ukrainian children’s morbidity
TRANSCRIPT

.
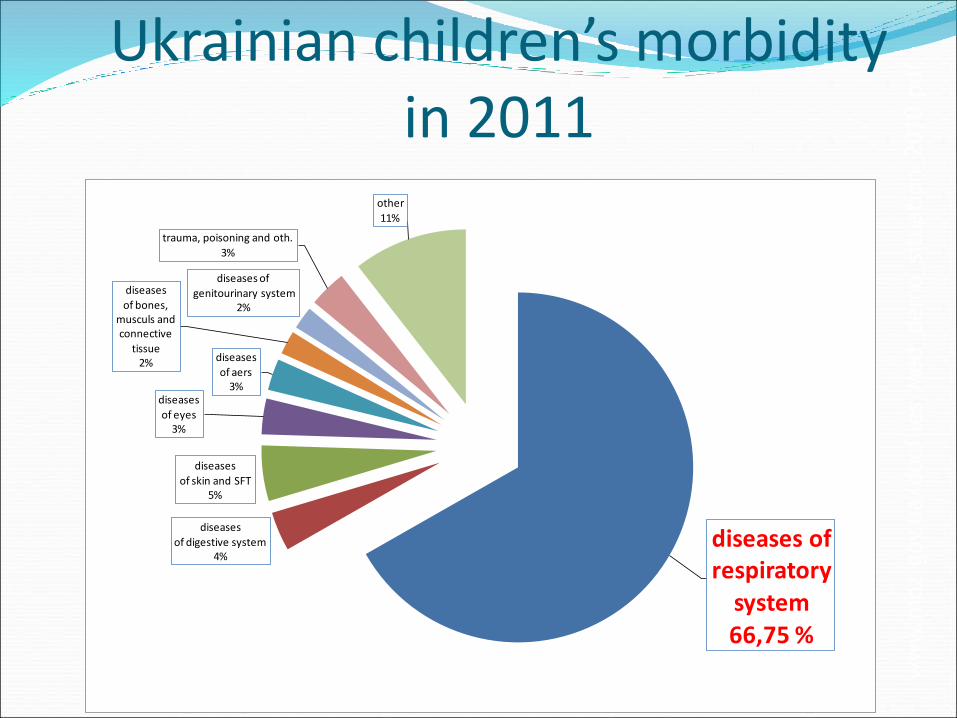
Ukrainian children’s morbidity in 2011
diseases of respiratory
system66,75 %
diseases
of digestive system4%
diseases
of skin and SFT5%
diseases
of eyes3%
diseases
of aers3%
diseases
of bones, musculs and connective
tissue2%
diseases of
genitourinary system2%
trauma, poisoning and oth.
3%
other
11%
www.m
oz.gov.ua/docfiles/Med_demo_situation_2010.pdf

respiratory tract
UPPER
( nose, pharynx)
MIDDLE
(larynx, trachea, bronchi)
LOWER
(bronchioles, alveoli)


