urgent care programme - wye valley
TRANSCRIPT

URGENT CARE PROGRAMME
A quality of care we would want for
ourselves, our families and our friends
URGENT CARE PROGRAMME
Objectives
To implement clinically led Urgent & Emergency Care projects to enable the delivery of safer, faster and better care to our patients.
To improve ‘patient flow’
Deliverables/Measures
As outlined by ECIP the successful programme will be measured against; Better patient outcomes Improvement to the Emergency Care 4 hour waiting standardOverall patient experience
The programme will also see improvements in; Ambulance handover times Time to assess Length of Stay Bed Occupancy DToC
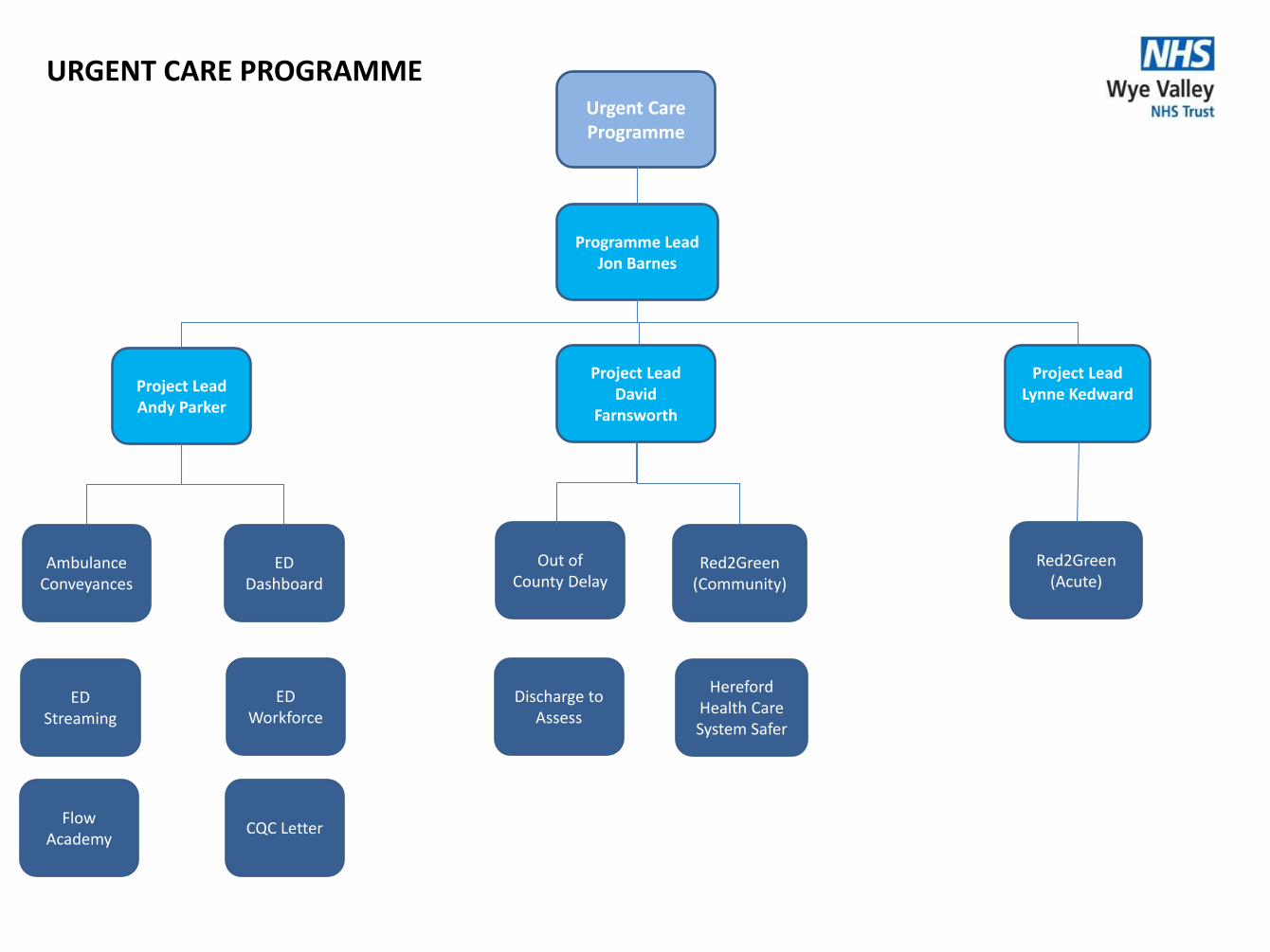
Urgent Care Programme
Project LeadDavid
Farnsworth
Programme Lead Jon Barnes
Project LeadAndy Parker
ED Dashboard
Ambulance Conveyances
Project LeadLynne Kedward
Red2Green (Community)
Out of County Delay
URGENT CARE PROGRAMME
Hereford Health Care System Safer
Discharge to Assess
ED Workforce
ED Streaming
CQC LetterFlow
Academy
Red2Green (Acute)

AMBULANCE CONVEYANCES
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Ambulance ConveyancesObjectives
To establish a process between Trusts where we are able to raise conveyance issues on a regular basis in a robust and open manner.
Reduction in Corridor waits
To improve relationships between Trusts
To establish real time conveyance audit
Deliverables/Measures
Reduction in the inappropriate conveyances to hospital
Development of audit process and documentation
Introduction of named link person at WMAS
Monthly reports on corridor waits to review data and trends
Development of an issues register to review and monitor progress

Ambulance conveyances
Project RAG Status
Risks/Issues Plans Overall Path to green
• Dependant on WMAS engagement• Collection of data via audit process
Achievements this period
• Agreed Audit days – 27 & 28 Nov. – no show from WMAS - escalated• Regular meetings at local level regarding Ambulance/ED audits• WMAS undertaking audit of out of area
Actions for next period
• Revised dates for audits with WMAS – 3 dates to be arranged for Jan’18
• Await outcomes of out of area audit – Feb/Mar’18• Review of NHSE letter – handover delays
Decisions required/ Project Commentary
1. Escalation process in place to A&E delivery Board
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Lack of engagement by WMAS M • To be raised at A&E delivery Board
• Audit dates do not happen causing delays H • Escalate to WMAS link person and refer to A&E delivery Board if needed
Project Lead
Andy Parker

