update/le point - caninerabiesblueprint.org point economics of humanand canine rabies elimination:...
TRANSCRIPT
Update/Le point
Economics of human and canine rabies elimination:guidelines for programme orientation*K. Bogel' & F.-X. Meslin2
Analysis of the present situation in canine-rabies-infected countries shows that in most cases the levels ofactivities for controlling the disease in man and in dogs are far too low to prevent human deaths due torabies and to eliminate the disease in the dog population. This article compares the two major orientationsof a rabies control programme, i.e., prevention of the disease in man by intensifying and modernizing post-exposure treatment (strategy A) and canine rabies elimination by controlling the disease in the animalreservoir (strategy B). The operation of both strategies (A+ B) together is also analysed.
Based on the available data and assumptions for calculations of the costs, the results show that whenthe strategies are applied independently of each other, the annual cost of strategy B amounts to 25-56% ofthat of strategy A. When the two strategies are applied together, the actual annual spending related to theimplementation of A + B becomes less than that of strategy A alone as from the fifth year followingprogramme initiation. The sensitivity of the results was tested against selected fluctuations in theassumptions. An estimation of the costs of control activities per avoided death, according to the strategyapplied, is also given.
In countries where resources allocated to rabies control are inadequate in both the health andveterinary sectors, the comparison in costs and effectiveness of the two programme strategies for rabieselimination strongly suggests that consideration should be given to a national programme of dog rabieselimination. On the other hand, for obvious ethical reasons, if attention is paid to improvement of post-exposure treatment, then the national authorities should consider a planning horizon close to 15 years.
IntroductionWith the exception of some areas in the SouthPacific, rabies persists as a major public healthhazard in many countries throughout the world.Global estimates show that about 35 000 persons diefrom rabies and about 3.5 million receive post-exposure treatment (PET) every year. Almost all thereported deaths occur in the developing countries
* A French translation of this article will appear in a later issue ofthe Bulletin.' Chief, Veterinary Public Health, Division of CommunicableDiseases, World Health Organization, 1211 Geneva 27, Switzer-land. Requests for reprints should be sent to this author.2 Scientist, Veterinary Public Health, Division of CommunicableDiseases, WHO.
Reprint No. 5073
and most cases of treatment (89.5%) are also there(1).
According to the FAO/WHO/OIE AnimalHealth Yearbook for 1986, 87 countries andterritories, with a total population of about 2.4billion, are infected by canine rabies. Even today,most developing countries concentrate the essentialpart of their resources allocated to rabies control onpost-exposure treatment. In these countries, in spiteof an average of 800 to 900 persons annually treatedper million inhabitants, the rate of human deaths dueto rabies is very close to 5 per million inhabitants (2).At the same time, vaccination coverage of the dogpopulation hardly exceeds 15%, which is far too lowfor eliminating the disease in dogs. National statisticsindicate that such levels of activity do not lead to amarked reduction of human rabies cases or of thenumber of PETs.
Bulletin of the World Health Organization, 66 (3): 281-291 (1990) ©D World Health Organization 190 281

K. Bogel & F.-X. Mesiln
To improve this situation all governments desir-ing to embark on an effective human and caninerabies control programme should first define theirpolicy on that issue. This paper provides comparativedata, both financial and technical, on the two majororientations of such a programme. It should serve asguidelines for health policy-makers and help them intheir decision-making process. The two programmeorientations under investigation are specified asfollows:
* Strategy A. Prevention of the disease in man byintensifying and modernizing post-exposure treat-ment.
This entails maximum coverage of the humanpopulation by PET. This may be done through anextended network of vaccination centres providedwith appropriate storage conditions and stocked withhighly potent human vaccines as well as rabiesimmunoglobulin (3). Once established, this high vac-cination coverage must be continued by the nationalhealth authorities if no canine rabies eliminationactivities are conducted simultaneously.
* Strategy B. Canine rabies elimination by control-ling the disease in the animal reservoir.
This entails countrywide immunization of dogsthrough mass vaccination campaigns or continuingvaccination schemes and adequate dog populationmanagement.'
Basic data
Strengthened PET delivery and human death rateIn Guayaquil (Ecuador) where the health infrastruc-ture and surveillance system are functioning well, thehigh number of PETs delivered in 1983 and 1984 (i.e.,about 2000 per million inhabitants)' did not preventthe annual occurrence of 4 human deaths per millioninhabitants. An evaluation in eight countries (Algeria,Brazil, El Salvador, Honduras, Sudan, Thailand,Tunisia and Turkey), with well organized reportingsystems for human rabies exposure and care, showedabout 2000 PETs administered and 2.7 humandeaths due to rabies reported per million inhabitants(1).
