update on challenging disorders of pigmentation in skin of
TRANSCRIPT

Update on Challenging
Disorders of Pigmentation
in Skin of ColorHeather Woolery-Lloyd, M.D.
Director of Ethnic Skin Care
Voluntary Assistant Professor
Miller/University of Miami School of Medicine
Department of Dermatology and Cutaneous Surgery

What Determines Skin Color?

What Determines Skin Color?
No significant difference in the number of
melanocytes between the races
2000 epidermal melanocytes/mm2 on head and forearm
1000 epidermal melanocytes/mm2 on the rest of the body
differences present at birth
Jimbow K, Quevedo WC, Prota G, Fitzpatrick TB (1999) Biology of melanocytes. In I. M. Freedberg, A.Z. Eisen,
K. Wolff,K.F. Austen, L.A. Goldsmith, S. I. Katz, T. B. Fitzpatrick (Eds.), Dermatology in General Medicine
5th ed., pp192-220, New York, NY: McGraw Hill

Melanosomes in Black and White Skin
Black WhiteSzabo G, Gerald AB, Pathak MA, Fitzpatrick TB. Nature1969;222:1081-1082
Jimbow K, Quevedo WC, Prota G, Fitzpatrick TB (1999) Biology of melanocytes. In I. M. Freedberg, A.Z. Eisen, K.
Wolff, K.F. Austen, L.A. Goldsmith, S. I. Katz, T. B. Fitzpatrick (Eds.), Dermatology in General Medicine 5th ed., pp192-
220, New York, NY: McGraw Hill

Role of Melanin-Advantages
Melanin absorbs and scatters energy from UV and visible
light to protect epidermal cells from UV damage

Disadvantages
Inflammation or injury to the skin
is almost immediately
accompanied by alteration in
pigmentation
Hyperpigmentation
Hypopigmentation

Dyschromias
Post-Inflammatory hyperpigmentation
Acne
Melasma
Lichen Planus Pigmentosus
Progressive Macular Hypomelanosis
Vitiligo

Post Inflammatory
Hyperpigmentation: Acne

PIH from Acne
Acne
hyperpigmented
macule
Patients are most
concerned with
pigmentation
Not the acne!!!

Pigment and Acne in Skin of Color
Common Questions
Does benzoyl peroxide bleach the skin?
No
Rarely can cause post-inflammatory
hypopigmentation
Post inflammatory hyperpigmentation
more common

Pigment and Acne in Skin of Color
Common Questions
Does benzoyl peroxide cause
hyperpigmentation in SOC?
Yes if patient develops irritation
Approximately 5% of the population is
sensitive to BP
Many can tolerate lower concentrations
(less than 5%)

Pigment and Acne in Skin of Color
Common Questions
Does minocycline cause
hyperpigmentaion in SOC?
Yes
Clinically can see overall darkening of
face
Also reported darkening of lips, scars, legs
Use other antibiotics as first line therapy
in SOC

Pigment and Acne in Skin of Color
Common Questions
Do retinoids cause hyperpigmentation in
SOC?
Yes if patient develops irritation
More common with tretinoin and tazarotene
Less common with adapalene but still
possible
Usually occurs within a month of use
Resolves once agent is discontinued

Do retinoids also treat
hyperpigmentation? Yes
Tretinoin
Tazarotene
Adapalene
Pigment and Acne in Skin of Color
Common Questions

Tretinoin
Influences melanosome transfer
Tretinoin 0.1% has been demonstrated to
be effective for melasma in a vehicle-
controlled trial
Slow results
Griffiths CE. Finkel LJ. Ditre et al.British Journal of Dermatology 1993;
129(4):415-21

Tretinoin for dyschromia
Blinded vehicle controlled trial
68 AA subjects with hyperpigmentation due to
acne, folliculitis, eczema, shaving irritation
40 weeks
Topical tretinoin 0.1% cream or vehicle applied
to face and arms
Investigator assessments and colorimetry
La Voo EJ. New Eng J Med Nov 1993

