update on antenatal testing - peacehealth on antenatal testing charlotte clausen, md ... (nipt) acog...
TRANSCRIPT

UPDATE ON ANTENATAL UPDATE ON ANTENATAL TESTINGCHARLOTTE CLAUSEN, MDCENTER FOR GENETICS AND MFMSEPTEMBER 7TH 2012SEPTEMBER 7TH, 2012

Disclosure
I have nothing to disclose I have nothing to disclose I have no affiliation with any company mentioned
during this presentationduring this presentation

Objectivesj
Describe the different techniques to evaluate fetal Describe the different techniques to evaluate fetal DNA
Distinguish between the different screening and Distinguish between the different screening and diagnostic options
Identify appropriate candidates for non invasive Identify appropriate candidates for non invasive prenatal testing(NIPT)

ACOG Practice Bulletin 2007
All pregnant women should be offered screening All pregnant women should be offered screening Invasive diagnostic testing for aneuploidy should be
available to all women, regardless of maternal available to all women, regardless of maternal age.
Pretest counseling should include a discussion of the Pretest counseling should include a discussion of the risks and benefits of invasive testing compared with screening tests.

Basic Molecular and Cytogeneticsy g
Karyotype Karyotype Chromosomal constitution
of an individual

Most common chromosomal b litiabnormalities
Chromosomal abnormality Incidence Rates
XXY, XXX, Turner Syndrome 1/500
Down Syndrome 1/700Down Syndrome 1/700
Cystic Fibrosis 1/2,500
Trisomy 18 1/5,000
Fragile X 1/8,000
SMA 1/10,000
Trisomy 13 1/16,000

Age-related risk at live birthg
Maternal age at delivery Risk of Down syndrome Risk of any chromosomal abnormality
25 1/1,200 1/476
30 1/1,000 1/385/ /
35 1/400 1/192
40 1/100 1/6640 1/100 1/66
45 1/35 1/21

So, what is a screening test?, g
Goal is to define risk for a disease in an asymptomatic y ppopulation
Ideal characteristics Identify common and important fetal disorders Cost-effective and easy to perform High detection rate High detection rate Reliable and reproducible Test for disorders that have a diagnostic test available Allow time to act on results if desired

History of antenatal testingy g
1966- amniocentesis 1970’s- age alone 1980’s
AFP Triple screen- 72% detection 5% False positive Quad screen- 79% detection 5% False positive Penta screen- 83% detection 5% False positive1980’ CVS 1980’s- CVS
1990’s – First Trimester screen- 80-85% 5% False positive First Trimester screen- 80-85% 5% False positive Sequential screen 90-94% detection 3-5% FP
2010’s- Non-invasive prenatal diagnosis(fetal DNA)

Current Methods of Aneuploidy D t tiDetection
Confirmation of Diagnosis Confirmation of Diagnosis Invasive detection methods Chorionic villous sampling – first trimesterp g Amniocentesis – second trimester Potential complications: procedure-related loss 1/200
Evans MI and Wapner RJ. Invasive Prenatal Diagnostic Procedures 2005. Sem in Perina

New kid on the block….
Non-invasive prenatal testing(NIPT) Non invasive prenatal testing(NIPT)

Non-invasive prenatal diagnosisp g
Intact fetal cells Intact fetal cells 1 in a million of total cell population Can persist for years Can persist for years
Cell-free DNA Cell-free mRNA Cell-free mRNA
Lo

Circulating Cell Free Fetal DNAg
1997 article by Lo in Lancet
Lo YM, Corbetta N, Chamberlin PF et al. Presence of fetal DNA in maternal plasma and serum. Lancet 1997;350: 485-487.
Based on previous findings of tumor DNA present in patients Based on previous findings of tumor DNA present in patients with cancer
30 pregnant women with male fetuses Serum and plasma analyzed 70 – 80% detection rate
Lo et al. Presence of fetal DNA in maternal plasma and serum. Lancet 1997

Circulating Cell Free (ccf)Fetal (ccff) DNADNA Source of ccff is thought to be from placental cells
through breakdown of fetal cells in circulation Circulating fetal DNA thought to comprise 3 – 6% of all
DNA in circulating maternal plasma. Now it’s known to DNA in circulating maternal plasma. Now it s known to range from 3 – 40%, with an average of about 10%
Detection starting at as early as 5 weeks. Consistently seen at 10 weeks seen at 10 weeks
Little risk of interference of ccff from previous pregnancies
Half-life of ccff is 15 minutes and is undetectable within 2 hours postpartum
Ehrich et al. Noninvasive detection of fetal T21 by sequencing of DNA in maternal blood. AJOG 2011

Clinical uses of cffDNA
RhD Genotypingyp g Fetal DNA collected from maternal serum Used for women who with partners who are
heterozygous for RhD allele Assays used in RhD genotyping are reliable,
reproducible, and routinely used in Europe
Sex-determination For inherited disorders CAH, hemophilia, duchenne’s
Bianchi et al. Noninvasive prenatal diagnosis of fetal Rhesus D. Obstet Gynecol 2005.Queenan, JT. Noninvasive Fetal Rh Genotyping: The time has come. Obstet Gynecol 2005.

