unemployment and suicidal behaviour: a review of the literature
TRANSCRIPT

Sot. Sci. Med. Vol. 19. No. 2, pp. 93-115, 1984 Printed in Great Britain
0277-9536184 $3.00 + 0.00 Pergamon Press Ltd
UNEMPLOYMENT AND SUICIDAL BEHAVIOUR: A REVIEW OF THE LITERATURE*
STEPHEN PLAIT
MRC Unit for Epidemiological Studies in Psychiatry, University Department of Psychiatry, Royal Edinburgh Hospital, Momingside Park, Edinburgh EHlO SHF, Scotland
Abstract-In order to provide a framework for reviewing the voluminous literature on unemployment and suicidal behaviour, the author distinguishes between two categories of deliberately self-harmful act: those with fatal outcome (suicide) and those with non-fatal outcome (parasuicide); and differentiates four major types pf quantitative research report: individual-cross-sectional; aggregate-cross-sectional; individual- longitudinal; and aggregate-longitudinal. Methodological issues and empirical research findings are discussed separately for each type of study and each category of deliberate self-harm.
Cross-sectional individual studies reveal that significantly more parasuicides and suicides are un- employed than would be expected among general population samples. Likewise, parasuicide and suicide rates among the unemployed are always considerably higher than among the employed. Aggregate-cross-sectional studies provide no evidence of a consistent relationship between unemployment and completed suicide, but a significant geographical association between unemployment and parasuicide was found. Results from all but one of the individual longitudinal studies point to significantly more unemployment, job instability and occupational problems among suicides compared to non-suicides. The aggregate longitudinal analyses reveal a significant positive association between unemployment and suicide in the United States of America and some European countries. The negative relationship in Great Britain during the 1960s and early 1970s has been shown to result from a unique decline in suicide rates due to the unavailability of the most common method of suicide.
However, despite the firm evidence of an association between unemployment and suicidal behaviour, the nature of this association remains highly problematic. On the basis of the available data, the author suggests that macro-economic conditions, although not directly influencing the suicide rate, may nevertheless constitute an important antecedent variable in the causal chain leading to self-harmful behaviour. Further empirical research based on a longitudinal design is recommeded as a matter of urgency so that a more definitive assessment of the aetiological significance of unemployment in parasuicide may be made.
Frank Allaun, M.P.: “Has [the Secretary of State for the Home Department, Mr David Mellor] read the recent report of a young worker with a wife and baby who hanged himself, according to the coroner, because he had been out of work for nine months? Does he relise the growing number of tragedies resulting from the spread of unemployment?”
David Mellor, M.P.: “There is no reason to link unemployment with suicide. I should have thought that it would not be seemly to have party dis- putations on why people commit suicide” [I].
INTRODUCTION
With the inexorable rise of unemployment over the past decade in Europe and the United States to levels unknown since the depression of the 193Os, social scientists have once again turned their attention towards the delineation and measurement of its im- pact upon society. Among the most extreme behav- ioural responses to the experience of unemployment is the act, or even the serious contemplation, of suicide. The existence and nature of any association between the economic climate and suicidal behaviour has been the subject of debate for more than 150
*This is a considerably revised version of a paper presented to the WHO Workshoo on Health Policv in Relation to Unemployment in the’community, Nufiield Centre for Health Services Studies, Leeds 13-15 December 1982
years. Falret [2] contended that suicide rates tend to rise during periods of rapid social change and in times of economic depression. By the time that Durkheim wrote his seminal work on suicide, he believed that Falret’s contention had been confirmed to such an extent that he was able to write: “It is a well-known fact that economic crises have an aggravating effect on the suicidal tendency” [3]. However, many contemporary researchers have tended to question Durkheim’s assumption. The recent heated exchange between Brenner [4, 51, Gravelle et al. [6] and Eyer [7-91, demonstrates that the issue is far from being resolved.
So what is the evidence on the association between unemployment (nowadays the most commonly used indicator of economic recession) and ‘the suicidal tendency? If there is any such association, is it possible to postulate a direct causal link? If un- employment is the new ‘great plague’, then, as a Lancet editorial puts it colourfully, “we need to know the enemy before we choose the weapon-is it the uncertain status of unemployment, the behavioural reaction (more drink, more cigarettes) to being with- out a job, or the fact of relative poverty. . . or is it some complex interaction of all three?” [IO]. In other words, what is it about unemployment that is sui- cidogenic? Answers to these questions are needed urgently, in view of the extremely high levels of unemployment which prevail not only in the U.K. but throughout Europe and also in the United States.
SS.M 19 2-a 93

91 STEPHEN PLATT
As Gravelle et al. [6] note. Brenner’s conclusion [5] that fluctuations in mortality are largely explained by current and lagged unemployment rates “is im- portant because it suggests that the social costs of unemployment may be higher than had previously been thought“. If Brenner is correct, this may be a rather phlegmatic British understatement. On aggre- gate, the statistical associations which Brenner de- rives from a multivatiate regression analysis reveal that a single percent increase in the unemployment rate in the United States, if maintained over 6 years, could be associated with 36,890 additional deaths and a rise in indicators of social morbidity [I 11.
‘THE SUICIDAL TENDENCY’: DISTINCTIONS AND DEFINITIONS
In the following review two types of suicidal behaviour (defined as a deliberately self-harmful act) will be distinguished: those with fatal outcome (i.e. suicide) and those with non-fatal outcome [once termed ‘attempted suicide’ but nowadays more com- monly referred to as ‘parasuicide’ [12] or ‘deliberate self-harm’ (DSH)]. Since each study tends to adopt a somewhat idiosyncratic nominal definition of suicide/parasuicide, and it is not unusual to find operational and nominal definitions at variance with each other within-the same study, comparisons be- tween different investigators are thereby made more problematic. Nevertheless, a common element in both types of suicidal behaviour is the presence of a deliberate intention to endanger the integrity of the bilogical organism and influence the potentiality of further conscious experience. Shneidman [ 131 uses the term ‘cessation’ to refer to the final ending of con- sciousness, and describes four basic orientations which the individual may adopt towards his own demise: intentioned (where “the individual plays a direct and conscious role in his own demise”), subin- tentioned (“the individual plays an indirect, covert, partial or unconscious role. .“), unintentioned (“the person psychologically plays no significant role. .“) and contraintentioned (“an individual who uses the semantic blanket of ‘Suicide!’ with a conscious absence of any lethal intention”). Although some ‘suicides’ will be unintentioned (‘accidents’), most are probably cessation-intentioned, while the majority of acts of deliberate self-harm are cessation- unintentioned or cessation-contraintentioned. This is not, of course, to deny that some parasuicides are cessation-(sub) intentioned [14]. However, as Stengel and Cook [I51 pointed out in their influential mono- graph 25 years ago, the great majority of patients usually described as ‘attempted suicide’ do not have an unequivocal wish to die. While the variety and complexity of motivation for ‘attempted suicide’ has been illustrated by a number of authors [16], most would probably agree with Kessel’s view [14] that what is more commonly sought is not the cessation of consciousness but its interruption, defined by Shneidman [ 131 as “the stopping of consciousness with the actuality, and usually the expectation, of further conscious experience. It is a kind of tem- porary cessation”.
Stengel and Cook [ 151 were the first to draw a clear distinction between suicide and parasuicide (‘at-
tempted suicide‘). Decrying the traditional concep- tualisation of attempted suicides as merely failed suicides, they not only pointed to the complexity of motivation in non-fatal suicidal behaviour but also identified important epidemiological differences be- tween attempted suicide and completed suicide popu- lations. Subsequent researchers have maintained the distinction between the two types of behaviour [ 171. whilst noting that they are related: “two separate. but overlapping, populations” [ 181. There is abundant empirical evidence of epidemiological differences be- tween suicide and parasuicide populations [19] but less widespread consensus on the extent to which the two behaviour types are differentiated on non- epidemiological variables. However, research evi- dence is available which suggests characteristic differences in relation to the methods of self-harm which have been used. clinical aspects (e.g. psychiatric diagnosis, personality diagnosis, previous psychiatric treatment and physical illness), psycho- logical features and personality patterns [20].
TYPES OF STUDY FOUND IN THE LITERATURE
The numerous quantitative research reports [21] which have been concerned with the association between unemployment and ‘the suicidal tendency’ can be differentiated into four major types. Following Dooley and Catalan0 [22], we distinguish two orthog- onal dimensions: (a) individual vs aggregate measures of unemployment and suicidal behaviour; and (b) cross-sectional vs longitudinal collection of measures. Individual studies measure the relationship between the employment status and suicidal behaviour of individuals, while aggregate studies consider the re- lationship between the unemployment rate and the (para)suicide rate over time or over geographical areas. The temporal design of the research can either be cross-sectional, measuring the relationship be- tween unemployment and suicide data across individ- uals or groups at one point in time; or longitudinal, where unemployment in individuals or aggregates is associated with subsequent suicidal behaviour over two or more points in time. The four types of study which result from the intersection of these two dimensions are: individualLcross-sectional (Type I); aggregate-cross-sectional (Type 2); individual- longitudinal (Type 3); aggregate-longitudinal (Type 4). The methodological limitations of each type will be discussed below and substantive findings presented in the next section.
Type 1: individual-cross-sectional studies
The majority of research projects investigating the association between unemployment (or, more gener- ally. employment status) and suicidal behaviour at the individual level have been based on cross- sectional surveys of parasuicidesisuicides. Un- fortunately, formidable methodological and concep- tual problems arise which tend to make comparisons between studies rather doubtful and perhaps invalid. Wide variations can be found in the definition of both unemployment and parasuicide/suicide. In the case of unemployment. it is rarely made clear whether the non-registered jobless are included in the sample and there is a lack of consistency in the classification of

Unemployment and suicidal behaviour 95
married women who are not in paid employment (i.e. ‘housewife’ vs ‘unemployed’). The definitional prob- lem tends to differ for suicide and parasucide. In research on completed suicide, the major issue con- cerns variation between nominal and operational definitions within the same study. While each re- searcher tends to have a fairly clear idea of what s/he means by suicide, in actual fact the data are almost invariably derived from official records (e.g. coroners’ courts) or government statistics which use their own operational criteria to decide what constitutes a suicide. In parasuicide research differences between operational definitions used in the various treatment centres are not uncommon [23].
The major methodological shortcoming of the Type 1 study is that the direction of causality cannot be resolved. While there may be a relationship or association between suicidal behaviour and un- employment, it is not possible, on the basis of a cross-sectional study alone, to claim that un- employment causes suicide or parasuicide. The major alternative model is that the relationship is spurious, the result of self-selection processes. Thus, individu- als with a psychiatric illness or ‘personality disorder’ may be more vulnerable to suicidal impulses and also more likely to behave in such a way that increases their risk of being dismissed from, or impulsively quitting, their job (compared to those who are not psychiatrically ill or personality disordered).
T_+pe 2: aggregate-cross-sectional studies
In Type 2 and Type 4 (aggregate) studies, un- employment and suicide/parasuicide are treated as emergent macro-social variables rather than as prop- erties or characteristics of individuals. In the cross- sectional approach, the investigator calculates re- lationships (ecological correlations) between unemployment and suicidal behaviour rates across geographical areas (e.g. city wards, countries) at one point in time. This type of correlation can point to the presence and strength of association between un- employment and suicidal behaviour, but neither can be used to make any claims about the direction of causality. Furthermore, the relationship between the variables may be spurious. For instance, the variation in the dependent variable (suicide/parasuicide rate) may be ‘due to’ change in extraneous variables other than the hypothetical causal variable (unemployment rate) [24]. Another major limitation of the ecological approach is that a strong association between two rates cannot be used as evidence of an association at the individual level. Such an erroneous inference would, of course, be an example of the ecological fallacy [25]: even where the suicide and un- employment rates are highly correlated, the suicidal or unemployed populations may consist of the same, overlapping or different individuals. However, sociol- ogists continue to use aggregate data to make infer- ences about individuals, because appropriate individual-level data are often not available; and, under certain conditions, aggregate level data do provide unbiassed estimates of individual-level re- lationships [26]. Furthermore, it is sometimes possible to investigate empirically whether ecological cor- relations are accompanied by individual correlations.
A relevant example here is provided in the work of Philip and McCulloch [27].
Two further methodological points concerning ecological (geographical) correlations are made by Bagley et al. [28], among others. The first concerns the size of the areas used for the analysis. Although studies have sometimes based their analysis upon boroughs of over 100,000 people [29] or on city wards of over 10,000 people [27], problems are likely to ensue as a result of the social heterogeneity of such large areas. “In theory the problems of ecological correlations should be decreased if smaller areas are used, since the population of such areas is more homogeneous’ [28]. The second problem is that of ‘spatial autocorrelation’. This refers to the fact that while the units of analysis used in calculating cor- relation coefficients are presumed to be independent of one another, this situation rarely holds with geo- graphical data: contiguous areas tend to be like one another in social and economic characteristics.
“The practical implication of this problem is that cor- relation coefficients using ecological data will incoporate two measures in a virtually unquantifiable combination: the covariance of data, and the degree of similarity which contiguous social areas possess. This means that correlation coefficients will be higher than those which measure covar- iance alone. This also means that the application of significance testing to the correlations obtained is inap- propriate” [28].
Type 3: individual-longitudinal studies
Dooley and Catalan0 note that “few interpret- able studies are available to meet the need . . . for individual-level analysis of the impact of economic change on disorder” [22]. The most powerful tool in individual longitudinal studies, the prospective co- hort design, is in fact almost unknown in research where suicidal behaviour constitutes the dependent variable. This omission is not only due to the tech- nical and practical difficulties associated with quasi- experimentation, but also (and perhaps more im- portantly) because of the rarity of extreme deviant behaviour such as suicide. According to Dooley and Catalano, the retrospective design suffers from the same major shortcoming as the cross-sectional ap- proach, in that it cannot provide unambiguous evi- dence in favour of either competing explanation of the economic changeaisorder relationship (i.e. self- selection us causal mechanisms). However, this simi- larity in methodological deficiency between the ap- proaches may be more apparent than real. Dooley and Catalan0 apply the label longitudinal to studies by Sainsbury [29], Breed [30] and Tuckman and Lavell [31], among others, which merely report the percentage of suicides who were unemployed at the time of their death. The temporal design of all three studies is cross-sectional, not longitudinal, or else it becomes impossible to differentiate meaningfully be- tween the two types. The distinction between pro- spective and retrospective approaches depends on whether or not the supposed effects have occurred at the time of the investigation. The importance of the distinction lies in certain practical issues and not in any conceptual differences or differences in inter- pretation of findings [32].

