trastuzumab (herceptin): a retrospective analysis of the effects of long-term application in a...
TRANSCRIPT

1 3
Arch Gynecol ObstetDOI 10.1007/s00404-014-3261-1
GynecOlOGIc OncOlOGy
Trastuzumab (herceptin): a retrospective analysis of the effects of long‑term application in a series of patients with breast cancer
Simona Moga · Stephanie Juhasz‑Böss · David Bardens · Nicole Kranzhöfer · Sogand Nemat · Erich‑Franz Solomayer · Ingolf Juhasz‑Böss
Received: 7 October 2013 / Accepted: 16 April 2014 © Springer-Verlag Berlin Heidelberg 2014
follow-up time was 113.5 months (range 50–240 months). Three of the patients had a treatment interruption for an average of 2.6 months (range 3–5), which was not due to side effects. The left ventricular ejection fraction (lVeF) was controlled at regular intervals in all of the patients. Upon the beginning of the trastuzumab treatment, the mean lVeF was 68 %. In one patient, the trastuzumab treatment was discontinued after 41 months because of a decrease of the lVeF below normal levels.Conclusion Trastuzumab is well tolerated even during long-term use. Patients with HeR2 overexpression and metastases can be treated well with trastuzumab for up to 119 months.
Keywords Breast cancer · Metastasis · Trastuzumab · Antibody therapy · long-term therapy
Introduction
With an incidence of over one million diagnosed cases world-wide per year, breast cancer is the most common malignant tumor in the female. About every eighth woman in Germany is developing breast cancer in the course of her life and breast cancer is the most common cause of cancer-related deaths [1].
About 20 % of all mamma carcinomas do overexpress human epithelial growth factor 2 (synonyms: HeR2, Her2/neu, erbB-2) [2]. The published rates of HeR2 posi-tivity tend to differ from publication to publication, this may be due to error-prone testing methods. The central role of HeR2 for growth and development of normal breast tis-sue has already been known since 1980s. The transmem-brane tyrosine kinase receptors HeR1, -2, -3 and -4 usually regulate the growth and development of various tissues and can be considered as classical oncogenes [2, 3].
Abstract Introduction About 20 % of all mamma carcinomas are HeR2 positive. The overexpression of HeR2 is considered to be a negative prognostic factor. Trastuzumab is a mono-clonal anti-HeR2 antibody developed to target HeR2 over-expressing tumor cells. So far, there is only little data avail-able on long-term effects of trastuzumab. This is why we analyzed the medical records of our patient collective with respect to tolerability and oncological outcomes of long-term trastuzumab treatment.Materials and methods Our retrospective observational study included all patients of the Saarland University Hos-pital with breast cancer who received trastuzumab for more than 18 months between 2003 and 2012. We analyzed the medical records with respect to oncological outcome, toler-ability and cardiac side effects.Results A total of n = 15 patients had been treated with trastuzumab for over 18 months with a mean therapy dura-tion of 57.2 months (range 18–119 months). The mean
S. Moga · S. Juhasz-Böss · D. Bardens · e.-F. Solomayer · I. Juhasz-Böss Department of Obstetrics, Gynecology and Reproductive Medicine, Saarland University Hospital, Homburg, Germany
S. Moga (*) Klinik für Frauenheilkunde, Geburtshilfe und Reproduktionsmedizin, Universitätsklinkum des Saarlandes, Kirrberger Str. 1, 66421 Homburg, Germanye-mail: [email protected]; [email protected]
n. Kranzhöfer Outpatient Oncology center, Saarland University Hospital, Homburg, Germany
S. nemat Department of Diagnostic and Interventional Radiology, Saarland University Hospital, Homburg, Germany

Arch Gynecol Obstet
1 3
HeR2 positive breast cancer patients have an unfavora-ble prognosis. HeR2 overexpression or HeR2 gene ampli-fications, respectively, are associated with shorter relapse-free survival and shorter overall survival. Due to its central molecular biological role in the pathogenesis of breast cancer, HeR2, it is the most important target when treating HeR2 positive mamma carcinoma.