Tretinoin for dyschromia
Evaluated hyperpigmented and normal skin
Hyperpigmented skin
Improvement in affected skin seen clinically at
4 weeks with tretinoin vs 24 weeks with vehicle
Normal skin
No significant lightening observed clinically but
mild skin lightening was observed via
colorimetry in the tretinoin group
La Voo EJ. New Eng J Med Nov 1993

Tretinoin for dyschromia
Tretinoin 0.1% cream achieved
more rapid clearance of
hyperpigmented lesions
compared to vehicle
4 weeks vs 24 weeks
La Voo EJ. New Eng J Med Nov 1993

Patient with acne and hyperpigmentation
treated with Tretinoin 0.1% cream
La Voo EJ. New Eng J Med Nov 1993

Tazarotene for PIH
Blinded vehicle controlled trial
74 patients from darker racial ethnic groups
who had acne
Once-daily application of tazarotene cream was
shown to be effective against PIH
Reductions in overall PIH severity and in the
intensity and area of hyperpigmentation was
observed when compared to vehicle within 18
weeks (P< or =.05).
Grimes P. Callender V. Cutis. 77(1):45-50, 2006
Jan.

Adapalene in Black Africans for PIH
Open label trial of patents with acne
N=44
Identified 5 lesions on each patient and observed color change over 4 weeks
66% of patients experienced reductions in both number of hyperpigmented macules and density of the hyperpigmentation
Jacyk WK J Eur Acad Vener Dermatol Vol15 Suppl3 2001

Tazarotene vs Adapalene for PIH
Blinded controlled trial n=180
Evaluated in improvement in acne and PIH
Demographics (Total “nonwhite” subjects=62%)
Black 29%
Asian 12%
Hispanic 15%
Other 6%
Tanghetti E et al J Drugs Dermatol. 2010 May;9(5):549-58

Tazarotene vs Adapalene
Both tazarotene 0.1% cream and adapalene 0.3% gel were effective for acne
The percentage of non-white patients with compete resolution of their PIH at week 16
20 % (5/25) in the tazarotene 0.1% cream group
7% (2/29) in the adapalene 0.3% gel group
Tazarotene 0.1% cream was more effective than adapalene 0.3% gel in reducing PIH
Subjects experienced more erythema, peeling, dryness and burning with tazarotene compared to adapalene
Tanghetti E et al J Drugs Dermatol. 2010 May;9(5):549-58

Isotretinoin reduces hyperpigmentation in acne
Ten black patients, ranging in age from 17 to 34 years, were treated for nodulocystic acne with 1 mg/kg/d of isotretinoin for 20 weeks
The authors concluded
“isotretinoin is as safe and effective in the black patient with acne as it is in the white patient with acne”
An additional benefit in black patients was the prevention of new, and repression of old, post-inflammatory hyperpigmentation.
Kelly, A. Paul, and Darlene D. Sampson. "Recalcitrant nodulocystic acne in black Americans: treatment with
isotretinoin." Journal of the National Medical Association 79.12 (1987): 1266.

Before and after 20 weeks
Isotretinoin 1mg/kg
Kelly, A. Paul, and Darlene D. Sampson. "Recalcitrant nodulocystic acne in black Americans: treatment with
isotretinoin." Journal of the National Medical Association 79.12 (1987): 1266.

Retinoids work for PIH in acne
Don’t hesitate to use them in skin of color
Choose the one that best suits your patients
needs!

Acne and Post-Inflammatory
Hyperpigmentation - Treatment
Acne and dyschromia (<16yo)
Retinoids
not only improve acne but also pigmentation
Azelaic acid 20% cream or 15% gel
Works on hyperpigmentation and acne
Moisturizer with sunscreen
Consider natural therapies (soy, licorice or
emblica)

Acne and Post-Inflammatory
Hyperpigmentation
Acne and dyschromia (>16yo)
Add hydroquinone
2% available OTC
4% available with a prescription
6-8% can be compounded
Apply only to the affected area as needed
Avoid continued long term use
Less than 2 months
Maintain with alternate therapies