WI STEPHEN PLATT
T,vpe 4: aggregate-longitudinal studies
Aggregate-longitudinal studies report the associ- ation between unemployment rates and rates [33] of suicidal behaviour in a defined geographical area (city. country) over time (usually measured in calen- dar years). In early studies it was usual to provide a graph or set of data describing trends in suicide and unemployment without any formal statistical test. However, over the years a number of different anal- ytic strategies have become avai!able for use in assessing more objectively the presence and strength of a relationship over time between two or more aggregate phenomena. Collectively, these methods are usually referred to as concomitant time series (CTS) analysis. (For an introduction to CTS analysis, see [34-361.) The simplest statistical model applied to time series analysis is the ordinary least-squares (OLS) regression model, usually expressed by the Pearson correlation coefficient (r). OLS regression assesses the synchronous linear relationship between two time-series variables. However, this method of CTS analysis does not probe the temporal precedence of the variables under study: it provides no evidence concerning whether the presumed cause precedes the presumed effect. Another major shortcoming is that autocorrelated error (which occurs when the residuals from an OLS regression are not independent) fre- quently renders OLS inappropriate. Consequently, various more sophisticated multiple regression tech- niques (mainly based on cross-sectional analysis) have been applied in order to examine the issue of temporal precedence and overcome the problem of autocorrelated error. The most well-known exponent in this area of research is Harvey Brenner. In his work the unemployment rate has been conceptualised as “a general and sensitive indicator of the extent of the recession phase of the business cycle” [37] and suicide is one of the mortality categories chosen to represent causes of death ‘reactive to mental stress’. A number of other authors interested in exploring the aggregate relationship between unemployment and suicide [38, 391 also use multiple regression methodology; and Mark [35] actually illustrates eight different ap- proaches to the statistical analysis of concomitances in time series by means of data on United States suicide and unemployment rates for the years 1900-1975.
However, a number of technical, methodological and conceptual criticisms have been levelled at time series analysis in general [8,9,22,40-42] and at Brenner’s work, in particular [6, 7,43--17]. Thus, Dooley and Catalan0 question the appropriateness of econometric prediction methods for hypothesis test- ing in this field:
“Until the questions of the existence, sign. and lag of the economic change-disorder relationship are settled, it may be premature to use techniques designed primarily to measure the magnitude of the relationship for forecasting purposes. Econometric techniques, if continued. would be more inter- pretable and widely convincing if they entailed theoretical speclficatlon of detrending techniques. anticipated re- gression models and distributed polynomial patterns” [22].
Kasl [41] is severely critical of the failure to offer any rationale for the detrending adjustments made in time series analyses, given the likelihood that such adjust-
ments will seriously distort the basic data. He is also sceptical of the manner in which investigators ‘scan’ their data in order to determine the ‘optimal’ lag. Scepticism turns to ridicule when the lag time is extended to minus one year. as in Brenner [48]. Marshall and Hodge [49] also refer to the use in Pierce’s work [50] of ‘negative lead’ correlations and comment:
“That a hypothesis involving the effect of econonnc condi- tions upon suicide could be tested if the dependent variable is lagged 1 to 3 years behind the independent variable presents a problem of causation. It is clearly difficult to comprehend how an event or condition existing in any giLen year could have an impact on events which occurred between I and 3 years earlier” (p. 106).
Kasl follows Eyer [9] in believing that “the selection of a proper lag should be neither an a priori arbitrary decision, nor an a posteriori optimising-of-results decision, but should be carried out with reference to relevant data from independent studies” [41]. Grav- elle et al. [6] have criticised Brenner’s work on England and Wales [5] on the grounds that the model is incorrectly specified, that it omits relevant vari- ables, that better data could have been used, and that Brenner’s estimates are artefacts arising from his choice of time period.
On the crucial question of the ability of the aggre- gate longitudinal strategy to resolve the competing claims of the social causation or selection hypotheses. Dooley and Catalan0 [22] are doubtful. while Kasl [41] is contemptuously dismissive. Brenner himself stresses that:
“One cannot establish causation with these procedures. At most, one can test specific hypotheses which are ideally grounded on sound theoretical considerations and earlier research findings. In these tests, the hypotheses are either supported or unsupported by the statistical evidence. Even when they are supported on the basis of statistically significant relations, they are not proven since the statistical tests only indicate whether or not the findings may result from “chance” factors at specific levels of probability. [T] here is also the issue of possible spuriousness even for the relations found to be statistically significant. Regardless of stringent controls, outside influences may have un- observable effects on the relationships. The possibility re- mains that we have not taken all relevant factors into account, especially since the state of our knowledge in the fields involved is incomplete. Thus, it is possible that some unknown factor may be influencing both the economic trends and those of the pathological indices” [I 11.
Cook et al. concur with Brenner that
“CTS studies share the classical inferential ambiguities associated with correlational research. Most notably, an obtained relationship between X and Y (whether syn- chronous or lagged or both) might alternatively be ex- plained in terms of a third variable, Z. which causes both X and Y” [34].
Possible candidates for such third variables which ‘account for’ the obtained relationship between un- employment and suicide include “confidence in the political system” [35] and “some as-yet not clearly identified societal impulse [which may possibly] intluence suicide before it is reflected in the econ- omy”[49]. While these suggestions are insufliciently

Unemployment and suicidal behaviour 97
specific and concrete to be of great heuristic value, the general methodological point remains valid. Un- fortunately, a number of CTS analysts are prone to adopt a vulgar Marxist viewpoint which decrees that all changes in the societal superstructure (including health and social customs) are determined solely by changes in the economic infrastructure. Concomitant changes at both levels are assumed to reflect un- directional causation (from the infrastructure to the superstructure). The dangers of this position are well described by Marshall and Hodge:
“It is also unlikely that the economy is the lumbering, always exogenous deux es machina it is frequently portrayed to be. It is often implicitly assumed that the independent and arbitrary perturbations, trends and cycles of the economy “cause” everything to happen; all social and political life waits for the economy to tell it what to do. It certainly does not require revolutionary insight, however, to suspect that social life influences the “exogenous” economy” [49].
THE RELATIONSHIP BETWEEN SUICIDE AND UNEMPLOYMENT: EMPIRICAL EVIDENCE FROM THE
LITERATURE
Type 1 studies (individual-cross-sectional)
Two case control studies report significantly more unemployment among psychiatric patient suicides than their matched psychiatric controls. Robin et al. [51] found that 10 out of 42 male psychiatric patient suicides (in Southend, England, during the period 1952-1965) were unemployed at the time of their death, compared to only one psychiatric control. However, among females, there was only one un- employed suicide (out of 50) but five unemployed controls (also out of 50). Roy [52] reports that 60 (67”,/,) out of 90 psychiatric patient suicides (in Tor- onto, Canada, during the period 1968-1979) were unemployed at the time of their death compared to 44 (490,;) of the psychiatric controls (P < 0.02). The difference was extremely pronounced among the men,
with 7276 of suicides unemployed compared to 43’1,,; of the controls. but nonsignificant among the women.
Several other studies have noted the extent of unemployment among a sample of suicides; the main findings are summarised in Table 1. Although none provides information on the extent of unemployment among a suitable control group [53] a few do refer to the level of unemployment prevailing among non- suicides. Thus, Sainsbury [29] contrasts the un- employment rate among the males in his suicide sample (32.5%) with the unemployment rate of 1 I. 1’;; for the local male population. Tuckman and Lavell note that: “For those below the age of 65, the incidence of unemployment is considerably greater than that found in the general population of Philadel- phia, and even this is an underestimation since no information was available on employment for about 30% of cases” [31]. In Yap’s sample of male and female suicides, 29% were unemployed at the time of death; the comparable figure for males and females in the genera1 population was 13.2% [54].
Four studies compare suicide rates among the unemployed with sucide rates among other groups. Sainsbury [29] reports a suicide rate for the un- employed (73.4 per 100,000) which was over five times that of the local population (14.1 per 100,000). The suicide rate for the unemployed in Yap’s sample was 37.2 per 100,000, higher than that of any of the occupational groups [54]. Cumming et al. [55] analyse suicide rates among women in British Columbia, by marital status, age and employment status for the years 1961 and 1971. The 1961 findings reveal that among 25-44 year olds those who are not in the labour force have an excessive rate of suicide com- pared to those who are in the labour force. While this difference by employment status holds for all marital categories, it is most pronounced for the widowed and the divorced. However, among women aged 15-24 the employed are at greater risk than the not employed. In the 45-64 age group, the not employed
Table 1. Uncontrolled studies reporting the proportion of suicides who were unemployed at time of death
Time oeriod Source
Stearns (1921) [58] Sainsbury (1955) [29]
Tuckman and Lavell (1958) [31]
Stengel and Cook (1958) [25] Yap (1958) [54] Breed (1963) [30] Maris (1981) [53]
Place
Massachusetts, U.S.A. London. England
Philadelphia, U.S.A.
London. England Hong Kong New Orleans, U.S.A. Illinois, U.S.A.
covered N in series* ___ 1920-1921 167 M&F 19361938 203 M
137 F 1951-1955 485 WM
59 BM 69 WF
1953 73 M 1953-1954 190 M&F 1954-1959 103 WM 1966-1968 146 M
“, Unemployed
69 33
26 25 25
7 29 21 35
Sathyavathi (1977) [60]
Pallis CI al. (1982) [134]
Sanborn CI al. (1974) [66] Ovenstone (1972. 1973) [19.59] Kraft and Babiglan (1976) (561
Morris er CT/. (1974) [I351
Bangalore. India
West Sussex and Portsmouth. England
New Hampshire. U.S.A. Edinburgh. Scotland Monroe County. New York. U.S.A.
Philadelphia. U.S.A.
120 F 32 1967-1973 919 M 16
746 F 3 1968 75 M&F 12
1968-1970 15 M 13t 1969-1971 56 M 46: 1969-1971 118 M 21
61 F 7 1972 103 WM 23
50 BM 34
l M = male: F = female: W = white: B = black. t53”, altogether not working. :Percentage of suicides who were unemployed. or though employed. not working
63 WF IO 20 BF 15

9x STEPHEN PLATT
have higher rates among the married and single. but the employed have higher rates among the widowed. Overall, the regression analysis shows that the stan- dardised regression coefficient associated with em- ployment status is not significant. By contrast, the 1971 regression analysis points to a clearly beneficial effect of work on the suicide rate. Among married, widowed and divorced of all ages the suicide rate among the not employed is higher than that among the employed. The same finding holds also among the single aged under 45 years, but among those aged over 45 years the suicide rate among the employed is greater. Kraft and Babigian [56] report that the rate of 91.8 suicides per 100,000 among the ‘chronically unemployed’ (not defined) is five times the rate for other groups. In a further study, Iga et al. [57] refer to the fact that “in Tokyo, unemployed males show a significantly higher suicide rate than the employed” (p. 510), but no figures are given.
In their discussion of the cross-sectional associ- ation between unemployment and suicide a number of authors also comment upon the ‘reasons for’ or ‘causes of’ unemployment in their sample. Thus, Stearns [58] shows that out of 167 suicides “36 were unemployed because they were unable to obtain work, 62 because of sickness or old age and 7 for unknown causes”. Tuckman and Lavell [31] claim that in half of the unemployed cases, poor physical or mental health was given as the main reason for unemployment; in 3% of cases, the reasons were lack of seasonal opportunities for work or poor job performance; and in the remaining cases the reason was unknown. In Breed’s series, 50% were not work- ing full time [30]. The reasons given were as follows: 13 were ‘fired’ (of whom 3 were laid off with others in a work force), 3 quit 1-6 days prior to suicide and 12 quit at least 7 days prior to suicide. Ovenstone states that the ‘principal reason’ for unemployment (or non-work among those technically employed) was psychiatric morbidity: 18 out of the 26 unemployed/not working were rated as suffering from psychiatric illness or personality disorder [59].
which unemployment can be implicated as a likely ‘cause’ of suicide in individual cases. In view of the inherent methodological limitations of this type of exercise, the results should be taken as possibly useful pointers to underlying causal processes rather than accepted uncritically as substantive findings. Stearns [58] claimed that, despite the fact that over 60”, of his sample of suicides were unemployed. “. in no case could [unemployment] be said to be the sole cause [of suicide] . . .” [N]one of this series show suicide as an immediate reaction to the loss of a job”. Likewise. Yap [54] rates only 7 out of 136 males and 1 out of 82 females under the heading ‘unemployment’ in his analysis of suicide by ‘main precipitating cause’. He notes: “A number of cases under [the heading] ‘insan- ity’ and ‘somatic illness’ were in fact unemployed. but they were not classified as such because their un- employment was clearly a consequence of their dis- ease. In some of the other categories too the subjects were unemployed, but unemployment was not con- sidered to be the main precipitating cause of their [suicidal behaviour]“. On the other hand. Sainsbury [29] claims that “lack of occupation was a factor” among 57 out of the 78 unemployed in his sample who committed suicide: in 24 cases a primary factor. in 33 cases a secondary factor. However, his analysis does not rule out the possibility that the relationship between suicide and unemployment is spurious rather than causal: 9 of the unemployed were dismissed from their jobs, 23 were out of work due to illness, and seven suffered from “chronic lack of employment due to mental or physical incapacity”. The only study which unequivocally links unemployment with sub- sequent suicide unfortunately provides no informa- tion on reasons for unemployment in the sample. Sathyavathi [60] merely states that 657, of the 171 unemployed suicides took their lives “either due to the sole reason of unemployment or for other reasons in addition to the reason of their unemployment”.
Finally, a number of Type I studies attempt to make a retrospective assessment of the extent to
Type 2 studies (aggregate-cross-sectional)
Table 2 lists nine publications ‘in which cross- sectional geographical correlations between suicide and unemployment have been reported. It should be
Table 2. Aggregate-cross-sectional studies of suicide and unemployment rates: results from seven* separate studies
Author(s) Place Year(s) Significance of correlation
Samsbury (1955) [29] London 1929-1933 Nonsignificant negative correlations (r = - 0.14,
(29 boroughs) Walbran PI ul. ( 1965) (621
Lester (1970) [6l]
Pennsylvania
(I3 Principal Labour
Market Areas)
Pennsylvania
(I3 Principal Labour
Market Areas)
Wallis and Maliphant f 1967) [I361 London
(28 boroughs) Sainrbury CI (I/. (1980) [8X] Europe
-0.18)
1954-1961 “Little evidence of geographic correlation be-
tween rates of unemployment and rates of suicide”
No formal statistical test
1954-1961 Formal statistical test of Walbran er crl. data. Nega-
tive correlations for 6 of the 8 years (two being
significant). Overall. slgnilicant nqorw correlation
between two variables
1960-1962 No relatlonship
1961-1963 Nonsigniticant neratwe correlation
Bagley cl ul. (1973) [28]
Farmer ef ul. ( 1977) [ 137)
Buglass and Dulry (1978) [64]
Buglass e, (I/. C 1980) [63]
(IX countries)
BrIghton
(I9 wards) London
(33 boroughs) Edinburgh
(23 city wards) Edmburgh
(23 c,ty wards)
1963-1969 Suwde rate and percent unemployed correlated
r=0.55(P<O.OI)
1969 1973 No relatlonship
1968 1974 No relationshlp
1971-1973 No relationship
*Nine reference\ ue listed but these cover seven mdependant analyses (see text).