Noninvasive Aneuploidy Detectionp y
Aneuploidy detection is much more challenging Aneuploidy detection is much more challenging Single nucleotide polymorphisms DNA methylation DNA methylation Fetal mRNA

Cell-free fetal DNA
2007 Digital PCR
Lo YM, Lun F, Chan KC, et al. Digital PCR for the molecular detection of fetal chromosomal aneuploidy
2008 detection of Trisomy 21 2008 detection of Trisomy 21
Chiu RW, Chan KC, Gao Y, et al. Noninvasive prenatal diagnosis of fetal chromosomal aneuploidy by massively parallel genomic sequencing of DNA in maternal plasma Proc Natl Acad Sci USA 2008;105:20458-of DNA in maternal plasma. Proc Natl Acad Sci USA 2008;105:2045820463
Fan HC, Blumenfeld YJ, Chitkara U, Hudgins L, Quake SR. Noninvasive diagnosis of fetal aneuploidy by shotgun sequencing DNA from diagnosis of fetal aneuploidy by shotgun sequencing DNA from maternal blood. Proc Natl Acad Sci USA 2008;105:16266-16271

Massively Parallel Shotgun Sequencing (MPSS)(MPSS) Start with DNA fragments in maternal plasma Sequence and align the fragments (figure out if fragment is fetal or
maternal, and on which chromosome it belonged) Sequences that belong to potentially more than one chromosome are
h f h thrown out of the count Determine the % contribution of unique sequences mapped to each
chromosome (unique count for chrN/total unique count)C h % h N d i d d Compare the % chrN to a predetermined z-score to detect a potential aneuploid
Z-score of aneuploid chromosomes is expected to be higher (z-score >3 0) >3.0)
Chiu et al Noninvasive prenatal diagonsis by fetal chromosomalChiu et al. Noninvasive prenatal diagonsis by fetal chromosomal aneuploidy by MPGS of DNA in maternal plasma. PNAS 2008.
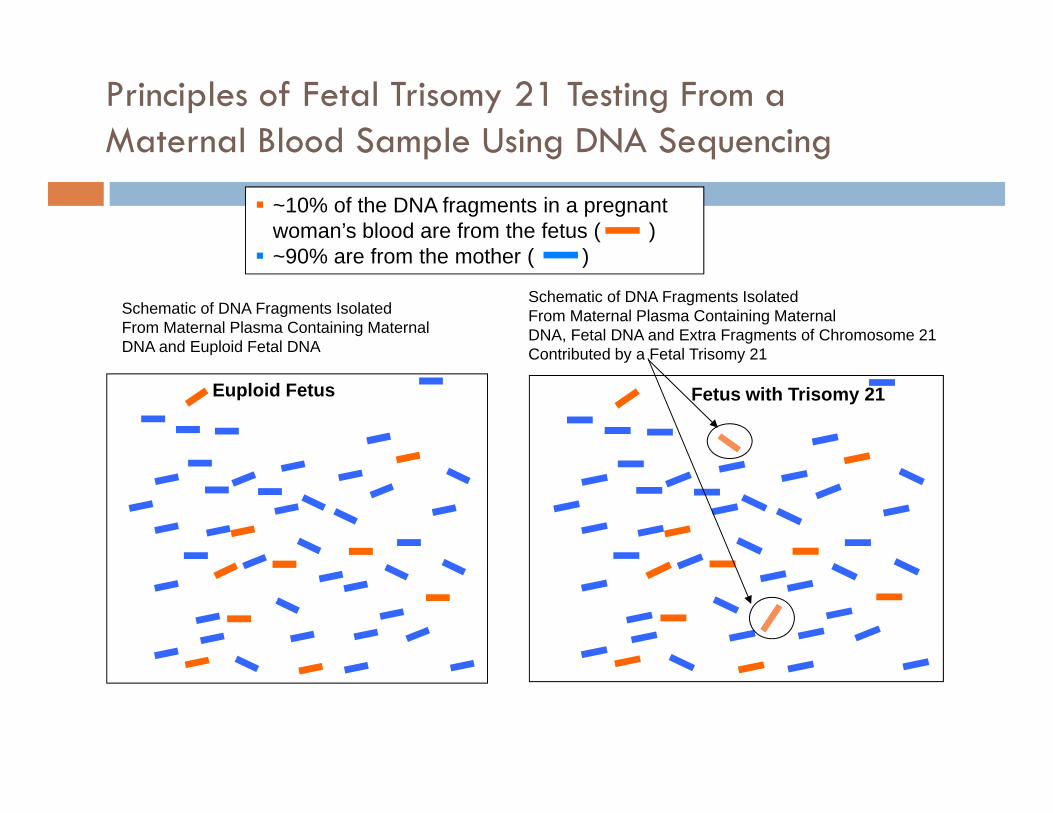
Principles of Fetal Trisomy 21 Testing From aMaternal Blood Sample Using DNA Sequencing
~10% of the DNA fragments in a pregnant woman’s blood are from the fetus ( ) 90% are from the mother ( )
Maternal Blood Sample Using DNA Sequencing
~90% are from the mother ( )
Schematic of DNA Fragments IsolatedFrom Maternal Plasma Containing MaternalDNA and Euploid Fetal DNA
Schematic of DNA Fragments IsolatedFrom Maternal Plasma Containing MaternalDNA, Fetal DNA and Extra Fragments of Chromosome 21Contributed by a Fetal Trisomy 21Contributed by a Fetal Trisomy 21
Euploid Fetus Fetus with Trisomy 21

