update on sterilization standards - s3. · pdf fileexpiration of enduring materials ......
TRANSCRIPT

1
Update on Sterilization Standards
Susan Klacik
IAHCSMM Representative to AAMI
Klacik Consulting LLC
DisclosureFaculty
Sue Klacik, BS in Business, CRCST, CIS, FCS
No conflict• It is the policy of the Ambulatory Surgery Center Association (ASCA) to ensure that all individuals who have the ability to
control or influence the content of an educational activity disclose all financial relationships with any entity whose products or services are pertinent to the content of the educational activity. The financial disclosure will include the name of the entity, and the nature of the relationship the individual has with the entity during the time the relationship is in effect and for 12 months afterward.
Requirements for successful completion of the educational activity
• Attendee must be present for the duration of the educational program
• Completed evaluation form
Expiration of enduring materials
• Contact hours will be awarded until June 30, 2016 for the educational program– ASCA is an approved provider for nursing contact hours by the California Board of Registered
Nursing, Provider #6949
– ASCA is an approved provider for Administrator Education Units (AEUs) by BASC Provider #3272
Commercial Support: None
Sponsorship: None

2
Objectives
• Discuss CDC & FDA Joint Health Alert for instrument sterilization
• Apply the updated AAMI standards to the ASC processes
• Discuss SGNA 2015 Flexible Endoscope Standard
• Discuss new standards for flexible endoscope processing.
CDC & FDA Health Alert
Joint Alert Issued September 11, 2015Alert issued due to identified lapses in healthcare reprocessing practices resulting in a critical gap in patient safety.

3
CDC & FDA Health Advisory Recommendations
Have an expert/consultant asses reprocessing procedures to assure
• Reprocessing is performed correctly
• Adequate time is allowed/taken
• All steps from the instructions for use (IFU) are followed
CDC & FDA Alert Recommendations
Training
• Through training upon hire, annually and w/ new instrumentation
• Provide demonstrated competency
• Maintain documentation of training and competency
• Have IFUs available

4
CDC & FDA AlertRecommendations
Audit & Feedback
Perform regular reprocessing documented audits
• Prompt cleaning
• Use disinfects according to IFUs
• Monitor sterilizer performance
• Monitor AER performance
• Conduct audits & feedback in all areas performing reprocessing
CDC & FDA Alert Recommendations
Infection Control Policies & Procedures
• Ensure adequate time for all reprocessing steps
• Ability to identify patient ready items
• Have policies & procedures for processing errors;
– Assess the error for risk of infection
– Identification & notification of patients
– Follow patients

5
CDC & FDA Alert Recommendations
Infection Control Policies & Procedures
• Personnel responsible for re-processing & Infection Prevention consulted for new products
• Maintain documentation of all re-processing activities
• Follow manufacturers recommendations for maintenance & repair of their medical devices
The Joint Commission
• Discusses critical reprocessing standards and recommended practices to follow for high-level disinfection and sterilization

6
TJC BoosterPak
• Leadership
• Risk Assessment
• Environment of Care
• High-level Disinfection
• HR Competency & Training
• Listing of Standards relating to HLD & Sterilization

7
Amendment to Containment devices for
reusable medical device sterilization
ANSI/AAMI ST77/Amendment A.1/CDV-1
Container Cleaning
inappropriate for use due to interactions with the reprocessing steps (i.e., cleaning, disinfection and/or sterilization) appropriate cautions should be included in the container manufacturers accompanying validated written instructions for use.
ANSI/AAMI ST77/Amendment A.1/CDV-1

8
Chemical Indicator Terminology Change
Reprinted from ANSI/AAMI/ISO 11140-1:2014 with permission ofAssociation for the Advancement of Medical Instrumentation, Inc. (C) 2015 AAMI
www.aami.org All rights reserved. Further reproduction or distribution prohibited.
CSS Utility Requirements
• Medical grade air/Instrument air
• Temperature and humidity