Hydroquinone Sensitivity
A subset of patients are sensitive to and irritated by HQ
Irritation from HQ is frequently due to
HQ
sodium metabisulfite (a common preservative in HQ preparations)
Continuing HQ despite irritation can lead to post-inflammatory hyperpigmentation
Pei-Ying Huang, Chia-Yu Chu (2007) Allergic contact dermatitis due to sodium metabisulfite in a bleaching cream Contact Dermatitis 56 (2) , 123–124
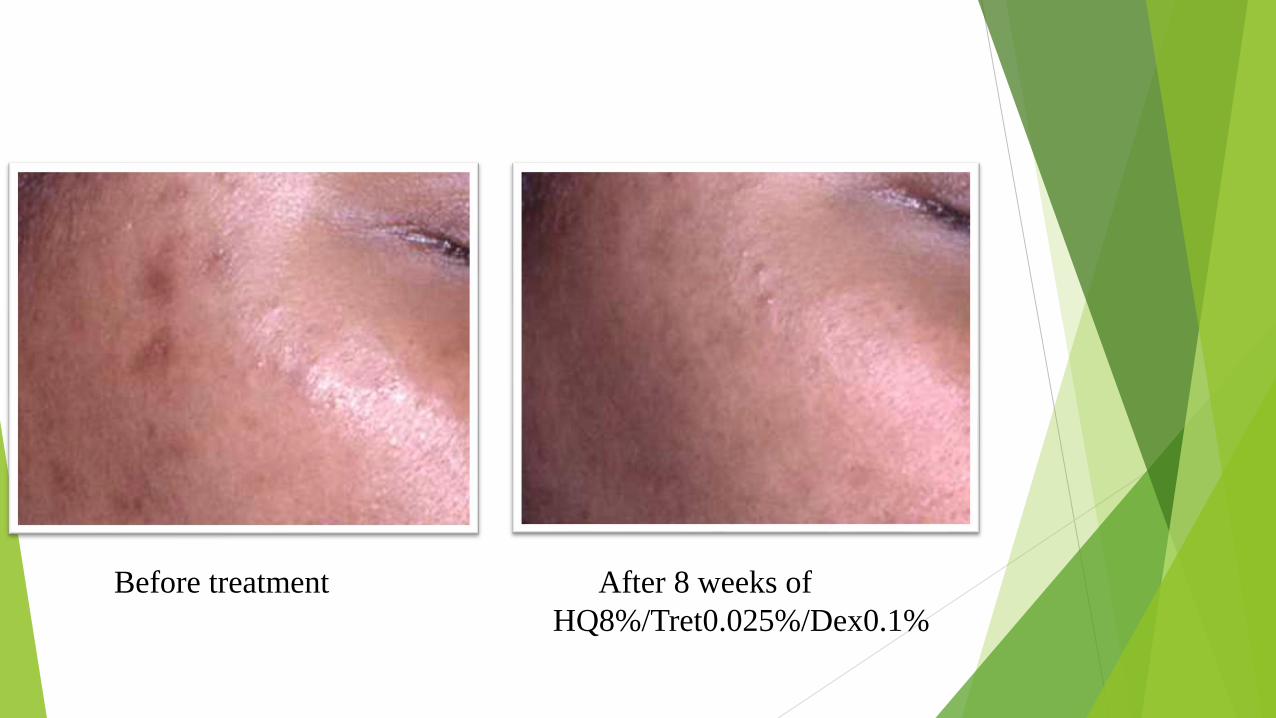
Before treatment After 8 weeks of
HQ8%/Tret0.025%/Dex0.1%

Hydroquinone Halo
Occurs when hydroquinone is
applied with the fingertips
To avoid the hydroquinone halo
Advise patient not to rub HQ in with
fingertips
Utilize cotton tipped applicator to
spot treat
Apply HQ to dark spots first and then
apply retinoid to full face

Post-Inflammatory Hyperpigmentation-
Summary
Prevention is the best therapy
Remember post inflammatory
hyperpigmentation can take an average of
4 months to clear

Melasma

Clinical Pearls in Hyperpigmentation
-Focus on Melasma
Melasma Dialogue
Treatment Plan
Maintenance Plan

Melasma Dialogue
• Just as important as the
treatment plan
• Patient must understand the
natural course of melasma
• Take time with new patients
• Ask about meds (specifically-
hormones)

