urgent and emergency care review - nhs...
TRANSCRIPT

Urgent and Emergency Care ReviewProgress Update & Urgent Care Network Development
Keith WillettNHS Confederation 2014
If its really
seriousI want
specialist care
Treat me as close to my home as possible please
Help me to help myself and not bother the NHS
If only they could talk to my GP?

THE REVIEW’S VISION …..
For those people with urgent but non-life threatening needs:
• We must provide highly responsive, effective and personalised services outside of hospital, and
• Deliver care in or as close to people’s homes as possible, minimising disruption and inconvenience for patients and their families
For those people with more serious or life threatening emergency needs:
• We should ensure they are treated in centres with the very best expertise and facilities in order to maximise their chances of survival and a good recovery

Current provision of urgent and emergency care services
3
>100 million calls or visits to urgent and emergency services annually:
• 438 million health-related visits to pharmacies (2008/09)Self-care and self
management
• 24 million calls to NHS• urgent and emergency care telephone servicesTelephone care
• 300 million consultations in general practice (20010/11)Face to face care• 7 million emergency ambulance journeys999 services• 14.9 million attendances at major / specialty A&E
departments (2012/13)• 6.9 million attendances at Minor Injury Units, Walk in Centres etc (2013/13)
A&E departments
• 5.3 million emergency admissions to England’s hospitals (2012/13) Emergency admissions

Helping people help themselves
Self care:• Better and easily accessible information about self-treatment options– patient and specialist groups, NHS Choices, pharmacies
• Accelerated development of advance care planning
• Right advice or treatment first time - enhanced NHS 111 - the “smart call” to make:• Improve patient information for call responders (SCR, care plan)• Comprehensive Directory of Services• Improve levels of clinical input (mental and dental heath, pharmacy) • Booking systems for GPs, into UCC or A&E, dentist, pharmacy
4

Highly responsive urgent care service close to home, outside of hospital
5
• Faster, convenient, enhanced service:
• Same day, every day access to general practitioners, primary care and community services
• Harness the skills and accessibility of community pharmacy
• Develop 999 ambulances so they become mobile urgent community treatment services, not just urgent transport services
• 24/7 clinical decision-support for GPs, paramedics, community teams from (hospital) specialists – no decision in isolation
• Support the co-location of community-based urgent care services in coordinated Urgent Care Centres.

Serious and life threatening conditions – expertise and facilities
6
• Two levels of hospital based emergency centres• Emergency Centres* - capable of assessing and initiating treatment for
all patients
• Specialist (Major) Emergency Centres* - 40-70 larger units, capable of assessing and initiating treatment for all patients, and providing a range of specialist services (direct, transfer or bypass).
• Emergency Care Networks
• Connecting all services together into a cohesive network so the overall system becomes more than just the sum of its parts
• Strategic and Operational

The new system
7

Progress update • Second phase of the Review: Aims to convert the work done so
far into a national framework to guide commissioning of UEC services
• Delivery Group of experts from across UEC system have been working to describe the key national products to deliver the outcomes set out in the Stage 1 Report – primacy to out-of-hospital
• Stage 1 Report recommended development of Urgent Care Networks, and designation/standards for Urgent Care Centres, Emergency Centres and Specialist (Major) Emergency Centres within those networks and for ambulance services. Currently developing those guidance
…….. would like contributions on the initial ideas
8

Progress update
9
• Continue to “build in public”
• 8 Work Programmes:
• WHOLE SYSTEM PLANNING AND PAYMENT, COMMISSIONING AND ACCOUNTABILITY
• PRIMARY CARE ACCESS – NHSE strategy• 111 service specification and standards• DATA, INFORMATION AND CARE PLANNING• COMMUNITY PHARMACIES – Call for Action• EMERGENCY DEPARTMENTS and EMERGENCY
CARE NETWORKS• AMBULANCE TREATMENT SERVICE• WORKFORCE (HEE)
ITERATIVE

Primary and Community Care
• Provision of primary and community services must be addressed at the same time as the development of Urgent Care Networks, and the designation within them, through a unified and coordinated approach. NHSE Primary Care strategy, GP contract
• UEC focus shift: hospital supported in community • Through development and coordination of exiting
services, particularly in primary and community care, to provide a clear and constant offer underpinned by established service specifications for each component, and agreed pathways of care that support effective patient flow.
10