Ambulance Conveyances
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Audit dates to be confirmed with WMAS Nov/Dec2017
Dates cancelled, only one date completed, 3 to be arranged in Jan’18
Review of NHSE letter and agree actions Dec 2017
Actions from NHSE letter Jan 2018 This may form a separate project
Review of Audit data Jan 2018
Implement actions from audit March 2018
Establish agreed processes for handover delays with WMAS
Ensure above is recorded correctly within ED and dedicated owner/s of task
Agree structure forum to review Ambulance conveyance and challenge
Urgent Care Project Update – December 2017

ED DASHBOARD
PROJECT
A quality of care we would want for
ourselves, our families and our friends

ED Dashboard
Objectives
To provide a dashboard that will enable analysis of trends to inform relevant staff on a daily basis.
To be used to target issues and implement plans/actions.
Provide visibility of trends and impact of actions.
Deliverables/Measures
Easy to use “drill down” function of key metrics
Data to be “live”, so staff can review the current situation in ED
Analysis of performance (root cause) and actions implemented
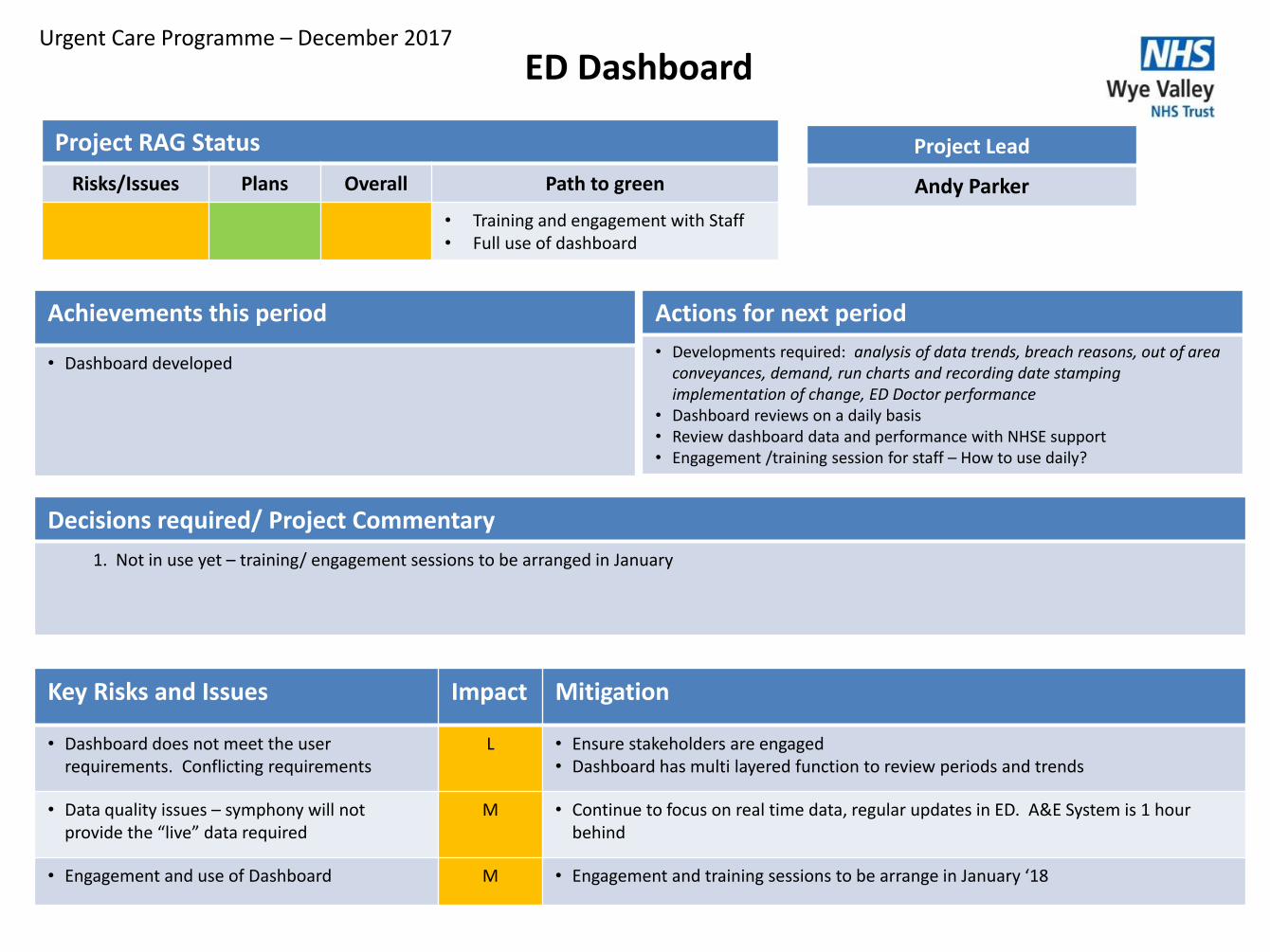
ED Dashboard
Project RAG Status
Risks/Issues Plans Overall Path to green
• Training and engagement with Staff• Full use of dashboard
Achievements this period
• Dashboard developed
Actions for next period
• Developments required: analysis of data trends, breach reasons, out of area conveyances, demand, run charts and recording date stamping implementation of change, ED Doctor performance
• Dashboard reviews on a daily basis• Review dashboard data and performance with NHSE support• Engagement /training session for staff – How to use daily?
Decisions required/ Project Commentary
1. Not in use yet – training/ engagement sessions to be arranged in January
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Dashboard does not meet the user requirements. Conflicting requirements
L • Ensure stakeholders are engaged• Dashboard has multi layered function to review periods and trends
• Data quality issues – symphony will not provide the “live” data required
M • Continue to focus on real time data, regular updates in ED. A&E System is 1 hour behind
• Engagement and use of Dashboard M • Engagement and training sessions to be arrange in January ‘18
Project Lead
Andy Parker

ED Dashboard
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Confirm basic requirements/metrics required is on an easily accessible platform
Test metrics with Key stakeholders and adapt accordingly
Jan’18 During engagement Session
Training/Engagement sessions to be held Jan’18 Use of Dashboard as part of daily routine
Urgent Care Project Update– December 2017
ED STREAMING
PROJECT
A quality of care we would want for
ourselves, our families and our friends

ED Streaming
Objectives
To establish a clear streaming model that provides deliverable performance and quality by April 2018.Focus on senior decision making at the front door.
To test processes in preparedness for Primary Care Streaming by October 2017
Deliverables/Measures
Meet CQUIN target 2017/18– Sepsis – time to first antibiotic
Model fully implemented by April 2018
Develop Performance related reports – Numbers of patients seen by GP’s and outcomes.