Principles of Fetal Trisomy 21 Testing From aM t l Bl d S l U i DNA S i
GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10GACACGGTGGAGCTCGGCCACACCAGGCCCAGCTGG chr14GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10
Maternal Blood Sample Using DNA Sequencing
Sequencing tells you which chromosome the ccf fragment
TCCGCCCAGGCCATGAGGGACCTGGAAATGGCTGAT chr21
ACAGTGGTGGGGCCCATCCCTGGGTGAGGCTCAGTT chr21GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10TCCGCCCAGGCCATGAGGGACCTGGAAATGGCTGAT chr21GACACGGTGGAGCTCGGCCACACCAGGCCCAGCTGG chr14
chromosome the ccf fragment comes from
GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10ACAGTGGTGGGGCCCATCCCTGGGTGAGGCTCAGTT chr21GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10GACACGGTGGAGCTCGGCCACACCAGGCCCAGCTGG chr14GGCCCTGGGGACAGTCTCCAATCCACTGAGTCATCT chr10
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 X Y

Principles of Fetal Trisomy 21 Testing From aMaternal Blood Sample Using DNA SequencingMaternal Blood Sample Using DNA Sequencing
The total number of ccf-fetal fragments vs. ccf-maternalfragments of any one chromosome is proportional to the g y p psize of the chromosome, and is consistent from sample to sample, and patient to patient.
Sequencing tells you which chromosome the combinedSequencing tells you which chromosome the combined maternal and fetal fragments come from.
Chromosome 1 Chromosome 21

Principles of Fetal Trisomy 21 Detection Using DNA Sequencingq g
DNA MPS* does not differentiate which fragments come from the mother and which from the fetus.
The quantitative over-t ti f T i 21representation of Trisomy 21
fragments in an affected pregnancy is significant and can be measured with high
Unaffected Fetus Fetus with Trisomy 21
gprecision.
* MPS - Massively Parallel Sequencing

Schematic illustration of the procedural framework for using massively parallel genomic sequencing for the noninvasive prenatal detection of fetal chromosomal aneuploidy.seque c g o t e o as e p e ata detect o o eta c o oso a a eup o dy
Fetal or maternal?Which chromosomeDoes it belong to?
% Ch N% Chromosome N
Z-score
Chiu R W K et al. PNAS 2008;105:20458-20463
©2008 by National Academy of Sciences

Fetal aneuploidy is detectable by the overrepresentation of the affected chromosome in maternal blood.
Fan H C et al. PNAS 2008;105:16266-16271
©2008 by National Academy of Sciences

DANSR vs Massively Parallel Shotgun Sequencing Assay Comparison
Chr 18 and 21 cfDNAOth Ch fDNA
cfDNA in blood
Other Chr cfDNAUnmapped cfDNA
DANSR (Directed analysis) MPSS (Random analysis)
Same cfDNA fragments from select Random cfDNA fragments from all gchromosomes analyzed every timeOnly relevant cfDNA fragments go onto DNA sequencing96 patient samples analyzed
gchromosomes analyzed every timeAll cfDNA fragments go onto DNA sequencing regardless of relevance4-8 patient samples analyzed p p y
simultaneouslyp p y
simultaneously
25