Melasma- Manage Expectations
*What I tell every patient*
“Melasma is a chronic condition”
“Disease of women in their 30’s, 40’s, and 50’s”
“Tends to resolve in later decades. You won’t
have this forever”
“There is no one simple “cream or peel” that
you use once to make it go away” BUT
“There are many great treatments to
keep your melasma under control”

*Our Goal*
Decrease Pigment Size and Intensity and Prevent
Flares
WITH TREATMENT/MANAGEMENTNO TREATMENT

Treatment Plan
Sun avoidance and sun protection
Treatment Phase
Maintenance Phase

Sun Avoidance and Sun Protection

Sun Avoidance and Sun Protection
Spend time to emphasize the importance
of sun block and sun avoidance
In some ways this is more important than
the treatment itself
“10 minutes of unprotected sun exposure
and the melasma will come right back”

Sun Avoidance and Sun Protection
Broad Spectrum UVA/UVB Blocker
Add Visible light coverage if possible
Look for sunscreens that contain Iron Oxide
Iron oxide is a pigment so color matching different skin types can be challenging
Add an oral agent

UV-Visible Light Sunscreen vs
UV only Sunscreen in Melasma
68 patients with melasma were randomized in two groups to receive HQ 4 % plus either
UV-VL sunscreen SPF ≥ 50
UV-only sunscreen SPF ≥ 50
8 weeks
Assessed by
Melasma Activity and Severity Index
Colorimetry (L*)
Histological analysis of melaninCastanedo‐Cazares, Juan Pablo, et al. "Near‐visible light and UV photoprotection in the treatment of melasma: a double‐blind
randomized trial." Photodermatology, photoimmunology & photomedicine 30.1 (2014): 35-42.

UV-Visible Light Sunscreen vs
UV only Sunscreen in Melasma
Improvement in UV-Visible light group showed
15% greater improvement over UV only sunscreen for
MASI
28% greater improvement over UV only sunscreen for
colorimetry (L*)
4% greater improvement over UV only sunscreen for
melanin
Castanedo‐Cazares, Juan Pablo, et al. "Near‐visible light and UV photoprotection in the treatment of melasma: a double‐blind
randomized trial." Photodermatology, photoimmunology & photomedicine 30.1 (2014): 35-42.

Polypodium Leucotomos
Oral Photoprotection
Tropical fern plant
Antioxidant
Provides systemic photoprotection
Significant decrease in erythema
sunburn cells
cyclobutane pyrimidine dimers
Middelkamp-Hup MA, Pathak MA, Parrado C et al. J Am Acad Dermatol. 2004 Dec;51(6):910-8.
Woolery-Lloyd, Martin, Caperton, Poster AAD 2012
Polypodium Leucotomos
Investigator Initiated, double blinded, placebo controlled
21 subjects, 12 weeks
PL 240 mg BID vs placebo pill BID
Both groups used sunscreen SPF 45
Patient Assessment Mild and Moderate Improvement
PL subjects- Mild Imp 50%, Moderate Imp 13%
Placebo subjects- Mild Imp 17%, Moderate Imp 0%
MELASQOL Improvement
59% of PL subjects
27% of placebo (p<0.05)Woolery-Lloyd, Martin, Caperton, Poster AAD 2012

Woolery-Lloyd, Martin, Caperton, Poster AAD 2012

Photos – Polypodium leucotomos
Baseline Week 12
Woolery-Lloyd, Martin, Caperton, Poster AAD 2012

Treatment Phase

Treatment Phase
Start with HQ for 1-2 months
Modified Kligman from compounding pharmacy
Hydroquinone 8%/Tretinoin 0.025%/ Dexamethasone 0.1%
Emphasize the importance of hydroquinone holidays
Why? – Because the effect of HQ plateaus over time
The longer the time periods between HQ the better
Goal 2-3 courses per year at the most

Treatment Phase - Clinical Pearl
Add Hydrocortisone 2.5% cream at night for the first month and then as needed after excessive sun exposure
Why add a steroid?
Multiple studies to support the use of fluorinated steroids in melasma
Hydrocortisone 2.5% may offer some benefit without unwanted side effects
Most importantly - may reduce any irritation caused by the modified Kligman formula
Tell patient to stop HQ if any redness or irritation