Unemployment and suicidal behaviour 99
noted that the study by Lester [61] is a replication and extension of the previous work by Walbran er al. [62] which uses the same data. Likewise the Scottish Office study of Edinburgh during 1971-1973 [63] uses data which are included in the analysis by Buglass and Duffy [64]. Thus, the nine publications cover seven separate independent tests of the association between suicide and unemployment rates over geographical areas.
Only one conclusion can be drawn from Table 2: there is no such ecological association between sui- cide and unemployment rates. The findings of Bagley et al. [28] of a significant positive association have to be set against those of Lester [61] which reveal a significant negative correlation (averaged over 8 years). The other studies report no relationship at all between the two variables. Lester [61] puts forward two possible explanations for the negative cross- sectional association between unemployment and sui- cide: firstly, that in areas of low unemployment, the existence of areas of high unemployment may cause the employed individual to feel threatened with the loss of his job, this threat acting as a precipitant of suicide; and, secondly, that those who are un- employed in areas of high unemployment migrate to areas with low unemployment to look for work.
One relevant non-geographical Type 2 study has been carried out by Rushing [65] who looked at the relationship between suicide rates (and SMRs), me- dian income and unemployment rates among men aged 20-64 in 64 occupations in the U.S.A. during 1950. He found that the effects of unemployment are clearly stonger at the lower income levels. For the high income group of occupations, the unemployment-suicide relationship was non-existent; for the low income group, the correlation was highly positive. Rushing concludes that the results “clearly suggest that unemployment increases the tendency to suicide among low income groups, while employment may do so among high income groups”.
Type 3 studies (individual-longitudinal)
1 have located eight studies employing a longi- tudinal design which touch upon the association between unemployment and suicide at the individual level. (Although studies by Ovenstone [19,59] and Sanborn et al. [66] contain some information relating to employment status during the time prior to suicide, they are essentially cross-sectional in design and are included in the section above describing Type 1 studies.) Three retrospective analyses are reported by Humphrey 1671, Olsen and Lajer [68] and Shepherd and Barraclough [69]. Humphrey compared suicide victims (N = 98) homicide offenders (N = 62) and a control group of (non-suicidal, non-homicidal) psy- choneurotic controls (N = 76) in respect of their experience of ‘occupational loss’. Occupational loss was measured by allocating points for each per- manent loss of job, downward mobility, retirement and being laid off from job for more than 2 months in the past year. 95:; of the total sample with high occupational loss were suicides; only 5% were homi- cides and none were controls [67]. Olsen and Lajer investigated the association between unemployment and cause of death (‘natural’ or ‘violent’, i.e. ‘suicide’ or ‘accident’) in a retrospective study of bricklayers
and carpenters/cabinetmakers in Denmark during the years 1971-1975. The bricklayers had significantly more unemployment periods, and a significantly higher suicide rate, than the carpentersicabinet- makers. For both occupations considered together, it was found that there were significantly more un- employment periods in the group of violent deaths compared with natural deaths [68].
In a case control study, Shepherd and Barraclough [69] looked at the work record of 75 suicides (includ- ing 40 males) and 150 controls (80 males) matched by age, sex, location and whether ever married. They found that significantly fewer suicides were in paid employment at the time of their death and more were off sick or unemployed. Among the men, IO suicides (25%) were not working although economically active and only 4 controls (5’;/,). Altogether, 9 suicides were unemployed (compared to controls): 2 had been dismissed, I for drinking, the other for chronic fault-finding and dissatisfaction; 7 had given up their jobs voluntarily and were then unable or unwilling to find another. of whom 5 gave up work impulsively and 2 gave up as a result of progressive inability to measure up to the demands of work. There was also evidence that, compared to the controls, the em- ployed suicides had been off sick to a greater extent during the previous year. In the whole group the suicides showed more job instability measured by the number of jobs held in the last 3 years [70].
The remaining individual-longitudinal studies are prospective in design. Theorell ef al. [71] found that unemployment lasting over a month or other change at work during the preceding year was significantly associated with subsequent death and ‘neurosis’ (defined as ‘suicide or neurosis, psychoneurosis, anx- iety, neurotic depression or asthenia episodes causing sick leave > 30 days’). In order to help ensure inde- pendence of the economic change from the dependent variable, all subjects who had been on sick leave for at least 30 days were excluded. The authors do not state how many of the ‘neurosis’ group (N = 32) or ‘all death’ group (N =42), if any, were in fact suicides.
Cobb and Kasl looked at the frequency of suicidal behaviour in their pioneering longitudinal in- vestigation of the health and behavioural effects of job loss among 100 married male blue-collar workers (aged 35-60) in two factories which were about to close down permanently [72]. There were two com- pleted suicides, giving a rate about 30 times the rate expected of blue-collar men of this age group. One man was also known to have threatened suicide and another ‘presumably made an attempt’. The authors conclude by expressing their belief that “there was an excess of suicide during the period around the closing of the plant though the figures are not statistically significant” [73].
Two prospective longitudinal studies examine the extent of occupational problems among suicides com- pared to a group of matched controls. In a psychiatric cohort study of 3563 persons (the Lundby study), Hagnell and Rorsman found that 23 men and 5 women had committed suicide during the 25 year follow up period. Each of these 28 suicides was matched by age, sex and geographical area with two individuals drawn from the cohort and still alive at
100 STEPHEN PLATT
the end of the observation period. The authors claim that half (504;) of the suicidal group experienced “[major] occupational problems which probably can explain, at least partly, why they took their lives”. The comparable figure in the non-suicide group was l8”/ (10 out of 56). The difference between the two groups was statistically significant at the 1% level. Examples of ‘major occupational problems’ (not formally defined) included dismissal, strain due to excessive responsibility, accident at work, embezzle- ment and occupational discontent [74]. Borg and Stahl followed-up 2184 psychiatric in- and out- patients for l-2 years. The 21 males and 13 females who committed suicide during the period of obser- vation were matched by age, sex, diagnosis and patient status with controls from the original census. In contrast to the findings of the Lundby study, Borg and Stahl discovered more ‘problems at work’ (in- cluding unemployment, conflicts with fellow workers, unhappiness at work, high level of stress and bad economy) among the controls (13 out of 34) than among the suicides (4 out of 34). This difference was not, however, statistically significant [75].
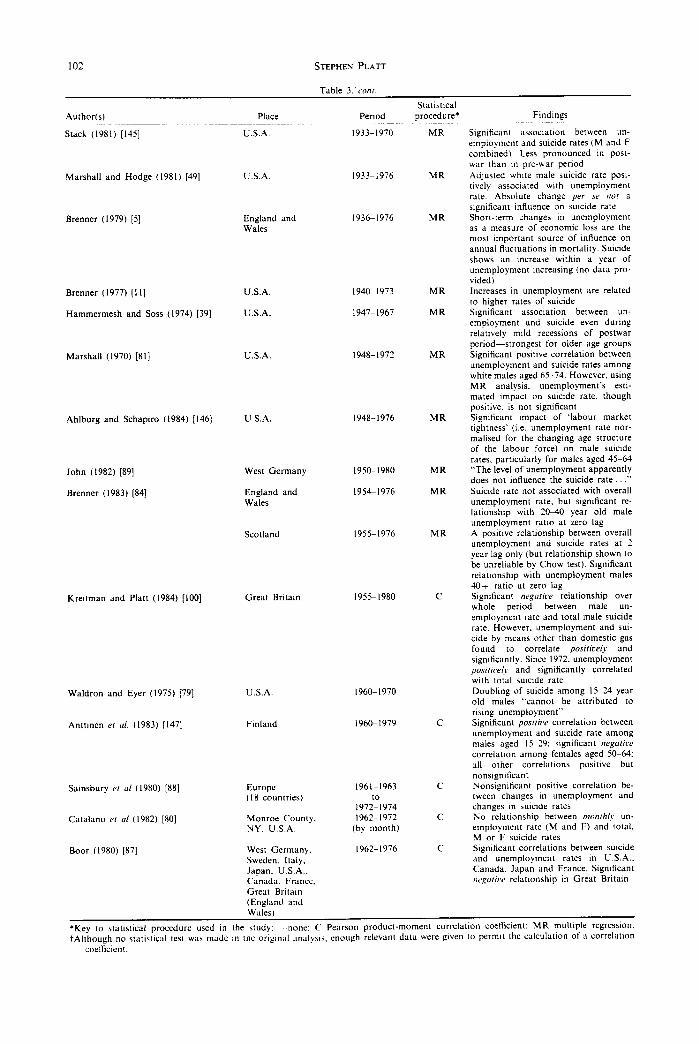
nomic recession) and suicide. The references are listed in approximate chronological order of the time period covered in the analysis.
Seven authors fail to make any statistical test of the data (although it is possible to calculate a correlation coefficient from the information provided by Stearns [SS]). The correlational and multiple regression anal- yses relating to the United States of America are almost unanimous in finding a positive association between undesirable economic change (e.g. increased unemployment) and suicide [78]. An exception is Pierce [50], who found a positive association between absolute economic change (i.e. change per se) and suicide. However, Marshall and Hodge [49] claim that the results of their own analysis of suicide and employment rates provide no support for Pierce’s findings: “
. there is little evidence. . to support Pierce’s suggestion that the recent history of the United States confirms Durkheim with respect to the importance of change, per se, rather than directional change or the state of the economy as an influence upon suicide” (p. 106).
The most impressive evidence of a link between suicide and unemployment based on general popu- lation data comes from the OPCS Longitudinal Study, a continuous multi-cohort study following random samples of individuals through time. The first report [76] is primarily concerned with re- lationships between mortality in the 5 years following the 1971 Census and characteristics of individuals at Census. The sample used is based on those people selected from the 1971 Census (England and Wales) and subsequently traced in the NHS Central Register; these 513,073 persons represent 1.05% of the 1971 Census population. The standardised mortality ratio (SMR )---set at 100 for the whole population-of men of working age (15-64 years) who were seeking work was raised by 30’//, whereas for those in work it was 14% less than average. Noting (somewhat sur- prisingly) that “there are no clear health grounds for expecting this category to record high mortality”, the authors recommend that an explanation of the excess deaths among those seeking work should be sought by
Two studies actually find no relationship between unemployment and suicide rates [79,80] and Mar- shall [81], although reporting a significant positive correlation, notes that unemployment’s estimated impact on the suicide rate is not significant when multiple regression analysis is employed. However, these findings do not constitute a convincing refuta- tion of the other evidence: in two analyses [79, 811 only restricted age bands are covered, while Catalan0 et al.3 attempt to examine trends in suicide and unemployment on a monthly basis is likely to lead to considerable instability in the computed rates [80].
“looking at the distribution of these men by social class; also at a tendency that men who are less healthy but nevertheless able to work may be unable to hold down a job for a long period and therefore feature disproportionately in their group; and at the possible adverse effects of unemployment”
(~26).
The evidence relating to Great Britain is more conflicting. Swinscow [33] found a significant cor- relation between suicide and unemployment over the period 1923-1947, but his analysis is somewhat un- satisfactory in that it uses actual numbers rather than rates [82]. Ahlburg’s study [83] shows that during the 1920s England and Wales experienced a significantly higher rate of change in suicide (after controlling for the rate of change of unemployment) than most other European countries, U.S.A. and Canada. Brenner [5] states that suicide showed an increase within a year of unemployment increasing in England and Wales over the years 1936-1976 but provides no data. When he repeats the analysis for the years 1954/5-1976, no relationship at all is found between total un- employment rate and suicide rate in England and Wales; and the positive relationship at two years lag only in Scotland is shown to be of doubtful reliability. The only significant association with suicide are the variables “unemployment males 20-40 ratio” (in England and Wales) and “unemployment males 40 + ratio” (in Scotland) [84].
When SMRs are characterised by cause of death, it becomes apparent that factors resulting in excess mortality from accidents and violence (SMR = 222) and from malignant neoplasms (SMR = 142) have contributed the major part of the excess overall mortality. “Unemployment may have contributed to an excess of deaths from suicide and related causes” (P. 27).
Type 4 .studies (u~~re~ate-longitudincrl)
Table 3 summarises the results of 30 studies [77] which have looked at the temporal association be- tween unemployment (or a related indicator of eco-
Kreitman and Platt [85] report a significant nega- tive correlation between the male unemployment rate and the total male suicide rate in Great Britain during the years 1955-1980. When the time period was further broken down, the relationship between the two variables demonstrated considerable instability: nonsignificantly positive between 1955 and 1963. significantly negative between 1964 and 1972 and significantly positive between 1973 and 1980. In a

