value reliability risky unsafe a proposition where
TRANSCRIPT

7/16/2012
1
What Does All This Mean?Organizing Around 3 Skills for Reliability
Craig Clapper, PE, CMQ/OEChief Knowledge Officer, Health Performance Improvement
© 2012 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.This material is a proprietary document of Healthcare Performance Improvement LLC. Reproducing, copying, publishing, distributing, presenting, or creating derivative work products based on this material without written permission from Healthcare Performance Improvement is prohibited.
Quality An objective appraisal (from a producer perspective) of safety(protection from harm) and effectiveness
Satisfaction A subjective appraisal (from a user perspective) of quality > expectations
Value A subjective appraisal of satisfaction relative to cost and time (to realization).
Reliability A probability that a system will yield a specified result; expressed as a ratio (0.01 or 1:100 or 1%) or a frequency ( 1 per yr)
Risky A proposition where effectiveness > potential harm
Unsafe A proposition where potential harm > effectiveness
Healthcare Reliability Dictionary
“Based on our review of the scant evidence, we believe that preventable medical harm still accounts for more than 100,000 deaths a year… the Centers for Disease Control and Prevention (CDC) estimates that hospital-acquired conditions alone kill 99,000 each year…
In this report, we give the country a failing grade on progress…” Consumers Union (2009)
Death By Numbers44,000 to 98,000 patient deaths per year from medical errorsTo Err is Human, Institute of Medicine (1999)
A Lot of TalkPatient safety publications before andafter the IOM report, To Err is Human
Quality & Safety in Health Care (2006)
Hospitals Are Dangerous Arm yourselves accordingly
What Will It Take?Patient Safety Rounds
+Address TJC Patient Safety Alerts
+Non-Punitive Approach to Reporting
+Crew Resource Management
+Strategies in Targeted Venues(e.g. bundles to reduce VAP or SSI)
But will this produce significant, sustainedreduction in Serious Safety Events and
improved Quality across the organization?
The Swiss-Cheese Effect
Adapted from James Reason, Managing the Risks of Organizational Accidents (1997)
Active Errorsby individuals result in initiating action(s)
EVENTS ofHARM
Multiple Barriers - technology, processes, and people - designed to stop
active errors (our “defense in depth”)
Latent Weaknesses in barriers
PREVENTThe Errors
DETECT & CORRECTThe System Weaknesses
7/16/2012
2
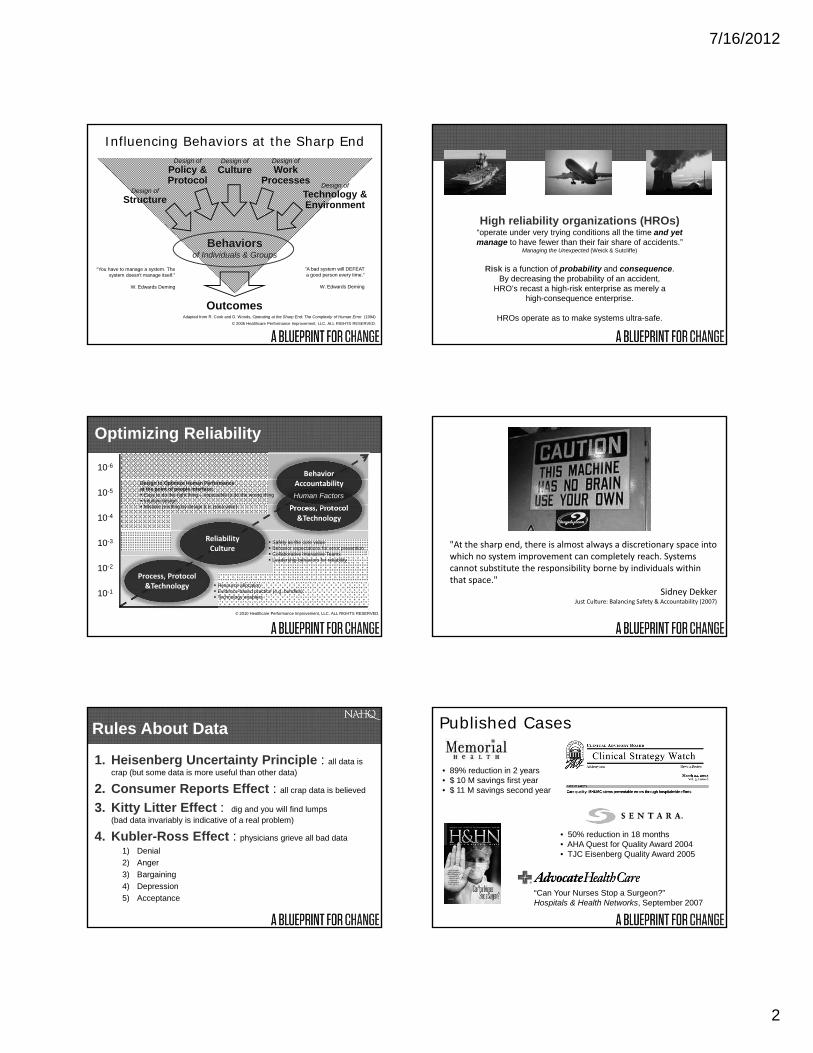
Influencing Behaviors at the Sharp End
Adapted from R. Cook and D. Woods, Operating at the Sharp End: The Complexity of Human Error (1994)
Design of
Culture
Outcomes
Behaviorsof Individuals & Groups
Design of
Structure
Design of
Technology & Environment
Design of
WorkProcesses
Design of
Policy &Protocol
© 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