NHS 111• Enhanced 111 service: Smart call to make, helping people get the right advice
or treatment in the right place, first time. This service will:
• Be an integral part of the Urgent Care Network
• Have knowledge about you and your medical problems, so the staff advising you can help you make the best decisions;
• Allow you to speak directly to a wider range of professionals (e.g. a nurse, doctor, paramedic, member of the mental health team, pharmacist or other healthcare professional);
• If needed, directly book you an appointment at whichever urgent or emergency care service can deal with your problem, as close to home as possible;
• Still provide you with an immediate emergency response if your problem is more serious, with direct links to the 999 ambulance service, and the enhanced ability to book appointments at Emergency Centres.
11

Ambulance Services• Transport Treatment: Community-based provider of mobile urgent and
emergency healthcare, fully integrated within Urgent Care Networks. Principles to underpin this transformation would include:
• Clear emphasis on supported treatment in community settings
• Single consistent triage system, DoS and universal referral rights
• Successful “hear and treat” - requires closer integration with 111, timely access to relevant patient information and care plans, support of interdisciplinary clinical hub
• “see and treat”, inter-disciplinary working across traditional organisational and professional boundaries, with guaranteed timely access to primary care, mental health provision, social care and specialist clinical advice 24/7
• Development of the ambulance workforce, education programmescoupled with changes to organisational culture, will be essential to long-term success
12

Urgent Care Networks• Networks would focus on:
• effective, joined-up pathways of care across boundaries for physical and mental health irrespective of entry portal
• all patients managed to agreed pathways mutual trust in system
• no clinical decision made in isolation
• Networks would function at two levels:
1. Strategic Urgent Care Networks would operate over larger areas and populations encompassing specialist provision, and bring together all relevant stakeholders to plan, oversee and monitor network performance
2. Operational Urgent Care Networks would describe local communities of clinicians who work together to achieve the best outcomes for patients within the urgent care system. Several Operational Networks will exist within one Strategic Network.
13

Urgent Care Centres
• Community-based primary care facilities providing access to urgent care for a local population.
• To encompass Walk-in Centres, Minor Injuries Units, “Darzi” Centres etc, including those currently designated as “Type 3 A&E Departments”.
• A consistent nomenclature should be accompanied by a consistent service, so that patients are clear about what they can expect from all Urgent Care Centres
• To achieve this it is suggested that two important principles underpin the development of Urgent Care Centres:
• access to a full range of urgent care services
• 24/7 access to the Urgent Care Network
14

Emergency Centres (hospital)• Hospital based facilities able to receive a full range of emergency patients,
of all ages, and which provide for the reception, resus, diagnosis and onward referral
• Would include an Emergency Department, which is under the continuous supervision of one or more consultants in Emergency Medicine, who are not necessarily continuously present, but have clinical accountability for the care delivered in that ED.
• ECs would contain some inpatient facilities (hospital beds), as well as a range of supporting services and outpatients
• In rural areas ECs would be the initial receiving destination for almost all emergency and ambulance patients.
• In more urban environments, ambulance staff may bypass ECs in favour of Specialist (Major) Emergency Centres when the patient has identified specialist needs, and the increase in journey time is clinically justified.
15

Specialist (Major) Emergency Centres
• Would have all the features of an Emergency Centre, but also include specialist facilities that receive patients from ECs, or directly from an ambulance which has bypassed an EC.
• Concentration of specialist expertise, and services which are likely to fall within the remit of specialist commissioning. Provide support and coordination to the whole Network working in partnership with the other system components to ensure access to specialist care in a timely way
• EDs, integral to SECs, would provide consultant presence over extended hours, immediate access to enhanced diagnostics, such as CT and MRI scanning and interventional radiology, and a wider range of facilities.
16

Emergency Centres & Specialist (Major) Emergency Centres
• Consider the designation and likely service configuration in ECs and SECs: Do our initial ideas look right?
• How will SECs link to specialist commissioning plans?
• Designation: How much will be for local CCGs? What is needed nationally to support designation?
17