Unemployment and suicidal hehaviour 101
previous paper, Kreitman [86] had shown that the the following decade suicide specifically due to CO carbon monoxide (CO) content of domestic gas fell decreased dramatically. He argued convincingly that markedly in Great Britain after 1962, and that during there was a direct causal relationship between these
Table 3. Aggregate-longitudinal studies of suicide and unemployment (or associated indicator of economic recession): evidence from the literature
Author(s) Place
Thomas (1927) [I381 England
Eyer (1977) [9] U.S.A.
Ogburn and Thomas (1922) 11391 U.S.A. (100 cities)
1900-1920 C
Henry and Short (1954) [140] USA 1900-1947 C
Cook er al. (1980) [34] U.S.A 1900-1975 C
Mark (1979) [35] U.S.A. 1900-1975 C
Hurlburt (1932) [I411 U.S.A. (cities of over 100,000 population) Australia
1902-1925 -
Windschuttle (1979) [ 1421 1905-1976 -
Stearns (1921) [SS]
Dublin and Bunzel (1933) [143]
Lendrum (1933) [93]
Pierce (1967) [SO] U.S.A 1919-1940 C
Massachusetts, U.S.A.
U.S.A. Massachusetts, U.S.A. 10 Eastern States, U.S.A. Detroit, U.S.A.
Vigderhous and Fishman (1980) [38] U.S.A. 1920-1969 MR
Ahlburg (1983) [83]
Swinscow (1951) (331 Great Britain 1923-1947
MacMahon er a/ (1963) [144] U.S.A 1929-1959
Germany, Belgium Netherlands, England and Wales. Switzerland, Austria, U.S.A., Canada, France, Italy
Period Statistical
procedure* Findings
1853-1913
187&l 975
1908-1918
1911-1931 1910-1931
1910-1931
1912-1930
1921/2-1931/2 MR
C
-
-
C C
C -
C
-
Index of business conditions negatively correlated with suicide rate Graph of trends in suicide rate by age and unemployment rate. “Suicide typi- cally peakIs] within weeks of the peak of the unemployment rate in the business cycle” _ Negative correlation between cycles of suicide rates and cycles of business conditions Suicide rate of males correlated nega- tively with fluctuations in business (fur- ther correlations given for age-sex, race-sex categories) Suicide and employment rates significantly negatively correlated (zero lag) Suicide and unemployment rates significantly positively correlated (zero lag) Presents chart suggesting “a degree of causal relationship between business ac- tivity and suicide” Graph of male suicide rate and percent of males unemployed. Claims that “the peaks and troughs in the male suicide rate correlate very closely to the level of unemployment” Mean annual percentage of un- employment highly correlated with sui- cide rate?
Inverse correlation between suicide death rate and index of business prosperity
Graph of annual suicide rate and stock market averages. Claims “there is little apparent correlation between the two curves”, but no statistical test is made Percent of labour force unemployed correlated at zero lag and 3 year lag with white male suicide rate, but pres- ence of autocorrelation detected. Public definition of economic situation (index based on common stock prices) and age-standard&d white male suicide rate correlated with one year lag-no evi- dence of autocorrelation Zero-order correlation between un- employment and suicide rates (M and F) highly significant. Regression anal- ysis shows that unemployment “had a dramatic impact upon suicide rates of. males”, particularly during period 1920-1940 Strong inverse relationship across coun- tries between % change in suicide rates and y0 change in several economic indi- cators, including unemployment. After controlling for rate of change of un- employment, England and Wales and Italy had a significantly higher rate of change in suicide than all other countries Significant correlation between N of male suicides and N of male unemployed “Suicide rates for males in the 45-54 year age group show a remarkable correlation with total unemployment rates in the same year”. Presents graph but no statistical test
[Table 3 continued ouerleaf
102 STEPHEN PLATT
Author(s) Place
Table 3:cow.
Period Statistical
procedure* Findings
Sigmficant association between un- employment and suicide rates (M and F combined). Less pronounced in post- war than m pre-war period Adjusted whne male suicide rate posi- twely associated wth unemployment rate. Absolute change per se GOI a sq”ficant mftuence on stucide rate Short-term changes in unemployment as a measure of economic loss are the most important source of influence on annual Ructuatlons in mortality. Suicide shows an increase within a year of unemployment mcreasing (no data pro- vided) Increases I” unemployment are related to higher rates of suicide Significant association between un- employment and suicide eve” durmg relatively mild recessions of postwar period-strongest for older age groups Significant positive correlation between unemployment and suicide rates among white males aged 65-74. However. using MR analysis. unemployment’s esti- mated impact on suxide rate. though positive. is not significant Significant “npact of ‘labour market tightness’ (i.e. unemployment rate nor- malised for the changing age structure of the labour force) on male suicide rates. particularly for males aged 45-64 “The level of unemployment apparently does not influence the suicide rate. .” Suicide rate not associated with overall unemployment rate. but w&cant re- lationship with 2o-40 year old male unemployment ratio at zero lag A positwe relationship between overall unemployment and suicide rates at 2 year lag only (but relationship show” to be unreliable by Chow test). Significant relatIonship wtth unemployment males 40+ ratio at zero lag Significant wgatiw relationship over whole period between male un- employment rate and total male suicide rate. However. unemployment and sui- cide by means other than domestic gas found to correlate postrice!\ and sigmficantly. Since 1972. unemployment positice/: and signiticantly correlated with total suzlde rate Doubling of suictde among IS-24 year old males “cannot be attributed to rising unemployment” Significant posiriw correlation between unemployment and wcide rate among males aged 15-29: significant negariw
correlation among females aged 50-64: all other correlations positive but nonstgnificdnt NonsIgnificant positive correlation be- tween changes m unemployment and changes in suictde rates No relationship between monrhly un- employment rate (M and F) and total. M or F suicide rntes Significant correlations between suicide and unemployment rates m U.S.A.. Canada. Japan and France. Sigmficant nqariw relatIonship m Great Britain
Stack (1981) [145] U.S.A. 1933-1970 MR
Marshall and Hedge (1981) [49] U.S.A. 1933-1976 MR
1936-1976 MR Brenner (1979) [5] England and Wales
Brenner (1977) [I I]
Hammermesh and Soss (1974) [39]
U.S.A.
U.S.A.
194&1973 MR
1947-1967 MR
Marshall (1970) [Bl] U.S.A. 1948-1972 MR
Ahlburg and Schapiro (1984) [I461 U.S.A. 1948-1976 MR
John (1982) [89]
Brenner (1983) [84]
West Germany
England and Wales
1950-1980
1954-1976
MR
MR
Scotland 1955-1976 MR
Kreitman and Platt (1984) [IOO] Great Britam 1955-1980 C
Waldron and Eyer (1975) [79]
Anttine” er ul. (1983) [I471
U.S.A.
Finland
1960-1970
1960-1979 C
Europe (IX countries)
Monroe County. NY, U.S.A.
1961-1963 C to
1972-1974 1962-1972 c
(by month)
Samsbury CI ul (1980) [X8]
Cat&no CI crl (1982) 1801
Boor (1980) [87] West Germany. Sweden, Italy. Japan. U.S.A.. Canada. France. Great Brttatn (England and
1962-1976 C
Wales)
‘Key to statistical procedure used in the study. “one; C Pearson product-moment correlatlo” coelficlent: MR multiple regression. tAlthough no statistxal test was made I” the original ;~“alysls. enough relevanl data were gwe” to permit the calculatmn of a correlation
coellicient.
Unemployment and suicidal behaviour
two phenomena. Overall, the decrease in CO suicide was sufficiently large to lower the total suicide rate after 1962 and accounts for the findings of a negative correlation between unemployment and suicide dur- ing the following decade. Unemployment and suicide by means other than domestic gas were found to correlate significantly and positively between 1955 and 1980, including during the years 1964-1972 [85].
A few studies report relevant data concerning other European countries. During the period 1962-1976, Boor [87] found a significant positive relationship between suicide and unemployment rates in the U.S.A., Canada, Japan and France; correlations for Germany, Sweden and Italy, though positive, were not significant; and in Great Britain the correlation was significantly negative. Boor’s findings are largely replicated by Sainsbury’s discovery of a nonsignificant association between changes in un- employment and suicide in Europe over the same period [88] and John’s failure to uncover any tempo- ral association in West Germany during the period 1950-1980 [89]. To my knowledge, only one attempt has been made to examine the impact of un- employment on suicide at different historical periods. Ahlburg and Schapiro [90] contrast the independent effect of the economy on suicides during the Great Depression and the post-Second World War period. The results of this analysis suggest to them that the suicide rate is now about twice as responsive to unemployment as was the case during the great depression.
from cross-sectional surveys of parasuicide samples. Wherever possible, data are given for males only. (If no separate analysis for males has been made, then data refer to both sexes together.) The exclusion of females arises out of the confusion concerning their correct employment status classification, especially among those who are married. In some studies, all married women or women with children (whether married or not) are automatically rated ‘housewives’. In other studies, these groups of women are rated ‘unemployed’ if they are registered as such or even if they merely express an interest in obtaining paid employment. In general, the bulk of studies on parasuicide and unemployment fail to discriminate between groups of women with differing degrees of involvement in the labour market. Warr and Parry [91] have highlighted the same deficiency in studies which examine the relationship between women’s psychological well-being and paid employment.
THE RELATIONSHIP BETWEEN PARASUICIDE AND UNEMPLOYMENT: EMPIRICAL EVIDENCE FROM
THL LITERATURE
Type 1 studies (individual-cross-sectional)
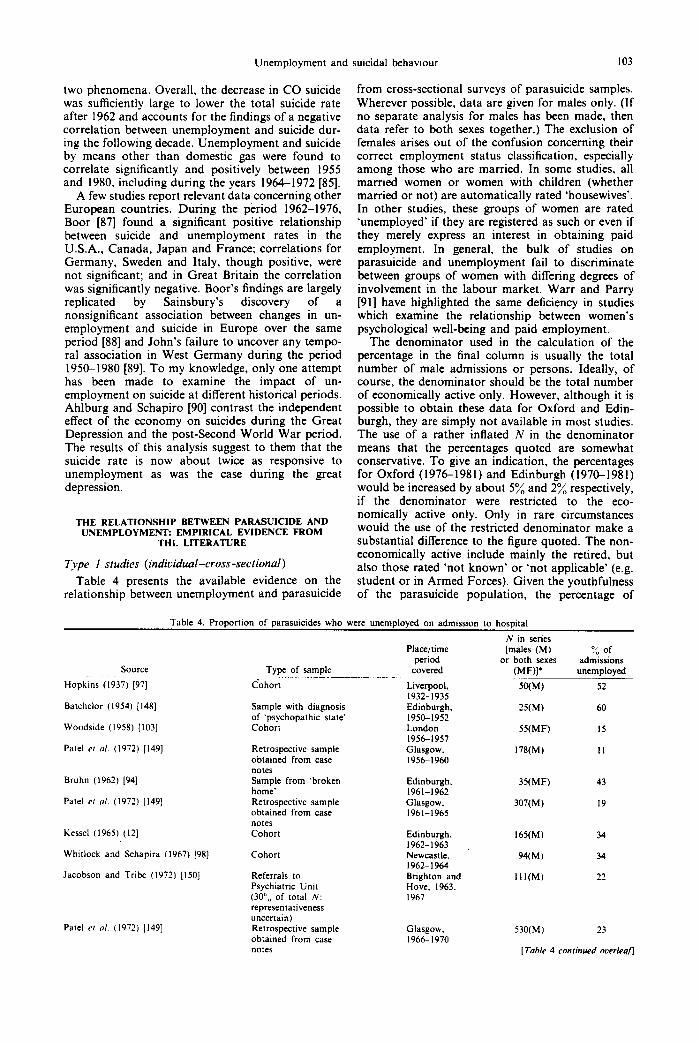
Table 4 presents the available evidence on the relationship between unemployment and parasuicide
The denominator used in the calculation of the percentage in the final column is usually the total number of male admissions or persons. Ideally, of course, the denominator should be the total number of economically active only. However, although it is possible to obtain these data for Oxford and Edin- burgh, they are simply not available in most studies. The use of a rather infIated N in the denominator means that the percentages quoted are somewhat conservative. To give an indication, the percentages for Oxford (19761981) and Edinburgh (1970-1981) would be increased by about 5% and 2% respectively, if the denominator were restricted to the eco- nomically active only. Only in rare circumstances would the use of the restricted denominator make a substantial difference to the figure quoted. The non- economically active include mainly the retired, but a!so those rated ‘not known’ or ‘not applicable’ (e.g. student or in Armed Forces). Given the youthfulness of the parasuicide population, the percentage of
103
Table 4. Proportion of parasuicides who were unemployed on admission to hospital
N in series Place/time [males (M) :/. of
period or both sexes admissions SOWX Type of sample covered (MF)l* unemployed
Hopkins (1937) [97[ cohort Liverpool, SO(M) 52 1932-193s
Batchelor (1954) [ 1481 Sample with diagnosis Edinburgh. 25w) 60 of ‘psychopathic state’ 1950-1952
Woodside (I 958) [ IO31 Cohort London SXMF) I5
Pate1 er 01. (1972) [I491 Retrospective sample obtained from case
Bruhn (1962) [94]
Pate1 CI a/. (1972) [I491
Kessel (1965) (121
notes Sample from ‘broken home’ Retrospective sample obtained from case notes Cohort
Whitlock and Schapira (1967) [98] Cohort
Jacobson and Tribe (1972) [I501 Referrals to Psychiatric Unit (30”,, of total N: representativeness uncertain)
Pate1 c, al. (1972) (1491 Retrospective sample obtained from case notes
19561957 GbdSgOW’.
1956-1960 178(M) II
Edinburgh. 1961-1962 Glasgow. 1961-1965
35(MF) 43
307(M) I9
Edinburgh, 1962-1963 Newcastle. 1962-1964 Brighton and Hove. 1963. I967
165(M) 34
94(M) 34
I I l(M) 22
Glasgow. 1966-1970
530(M) 23
[Table 4 conrimed overleajl

104 STEPHEN PLAT?
Table 4. conr.
Source Type of sample
Smith and Davidson (1971) [IO51 Cohort
MRC Unit. Edinburgh [151] Cohort
Pate1 et al. (1972) [I491 Cohort
Morgan er ol. (1975) [IO41 Non-random sample; representativeness uncertain Representative sample Cohort
Pallis er 01. (1982) [I341
Bancroft et al. (1975) 1231
O’Brien, (1981) [I321
Hawton [I511
MRC Unit, Edinburgh [151] Cohort
Cohort of young adults (aged 15-30) Cohort
Hawton er al. (1982) [96]
Lendrum (1933) [93]
?ap (1958) [54]
Cohort ICI8 year olds Cohort
Non-random sample; representativeness uncertain
Edwards and Whitlock (1968) [95] Cohort
Maris (1981) [53] Cohort
Okasha and Lotaif (1979) [92] Random sample
Plawtime period
covered
Newcastle. 1966-1969 Edinburgh, I970 1971 1972 1973 1974 1975 Glasgow. 1971-1972 Bristol. 1972
Chichester. 1972-1973 Oxford. 1972-1973 London. 1975 Oxford, 1976 1977 1978 I979 I980 1981 1982 Edinburgh, 1976 1977 1978 1979 1980 1981 1982 Oxford. I979 Detroit, USA 1927-1930 Hong Kong, 1953-1954
Bnsbane. 1965-1966 Baltimore. U.S.A.. 1970 Cairo. Egypt, 1975
.V in series [males (M)
or both sexes (MF)]’
209(M)
0” of Admissions
unemployed
47
344(M) 42 439(M) 52 445(M) 47 428(M) 49 423(M) 44 430(M) 46 207(M) 55
IZI(M) 36
146(MF) 9
188(M) 15
193(MF) 48
2:3(M) 26 252(M) 26 219(M) 33 207(M) 29 205(M) 33 251(M) 39 213(M) 47
541(M) 49 522(M) 53 465(M) 47 432(M) 40 444(M) 47 571(M) 57 501(M) 62 25(MF) 28
363(M) 17t
127(MF) 28
197(M) 18
64( M F) 33
?OO(MF) 23:
*Data are given for males only, wherever possible (for reasons see text). If no separate analysis for males has been made, then data on both s&es are given.
t23% of the economically active. :53”/” of the economically active.
males who are retired is relatively small (67; of admissions in Edinburgh, 7% in Oxford, in 1981). There should be no missing data, but invariably some ‘not knowns’ are registered, especially when mass data are gathered routinely, e.g. in Oxford and Edinburgh. (However, even in these centres the pro- portion of cases rated ‘not known’ on this variable in 1981 were 0% and under I%, respectively.) The number of cases rated ‘not applicable’ will vary, depending mainly on the admission criteria to the hospital, in particular, the inclusion or exclusion of under 16 year olds. It would appear, however, that most reports in the literature concern parasuicide populations aged 15 or 16 years and over. The only study where the omission of ‘not applicable’ cases makes an appreciable difference to the quoted per- centage of unemployed is that of Okasha and Lotaif
[92]. Over half of their sample was not economically active (40”/, were students and 16.5% housewives). Thus while 23% of the total n of male and female parasuicides were unemployed, the figure for eco- nomically active parasuicides was 53%.
Most of the data in Table 4 come from British sources. As far as possible the studies are listed in chronological order of the time period covered. The few relevant non-British studies are listed at the end.
Although Table 4 has been set out in rough chronological order to help indentify trends over time, the differences in the types of sample used in the surveys makes this a rather difficult exercise. The most valid and generalisable results are undoubtedly found in the cohort studies. The first such recent studies with a reasonable sample size (Edinburgh, 196221963; Newcastle, 196221964) show identical