“You have to manage a system. The system doesn't manage itself.”
W. Edwards Deming
"A bad system will DEFEAT a good person every time.“
W. Edwards Deming
High reliability organizations (HROs)“operate under very trying conditions all the time and yet manage to have fewer than their fair share of accidents.”
Managing the Unexpected (Weick & Sutcliffe)
Risk is a function of probability and consequence.By decreasing the probability of an accident,
HRO’s recast a high-risk enterprise as merely ahigh-consequence enterprise.
HROs operate as to make systems ultra-safe.
10-6
10-5
10-4
10-3
10-2
10-1
Optimizing Reliability
ReliabilityCulture
Safety as the core value Behavior expectations for error prevention Collaborative Interactive Teams Leadership behaviors for reliability
Process, Protocol&Technology Resource allocation
Evidence-based practice (e.g. bundles) Technology enablers
Process, Protocol&Technology
BehaviorAccountability
Human Factors
Design to Optimize Human Performanceat the point of people interface: Easy to do the right thing – impossible to do the wrong thing Intuitive design Mistake proofing by design (i.e. poka yoke)
© 2010 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
"At the sharp end, there is almost always a discretionary space into which no system improvement can completely reach. Systems cannot substitute the responsibility borne by individuals within that space."
Sidney DekkerJust Culture: Balancing Safety & Accountability (2007)
Rules About Data
1. Heisenberg Uncertainty Principle : all data is crap (but some data is more useful than other data)
2. Consumer Reports Effect : all crap data is believed
3. Kitty Litter Effect : dig and you will find lumps (bad data invariably is indicative of a real problem)
4. Kubler-Ross Effect : physicians grieve all bad data
1) Denial
2) Anger
3) Bargaining
4) Depression
5) Acceptance
Published Cases
• 89% reduction in 2 years• $ 10 M savings first year• $ 11 M savings second year
• 50% reduction in 18 months• AHA Quest for Quality Award 2004• TJC Eisenberg Quality Award 2005
“Can Your Nurses Stop a Surgeon?”Hospitals & Health Networks, September 2007

7/16/2012
3
Serious SafetyEventRateSSER
78% Reduction SSER across the System in 29 Months2 Hospitals at Zero Events for over 12 months!
116 days since last event across the system
0.00
0.20
0.40
0.60
0.80
1.00
Jan-
08
Fe
b-0
8
Ma
r-0
8
Ap
r-0
8
Ma
y-08
Jun-
08
Jul-0
8
Au
g-08
Se
p-08
Oct
-08
No
v-08
De
c-08
Jan-
09
Fe
b-0
9
Ma
r-0
9
Ap
r-0
9
Ma
y-09
Jun-
09
Jul-0
9
Au
g-09
Se
p-09
Oct
-09
No
v-09
De
c-09
Jan-
10
Fe
b-1
0
Ma
r-1
0
Ap
r-1
0
Ma
y-10
Jun-
10
Jul-1
0
Au
g-10
Se
p-10
Oct
-10
No
v-10
De
c-10
Jan-
11
Fe
b-1
1
Ma
r-1
1
Ap
r-1
1
Ma
y-11
Jun-
11
Jul-1
1
Au
g-11
Se
p-11
Oct
-11
Eve
nt
Rat
e
5 Hospital System – Southern USJanuary 2008- October 2011
Rolling 12 month Serious Safety Events expressed per 10,000 adjusted patient days
