pneumonia krn ventilator peri
DESCRIPTION
pneumoni karena ventilator periTRANSCRIPT

DOI: 10.1542/neo.15-6-e2252014;15;e225Neoreviews
Jeffery S. GarlandVentilator-Associated Pneumonia in Neonates: An Update
http://neoreviews.aappublications.org/content/15/6/e225located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1526-9906. 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Online the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,it has been published continuously since . Neoreviews is owned, published, and trademarked by Neoreviews is the official journal of the American Academy of Pediatrics. A monthly publication,
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

Ventilator-Associated Pneumonia inNeonates: An UpdateJeffery S. Garland, MD,
SM*
Author Disclosure
Dr Garland has
disclosed no financial
relationships relevant
to this article. This
commentary does not
contain a discussion of
an unapproved/
investigative use of
a commercial product/
device.
Practice Gaps
1. Accurately determining the specific organism responsible for ventilator-associated
pneumonia is challenging in neonates.
2. Few randomized trials have been conducted to evaluate measures to prevent
ventilator-associated pneumonia in neonates.
3. It is not known whether a level or head-elevated position influences the risk of
ventilator-associated pneumonia (VAP).
AbstractHealth-care–associated infections affect neonatal morbidity and mortality, as well aslength of stay and hospital costs. Ventilator-associated pneumonia (VAP) accountsfor 6.8% to 32.2% of these infections. Low birthweight, duration of mechanical ven-tilation, opiate treatment for sedation, frequent suctioning, and reintubation have allbeen shown to increase the risk of VAP. Both Gram-positive and Gram-negative or-ganisms that originate from endogenous or exogenous sources are responsible forVAP. Accurately diagnosing VAP in neonates is challenging because procedures suchas tracheal aspirate culture and Gram-stain have low sensitivity, specificity, and positivepredictive value. Although several authors have shown that bronchial aspirates throughnonbronchoscopic bronchoalveolar lavage improve diagnostic accuracy, further stud-ies are needed to investigate the diagnostic value and safety profile of these procedures.Very few randomized trials have been conducted in neonates to evaluate methods toprevent VAP, and thus most neonatal VAP prevention recommendations are based onadult trials. This review summarizes the epidemiology, pathogenesis, diagnosis, andtreatment of VAP and touches on a number of practical steps to prevent VAP inneonates.
Objectives After completing this article, the reader should be able to:
1. Describe the risk factors for neonatal ventilator-associated pneumonia (VAP).
2. Describe the current methods used to diagnose neonatal VAP.
3. List the most common organisms responsible for neonatal VAP.
4. Explain initial treatment of neonatal VAP.
5. Outline steps to prevent neonatal VAP.
IntroductionThe Centers for Disease Control and Prevention (CDC) defines ventilator-associated
pneumonia (VAP) as an episode of pneumonia in a patientwho requires a device to assist or control respiration througha tracheostomy or endotracheal tube within 48 hours beforethe onset of the infection. (1) Although the exact incidenceof VAP is difficult to determine, VAP may be responsible foras many as one-third of the health-care–related infections inneonates. (2)(3)(4)(5)(6) The present review summarizesthe epidemiology, suspected pathogenesis, diagnosis, treat-ment, and strategies for the prevention of VAP in neonates.
Abbreviations
CDC: Centers for Disease Control and PreventionNHSN: National Healthcare Safety NetworkSDD: selective digestive tract decontaminationVAP: ventilator-associated pneumonia
*Director of Neonatal-Perinatal Research, Wheaton Franciscan Healthcare–St Joseph Hospital, Milwaukee, WI.
Article infectious diseases
NeoReviews Vol.15 No.6 June 2014 e225
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

EpidemiologyIncreased permeability of the skin and mucous mem-branes, decreased complement activity, lower concen-trations of immunoglobulins, and an immature anddysregulated immune system together increase the riskof health-care–acquired infections in critically ill neo-nates. Multiple physiologic mechanisms optimally protectthe lung parenchyma from infection, including: anatom-ical barriers; the cough reflex; the tracheobronchial mu-cociliary lining and secretions; and cell-mediated andhumoral immunity, including the phagocytic functionsof alveolar macrophages and neutrophils. If these de-fenses are impaired, absent, or overcome by a highinoculum of organisms or those of unusual virulence,pneumonitis ensues.
Data from the CDC’s National Healthcare Safety Net-work (NHSN) (2006–2008) at 304 participating hospi-tals revealed VAP rates of 2.36 and 2.08 per 1,000device-days among neonates weighing less than 750 gand between 750 and 1,000 g, respectively. (7) The truerate of neonatal VAP is difficult to establish. Radiographicidentification of neonatal pneumonia is difficult, compro-mised by evolving parenchymal changes due to broncho-pulmonary dysplasia and frequent episodes of atelectasis.Diagnostic procedures commonly used in adults to diag-nose VAP (eg, bronchoscopic bronchoalveolar lavage,protected specimen brushing) arerarely used in the neonatal intensivecare unit (NICU), in part due to thesmall size of neonatal endotrachealtubes. Retrospective cohort studiesconducted at single institutions re-port higher VAP rates (10.9–52 in-fections per 1,000 ventilator-days)than NHSN data. (2)(8)(9)(10)(11)(12)(13) Risk factors reportedto be significantly associated withVAP among ventilated neonatesalso vary from study to study. Lowbirthweight, prolonged mechanicalventilation, opiate treatment for se-dation, frequent suctioning and re-intubation, bloodstream infection,and steroid use have all been notedto be associated with increased riskof VAP. (14)(15)
PathogenesisOrganisms responsible for VAPcan originate from endogenous or
exogenous sources (Figs 1 and 2). A number of inves-tigators have described the role of pharyngeal andsubglottic secretions in the development of VAP inadults. (16)(17)(18)(19)(20) Contaminated oral orgastric secretions of intubated, ventilated adult patientscan pool above the cuff of the endotracheal tube, leakaround the cuff, and enter the lower respiratory tract. Be-cause neonates are ventilated with uncuffed endotrachealtubes, they are likely at greater risk for aspiration of con-taminated oral or gastric secretions. Within the first 48hours of mechanical ventilation, (21)(22) Gram-positiveoral organisms begin to colonize the trachea and endotra-cheal tube, and Gram-negative bacilli generally colonizeendotracheal tubes in place for longer than 48 hours.One study provided some evidence that neonatal position-ing may influence the incidence of lower respiratory tractbacterial colonization. (23) In this study, tracheal coloni-zation was less common among neonates placed in a lateralposition compared with neonates nursed in a supineposition.