Relative Chromosome Dosage (RCD)(RCD) Measures the total amount of a specific locus on a Measures the total amount of a specific locus on a
potentially aneuploid chromosome (ex: Chr21) Measures both maternal+ fetal total Measures both maternal+ fetal total Total dosage is compared to reference

Current NIPTs
Sequenom MaterniT21plus – launched 10/2011 Sequenom MaterniT21plus launched 10/2011
Verinata Verifi - launched 3/2012
Ariosa Harmony l h d 6/2012 Ariosa Harmony – launched 6/2012
Natera- no published clinical data
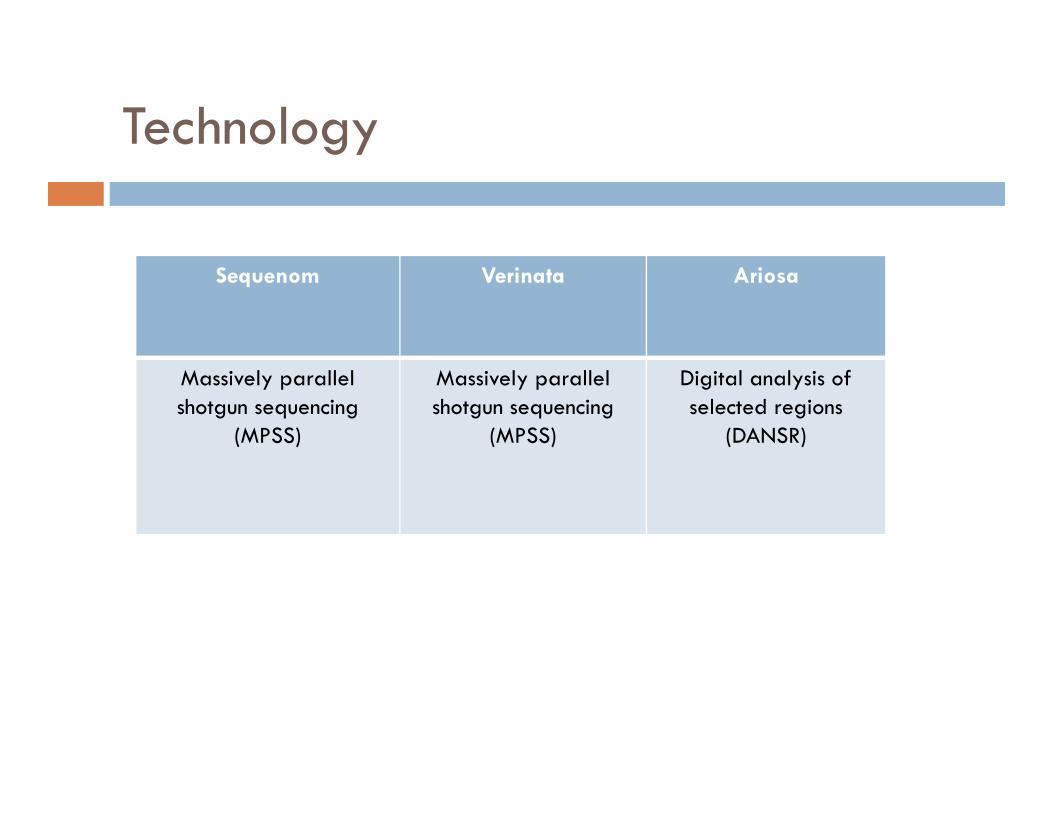
Technologygy
Sequenom Verinata Ariosa
Massively parallel shotgun sequencing
(MPSS)
Massively parallel shotgun sequencing
(MPSS)
Digital analysis of selected regions
(DANSR)

Risk Calculation
Z-score(Sequenom)
Total maternal and fetal/total reference
Mean chromosomal amount + 3 SD
>3 is positive <3 is negative >3 is positive, <3 is negative
Normalized chromosomal value(Verinata)
Total maternal and fetal/custom reference
>4SD is positive, 2.5-4 is no-call, <2.5 is negative
FORTE(Fetal-fraction optimized risk of Trisomy Evaluation) (Ariosa)
LR = cfDNA of specific chr/total cffDNA LR = cfDNA of specific chr/total cffDNA
Provides individualized risk score
Maternal age + GA x LR of result
Accounts for fetal fraction

Study Datay
Sequenom Verinata Ariosa
total n= 2,437 651 4097
# of published 4 3 4# of published studies
4 3 4
T21 249 102 205
T18 62 44 113
T13 12 15 -
XO ? 19 - 20 -