APF of nose Relatively small size.
Narrow nasal passages (lower
nasal conchas are absent,
they get formed by the age of
4 years).
mucous membrane
abundantly vascularised.
cavernous submucosal tissue
develops by the age of 8-9
years.
nasal
obstruction
impediment
during suckling,
dyspnea.
hyperaemia and edema
possibility to suckle
rare nasal
hemorrhage
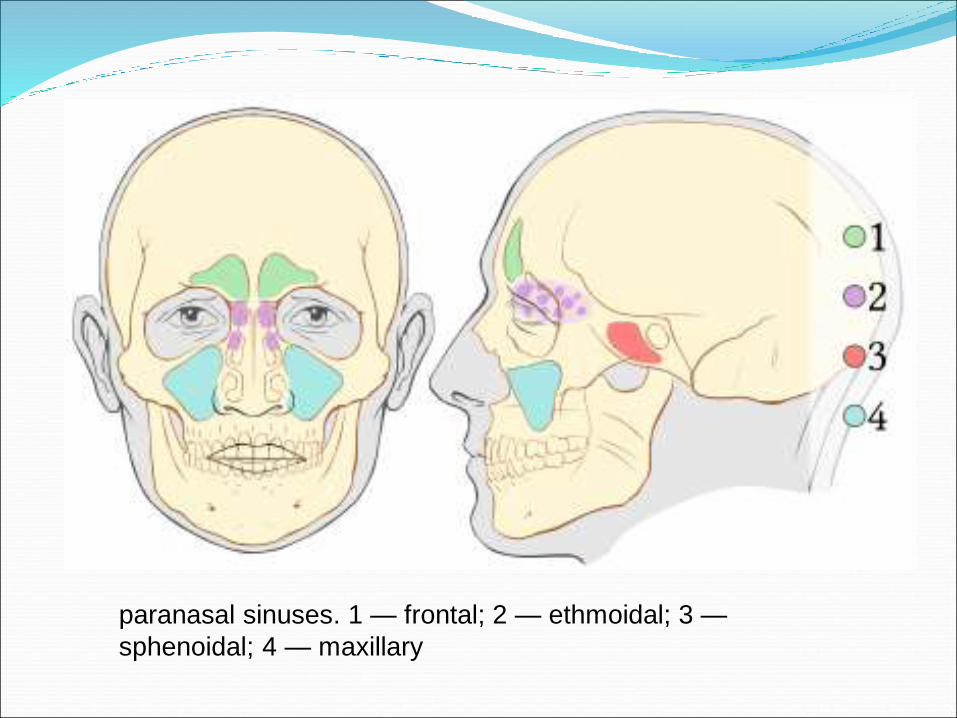
paranasal sinuses. 1 — frontal; 2 — ethmoidal; 3 —
sphenoidal; 4 — maxillary

sinuses new
born
2 years 6 years 7
years
12
years
15
years
20
years
maxillary undeve
loped
get
formed
frontal - start to
develop
get
formed
sphenoidal undeve
loped
get
formed
ethmoidal - start to
develop
get
formed
Functions of paranasal sinuses Decrease of relative weight but keep volume of skull front
section, especially facial bones – place of fastening for
facial muscles.
Increase of vocal resonance
Insuring of shock-resistant buffer in case of trauma
isolation of sensible structures (roots of teeth, eyeballs)
from fast temperature fluctuation in nasal cavity during
inhalation and exhalation.
Moistening, cleaning and warming of air due to slow
airflow into the sinuses.
provoke sneezing.

Nasolacrimal duct is short with
underdeveloped valves that
simplify infection of
conjunctival sac from nasal
cavity.

APF of pharynxnarrow and more
vertical

location of Eustachian tube in adults (above) and children
(short, wide, straight, horizontal)

Pharyngeal Waldeyer’s lymphoid ringmaximal development in 5-6 years
1 — lingual tonsil;
2 — palatine tonsils;
3 — pharyngeal
tonsil;
4 — tonsils of torus
tubaris;
5 — lymphatic
follicles in mucous
membrane of back of
the throat.

normal adenoids enlarged adenoids

Fauces


APF of larynx After birth the form is funnel-shaped,
later on – cylindrical.
Located higher, it’s relatively longer
and narrow.
Mucous membrane is very gentle,
soft, considerably vascularised.
Rich in lymphoid tissue.
Muscles of vocal fissure get tired
easily
Vocal fissure is relatively narrow till
the age of 6-7, vocal cords are short
disturbance
of respiration
up to
stenosis
hoarseness
high pitched
voice

Th 6
С 7
С 4
Th 3-4
4 sm
12 sm
APF of trachea
The walls are soft and get palpated easily.
The mucous membrane is soft, abundantly
vascularised and relatively dry.

APF of bronchi
Narrow and soft.
Muscular and elastic fibers are poorly
developed (by the age of 7 years).
The mucous membrane has rich
vascularization, covered with ciliated
epithelium, which carries out mucociliary
clearance.

APF of lungs Breathing surface is
relatively large.
Relatively big lungs occupy
more place into the chest,
they are squeezed into the
ribs, intercostal space are
smoothed out. The chest is
always in state of inhalation.
The ribs are almost
perpendicular to spine.