Organisms responsible for VAP may also originatefrom the stomach, although the exact role gastric floraplays in the pathogenesis of VAP has been questioned.(24)(25) Torres et al (26) noted that VAP in adultswas more common among supine patients comparedwith semi-recumbent patients. Farhath et al (27) noted
Figure 1. Endogenous sources of organisms responsible for ventilator-associatedpneumonia (VAP). (Courtesy of Walt Earhart, Wheaton Franciscan Healthcare. From:NeoreviewsPlus� August 2010, Question 8, by AAP.)
infectious diseases ventilator-associated pnuemonia
e226 NeoReviews Vol.15 No.6 June 2014
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

that pepsin, a marker for gastric contents, was detected inthe trachea of 92% of a cohort of ventilated neonates, sug-gesting that contaminated gastric contents could maketheir way into the trachea of ventilated neonates. Basedon trials that used rigorous culturing techniques and stan-dard definitions of VAP, oropharyngeal colonization likelyplays a greater role than aspiration of contaminated gastricsecretions. (22) Although previous bloodstream infectionhas been identified as a risk factor for VAP, these infectionsdo not seem to be the source of VAP. (13) Bloodstreaminfections and translocation of bacteria from the gastroin-testinal tract are also believed to be an uncommon sourceof endogenous organisms responsible for VAP.
Exogenous sources may also be responsible for thepathogens causing VAP (Fig 2). Shortly after intubation,bacteria can coat the surface of endotracheal tubes andbecome enveloped within a biofilm produced by the mi-crobes. This biofilm can serve as an exogenous source oforganisms responsible for VAP. In a study of adult pa-tients, Adair et al (28) noted that 70% of patients whohave VAP had the same pathogens isolated from endotra-cheal biofilms and tracheal secretions. Pathogens thatcontaminate ventilator circuits, airway suctioning equip-ment, humidifiers, nebulizers, and, most importantly, care-givers’ hands (29) are sources of exogenous contamination
that can lead to VAP. Gram-negativeorganisms, which often colonize en-dotracheal tubes, are frequentlynoted in the flora that colonize thehands of caregivers. (30)(31)
MicrobiologyIn adult and pediatric patients inwhom reliable cultures can be ob-tained, Staphylococcus aureus andGram-negativeorganisms (Pseudomonasaeruginosa, Escherichia coli, Klebsiellapneumoniae, Enterobacter species, andAcinetobacter species) are the mostcommon pathogens responsible forVAP. Gram-negative organisms werenoted in 94% of tracheal aspiratesfrom neonates who had VAP in a co-hort reported by Apisarnthanaraket al. (13) S aureus was recoveredfrom w25% of cases, and multipleorganisms were recovered from air-way secretions in 58%of cases. In a re-cent work by Cernada et al, (32)gram-negative organisms (particu-
larly P aeruginosa) were responsible for 62% of VAPcases. This study diagnosed VAP by using bronchoalveolarlavage with a blind protected catheter; with this tech-nique, only 3 (16.7%) of 18 neonates had polymicrobialinfections.
DiagnosisThe primary controversy regarding VAP in neonates isthe criteria used to establish the diagnosis. (33) TheCDC’s NHSN VAP criteria included radiographic, clin-ical, and microbiologic elements. (1) The difficulty in ob-taining noncontaminated microbiologic specimens thatmeet quantitative definitions for infection led the CDCto include a purely clinical definition of VAP for infantsaged £1 year, as shown in Table 1. The criteria havenot been validated in neonates, and they are often opento subjective interpretation because they overlap witha number of disease processes. As of January 1, 2014,the CDC and NHSN no longer analyze data for neonatalpneumonia because the diagnosis is so subjective accord-ing to a CDC working group. (34) Neonatal units maystill perform internal VAP surveillance, but the data willnot be analyzed by the NHSN.