ED Streaming
Project RAG Status
Risks/Issues Plans Overall Path to green
• Successful recruitment and model in place
Achievements this period
• Increased Primary Care streaming sessions within ED• Building work on schedule• Ongoing review of GP productivity via weekly meetings• Operational Group established• Increased Coverage from Taurus from Jan’18
Actions for next period
• Draft SOP’s - ongoing• Undertake formal review at UCBP - ongoing• Agree SLA with Taurus – ongoing• Two system issues to be discussed and resolved• Advertise for navigator/triage trainer• Increase Primary Care streaming session in ED
Decisions required/ Project Commentary
1. Operational issues to resolve APEX and X-ray reviews2. Resolve Navigation remit – trial via Perfect weekend/ongoing3. Resolve EMIS/Symphony recording and reporting issues
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Reliable and accurate data collection and analysis
• Delays in change for the better may cause issues with staff engagement
• Availability of GP Streamer/Navigator
M • Dedicated information support to collect and provide summary of key headlines
M • It is vital that any change deemed necessary following perfect week is done in a timely manner to max. on high staff morale.
H • Regular GP and Navigation to increase productivity – Look to source from other provider or own
Project Lead
Andy Parker

ED Streaming
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Planning for Perfect Week Complete
Run Perfect Week Complete
Report to Urgent Care Board - monthly Complete
Complete Business Case Complete
Proceed with Interim arrangements Ongoing
Commence Estates Work Ongoing
Develop Workforce plan Jan 2018
Complete Estates work Feb 2018
Contract – Increase in hours of GP’s in ED –cover will be 10.00 am to 10.00 pm
Jan 2018 GP recruited by Taurus to start in Jan 2018
Weekly meetings with Taurus to discuss issues eg. two systems, IG issues
ongoing Weekly meetings set up and will be ongoing to resolve issues
Urgent Care Project Update – December 2017

ED WORKFORCE
PROJECT
A quality of care we would want for
ourselves, our families and our friends

ED WorkforceObjectives
To establish a clear documented workforce ‘plan on a page’ of the current establishment and skill mix for Nursing and Medical staff that shows the establishment against a revised workforce plan that delivers the clinical safety of patients and NHS targets for ED within the budget.
Recruitment trajectory for department
Mapping of workforce Vs demand
Review of skill mix and staff grades against new roles and ways of working
Workforce budget to match financial envelope
Reduction in Agency spend
Deliverables/Measures
Reduction in Agency Spend and Usage
Achieve CQUIN – Sepsis – time to first antibiotic
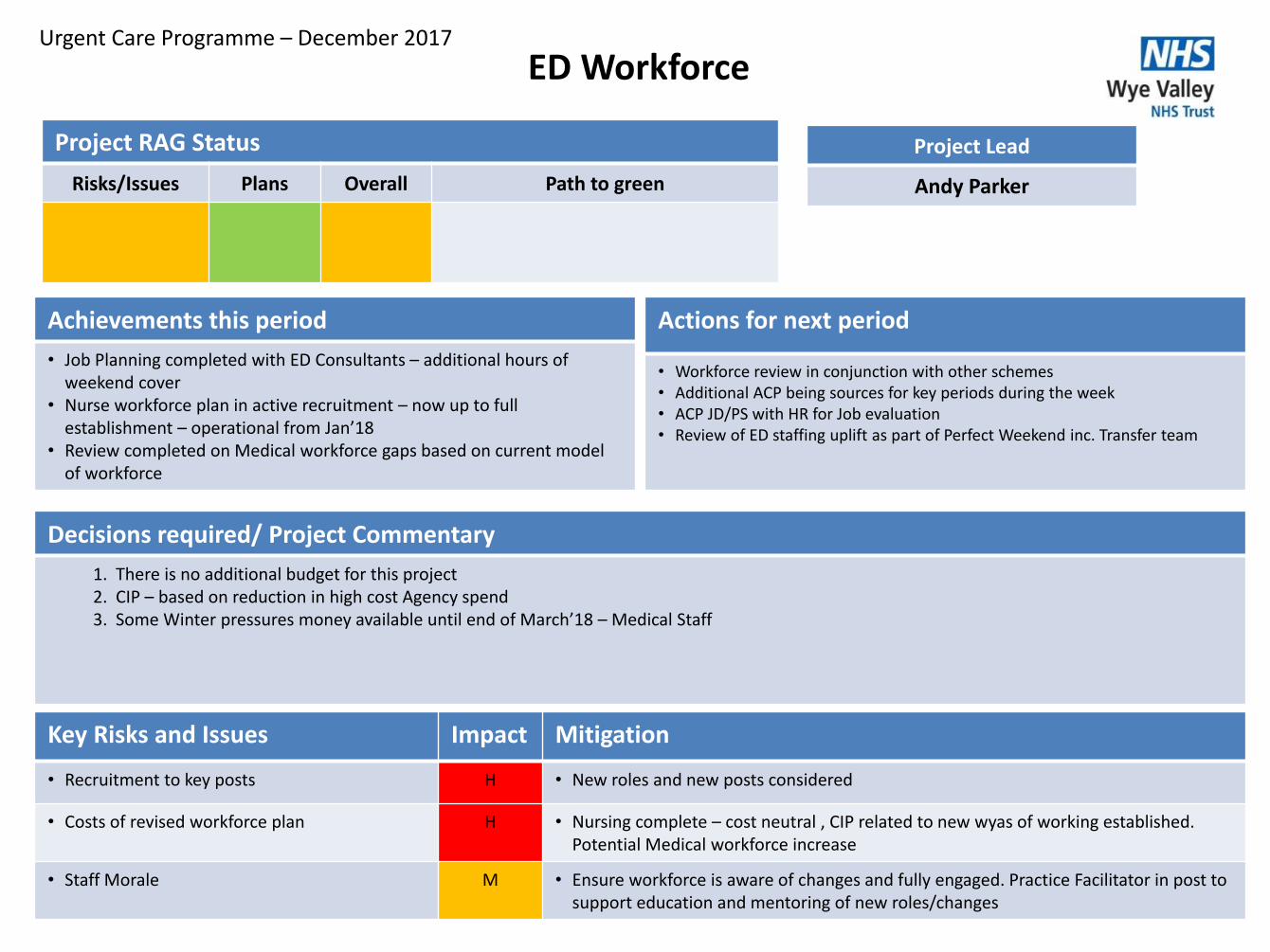
ED Workforce
Project RAG Status
Risks/Issues Plans Overall Path to green
Achievements this period
• Job Planning completed with ED Consultants – additional hours of weekend cover
• Nurse workforce plan in active recruitment – now up to full establishment – operational from Jan’18
• Review completed on Medical workforce gaps based on current model of workforce
Actions for next period
• Workforce review in conjunction with other schemes• Additional ACP being sources for key periods during the week• ACP JD/PS with HR for Job evaluation• Review of ED staffing uplift as part of Perfect Weekend inc. Transfer team
Decisions required/ Project Commentary
1. There is no additional budget for this project2. CIP – based on reduction in high cost Agency spend3. Some Winter pressures money available until end of March’18 – Medical Staff
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Recruitment to key posts H • New roles and new posts considered
• Costs of revised workforce plan H • Nursing complete – cost neutral , CIP related to new wyas of working established. Potential Medical workforce increase
• Staff Morale M • Ensure workforce is aware of changes and fully engaged. Practice Facilitator in post to support education and mentoring of new roles/changes
Project Lead
Andy Parker