In children of 1 year of life upper
lobes of left lung is poorly
developed; upper and middle lobs
of right lung are almost identical
with size. The sizes of lobs
corresponds to adult sizes by the
age of 2 years.
Interlobar fissures are
undeveloped
absence of interlobar pleurisy

segments are well
delimited (sometimes
2,4,5,6 segments in the
left lung are fully
delimited)
segmental pneumonia
more often inflamation
locates in 4, 5, 6
segments of the left lung
and in 2, 10 segments of
the both lungs. 10 segments

root of lung is spacious, with a lot of blood vessels and lymph nodes
possible development ofbronchoadenitis.
elastica is undeveloped
atelectasis

a lot of interstitial connective tissue
are around alveoli
frequent interstitial pneumonia
in children of 1 year of life.
functional particularities of breathing
frequent and superficial
respiration rate of newborn = 40-60 per
1 min, 1 year = 30-35, 5 years = 25, 10
years = 20, more than 10 years = 18-
16 per 1 min.
respiration rate is considerably unsteady
(because of psychic excitement,
physical activity, changing of body and
environment temperature)
physiological arrhythmia and apnea (first 3 months of life)
diaphragmatic type of breathing (first 6 months of life)
small
respiratory
volume,
considerable
resilience
immaturity of
respiratory center.
weakness of
respiratory
muscles, horizontal
disposition of ribs.

The lung buds form during the 4th week
Initially appear as the respiratory diverticulum, which is a ventral
outgrowth of foregut endoderm

Splitting of foregut into esophagus and trachea
Tracheo-esophageal ridges: longitudinal ridges that eventually fuse
to separate trachea from esophagus.

Tracheo-esophageal fistulas /
esophageal atresia
Incomplete separation and/or atresia of trachea and esophagus (B on
right shows esophageal atresia)

Differentiation of pleural membranes
The lung buds “punch” into the visceral mesoderm. The mesoderm,
which covers the outside of the lung, develops into the visceral
pleura. The somatic mesoderm, covering the body wall from the
inside, becomes the parietal pleura. The space between is the
pleural cavity.

Separating the abdominal and thoracic cavities: development of the septum transversum and diaphragm
Extension of the
septum transversum
partially divides
abdominal and
thoracic cavitiesGrows in a roughly transverse
plane from front to back
Angled downward such that
front of septum is at about T7,
back edge is at about T12

Congenital diaphragmatic hernias
Relatively common (1/2000 births)
Hiatal hernias are most frequent,
but effects are rather minor due to
small size of defect
Hernias due to failure of one or both
pleurpericardial membranes to
close off pericardioperitoneal canals
have much more significant clinical
impact because herniated
abdominal contents interfere with
lung development.
80-90% of hernias with clinical
impact are on the left side. Large
defects have high mortality due to
extent of lung hypoplasia and
dysfunction.

First three branching events are
stereotyped:
After the initial bifurcation into
two primary bronchi, two buds, or
secondary bronchi, form on the
left and three on the right
predicting the five lobes of the
adult human lung. Ten tertiary
(segmental) bronchi form in the
right and left lungs - establishing
the brochopulmonary segments
of the adult human lung.
Initial Patterning of the Lung:

Development of the human lung
7 trachea; 1 Left main bronchus; 6 right main bronchus; others lobes

Agenesis of the lungs:
Can occur bilaterally or unilaterally. Unilateral lung agenesis is compatible with
live as remaining side hyperexpands and compensates.
Lung aplasia:
Is defined as unilateral absence of the lung with preservation of main bronchus
remnant at the tracheal bifurcation.
Lung hypoplasia:
Often caused by congenital diaphragmatic hernias or congenital heart disease.
Characterized by reduced lung volume.

Pseudoglandular
Period (5-17
weeks):
By 17 weeks, all major
elements have formed,
except those involved with
gas exchange (fetuses
unable to survive if born at
this stage).
Canalicular Period
(16-25 weeks):
Bronchi, terminal bronchioles
become larger, lung tissue
becomes highly vascular.
Alveolar ducts form by week
24. By end, some terminal
sacs have formed so
respiration is possible (small
chance of survival at this
stage).
Terminal Sac
Period (24 weeks
to birth):
Many more terminal sacs
develop, their epithelium
becomes very thin and
capillaries bulge into the
developing alveoli.
Blood-air barrier
becomes well-developed.
(By 26-28 wks, 1000 gr
fetus has a sufficient # of
sacs and surfactant to
survive.)
Alveolar Period (late
fetal period to age 8):
Alveoli-like structures are
present by 32 weeks.
Epithelial lining of sacs
attenuate to extremely thin
squamous epithelia, capable
of gas exchange. 95% of
characteristic, mature alveoli
develop after birth.
Stages of maturation of the lungs

Canalicular
Period:
(16th-26th week)
Terminal Sac Period:
(24th weeks to birth)
Type I squamous cells
Alveolar Period:
(late fetal thru childhood,
Type II, surfactant-
producing cells)
Development of lung tissue involved in air exchange

At birth:
Alveoli continue to mature after birth. Growth of lungs
after birth due primarily to increase of respiratory
bronchioles and alveoli. Only 1/6 of adult alveoli present
at birth.
Lungs are fluid filled; fluid squeezed out and into
lymphatics and blood vessels, expelled via trachea at
delivery.
Surfactant remains on surface, lowers air/blood tension.