' Report of a WHO Consultation on Dog Ecology Studies Relatedto Rabies Control. Geneva, 1988 (unpublished document WHO/Rab.Res./88.25, 1988).Provincial HeaV Adminlsletdon of Guayas. Monthly reports,
Zoonoses Section. Guayaquil, Ecuador, 1983, 1984 (in Spanish).
Dog rabies control programme and human healthProgrammes being coordinated by WHO in threedeveloping countries with human populations rang-ing from 7 to 16 million show that the number ofhuman deaths may decrease rapidly when approp-riate control measures are taken to stop circulationof the virus among the canine population. In SriLanka the average number of human deaths reportedfor the whole country was halved between the period1980-83 and the four years following the initiationin 1984 of the new "Accelerated Intensive RabiesControl Programme",' whilst in Tunisia the annualaverage of 10 deaths from rabies in 1978-82 (prior tothe launching of the national programme) decreasedto 4 during the period 1983-87 (4).d In Guayaquil,Ecuador, where the rabies control project wasinitiated in September 1985, no human rabies caseshave been reported since May 1986.'
Dog population and dog oacessibilItyIn general, North American and European countriesreport a dog/inhabitant ratio of between 1:10 and1:6;' data available from 14 developing countries ofAfrica, Asia, South and Central America give anaverage of 1:8.'
The accessibility of dogs, i.e., the proportionof dogs which can be vaccinated and those whichare unsupervised, has been studied during WHO-coordinated research projects on dog populationsin project areas of Asia, Africa and Latin America.These studies have shown the following.
-Firstly, the proportion of dogs not associated withparticular household(s) and person(s) is less than10% of the total dog population and these animalsdo not seem to play a significant role in thereproductivity of this population.
-Secondly, 70-75% of dogs are accessible tocontrol measures, particularly vaccination, if theapproach is adapted to the dog-man relationshipand the community is fully involved in the rabieselimination programme, i.e., veterinary policingmeasures should be largely replaced or supplemen-
'G.L.A. Colonne. Statistical profile of rabies In Sri Lanka.Colombo, Ministry of Health, 1988.d Mllnstire de l'Agrlculture, Direction de Is Production Animale.Bulletin 6pid6miologique trimestriel de la rage en Tunisie, Vol. 1,No. 1-4, 1986; Vol. 2, No. 5-8, 1987 (in French).' Provncal Healih Adminisradon of Quay". [Evaluation of aPilot Rabies Control Programme in the city of Guayaquil.]Guayaquil, Ecuador, 1985-86, 1986-87 (in Spanish).' The dog population in urban and rural areas. In: Guidelines fordog rabies control. Geneva, 1983 (unpublished WHO documentVPH/83.43), pp. 2.1-2.27.
282 WHO Bulletin OMS. Vol 68 1990.

Economis of human and canine rabies elimination
ted by active community participation in rabiescontrol activities.
-Thirdly, the density of a dog population cannotsignificantly be reduced by dog catching and kill-ing activities. In general, programmes to reduce thedog population do not remove more than 3-5% ofthe dogs annually, so that the influence on thepopulation density is insignificant if not counter-productive owing to increased mobility and con-tact rates of the dogs and rejuvenation throughincreased reproductivity. Unless specific ecologicalsituations indicate the contrary, dog populationcontrol should not be achieved by controlling straydogs but rather by promoting responsible dogownership.9
Vaccine prices and administration costsHuman vacines. Few data are available concerningadministration costs. According to D.N. Regmi (per-sonal communication, 1985), vaccine administrationcosts in Nepal were estimated at about US$ 0.80 perinjection, including personnel, syringes, needles, andcold chain facilities. Therefore, the delivery costmight be at least $1 per injection in developingcountries. Several types of safe and highly potentvaccines are now available, e.g., human diploid-cellvaccine (HDCV), highly purified duck-embryo vac-cine (DEV), purified chick-embryo cell vaccine(PCEC) and Vero cell rabies vaccine (5). Vaccineprices (FOB) vary from $7.85 to $16.00 per dose;approximately 25% should be added for packing,freight and insurance (PFI) (costing for human rabiesvaccines given by Supply Services, WHO, Geneva,May 1988). Considering the actual decreasing trendin the prices of the human antirabies vaccine, a meanprice of US$ 10 (CIF) will be used in the followingcalculations. Therefore, cost of a complete 5-doseregimen (plus administration costs) will be US$ 55.