ED Workforce
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Workforce plan for Nursing established Complete
Workforce plan for Medical established Now included in ED Streaming bid
Profile against ‘Perfect Week’ establishment
Realign working hours to match demand and future ED Streaming
31 Jan 2018 ENP’s delayed – on Hold Review required
Understand ED Medical workforce gaps Review alternative workforce to bridge gap – part of Business planning and workforce plan
Geriatrician to work in ED 3 x afternoons a week
31 Jan 2018
Acute Physician working in ED 31 Jan 2018
Urgent Care Project Update– December 2017

HOSPITAL @ NIGHT
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Hospital @ NightObjectives- Phase 1
Data- capture
Bleep filtering
Change of practice – non-urgent tasks/ bleeps to FY1’s
Engagement of different staff groups
Deliverables/Measures
Data capture tool

Hospital @ Night
Project RAG Status
Risks/Issues Plans Overall Path to green
• Data capture , data quality, development of phase 2 (dependant on cross over between specialities-surgery to agree )
Achievements this period – Phase 1
• Agreed Go Live will capture data only• Go Live data agreed – 29 November 2017• Data capture process agreed• Communication plan in place
Actions for next period – Phase 1 continued
• Reiterate nursing ward communications • Handover at 22:00 and 06:00 by FY1s to site team; Suggestion: a copy of
written handovers/ notes taken during medical/surgical handovers to be handed over to the site team at 22:00 and 06:00
• Site team to verify/chase the handover requirements • Site team to reinforce communication regarding hospital at night ie . via ward
visits at night• Communication through trust talk, team brief, emails.• Monitoring of database information and sharing of reports with relevant
groups
Decisions required/ Project Commentary
Phase 1’s success is dependant on a) Data quality and b) Staff engagement and change of practice Phase 2’s success is dependent on cross cover of specialities
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Data quality • Process maps , communication plans implemented and ongoing
• Staff engagement /change of practice • Reiterate communication and manage staff groups
Project Lead
Andy Parker
Actions for next period – Phase 1
• Monitor Go Live – 29 November 2017• Ensure Data capture on Go Live• Review will take place in January 2018• Feedback and engagement from FY1s
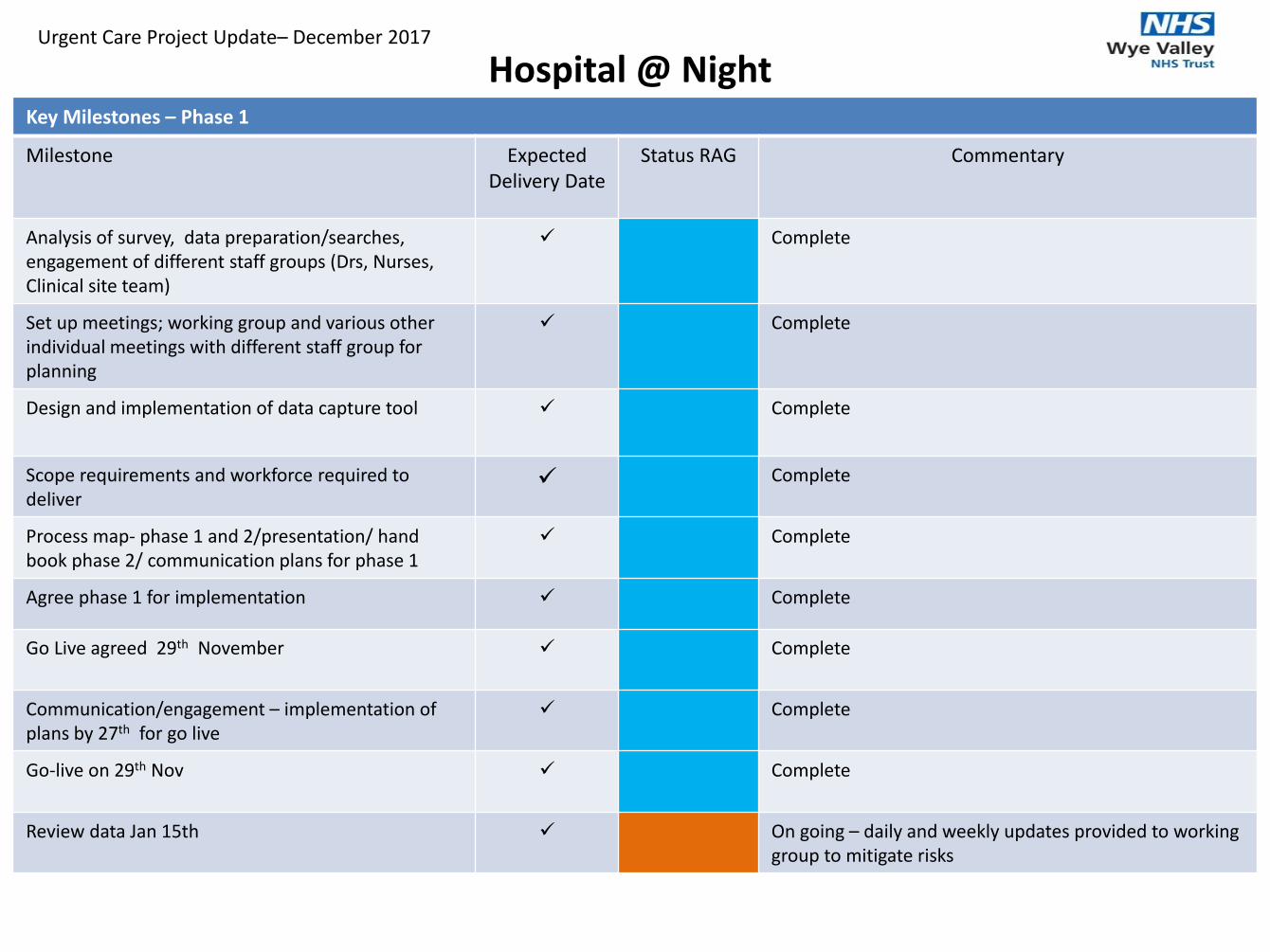
Hospital @ NightKey Milestones – Phase 1
Milestone Expected Delivery Date
Status RAG Commentary
Analysis of survey, data preparation/searches, engagement of different staff groups (Drs, Nurses, Clinical site team)
Complete
Set up meetings; working group and various other individual meetings with different staff group for planning
Complete
Design and implementation of data capture tool Complete
Scope requirements and workforce required to deliver
Complete
Process map- phase 1 and 2/presentation/ hand book phase 2/ communication plans for phase 1
Complete
Agree phase 1 for implementation Complete
Go Live agreed 29th November Complete
Communication/engagement – implementation of plans by 27th for go live
Complete
Go-live on 29th Nov Complete