)78% Reduction SSER across the System in 29 Months
2 Hospitals at Zero Events for over 12 months!
116 days since last event across the system
78% Reduction SSER across the System in 29 Months2 Hospitals at Zero Events for over 12 months!
116 days since last event across the system
Personal Safety Improvements(5 hospital system – South Eastern US)
$0
$100,000
$200,000
$300,000
$400,000
$500,000
$600,000
CY 07 CY 08 CY 09 CY 10
Workman's Compensation Costs
Over $1, 200,000 savedyear to date!
0
2
4
6
8
10
12
14
16
18
20
Sep
-06O
ct-06
Nov-06
Dec-06
Jan-07F
eb-07M
ar-07
Apr-0
7M
ay-07
Jun-07Jul-0
7A
ug-07
Sep
-07O
ct-07
Nov-07
Dec-07
Jan-08F
eb-08M
ar-08
Apr-0
8M
ay-08
Jun-08Jul-0
8A
ug-08
Sep
-08O
ct-08
Nov-08
Dec-08
Jan-09F
eb-09M
ar-09
Apr-0
9M
ay-09
Jun-09Jul-0
9A
ug-09
Sep
-09O
ct-09
Nov-09
Dec-09
Jan-10F
eb-10M
ar-10
Apr-1
0M
ay-10
Jun-10Jul-1
0A
ug-10
Sep
-10O
ct-10
Nov-10
Dec-10
Jan-11F
eb-11M
ar-11
Apr-1
1
Month
Monthly Lost Time ClaimsJuly 06 - April 2011
Over 300 Serious Injuries prevented90% reduction in OSHA IIR
Complementary Strategies
© 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
…and on, and on, and on…
Central LineInfections
HandHygiene
Surgical SiteInfections
Codes Outsidethe ICU
Culture
Process Bundle People Bundle
4 for VAP Prevention1. Elevation of the head of the bed to
between 30 and 45 degrees2. Daily “sedation vacation” and daily
assessment of readiness to extubate3. Peptic ulcer disease (PUD) prophylaxis4. Deep venous thrombosis (DVT)
prophylaxis (unless contraindicated)
Read More: Community Health Network Reduces Deadly Infections Through Culture of Reliability, American Society for Quality
(June 2008)
Improving Quality Using High ReliabilityEast Coast System ‐ 8 Hospitals
National Data Source: ASHRM Hospital Professional Liability & Physician Liability 2009 Benchmark Analysis
Finance’s Interest in SafetyMulti-Hospital East Coast System
7/16/2012
4
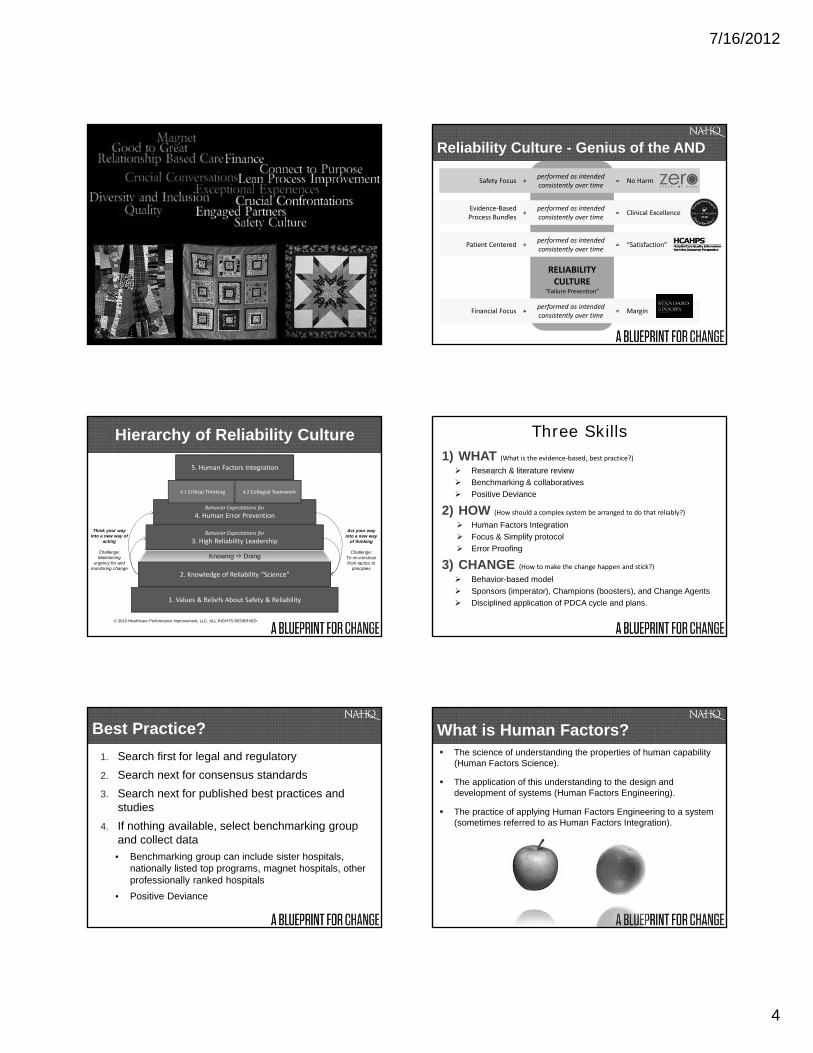
RELIABILITYCULTURE
“Failure Prevention”
Evidence‐BasedProcess Bundles