Trastuzumab (Herceptin®) is a humanized monoclonal antibody that binds to the extracellular domain of HeR2, preventing the receptor from dimerization. Thereby, the signal transduction is being inhibited and the body’s own immune system is being activated through antibody-medi-ated cellular cytotoxicity [2–4]. Those two mechanisms inhibit the survival of HeR2 positive tumor cells. Trastu-zumab is the first commercially available humanized anti-body for the treatment of breast cancer. After several studies had proven, the superiority of Trastuzumab in the treatment of metastasized HeR2 positive breast cancer was approved by the FDA in the USA in 1998 [2]. The european approval for that indication followed in 2000, and since 2006 Trastu-zumab is also approved for adjuvant therapies [2].
The testing and the therapeutic approach of Trastuzumab can be considered as a prime example of targeted cancer therapy [2, 3]. HeR2 status is a valuable predictive marker of therapeutic response.
current therapy guidelines recommend that patients with strongly positive HeR2 stains (IcH 3+, equals a positive staining of >30 % of all cells) or IcH 2+ (weak to moder-ate complete membrane staining in more than 10 % of the tumor cells) with positive fluorescence in situ hybridization (FISH) or chromogenic in situ hybridization (cISH) should be treated with Trastuzumab [2].
Usually, the HeR2 status is determined in the primary tumor tissue. Since there can be discrepancies between the primary tumor and distant metastasis, a new reevaluation of the HeR2 and receptor status should be performed from metastatic tissue. This is necessary especially in the cases when time between initial diagnosis and tumor dissemina-tion has been longer or in cases of rapidly progressive dis-ease under palliative chemotherapy [5–7].
There exist four large multicentric studies (nSABP B-31, nccTG n 9831, HeRA and BcIRG 006) on adju-vant therapies of the HeR2 positive breast cancer that examined Trastuzumab in various dosages and combi-nations [2]. All of these studies show that the additional administration of Trastuzumab to adjuvant chemotherapies is significantly reducing recurrence rates and that Trastu-zumab is tolerable regarding cardiac side effects. Giving Trastuzumab for 1 year in addition to adjuvant chemother-apy is standard today [2, 3, 8].
Giving Trastuzumab as a monotherapy or in combination with chemotherapies or endocrine therapies is also a standard treatment of metastasized HeR2 positive breast cancer. But
despite all the progress that has been made to improve drug therapies, metastasized breast cancer remains an incurable disease. Most of the patients suffer from rapid progression of the disease and only few reach long-lasting remission.
Due to the poor prognosis of the disease, there is only few data available about long-term treatment with Trastu-zumab. This is why we analyzed the medical records of our patient collective in terms of therapy duration, oncological outcome and tolerability of Trastuzumab.
Materials and methods
Our retrospective study includes all breast cancer patients who were treated with Trastuzumab for more than 18 months (defined as the time between the first and the last drug administration) at our University Hospital between March 2003 and December 2012. The primary endpoint of the study was the duration of the therapy. Secondary endpoints were co-administered chemotherapy agents, progression-free survival during Trastuzumab therapy, Trastuzumab admin-istration in spite of progression, localization of metastases, cardiac tolerability, and follow-up time (defined as time between diagnosis and examination or death, respectively).
The Her-2 status was determined on the basis of the Her-ceptTest™ (DAKO, Denmark) either in the primary tumor tissue at time of the first diagnosis or in metastatic tissue at time of diagnosis of metastatic disease. In the cases of weak to moderate complete membrane staining in more than 10 % of the tumor cells (IHc 2), a FISH (Zytomed Systems, Ger-many) was needed to re-evaluate the Her2 status.