STRATEGIC URGENT CARE NETWORK:CCGs / NHS ENGLAND / UCWG / HEALTH AND WELL‐BEING BOARD / LOCAL AUTHORITY /
PUBLIC HEALTH / HEALTHWATCH
NETWORK CONFIGURATION
OPERATIONAL URGENT CARE NETWORKS
ASSURANCE PROCESS
SCN ENABLING
PROVIDER(S)
HOST (LEAD) COMMISSIONER
CLINICAL SENATE
PATHWAY EVALUATION:PROMS, PREMS
AND F&F
NETWORK AIM = QUALITY AND CONSISTENCY
PUBLIC‐FRIENDLY VERSION OF THIS NECESSARY: WHAT CAN YOU EXPECT? WHERE SHOULD YOU GO?
AHSN PRIMARY CARE CLINICIAN
CLINICAL ADVISORY GROUP
SECONDARY CARE CLINICIAN(S)
Providerfeedback
Pathwayreview
Network Structure
Accountability
Clinical Governance
Evaluation
Key
Commission Providers or Pathways
CONSIDER OTHER MODELS: E.G. ALLIANCE COMMISSIONING, PARTNERSHIP OR SINGLE LEAD

Strategic and Operational Urgent Care Networks
• Do our initial ideas about governance and accountability look right?
• If not:• Where should accountability lie?• How will network governance work?• How will networks function in practice?• What is needed nationally to make them happen?
• System metrics: i) relevance to patient
ii) place and timeliness of assessment
iii) place and timeliness of definitive care
19

Timelines and Next Steps
20
For 2014/15:
• Update on Urgent and Emergency Care Review (June 2014)
• Working with Urgent Care Working Groups, CCG and Area Teams as they develop and deliver against their 2 year operational and 5 year strategic plans (roadshows during June-Sept 2014)
• Working through the NHS Commissioning Assembly to co-produce commissioning guidance and specifications (throughout 2014/15)
• Release guidance, standards and outcome metrics for Commissioners regarding UEC Networks, Urgent Care Centres, Emergency Centres and Specialist (Major) Emergency Centres and clinical models and for Ambulance Services (Autumn 2014)
For longer term changes (e.g. workforce, configuration of services, etc) we anticipate that it will take 3-5 years to enact the major transformational change envisaged by the Review.

DELIVERY PLAN – big ticket itemsBetter support for self care
Promote effective self‐care 1. Develop self‐care resources2. Guidance produced on marketing campaigns (so that messages are same across the country so far as is practicable)3. Signposting/linkage to LTC third sector partners, etc, for advice and support
Introduction and roll‐out of advanced care planning
1. Development of national care plan template and tools to support delivery of 15m care plans by 2015
Right advice right place first time
Integrate pharmacy into the UEC system
2. Changes to national pharmacy contract to introduce minor ailments service etc.
Improve clinical input to NHS 111 and ambulance services ‐more ‘hear and treat’
1. Development of new national specification for NHS 111 to include recommended clinical input, and extended range of services for booking, including guidance on reprocurement2. Development of guidance on ambulance models to include support required in control room
Integrate system by improving referral rights through UEC system NHS 111 and NHS ambulance services, pharmacy, etc
1. Ensure national 111 specification and procurement strategy enable local referral rights2. Development of guidance on improving referral rights across UEC system
Enhance the DOS to be real time and accurate commissioning tool
1. DOS development work: Health and Social Care content