Maintenance Phase:
The Hydroquinone Holiday

Maintenance Phase
This is actually the most challenging aspect of treating melasma
Maintain with a hydroquinone free skin brightener
May need to rotate products
Only use HQ as needed
4-6 weeks a few times a year
Use hydrocortisone 2.5% cream at night as needed after any excessive sun exposure
Keep emphasizing sun block and sun avoidance
Patients who practice strict sun avoidance are the most successful

Hydroquinone Alternatives
Open label & Animal Studies Arbutin/Deoxyarbutin
Aloesin
Kojic Acid
Linoleic acid/alpha linoleic
acid/oleic acid
Ellagic acid
Acerola fruit extract
Methimazole
Dioic Acid
Tranexamic acid
Blinded Controlled Trials Soy
Flutamide
Licorice Extract
Vitamin C
Niacinamide
Azelaic Acid
Lignin Peroxidase
Phenylethyl resorcinol transaminic acid, tetrapeptides, niacinamide, plankton extracts, marine extracts, polysaccharides
Hydroxyphenoxyproprionic acid, ellagic acid, yeast, salicylic acid combination
N-acetylglucosamine-split face
Decapeptide -12
Kojic Acid/Emblica

Sample regimen-Treatment Phase
AM
Cleanse
Antioxidant with Skin brightener
Broad Spectrum UVA/UVB/VL PLUS Oral Antioxidant
PM
Cleanse
HQ 8%/ Tretinoin 0.025%/ Dexamethasone 0.1% ( 4-8 weeks)
Hydrocortisone 2.5% (4 weeks)
Moisturizer if needed

Sample regimen-Maintenance Phase
AM
Cleanse
Antioxidant with skin brightener
Broad Spectrum UVA/UVB/VL PLUS Oral Antioxidant
PM
Cleanse
HQ free skin brightener (ex: azelaic acid)
Hydrocortisone 2.5% (as needed if excessive sun exposure)
Moisturizer if needed

Clinical Pearls for Challenging Cases
Add oral photoprotection
Add Hydrocortisone 2.5% cream for 1 month while using
a high concentration HQ and after any excessive sun
exposure
Add visible light photoprotection if possible
Consider adding monthly chemical peels and micro-
needling
Set expectations so that the patient understands the
natural course of melasma

Lichen Planus Pigmentosus

Lichen planus pigmentosus
Starts in the third or fourth decade of life
Slight female predilection
Lesions initially appear as small, ill-defined oval to round macules, which later become confluent to form large areas of pigmentation
Pigmentation in different patients varies from slate grey to brownish-black

Lichen planus pigmentosus

Lichen planus pigmentosus
Common diagnosis in India
Constituted 4.1% (124 ⁄ 3020) of
patients referred to the
pigmentary clinic
In earlier reported series,
pruritus was present in 50% to
62%
May also have associated LP or
FFA
Kanwar, A. J., et al. "A study of 124 Indian patients with lichen planus
pigmentosus." Clinical and experimental dermatology28.5 (2003): 481-485.

New onset dermal pigmentation on the
neck present for 4 months

Lichen planus pigmentosus
“LPP probably represents a lichenoid reaction to an
unknown agent or stimuli”
Treatment is challenging
Prednisone
Topical steroids
Tacrolimus / Pimecrolimus
Glycolic acid
Azelaic acid
Kanwar, A. J., et al. "A study of 124 Indian patients with lichen planus
pigmentosus." Clinical and experimental dermatology28.5 (2003): 481-485.