Sensitivity/Specificity - Totalsy/ p ySequenom Verinata Ariosa
T21 detection 249/251 102/102 205/205T21 detection 249/251(99.2%)
102/102(100%)
205/205(100%)
FPR 4/1880(0.2%)
0/438 3/3547(0.08%)
T18 detection 59/59(>99.9%)
43/44(97.7%)
111/113(98.2%)
FPR 5/1688(0.3%)
0/499 2/3547(0.05%)
T13 detection 11/12(91.7%)
11/15(73.3%)
-(91.7%) (73.3%)
FPR 16/1688(0.9%)
0/531 -
XO detection NA 15/16(93.8%)
NA
FPR NA 0/464 NA

MaterniT21plus (Sequenom) H R li bl i it i d t ti T21? How Reliable is it in detecting T21?
Multicenter (27 international sites) trial funded by Multicenter (27 international sites) trial funded by Sequenom
Blinded nested case control of 1694 women (212 Blinded nested case control of 1694 women (212 DS/1484 controls) undergoing invasive testing
DS detection rate was 98.9% (209/212) DS detection rate was 98.9% (209/212) Detection rate improved to 210/212 after
accounting for GC content in DNAaccounting for GC content in DNA FP rate of 0.2% with testing failure in 0.8%
Palomacki et al. Genetics in Medicine; 13(11); 2011.

MaterniT21plus (Sequenom) How li bl i it f T18 T13?reliable is it for T18 or T13?
Nested case control of 62 women with T18 and 12 with T13 matched with euploid controls
T18 (62 samples) 3 with insufficient fetal DNA 59 sampled had z-scores >3.88 c/w T18 (DR 100%) FP rate of 0 3% (5/1688 euploid samples) FP rate of 0.3% (5/1688 euploid samples)
T13 (12 samples) 11/12 with z-scores > 7.17 (DR 91.7%)/ ( ) 1/12 with normal z-score (FN 8%). 16/1688 with abnormal z-score (FP rate 0.9%)
Palomacki et al. DNA sequencing of maternal plasma reliably identifies T13 and T18. Genetics in Medicine 2011.

MaterniT21plus (Sequenom)p ( q )
Results: “Positive” vs. “Negative” based on z-score. Results: Positive vs. Negative based on z score. 1% chance for no result Eventual/potential ability to give results on other Eventual/potential ability to give results on other
chromosomes including X and Y Will accept samples on twins and IVF/egg donor Will accept samples on twins and IVF/egg donor Long term potential for genome wide studies

MaterniT21 (Sequenom)( q )

Verifi (Verinata) MELISSA t dMELISSA study Prospective, blindedp , 532 samples
89/89 T21 100% 35/36 T18 97.2% 11/14 T13 78.6% 232/233 XX 99.6% 184/184 XY 100% 15/16 XO 93 8% 15/16 XO 93.8% Also reported on complex variations 3/3 translocation 21,
1/1 mosaic T18, mosaic 2/7 monosomy X/ , / y
Bianchi DW et al. Genome-wide fetal aneuploidy detection by maternal plasma DNA sequencing. Obstet Gynecol. 119;890-901 (2012)