Microbiologic criteria for VAP are shown in Table 2.(1) Note that these criteria presume that pulmonaryspecimens are obtained by using invasive testing, such
Figure 2. Exogenous sources of organisms responsible for ventilator-associatedpneumonia (VAP). (Courtesy of Walt Earhart, Wheaton Franciscan Healthcare. From:NeoreviewsPlus� August 2010, Question 8, by AAP.)
infectious diseases ventilator-associated pnuemonia
NeoReviews Vol.15 No.6 June 2014 e227
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from
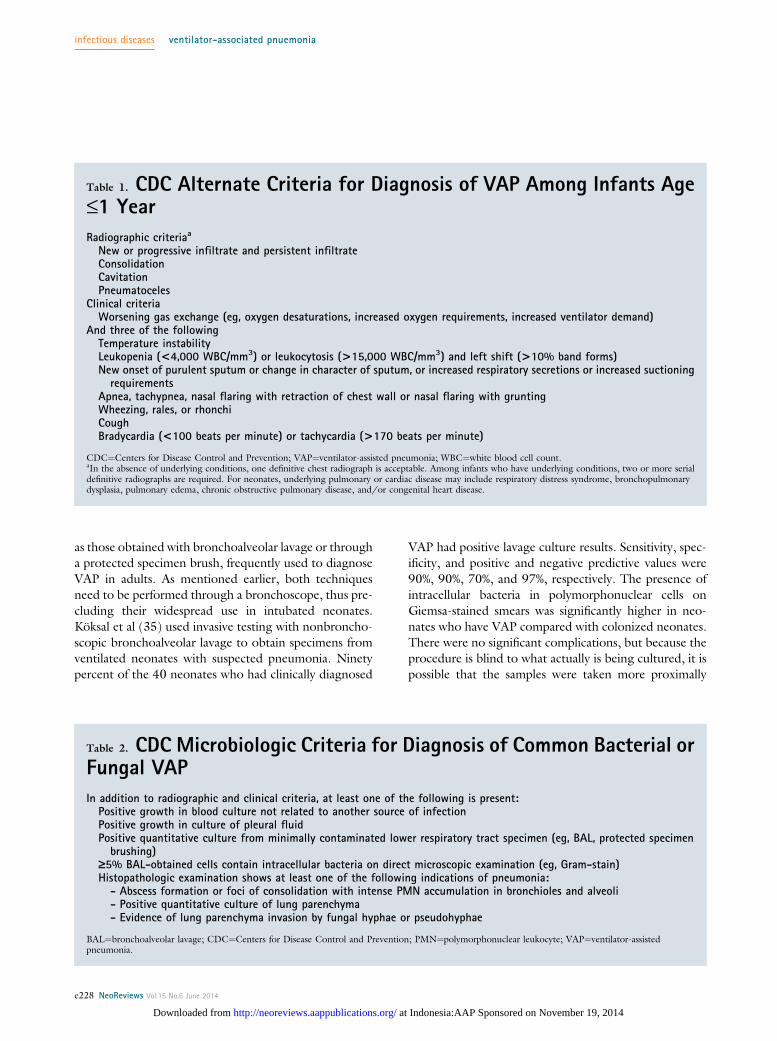
as those obtained with bronchoalveolar lavage or througha protected specimen brush, frequently used to diagnoseVAP in adults. As mentioned earlier, both techniquesneed to be performed through a bronchoscope, thus pre-cluding their widespread use in intubated neonates.Köksal et al (35) used invasive testing with nonbroncho-scopic bronchoalveolar lavage to obtain specimens fromventilated neonates with suspected pneumonia. Ninetypercent of the 40 neonates who had clinically diagnosed
VAP had positive lavage culture results. Sensitivity, spec-ificity, and positive and negative predictive values were90%, 90%, 70%, and 97%, respectively. The presence ofintracellular bacteria in polymorphonuclear cells onGiemsa-stained smears was significantly higher in neo-nates who have VAP compared with colonized neonates.There were no significant complications, but because theprocedure is blind to what actually is being cultured, it ispossible that the samples were taken more proximally
Table 1. CDC Alternate Criteria for Diagnosis of VAP Among Infants Age£1 Year
Radiographic criteriaa
New or progressive infiltrate and persistent infiltrateConsolidationCavitationPneumatoceles
Clinical criteriaWorsening gas exchange (eg, oxygen desaturations, increased oxygen requirements, increased ventilator demand)
And three of the followingTemperature instabilityLeukopenia (<4,000 WBC/mm3) or leukocytosis (>15,000 WBC/mm3) and left shift (>10% band forms)New onset of purulent sputum or change in character of sputum, or increased respiratory secretions or increased suctioningrequirements
Apnea, tachypnea, nasal flaring with retraction of chest wall or nasal flaring with gruntingWheezing, rales, or rhonchiCoughBradycardia (<100 beats per minute) or tachycardia (>170 beats per minute)
CDC¼Centers for Disease Control and Prevention; VAP¼ventilator-assisted pneumonia; WBC¼white blood cell count.aIn the absence of underlying conditions, one definitive chest radiograph is acceptable. Among infants who have underlying conditions, two or more serialdefinitive radiographs are required. For neonates, underlying pulmonary or cardiac disease may include respiratory distress syndrome, bronchopulmonarydysplasia, pulmonary edema, chronic obstructive pulmonary disease, and/or congenital heart disease.
Table 2. CDC Microbiologic Criteria for Diagnosis of Common Bacterial orFungal VAP
In addition to radiographic and clinical criteria, at least one of the following is present:Positive growth in blood culture not related to another source of infectionPositive growth in culture of pleural fluidPositive quantitative culture from minimally contaminated lower respiratory tract specimen (eg, BAL, protected specimenbrushing)
‡5% BAL-obtained cells contain intracellular bacteria on direct microscopic examination (eg, Gram-stain)Histopathologic examination shows at least one of the following indications of pneumonia:- Abscess formation or foci of consolidation with intense PMN accumulation in bronchioles and alveoli- Positive quantitative culture of lung parenchyma- Evidence of lung parenchyma invasion by fungal hyphae or pseudohyphae
BAL¼bronchoalveolar lavage; CDC¼Centers for Disease Control and Prevention; PMN¼polymorphonuclear leukocyte; VAP¼ventilator-assistedpneumonia.
infectious diseases ventilator-associated pnuemonia
e228 NeoReviews Vol.15 No.6 June 2014
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

from the trachea. Cernada et al (32) used a blind pro-tected catheter to assist in diagnosing pneumonia in an-other cohort of neonates who had suspected VAP. Theydid not report sensitivity or specificity of the procedure. Alimitation of both of these studies is that they were com-pared with clinically diagnosed VAP and not with a goldstandard such as a lung biopsy or tissue sample. Largertrials need to be conducted to assess the diagnostic valueand safety profile of the procedures.