Unemployment and suicidal behaviour 105
percentages (34%) of male parasuicides who were unemployed on admission. Thereafter, the tendency is generally towards a higher percentage, although marked fluctuations are evident (e.g. Edinburgh, 1970-1982). The Newcastle cohort of 1966-1969 showed a rate of 477& which increased to over 50% in Edinburgh and Glasgow in 197 l-l 972. The Oxford figures are consistently and strikingly lower than those of Edinburgh over the years 1976-1982. Both series, however, show marked increases in the per- centage of unemployed male parasuicides between 1979 and 1982.
rates (males only) were 24, 149, 234 and 1186. Bancroft et al. [23] report a rate of 145 per 100,000 working males (Oxford area, 1972-I 973), compared to 361 per 100,000 males ‘seeking work, sick, other’.
Some of the studies listed in Table 4 have drawn attention to the fact that the unemployment rate among parasuicides is far greater than the un- employment rate in the general population. Thus, Lendrum [93] notes that while 22.6% of his cohort of attempted suicides were unemployed, the proportion in the population of which they were a sample was 12.2%. Bruhn [94] contrasts the figure of 43% un- employed in his sample with a figure of 17% among matched controls (psychiatric out-patients with no suicide attempt) and less than 4% for the population of Edinburgh. Edwards and Whitlock [95] found that 18% of their cohort of male parasuicides were un- employed in Brisbane, 1965-1966; the rate among general population males was 1.3% in Australia in the same year. Hawton et al. [96] state that the propor- tion of 16-18 year old parasuicides who were un- employed (28%) “was far higher than that of 16-18 year olds in the general population in the Oxford area at the mid-point of the study (7.3 per cent) [1979]“. Other authors [97,98] merely draw attention to the fact that unemployment among their sample of para- suicides is higher than expected or higher than the average in the general population, without providing exact information.
Kreitman [ 161 gives parasuicide rates among males in Edinburgh for the period 1968-1970, by employ- ment status. The rate per 100,000 employed was 92 (1 in 1088); per 100,000 unemployed it was 2444 (1 in 40), giving a ratio of nearly 27 : 1. Elsewhere I have presented data on parasuicide rates by employment status in Edinburgh over the years 1968-1982. This analysis reveals a relative risk of parasuicide among the unemployed (compared to the employed) of about 11: 1 during the period 1976-1982. A steep gradient in the relative risk ratio by duration of unemployment was noted. In 1982, Edinburgh men who had been unemployed less than 6 months ran more than six times the risk of parasuicide than did their employed counterparts. This relative risk rose to over 10: 1 among those unemployed 6-12 months, and to nearly 19: 1 among the long-term unemployed [IOO]. Preliminary results from another British study provide indirect confirmation of a relationship be- tween suicidal behaviour and duration of un- employment. Starting in September 1982, Birt has been recording, amongst other key personal data, the employment status of men aged 25-64 and women aged 25-59 becoming ill or dying on account of certain specified conditions (including poisoning) and resident within a defined geographical area (Stock- port, Greater Manchester). Analysis of the first 194 subjects entering the study show a crude incidence rate of 0.39 per 1000 employed compared to 1.07 per 1000 unemployed for less than 1 year and 1.38 per 1000 long-term unemployed. (These differences are significant; the overall rate among all unemployed was 1.18 per 1000 [IOI].)
I have located five published references to para- The evidence of the overrepresentation of the suicide rates among the unemployed compared to the unemployed among parasuicides is overwhelming; employed. Yap [54] gives details on a sample (whose clearly the relative risk of parasuicide is very much representativeness is uncertain) of attempted suicides elevated for the unemployed compared to the em- in Hong Kong, 1953-1954. The unemployed consti- ployed. But is joblessness a significant aetiological tuted 28% of the sample but only 13% of the popu- factor, and if so, in what way? Cross-sectional sur- lation (both sexes, 15 years and over). Although no veys of parasuicide populations cannot, as we have attempted suicide rate is given for the employed as a seen, provide definitive answers to these questions, group, rates are given for individual occupations. The but they can give some useful pointers to possible rate for the unemployed (23.9 per 100,000) is second associations between parasuicide and unemployment. only to the rate for businessmen (36.5); no other rate For instance, we can examine the extent to which is above 16 per 100,000. Kessell et al. [99] showed that unemployment is given as an immediate cause of in a provincial region of Victoria, Australia, the parasuicide. A number of studies have examined the attempted suicide rate of the unemployed over the events leading up to the parasuicide and Table 5 years 1971-1972 was 2686 per 100,000 unemployed provides evidence of the frequency with which un- males (1 in 37), more than nineteen times the average employment or associated socio-economic factors are rate of 137 per 100,000 males. The incidence in a judged to have been major precipitants. However, metropolitan region of Victoria was 1186 per 100,000 before accepting at face value the findings presented males (1 in 84), more than eleven times the area in Table 5, a certain number of difficulties should be incidence of 100 per 100,000 males. The rates of noted. Firstly, studies differ in the meaning given to attempted suicide among unemployed men and ‘unemployment’ and in the range of problems which women were very similar. When the employed group I have included under the rubric ‘related socio- was differentiated into different occupational catego- economic factors’. Secondly, none of the studies ries, the contrast with the unemployed is even more listed presents a clear account of the manner in which striking. Thus, the suicide attempt rate per 100,000 the rating is made. Is the parasuicide directly asked males in the provincial region was 21 for about the events which precipitated the overdose? If professionals/managers: 109 for white-collar workers; so, how? Is his reply accepted and recorded, or merely 234 for blue-collar workers; and 2686 for the un- used as a guide by’ the interviewer? If the parasuicide employed. In the metropolitan region the respective is not asked, how is the information gathered?
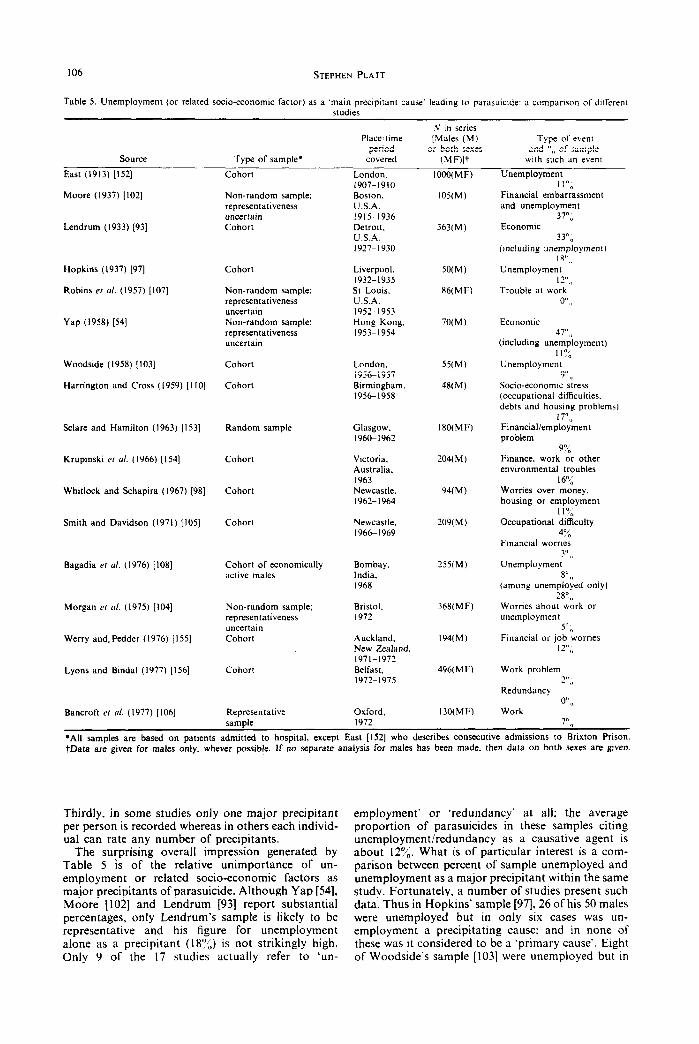
106 STEPHEN PLATT
Table 5. Unemployment (or related so&-economic factor) as a ‘main precipitant cause’ leading to parasuicide: a comparison of dllrcrent studies
Source Type of sample*
Place:time period
covered
.V in series [Males (M)
or both sexes
(MF)lt
Type of e\ent and “,, of sample
wth such an event
East (1913) [I521
Moore (1937) [IO21
Cohort
Lendrum (1933) [93]
Non-random sample; representativeness uncertain Cohort
Hopkins (1937) [97]
Robins er c/l. (1957) [IO71
Cohort
Yap (1958) [54]
Non-random sample: representativeness uncertain Non-random sample; representativeness uncertain
Woodside (1958) [IO31
Harrington and Cross (1959) (I IO]
Cohort
Cohort
Sclare and Hamilton (1963) [ 1531 Random sample
Krupinski et crl. (1966) [I541 Cohort
Whitlock and Schapira (1967) [98] Cohort
Smith and Davidson (1971) [IO51 Cohort
Bagadia Ed 01. (1976) [ IOS] Cohort of economically active males
Morgan er al. (1975) [IO41
Werry and. Pedder (1976) [I551
Non-random sample; representativeness uncertain Cohort
Lyons and Bindal (1977) [I561 Cohort
Bancroft er crl. (1977) [ 1061 Representative vamole
London. 1907-1910 Boston. U.S.A. 1915-1936 Detroit. U.S.A. 1927-1930
Liverpool, 1932-1935 St Louis. U.S.A. 1952-1953 Hong Kong. 1953-1954
London. 19561957 Birmingham. 19561958
Glasgow, 1960-1962
Victoria. Australia. I963 Newcastle. 1962-1964
Newcastle, 1966-1969
Bombay, India. 1968
Bristol, I972
Auckland. New Zealand. 1971-1972 Belfast. 1972-1975
Oxford. I972
IOOO(MF)
105(M)
363(M)
50(M)
86(MF)
70(M)
55(M)
48(M)
180(MF)
204( M )
94(M)
209(M)
255(M)
368(MF)
194(M)
496(MF)
130(MF)
Unemployment I I”,
Financial embarrassment and unemployment
37”, Economic
33”, (m&ding unemployment)
Iv,, Unemployment
Iz” 0 Trouble at work
o”,,
Economic 47”,,
(including unemployment) I I”,
Unemployment
9” I, Socio-economic stress (occupational difficulties. debts and housing problems)
I7”0 Financial/employment problem
90’ Finance, work zr other environmental troubles
16% Worries over money, housing or employment
I IS, Occupational difficulty
4% Fmanclal worrxs
Unemploymen:“”
8” I, (among unemployed only)
28”,, Worries about work or unemployment
5” 0 Financial or job worries
12”,,
Work problem ?” 0
Redundancy
0” I, Work
7””
*All samples are based on patients admitted to hospital, except East [I521 who describes consecutive admissions to Brixton Prison. tData are given for males only, whever possible. If no separate analysis for males has been made, then data on both sexes are given.
Thirdly, in some studies only one major precipitant per person is recorded whereas in others each individ- ual can rate any number of precipitants.
The surprising overall impression generated by Table 5 is of the relative unimportance of un- employment or related socio-economic factors as major precipitants of parasuicide. Although Yap [54], Moore [IO21 and Lendrum [93] report substantial percentages, only Lendrum’s sample is likely to be representative and his figure for unemployment alone as a precipitant (18’J$ is not strikingly high. Only 9 of the 17 studies actually refer to ‘un-
employment’ or ‘redundancy’ at all; the average proportion of parasuicides in these samples citing unemployment/redundancy as a causative agent is about 12’7& What is of particular interest is a com- parison between percent of sample unemployed and unemployment as a major precipitant within the same study. Fortunately, a number of studies present such data. Thus in Hopkins’ sample [97], 26 of his 50 males were unemployed but in only six cases was un- employment a precipitating cause; and in none of these was it considered to be a ‘primary cause’. Eight of Woodside’s sample [IO31 were unemployed but in

Unemployment and suicidal behaviour 107
only five cases was unemployment a ‘precipitating stress’. Whitlock and Schapira [98] report that 34% of their sample of males were unemployed but only I 1% registered ‘worries over money, housing or employ- ment’ as a ‘main precipitant cause’ of the suicide attempt. Although 36% of Morgan’s sample [104] were unemployed, only 5% claimed that ‘worries about work or unemployment’ triggered that para- suicidal act. Similar discrepancies are found in the studies by Smith and Davidson [ 1051, Bancroft et al. [106] and Yap [54]. Robins ef al. [107] note that although 41 out of 86 patients admitted to hospital after a suicide attempt had experienced ‘job difficulties’ in the 6 months prior to the suicide attempt (i.e. quitting work, being fired, being de- moted, excessive friction with others at work), ‘trouble at work’ was never given by the patient as a main reason for his behaviour. According to Bagadia et al. [log], “unemployment was the cause for at- tempted suicide in only 27.8% of the unemployed group”. The only exception to this pattern is pro- vided by Lendrum [93], who found that while 63 out of 363 male attempted suicides were unemployed (with a further 76 cases rated ‘not known’ on employ- ment status), 66 mentioned unemployment as a mo- tive for their suicidal behaviour! Otherwise, it would appear that while a significant proportion of para- suicides are unemployed on admission to hospital, only a limited number claim that the state of being unemployed is of significance as an immediate cause or precipitant of their suicidal behaviour. Certainly, unemployment appears to be unimportant as a major precipitant, both absolutely and relative to other precipitants. Virtually all studies reach the conclusion that the most important single type of triggering event in parasuicide is ‘interpersonal conflict’, a broad category which includes marital discord, kin disharmony, broken/unhappy love affair, dispute with parents, infidelity, etc. [98, 104, 109-l 131. The relative importance of interpersonal conflict and socio-economic factors (including unemployment) as precipitants of parasuicide are demonstrated in a number of studies. To take only two examples, 65% of a representative sample of suicide attempters in Oxford experienced an event (usually a quarrel) involving a ‘key person’, whereas only 7% experi- enced events in the ‘work’ category [106]. Among parasuicide admissions to Bristol Royal Infirmary, 510/L described a major precipitating factor involving interpersonal conflict, whereas only 5% referred to worries about work or unemployment [104].
Type 2 studies (aggregate-cross-sectional)
Macro-level analysis of the relationship between unemployment and parasuicide has been extremely limited. Buglass and Duffy [64] demonstrate the existence of a significant association between para- suicide and unemployment (men seeking work, women seeking work and unemployment in young people) across twenty-three city wards in Edinburgh, 1968-73. Significant ecological correlations for the same town in 1973 alone are also reported, in this case between parasuicide and men and women (sepa- rately) seeking work [63]. In both these studies the correlation was higher for men seeking work than for women seeking work. Bagley ef al. [28] also report a
significant positive correlation between parasuicide rates and percent unemployed across nineteen wards in Brighton, 1966-68. It is noteworthy that the studies in both Edinburgh and Brighton also show high correlations between parasuicide and indicators of poverty (e.g. free school meals, non-payment of electricity bills, clothing grants, no inside W.C., no hot tap); and, in Edinburgh alone, parasuicide is linked to juvenile delinquency (e.g. truancy, children referred to the Reporter). Buglass and Duffy [64] characterise the areas where parasuicide is common, and suicide relatively rare, as “lower class districts with associated problems of unemployment, poverty and juvenile delinquency”.
Type 3 studies (individual-longitudinal)
Fruensgaard et al. [114] report on the psycho- logical characteristics of 70 unemployed patients (47 men, 23 women) admitted to a psychiatric emergency department in Odense, Denmark. The main reason for admission in about half the sample was suicidal behaviour. It was, estimated that for 41% of the whole sample unemployment had played an important part in the current psychiatric illness, although for only 11% was it the sole etiological factor. Other poten- tially causal external factors were also registered in three-quarters of the sample. “It seemed that un- employment was most often one of several stressing facets of a complicated interplay” (p. 143). In the case of suicidal behaviour, the authors claim that “un- employment is a significant external factor. . . . How- ever, this effect of unemployment seems most often to be interrelated with other external factors” (p. 144).
No other relevant individual-longitudinal study (where parasuicide is the behavioural outcome measure) is known to the author.
Type 4 studies (aggregate-longitudinal)
In view of the absence of any formal analysis of the relationship between parasuicide and unemployment, I have examined the relevant data for Edinburgh [loo]. Table 6 presents a summary of the main findings. It reports the male parasuicide person rate, the male unemployment rate and the percentage of economically active male parasuicides who were un- employed on admission, for the years 1968-1982. The rank ordering for each variable across the years is given in parenthesis. Unemployment rate is cor- related significantly with both the parasuicide (per- son) rate (r,, = 0.88, P < 0.001) and with percent of admissions who were unemployed (rr = 0.75, P < 0.01). When unemployment is lagged one year, both correlations are reduced but still significant (r,?=O.71, P co.01 and r,Y= 0.56, P < 0.05, re- spectively).
DECUSSION
The main findings that emerge from the preceding review of the literature on the relationship between unemployment and suicidal behaviour can be briefly summarised. The cross-sectional individual studies reveal that significantly more (para)suicides are un- employed than would be expected among general population samples. Likewise, (para)suicide rates among the unemployed are always considerably