Verifi (Verinata) ( )
Results: “Aneuploidy detected/Aneuploidy not detected”p y / p y Least amount of published data “no call” results for patients between 2.5-4 SD-2.6% Failure rate – 2.6% (2% could be re-run) Eventual/potential ability to give results on other chromosomes
including X and Y Will accept IVF/egg donor samples M X il bl h ti h i di d Monosomy X available when cystic hygroma is diagnosed Long term potential for genome wide studies
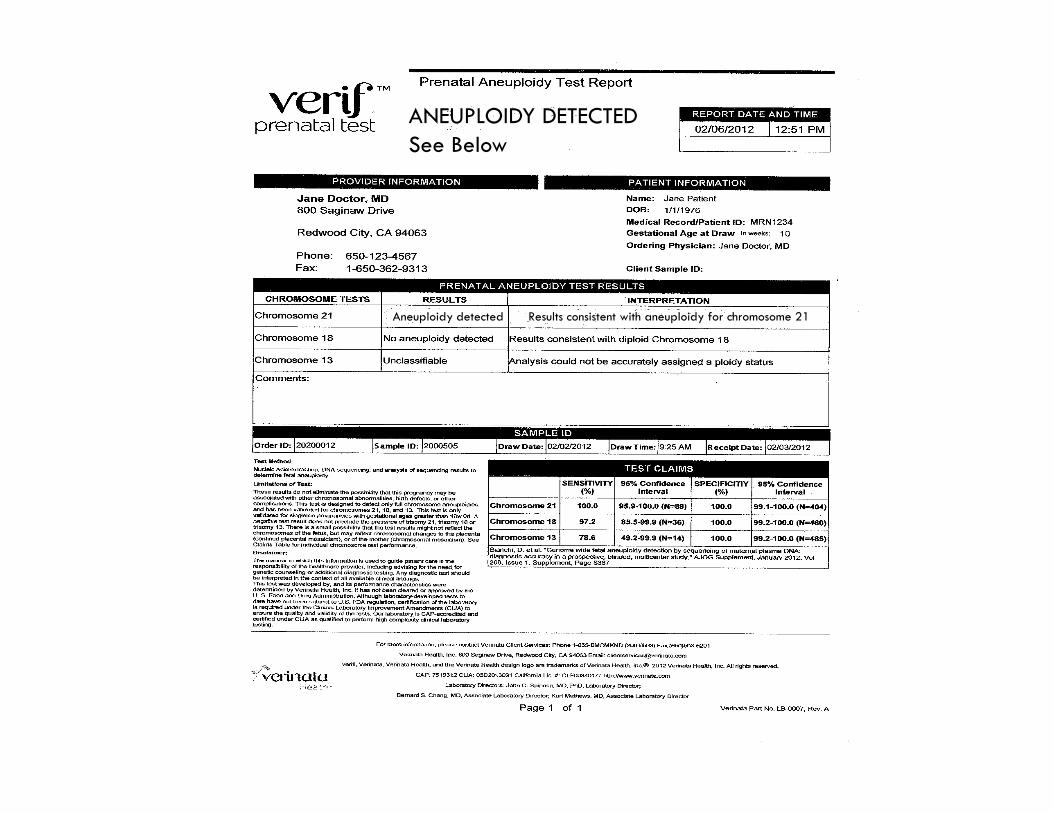
ANEUPLOIDY DETECTEDSee BelowSee Below
Aneuploidy detected Results consistent with aneuploidy for chromosome 21

Harmony (Ariosa) y ( )
P ti bli d d Prospective, blinded NICE trial 81/81 T21 1/2888 FP 0 03% 81/81 T21 1/2888 FP 0.03% 37/38 T18 2/2888 FP 0.07%
4.5% failure rate 4.5% failure rate 39% of abnormal karyotypes were other than T21/T18
Norton ME, Brar H, Weiss J, et al. Non-Invasive Chromosomal Evaluation(NICE) Study: results of a multicenter prospective cohort study
for detection of fetal trisomy 21 and trisomy 18. AJOG 137.e1-e8. Aug 2012.

Harmony (Ariosa) y ( )
Up to 4 6% chance for no result Up to 4.6% chance for no result
Can’t do on twins or IVF with egg donor at this time
Technology may be limiting in the future
Offering to the general population
Results predict PPV and NPV allowing providers to counsel patients appropriately
Largest published data set
Inclusion of clinical information in risk assessment
Targeted sequencing means decreased cost
Future studies Future studies
T13 validation
NITE- 500 subjects. European eval of T21 and T18
NEXT 25 000 bj t i H t t 1st t i t i f NEXT- 25,000 subjects comparing Harmony to current 1st trimester screening for T21

Harmony (Ariosa)y ( )

Natera
Technology based on Parental SupportTM
Targeted sequencing approach measuring SNP’s, then incorporates high fidelity parental allelic information and crossover frequency data to model a set of hypothesis(monosomy, disomy and trisomy). Gives maximum likelihood estimation.
Abstract data
166 samples 166 samples >99% detection for euploid, T21, T18, T13, X and Y 10% failure rate requiring redraw then <1% failure
PreNatus trial- enrolling 1,000 pts.
No NIPT published
Has used technology for Paternity and preimplantation genetics for some as used ec o ogy o a e y a d p e p a a o ge e cs o so e time

Still a screening testg
Positive results need to be taken in the context of disease prevalence The less prevalent a disease, the more likely a positive test is a false positive
1,000 womenTest accuracy:
100% detection
0.2% false positive
1,000 women
1 T21 999 non-T21
T21 prevalence:
1 in 1,000
1 2 9970
Test + Test +Test - Test -
Positive test result is truly right only 1/3 of the time fat extreme test performance

Probability of Trisomy 21y y
Maternal Pretest Prob at 12 Positive test result Negative test resultage(years) weeks
20 1 in 1068 1 in 23 1 in infinity
25 1 in 946 1 in 21 1 in infinity
30 1 in 626 1 in 14 1 in infinity
32 1 in 461 1 in 11 1 in infinity
34 1 in 196 1 in 8 1 in infinity34 1 in 196 1 in 8 1 in infinity
36 1 in 196 1 in 5 1 in infinity
38 1 in 117 1 in 3 1 in infinity
40 1 in 68 1 in 2 1 in infinity
Chiu RW, Akolekar R, et al. Non-invasive prenatal assessment of trisomy 21 by multiplexed maternal plasma DNA sequencing: large scale validity
study. BMJ. 342, e7401. 2011