Review data Jan 15th On going – daily and weekly updates provided to working group to mitigate risks
Urgent Care Project Update– December 2017

Hospital Out of HoursObjectives – Phase 2
Multi-disciplinary whole Hospital handover
Working as one team cross-covering specialities when necessary
Handover to the speciality teams in the morning
Deliverables/Measures
Prioritise patient-related tasks based on clinical need
Will ensure that the right health professional is guided to the right place at the right time.
Admissions will be dealt with by a multidisciplinary team that will bring in on-call medical staff whenever needed.
Reduction in delays in speciality referral in ED overnight
Potential reduction in Medical Agency spend

FLOW ACADEMY
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Flow AcademyObjectives
Sustainable improvement is best delivered by people on the frontline
Team ownership of ideas and decisions – what to improve and how to improve`
Focus on patient
Use of a number of tools to improve service delivery and quality of care
Make small changes to deliver measurable improvements
Trustwide ownership of flow at all levels within the Trust
Deliverables/Measures

Flow Academy
Project RAG Status
Risks/Issues Plans Overall Path to green
Achievements this period
• Lodging SOP for patients awaiting transport in ED updated• Medical assessment clerking form on Symphony• Expedited referrals to Medical/Surgical teams• Clinical review of ‘Blended’ ED and medical workforce• Perfect weekend – completed• Dedicated presence of Acute Physicians in ED• ED Huddles – implemented• ED weekend Sister SitRep trialled
Actions for next period
• ED/Ward handover process – further work required• External calls to ED Reception from Switch – final training for switch staff• Scope/Business case for Surgical SAU• Clerking of surgical/T&O patients in ED• ED checklist to be implemented• Flow Academy fortnightly action reviews to close actions down and update
team.• Live dashboard of MIU/ED waiting times for internet• Fit2Sit – ongoing review• ED Huddles – further review /implement overnight• Direct referral of stroke patients to ward by CNS’s• Set up operational meetings twice a month to action outputs of Flow
Academy
Decisions required/ Project Commentary
1. Orthopaedic attendance at Flow Academy to discuss ED delays and clerking
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Staff engagement with Flow Academy H
• Capacity within ED to drive through changes and embed
M Interim ED Manager in post- reduced portfolio for matron
• Delivery of schemes on time H
• Culture of department H • Continual work with teams and Exec. Support to assist in delivery changes. Ensuring leaders lead by example challenge/resolve issues.
Project Lead
Andy Parker

Flow Academy
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Fit2Sit Implemented
Joint Medical Clerking document Implemented
Clinical review of ‘Blended’ ED and Medical workforce
Completed
Perfect Weekend – 9 &10 Dec Completed
ED Huddles Implemented
Direct referrals for Stroke patients to ward by CNS’s
Implemented
Clerking of Surgical/T&O patients in ED Jan 2018 In discussions
Set up Operational meeting twice a month to action outputs of Flow Academy
Jan 2018 Ongoing
Urgent Care Project Update– December 2017