The left ventricular ejection fraction (lVeF), a marker for cardiac tolerability, was assessed by echocardiography or radionuclide ventriculography either in the cardiologic department of our clinic or by a local resident cardiolo-gist. lVeFs of 55 % or more were considered as normal. cardiac events were defined as a decrease in lVeF below normal values (<55 %), a drop in lVeF of more than 20 % below the initial value or the appearance of clinical symp-toms of cardiac insufficiency.
Our data were collected in an excel worksheet (Version 2007, Microsoft, Washington Dc, USA). The subsequent statistical analysis was performed using SOFA Statistics (Version 1.4.0, Paton-Simpson & Associates ltd, new Zealand). For continuous variables, averages and stand-ard deviations were calculated. For discrete variables, fre-quency distributions were determined.
Results
In our clinic each year, we treat about 230 patients with breast cancer. About 13 % have a positive Her2 status and

Arch Gynecol Obstet
1 3
thus receive Trastuzumab. The majority of them are in an adjuvant situation though, only 3–4 patients per year receive Trastuzumab within a palliative situation. During the study period between March 2003 and December 2012, a total of 15 patients had been treated in our department with Trastuzumab for more than 18 months. The patients received the treatment for an average of 57.2 months (range 18–119).
The Trastuzumab application form was intravenous, respecting a 3-week interval between the administrations (loading dose 8 mg/kg BW, maintenance dose 6 mg/kg BW). none of the patients of this series were treated within a clinical trial. The mean age of the patients at the time of initial diagnosis was 49.5 years (range 30–74). The mean follow-up time was 113.5 months (range 50–156).
Table 1 gives an overview about the patient character-istics. A total of 4 of the 15 patients were remained free of metastases. These patients received an adjuvant therapy with Trastuzumab for an average of 23 months, two of them within the scope of the treatment of local recurrences. In all of these cases, the combination partner was a taxane. Today, after the publication of the HeRA trial, the adjuvant treatment with Trastuzumab is recommended for the dura-tion of 1 year [9]. At the time these four patients received their treatment, these results were not available yet. The treatment duration was established by the supervising therapist provided that there was a very good tolerability to Trastuzumab.
At the end of the observation period, one of these four patients was still alive, while the other three were lost to follow up.
A total of 11 of the 15 patients were diagnosed with metastases during the study period. The distant metasta-ses were localized as follows: liver metastases in six of the cases, bone metastases in five of the cases, lung metasta-ses in two of the cases, mediastinal or lymph node metas-tases, respectively, in two of the cases. Three of the patients had multiple metastases. Two of them already showed
metastases at the time of their initial diagnosis, nine patients developed metastases within a mean period of 4 years fol-lowing their initial diagnosis (range 4 months–12 years).
All of the 11 patients with metastatic breast cancer received Trastuzumab as first-line therapy at the time of metastasis diagnosis (n = 6 in combination with taxanes, n = 1 in combination with epirubicin and cyclophospha-mide, n = 1 with vinorelbine and n = 3 as a monotherapy). At the data evaluation time, four of them were still under treatment with Trastuzumab, alive and with stable disease (two of them presented hepatic, one pulmonary and one lung metastases).
During the therapy with Trastuzumab, seven patients had a progress of tumor growth. Among two of these patients, Trastuzumab therapy was stopped and they received a tar-geted therapy with lapatinib. In five of the cases, the Trastu-zumab administration was continued as a treatment beyond progression. combination partners were endocrine agents in two of the cases, capecitabine and vinorelbine in other two cases. Finally, surgical removal of the liver metasta-sis was performed in one case; this patient was still under Trastuzumab treatment, alive with no sign of progress at data evaluation time. The other four patients received a Trastuzumab treatment over 3–5 therapy lines, in combina-tion with endocrine agents, capecitabine, vinorelbine and, respectively, eribulin. One of the patients received a dual Her2 blockade with pertuzumab. At the end of our observa-tion period, these four patients died during the therapy due to tumor progression.