In many NICUs, tracheal aspirate cultures and Gram-stains are commonly used to try to establish the diagnosisof VAP in neonates. Tracheal aspirates have low sensitiv-ity, specificity, and positive predictive value for diagnos-ing VAP because it is difficult to distinguish betweentracheal colonization and true pneumonia. (36) However,tracheal colonization of the airway with Gram-negativebacteria has been associated with adverse outcomes.(37) Tracheal aspirates from neonates who have sus-pected VAP may play a role in helping to identify or-ganisms colonizing the airway and aid in the choiceof appropriate antibiotic therapy. This finding maybe of value, given evidence that there is a greater risk ofdeath in adults from VAP if their pneumonia was initiallytreated with the wrong antibiotic. (38)(39) Furthermore,a sterile tracheal aspirate culture may also be of value inthat sterile cultures have a high negative predictive valuefor VAP. (40)
Routine use of clinical biomarkers such as C-reactiveprotein, soluble triggering receptor expressed on mye-loid type 1 cells, or procalcitonin to help identify VAPhas not been supported in ventilated adults. (41) Stud-ies have not been conducted to determine the utilityof biomarkers for the diagnosis of VAP in neonatalpatients.
TreatmentThere are no clear consensus guidelines for the optimaltreatment of neonatal VAP. Most treatment recommen-dations are taken from adult guidelines and are supportedby epidemiologic principles. Initial treatment should in-clude broad empiric therapy, preferably informed by localbacterial colonizing and antimicrobial sensitivity data.Local NICU antibiotic combinations for the empirictreatment of late-onset bloodstream infections shouldbe used for suspected VAP, unless individual infantcolonizing information is available. Empiric treatmentwill often include an antipseudomonal agent such aspiperacillin/tazobactam or ticarcillin/clavulanate to pro-vide coverage of both Gram-negative and Gram-positiveorganisms. Carbapenems may be more appropriate for
initial empiric therapy if local flora include extensive beta-lactamase–producing organisms. Additional Gram-negativecoverage with an aminoglycoside is controversial but maybe indicated when bacteremia is suspected or significantsystemic symptoms are present. If systemic symptomsare absent and the blood culture result is negative, de-escalating therapy by discontinuing the aminoglycosidesmay be appropriate. Gram-positive coverage for methicillin-resistant S aureus may be required if local epidemiologicdata dictate its use.
Overall, multiple risk factors (eg, prolonged me-chanical ventilation, previous antibiotic exposure, mul-tisystem illness) place neonates at increased risk formultidrug-resistant VAP, and there is no validatedmeans of assessing VAP severity or VAP improvementafter treatment, as there is in adults. Because of thesefactors, most neonates who have VAP will receive a fullcourse of empiric broad-spectrum antibiotic therapyunless specific culture results allow for the use of morenarrow-spectrum therapy. (14)(15)
Prevention of VAPThe CDC (42) and the American Thoracic Society (43)have published guidelines for the prevention of health-care–associated pneumonia. “Bundles” bring togethera number of evidence-based practices that, when appliedas a single intervention (ie, the bundle), may result in im-provement that is greater than single evidence-basedpractices. (44)(45)(46) These recommendations addressthe following specific items.
Management of secretions and techniques forsuctioning
Adult VAP prevention bundles often include 30° to 45°of head elevation to prevent aspiration of contaminatedoropharyngeal and gastric fluids. The results of Alyet al (23) and Farhath et al (27) suggest that gravitymay be used to prevent pathogens from gaining entry in-to the lower respiratory track of ventilated neonates.Farhath et al showed that a majority of ventilated neo-nates aspirated gastric pepsin, perhaps providing supportfor elevating the head of the neonatal bed, but this studydid not evaluate the association between the presenceof pepsin in the trachea and VAP. Aly et al evaluatedtracheal colonization in supine and lateral-nursed venti-lated infants and found that the lateral-nursed infantshad less tracheal bacterial colonization; however, thestudy did not specifically assess VAP. The optimum po-sition to nurse neonates for the prevention of VAP needsfurther investigation.
infectious diseases ventilator-associated pnuemonia
NeoReviews Vol.15 No.6 June 2014 e229
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

The CDC recommends that secretions be clearedfrom above the cuff of the endotracheal tube anytimethe tube is repositioned or removed. (42) Neonates areusually cared for with uncuffed endotracheal tubes. Suc-tioning the oropharynx around the endotracheal tube be-fore adjusting it or removing it may reduce risk ofmicroaspiration of contaminated oropharyngeal secre-tions. Although close systems are frequently used forthe care of ventilated neonates, they may present the po-tential for bacterial contamination if pooled secretions inthe lumen are reintroduced into the respiratory tract withrepeated suctioning. Conversely, closed suctioning couldpotentially reduce environmental contamination of therespiratory tract. In a study of 133 ventilated neonatesrandomized to a closed or open suction system, no differ-ence was noted in tracheal colonization patterns betweengroups, nor were there differences in VAP rates amongtreatment groups. Physiologic disruptions were less withthe closed suction systems, and NICU nurses indicatedthat these systems were easier to use than open suctionsystems. (47) At minimum, separate suctioning equip-ment should be used for tracheal and oral secretions.