RED2GREEN (ACUTE)
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Red2Green (Acute)
Objectives
Introduction of Red2Green principles across all in-patient areas
Ensure ownership and sustainability of principles through embedding R2G as ‘Business as Usual’
Deliverables/Measures
Develop schedule of roll out ward by ward, month by month by April 2018
Implement roll out by August 2018
Implement Red2Green Dashboard on EPR by March 2018
Data capture is ‘live’, visible and maintained as each ward goes live
Red2Green data is reviewed at site safety meetings by March 2018
Organisational ownership of the issues preventing discharge – actions required as trends identified

Red2Green (Acute)
Project RAG Status
Risks/Issues Plans Overall Path to green
• Embed in 1 ward for medicine and 1 ward for surgery
• Implement R2G data collection in Maxims • Roll out ward by ward in each division• Embed review of red day trends and actions
in Site Safety meetings
Achievements this period
• Pop up banners strategically place around the Trust
Actions for next period
• Continued work with MAXIMS to embed R2G in electronic system• Change to data capture arrangements using new spreadsheet• Reporting is being built into site safety meetings• Implementation of Whiteboard on Frome ward• Review of further whiteboard options for other wards
Decisions required/ Project Commentary
1. Following last Urgent Care Programme Board, it was agreed to re-focus on two key wards and then roll out ward by ward2. Data capture capability to be delivered in February3. Exploring use of Whiteboards on Monnow and GAU aligned with release of R2G data capture capability in Maxims
Urgent Care Programme – January 2018
Key Risks and Issues Impact Mitigation
• Delays in release of Maxims capability M • Continue manual data capture
• Lack of funding for whiteboards M • Explore use of EPR programme finance
• Clinician engagement M • With each area of agreed roll out, meetings and support to be given to whole team
Project Lead
Lynne Kedward

Red2Green (Acute)
Key Milestones
Milestone Expected Delivery Date
Status RAG Commentary
Identify one ward from each division to run R2G on 7th November 2017
Complete - Monnow identified for Surgery, GAU identified for Medicine
Develop standard data collection proforma 7th November 2017
Complete - New proforma developed
Maxims data capture capability to be delivered in February
14th February 2018
Functionality delivered in 12.2.5 29th January, will be available following 2 weeks of testing on 14th February
Exploring use of Whiteboards on Monnow and GAU aligned with release of R2G data capture capability in Maxims
14th February 2018
Build R2G red day trend data into site safety meetings 21st February 2018
Maxims functionality will assist in delivering this through dashboard access at site safety meetings
Identify next two wards for roll out of R2G 28th February 2018
To be identified by the Divisions
Urgent Care Project Update– January 2018

Data capture (in Maxims)On the Ward Data View there will be a dedicated Bed Day column with a new icon. On selection of the icon, this will open a new dialog (Figure 1) in edit mode allowing a user to enter information relating to the Red and Green Bed Days. The recording HCP details will default to the logged in user. If a user selects the Green radio button and saves this will display as an icon on the ward data view against the selected patient with the day number also displayed calculated from the Admission Date
If a user selects the Red radio button and selects save this will display as an icon on the ward data view against the selected patient with the day number also displayed calculated from the Admission Date On selection of the Red radio button, this will display the Red Bed Day Reason field which will be mandatory. This is a locally configured look up combo. There will be a free text comments field that can be completed for Red days only. The Bed Day dialog will have a grid which will display a Bed Day Status record for each day since the admission date. Any date that does not have a Bed Day record will have a status of outstanding. On selection of a row the corresponding information will be available in the Bed Day Details pane. A user will be able to create of new record or update an existing record accordingly. This will in turn update the Bed Day Status on any related form/dashboard.

Data capture (in Maxims)Figure 1 Bed Days Dialog
Field Name Description
Grid
Date Date relating to Bed Day Record
Bed Day Status This will display the Bed Day Status which will be either Red, Green or Outstanding
Bed Day System Look up type with two look up instances – Red & Green (please colour the
instances accordingly) (Mandatory)
Red Bed Day Reason Look up type – locally configurable. This will only be displayed if Red has been selected in
the Bed Day field. (Mandatory)
Comments Free Text field – 500-character limit
Recording HCP Default logged in user – read only
Recording Date/Time Default to current date/time - read only

Data capture (in Maxims)
A running total of both Green and Red days needs to be available to access for each patient. (Figure 2) We are exploring the use of a dashboard for ward/hospital totals – needs discussion. Needs incorporating into Bed Management dashboards Figure 2 Red and Green Bed Days
This functionality will be delivered in version 12.2.5 on the 29th January. This will require 2 weeks of testing and the provisional date for this to be deployed in to our ‘Live’ environment is the 14th February.

Awaiting Community Services
Example Ward Data

OUT OF COUNTY DELAY
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Out of County Delay
Objectives
To reduce the impact of delays in repatriating Out of County patients to their own bed
Deliverables/Measures
Improvement of patient discharge performance from community sites
Improvement quality of patient experience (FFT)
Improvement on Length of Stay