Surfactant deficiency

Respiratory Distress Syndrome/Hyaline Membrane DiseaseThis disease affects 2% of live
newborn infants, with
prematurely born being most
susceptible. 30% of all
neonatal disease results from
HMD or its complications.
The reason of syndrome is the immaturity or damage of
surpfactant. The basic signs –infringements of function of
respiration – tahypnea, the mixed dyspnea, cyanosis and
periodic types of respiration.

Respiratory Distress Syndrome

Respiratory Distress Syndrome
The foam on the lips innewborn and infants isan equivalent of cough.

Positional Nasal Deformity
Positional Nasal Deformity
An occasional finding on physical
exam is an asymmetric
appearance of the nose due to a
positional deformity. Most likely,
this results from an unfortunate
position in utero. The nares in this
case are asymmetric and slightly
flattened towards the infant's right,
even though the septum is still
centrally located.
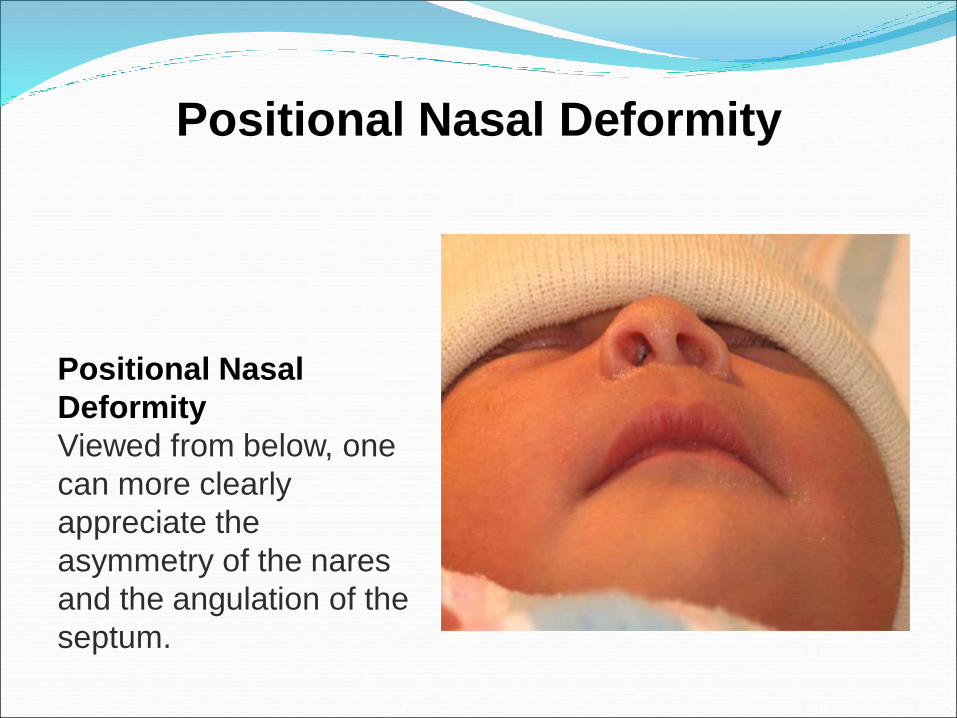
Positional Nasal Deformity
Positional Nasal
Deformity
Viewed from below, one
can more clearly
appreciate the
asymmetry of the nares
and the angulation of the
septum.

Positional Nasal Deformity

Dislocated Nasal Septum
From this view, the
deformity is more easily
seen. The septum is not
straight. Compressing
the tip of the nose gently
can also help distinguish
this condition from a
positional problem.