DELIVERY PLAN – big ticket itemsHighly responsive out of hospital services
Develop the ambulance service model to offer more treatment on the scene
1. Development of Guidance on models for treatment on scene by ambulance service2. HEE work on paramedic Development and training3. Enable GPs to offer support to ambulance and A&E (in enhanced service to go live from April 14)
Develop community pharmacy facilities to wider range of services
1. Principles for extended pharmacy offer, backed up by contractual changes
Successful models of care for improved primary care access
- in and out of hours
1. Principles for improved primary care access 24/7, accompanied by necessary national contractual incentives2. Headline specification for local urgent care facilities
Successful models of care for improved community services - in and out of hours
1. Principles for improved community services (in and out of hours) accompanied by necessary national contractual incentives2. Headline specification for local urgent care facilities
7/7 access to hospital specialistadvice to PC and key OOH services
1. Hospital specialists: who should be available, appropriate response times – academy/colleges/specialist (NHSE)
Specialistcentres to maximise recovery
Designation of major emergency centre and emergency centres
1. Develop national specifications in conjunction with clinical stakeholders2. Determine process for accreditation and designation of facilities
Matching hospital resources to patient acuity and complexity
1. Develop appropriate tools and guidance on flow
DELIVERY PLAN – big ticket items
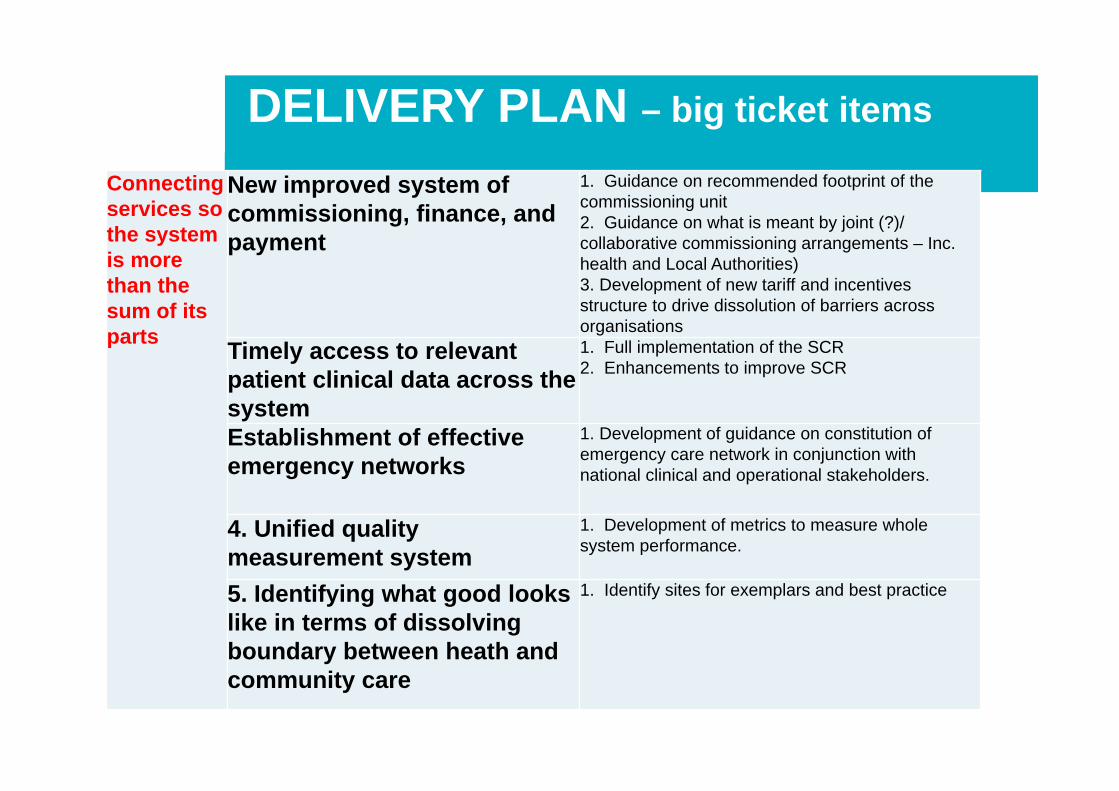
Connecting services so the system is more than the sum of its parts
New improved system of commissioning, finance, and payment
1. Guidance on recommended footprint of the commissioning unit2. Guidance on what is meant by joint (?)/ collaborative commissioning arrangements – Inc. health and Local Authorities)3. Development of new tariff and incentives structure to drive dissolution of barriers across organisations
Timely access to relevant patient clinical data across the system
1. Full implementation of the SCR2. Enhancements to improve SCR
Establishment of effective emergency networks
1. Development of guidance on constitution of emergency care network in conjunction with national clinical and operational stakeholders.
4. Unified quality measurement system
1. Development of metrics to measure whole system performance.
5. Identifying what good looks like in terms of dissolving boundary between heath and community care
1. Identify sites for exemplars and best practice