9
ASHRAELocation Temperature Humidity
Decontamination Room 60°F-73° F Max 60%
Clean Work Room 60°F-73° F 20% to 60%
Clean/Sterile Storage < 75°F Max 60%
HVAC Design Manual for Hospitals and Clinics. 2nd ed. Atlanta, GA: ASHRAE; 2013: 151-202
Instrument Air
A medical gas that falls under the general requirements for medical gases as defined by the NFPA 99: Health Care Facilities Code, is not respired, is compliant with the ANSI/ISA S- 7.0.01, Quality Standard for Instrument Air, and is filtered to 0.01 micron, free of liquids and
hydrocarbon vapors, and dry to a dew
point of -40o F (-40o C).

10
Cleaning Implants
Implants should be free of all contaminates and residues that could result in adverse effects to the patient.
AORN February 2016, Vol. 103, No. 2 Clinical Issues 1.2
Cleaning Implants
• Implants should not be processed through a washer/disinfector with a lubrication cycle
• Manufacturers of implants do not recommend using lubricants/instrument milk
AORN February 2016, Vol. 103, No. 2 Clinical Issues 1.2

11
Cleaning Implants
• The use of lubricants can have an effect on implants.
• Cytotoxicity is a concern, since the sterile tissue will have prolonged contact with lubricant residue
• Several implant manufacturers recommend using critical water as a final rinse to remove all residues.
AORN February 2016, Vol. 103, No. 2 Clinical Issues 1.2
Cleaning Implants
Implants pose a risk of producing pyrogenic reactions in patients if materials such as endotoxins (or any other substances that cause pyrogenic reactions, such as bacterial cell wall constituents) remain on the device at sufficient levels after reprocessing.
AORN February 2016, Vol. 103, No. 2 Clinical Issues 1.2

12
Cleaning Implants• Most washer/disinfectors
can be programmed for customized cycles that exclude the lubrication cycle.
• Implants are critical devices, thus the final rinse should be with critical water to prevent water contaminates from being deposited on them.
AORN February 2016, Vol. 103, No. 2 Clinical Issues 1.2
AORN Dress Code Changes
Recommendation I.c.2
The perioperative or sterile processing team member should wear scrub attire that covers the arms while preparing and packaging items in the clean assembly section of the sterile processing area

13
AORN Dress Code Changes
Recommendation I.c.4
• When a long-sleeved jacket is worn, it should be snapped closed or buttoned up the front.
• Wearing the jacket snapped or buttoned closed helps prevent he edges of the front of the jacket from contaminating sterile areas.
AORN Dress Code Changes
Recommendation III
III.a1 Personnel wearing scrub attire should not remove the surgical
head covering when
leaving the perioperative
area

14
2015 SGNA Flexible Endoscope Re-Processing Standards
Personnel
• Personnel must demonstrate competency for all endoscopes and instruments
• Personnel processing specialty endoscopes that are used infrequently should have more frequent competencies
• Breaches in reprocessing should be reported
• Temporary personnel should not be allowed to clean or disinfect instruments

15
Spill Containment Plan
A spill containment plan should be in place that includes:
SDS for chemicals used
Written procedures to contain the spill and deactivate the chemical
A communication plan
• An evacuation plan.
All personnel are trained to handle the chemicals safely
Added step• Precleaning• Leak testing• Manual cleaning• Rinse • Visual inspection• High-level disinfection
(manual or automated); • Rinse after high level
disinfection; • Drying • Storage
Visual inspection• Visually inspection • Use magnification and
adequate lighting to assist in visual inspection
• Consider use of rapid cleaning monitor to check for debris in channels
• Repeat manual cleaning step(s) if the scope is not clean.