Drug Induced
Hyperpigmentation

Drug Induced facial hyperpigmentation
Common in African American
population
Clinically dark brown
hyperpigmentation on the face
(not slate grey)
Most common cause is HCTZ
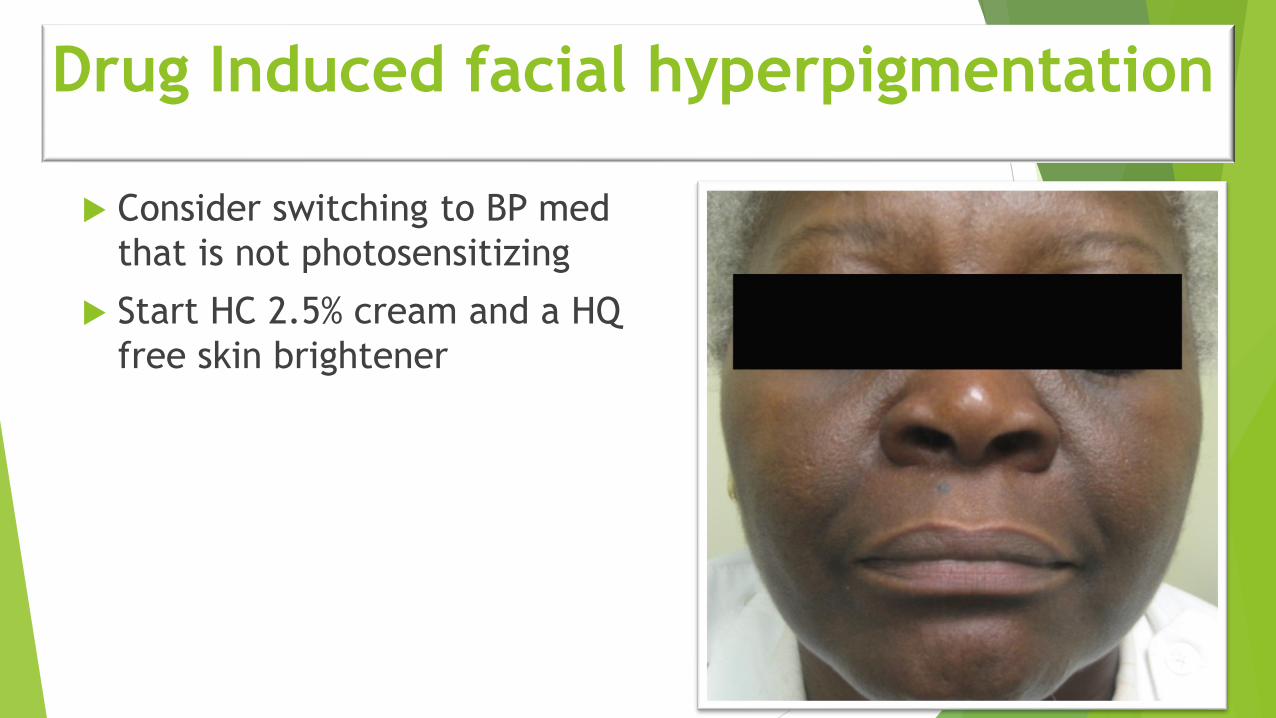
Drug Induced facial hyperpigmentation
Consider switching to BP med
that is not photosensitizing
Start HC 2.5% cream and a HQ
free skin brightener

BP drugs that don’t cause
photosenitivity
Atenolol
Labetalol
Angiotensin receptor blocker
except losartan
Clonidine
Amlodipine
Verapamil
BP drugs associated with
photosensitivity
Metoprolol
All ace inhibitors
Thiazide
Bumetanide
Lasix
Diltiazem
Losartan
Drug Induced facial hyperpigmentation