Veterinary vccines. In Thailand and Tunisia vaccineadministration costs per dose range from US$ 0.52 to0.95 (see Table 1). In Sri Lanka, in 1985, a similarcalculation gave a value of approximately $0.63. Thedifferences between Asian and north African coun-tries are mainly due to the cost of manpower (seesalary component of Table 1). The upper limit of theabove range ($0.95) will be used in the following.
The vaccines applied in these cost estimates wereimported liquid, adjuvanted products containing atleast 2 I.U. per dose. A single inoculation of thisvaccine should provide an immunity for at least 2years (6). These vaccines cost between $0.27 and
2 See footnote a on page 282.
Table 1: Costs of vaccine applikatlon In dogs
Bangkok (Thailand)" Nabeul (Tunisia)b(36 668 dogs) (53 534 dogs)
(USS) (US$)
Salary 7480.40 41 598.00Vehicles (cost peryear considering a5-year amortization) 7143.90 6234.50
Petrol 3791.90Public educationand Information 769.20 687.90
Vaccinationcertificates - 1304.30
Miscellaneousexpenses - 776.40
Material forvaccination - 256.20
Total 19 184.90 50 857.30
Cost per dog 0.52 0.95
' Data obtained from Dr Ch. Kulganchewin, Bangkok Metro-politan Health Centre, Bangkok.b In: B/lan des trols premieres ann6es d'ex6cution duProgramme national de lutte contre la rage en Tunlae (1982-83-84). Tunis, Ministere de l'Agriculture, Direction de la ProductionAnimale, August 1984.
$0.43 per dose (including packing, freight andinsurance) (costing for canine rabies vaccines givenby Supply Services, WHO, Geneva, June 1988). Thisgives an average price per dose of $0.35.
The total cost per vaccinated dog will thereforebe US$ 1.30.
Immunoglobulin prkes and admInIstratIon costs
The price of rabies immunoglobulin (RIG) of humanorigin (HRIG) varies from US$ 80 to $ 275 (FOB) fora patient weighing 50kg (20 I.U. per kg of bodyweight) (costing for rabies immunoglobulins given bySupply Services, WHO, Geneva, October 1987). Thisgives a mean price of $160 (PFI and delivery costs of$ 2 included). RIG of equine origin (ERIG) (purified)is available at a lower price, i.e., $50 total cost for a50 kg patient (40 I.U. per kg of body weight). Accord-ing to the type of RIG applied, the cost of associatedpassive and active immunization (RIG and vaccine)for a patient of 50kg would range from $ 105 to$ 215.
Total costs for post-exposure treatment havebeen kept to a minimum as only few data are avail-able for a better evaluation. However, when cost oftransportation of a patient to the vaccination centre,as well as costs of accommodation on the spot, plusjob opportunities lost are included, the costs of thevaccine doses applied represent only 30% of the totalcost of the treatment as found by S. Chutivongse inThailand .(personal communication, 1989).
WHO Bulletin OMS. Vol 68 1990.

K. Bogel & F.-X. Moslin
During a recent WHO Consultation onimprovement of rabies post-exposure treatment' theparticipants proposed new definitions to characterizethe nature of the exposure to rabies. Exposure, whichwould call for vaccine and serum application, wasdefined as any bite or scratch penetrating the skin orany lick on the mucous membrane. Under suchconditions it is assumed that 50% of the patientscoming to a rabies treatment centre in most countriesinfected with canine rabies should receive both vac-cine and serum. This percentage will be used in thecalculations given below.
Model conditions
Surveillance system
Both strategies A and B require an efficient rabiessurveillance system. Control of rabies in the caninereservoir may be achieved during the first phase ofprogramme implementation with minimum epidemio-logical surveillance. The latter would, however, haveto be strengthened considerably for the detection andcontrol of residual foci of infection. Obviously, inten-sive PET will lead to satisfactory results if associatedwith highly efficient surveillance of the disease inanimals. The costs related to epidemiological sur-veillance are not included in the following calcula-tions since laboratory and specimen collectionservices exist in all countries and will only requirestrengthening according to the efficiency level to bereached, irrespective of the control componentswhich are compared below.