Three of the patients had a Trastuzumab treatment inter-ruption for an average of 2.6 months (range 3–5), but in none of the cases, Trastuzumab was paused because of therapy-induced side effects.
The mean left ventricular ejection fraction, which was assessed by echocardiography or radionuclide ventriculog-raphy, respectively, was 66.8 % (range 57–84 %) before the beginning of Trastuzumab therapy. The lVeF was reas-sessed on a regular basis (at least once a year, usually every
Table 1 characteristics of patients that received Trastuzumab for more than 18 months
LVEF left ventricular ejection fraction
Parameter Mean ± standard deviation
Unit of measurement
number of patients
Patient age at the time of initial diagnosis 49.5 ± 10.6 years 15
Patient age at the time of tumor dissemination 49.9 ± 16.8 years 13
Time from initial diagnosis to tumor dissemination 4.0 ± 3.0 years 12
Duration of trastuzumab therapy 57.2 ± 33.7 Months 15
Follow-up time 113.5 ± 61.0 Months 15
lVeF before trastuzumab 68.4 ± 7.3 % 12
lVeF after trastuzumab 59.8 ± 7.4 % 12
Duration of therapy interruption 2.6 ± 1.1 Months 3

Arch Gynecol Obstet
1 3
3 months). At the beginning of the Trastuzumab treatment, none of the patients had any apparent cardiac disease. eight patients (73 %) were pre-treated with antracyclines. At the end of the Trastuzumab therapy or at the time of our data collection, respectively, the mean lVeF was 59.8 %. none of the patients reported cardiac side effects that lead to an interruption of the medication and none of the patients had a decrease in lVeF of more than 20 % below the initial value. Only one cardiac event was registered. The patient’s lVeF decreased below normal values to 46 % (initial value 57 %). At this patient, the Trastuzumab therapy was dis-continued after 41 months. later examinations showed that the lVeF of the patient had increased again and the patient remained relapse free.
no other Trastuzumab-related toxicities were encoun-tered among our patient series.
Discussion
In spite of intensive research, metastasized breast can-cer remains an incurable disease with an average survival time of about 2 years [10]. HeR2 overexpression is asso-ciated with poorer prognosis and poorer response rates to standard chemotherapies and to endocrine therapies [2–4, 10–12]. The development of HeR2-targeted therapies was a huge step forward in breast cancer therapy. By now, Tras-tuzumab is an essential part of the standard therapy in case of HeR2 overexpression, in adjuvant as well as in metasta-sized situations.
numerous retrospective and prospective studies have demonstrated that adding Trastuzumab to different types of chemotherapies is beneficial in terms of overall survival, (OS), progression-free survival (PFS), time to progres-sion (TTP) and overall response rate (ORR) in patients with metastatic breast cancer. A meta-analysis from 2010 showed increases of OS (22 %), PFS (37 %), TTP (44 %) and ORR (67 %) when adding HeR2-targeted agents to standard treatment [13].
nevertheless, only few patients with HeR2 positive breast cancer achieve long-term remission. This is why data on long-term treatment with Trastuzumab can only be found in few case reports. There are documented cases of patients who have had a long-term remission for up to 9 years [10, 14, 15]. Other authors describe the risks of dis-continuing maintenance therapy with Trastuzumab. They report a case of a woman that achieved a prolonged remis-sion of liver metastases. After 3 years, Trastuzumab was discontinued. However, 2 months later, brain metastases were detected [16].
Four of the patients with metastases in our study popula-tion remained progression-free under first-line Trastuzumab maintenance therapy for an average of 86 months (7.1 years,
range 41–114 months) during our study period (mean fol-low-up time 168 months, range 96–264 months). Statements about the optimal duration of Trastuzumab maintenance therapies cannot be made because of lack of data.