16
Storage
7 days if effectively reprocessed
• Storage cabinets should be able to be disinfected.
• Scopes should be vertically hung with detachable components removed.
• Store scopes according to cabinet IFU’s
• A 7-day storage only applies if the reprocessed endoscopes reprocessed and stored according to professional guidelines and manufacturer instructions.
Review AAMIST 91Flexible Endoscope Standard

17
Scope Processing Facility Layout
• The processing area should be physically separated from the patient procedure rooms.
• An area should be defined at the incoming end of the unidirectional flow process
• One way directional flow to reduce risks of cross-contamination
33
Decontamination Sinks
• Sinks should be deep enough to allow complete immersion of the endoscope.
• The sink should large enough that the scope will not be tightly coiled.
• Sinks should not be so deep that personnel have to bend over to clean instruments. The sink should enable a person of average size to work comfortably without undue strain on the back.
34

18
Transport of Used Flexible Endoscopes
• Transport one scope per container
• Coil in large loops• Do not transport with
sharps• Keep attachments with
scope• Mark with biohazard
label • Personnel must wear
appropriate PPE
Manual Cleaning ST91
• Clean soon as possible after use to prevent soil from drying on the device
• Use fresh cleaning solution for each endoscope
• The temperature of the cleaning solution should be monitored
• Use the correct size clean brush• Clean clean all attachments.• If using an automatic flushing system,
be sure it is compatible with the endoscope
19
Inspecting for Cleanliness ST91
• Visual inspection of the exterior scope
• Cleaning verification to verify the effectiveness of the cleaning process.
Drying ST 91
38
• Effective drying of endoscopes can reduce the risk of microbial contamination following high-level disinfection
• Drying can be achieved by using medical-grade forced air through all endoscopes channels.
• The use of syringes to dry channels is not recommended
• Drying should be facilitated by using 70–80% ethyl or isopropyl alcohol.
• Thoroughly dry all removable endoscope parts, do not attach to scope during drying & storage

20
Removal from Disinfection Process ST91
39
• PPE used for decontamination should not be worn when handling a scope or any of the accessories after they have gone through the disinfection process.
• PPE should be removed and hands washed.
• Non-latex gloves should then be worn when handling the scope and accessories.
Sterilization ST91
• Terminal sterilization is the preferred method
• Terminal sterilization is recommended for flexible and semi-rigid endoscopes that enter sterile body cavities.

21
Cleaning solution
41
• Be sure to use correct detergent dilution
• Check detergent for temperature parameters and monitor
• Check for expiration date
Automatic flushing system
42
• If an automatic flushing system is used, follow the manufacturer’s written IFU and ensure that it is compatible with the endoscope being processed.
• Fresh solution should be used with each endoscope. • The connection tubing and equipment should be cleaned
and disinfected according to the manufacturer's written instructions for use (IFU).
• Any quality assurance testing recommended by the manufacturer (e.g., daily volume verification) should be performed anddocumented.

22
Automatic Endoscope Re-processor (AER)
• Incoming water should be filtered using bacterial retentive filters as recommended in the AER manufacturer's written IFU
• Quality testing devices are available for many AERs to ensure that the solutions are flowing
• Testing should be performed at least weekly, after major repairs, or whenever there is a concern about equipment function
43
Verification and monitoring of the cleaning process
• Cleaning verification testing of endoscopes should be done on a regular basis
• Have a defined program of cleaning verification that includes frequency of testing, number, and types of endoscopes to be tested.
• This testing should include at a minimum testing of the biopsy channel
12.4.1 General considerations
44

23
12.4.2 Cleaning verification
45
• Visual inspection should be conducted to detect the presence of any residual soil
• Inspection using magnification and additional illumination might identify residues more readily than the unaided eye
• Video boroscopes may be used to visually inspect the internal channels of some medical devices
Testing cleaning efficacy Verify that the cleaning equipment used for reprocessing of medical devices is working
Test equipment
• Upon installation
• During routine use (daily)
• After repairs
• When changing to a new type of cleaning solution
12.4.4 Testing cleaning efficacy
46