Status of health Infrastructure
It is assumed that, at the time of programmeimplementation:
-the medical services are functioning and necessaryhealth infrastructures have been established;
-the veterinary services are well organized and needonly to set up appropriate animal vaccinationservices.
ParametersThe following parameters are used:
(i) Dog/inhabitant ratio: 1/8.(ii) PET/inhabitant ratio: 200/100000 before
effective canine rabies control is initiated.
h Report of a WHO Consultation on Rabies (European Bat Rabies,Postexposure Treatment and Potency Testing for Rabies Vac-cines). Essen, 1988 (unpublished document WHO/Rab.Res./88.30,Rev.1).
(iii) Cost of a vaccination regimen (5 doses) with-out immunoglobulin: US$ 55.
(iv) Proportion of patients receiving HRIG orERIG in addition to vaccine: 50%.
(v) Cost of immunoglobulin and its application:US$ 160 for HRIG, and US$ 50 for ERIG.
(vi) Dog vaccination requirements. Vaccinationcampaigns using canine rabies vaccines protecting forat least two years should reach 75% of the total dogpopulation at risk every two years. In intermediateyears, dogs that have since grown up or have not yetbeen vaccinated will be scheduled for vaccination(about 25% of the total population). Thus, onaverage about 50% of the total dog population willhave to be vaccinated annually.
(vii) Dog accessibility: 80%.(viii) Cost of dog removal and elimination. Re-
moval and elimination of dogs are considered feasibleand reasonable in rabies control only for enforcementof certain veterinary measures but not for reduction ofthe dog population density. In general, less than 5%of the dog population are affected each year byremoval programmes. It is not recommended toincrease this level.' It is assumed that the costs ofvaccination or removal of a dog are of the same orderof magnitude, so that these two control measurescannot be distinguished in the model.
(ix) Effectiveness of a dog rabies eliminationprogramme on the number of human deaths and PETdemand and delivery. From the various canine rabiescontrol projects coordinated by WHO, it seems real-istic to assume that, in a given area, the number ofhuman deaths would decrease quickly and reach zerolevel after 2-3 years, provided that a well plannedcomprehensive canine rabies control programme iscorrectly implemented. As observed in countrieswhere effective rabies control activities are carriedout, the number of PET increases during the 2-3years following the first dog mass vaccination cam-paign, because of increased public awareness of therabies threat, and then decreases. An increase of 25%of the PET demand over the first 3 years has beentaken into consideration in this model. The decreaseshould be progressive. Routine PET delivery servicesshould remain available until confirmation of therabies-free status of the area is secured. This calls forthe operation of a very effective surveillance system.It is assumed that 50% of the initial PET level (i.e.,1000 PET per 1 million) may be reached during the5th year following the first dog vaccination cam-paign, and a minimum number of PET (5% of initiallevel) may be permanently delivered each year as
' See footnote a on page 282.
284 WHO Bulletin OMS. Vol 68 1990.

Economics of human and canine rabies elimination
from the 7th year (people exposed in border zonesand overseas).
(x) Phases of a national canine rabies controlprogramme. For realistic planning and smoothimplemention of a programme, a decision should bemade on the size of the initial area to be covered bymass vaccination, and on plans for the expansion ofcontrol activities to other parts of the country. Inmost countries, the infrastructure of veterinary andcommunity services will permit initiation of theprogramme in areas of 1 million inhabitants (i.e.,125 000 dogs). Systematic programme developmentmay begin with operational research covering 20 000to 30 000 dogs. Following initial trials such areasshould, however, be sufficiently large to recognize arabies-free situation and thus allow for the reductionof the rate of PET. The programme expansion willlargely depend upon the availability of trained staffand dog rabies vaccine.
In each area the sequence of vaccination activitiesis as follows:
-An attack phase of two years aiming at establish-ing coverage in the dog population through crashmass vaccination campaigns (see costs for dogvaccination on page 283).
-A consolidation phase of four years during whichthe same immunization coverage of 75% (as des-cribed for the attack phase) is maintained. Themethodology may be different from that of theattack phase (e.g., dog vaccinations evenly dis-tributed over the year). In addition, this phaseshould ensure the elimination of the residual foci ofinfection by active search and special control acti-vities wherever needed. This is particularly neces-sary if the rabies elimination zone is borderingon areas still infected or in earlier phases ofprogramme development.