One recent study evaluated a low-sodium, physiolog-ically based solution for suctioning of ventilated neo-nates. (48) A significant reduction in the VAP rate wasdemonstrated after normal saline for airway suctioningwas replaced by the novel solution for airway suctioning.Further trials with the solutions are necessary to confirmthese results. Finally, respiratory tubing should bedrained away from ventilated infants to prevent aspirationof potentially contaminated condensate. (49) Breathingcircuits do not need routine changing unless they becomevisibly soiled or they malfunction. (42)
Extubation proceduresVAP reduction bundles often recommend “sedation va-cations” to assess extubation readiness. Because manycenters use minimal or no sedation for ventilated neo-nates, sedation vacations are uncommon in most units.Assessing for extubation readiness should be done ona daily basis. Noninvasive measures such as nasal contin-uous positive airway pressure and nasal prong ventilationmay help to reduce VAP rates. (9) Reintubation after ex-tubation should be avoided if possible because of the in-creased risk of VAP associated with reintubation. (50)
Gastrointestinal and oropharyngealinterventions.
Manipulation of gastrointestinal contents is part of adultVAP prevention. Although H2-blocker treatment is fre-quently a standard intervention in bundles to prevent
VAP in adults, current data do not support such treat-ment in ventilated neonates. In addition, the use ofH2-blockers is associated with increased risk of late-onsetfungal infection and necrotizing enterocolitis among verylow birthweight NICU infants. (51)(52)
Selective digestive tract decontamination (SDD) withenteral nonabsorbable antimicrobials and antimicrobialsapplied directly to the oropharynx can decrease gastroin-testinal colonization and potentially reduce respiratorytract infections from microaspiration of gastrointestinalorganisms. CDC guidelines (42) offer no recommenda-tion for the selective decontamination of the digestivetract. In a nonrandomized prospective trial of ventilatedneonates, those who underwent SDD with polymyxin E,tobramycin, and nystatin had fewer nosocomial infectionsof intestinal origin. (53) VAP episodes were not reportedseparately. SDD should be evaluated further before it isconsidered for neonates outside of clinical trials. Theuse of probiotic treatment to influence neonatal gastroin-testinal colonization has focused on reducing late-onsetbloodstream infections and necrotizing enterocolitis,but one recent trial of Lactobacillus reuteri administrationalso demonstrated the effect of probiotic administrationon the incidence of VAP. (54)
The CDC recommends a comprehensive oral hygieneprogram in patients at high risk for health-care–associatedpneumonia. (42) Although several groups have noteda reduction in VAP among adult patients treated withoral chlorhexidine gluconate decontamination, theCDC makes no recommendation for the use of an oralchlorhexidine gluconate rinse for the prevention ofVAP in ill patients. Chlorhexidine gluconate is not ap-proved for neonates less than age 2 months. Because neo-nates do not have gingivitis or the dental diseases adultsoften have, oral care may not provide the benefit it doesin adult patients. Until further data are available, adheringto the recommendation of the American Dental Associ-ation to wipe off the gums and keep the mouth clean afterfeedings and when needed seems prudent.
Infection control measuresHand hygiene is likely the most important infection con-trol intervention in health-care settings to reduce person–person transmission of bacteria. Pathogens responsiblefor neonatal VAP are carried on health-care workers’hands and in the infants’ gastrointestinal tracts. Respira-tory equipment can become colonized with these organ-isms. (55) Thorough hand-washing before and aftercontact with respiratory equipment should reducecross-contamination between patients.
infectious diseases ventilator-associated pnuemonia
e230 NeoReviews Vol.15 No.6 June 2014
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

Changes in endotracheal tube design have decreasedincidence of VAP in adults. A hole in the dorsal aspectof endotracheal tubes above the inflated cuff allows forclearing of subglottic secretions. The CDC recommendsthe use of such tubes in ventilated adults. (42) Unfortu-nately, such tubes are not available for neonates. Silver-coated endotracheal tubes, which are not available forneonates, have also been shown to reduce VAP in adultsby reducing biofilm formation and bacterial colonization.
Figure 3 summarizes how practical preventative inter-ventions relate to the steps in the pathogenesis of VAP.Improved diagnostic criteria and surveillance tech-niques for VAP in the neonatal population need to be es-
tablished before the effectiveness of these strategies canbe accurately assessed.
Figure 3. Relationship between preventative measures and pathogenesis of ventilator-associated pneumonia (VAP). (Adapted fromGarland JS. Strategies to prevent ventilator-associated pneumonia in neonates. Clin Perinatol. 2010;37(3):638. Copyright 2010,with permission from Elsevier.)
American Board of Pediatrics Neonatal–PerinatalContent Specifications
• Know the pathogenesis and causativeagents in an infant in whom neonatalpneumonia is suspected.