+performed as intendedconsistently over time
= Clinical Excellence
Patient Centered +performed as intendedconsistently over time
= “Satisfaction”
Reliability Culture - Genius of the AND
Safety Focus +performed as intendedconsistently over time
= No Harm
Financial Focus +performed as intendedconsistently over time
= Margin
1. Values & Beliefs About Safety & Reliability
2. Knowledge of Reliability “Science”
Behavior Expectations for
3. High Reliability Leadership
Behavior Expectations for
4. Human Error Prevention
4.2 Collegial Teamwork4.1 Critical Thinking
5. Human Factors Integration
Hierarchy of Reliability Culture
Think your way into a new way of
acting
Challenge:Maintaining
urgency for and monitoring change
Act your way into a new way
of thinking
Challenge:To re-construct from tactics to
principles
Knowing Doing
© 2010 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Three Skills1) WHAT (What is the evidence‐based, best practice?)
Research & literature review
Benchmarking & collaboratives
Positive Deviance
2) HOW (How should a complex system be arranged to do that reliably?)
Human Factors Integration
Focus & Simplify protocol
Error Proofing
3) CHANGE (How to make the change happen and stick?)
Behavior-based model
Sponsors (imperator), Champions (boosters), and Change Agents
Disciplined application of PDCA cycle and plans.
Best Practice?
1. Search first for legal and regulatory
2. Search next for consensus standards
3. Search next for published best practices and studies
4. If nothing available, select benchmarking group and collect data
• Benchmarking group can include sister hospitals, nationally listed top programs, magnet hospitals, other professionally ranked hospitals
• Positive Deviance
What is Human Factors? The science of understanding the properties of human capability
(Human Factors Science).
The application of this understanding to the design and development of systems (Human Factors Engineering).
The practice of applying Human Factors Engineering to a system (sometimes referred to as Human Factors Integration).