108 STEPHEN PLAIN
Table 6. Male unemployment and parasuicide in Edinburgh: 1968-1982
“; of economically active Male parasuicide (person) Male unemployment rate male parasuicides who were
rate (per 1O4J.000)* (“:)t unemployed on admission Year (rank) (rank) (rank)
1968 157 ---2.7 (15) (15) -44.7 (11) I969 172 (14) 3.3 (14) 40.2 (15) 1970 185 (13) 4.5 (12) 43.1 (12) 1971 218 (9) 5.6 (8.5) 54.2 (3) I972 223 (61 5.6 (8.5) 47.1 (6) 1973 207 (11) 4.6 (11) 46.7 (7) 1974 208 (10) 4.4 (13) 42.3 (13) 1975 201 (12) 5.4 (10) 45.2 (10) 1976 247 (2) 6.7 (7) 45.9 (9) 1977 237 (3) 8.0 (31 50.3 (4) 1978 219 (7.5) 7.2 (5) 46.0 (8) 1979 219 (7.5) 6.8 (6) 41.0 (14) 1980 226 (5) 7.7 (4) 49.2 (5) 1981 269 (1) 10.6 (2) 57.4 (2) 1982 229 (4) 12.8 (1) 63.2 (1)
*Mean rate per 100,000 for hospital&d male parasuicides. Edinburgh residents only, 2 I5 years old. The boundaries of the city of Edinburgh were enlarged in 1974. resulting in an increase of 5.5% in the total population. The detinition of an “Edinburgh resident” was changed accordingly. The Resistrar General’s mid-year estimate of the male population in Edinburgh aged b I5 years was used as the denominator in the calculation of the rate.
tMales registered with local employment and career services offices covering the Edinburgh. Portobello and Leith employment exchange areas on census day (June) as percentage of all male employees in employment and those registered as unemployed in the same area.
higher than among the employed. Increasing du- ration of unemployment is associated with increasing risk of parasuicide. Type 2 (aggregate-cross- sectional) studies provided no evidence of a con- sistent relationship between unemployment and completed suicide, but a significant geographical association between unemployment and parasuicide rates was found. Results from a!! but one of the individual longitudinal studies point to significantly more unemployment, job instability and occupa- tional problems among suicides compared to non- suicides. The exception is the investigation by Borg and Stahl [7S] which identified (nonsignificantly) more ‘problems at work’ among controls than among suicides (both samples coming from a psychiatric population). The OPCS longitudinal study [76] also found a high suicide rate among the unemployed in the general population. The aggregate longitudinal (Type 4) analyses point to a significant positive association between unemployment and suicide in the United States of America. The negative relationship in Great Britain in the 1960s has been shown to result from a unique decline in the suicide rate due to the unavailability of the most common method of suicide [85, 861.
On the relationship between unemployment and suicide
Despite this plethora of. research findings, a definitive choice between the competing self-selection and causal models remains highly problematic. We can confidently state that there is an association between uhemployment and suicide but we cannot specify with the same degree of confidence the nature of this association. My own interpretation of the evidence is that empirical support for a direct causal link at the individual level between unemployment and suicide is weak. Attempts to abandon completely any element of self-selection in the suicide- unemployment relationship lack credibility because they fail to take cognizance of one crucial fact: namely, that “although mental illness is not a
sufficient cause of suicide, it is for al! practical purposes in modern Western culture probably a necessary one” [115]. Retrospective studies by Bar- raclough et al. [116], Robins et al. [ 1171 and Dorpat and Ripley [118] show that over 90% of suicide victims are suffering from a major psychiatric illness (most frequently depression but often alcoholism) at the time of death. In his review of the evidence concerning conditions predisposing to suicide, Miles [1!9] concludes that virtually all the suicides in the United States can be attributed. to the following causes: depressive illness, alcoholism, schizophrenia, neurosis and personality disorder and drug addiction.
Even if this conclusion is considered to be valid [120], it does not ipsofacto rule out the possibility that it is the individual’s experience of unemployment which increases his/her vulnerability to psychological distress and psychiatric illness, and therefore the risk of suicidal behaviour. Indeed, recently Banks and Jackson [121] have demonstrated a definite causal link between unemployment in young school-leavers and increased psychiatric symptoms (measured by the twelve-item General Health Questionnaire); they also rule out the likelihood of the reverse causation hy- pothesis, i.e. that the psychologically disturbed can- not find jobs. However, this finding cannot neces- sarily be generalised to other older populations, and the data do not allow a reliable estimate to be made of the extent to which unemployment in the sample was associated with serious psychiatric disorder. About 40% of the unemployed were found to score above the threshold point on the GHQ- 12, compared to about 13% of the employed (and up to 20% in other general population surveys) [ 1221. This does not mean that 40”/, of the unemployed were psychiatric cases. It merely indicates that among these individu- als there was a moderate probability of being found on detailed assessment to be psychiatrically ill. In fact, most of the psychiatric symptomatology was probably mild and transient; Warr reports that when those previously unemployed find work again there is
Unemployment and suicidal behaviour I 09
a highly significant reduction in their mean GHQ score [ 1221.
The results of this type of investigation are there- fore of doubtful relevance for our understanding of the association between unemployment and suicide. Close scrutiny of Type 1 studies leads to the conclu- sion that among those who eventually commit suicide the temporal and causal sequence of events is quite different from the sequence sketched in the model above. Rather than unemployment leading to psychiatric illness and thereafter to suicide, there is more evidence in favour of the alternative model:
Psychiatric illness p Unemployment
1 Suiiide
As we have seen, detailed analyses of individual case histories by Tuckman and LavelI[31], Ovenstone [59], Yap [54], Stearns [58] and Breed [30], among others, lend strong support to the proposition that un- employment in suicide victims is to a large extent a consequence or reflection of an underlying psychiatric disorder: rather than unemployment be- ing a cause of psychiatric illness and suicide, it is more likely that the risks of both unemployment and suicide are elevated by the presence of a major psychiatric illness (in particular, depression). This conclusion is in line with Shepherd and Barraclough’s speculation that the high prevalence of psychiatric ill-health among their sample of suicides
“may also have been implicated in the higher rate of unemployment and greater number of job changes. . . Rather than their [the suicides’] work loss resulting from broad social and economic trends, it is more likely that their psychiatric morbidity interfered with their capacity for work, resulting in work loss with its attendant disadvan- tages, so that mental illness at once stimulated in them suicidal thinking and at the same time took away from them an effective protection against suicidal behaviour” [69].
The connection between unemployment and suicide (presented as a dashed line in the scheme above) reminds us of the fact that, while psychiatric illness may be directly implicated in suicidal behaviour, it may also operate via unemployment. In particular, the psychological consequences or correlates of pro- longed unemployment would appear to be likely to exacerbate the pre-existing psychiatric condition. The long-term unemployed are not only more vulnerable to, and less protected against, stressful life events and difficulties but also face more of these stressors by virtue of being without work. The effects of the psychiatric condition will be potentiated by the inter- action between symptoms, stress and vulnerability.
Thus far we have only considered individual-level (Type 1) studies which necessarily ignore the role of the economic climate. How, then, can we incorporate our conclusions about the relationship between suicide and unemployment at the individual level with the abundant evidence of a temporal association between suicide and the macro-economy, in a more complete model of the pathways to suicide? A simplified version of such a model may be roughly
sketched as follows. Macro-economic conditions. al- though not directly influencing the suicide rate, may nevertheless constitute an important antecedent vari- able’ in the causal chain leading to self-harmful behaviour. Consequent upon a deepening economic recession, individuals are subjected to greater levels of psychosocial stress. The experience of severe, undesirable life events and difficulties becomes more widespread leading to an increase in psychological disturbance and acute psychiatric illness in the most vulnerable individuals (some of whom may have previously enjoyed excellent psychological health) [123]. Even if a constant proportion of the psychiatric population becomes suicidal (irrespective of the eco- nomic climate), then as the pool of psychiatric cases enlarges the number of suicides (and therefore the suicide rate) will automatically rise [124]. The addi- tional psychiatric disorder ‘provoked’ by the eco- nomic recession may indeed be found dis- proportionately among the unemployed, causing an increase in the relative risk of psychiatric illness and suicide among the unemployed compared to the employed. (It would be a matter of considerable theoretical and practical significance to discover whether the increased suicide risk was associated with recent job loss or with long-term unemployment.) On the other hand, the health effects of the recession may be more pronounced among the currently employed, inasmuch as they become anxious about job security and anticipate some future negative changes in their lifestyle, standard of living, feelings of ‘happiness’, etc. arising out of the instability of the macro- economy [ 1251. If this were the case, we would expect to find that the relative risk of psychiatric illness and suicide among the unemployed (compared to the employed) would remain stationary or even decrease. due mainly to a rise in psychopathology among the employed. This trend might well be accentuated by the tendency for some workers made newly un- employed or redundant to experience relief rather than distress at their change in employment status. It is commonly assumed that all employment is ‘good’ and all unemployment ‘bad’. But unemployment may be ‘good’ for individuals tiho suffer from ‘bad’ employment, i.e. jobs that are inherently stressful or psychologically demeaning or subject to insecurity of tenure, or involve continual change of work environ- ’ ment or require some degree of pliysical separation and isolation from others [126].
On the relationship between unemployment and para- suicide
If the data permitted only the roughest outline of a model describing the pathways between economic climate and suicide, then any attempt to delineate the nature of the relationship between unemployment and parasuicide must be even more tentative. There is only one published study which uses a longitudinal design, and only two independent aggregate cross- sectional studies. We therefore have to rely almost exclusively on cross-sectional surveys of parasuicidal populations. On the available evidence, can we re- solve thz self-selection vs causal argument?
One point of interest is the discrepancy between the over-representation of the unemployed among the parasuicides, on the one hand, and the infrequent

110 STEPHEN PLATT
reference to unemployment as a major precipitating cause of parasuicide, at least by those who have committed the act, on the other. This somewhat paradoxical finding does not in fact rule out un- employment as a significant aetiological factor in parasuicide. It has already been pointed out that the rating of ‘precipitants’ of parasuicide is extremely problematic. In addition, the ‘perceptual set’ of psychiatrists may encourage a selective tendency to disregard social factors as precipitants in the quest to demonstrate ‘what everyone already knows’, i.e. in- terpersonal strife is the main event leading to para- suicide. There is also the possibility that, just as motives for behaviour tend to be formulated accord- ing to their likely acceptability to the person’s rele- vant audience [ 1271, so ‘causes’ or ‘precipitants’ might also be reported differentially according to their perceived acceptability in the hospital setting. On this latter point, however, it is difficult to see why inter- personal conflict should be considered more desirable as an excuse or justification [ 1281 for parasuicide than (recent) unemployment. On the former point- concerning psychiatrists’ ‘perceptual set’-the im- portance of interpersonal conflict as the major precip- itant has been demonstrated in so many studies in many different countries, and over at least a quarter of a century, that it appears to be a reliable and valid finding.
However, if unemployment is not a triggering or precipitating event, it could be aetiologically significant as a predisposing factor. That is to say, unemployment may be parasuicidogenic, not in the sense of being a ‘provoking agent’, but as an ongoing situation causing vulnerability which will increase the risk of suicidal behaviour when a provoking agent is present. (Unemployment may, of course, also have more than one aspect of causal importance: it may act as a provoking agent in some cases and a vulner- ability factor in others [129].) Thus, prolonged un- employment may be a significant predisposing factor in suicidal behaviour because it leads to: an increase in family tensions, arguments and violence; more depression and haplessness; increasing isolation from others; changes in role structure within the family; financial hardship and marital deprivation; loss of self-esteem and self-confidence; and feelings of re- duced self-worth; or any combination of these se- quelae. A provoking agent (e.g. argument with spouse) would be more likely to lead to parasuicide in the presence of unemployment (and its associated behavioural correlates) than in its absence.
This causal model of unemployment as a vulner- ability factor, or long-term difficulty, rather than as a crisis event, requires evidence that joblesness among parasuicides is not a recent condition and is of significantly longer duration than would be expected among the unemployed in the general population. The scanty data available on this important issue does indeed show that the long-term unemployed are significantly overrepresented in the parasuicide popu- lation [IOO, 104, 1051. However, while this finding supports the vulnerability (causal) model, it is of course also compatible with the possibility that cer- tain individuals are at risk of both long-term un- employment and parasuicide by virtue of certain personal characteristics. Although there is not such a
close association between parasuicide and psychiatric illness as was found for suicide, nevertheless surveys of parasuicides have repeatedly claimed that the majority of hospital-based cases are suffering from one or more of the following: a recognised psychiatric illness (usually depression). a personality disorder. alcoholism or alcohol abuse, or habitual drug misuse [ 1301. Furthermore, comparison between employed and unemployed parasuicides shows that significantly more of the unemployed have a previous history of parasuicide and psychiatric treatment; are classified as personality disordered or alcoholic: report a his- tory of family suicide or parasuicide: have behaved violently towards others in the past 5 years; disclose a previous criminal record and face police pro- ceedings at the time of admission; have a problem in the use of alcohol; and habitually misuse drugs [ 13 I]. These cross-sectional data certainly appear to fit well with the expected pathways of a self-selection model. O’Brien [132], for instance, concludes that the discov- ery of a relationship between previous overdose. personal disorganisation and unemployment in her sample of young adult parasuicides
“suggest[s] that unemployment may be a result of difficulties rather than the main cause. People suffering from emotional instability, and maybe alcohol or drug problems. will have difficulty in maintaining a job. or seeking employment”.
Yet, again, the evidence can be shown to be far from conclusive. For instance, very few parasuicide pa- tients are likely to be suffering from severe psychiatric illnesses [133] and most psychopathology has been shown (by Newson-Smith and Hirsch [130]) to be shortlived. Moreover, the significant differences be- tween employed and unemployed parasuicides could equally well arise because long-term unemployment leads to more interpersonal violence, psychiatric treatment, etc.
It would appear, then, that we are far from under- standing the nature of the relationship between un- employment and parasuicide. Further progress on model-building is unlikely until we have carried out- more empirical research based on a longitudinal design, at both the aggregate and individual levels. Admittedly, a prospective cohort study of parasuicide is not a practical or feasible proposition, but retro- spective data on reasons for unemployment, duration of unemployment and previous job history should be obtained in order to test out the importance of personality variables in both unemployment and parasuicide. A controlled retrospective longitudinal study similar to that conducted by Shepherd and Barraciough [69] on completed suicides is an urgent requirement in this area of research.
Acknowledgements-I received considerable help from a number of individuals in the course of preparing this review. In particular I would like to thank Mr Hugh O’Donnel of the Manpower Services Commission, Edinburgh. Mr Jim Connell of the Department of Physical Planning, Lothian Regional Council and Mr A. Spence of the Department of Employment, who all provided me with data on un- employment. Dr Keith Hawton, Department of Psychiatry. Warneford Hospital, Oxford, generously supplied me with unpublished data on the employment status of attempted suicides admitted in Oxford. The present revised version has benefited considerably from the constructive criticrsm of Dr