• Plan the clinical, imaging, and laboratoryfeatures and the management of aninfant in whom neonatal pneumonia issuspected.
infectious diseases ventilator-associated pnuemonia
NeoReviews Vol.15 No.6 June 2014 e231
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

References1. Centers for Disease Control and Prevention. Criteria for definingnosocomial pneumonia. Available at: http://www.cdc.gov/nhsn/PDFs/pscManual/6pscVAPcurrent.pdf. Accessed January 31, 20142. van der Zwet WC, Kaiser AM, van Elburg RM, et al. Nosoco-mial infections in a Dutch neonatal intensive care unit: surveillancestudy with definitions for infection specifically adapted for neonates.J Hosp Infect. 2005;61(4):300–3113. Gaynes RP, Edwards JR, Jarvis WR, Culver DH, Tolson JS,Martone WJ; National Nosocomial Infections Surveillance System.Nosocomial infections among neonates in high-risk nurseries in theUnited States. Pediatrics. 1996;98(3 pt 1):357–3614. Drews MB, Ludwig AC, Leititis JU, Daschner FD. Low birthweight and nosocomial infection of neonates in a neonatal intensivecare unit. J Hosp Infect. 1995;30(1):65–725. Ford-Jones EL, Mindorff CM, Langley JM, et al. Epidemiologicstudy of 4684 hospital-acquired infections in pediatric patients.Pediatr Infect Dis J. 1989;8(10):668–6756. Hemming VG, Overall JC Jr, Britt MR. Nosocomial infectionsin a newborn intensive-care unit. Results of forty-one months ofsurveillance. N Engl J Med. 1976;294(24):1310–13167. Hocevar SN, Edwards JR, Horan TC, Morrell GC, Iwamoto M,Lessa FC. Device-associated infections among neonatal intensivecare unit patients: incidence and associated pathogens reported tothe National Healthcare Safety Network, 2006-2008. InfectControl Hosp Epidemiol. 2012;33(12):1200–12068. Yuan TM, Chen LH, Yu HM. Risk factors and outcomes forventilator-associated pneumonia in neonatal intensive care unitpatients. J Perinat Med. 2007;35(4):334–3389. Hentschel J, Brüngger B, Stüdi K, Mühlemann K. Prospectivesurveillance of nosocomial infections in a Swiss NICU: low risk ofpneumonia on nasal continuous positive airway pressure? Infection.2005;33(5-6):350–35510. Cordero L, Ayers LW, Miller RR, Seguin JH, Coley BD.Surveillance of ventilator-associated pneumonia in very-low-birth-weight infants. Am J Infect Control. 2002;30(1):32–3911. Pessoa-Silva CL, Richtmann R, Calil R, et al. Healthcare-associated infections among neonates in Brazil. Infect Control HospEpidemiol. 2004;25(9):772–77712. Su BH, Hsieh HY, Chiu HY, Lin HC, Lin HC. Nosocomialinfection in a neonatal intensive care unit: a prospective study inTaiwan. Am J Infect Control. 2007;35(3):190–19513. Apisarnthanarak A, Holzmann-Pazgal G, Hamvas A, OlsenMA, Fraser VJ. Ventilator-associated pneumonia in extremelypreterm neonates in a neonatal intensive care unit: characteristics,risk factors, and outcomes. Pediatrics. 2003;112(6 pt 1):1283–128914. Garland JS. Strategies to prevent ventilator-associated pneu-monia in neonates. Clin Perinatol. 2010;37(3):629–64315. Cernada M, Brugada M, Golombek S, Vento M. Ventilator-associated pneumonia in neonatal patients: an update. Neonatology.2014;105(2):98–10716. Kollef MH. The prevention of ventilator-associated pneumo-nia. N Engl J Med. 1999;340(8):627–63417. de Latorre FJ, Pont T, Ferrer A, Rosselló J, Palomar M, PlanasM. Pattern of tracheal colonization during mechanical ventilation.Am J Respir Crit Care Med. 1995;152(3):1028–103318. George DL, Falk PS, Wunderink RG, et al. Epidemiology ofventilator-acquired pneumonia based on protected bronchoscopicsampling. Am J Respir Crit Care Med. 1998;158(6):1839–1847
19. Mahul P, Auboyer C, Jospe R, et al. Prevention of nosocomialpneumonia in intubated patients: respective role of mechanicalsubglottic secretions drainage and stress ulcer prophylaxis. IntensiveCare Med. 1992;18(1):20–2520. Vallés J, Artigas A, Rello J, et al. Continuous aspiration ofsubglottic secretions in preventing ventilator-associated pneumonia.Ann Intern Med. 1995;122(3):179–18621. Cardeñosa Cendrero JA, Solé-Violán J, Bordes Benítez A, et al.Role of different routes of tracheal colonization in the developmentof pneumonia in patients receiving mechanical ventilation. Chest.1999;116(2):462–47022. Feldman C, Kassel M, Cantrell J, et al. The presence andsequence of endotracheal tube colonization in patients undergoingmechanical ventilation. Eur Respir J. 1999;13(3):546–55123. Aly H, Badawy M, El-Kholy A, et al. Randomized, controlledtrial on tracheal colonization of ventilated infants: can gravity preventventilator-associated pneumonia? Pediatrics. 2008;122(4):77–77424. Bonten MJ, Gaillard CA, van Tiel FH, Smeets HG, van derGeest S, Stobberingh EE. The stomach is not a source forcolonization of the upper respiratory tract and pneumonia in ICUpatients. Chest. 1994;105(3):878–88425. Craven DE, Steger KA, Barber TW. Preventing nosocomialpneumonia: state of the art and perspectives for the 1990s. Am JMed. 1991;91(3B):44S–53S26. Torres A, Serra-Batlles J, Ros E, et al. Pulmonary aspiration ofgastric contents in patients receiving mechanical ventilation: theeffect of body position. Ann Intern Med. 1992;116(7):540–54327. Farhath S, He Z, Nakhla T, et al. Pepsin, a marker of gastriccontents, is increased in tracheal aspirates from preterm infants whodevelop bronchopulmonary dysplasia. Pediatrics. 2008;121(2):e253–e25928. Adair CG, Gorman SP, Feron BM, et al. Implications ofendotracheal tube biofilm for ventilator-associated pneumonia.Intensive Care Med. 1999;25(10):1072–107629. Alcón A, Fàbregas N, Torres A. Hospital-acquired pneumonia:etiologic considerations. Infect Dis Clin North Am. 2003;17(4):679–69530. van Ogtrop ML, van Zoeren-Grobben D, Verbakel-SalomonsEM, van Boven CP. Serratia marcescens infections in neonataldepartments: description of an outbreak and review of theliterature. J Hosp Infect. 