7/16/2012
5
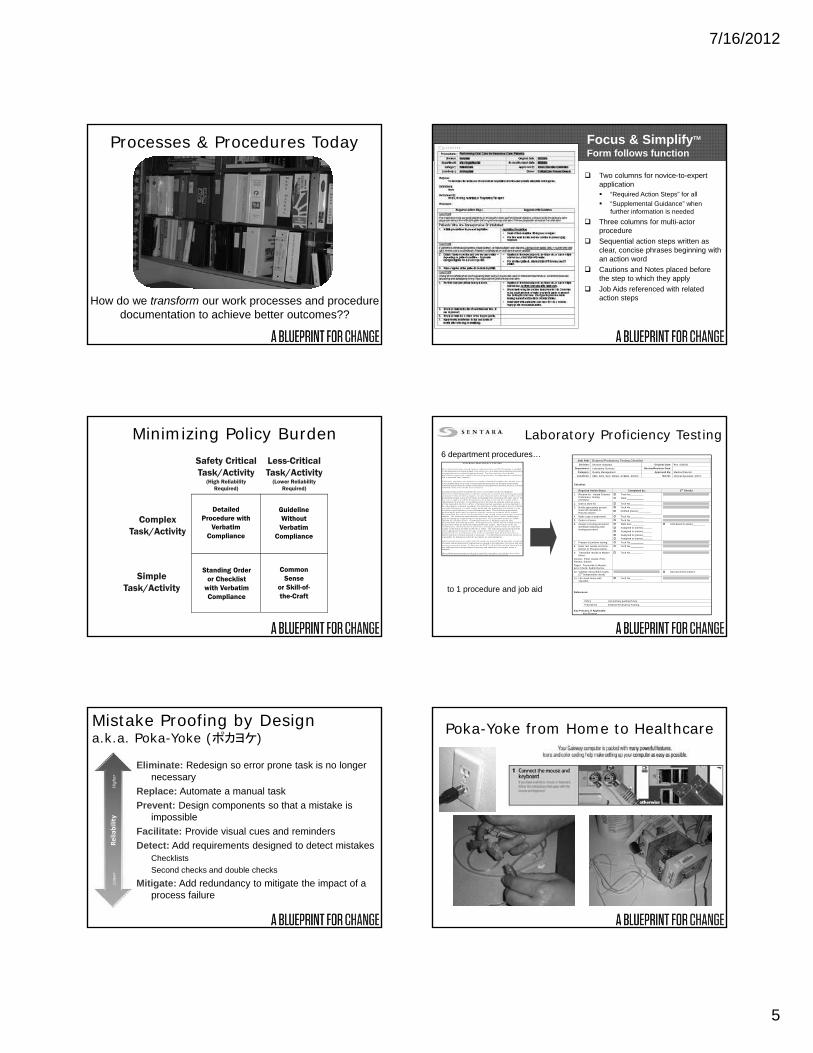
Processes & Procedures Today
How do we transform our work processes and procedure documentation to achieve better outcomes??
Focus & SimplifyTM
Form follows function
Two columns for novice-to-expert application “Required Action Steps” for all
“Supplemental Guidance” when further information is needed
Three columns for multi-actor procedure
Sequential action steps written as clear, concise phrases beginning with an action word
Cautions and Notes placed before the step to which they apply
Job Aids referenced with related action steps
Safety CriticalTask/Activity
(High ReliabilityRequired)
Less-CriticalTask/Activity
(Lower ReliabilityRequired)
ComplexTask/Activity
DetailedProcedure with
VerbatimCompliance
GuidelineWithoutVerbatim
Compliance
CommonSense
or Skill-of-the-Craft
Standing Orderor Checklist
with VerbatimCompliance
SimpleTask/Activity
Minimizing Policy Burden Laboratory Proficiency Testing
Job Aid: External Proficiency Testing ChecklistDivision: Sentara Hospitals Original Date: Rev. 5/05/05
Department: Laboratory Services Review/Revision Date:
Category: Quality Management Approved By: Medical Director
Locations: SBH, SCH, SLH, SNGH, SVBGH, SWCH Owner: Clinical Specialist, POCT
Checklist:
Required Action Steps: Completed by: 2nd Checks
1. Receive kit. Initiate ExternalProficiency TestingChecklist.
Tech No._________
Date:____________
2. Date & store kit. Tech No._________
3. Notify appropriate person.Hand off checklist toProcess Owner.
Tech No._________
Notified (name):_________
4. Make copy of paperwork. Tech No._________
5. Order in Cerner. Tech No._________
6. Assign to testing personnel.Schedule follow/up withtesting personnel.
Date due:_________
Assigned to (name):______
Assigned to (name):______
Assigned to (name):______
Assigned to (name):______
Scheduled f/u (date)_________
7. Prepare & perform testing. Tech No._________
8. Enter test results on forms.Deliver to Process Owner.
Tech No._________
9. Transcribe results to Masterforms.
On-line: Enter results, Print,Review, Submit.