Unemployment and suicidal behaviour III
Norman Kreitman (Medical Research Council Unit for and suicidal behaviour in Hobart. Ausr. N.Z. JI Epidemiological Studies in Psychiatry, Edinburgh) and Mr Mike Porter (Department of General Practice, University of
Psychiar 10, 237-242, 1976; Lester D. Relation be-
Edinburgh). Dr David Dooley (Public Policy Research tween attempted suicide and completed suicide. Psy-
Organization, Program in Social Ecology, University of chol. Rep. 27, 719-722, 1970; Lester D. Why People
California, Irvine) kindly brought to my attention a number Kill Themselves: A Summary qf Research Findings on
of relevant references I had originally missed. Suicidal Behauiour. Charles C. Thomas, Springfield, IL, 1972.
5.
6.
7.
8.
9.
IO.
11.
12.
13.
14.
15.
16.
17.
REFERENCES
House of Commons Parliamentary Debates (Han- sard), 37 (67). 366 (3 March 1983). Falret J. P. De L’hyponchondrie el du Suicide. Paris, 1822. Durkheim E. Suicide, p. 241. Routledge & Kegan Paul, London, 1952 (1897). Brenner M. H. Estimating the social costs of national policy: implications for mental and physical health, and criminal aggression. Joint Economic Committee of Congress Paper No. 5, U.S. Government Printing Office. Washington, DC, 1976. Brenner M. H. Mortality and the national economy: a review. and the experience of England and Wales, 1936-76. Lancer 2, 568-573. 1979. Gravelle H. S. E., Hutchinson G. and Stern J. Mor- tality and unemployment: a critique of Brenner’s time- series analysis. Lancer 2, 675-679, 1981. Eyer J. Review of ‘Mental Illness and the Economy’. Inr. J. Hlth Serc. 6, 139-148, 1976. Eyer J. Prosperity as a cause of death. In!. J. Hlth Serc. 7, 125-150, 1977. Eyer J. Does unemployment cause the death rate peak in each business cycle? A multifactor model of death rate change. Int. J. Hlrh Sert>. 7, 625-662, 1977. Lancer (editorial). Does unemployment kill? Lance1 1, 708-709. 1979. Brenner M. H. Health costs and benefits of economic policy. Inr. J. Hlth Sew. 7, 581-623. 1977. The term ‘parasuicide’. coined by Kreitman N., Philip A. E., Creer S. and Bagley C. R. (Parasuicide (letter). Br. J. Psychiar. 115, 746-747, 1969). refers “to a behavioural analogue of suicide but without consid- ering a psychological orientation towards death being in any way essential to the definition”. It replaces the term ‘attempted suicide’ which has been extensively criticised on the grounds that is assumes an intention to die is always present in such behaviour. (see e.g. Kessel N. Self-poisoning. Br. med. J. 2, 1265-1270 and 1336-1340. 1965.) Shneidman E. S. Orientation toward death: a vital aspect of the study of lives. Inr. J. Psvchiat. 2,167-200, 1966. Kessel N. The respectability of self-poisoning and the fashion of survival. J. Psychosomat. Res. 10, 29-36, 1966. Stengel E. and Cook N. G. Attempted Suicide, Its Social Significance and Effects. Chapman & Hall, London, 1958. ’ e.g. Kreitman N. Social and clinical aspects of suicide and arrempted suicide. In A Companion to Psychiatric Studies (Edited by Forrest A.), Vol. 1, pp. 38-63. Churchill Livingstone, Edinburgh, 1973; Birtchnell J. and Alarcon J. The motivation and emotiohal state of 91 cases of attempted suicide. Br. J. med. Psycho/. 44, 45-52, 1971; Bancroft J.. Skrimshire A. and Simkin S. The reasons people give for taking overdoses. Br. J. Psl,chiar. 128. 538-548, 1976; Bancroft J.. Hawton K.. S&kin S.. Kingston B.. Cumming C. and Whitwell D. The reasons people give for taking overdoses: a further Inquiry. Br. J. med. Psychol. 52,353-365, 1979; Stengel E. The complexity of motivations to suicide attempts. J. men/. Sri. 106, 1388-1393, 1960. There are, however, some dissenting views, See e.g. Koller K. M. and Cotgrove R. C. M. Social geography
18
19
20
21.
22.
23.
24.
25.
26.
27.
28.
Freeman D. J., Wilson K. Thigpen J. and McGee R. K. Assessing intention to die in self-injury behav- iour. In Psychological Assessment of Suicidal Risk (Edited by Neuringer C.), pp. 18-42. Charles C. Thomas, Springfield, IL, 1974. See, for example, Kreitman N. The epidemiology of suicide and parasuicide. Crisis 2, l-l 3, 1981; Ovenstone I. M. K. Spectrum of suicidal behaviours in Edinburgh. Br. J. prev. Sot. Med. 27, 27-35, 1973; Dorpat, T. L. and Ripley H. S. The relationship between attempted suicide and committed suicide. Compr. Psychiat. 8, 74-79, 1967; Wilkins J. Suicidal behaviour. Am. sociot. Reo. 32, 286-298, 1967; Kennedy P., Kreitman N. and Ovenstone I. M. K. The prevalence of suicide and parasuicide (‘attempted sui- cide’) in Edinburgh. Br. J. Psychiar. 124, 36-41, 1974; Shneidman E. S. and Farberow N. L. (Eds) Statistical comparisons between attempted and committed sui- cides. In. The Crv for He/n DD. 19-47. McGraw-Hill. New York, 196i;-Weiss 3. ‘G. A. The gamble with death in attempted suicide. Psychiarry 20 17-25, 1957; Gibbs J. P. (Ed.) Suicide. Harper & Row, New York, 1968; Schmid C. and van Arsdol M. D. Completed and attempted suicides: a comparative analysis. Am. social. Rev. 20, 273-283, 1955. For useful summaries of these differences see Kreitman N. op. cit., 1973, 1981; Kreitman N. and Dyer J. A. T. Suicide in relation to parasuicide. Medicine 36, 1827-1830, 1980. Space precludes consideration of anecdotal, literary or qualitative approaches to this topic. Dooley D. and Catalan0 R. Economic change as a cause of behavioural disorder. Psychol. Bull. 87, 450-468, 1980. See, for example, differences between Oxford and Edinburgh discussed in Bancroft, J., Skrimshire A., Reynolds F.. Simkin S. and Smith J. Self-noisonine and self-injury in the Oxford area: epidemiologic2 aspects 1969-73. Br. J. prec. Sot. Med. 29, 170-177, 1975. See Rosenberg M. The Logic of Survey Analysis. Basic Books, New York, 1968; and Susser M. Causal Think- ing in the Health Sciences: Concepts and Strategies of Epidemiology. Oxford University Press, London, 1973, among others, for extended discussions on the meth- ods used to screen causal models for extraneous fac- tors. Goodman L. A. Ecological regressions and behaviour of individuals. Am. social. Rev. 18. 663-664. 1953: Robinson W. S. Ecological correlations and the’behav: iour of individuals. Am. social. Ral. 15, 351-357, 1950; Selvin H. C. Durkheim’s ‘Suicide’ and problems of empirical research. Am. J. Social. 63, 607-619, 1958. Morganstem H. Uses of ecological analysis in epi- demiological research. Am. J. publ. Hlrh 72, 1336-1344, 1982; Firebaugh G. A rule for inferring individual-level relationships from aggregate data. Am. social. Rec. 43, 557-572, 1978. Philip A. E. and McCulloch J. W. Use of social indices in psychiatric epidemiology. Br. J. prec. Sot. Med. 20, 122-126. 1966; McCulloch J. W. and Philip A. E. Social variables in attempted suicide. Acta psychiar. stand. 43, 341-346, 1967. Bagley C., Jacobson S. and Palmer C. Social structure and the ecological distribution of mental illness. sui- cide and delinquency. Psychol. Med. 3, 177-l 87, 1973.

STEPHEN PLATT 112
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
49.
50.
51.
52.
53.
e.g. Sainsbury P. Suicide in London. Chapman & Hall, London, 1955. Breed W. Occupational mobility and suicide among white males. Am. social. Rea. 28, 179-188. 1963. Tuckman J. and Lavell M. Study of suicide in Philadel- phia. Publ. Hlrh Rep. 73, 547-553, 1958. MacMahon B. and Pugh T. F. Epidemiology: Prin- ciples and Methods. Little, Brown, Boston. 1970. Exceptionally, the data are presented as raw fre- quencies rather than rates (e.g. Swinscow D. Some suicide statistics. Br. med. J. 1. 1417-1422, 1951). Cook T. D., Dintzer L. and Mark M. M. The causal analysis of concomitant time series. Appl. sot. Psychol. Ann. 1, 93-135, 1980. Mark M. The causal analysis of concomitancies in time series. In Quasi-Experimentarion (Edited by Cook T. D. and Campbell D. T.), pp. 321-339. Houghton- Mifflin, Chicago, 1979. Box G. E. P. and Jenkins G. M. Time Series Analysis: Forecasting and Control. Hoiden-Day, San Francisco, 1976. Brenner M. H. Estimating the health costs of national economic policy in Scotland, 1950-1980. Paper presented at Conference on Unemployment and Health: The Scottish Perspective, Glasgow, 1981. Vigderhous G. and Fishman G. The impact of un- employment and familial integration on changing sui- cide rates in the U.S.A., 1920-1969. Sot. Psvchiur. 13, 239-248, 1978. Hammermesh A. S. and Soss. N. M. An economic theorv of suicide. J. Dolit. Econ. 82, 83-98, 1974. Sprui; I. P. Unemployment and health in macro-social analysis. Sot. Sci. Med. 16, 1903-1917. 1982. Kasl S. V. Mortality and the business cycle. Some questions about research strategies when utilising macro-social and ecological data. Am. J. publ. Hlrh 69, 784-788, 1979. Kasl S. V. Strategies of research on economic instabilitv and health. Psvchol. Med. 12, 637-649, 1982. . Stern J. Unemployment and its impact on morbidity and mortalitv. Centre for Labour Economics, L. S. E. Discussion Paper No. 93, London, 1981. Stern J. Does unemployment really kill? New Sot. 60,
421422, 1982. Pollack E. S. Book Review ‘Mental Illness and the Economy’. Am. J. publ. Hlth 64, 512-513, 1974. Colledge M. Economic cycles and health. Towards a sociological understanding of the impact of the re- cession on health and illness. Sot. Sci. Med. 16, 1919-1927, 1982. Marshall J. R. and Funch D. P. Mental illness and the economy: a critique and partial replication. J. Hlfh sot. Behac. 20, 282-289, 1979. Brenner M. H. Mental Illness and the Economv. Har- vard University Press, Cambridge, MA, 1973. Marshall J. R. and Hodge R. W. Durkheim and Pierce on suicide and economic change. Sot. Sci. Res. 10, 101-I 14, 1981. Pierce A. The economic cycle and the social suicide rate. Am. social. Reu. 32, 457462. 1967. Robin A. A., Brooke E. M. and Freeman-Browne D. L. Some aspects of suicide in psychiatric patients in Southend. Br. J. Psvchht. 114. 739-747, 1968. Roy A. Risk factors-for suicide in psychiatric patients. Archs gen. Psychiar. 39, 1089-1095. 1982. Although Breed [30] interviewed 206 controls (each suicide being matched by sex, race and age with two controls), no information on their employment status is presented in this report: and no comparison with the general population is made. Maris’s sample of national deaths is not matched to his sample of suicides (Maris R. W. Parhwqs to Suicide: A Surcey of Self-
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
71
72
Destrucrice Behariors. Johns Hopkins University Press, Baltimore, MD. 1981). Yap P. M. Suicide in Hong Kong. J. men/. Sci. 104. 266-301. 1958. Cumming E.. Lazar C. and Chisholm L. Suicide as an index of role strain among employed and not em- ployed married women in B;itish’Coiombia. Gun. Ret,. Social. Anthrov. 12. 463-469. 1975. Kraft D. P. and Babigian H. M. Suicides by persons with and without psychiatric contacts. .drchs gen. Psychiat. 33, 209-215. 1976. Iga M., Yanamoto J., Noguchi T. and Koshinaga J. Suicide in Japan. Sot. Sci. Med. 12. 507-516. 1978. Stearns A. W. Suicide in Massachusetts. Men!. Hyg. 5. 752-777, 1921. Ovenstone I. M. K. An epidemiological study of suicidal behaviours in Edinburgh. M.D. thesis. Umver- sity of Edinburgh, 1972. Sathyavathi K. Suicide among unemployed persons in Bangalore. Indian J. sot. Work 37, 385-392. 1977. Lest& D. Suicide and unemployment. A re- examination. Archs enoir Hlth 20. 277-278. 1970. Walbran B., MacMahon B. and Bailey A. E. Suicide and unemployment in Pennsylvania, 1954-6 I. Archs enoir. Hlfh 10, 11-15. 1965. Buglass D., Duffy J. and Kreitman N. A Register of Social and Medical Indices By Local Government Area in Edinburgh and the Lothians (2 parts). Central Research Unit, Scottish Office. Edinburgh. 1980. Buglass D. and Duffy J. C. The ecological pattern of suicide and parasuicide in Edinburgh. Sot. Sci. <Med. 12, 241-253. 1978. Rushing W. A. Income, unemployment and suicide: an occupational study. Social. Q. 9, 493-503, 1968. Sanborn D. E., Sanborn C. J. and Cimbolic P. Occupation and suicide. Dis. Nero. Syst. 35, 7-12. 1974. Humphrey J. Social loss: a comparison of suicide victims, homicide offenders and non-violent individu- als. Dis. Nero. Syst. 38, 157-l 60, 1977. Olsen J. and Lajer M. Violent death and un- employment in two trade unions in Denmark. Sot. Psychiaf. 14, 139-145, 1979. Shepherd D. M. and Barraclough B. M. Work and suicide: an empirical investigation. Br. J. Ps.vchiar. 136, 469-478, 1980. Sanborn er al. [66] found that IO out of 15 male suicides experienced some form of job change within the I2 months preceding their deaths, and 6 exhibited a history of job-hopping or job loss during their occupational lives. Ovenstone [59] reports that about half of 37 male suicides who were unemployed. not working or retired at the time of their death had been in the same situation for at least 2 years prior to death. Theorell T., Lind E. and Floderus B. The relationship of disturbing life-changes and emotions to the early development of myocardial infarction and other seri- ous illnesses. Inr. J. Epid. 4, 281-293. 1975. See, for example. Kasl S. V., Gore S. and Cobb S. The experience of losing a job: reported changes in health, symptoms and illness behavior. Psycho>omat. Med. 37. 106-122. 1975: Kasl S. V. and Cobb S. Some mental health consequences of plant closing and job loss, In Mental Health and the Economy (Edited by Ferman L. A. and Gordus J. P.). pp. 255-299. W. E. Upjohn Institute for Employment Research, Ka- lamazoo, 1979: Cobb S. and Kasl S. V. Termination: The Consequences of Job Loss. DHEW (NIOSH) Publication No. 77-224, Cincinatti. 1977.
73. Cobs S. and Kasl S. V. Some medical aspects of unemployment. Indusr. Geronf. 8, 8-15. 1972.
74. Hagnell 0. and Rorsman B. Suicide in the Lundby