24
Review of monitoring devices
Physical monitors provide information of the automated reprocessing equipment by:
• Displays
• Digital printouts
• Gauges
Must be examined to verify parameters were met
Initialed by operator
12.5.2.2 Use of physical monitors and process monitoring devices
47
Scope Handling
48

25
Storage
• A tag or label should be attached to the scope to document that the scope has been cleaned or high-level disinfected
• The tag should be labeled with the following information:
a) Date of processingb) Name(s) of person(s) who performed
the processingc) Date of high-level disinfection
49
Hang Time Risk Assessment• Type of endoscope (lumened or non-lumened)
• Condition of the endoscope after processing (e.g., dry or wet; )
• How the endoscope was transported from processing to storage
• Use of aseptic technique to remove the endoscope from the AER
• Conditions of storage environment
50
26
Hang Time Risk Assessment• Excessive handling during storage
• Manufacturer’s written IFU for storage
• Compliance with professional organization guidelines for storage
• Frequency of use
• Frequency, type, and results of quality monitoring of processing
• Quality of final rinse water (see AAMI TIR34)
51
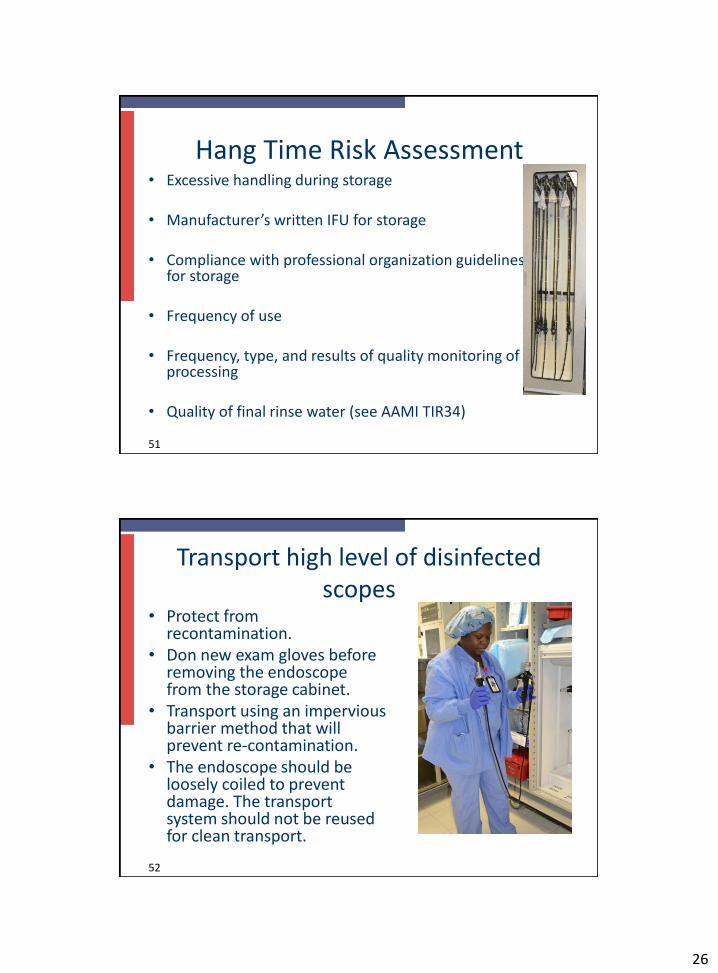
Transport high level of disinfected scopes
• Protect from recontamination.
• Don new exam gloves before removing the endoscope from the storage cabinet.
• Transport using an impervious barrier method that will prevent re-contamination.
• The endoscope should be loosely coiled to prevent damage. The transport system should not be reused for clean transport.
52