Studies have shown that maintaining Trastuzumab treat-ment beyond progression seems to be beneficial. What is more, those studies have shown that Trastuzumab therapy should be maintained even when co-administered chemo-therapy agents are changed [2, 4, 8, 12, 17–19]. The data that can be found in the literature show that patients have a statistically significant survival benefit when Trastuzumab treatment is continued as a single medication or in com-bination with chemotherapy as well as with new targeted therapies, like lapatinib or pertuzumab.
The most frequent combination partners with Trastu-zumab in our series were taxanes (66 %). Others were vinorelbine and capecitabine. This coincides with the data in current literature regarding efficacy in treating metastatic breast cancer and with the national and international guide-lines [20–22].
Other frequently used combination partners, especially in breast cancer patients with comorbidities, are endocrine agents. These are less toxic and the simultaneous applica-tion with Trastuzumab can be used as a maintenance treat-ment after or instead of chemotherapy.
In the last years, the concept of a dual Her2 receptor blockade was introduced due to the progress in the research of new targeting agents. Based on the new data of the cleOPATRA trial, the combination of Trastuzumab with pertuzumab should now be used as a standard first-line therapy in treating metastatic breast cancer [20, 23]. As data from this trial were not available at the time of therapy of most patients in our study, only one of them received a dual Her2 blockade with Trastuzumab and pertuzumab. Besides pertuzumab also the combination with lapatinib is available for patients who received multiple lines of chemotherapy.
Starting from now, HeR2-positive patients with Trastu-zumab and lapatinib refractory metastatic breast cancer can be further treated with Trastuzumab applying the concept of treatment beyond progression using the antibody drug conjugate Trastuzumab emtansine (T-DM1). Based on data of the eMIlIA trail, which showed for T-DM1 better results compared with lapatinib plus capecitabine, this new drug antibody complex was approved in november 2013 [20, 24–26].
It is likely that only a certain subgroup of patients, which is defined by the molecular profile of their tumor and its biological surroundings, profits from Trastuzumab mainte-nance therapy. Most of the patients that are mentioned in the literature and 54 % of the patients that were included in our study had liver metastases. This is why it is also pos-sible that the localization of metastases plays a certain role [10].
Arch Gynecol Obstet
1 3
One of the major concerns regarding long-term treat-ment with Trastuzumab is cardiac tolerability. In early registration trials, an increased rate of cardiac side effects was reported—especially when Trastuzumab was com-bined with anthracyclines [2, 10, 27]. In the course of fur-ther evaluations, stricter standards for cardiac screening and monitoring were established. Furthermore, there exist various other co-medications with less severe cardiac side effects.
experience has shown that the rates of cardiac side effects during Trastuzumab therapy, ranging from asymp-tomatic decreases in lVeF to severe heart insufficiency, are very low [2, 4, 28]. A comparison of cardiac events between different clinical studies can hardly be made because the studies differ in the choice of chemotherapeu-tic agents, inclusion and exclusion criteria, definitions of cardiotoxicity and the intervals between anthracycline and Trastuzumab applications [2]. However, available stud-ies reported rates of occurrence of cardiac events between <1 % (in combination with anastrozole) and 27 % (in com-bination with anthracyclines) [4, 27, 28].
The mechanism of Trastuzumab-associated cardiotoxic-ity is still not completely understood. But we know that it differs from anthracycline-induced cardiotoxicity in so far that anthracyclines lead to dose-dependent, irreversible and structural changes in cardiomyocytes. In contrast to that, Trastuzumab-induced cardiotoxicity is due to the blockage of the HeR2 signaling pathway and is reversible. It is based on cellular dysfunctions and does not show histological changes [2–4].
This explains why the cardiac function can fully recover to the initial value within 2–4 months after discontinuation of Trastuzumab, additional help of drugs to treat heart insuf-ficiency may be needed temporarily (e.g., β-blockers, Ace inhibitors) [2, 4, 28]. After the heart function is restored again, Trastuzumab may be reintroduced if it has proven to be effective. close controls of all cardiac parameters need then to be established and maintaining cardioprotective drugs should be considered [4, 28]. Reoccurrences of car-diac events after reintroducing Trastuzumab do not have to be worried about in the majority of the cases [4, 28].