Impact of using MPSS as a secondary test among high risk patientsamong high risk patients
2.8 million screening testsCurrently:
T21: 4362/5156 85% T18: 722/888 87%
Euploid: 148,079/2.8 mil 5.3%
114,307 invasive tests
Euploid: 148,079/2.8 mil 5.3%
,
548 procedure related losses
Palomacki et al. DNA sequencing of maternal plasma reliably identifies T13 and T18. Genetics in Medicine 2011.

NIPT as a secondary test y
MPSS will be offered to those with a screen POSITIVE test
T 21 4340/4384 98 9% T 21: 4340/4384 98.9%
T 18: 763/772
6,792 women who undergo
invasive testing
1,386 with failed testing
0.2% of 148,000 women with FP results = 296
23 – 34 procedure
related losses
Palomacki et al. DNA sequencing of maternal plasma reliably identifies T13 and T18. Genetics in Medicine 2011.

Cost and TAT
Sequenom Verinata AriosaSequenom Verinata Ariosa
List price $2400 $1,200 $795
Cash pay $475 up front $495 pt billed $795 pt billed
PPO $235 t bill d $200 t bill d $0 $795 t PPO $235 pt billed $200 pt billed $0 or $795 pt billed depending
on insurance
$ $ $OHP $475or sliding scale
$0 $0
DSHS $0 $0 $0DSHS $0 $0 $0
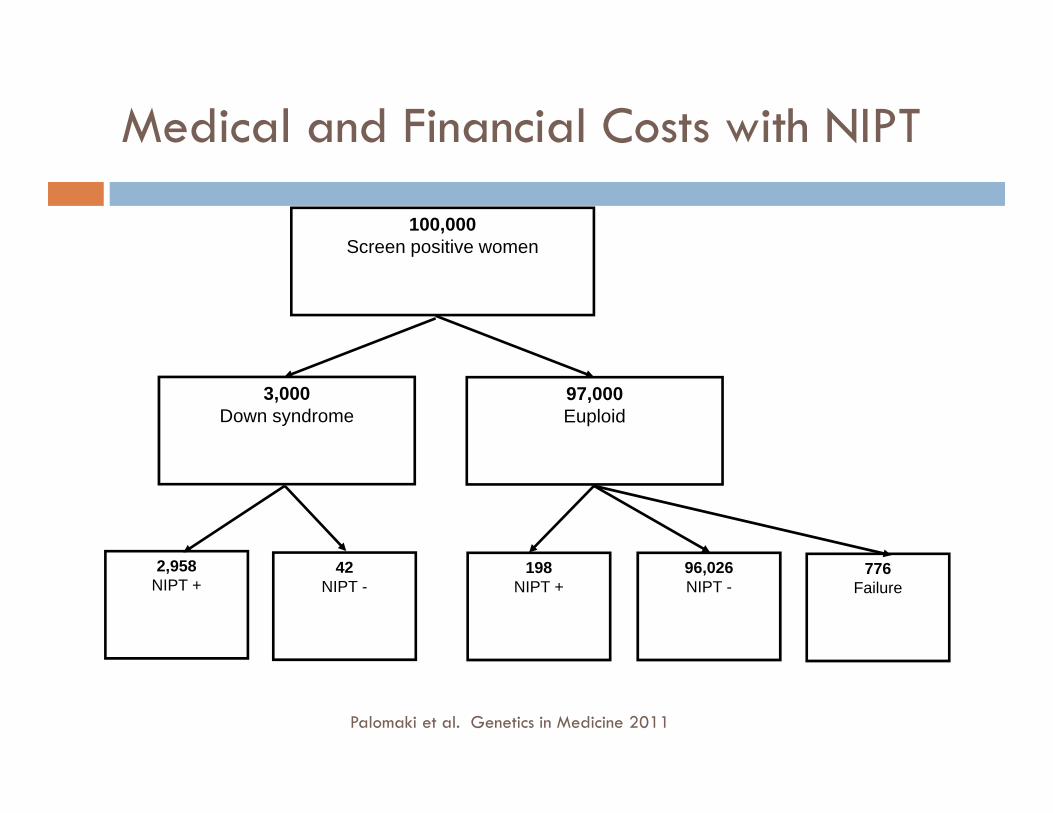
Medical and Financial Costs with NIPT
100,000Screen positive womenScreen positive women
3,000Down syndrome
97,000Euploid
2 9582,958NIPT +
42NIPT -
198NIPT +
96,026NIPT -
776Failure
Palomaki et al. Genetics in Medicine 2011