Stopped HCTZ and used
Moisturizer/Sunscreen with Soy Daily
June 2007 June 2008

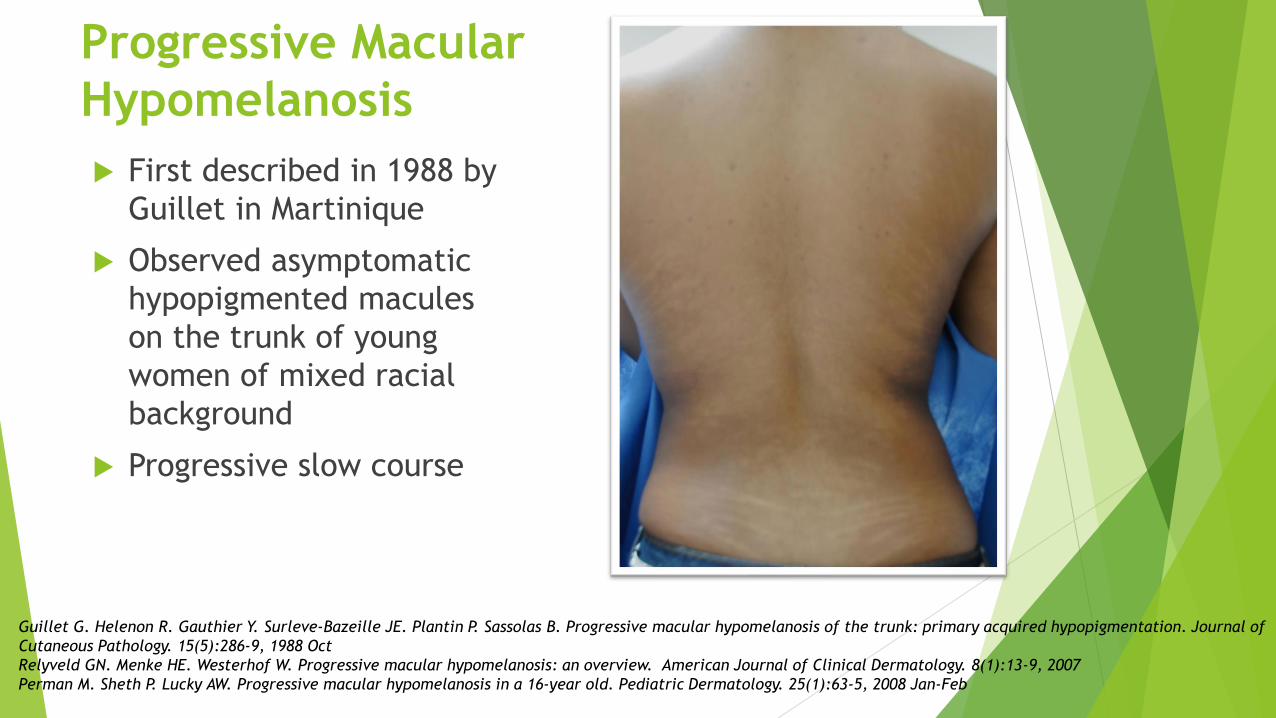
Progressive Macular
Hypomelanosis
First described in 1988 by
Guillet in Martinique
Observed asymptomatic
hypopigmented macules
on the trunk of young
women of mixed racial
background
Progressive slow course
Guillet G. Helenon R. Gauthier Y. Surleve-Bazeille JE. Plantin P. Sassolas B. Progressive macular hypomelanosis of the trunk: primary acquired hypopigmentation. Journal of
Cutaneous Pathology. 15(5):286-9, 1988 Oct
Relyveld GN. Menke HE. Westerhof W. Progressive macular hypomelanosis: an overview. American Journal of Clinical Dermatology. 8(1):13-9, 2007
Perman M. Sheth P. Lucky AW. Progressive macular hypomelanosis in a 16-year old. Pediatric Dermatology. 25(1):63-5, 2008 Jan-Feb

Differential diagnosis includes
extensive pityriasis alba and tinea
versicolor
Differs histologically and clinically
Progressive Macular Hypomelanosis
Relyveld GN. Menke HE. Westerhof W. Progressive macular hypomelanosis: an overview.
American Journal of Clinical Dermatology. 8(1):13-9, 2007

Propionibacterium acnes bacteria in hair follicles are the
cause of PMH as a result of production of a hypothetical
depigmenting factor
Red follicular fluorescence in the hypopigmented spots and
the absence of this phenomenon in normal skin when examined
under a Wood's light in a dark room
Cultivation of P. acnes from the follicles in the hypopigmented
spots but not from follicles in normal-looking skin
Improvement with topical antimicrobial treatment in
combination with UVA light
Progressive Macular Hypomelanosis
Etiology
Westerhof W. Relyveld GN. Kingswijk MM. de Man P. Menke HE. Propionibacterium acnes and the pathogenesis of progressive macular
hypomelanosis. Archives of Dermatology. 140(2):210-4, 2004 Feb
Relyveld GN. Menke HE. Westerhof W. Progressive macular hypomelanosis: an overview. American Journal of Clinical Dermatology.
8(1):13-9, 2007