Paper: Transcribe to Master,Error Check, Submit by fax.
Tech No._________
10. Validate transcribed results.(2nd independent check)
Second check (name):_________________________________
11. File result forms withchecklist.
Tech No._________
References:
Policy List primary guiding Policy
Procedures External Proficiency Testing
Key Process, If Applicable:Key Process
6 department procedures…
to 1 procedure and job aid
E X T E R N A L P R O F IC IE N C Y T E S T IN G
F or ex terna l p ro f icienc y tes ting , S en ta ra L abo rato ry S erv i ces P O C T p rog ram is en ro lledin the a pp rop r iate ava ila b le g rade d C A P su rve ys o r C A P-app ro ved a ltern ative p ro fici enc ytesting p ro g ra m s fo r pa tie n t tes ting pe rfo rm ed . Fo r those a nalytes w he re g rade dp ro f icienc y te sting is no t a vailab le , an in te rna l p ro fic ienc y tes ting p rog ram is e s tab lishedan d is exe rcise d sem i-a nnua lly.
P ro fic ienc y spec im ens a re re ceive d on a re gu lar sc he du le th rou ghou t the c ale ndar yea r. Itis the responsib ility o f all s ta ff to a ssu re th at the spe cim e ns are p roper ly s to red w he nre ce iv ed ; tha t the date o f rec eip t is ind ica ted on the pap erw o rk ; a nd that the P O C T sta ff isin fo rm ed o f th e a rriva l o f the su rve y m ate rial.
A ll in s truc tions nee ded to pe rfo rm the su rve y are include d w ith ea c h sh ipm en t.S pec im ens w ill be designate d to a spe cif ic nu rs in g u n it to e nsu re that a ll te s ting p ersonnelpa rticipate in the p ro ficie nc y p rog ra m . In som e in stanc es du e to the la rge num ber o f un itspe rfo rm in g te s ting , it m ay be nec essa ry fo r m u ltip le un its to pe rfo rm the sam e su rve y . Inth is ca se, a s in g le un it w ill be d esignate d as the p rim ary un it and the ir resu lts w ill besubm itted to the p rov ide r. T he n add itiona l un its w ill te s t the sam p le s and tho se re su ltsw ill be retaine d in the P O C T o ffic e. P ro f icien c y su rve y sp ecim e ns are to be hand le d inthe sa m e m a nner as pa tie n t spe cim ens. N o p ro f icienc y tes ting spe cim e ns m ay be re fe rre dto an o th er la bo ra to ry. F o r e ac h an aly te pe rfo rm e d , the a pp rop r iate in fo rm a tion is to b ere co rd ed on th e P ro fic ienc y S u rve y In fo rm ation S he et. T h e hea lthca re p ro fess ionalpe rfo rm in g th e p ro ficie nc y te s tin g m ust s ign the attes ta tio n s tatem e n t on the o r ig in aldoc um en tation tha t verif ies that the spec im ens w ere tre ated in the sa m e m anne r a s patie n tsam p le s . T he resu lts a re tran sc ribed and rev ie w e d by the P O C T S e n io r T e chno lo g is tp rio r to send ing the o rig inal fo rm s to the p rov ide r. T he tra nscribe d re su lts are doub le -ch eck ed b y on e o ther pe rson . T h e M e d ical D irec to r o r designe e s igns the fina ldoc um en tation be fo re be ing m ailed . A ll o rig inal su rve y resu lts m ust be m ailed /fa xe d tothe p rov ider w ith in the tim e f ram e ind ica ted fo r the ana lyt e. T he re m ust no t be a nyin ter la bo ra to ry c om m un ica tion on p ro f ic ien cy tes ting da ta be fo re resu lts are subm itted .C op ies o f the re su lts are file d in the P O C T o f fic e. T he re m ain ing spe cim ens sho u ld besto re d app rop ria tely base d on the type o f spec im en ( fro ze n o r re fr igerated ) in thede signa ted f re ez er o r re fr igerato r un til re su lts are ob tain ed from the p rov ider and it isde te rm ined th at no fu r ther ana ly sis is ne ce ssa ry . T he ind iv idual tha t m a ils th e su rve y isre sponsib le fo r m ak in g su re th at the spe cim e ns are s to re d p rop erly.