There was only one cardiac event in our study popu-lation that led to discontinuation of Trastuzumab after 41 months. The patient’s lVeF decreased to 46 % (initial value before the beginning of the therapy 57 %). Follow-up checks showed that the lVeF of the patient had increased again to normal values and the patient remained relapse free.
Due to the low number of cases, the statistical value of our data is low. nevertheless, the good cardiac tolerability among our patients coincides with the data in the literature.
In summary, it can be said that the benefits of using Tras-tuzumab for HeR2 positive breast cancer therapy outweigh
by far the risk of cardiac side effects. The remaining risk can be lowered through close screening and monitoring of patients at risk and through interdisciplinary care.
Conclusion
Despite all the progress that has been made in developing new HeR2-targeted agents such as pertuzumab and lapa-tinib, Trastuzumab still remains the gold standard in tar-geted HeR2 positive breast cancer therapy. The clinical challenge of palliative drug therapy for metastasized breast cancer pursues mainly two objectives: firstly, high effec-tiveness regarding progression-free survival needs to be achieved and at the same time therapy-induced and disease-related side effects need to be avoided; secondly, the best
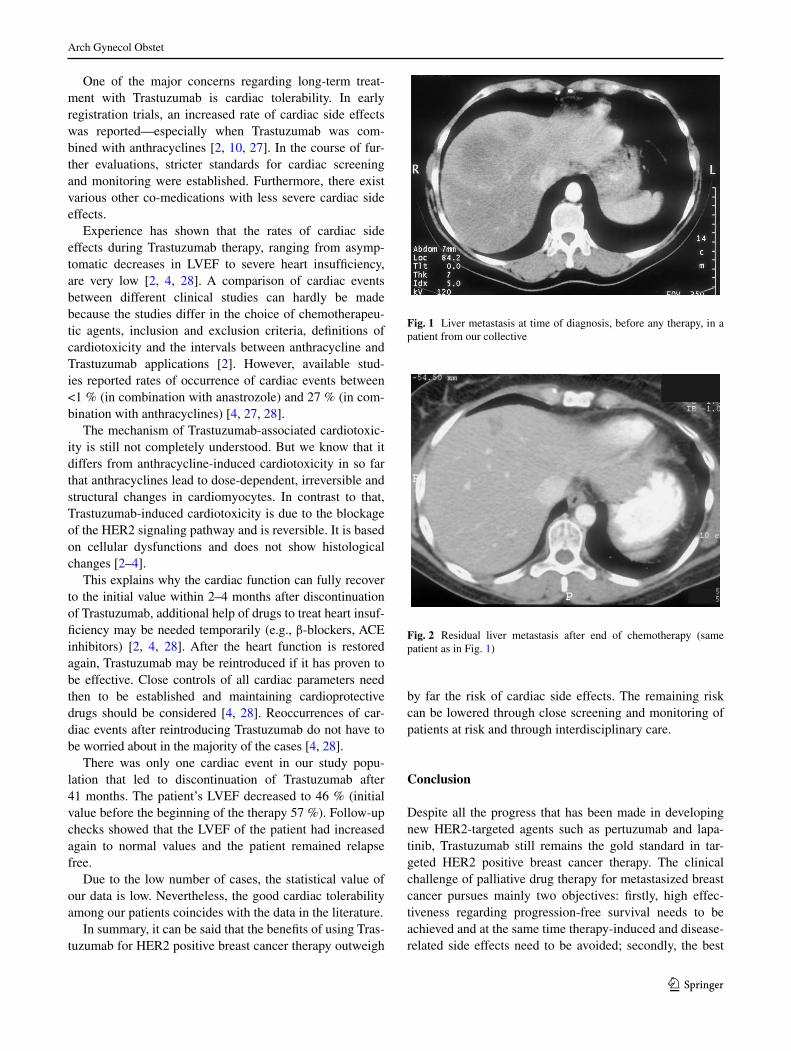
Fig. 1 liver metastasis at time of diagnosis, before any therapy, in a patient from our collective
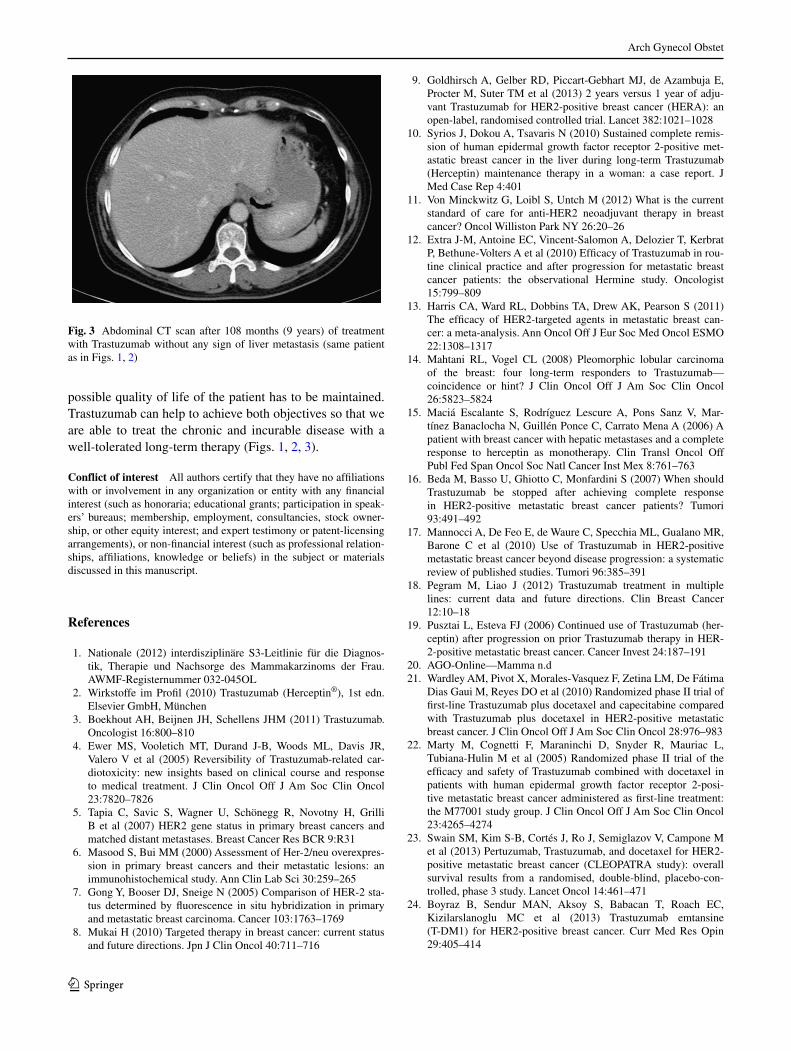
Fig. 2 Residual liver metastasis after end of chemotherapy (same patient as in Fig. 1)
Arch Gynecol Obstet
1 3
possible quality of life of the patient has to be maintained. Trastuzumab can help to achieve both objectives so that we are able to treat the chronic and incurable disease with a well-tolerated long-term therapy (Figs. 1, 2, 3).
Conflict of interest All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speak-ers’ bureaus; membership, employment, consultancies, stock owner-ship, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as professional relation-ships, affiliations, knowledge or beliefs) in the subject or materials discussed in this manuscript.