-The maintenance phase, which should definitelyensure the canine rabies-free status and be charac-terized by (a) intensive surveillance, (b) outbreakpreparedness, and (c) continuing vaccination of aproportion of the dog population which is atparticular risk (national borders, internationaltravellers). This proportion of the dog populationis assumed to be 20%.
The actual annual costs of PET administrationin an area of 100 000 inhabitants and of dog rabieselimination programmes over a period of 10 years areshown in Fig. 1 and 2, respectively. The evolution ofthe annual costs of a PET programme when a dograbies elimination programme is launched in parallelis shown in Fig. 3.
Fig. 1. Cost of post-exposure treatment programmesaccording to the percentage of treated cases receivingvaccine and equine rabies Immunoglobulin (ERIG) orhuman rabies Immunoglobulin (HRIG), per 100 000Inhabitants (for assumptions, see p. 283).
30
28 27 000
26-
24-
22-
-20 19000
° 18 _
1616~ /16 Vaccine+HRIG
o14012
'0 -1T0 Vaccine + ERiG8
6-
2
00 10 25 50% of treated cases receiving vaccine and immunoglobulin
Control strategies: results
Comparison of the costs of the two strategiesThe objective of a canine rabies elimination pro-gramme is the elimination of human rabies, therebycontrolling the disease in the animal reservoir. Thisobjective cannot be met by an intensified PET pro-gramme as described in this paper. Ranking analysisof mortality data collected in areas with negligibleimpact from dog vaccination shows that between6 and 15 human cases per million inhabi-tants are recorded annually. The same techniqueapplied to data on post-exposure treatment (PET)shows that areas with a relatively high rate of PETrecord approximately 3 deaths per million inhabi-tants annually.' Therefore, an intensified PETprogramme may lower the mortality level from an
X Motschwiller, E. [Epidemiologic and economic aspects of can-ine rabies and its control in Third World countries.] Inauguraldissertation, Veterinary Faculty of Ludwig-Maximillians Univer-sity, Munich, 1988, pp. 24 and 31 (in German).
WHO Bulletin OMS. Vol 68 1990. 285
K. Bogel & F.-X. Meslin
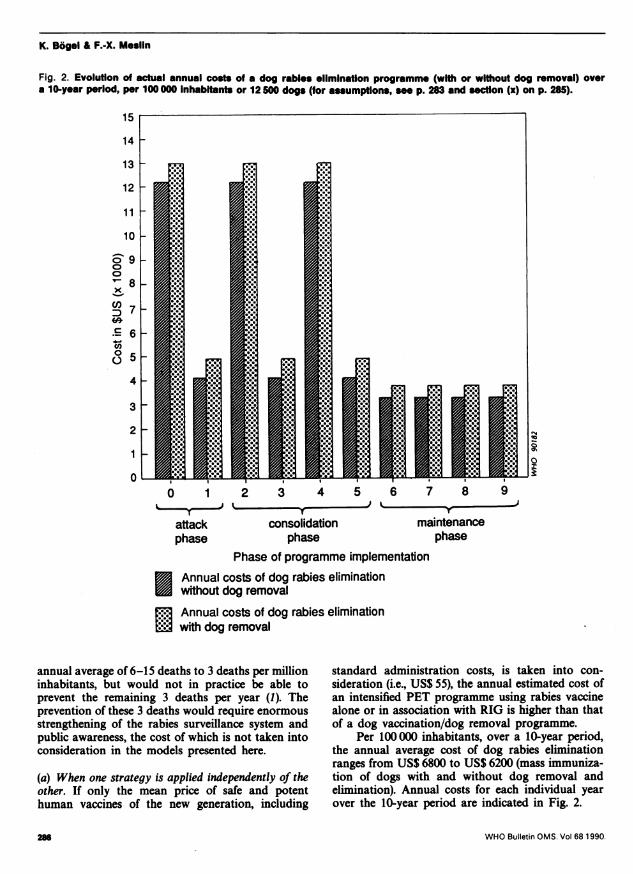
Fig. 2. Evolution of actual annual costs of a dog rabies elimination programme (with or without dog removal) overa 10-year period, per 100 000 Inhabitants or 12 50 dogs (for assumptions, se p. 283 and section (x) on p. 285).