1997;36(2):95–10331. Szabó D, Filetóth Z, Szentandrássy J, et al. Molecularepidemiology of a cluster of cases due to Klebsiella pneumoniaeproducing SHV-5 extended-spectrum b-lactamase in the prematureintensive care unit of a Hungarian hospital. J Clin Microbiol. 1999;37(12):4167–416932. Cernada M, Aguar M, Brugada M, et al. Ventilator-associatedpneumonia in newborn infants diagnosed with an invasive bron-choalveolar lavage technique: a prospective observational study.Pediatr Crit Care Med. 2013;14(1):55–6133. Baltimore RS. The difficulty of diagnosing ventilator-associatedpneumonia. Pediatrics. 2003;112(6 pt 1):1420–142134. Centers for Disease Control and Prevention. Surveillance forventilator-associated events. Available at: http://www.cdc.gov/nhsn/acute-care-hospital/vae/. Accessed March 3, 201435. Köksal N, Hacimustafaoğlul M, Çelebi S, Ozakin C. Non-bronchoscopic bronchoalveolar lavage for diagnosing ventilator-associated pneumonia in newborns. Turk J Pediatr. 2006;48(3):213–22036. Evans ME, Schaffner W, Federspiel CF, Cotton RB, McKeeKT Jr, Stratton CW. Sensitivity, specificity, and predictive value of
infectious diseases ventilator-associated pnuemonia
e232 NeoReviews Vol.15 No.6 June 2014
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

body surface cultures in a neonatal intensive care unit. JAMA.1988;259(2):248–25237. Cordero L, Ayers LW, Davis K. Neonatal airway colonizationwith gram-negative bacilli: association with severity of bronchopulmo-nary dysplasia. Pediatric Infectious Disease Journal. 1997;16(1):18–2338. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. Theinfluence of inadequate antimicrobial treatment of bloodstreaminfections on patient outcomes in the ICU setting. Chest. 2000;118(1):146–15539. Chastre J, Luyt CE, Trouillet JL, Combes A. New diagnosticand prognostic markers of ventilator-associated pneumonia. CurrOpin Crit Care. 2006;12(5):446–45140. Kirtland SH, Corley DE, Winterbauer RH, et al. The diagnosisof ventilator-associated pneumonia: a comparison of histologic,microbiologic, and clinical criteria. Chest. 1997;112(2):445–45741. Palazzo SJ, Simpson T, Schnapp L. Biomarkers for ventilator-associated pneumonia: review of the literature. Heart Lung. 2011;40(4):293–29842. Centers for Disease Control and Prevention (CDC). Guide-lines for prevention of healthcare-associated pneumonia. MMWR.March 26,2004;53(RR03);1–3643. American Thoracic Society; Infectious Diseases Society ofAmerica. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia.Am J Respir Crit Care Med. 2005;171(4):388–41644. Kollef MH. Prevention of hospital-associated pneumonia andventilator-associated pneumonia. Crit Care Med. 2004;32(6):1396–140545. Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T,Nolan T. Using a bundle approach to improve ventilator careprocesses and reduce ventilator-associated pneumonia. Jt Comm JQual Patient Saf. 2005;31(5):243–248
46. Lorente L, Blot S, Rello J. Evidence on measures for theprevention of ventilator-associated pneumonia. Eur Respir J. 2007;30(6):1193–120747. Cordero L, Sananes M, Ayers LW. Comparison of a closed(Trach Care MAC) with an open endotracheal suction system insmall premature infants. J Perinatol. 2000;20(3):151–15648. Christensen RD, Henry E, Baer VL, et al. A low-sodiumsolution for airway care: results of a multicenter trial. Respir Care.2010;55(12):1680–168549. Craven DE, Goularte TA, Make BJ. Contaminated condensatein mechanical ventilator circuits: a risk factor for nosocomialpneumonia? Am Rev Respir Dis. 1984;129(4):625–62850. Torres A, Gatell JM, Aznar E, et al. Re-intubation increasesthe risk of nosocomial pneumonia in patients needing mechanicalventilation. Am J Respir Crit Care Med. 1995;152(1):137–14151. Saiman L, Ludington E, Dawson JD, et al; National Epidemi-ology of Mycoses Study Group. Risk factors for Candida speciescolonization of neonatal intensive care unit patients. Pediatr InfectDis J. 2001;20(12):1119–112452. Terrin G, Passariello A, De Curtis M, et al. Ranitidine isassociated with infections, necrotizing enterocolitis, and fatal out-come in newborns. Pediatrics. 2012;129(1):e40–e4553. Herruzo-Cabrera R, García Gonzalez JI, García-Magan P, del Rey-Calero J. Nosocomial infection in a neonatal intensive care unit and itsprevention with selective intestinal decolonization. A multivariantevaluation of infection reduction. Eur J Epidemiol. 1994;10(5):573–58054. Rojas MA, Lozano JM, Rojas MX, et al. Prophylactic pro-biotics to prevent death and nosocomial infection in preterminfants. Pediatrics. 2012;130(5):e1113–e112055. Sole ML, Poalillo FE, Byers JF, Ludy JE. Bacterial growth insecretions and on suctioning equipment of orally intubated patients:a pilot study. Am J Crit Care. 2002;11(2):141–149
infectious diseases ventilator-associated pnuemonia
NeoReviews Vol.15 No.6 June 2014 e233
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

NeoReviews Quiz RequirementsTo successfully complete 2014 NeoReviews articles for AMA PRA Category 1 CreditTM, learners must demonstrate a minimum performance level of60% or higher on this assessment, which measures achievement of the educational purpose and/or objectives of this activity. If you score less than60% on the assessment, you will be given additional opportunities to answer questions until an overall 60% or greater score is achieved.