Unemployment and suicidal behaviour 113
75.
76.
71.
78.
79.
80.
81.
82.
83.
84.
85.
86.
87.
88
89.
90.
91.
Study: a controlled prospective investigation of stress- ful life events. Neuropsychobiology 6, 319-332, 1980. Borg S. E. and Stahl M. Prediction of suicide: a prospective study of suicides and controls among psychiatric patients. Acta psychiaf. stand. 65, 221-232, 1982. Fox A. .I. and Goldblatt P. 0. Longifudinal Study: Socio-demographic and Morrality D$erentials, 1971-1975. HMSO, London, 1982. Hagen makes an intriguing reference to a Russian study by Petrakov which apparently finds an associ- ation between the suicide rate and chronic un- employment. 1 have not been able to follow this matter further (Hagen D. Q. The relationship between job loss and physical and mental illness. Hosp. Communif. Psychiat. 34, 438-441, 1983). Schapiro and Ahlburg conclude from their calcu- lations that each percentage point increase in the unemployment rate is associated with about 320 more suicides (U.S.A., 1980). They contrast this figure with Brenner’s estimate of 900 additional suicides during a 6-year period (Schapiro M. 0. and Ahlburg D. A. Suicide: the ultimate cost of unemployment. J. Posf Keynsian Econ. 5, 276280, 1982-1983). Waldron J. and Eyer J. Socioeconomic causes of the recent rise in death rates for IS-24 year olds. Sot. Sci. Med. 9, 383-396, 1975. Catalan0 R. A., Dooley D. and Jackson R. Selecting a time-series strategy. Unpublished manuscript, 1982. Marshall J. R. Changes in aged white male suicide: 1948-1972. J. Geronr. 33, 763-768, 1978. The dangers of using numbers rather than rates is nicely illustrated by Cook ef al. [34] who show that the Pearson correlation between the N of suicides and the N of employed persons in the ‘J.S.A. over the years 190@-1975 was +0.83! Once population growth is ‘controlled for’ by using detrended data, the re- lationship becomes significantly negative (r = -0.59). Ahlburg D. A. The social costs of the Great Depres- sion: a cross-country study of suicide and economic contraction. Unpublished manuscript, 1983. Brenner M. H. Mortality and economic instability: detailed analyses for Britain and comparative analyses for selected industrialized countries. Inr. J. Hlrh Serc. 13, 563-619, 1983. (See especially, Table 6. p. 579.) “The age-sex-specific unemployment ratio is calcu- lated as the age-sex-specific unemployment rate divided by the total unemployment rate” (p.568) “The 2wO-year-old male unemployment ratio tends to indicate severe recession as well as a particularly heavy burden of unemployment on this age group” (p. 598). Kreitman N. and Platt S. Suicide, unemployment and domestic gas detoxification in Great Britain. J. Epid. Communit. H&h 38, 1-6, 1984. Kreitman N. The coal gas story: U.K. suicide rates, 1960-71. Br. J. prec. Sot. Med. 30, 86-93, 1976. Boor M. Relationships between unemployment rates and suicide rates in eight countries, 1962-1976. Pry- C/IO/. Rep. 47, 1095-1101, 1980. Sainsbury P., Jenkins J. and Levey A. The social correlates of suicide in Europe. In The Suicide Syn- drome (Edited by Farmer R. and Hirsch S.), pp. 38-53. Croom Helm, London, 1980. John J. Economic Instability and Health: Infant Mortality and Suicide Reconsidered. Paper presented to W.H.O. Workshop on Health Policy in Relation to Unemployment in the Community, Leeds (U.K.), December 1982. Ahlburg D. A. and Schapiro M. 0. Suicide and unemployment: some earlier evidence. J. Posr Keyn- sian Econ. In press. Warr P. and Parry G. Paid employment and women’s
92.
93.
94.
95.
96.
91.
98.
99.
100
101.
102.
103.
104
psychological well-being. Psychol. Bull. 91, 498-516. 1982. Okasha A. and Lotaif F. Attempted suicide. An Egyptian investigation. Acfa psychiaf. stand. 60, 69-75, 1979. Lendrum F. C. A thousand cases of attempted suicide. Am. J. Psychiat. 90, 479-500, 1933. Bruhn J. G. Broken homes among attempted suicides and psychiatric outpatients: A comparative study. J. menr: ki. 108, 7721179, 1962. Edwards J. E. and Whitlock E. A. Suicide and attempted suicide in Brisbane. Med. J. Aus!. 1, 932-938, 1968. Hawton K., O’Grady J., Osbom M. and Cole D. Adolescents who take overdoses: their characteristics. problems and contact with helping agencies. Br. J. Psychiaf. 140, 118-123, 1982. Hopkins F. Attempted suicide: an investigation. J. ment. Sci. 83, 71-94, 1937. Whitlock F. A. and Schapira K. Attempted suicide in Newcastle-upon-Tyne. Br. J. Psychiar. 113, 423434. 1967. Kessell A., Nicholson A., Graves G. and Krupinski J. Suicidal attempts in an outer region of metropolitan Melbourne and in a provincial region of Victoria. Aust. N.Z. JI Psvchiat. 9. 255-261. 1975. Platt S. Unemployment and Parasuicide (“attempted suicide”) in Edinburgh, 1968-1982. Unemploy. Unir Bull. 10, 4-5, 1983. Birt C. A. Unemployment, health and sickness in Stockport. In Study on rhe Infruence of Economic Insrabiliry on Health, Newsletter No. 3. Munich, 1983. Moore M. Cases of attempted suicide in a general hospital: a problem in social and psychological med- icine. New Engl. J. Med. 217, 291-303, 1937. Woodside M. Attempted suicide arriving at a general hospital. Br. med. J. 2, 411-414, 1958. Morgan H. G., Bums-Cox C. J., Pocock H. and Pottle S. Deliberate self-harm: clinical and socio-economic characteristics of 368 patients. Br. J. Psvchiaf. 127. 564-574, 1975. -
105. Smith J. S. and Davidson K. Changes in the pattern of admissions for attempted suicides in Newcastle- upon-Tyne during the 1960s. Br. med. J. 4, 412415. 1971.
106. Bancroft J., Skrimshire A., Casson J., Harvard-Watts 0. and Reynolds F. People who deliberately poison or injure themselves: their problems and their contacts with helping agencies. Psychol. Med. 7, 289-303, 1977.
107. Robins E., Schmidt E. H. and O’Neal P. Some interrelations of social factors and clinical diagnosis in attempted suicide: a study of 109 patients. Am. J. Psychiat. 114, 221-231, 1957.
108. Bagadia V. N., Ghadalia H. N. and Shah L. P. Unemployment and attempted suicide. Indian J. Psychiat. 18, 131-139, 1976.
109. Fieldsend R. and Lowenstein E. Quarrels, separations and infidelity in the two days preceding self-poisoning episodes. Br. J. med. Psychol. 54, 349-352, 1981.
110. Harrington J. A. and Cross K. W. Cases of attempted suicide admitted to a general hospital. Br. med. J. 2, 463-467. 1959.
111. Adam K.. Bianchi G.. Hawker F., Naim L., Sanford M. and Starr G. Interpersonal factors in suicide attempts: a pilot study in Christchurch. Aust. N.Z. Jl Psychiat. 12, 59-63, 1978.
112. Paykel E. S., Prusoff B. H. and Myers J. K. Suicide attempts and recent life events: a controlled com- parison. Archs gen. Psychiar. 32, 327-333, 1975.
113. Paykel E. S. Recent life events and attempted suicide. In The Suicide S.vndrome (Edited by Farmer R. and Hirsch S.), pp. 105-I 15. Croom Helm, London, 1980.
114. Fruensgaard K., Benjaminsen S., Joensen S. and

STEPHEN PLATT 114
115
116
117.
118.
119.
120.
121.
122.
123.
Helstrup K. Psychosocial characteristics of a group of unemployed patients consecutively admitted to a psychiatric emergency department. Sot. PsJ~#tiur. 18, 137-144, 1983. Brown J. H. Suicide in Britain. More attempts, fewer deaths, lessons for public policy. Archs gen. Ps.rchiat. 36, I1 19-1124. 1979. Barraclough B., Bunch J.. Nelson B. and Sainsbury P. A hundred cases of suicide: clinical aspects. Br. J. Psychiat. 125, 355-373, 1974. Robins E., Gassner S., Kayes J., Wilkinson R. H. and Murphy G. E. The communication of suicidal intent. A study of 134 consecutive cases of successful (com- pleted) suicide. Am. J. Psychiat. 115, 724-733, 1959. Dorpat T. and Ripley H. S. A study of suicide in the Seattle area. Compr. Psychiat. 1, 349-359, 1960. Miles C. P. Conditions oredisnosine to suicide: a review. J. new. ment. Dis.* 164, ‘231-246, 1977. It should be noted that many non-psychiatrists are 10th to accept the validity of this association between suicide and psychiatric illness. According to Maris [53] “most suicides are not psychotic, nor even necessarily irrational”. He goes on to criticise studies which report a prevalence of mental illness among suicides approaching loo”,;: “It is well-known that when investigators are aware in advance of their diagnosis that they are evaluating a suicide, their post facturn diagnosis of mental illness is higher than when the subject is evaluated without prior knowledge of sui- cide” (p. 207). Baechler contends that since suicide is a positive act (“one logical and universal way.. of resolving a problem”), the “really mentally ill” cannot commit suicide. “Where consciousness is eclipsed, no suicides are to be found”. (Baechler J. Suicides, p. 45. Basil Blackwell, Oxford, 1979.) Banks M. H. and Jackson P. R. Unemployment and risk of minor psychiatric disorder in young people: cross-sectional and longitudinal evidence. Psychol. Med. 12, 789-798, 1982. Warr P. Some studies of psychological well-being and unemployment. MRC/ESRC Social and Applied Psy- chology Unit, Memo No. 431, Sheffield, 1981. Evidence of an association at the aggregate level between changes in the economy and changes in the incidence of psychiatric illness, though strong [4,47.48], is not conclusive (see, for example, Stokes G. and Cochrane R. The relationship between na- tional levels of unemployment and the rate of admis- sion to mental hospitals in England and Wales, 1950-1976. Sot. Psvchiar In press), Catalan0 R. A., Dooley C. D. and Jackson R. L. Economic predictors of admissions to mental health facilities in a non- metropolitan community. J. Hlth. sot. Behur. 22, 284-297, 1981; Barling P. and Handal P. Incidence of utilization of public mental health facilities as a function of short term economic decline. Am. J. commanil. Psvchol. 8, 3 l-39, 1980: Dooley C. D.. Catalan0 R. A.. Jackson R. L. and Brownell A. Economic. life, and symptom changes in a non- metropolitan community. J. Hlfh. sot. Behau. 22, 144-154, 1981). Partial support for the hypothesised link between economic contraction, an increase in undesirable stressors and an increase in the incidence of illness and injury has been reported by Catalan0 R. and Dooley D. The health effects of economic instability: a test of the economic stress hypothesis. J. Hlrh. sot. Behar. In press. Qualitied support is also reported for the provocation explanation. whose central tenet is that economic instability somehow cau.;es disorder in previously healthy people which, in turn, increases their likelihood to seek help. How- ever, the same study found evidence m favour of a rival explanation which axsumcs that economic in-
124
125.
126.
127.
128.
129.
130.
131.
132.
133
134
135
stability can lead to help seekmg without causing disorder in previously healthy people (Dooley D. and Catalan0 R. Why the economy predicts help seek- ing: a test of competing explanations. Submitted for publication). According to an alternative version of this model the impact of economic conditions upon the health of the population would not be reflected in an increase In the number of persons with psychiatric symptoms. but in an increase in the proporrion of the psychiatric pool suffering from a major disorder. Given the association between such disorders and suicide. the suicide rate would be likely to rise also. For further discussion on the stressful effects of the recession upon the employed as well as the un- employed, see, for example. Brenner [37]. Warr P. Job loss, unemployment and psychological well-being. In Role Transitions (Edited by van de Vilert E. and Allen V.). Plenum Press. New York. 1983; Brodsky C. M. Suicide attributed to work. Suicide Life Threat. Behac. 7, 216229. 1977. See also Karcher C. J. and Linden L. L. Is work conducive to self-destruction? Suicide &ye rhrea/. Belnrc. 12, 151-175, 1982. Mills C. W. Situated actions and vocabularies of motives. Am. social. Rer. 5, 904-913. 1940. Scott M. B. and Lyman S. M. Accounts. Ani. social. Rev 33, 46-62, 1968. I am here following the terminology of Brown G. W. and Harris T. Social Origins of Depression. p. 47. Tavistock, London. 1978. In their study of overdose patients assessed using the Present State Examination. Newson-Smith and Hirsch found that psychiatric symptoms were common dur- ing the four weeks preceding the act. 31”,, of patients had a definite psychiatric disorder and a further 29”,, were in the border-line or ‘threshold’ categ,ory. All but one patient in these two groups were diagnosed as suffering from depressive disorders. Urwin and Gib- bons found that 307; of their sample of self-poisoners had definite disorders and 42”, were in the borderline group. Most were suffering from depression. A quar- ter of the men and just over I in 10 of the women were classified as having personality disorders. Only one- third of male parasuicide admissions to the Regional Poisoning Treatment Centre. Edinburgh. in 1980 were not classified as either psychiatrically ill or personality disordered or alcoholic. This proportion rose to just under a half in 1981. About a third of male admissions in both years had received previous inpatient psychiatric care. Just under 1 in 5 males reported habitual drug misuse (unpublished data). (Newson- Smith J. G. and Hirsch S. R. Psychiatric symptoms in self-poisoning patients. PsychoI. Med. 9, 493-500. 1979; Urwin P. and Gibbons J. L. Psychiatric diagno- sis in self-poisoning patients. Ps~chol. Med. 9. 501-507, 1979.) Platt S. and Duffy J. Parasuicide and unemployment: an empirical analysis based on a three-year cohort of male parasuicide admissions. Submitted for publica- tion. O’Brien S. E. M. A survey of young adults admitted to hospital for self-poisoning in a Central London District, February 1975-August 1976. Ph.D. Thesis. University of London, 198 I. Morgan et al. [IO31 report that only 12”,, of their sample of 337 parasuicides were diagnosed as suITering from a major functional psychotic illness. Pallis D. J.. Barraclough B. M.. Levey,A. B., Jenkins J. S. and Sainsbury P. Estimating suicide risk among attempted suicides: I The development of new clinical scales. Br. J. Psychiur. 141, 37-44. 1982. Morris J. B., Kovacs M.. Beck A. T. and Wolffe A.

Unemployment and suicidal behaviour 115
136
137
138
139
140
141
142
143.
144.
145.
146.
Notes toward an epidemiology of urban suicide. Compr. Psrchiur. 15, 537-547. 1974. Wallis C. P. and Maliphant R. Delinquent areas in the county of London: ecological factors. Br. J. Criminal. 147. 7, 250-284, 1967. Farmer R. D. T.. Preston T. 0. and O’Brien S. E. M. Suicide mortality in Greater London: Changes during the past 25 years. Br. J. prev. Sot. Med. 31, 171-177, 148. 1977. Thomas D. S. Social Aspects q/ the Business Cycle. 149. Knopf. New York, 1927. Ogburn W. F. and Thomas D. S. The influence of the 150. business cycle on certain social conditions. J. Am. Statist. Ass. 18, 324-340. 1922. Henry A. F. and Short J. F. Suicide and Homicide. 151. Free Press, New York, 1954. 1.52. Hurlburt W. C. Prosperity, depression and the suicide rate. Am. J. Social. 37, 714-719, 1932. Windschuttle K. Vnemploymenf. Penguin Books, 153. Ringwood, Australia, 1979. Dublin L. I. and Bunzel B. To Be or Not To Be, A 154. St& @Suicide. Harrison Smith & Robert Haas, New York, 1933. MacMahon B., Jonhson S. and Pugh T. F. Relation of suicide rates to social conditions. Publ. Hlrh Rep. 155. 78, 285-293, 1963. Stack S. Divorce and suicide: a time series analysis, 156. 1933-1970. J. Fam. Iss. 2, 77-90, 1981. Ahlburg D. A. and Schapiro M. 0. Socioeconomic
ramifications of changing cohort size: an analysis of U.S. postwar suicide rates by age and sex. Submitted to Demography. Anttinen E., Jarventie I. and Makela R. Economic cycles, unemployment and committed suicides in Finland in 1960-1979. Paoer nresented to VII World Congress of Psychiatry, Vienna. 1983. Batchelor 1. R. C. Psychopathic states and attempted suicide. Br. med. J. 1, 1324-l 327, 1954. Pate1 A. R., Roy M. and Wilson G. M. Self-poisoning and alcohol. L&et 2, 1099-1103, 1972. - Jacobson S. and Tribe P. Deliberate self-iniurv tat- tempted suicide) in patients admitted to hospiial in mid-Sussex. Br. J. Psychiaf. 121, 379-386, 1972. Unpublished data. East W. N. On attempted suicide, with an analysis of 1000 consecutive cases. J. mew. Sci. 59, 428-478. 1913. Sclare A. B. and Hamilton C. M. Attempted suicide in Glasgow. Br. J. Psychiar. 109, 609-615, 1963. Krupinski J., Staller A. and Polke P. Attempted suicides admitted to the mental health department, Victoria, Australia: a socio-demiological study. Int. J. sot. Psychial. 13, 5-13, 1966. Werry J. S. and Pedder J. Self-poisoning in Auckland. N.Z. med. J. 83, 183-187, 1976. . Lyons H. A. and Bindal K. K. Attempted suicide in Belfast. Ir. med. J. 70, 328-332, 1977.