15
14
13
12
11
10
o 9
8x
D7C600- 6o 5
0 1 2 3 4 5 6 7 8 9i T T
attack consolidation maintenancephase phase phase
Phase of programme implementation* Annual costs of dog rabies elimination
without dog removal
3 Annual costs of dog rabies eliminationB with dog removal
annual average of 6-15 deaths to 3 deaths per millioninhabitants, but would not in practice be able toprevent the remaining 3 deaths per year (1). Theprevention of these 3 deaths would require enormousstrengthening of the rabies surveillance system andpublic awareness, the cost of which is not taken intoconsideration in the models presented here.
(a) When one strategy is applied independently of theother. If only the mean price of safe and potenthuman vaccines of the new generation, including
standard administration costs, is taken into con-sideration (i.e., US$ 55), the annual estimated cost ofan intensified PET programme using rabies vaccinealone or in association with RIG is higher than thatof a dog vaccination/dog removal programme.
Per 100 000 inhabitants, over a 10-year period,the annual average cost of dog rabies eliminationranges from US$ 6800 to US$ 6200 (mass immuniza-tion of dogs with and without dog removal andelimination). Annual costs for each individual yearover the 10-year period are indicated in Fig. 2.
WHO Bulletin OMS. Vol 68 1990.
e4_u
a
286

Economics of human and canine rabies elimination
Fig. 3. Evolution of the annual costs of a post-exposure treatment programme launched In parallel with a dog rabieseliminatlon programme, per 100 000 Inhabitants (for assumpftons, se p. 283 and section (Ix) on p. 284).
0 1 2 3 4 5 6 7 8 9Years
PET programme with HRIG beingadministered in 50% of treated cases
j3 PET programme with ERIG being3 administered in 50% of treated cases
By comparison, for an area of 100 000 inhabi-
tants and 200 patients, according to the assumption,the cost range of an intensive PET programme variesfrom US$ 11 000 (modern vaccine alone) toUS$ 27 000 (vaccine and HRIG in 50% of the treatedcases) per year (see Fig. 1). In the absence of effective
canine rabies control measures, these annual costsare assumed to remain stable over the 10-year period.
Comparison of Fig. I and 2 shows that (i) ifhuman vaccines are applied alone, without immuno-globulin, the average annual cost (over 10 years) ofthe dog rabies elimination programme amounts to
WHO Bulletin OMS. Vol 68 1990.
35
30
25
0
o 20C,)x1-cn
*C 15.-4cn00
10
5
0

K. Bogel & F.-X. Meslin
Table 2: Comparison of actual annual cosb of strateglsA+ B versus strategy A alone (per 100 000 InhabItants)
Annual cost of Annual cost ofstrategy (A + B)' strategy Ab
Year (USS) (USS)
0 32 190 16 0001 24 063 16 0002 32 190 16 0003 20 063 16 0004 24190 16 0005 12 063 16 0006 7 250 16 0007 4 050 16 0008 4050 160009 4 050 16 00010 4 050 16 000
Dog rabies elimination +PET (ERIG in 50%).b PET (ERIG in 50%) alone.
about 56% of the cost of the PET programme; and(ii) this average annual cost of the dog rabies elimina-tion programme (without dog removal) amounts to39% of that of an intensive PET programme usingERIG in 50% of the treated cases and to only 23% ofthat of a PET using HRIG in 50% of the treatedcases.
(b) When the two strategies are applied in association.In countries or areas where resources would allowthe strict application of the two strategies, the execu-tion of a dog rabies elimination programme shouldimprove the epidemiological situation and induce adecrease in PET administration in a very progressiveway as described in the assumptions. As can be seenfrom Table 2, the actual annual spending related tothe implementation of an intensified PET pro-gramme using ERIG in 50% of the treated cases andassociated with a dog rabies elimination programme(strategy A + B) will be less than that for a PETprogramme (same characteristics as above) conduc-ted alone as from the 5th year following initiation.However, in view of the additional expenses incurredfrom year 0 to year 4, the accumulated cost of thestrategies A + B will approximately equal that ofstrategy A after 10 years of implementation (seeTable 3).
Discounting these annual flows (using a 10%rate of discount) to produce a net current cost foreach option confirms that the preferred strategy issensitive to the time horizon chosen. If the planninghorizon is less than 16 years, strategy A is less costly.For any larger horizon, A+ B is the preferred option.Fig. 4 shows the flow of the cumulative current costsof strategy A+ B, and strategy A alone.