A pprox im ate ly fou r to s ix w ee ks afte r the re su lts are re ce ived b y the p rov ide r, a sum m aryo f resu lts and in te rlab o ra to ry com p arison is retu rne d to the labo ra to ry fo r rev ie w a nd an yne cessa ry c o rrective ac tion . A t th is tim e, the PO C T staff w ill also ev aluate th e resu lts o fan y add itional un its tha t perfo rm ed th e su rve y a nd de te rm ine if co r re ctive action isre qu ired .
T he acc red it in g p ro g ra m assig ns to e ac h re sul t a s ta nd a rd d ev ia tio n ind e x to d e scrib e ho w far a re sul t isfro m th e gro u p m ea n a s m ea sure d in sta nd ard d ev ia tio n u n its . R e sul ts a re rev ie w ed an d
Mistake Proofing by Designa.k.a. Poka-Yoke (ポカヨケ)
Eliminate: Redesign so error prone task is no longer necessary
Replace: Automate a manual task
Prevent: Design components so that a mistake is impossible
Facilitate: Provide visual cues and reminders
Detect: Add requirements designed to detect mistakesChecklists
Second checks and double checks
Mitigate: Add redundancy to mitigate the impact of a process failure
Lower
Reliability
Higher
Poka-Yoke from Home to Healthcare

7/16/2012
6
Error Proofing Tactics
Constraints Provide design features that compel or exclude actions. Constraints may be physical, semantic, cultural, or logical .
Affordances Provide guidance for operation of device by providing features that allow certain actions.
Natural Mappings Design one‐to‐one correspondence between controls and device being controlled.
Visibility Make operation of the device visible.
Feedback Give each action an immediate and obvious effect.
Norman’s Tactics for Knowledge in the Environment
Agency for Healthcare Research and QualityPrepared by John Grout (Berry College)
Changing Behaviors
Set Expectations
Educate & Build Skill
Reinforce & Build
Accountability
© 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Non-Technical SkillsNon-technical skills describe how people interact with technology, environment, and other people. These skills are similar across a wide range of job functions. These skills include attention, information processing, and cognition.
Flin, O’Connor, and CrichtonSafety at the Sharp End
Generic non-technical skills:
Situational awareness Attention Communication
repeat backs call outs phonetic & numeric clarification clarifying questions inquiry, advocacy, assertion
Critical thinking Protocol use Decision-making
Power Distance
Large Distance• Relations are autocratic and
paternalistic• Power acknowledged based on
formal, hierarchical positions
The perceived distance – not necessarily the real difference –as seen by the subordinate
Small Distance• Relations are consultative and
democratic• Relate as equals regardless of
formal positions
Reference: Hofestede, Geert. Culture’s Consequences, 2001 (2nd edition).
Collegial Interactive Teams (CIT) = Tone + ToolsContext• Patient focused – like we’re
caring for a loved one
Collegiality• Greetings & introductions• Eye contact &
open body language• Relationships• Team goals – use “we”
and “us” vs. “I” and “you”
Coordination• Who’s in charge• Roles & responsibilities• Brief>Execute>Debrief
– pocket card in-hand
Communication• Information – ready
& in hand• 3-way repeat backs• Clarifying questions• Phonetic/numeric
clarifications• SBAR for requestsConfidence in Speaking Up
• Cross Monitoring – peer checking & peer coaching• “If anyone – regardless of role or experience – senses a
problem that would compromise safe, quality care, I expect you to speak up.”
Make Reliability a Reality
Collegial
Interactive
Team
Critical Thinking
Safety Culture
Critical ThinkingQuestioning AttitudeProactive hindsightSTEPSORT(Train using case study in modules)
Culture of SafetyPatient first, every timeSafety firstImportance of attention (self‐check)Importance of compliance (Red Rules)Cross monitoringSpeaking‐up for safety as a concept(Train using leader modules)
Collegial Interactive TeamsSituational awarenessCommunication bundle:• Repeat‐back• Call out• Phonetic & numeric clarification• Clarifying questionsSpeak‐up (inquiry‐advocacy‐assertion)Brief‐Execute‐Debrief(Train in teams using simulation)
STEP = Story, Test story, Eliminate gaps in story, Plan to proceedSORT = Statement of problem, Options, Rule-out options, Test and take action

7/16/2012
7
Questioning Attitudewith Validate & Verify Technique
Validate: Does it make sense to me?