Congenital Anomalies of the Larynx
Laryngomalacia (most common) – most frequent cause of stridor in infants and children
- Starts in first weeks of life, symptoms increase up to 6 months
- Symptoms: inspiration stridor, less in prone position, increased by any exertion

Airway Foreign Body
Most seen in children age 3-4 years
Clinical: sudden onset of respiratory distress, choking, cough, hoarseness, shortness of breath, wheezing (asymmetric) and decreased breath sounds (asymmetric); depends on location
Complications: obstruction, infection, mediastinitis
Diagnosis – chest x-ray
Therapy – removal by bronchoscopy

Airway Foreign Body

Сongenital stridor
•Whistling respiration – a stridor.The stridor can be congenital –anomaly of a structure of a larynxand acquired – a paralysis of vocalchords, compression of respiratorytract from outside (by tumor,enlarged lymph node, thymus)
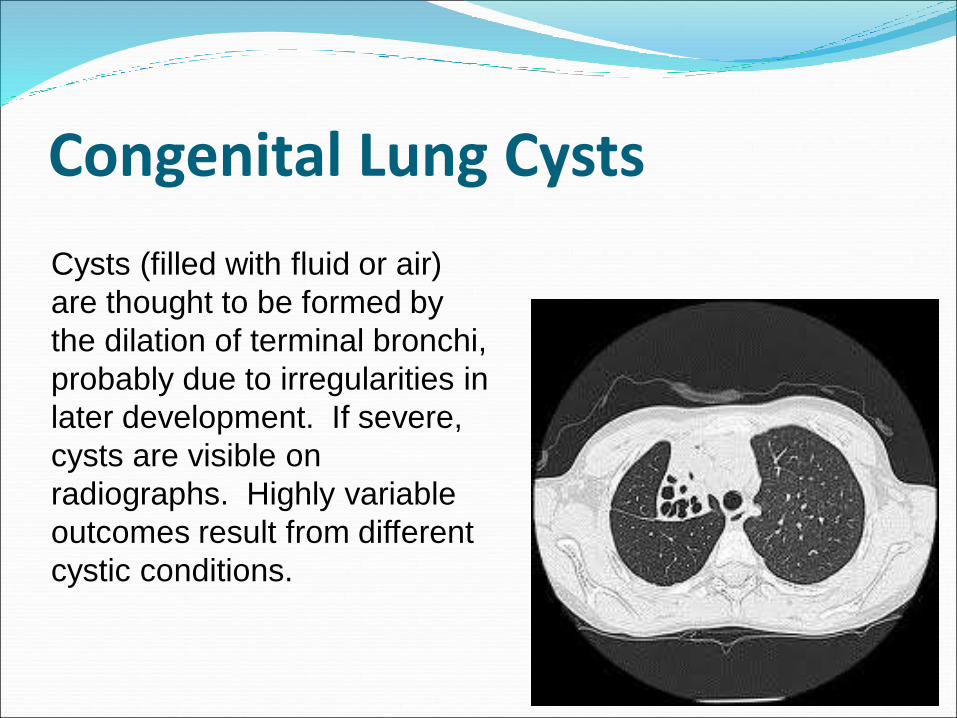
Congenital Lung Cysts
Cysts (filled with fluid or air)
are thought to be formed by
the dilation of terminal bronchi,
probably due to irregularities in
later development. If severe,
cysts are visible on
radiographs. Highly variable
outcomes result from different
cystic conditions.

Congenital Lung Cysts Cystic fibrosis – major cause of severe chronic
lung disease and most common cause of exocrine
pancreatic deficiency in children
Clinical presentation from RT
-Cough, purulent mucus – early in first year, extensive
bronchiolitis, then pulmonary function test
abnormalities, dyspnea; finally – cor pulmonale,
respiratory failure, and death; high risk for
pneumothorax
-Examination: hyper-resonance, rales, expiratory
wheezing, clubbing, cyanosis (late)

first breathhydraulic pressure + natural resistance
increasing of excitability of respiratory center’s neurons
activation of reticular formation
hypoxia + afferent impulses

A comparison of the
first breath (lower loop)
with a breath at one day
of age (top loop). Note
that before the first
breath the lungs
contain no air at all. At
the end of the breath,
functional residual
capacity is immediately
achieved; about 15 ml
of air remains. The first
breath takes in about 45
ml of air. 24 hours later,
FRC is about 90 ml, far
less pressure is
generated, and only
about 15 ml of air is
inhaled.