(c) Sensitivity of the results to assumptions. In view ofthe uncertainty of the assumed parameters, the sen-sitivity of the results given by our model has beentested vis a vis some assumptions made for thecomputation of the individual costs of strategy A andstrategy B.
The sensitivity of the model was tested:
-for strategy A against (i) variations of the per-centage of treated cases receiving ERIG (from50% to 25% and 10%), and (ii) decrease in thecost of a human vaccine dose (from $10 to $8and $4);
-for strategy B against a decrease of the cost ofvaccine administration to dogs (from $0.95 perdog to $0.65).
Table 3: Comparison of the cumulative costs ofstrategies A+ B versus strategy A alone (per 100 000Inhabitants)
Cumulative costs of Cumulative costs ofstrategy (A+ B)" strategy Ab
Year (US$) (US$)
0 32 190 16 0001 56 253 32 0002 88 443 48 0003 108 506 64 0004 132 696 80 0005 144 759 96 0006 152 009 112 0007 156 059 128 0008 160 109 144 0009 164159 160 00010 168 209 176 000
Dog rabies elimination+PET (ERIG in 50%).PET (ERIG in 50%) alone.
The sensitivity of the results to fluctuations inthe assumptions was evaluated by considering theirimpact on the period of time necessary for theaccumulated actual costs of strategy A+ B to equalthose of strategy A applied alone. As shown insection (b) above, this period is 10 years for ourmodel. Any decrease in the costs of strategy A (cost ofstrategy B remaining constant) will lengthen thisperiod. Any decrease in the cost of strategy B (costsof strategy A remaining constant) will shorten thisperiod. The reverse will also be true. It appearsthat variations (increase or decrease) in the costof a strategy by about 1% will change the period(lengthened or shortened time) by approximately onemonth.
For example, a decrease by 27% of the cost ofstrategy B due to a lesser cost of vaccine administra-tion will shorten the time period by about two years
WHO Bulletin OMS. Vol 68 1990.288

Economics of human and canine rabies elimination
Fig. 4. Comparison of cumulative current costs of strategy A versus strategy A+ B, per 100 000 Inhabitants.
150
140
130
12
110
10090.iLL70
60
50
40
30
20
8Years
MMStrategy A alone
or 20% of the time required in our model (see section(b) above), whereas a decrease by 15% of the cost of aPET programme due to the application of ERIG inonly 25% of the treated cases will increase the abovetime period by about one year (11 years instead of10). If variations of similar magnitude moving in thesame direction (decrease or increase) are observed inthe costs of each strategy (for example, PET pro-gramme with ERIG in 10% of the treated cases anddog rabies elimination with a cost per vaccinated dogof only $1), then no change is observed in the aboveperiod of time which remains as 10 years after theyear of implementation.
Number of human deaths avoided and cost peravoided deathThe model conditions described in this paper permitan estimation of the costs of control activities, accor-ding to the strategy applied, in order to avoid one
human death due to rabies. The assumptions used tocalculated this cost are as follows:
(i) Rabies mortality rates prior to the initiation ofcontrol activities are assumed to range from 6 to 15per million inhabitants (see above).
(ii) When a PET programme with a coverage of2000 PET per million is applied in isolation (strategyA), then 3 human deaths are reported annually.
(iii) Rabies vaccination ofdogs (strategy B) aimingat the elimination of the disease is assumed to reducethe disease incidence in man to zero during the thirdyear of programme implementation. During the firsttwo years a death rate due to rabies representing20% of the initial rate is taken into consideration inTable 4.
(iv) When an intensified post-exposure treatmentprogramme is carried out in association with dograbies elimination (strategy A + B), then the incidenceof the disease is expected to reach zero during the
WHO Bulletin OMS. Vol 68 1990.
0
C/)
.600
E Strategy A + B
289

K. Bogel & F.-X. Meslin
Table 4: Coats per avoided deaths
Reduction inannual number Mean annual Cost per
Strategy/ Annual average cost of human deaths number of deathcontrol of control measure avoided avoidedmeasure (USS) From To deaths (US$)
Strategy A:Intensified PETusing ERIG in 50% oftreated cases (PETcoverage of 2000per million)
Strategy B:Dog rabies elimination(without dog removal)
Strategy A + B:Intensified PET using ERIG
in 50% of treated casesplus dog rabieselimination
160 000
62 000'
164 200'
15 36 3
15 06 Ob
15 0'6 0'
123
14.45.8
14.75.9
13 33053 330
4 30010 690
1117027 830
' During a 10-year programme (see Table 3 and Fig. 2).b A 20% mortality rate will be reported during the first two years of programme implementation.' A 20% mortality rate will be reported during the first year of programme implementation.
second year of project implementation. During thefirst year a death rate equal to 20% of the initial rateis still expected to be reported (see Table 4).