Biopsy from lesional skin of 8 women demonstrated gram-positive bacteria in the pilosebaceous duct, and a mild perifollicular lymphocytic infiltrate was seen
7/8 cultured biopsy specimens grew P. acnes in affected skin
No bacteria identified in normal skin
histology and culture negative
Proposed that these strains of P acnes may produce a factor that interferes with melanogenesis
Progressive Macular Hypomelanosis Etiology
Westerhof W. Relyveld GN. Kingswijk MM. de Man P. Menke HE. Propionibacterium acnes and the pathogenesis of
progressive macular hypomelanosis. Archives of Dermatology. 140(2):210-4, 2004 Feb

Progressive Macular Hypomelanosis-
Wood’s Lamp

P Acnes strains (PMH 5 and PMH7)

Combination therapy with clindamycin and
benzoyl peroxide
UVA three times a week for a period of 12
weeks
NBUVB
Oral doxycyclineChung YL. Goo B. Chung WS. Lee GS. Hann SK. A case of progressive macular hypomelanosis treated with narrow-
band UVB. Journal of the European Academy of Dermatology & Venereology. 21(7):1007-9, 2007 Aug.
Progressive Macular Hypomelanosis Treatment

UVA plus benzoyl peroxide 5% gel QAM and clindamycin 1% lotion QHS vs UVA plus fluticasone
45 patients
26 week randomized within-patient left-right comparison study
Repigmentation rate
62% benzoyl peroxide/clindamycin/UVA side
22% fluticasone/UVA side
p <0.0001
Progressive Macular Hypomelanosis
Treatment
Relyveld GN. Menke HE. Westerhof W. Progressive macular hypomelanosis: an overview. American Journal of Clinical
Dermatology. 8(1):13-9, 2007

BeforeAfter 3 months of
Benzoyl Peroxide 4% wash and
Clindamycin lotion

Vitiligo

Vitiligo
1-2 percent of the
world's population
Over 40 million
people are
affected
Affects all races
More noticeable in
people of color

Vitiligo-Work Up
Ask about family history of autoimmune disease
Do autoimmune work up
ANA/Thyroid antibodies
NALP1 is the gene associated with vitiligo and autoimmune thyroid disease
N Engl J Med. 2007 Mar 22;356(12):1216-25

Vitiligo-Treatment
Topical steroids
Intermittent treatment with Class I steroid for 1-2 weeks can be very effective
Topical Immunomodulators
Tacrolimus and Pimecrolimus
Oral antioxidants/vitamins
NB-UVB
Age dependent
Juhlin L, Olsson MJ. Improvement of vitiligo after oral treatment with vitamin B12 and folic acid and the importance of sun exposure. Acta Derm Venereol 1997;77:460
Schallreuter KU, Wood JM, Lemke KR, Levenig C. Treatment of vitiligo with a topical application of pseudocatalase and calcium in combination with short-term UVB exposure: a case study on 33 patients. Dermatology 1995;190:223

Vitiligo
Topical tacrolimus is
effective
Works best on the face
Combine with 10 minutes of
sunlight/day
Twice daily application is
most effective
Radakovic S. Breier-Maly J. Response of vitiligo to once- vs. twice-daily topical tacrolimus: a controlled
prospective, randomized, observer-blinded trial. Journal of the European Academy of Dermatology &
Venereology. 23(8):951-3, 2009 Aug.
Grimes PE. Soriano T. Dytoc MT. Topical tacrolimus for repigmentation of vitiligo. Journal of the American
Academy of Dermatology. 47(5):789-91, 2002 Nov.

Vitiligo-Coverage
Coverage makeup
Dermablend/Covermark
Waterproof/smudge resistant
Dyoderm or VitaDye
Stain
Mineral Makeup
Contains zinc oxides, titanium dioxide, iron oxides
Offers sun protection SPF 15-30
Cover FX

Coverage Make Up

Vitiligo
Support Groups
National Vitiligo Foundation
www.nvfi.org

Thank You!