Verify: Check with an independent, qualified source
Patient
Technology
Professionals
Medical RecordDocumentation Procedures &
References
Peer CheckingWatching-out for each other. Peers share situational awareness and provide on-the-spot second opinions.
Peer CoachingInvolves feedback. Peers provide a 5:1 ratio of positive to negative feedback to reinforce good habits, extinguish poor habits, and build better practice habits.
Multiply Your Error Probability0.001 x 0.001 = 10-6
Cross Monitoring
Making it Stick:“It’s Hawthorne Until Habit”
20%
Eve
nt R
ate
Awareness
Skill Acquisition
Habit Formation
Performance
Time
100%
2 Years
© 2006 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Novice ‐ Advanced Beginner ‐ Competent ‐ Proficient ‐ ExpertSource: Patricia Benner, From Novice to Expert (1984)
Unconsciously incompetent ‐ Consciously incompetent ‐ Consciously competent ‐ Unconsciously competent"Four Stages of Learning," a theory posited by 1940's psychologist Abraham Maslow
Leading Causes of Action Failure
Hidden non-commitment(there seems to be agreement, but managers later back out)
Soft cost – benefit analysis(the best root solution is always the cost effective solution)
Medical Staff resistance(Involve physicians early in the process and rely on tactful diplomacy)
Poor implementation accountability(Corrective Action Plan should have responsible parties by name and date)
From Maximize Patient Safety with Advanced Root Cause Analysis; Corbett, Clapper, & Johnson; 2004.
Plan the Work – Work the PlanA4 Action Plans
One-page, problem, causes, and actions with names & due dates
“A4” refers to the size of the paper. The plan is intended to fit on a single page. A4 is a letter-
sized page; A3 is legal.
Managing Complex ChangeVision Skills Incentives Resources Action Plan
Effective Change
Confusion
Anxiety
Gradual Change
Frustration
False Starts
Skills Incentives Resources Action Plan
Vision Incentives Resources Action Plan
Vision Skills Resources Action Plan
Vision Skills Incentives Action Plan
Vision Skills Incentives Resources
=
=
=
=
=
=
Source: Brandeis University Center for Youth & Communities

7/16/2012
8
Rapid Cycle FeedbackLearning is “doing” with “feedback”
© 2008 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Do
Feedback
TraditionalFeedback Cycle
OptimalFeedback Cycle
Time
Per
form
ance
Technical SkillsTechnical +
Non‐Technical Skills
Non‐Technical Skills
(Individual & Team)
Simulation in the Lab
Pre‐JobBriefing
Real‐Time SimTeachingon the Spot
Simulation at the Line
Is there any technical skill that does not also require non‐technical skills? NO! Eliminatetechnical simulation in
isolation!
Off‐Line Education & Training Real‐Time Simulation
Best UseInitial education on new concepts; intensive skill development
Reinforcement and application of known concepts; development of critical thinking and analytical problem solving
Location Classroom, training lab, meeting On‐the‐job
Nature Objective‐bound Time‐bound
Prep Time Longer Short to none
Touch Time Longer (>30 minutes, typically hours) Short (30/60/90 seconds; typically <5 minutes)
Frequency Episodic; longer time between sessions Often; shorter time between touches
Facilitator Trained instructors or manager Manager or coworker
Costs Salary of instructors/learners; supplies None
To build and reinforce technical skills and critical thinking skills
To build and reinforce technical skills and critical thinking skills
Build real-time simulation as a leadership competency!
© 2011 Healthcare Performance Improvement, LLC. ALL RIGHTS RESERVED.
Simulation Continuum
Sim Center Sim Center In‐Situ Sim
Technical skills Team skills
EnvironmentProtocolEBM + human factors
Technical+ CIT skills
A fool’s choice:o technical skills in isolation, oro team skills in isolation
Perfect practice makes perfect.
Practice only makes permanent.
“What you do every day is what you do in an emergency.” Joe Martin, Battalion Chief - LAFD
A Triple Play
Craig Clapper, PE, CMQ/OEPartner & Chief Knowledge Officer
Healthcare Performance Improvement, LLC5041 Corporate Woods Drive, Suite 180
Virginia Beach, VA 23462(757) 226-7479 www.hpiresults.com