Strategies B and A+ B compare favourably withstrategy A, whether the initial mortality rate is highor moderate. Costs per death avoided in the dograbies elimination programme remain within therange of those of some common health interventions(e.g., for malaria eradication, community watersupply, sanitation).
ConclusionsComparison of the costs and effectiveness of the twoprogramme components for rabies elimination oroptimum PET is largely theoretical in the cost com-putations since no situation exists in which either theone or the other measure is taken alone. However, inrecent years the health services of a number ofcountries have paid considerable attention to rabiesPET in the course of the development of primaryhealth care and public health. Ethical reasons appearto predominate in this process and lead to anexplosive increase in costs, particularly when thegovernments decide to provide, instead of classicalnervous tissue vaccine, the new generation of humanvaccines which are safer and more potent.
On the other hand, the veterinary health servicesare often facing major problems in animal produc-tion due to the absorption of available resources for
mass vaccination programmes against other diseasesin livestock while dog rabies elimination is neglected.It is a general observation that resources are ofteninadequate both for the elimination of rabies in dogsand for the PET service.
However, the results of this analysis stronglysuggest that consideration should be given to anational programme of dog rabies elimination forsimple economic reasons. This appears to be par-ticularly important in countries where at present theallocated resources are inadequate in both the healthand veterinary sectors so that the problem of rabiespersists without a marked improvement in spite ofthe measures taken.
Ethical and economic reasons call for intersec-toral cooperation and in particular the leading role ofthe agriculture/veterinary sector in rabies eliminationsince an intensive PET programme using vaccinealone cannot prevent about 3 human cases of rabiesper million annually or reduce the fear of the diseasein all those who are exposed and treated. Substantialexpenses for PET delivery can and should beavoided.
In some countries it may take 5-10 years, follow-ing the elimination of dog rabies in large areas, beforethe health service can significantly reduce the treat-ment of persons after animal bites. In other countries,rabies surveillance data are regularly assessed by aninterdisciplinary/sectoral rabies or zoonoses commit-tee which also advises on the provision and use ofvaccines and immunoglobulin in humans. Recogni-
WHO Bulletin OMS. Vol 68 1990.29
Economks of human and canine rabies elimination
tion of rabies-free areas, if well identified, can soonreduce the costs for PET services.
This analysis provides convincing arguments forthe adoption of a national intersectoral strategywhich, by concentrating the available resources, willreduce the burden to national budgets and lead toincreased health and an improved infrastructuralservice. In particular, countries which are planning toreplace classical (and unsatisfactory) procedures forhuman post-exposure treatment should choose thepositive cost-effectiveness approach shown in thisanalysis. The results should also encourage researchworkers to continue their efforts to develop cheaperhuman vaccines and immunoglobulins.
References
1. Acha, P.N. & Arambulo III, P.V. History and currentstatus. In: Kuwort, E. et al., ed. Rabies in the tropics,
Proceedings of an international seminar, Tunis 1989.Berlin-Heidelberg, Springer Verlag, 1985, pp. 343-359.
2. Bogel, K. & Moetchwiller, E. Incidence of rabies andpost-exposure treatment in developing countries.Bulletin of the World Health Organization, 64: 883-887(1986).
3. Postexposure treatment. In: WHO Technical ReportSeries No. 709, 1984 (WHO Expert Committee onRabies' seventh report), pp. 28-31.
4. [Reports of operations in the Institut Pasteur, Tunis].In: Archives de l'lnstitut Pasteur de Tunis, Vol. LX-LXIV. Tunis, Soci6t6 d'Art graphique d'Edition et dePresse, 1983-1987 (in French).
5. Transfer of technology for production of rabies vac-cine: Memorandum from a WHO meeting. Bulletin ofthe World Health Organization, 63: 1013-1018 (1985).
6. Vaccine administration in different animal species. In:WHO Technical Report Series No. 709, 1984 (WHOExpert Committee on Rabies: seventh report), pp. 39-40.
WHO Bulletin OMS. Vol 68 1990. 291