may help decrease antibiotic resistance
• Maybe able to use higher thresholds in trauma patients
• Appears safe to with-hold antibiotics if patient not have large quantity of bacteria, if patient is getting better and lack of ongoing data that patient has lung infection
Prevention

DECREASE SEDATION• Documentation that daily interruption of
infusions of analgesics and sedatives led to:– Significant reduction of mechanical ventilation– Shorter ICU length of stay– Fewer diagnostic tests for mental status--With less posttraumatic stress disorder (PTSD)
Kress JP Am J Respir Crit Care Med. 2003:168:1457-1461;Schwickert WD Crit Care Med 2004;32:1272-1276
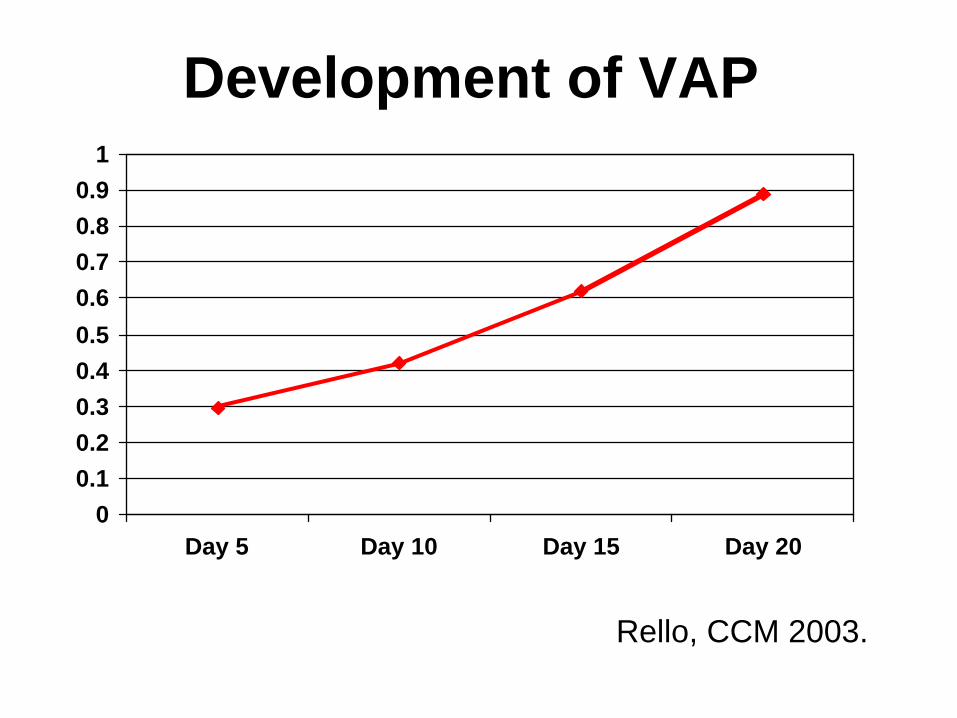
Development of VAP
00.10.20.30.40.50.60.70.80.9
1
Day 5 Day 10 Day 15 Day 20
Rello, CCM 2003.

Prone Position?• Meta-analysis of prone position trials• Found a non-significant trend to
decrease VAP [23% reduction in the odds for VAP]
• Could be due to decreased aspiration of secretions
Abroug Intensive Care Med 2008 Epub ahead of print March 19

Tracheostomy• Advantages of tracheostomy-Decreases airway resistanceFewer oral-labial ulcerationsBetter oral hygieneImproves airway securityBetter patient comfortMaybe fewer pulmonary infectionsCombes A Crit Care Med 2007;35:802-7

Tracheostomies in France• Retrospectively analyzed 1629 consecutive
patients ventilated for more than 3 days- found 506 patients
• 166 tracheostomized after a median ventilation of 12 days
• Increased mortality in patients without trachs- -48% vs 37% in hospital mortality
[p= .03]• Matched case-control-trach patients again
lower in hospital mortality[36% vs 50%]Combes A Crit Care Med 2007;35:802-7

More on Tracheostomies• Kollef studied 521 patients ventilated for >
12h and the 51 patients with trachs had lower ICU and hospital mortality rates
• Rumbak- prospective, randomized trial of 120 patients where patients had trach within 48h;the patients with early trachs had 32% mortality with 62%mortality with later trach
Rumbak MJ Crit Care Med 2004;32:1689-1694Kollef MH Crit Care Med 1999;27:1714-1720

Why Trach?• Less sedation--so probably less aspiration of
both oral and GI flora• Endotracheal Tube in mouth leads to more
changes in oral flora with probably more pathogenic flora colonizing mouth and being aspirated
• Safer when moving patient--patient gets out of bed more
Chlorhexidine• Koeman et al: Decreased VAP if use
Chlorhexidine in gel on teeth and gums• Segers et al: Decreased VAP if use
chlorhexidine rinses 4 times a day and put into nares
• Chlorhexidine has been shown to be a superior antiseptic rinse in periodontal literature
Segers P JAMA 2006;296:2460-2466Koeman M Am J Respir Crit Care 2006;173:1348-1355


Subglottic Suction Devices• New device coming from the makers of LMA--
in anesthetized patients, 5% vs 67% VAP with standard cuffs
• Studies with CAS System have shown an absolute decrease of VAP by 5% and prolongs the time to VAP
Young PJ Crit Care Med 2006;34:632-639Valles J Ann Intern Med 1995;122:179-86

Surveillance Cultures• W/in 12 h of admission, blinded
miniBAL ; 20-30mL sterile saline• Repeated every 48 h and then 3 times a
week; not done on >70% Fi02• Did gram stains and % of intracellular
organisms• Daily screening with CPISBoots Respirology 2008;13: 87-96

Surveillance Cultures cont• Surveillance cultures predicted up to
90% of the organisms causing VAP• Concordance of 90% if specimen within
48 h of VAP• Did not find quantification of cultures
helpful• Found high and stable concentrations of
MRSA and P.aeruginosa-- no change with antibiotic therapy
• Boots Respirology 2008;13: 87-96

Conclusions RE: Prevention• Consider tracheostomies by 14 days-• If new study results compelling, more
trachs• Consider chlorhexidine- downside is
possible discoloration of teeth that can be cured with polishing teeth
• Consider subglottic suctioning systems

Predictions for Future
• Antibiotics should be given only to patients who are infected
• Infections will be diagnosed quickly using molecular techniques to identify patients with a high burden of bacteria and signs of infection using objective data, which will include biomarkers
