cervical cancer screening - peacehealth€¢ 2006 hpv testing incorporated into screening ... new...
TRANSCRIPT

Cervical Cancer Screening
Past… PRESENT…Future
Audrey P. Garrett, MD, MPH Women’s Health Symposium
September 7, 2012

Disclosure
• On Speaker bureau for Merck for Gardasil • On Speaker bureau for Hologic for Cervista

Objectives
• Review basis for new guidelines • Review platforms for new guidelines • Review guidelines • Convince of the rationale for use of HPV
testing in cervical cancer screening • Review strategies for discussing test results
with patients

Cervical Cancer
• 500,000 cases annually – 250,000 deaths annually
• Most common cause of cancer death • >80% occur in developing countries • 95% have never had a pap smear

Cervical Cancer: USA
• 12,200 cases annually • 4210 deaths 2010 • >60% have had no recent pap
– 83% population report screening in past year
• Death rate decreasing 4%/year – Decreased 70% since 1955

Cervical Cancer Hero • George Papanicolau: 1883-1962
Mary (wife/ MA)

Cervical Cancer Screening
• 1928 first cancer diagnosis by pap • 1941 paper presented • 1965 American Cancer Society
– Annual pap smear screening

Cervical Cancer Hero: Harald zur Hausen: Nobel Prize in Medicine, 2008

Understanding HPV: timeline
• 1973 zur Hausen hypothesis • 1983 HPV 16 isolated by Southern Blot • 1998 HPV test commercially available • 2001 vaccine trials started • 2006 HPV vaccines commercially available • 2006 HPV testing incorporated into screening • 2009 genotyping available and endorsed • 2011 4 FDA approved HPV testing platforms


HPV testing platforms
• 1998 Digene HC 2 (Qiagen) – Nucleic acid hybridization with signal amplification
using chemiluminescence • Hologic
– Invader technology, first to offer genotyping • Genprobe
– Qualitative detection of E6/E7 viral mRNA • Cobas/Roche
– PCR, uses single throughput technology
BY MIKAELA CONLEY @MIKAELACONLEY FOLLOW ON TWITTER
MAR 15, 2012 12:41PM NEW GUIDELINES DISCOURAGE YEARLY PAP TESTS

March 14, 2012
BY MIKAELA CONLEY @MIKAELACONLEY FOLLOW ON TWITTER
MAR 15, 2012 12:41PM NEW GUIDELINES DISCOURAGE YEARLY PAP TESTS


Screening Test
• Cervical cancer was common – 26,000 deaths/yr in early 20th century – 300,000 cases/yr of CIN3 now
• Lengthy pre-invasive process • Testing available
– Cervix accessible – Test inexpensive and “easy”
• Therapeutic intervention

Screening Test • Efficacy of test dependent on epidemiology
– Prevalence – Incidence
• Heavily pre-screened populations – Decrease prevalence – Stable incidence – Smaller incident lesions (lead time bias)
• Altered epidemiology of target lesion

Cervical Cancer and HPV
• HPV is ubiquitous • 100 subtypes identified • 40 predilection for ano-genital mucosa • 15 high risk sub-types • HPV 16, 18 most virulent and persistent
– 50% high grade dysplasias – 70-80% invasive cervical cancers

Cervical Cancer and HPV Biologic Plausibility
• HPV interacts with host genome – E6 and E7 interact P53 and RB
• Archival slides demonstrate presence • Prospective studies link HPV and dysplasia • 99% cervical cancers test positive • Vaccine data demonstrates efficacy

CaCx screening and HPV
• Pap swipes the ectocervix – Can miss endocervical lesions – Can miss very small lesions
• HPV represents risk of disease – Much stronger negative predictive value – Allows us to focus on those at risk – Allows us to reassure those at less risk

Neg HPV test offers better protection over years than negative Pap test
• Joint European Cohort Study • HPV vs conventional pap in 6 countries • N= 24,295
Dillner, BMJ, 2008
3 yrs 4 yrs 5 yrs 6 yrs
pap 0.51% 0.69% 0.83% 0.97%
HPV 0.12% 0.19% 0.25% 0.27%