NOTE: Learners can take NeoReviews quizzes and claim credit online only at: http://neoreviews.org.
1. A 10-day-old, 28-week-gestational-age male infant who has been on the ventilator has worsening clinicalstatus and is suspected of having pneumonia. Which of the following statements regarding the development ofventilator-associated pneumonia (VAP) is correct?
A. Radiographic characteristics of VAP are very distinct and consistent, with a diffuse pattern of consolidationat onset.
B. A patient needs to be intubated for at least 5 days before onset of infection to have an official diagnosis ofVAP.
C. Opiate treatment for sedation has been associated with increased risk of VAP.D. A key feature in effective prevention of VAP is frequent suctioning and periodic replacement of the
endotracheal tube.E. A concurrent bloodstream infection rules out the diagnosis of VAP.
2. In the 10-day-old, 28-week-gestational-age patient, which of the following statements regarding diagnosisof VAP is correct?
A. It would be considered the standard of care to perform bronchoscopic bronchoalveolar lavage for thepurpose of diagnosis in this patient.
B. The definition of VAP for neonates has been well established since the 1998 criteria published in a jointeffort between the Centers for Disease Control and Prevention and the American Academy of Pediatrics.
C. A sterile tracheal aspirate culture has a high negative predictive value for VAP.D. Tracheal aspirates have excellent sensitivity (>98%) but poor specificity for diagnosis of VAP.E. C-reactive protein has been very useful in the diagnosis of VAP, for distinguishing VAP from other disease
processes, and for use in trials for establishing diagnostic criteria.
3. A tracheal aspirate is obtained from the patient who is suspected of having VAP. Which of the following hasbeen found regarding tracheal aspirates in neonates who have VAP?
A. Gram-positive organisms are the most common bacteria noted in tracheal aspirates.B. In general, the most common finding from tracheal aspirates of neonates suspected of having VAP are
sterile or have a single-organism growth.C. Streptococcus gallolyticus is found in 50% of neonates who have VAP.D. Bronchoalveolar lavage with a blind protected catheter generally results in higher recovery of
polymicrobial infections.E. Pseudomonas aeruginosa is a pathogen recovered from airway secretions in VAP by using both tracheal
aspirate and bronchoalveolar lavage methods.
4. The clinical care team has determined that the patient has VAP. What are appropriate principles regardingtreatment for VAP in neonates at this gestational age?
A. Clear consensus guidelines for the treatment of very low birthweight infants were published by the Centersfor Disease Control and Prevention (CDC), first in 1999 and updated in 2010.
B. In the majority of cases, if the patient’s condition is stable, the treatment of VAP is extubation tocontinuous positive airway pressure or nasal cannula, and does not require antibiotics.
C. Antibiotics should only be started after a pathogenic organism associated with VAP has been identified.D. Empiric treatment may include an antipseudomonal agent such as piperacillin/tazobactam.E. Because organisms causing VAP are generally derived from mouth flora, penicillin is a reasonable first-line
treatment or can be used if treatment is desired when no organism is recovered.
infectious diseases ventilator-associated pnuemonia
e234 NeoReviews Vol.15 No.6 June 2014
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

5. Your neonatal intensive care unit (NICU) is developing a bundle for prevention of VAP. Which of the followingcomponents may be a reasonable part of the protocol based on the studies discussed in this article?
A. Neonate should be positioned in the prone position at least one-half of the time if he or she has beenintubated for more than 2 days.
B. Separate suctioning equipment should be used for tracheal and oral secretions.C. Respiratory circuits should be changed on a routine basis, daily or twice a day.D. Normal saline has been shown to be the optimal solution for airway suctioning compared with all other
solutions.E. To minimize gastric aspiration, moderate sedation for vigorously moving infants should be applied,
preferably with opioids.
infectious diseases ventilator-associated pnuemonia
NeoReviews Vol.15 No.6 June 2014 e235
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.15-6-e2252014;15;e225Neoreviews
Jeffery S. GarlandVentilator-Associated Pneumonia in Neonates: An Update
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/15/6/e225including high resolution figures, can be found at:
Referenceshttp://neoreviews.aappublications.org/content/15/6/e225#BIBLThis article cites 53 articles, 11 of which you can access for free at:
Permissions & Licensing
http://neoreviews.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://neoreviews.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
at Indonesia:AAP Sponsored on November 19, 2014http://neoreviews.aappublications.org/Downloaded from