Out of County Delay
Project RAG Status
Risks/Issues Plans Overall Path to green
Achievements this period
• Shropshire/Herefordshire Equipment pathway review (NHSE led)• Shropshire engagement in bi-weekly calls - continue• Senior teleconference with Shropshire led by WVT Deputy COO• Engagement with Powys and escalation agreed
Actions for next period
• Escalation of Powys ASC engagement by COO• Council lead on trusted assessor programme – being discussed• Engagement with Powys – Deterioration in performance• CCG Powys transfer workshop
Decisions required/ Project Commentary
1. Senior Executive engagement in this work including COO. Limited capacity across Powys provision remains problematic
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Reliance on Partner engagement M/H • NHSE leadership and WVT executive support required
• IBCF guidance – reporting conflict with overall DTOC performance
M • Improve accuracy of Trust recording system by January 2018
Project Lead
David Farnsworth
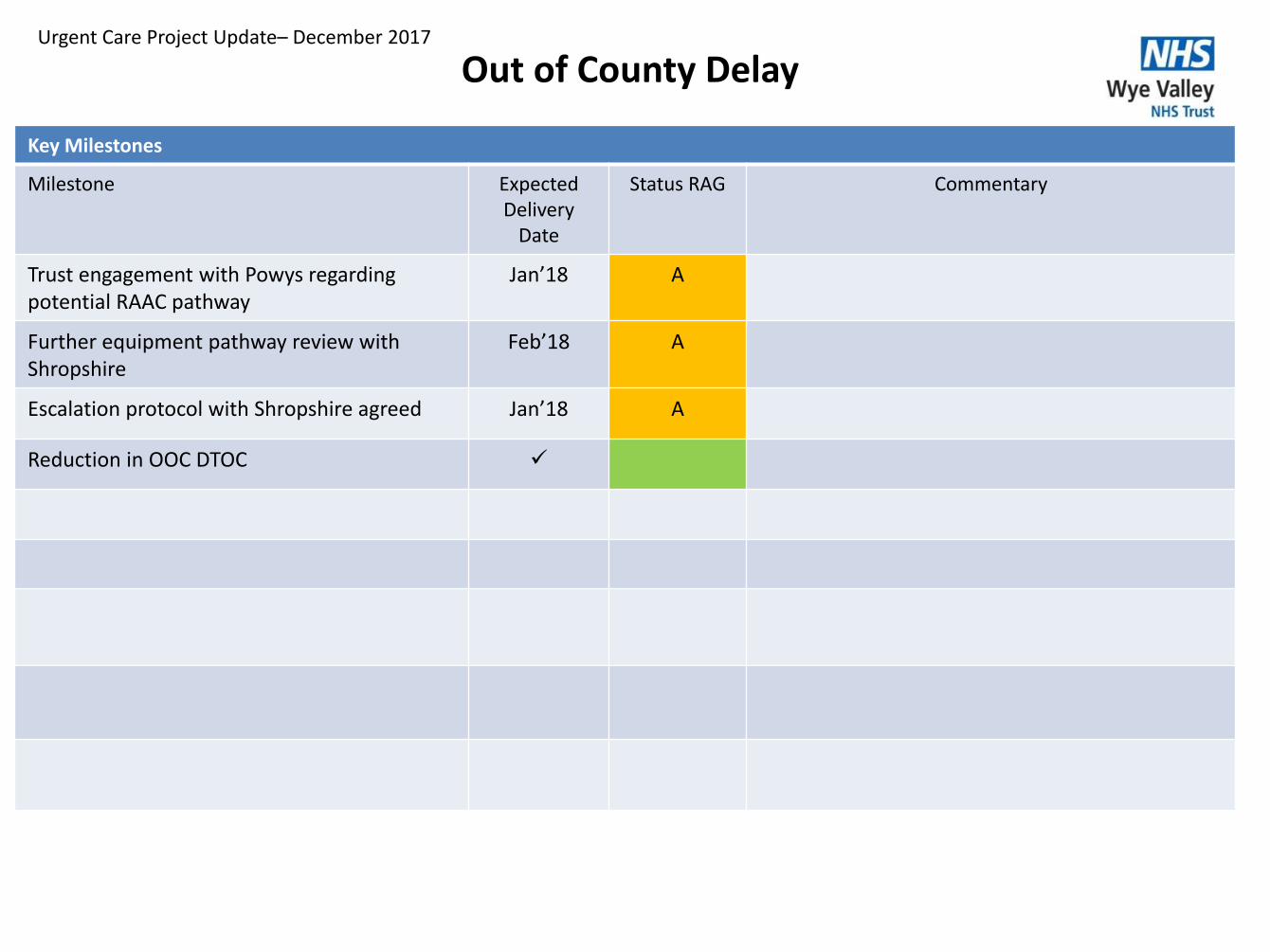
Out of County Delay
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Trust engagement with Powys regarding potential RAAC pathway
Jan’18 A
Further equipment pathway review with Shropshire
Feb’18 A
Escalation protocol with Shropshire agreed Jan’18 A
Reduction in OOC DTOC
Urgent Care Project Update– December 2017

DISCHARGE TO ASSESS
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Discharge to Assess
Objectives
To develop and implement an alternative route to care (step up or step down) which supports a reduced reliance on community hospital based care by April 2018.
Deliverables/Measures
Reduced admissions to community beds
Improvement of patient discharge performance from community sites (LoS)
Improved Patient feedback (FFT)
Reduced numbers of patients going into long term care (HC Commissioning Dashboard)