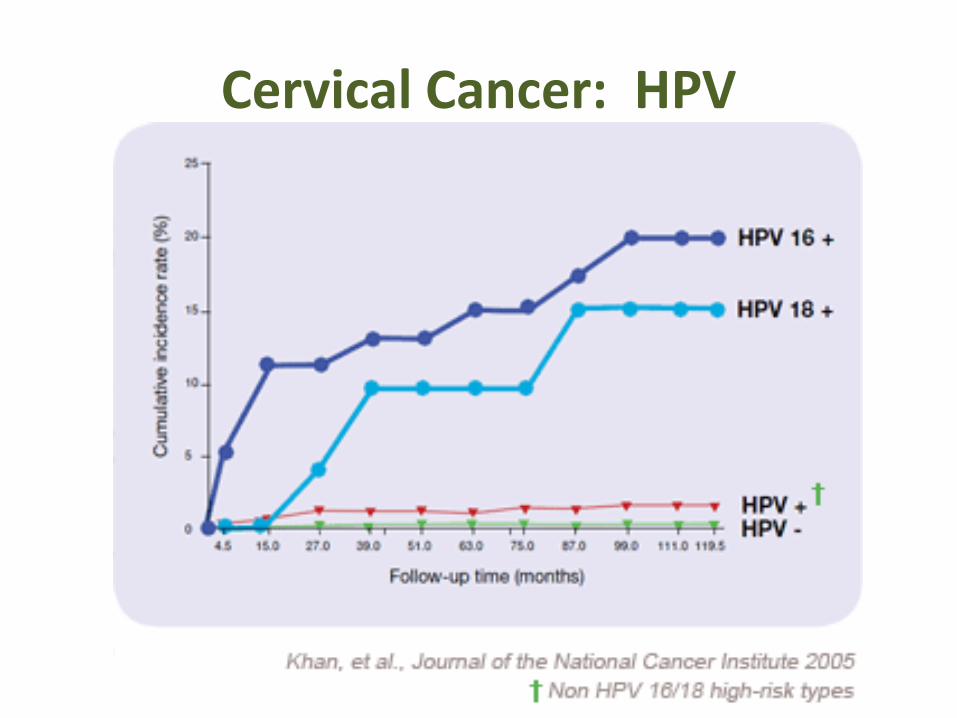
Cervical Cancer: HPV

Cervical Cancer: Prevention
• Pap test: – 20% false negative rate – Compensate with frequent paps – 1 in 5 will have an abnormal pap
• Pap test 2012: – Changing epidemiology – Better testing available – Changing recommendations

Cervical Cancer Prevention: Get with the times…
“This dial phone has always worked for me…” “My patients would never be able to understand a more modern test…”

Cervical Cancer Prevention: HPV
• HPV testing is more sensitive and specific – 3 successive paps at 20% false neg: 3/1000 – Pap and HPV at 3 yrs: 1/1000
• HPV is highly predictive of disease – If HPV 16 pos, 17% risk at 10 yrs – If HPV 16/18 neg, <4% risk at 10 yrs
• HPV testing can decrease mortality from cervical cancer – NEJM Apr, 2009

Cervical Cancer: HPV

How much protection do we lose by not doing Pap tests every year?
• Percentage reduction in rate of invasive cacx in cohort of women aged 35-64 with different frequencies of screening – Next pap 1 year: 93.5%
• 30 paps required over 30 years – Next pap 2 years: 92.5%
• 15 paps over 30 years – Next pap 3 years: 90.8%
• 10 paps over 30 years – Next pap 5 years: 83.6%
• 6 paps required over 30 years – 3 well timed paps in a lifetime
• South Africa: 95% reduction in cacx mortality
IARC BMJ 293: 1986