Medical and Financial Costs with NIPT
DS +/MPSS +(TP)
DS+/MPSS negative (FN)
MPSS positive(FP)
MPSS negative(TN)
MPSSFailure
Cost
Diagnostic test costs with full uptake
2958 42 198 96,026 776 100,000,000
NIPT reduced diagnostic test costs
2958 0 198 0 776 3,932,000
costs
Potential savings 0 42 0 96,026 0 96,068,000
Cases not 0 42 42Cases not detected
0 42 42

International Society for Prenatal Di iDiagnosis October 2011 October 2011
Women need detailed pretest counseling Not fully diagnostic and is an advanced screening test Not fully diagnostic and is an advanced screening test Confirmation of results through invasive testing is
required Cautioned that before routine population screening for
fetal Down syndrome is introduced, additional trials are d d i l l i l i k l ineeded, particularly in low-risk populations.
Benn PA, Borrell A, Crossley J, et al. Aneuploidy screening: a position statement on behalf of the Board of the International Society for Prenatal
Diagnosis. Prenat Diagn 2011;31: 519-22.

Genetic counselingg
General discussion of NIPT (not lab specific)( p ) Specific chromosomes evaluated Detection rate, false positive and false negative rate Not a diagnostic test Failed specimen possibilities
Ad t i t th f NIPT i t i i til Advocate against the use of NIPT in twin pregnancies until more data is published
Will facilitate testing if requested after informed consentg q

Test Restrictions
Sequenom Verinata Ariosa
Gestational age 10+ wks 10+ wks 10+ wks
Multiple gestation? Yes No No
Assisted Reproduction?
Yes Yes No egg donor pregnanciesReproduction? pregnancies
Intended for- AMA, abnormal serum screen
AMA, abnormal serum screen
General population data not validatedserum screen,
abnormal US, fam hx
serum screen, abnormal US, fam
hx
– data not validated

Points to consider
Case by case challenges Case by case challenges Discomfort/legalities of not offering test How to implement for the general population How to implement for the general population
Await low-risk studies Build infrastructure Build infrastructure Decrease cost
Rapidly moving target Rapidly moving target Social and ethical concerns (ie universal disclosure
of gender)of gender)

Future
Monitor results of test introduced into practicep Study performance in low-risk population Further testing in multiple gestation Further testing in mosaic conditions Detection of subchromosomal abnormality, single gene
disorders Complete fetal genome sequencing
Implications for in utero therapy Implications for in utero therapy Transcriptomic evaluation of gene activity
Prediction of pregnancy-associated complications Prediction of pregnancy associated complications

Thank you for your attention Thank you for your attention Questions?

Points to consider
Only validated for high-risk population - ? Ariosa Lack of large scale clinical trials/data – data starting to come in but not much DNA is placental in origin
Maternal DNA not separated from fetal DNA
Mosaicism Multiples Egg donors Unable to distinguish trisomy vs translocation Diagnostic testing recommended for confirmation Increased detection rate and increased power to excludep Decrease in losses due to fewer procedures Positive result = very high risk for aneuploidy Cost - $795 - $1900$ $ Routine screening and diagnostic testing still indicated for other issues

Nuchal translucency ultrasoundy
Correct gestation age Correct gestation age Early diagnosis of fetal malformation Diagnosis of multifetal gestation and chorionicity Diagnosis of multifetal gestation and chorionicity Can see cystic hygroma: 50% aneuploidy
M t T21 M X b t b th Most are T21 or Monosomy X, but can be others
Screening for low risk populations
FORTE vs. Z-score Comparison p
FORTE Z‐Score Provides individualized
risk score• Groups all trisomies into
one category
Accounts for fetal fraction
C i t th
• Does not factor in fetal fraction
Can incorporate other clinical risk factors
FORTETM (Fetal-fraction Optimized Risk of Trisomy Evaluation) – refers to the algorithm that incorporates DANSR assay results (chromosome counts, fetal fraction), and other clinical information to provide a individualized risk score
Normalized chromosomal value vs. Z th dZ-score method NCV Z-score NCV
#counts Chr 21/Counts on Custom reference Chr
Z score # counts Chr 21/# counts
all Chr High precision, removes
variation M i i d i
GC correction Z-score result
Maximizes dynamic range Sample to sample variability
Reduces dynamic range Reduces dynamic range