Discharge to Assess
Project RAG Status
Risks/Issues Plans Overall Path to green
A/G • Subject to Commissioning arrangements with Shaw Healthcare
Achievements this period
• Home first soft launch – limited ASC staffing capacity• Further workshop process planning across teams• CCG and LA review of commissioning arrangements with Shaw –
agreement on mixed nursing and residential provision• Limited recruitment by ASC to reablement workers – proposed WVT
recruitment?
Actions for next period
• Further meeting with Shaw to agree staffing requirement• Meeting required with GP practices to scope cover• Commencement of working party for mobilisation of D2A
Decisions required/ Project Commentary
1. There is a proposed financing from Better Care fund - £200k in year/£400k 18/19. Potential to be linked to CIP delivery2. Reviewing staffing potential for Home First team subject to closure of Hillside and staffing released
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Staff engagement H • Full engagement programme to be implemented (clarity on timescales from CCG)
• CCG led engagement/consultation H • Events scheduled with Trust participation - complete
• Finance H • Dependant on commissioner investment
• Recruitment M • Will link to Trust recruitment & training programmes
Project Lead
David Farnsworth
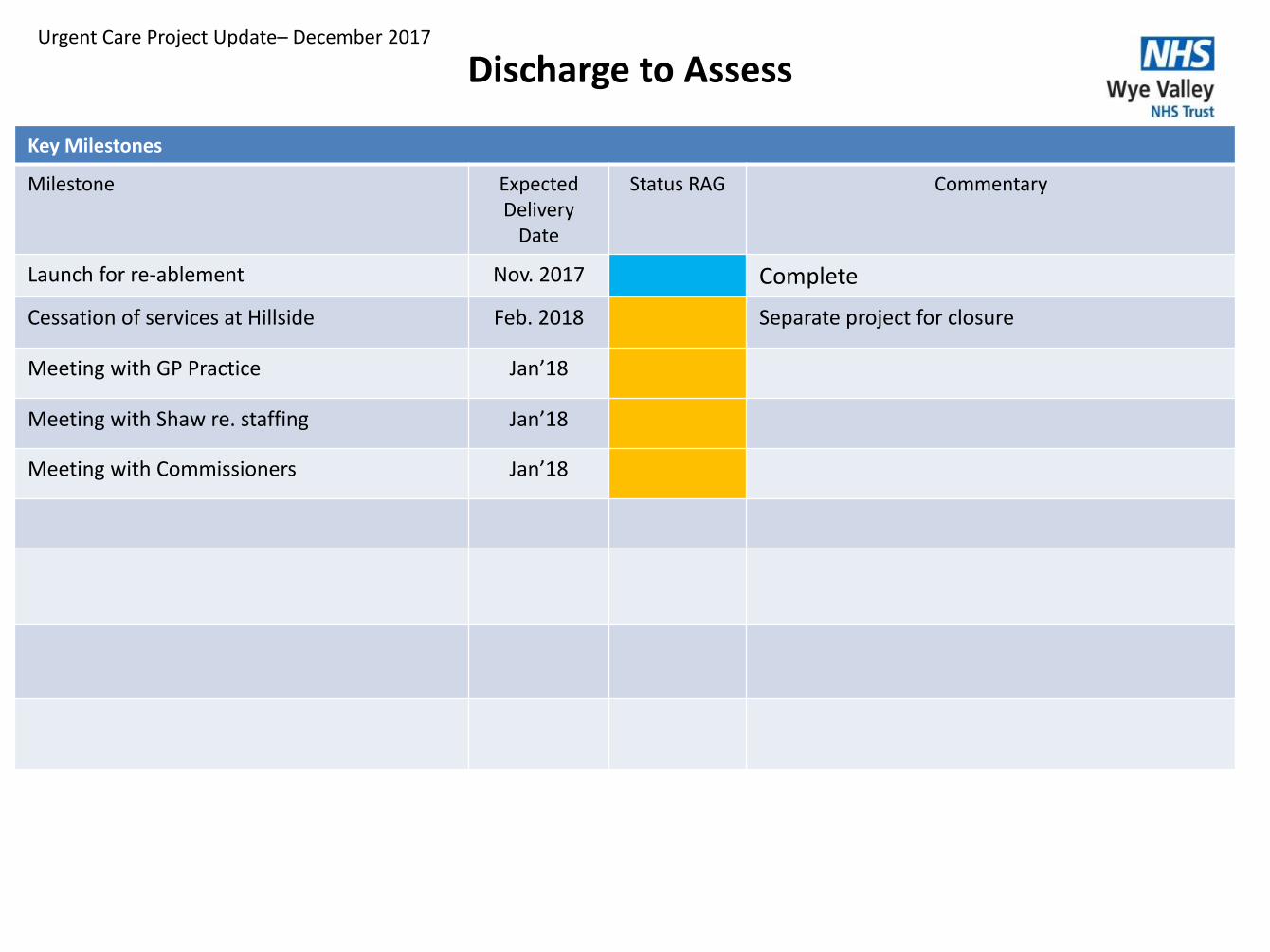
Discharge to Assess
Key Milestones
Milestone Expected Delivery
Date
Status RAG Commentary
Launch for re-ablement Nov. 2017 Complete
Cessation of services at Hillside Feb. 2018 Separate project for closure
Meeting with GP Practice Jan’18
Meeting with Shaw re. staffing Jan’18
Meeting with Commissioners Jan’18
Urgent Care Project Update– December 2017

RED2GREEN (COMMUNITY)
PROJECT
A quality of care we would want for
ourselves, our families and our friends

Red2Green (Community)Objectives
To identity added value in a patients journey and support more effective discharge
Introduction of Red2Green principles across all wards and units by September 2017
Ensure ownership and sustainability of principles through embedding it as ‘Business as Usual’
Deliverables/Measures
Implement roll out by September 2017
Daily huddles by each ward reviews Red2Green data
Daily constraint recording at each ward and escalation process in place
Weekly constraint trend capture and escalation to Divisional Director
Implement Red2Green Dashboard on EPR
Organisational ownership of the issues preventing discharge – actions required and feedback to local teams put in place

Red2Green (Community)
Project RAG Status
Risks/Issues Plans Overall Path to green
On track
Achievements this period
• Continued running at all community Hospital sites• Data collection and sharing in place• Development plan in place following ECIP review• Admin support in place to support data collection and action log and
plans to improve process• Weekly divisional constraints reporting• Monthly constraints reporting to AEDB and UCPB
Actions for next period
• Increased visibility at all sites• Cultural and Clinical Development plan for Community Hospitals• Refresh of Training• Wider circulation of constraints• Strategic escalation of continuing constraints inc. out of county
placements
Decisions required/ Project Commentary
1. There is a small budget associated with this project (linked to regional funding) – equipment purchased2. Need to work with Acute Red2Green project to enable EPR data collection
Urgent Care Programme – December 2017
Key Risks and Issues Impact Mitigation
• Staff engagement M • Refreshed engagement sessions planned with support from regional leads including therapy engagement
• Limited utilisation of data M • To implement electronic collection of red data and circulation to division
• Influence to resistant strategic constraints M • Executive support to cross organisational engagement
Project Lead
David Farnsworth

Red2Green (Community)
Key Milestones
Milestone Expected Delivery Date
Status RAG Commentary
Data reporting to Division Sept. 2017 Complete - ongoing
Monthly reporting to AEDB/UCPB October 2017 Complete
Refocus on programme as part of Perfect Week
January 2018 Planning during Dec. as part of preparation for Perfect Week
Provision of constraint reporting into EPR March 2018 Need to link in the Acute Red2Green project to avoid duplication
External review of project from ECIP April 2018 Dependant on capacity of ECIP team
Business as Usual May 2018 Will depend on ECIP review
Urgent Care Project Update– December 2017