27
Quality Assurance Check List for Storage of Flexible Endoscopes
Storage of Sterilized Scopes Yes No Action
Endoscopes are rotated according to
policy
Storage conditions are monitored
according to AAMI ST79
Endoscopes are identified and labelled
Endoscope storage risk assessment checklist
Used with permission from AAMI taken from ANSI/AAMI ST91:2015 Flexible and
semi-rigid endoscope processing in health care facilities
Table 2—Endoscope storage risk assessment checklist
53
Used with permission from AAMI taken from ANSI/AAMI ST91:2015 Flexible andsemi-rigid endoscope processing in health care facilities Table 2—Endoscope storage risk assessment checklist
Storage of high level disinfected scopes Yes No Action
Endoscopes are stored so that residual fluid does not
remain in the channel
Endoscopes are stored, with their detachable parts
dismantled, in a manner that keeps them secure and
together with the scope as a unique set
If storage cabinet is used, temp and humidity are
monitored
Endoscopes are stored vertical no coil position
If a storage cabinet is used and has filters they are
changed and monitored in accordance with manufacturers
written IFU
If no storage cabinet is used, temp and humidity are
monitored in the storage area
Each Endoscope is tagged/identified with info such as last
processed, serial number etc.
54

28
Training and Competency
55
• Personnel involved in endoscope processing should be trained with demonstrated competency verification:– Upon hire
– Annually
– Designated intervals
– New endoscopes
– New equipment
– New products
Training & Competency
56
Perform competencies for the following:– All scope models used
– Leak testing
– Manual cleaning (Include detergent use)
– High level disinfection (Include manual HLD)
– Operation of AER
– Scope transportation
– Use of PPE

29
2016 AORN Guideline for Processing Flexible Endoscopes
Record the times that the endoscopy procedure is completed and the cleaning is initiated
• Biofilm begins to form within minutes
• Processing personnel need to know how long the endoscope has sat before processing
• May need to implement “delayed processing”
Recommendation IV
2016 AORN Guideline for Processing Flexible Endoscopes
Mechanically clean and mechanically process flexible endoscopes by exposure to a high-level disinfectant or a liquid chemical sterilant or mechanically clean and sterilize
• Evidence shows that mechanical processing improves cleaning effectiveness
• Minimizes personnel exposure to biohazardous materials
• Can be monitored for quality and consistency
• Provides better rinsing of disinfectants
• Reduces the potential for breeches in recommended processing protocols associated with human error and noncompliance
Recommendation VIII

30
2016 AORN Guideline for Processing Flexible Endoscopes
Use cleaning verification tests
• Cleaning verification reduce errors in manual cleaning
• Improve effectiveness.
• Cleaning verification testing– new endoscopes are purchased
– established intervals, such as after each use, daily.
Recommendation XIII
2016 AORN Guideline for Processing Flexible Endoscopes
Use a drying cabinet for storage• Optimal storage of flexible endoscopes
facilitates drying, decreases the potentialfor contamination• Provides protection from environmental
contaminates• Internal and external surfaces should
be continuously dried to suppress bacterial growth
Recommendation IX

31
2016 AORN Guideline for Processing Flexible Endoscopes
Use a team to determine maximum storage
time
• AORN no longer recommends a 5 day storage
• Storage based on many factors assemble a multidisciplinary team including infection preventionists, endoscopy RNs,
endoscopy processing personnel,
endoscopists, etc to review process
Recommendation IX
2016 AORN Guideline for Processing Flexible Endoscopes
received e
Flexible endoscopes and accessories processed by techs whose primary duties are to clean and process flexible endoscopes minimizes variability and improves processing effectiveness.
Recommendation II
Ensure cleaning and processing is conducted by individuals who have received education and completed competency verification activities related to endoscope processing

32
Questions??????
References
• ANSI/AAMI ST77/Amendment A.1/CDV-1 Containment devices for reusable medical device sterilization
• CDC Health Alert Network September 11, 2015, CDCHAN-00382
• 2015 Society of Gastroenterology Nurses and Associates, Inc. (SGNA) Standards of Infection Prevention in Reprocessing Flexible Gastrointestinal Endoscopes
• AORN “Guideline for Processing Flexible Endoscopes” 2016