How many cancers do we prevent:
• Assuming at least 3 consecutive neg paps • Cancers prevented by doing annual pap rather
than Q 3 yr – Age 30-44: 3/100,000 women – Age 45-59: 1/100,000 women
• Additional testing necessary to find each cancer – Age 30-44: 69,665 paps plus 3861 colpos – Age 45-59: 209,324 paps plus 11,502 colpos
Sawaya et al, NEJM, 2003

Rate of progression CIN3-> CA
• Increases with age – 80: 10% per year – 20-24: 0.5% per year – Adolescents: negligible
Moscicki, Cox, et al, JLGTD, 2010

Cervical Cancer Screening: ASCCP/ACOG guidelines
• No paps under 21 – Controversial but Public Health based – Difference between pap and pelvic exam – STD screens if sexually active
• HPV testing not useful under 21 – High prevalence – 90% infections resolve


Cervical Cancer Screening: ASCCP/USPSTF guidelines
• Primary cytology screening 21-29
– Triennial screening – REFLEX HPV testing for ASCUS
• Women 30-65: lengthened intervals – Triennial screening with cytology – Cotesting every FIVE years – CANNOT risk assess without HPV

Cervical Cancer Screening: Women over 30
• Cytology with HPV testing
– Pap NIL, HR HPV neg: retest 5 yrs
• Pap abnormal, regardless of HPV – Triage appropriately

Cervical Cancer Screening: Women over 30
• Pap normal, HR HPV positive
– Repeat both 12 months • If HPV persistently positive, colpo
• Pap normal, HR HPV positive – Immediate reflex to HPV 16/18
• If positive, colpo • If negative, repeat


Cervical Cancer Screening: Women over 30
• Cytology with HPV testing
– May require alteration/ attention to req – May require patient education – May require EMR tickler system – Does NOT mean that patient does not need
annual exam – This is the stronger test

Cervical Cancer Screening: “other” guidelines
• Women over 65 – If adequate prior testing, cessation of screening
• Women who have had hysterectomy – If for non-HPV related causes, no screening
• Women who have had vaccination – Routine screening
• Women with new sexual partners – Routine screening

Cervical Cancer Screening: “higher risk women”
• Immunocompromise – HIV – Transplant recipient
• DES exposure in utero • Women with symptoms
– Aka not SCREENING
• Women with prior HPV related disease/treatment

The Changing Landscape of Cervical Cancer Screening
• New epidemiology – Understanding other HPV strains
• New vaccines – To cover that new understanding
• New recommendations – To accommodate that new
understanding

Cervical Cancer: Vaccines GARDASIL (Merck)
16, 18, 6, 11 2006 for girls 9-26, 2009 for boys 9-26 2010 gained indication for anal cancer
Cervarix (GSK) 16,18
2009 for girls 9-26 34% of eligible patients are vaccinated
ACOG recommends documenting vaccine status at each visit

Risk Stratification with HPV Types 16 and 18 in Women ≥ 30 Years of Age with Negative Cytology
HPV 16 positive HPV 18 positive Non-HPV 16/18 positive HPV-negative
In women ≥ 30 years of age, 10-year cumulative incidence of ≥ CIN 3 was 20% and 18% for HPV 16/18, respectively
Khan MJ, et al. J Natl Cancer Inst. 2005;87(14):1072-1079.
Follow-up Time (Years)
Cum
ulat
ive
Inci
denc
e Ra
te o
f ≥
CIN
3 (%
)
0
5
10
15
20
25
0.4 1.25 2.25 3.25 4.25 5.25 6.25 7.25 8.25 9.25 9.95

Smith J, et al. Int J Cancer. 2007;121:621-632.
16 alone
16 + 18
+ 35
+ 31
+ 33
+ 45
+ 52
+ 58
+ 59
54.7%
76.4%
83.7%
87.6%
91.0%
93.6%
94.2%
94.4%
94.5%
Cumulative Prevalence Incremental Prevalence
> 75% of Squamous Cancers in the United States Are Caused by HPV 16/18
HPV
Type
s
Proportion of Cancers Associated with HPV Types
Why Are HPV 16/18 Important?