References
1. nationale (2012) interdisziplinäre S3-leitlinie für die Diagnos-tik, Therapie und nachsorge des Mammakarzinoms der Frau. AWMF-Registernummer 032-045Ol
2. Wirkstoffe im Profil (2010) Trastuzumab (Herceptin®), 1st edn. elsevier GmbH, München
3. Boekhout AH, Beijnen JH, Schellens JHM (2011) Trastuzumab. Oncologist 16:800–810
4. ewer MS, Vooletich MT, Durand J-B, Woods Ml, Davis JR, Valero V et al (2005) Reversibility of Trastuzumab-related car-diotoxicity: new insights based on clinical course and response to medical treatment. J clin Oncol Off J Am Soc clin Oncol 23:7820–7826
5. Tapia c, Savic S, Wagner U, Schönegg R, novotny H, Grilli B et al (2007) HeR2 gene status in primary breast cancers and matched distant metastases. Breast cancer Res BcR 9:R31
6. Masood S, Bui MM (2000) Assessment of Her-2/neu overexpres-sion in primary breast cancers and their metastatic lesions: an immunohistochemical study. Ann clin lab Sci 30:259–265
7. Gong y, Booser DJ, Sneige n (2005) comparison of HeR-2 sta-tus determined by fluorescence in situ hybridization in primary and metastatic breast carcinoma. cancer 103:1763–1769
8. Mukai H (2010) Targeted therapy in breast cancer: current status and future directions. Jpn J clin Oncol 40:711–716
9. Goldhirsch A, Gelber RD, Piccart-Gebhart MJ, de Azambuja e, Procter M, Suter TM et al (2013) 2 years versus 1 year of adju-vant Trastuzumab for HeR2-positive breast cancer (HeRA): an open-label, randomised controlled trial. lancet 382:1021–1028
10. Syrios J, Dokou A, Tsavaris n (2010) Sustained complete remis-sion of human epidermal growth factor receptor 2-positive met-astatic breast cancer in the liver during long-term Trastuzumab (Herceptin) maintenance therapy in a woman: a case report. J Med case Rep 4:401
11. Von Minckwitz G, loibl S, Untch M (2012) What is the current standard of care for anti-HeR2 neoadjuvant therapy in breast cancer? Oncol Williston Park ny 26:20–26
12. extra J-M, Antoine ec, Vincent-Salomon A, Delozier T, Kerbrat P, Bethune-Volters A et al (2010) efficacy of Trastuzumab in rou-tine clinical practice and after progression for metastatic breast cancer patients: the observational Hermine study. Oncologist 15:799–809
13. Harris cA, Ward Rl, Dobbins TA, Drew AK, Pearson S (2011) The efficacy of HeR2-targeted agents in metastatic breast can-cer: a meta-analysis. Ann Oncol Off J eur Soc Med Oncol eSMO 22:1308–1317
14. Mahtani Rl, Vogel cl (2008) Pleomorphic lobular carcinoma of the breast: four long-term responders to Trastuzumab—coincidence or hint? J clin Oncol Off J Am Soc clin Oncol 26:5823–5824
15. Maciá escalante S, Rodríguez lescure A, Pons Sanz V, Mar-tínez Banaclocha n, Guillén Ponce c, carrato Mena A (2006) A patient with breast cancer with hepatic metastases and a complete response to herceptin as monotherapy. clin Transl Oncol Off Publ Fed Span Oncol Soc natl cancer Inst Mex 8:761–763
16. Beda M, Basso U, Ghiotto c, Monfardini S (2007) When should Trastuzumab be stopped after achieving complete response in HeR2-positive metastatic breast cancer patients? Tumori 93:491–492
17. Mannocci A, De Feo e, de Waure c, Specchia Ml, Gualano MR, Barone c et al (2010) Use of Trastuzumab in HeR2-positive metastatic breast cancer beyond disease progression: a systematic review of published studies. Tumori 96:385–391
18. Pegram M, liao J (2012) Trastuzumab treatment in multiple lines: current data and future directions. clin Breast cancer 12:10–18
19. Pusztai l, esteva FJ (2006) continued use of Trastuzumab (her-ceptin) after progression on prior Trastuzumab therapy in HeR-2-positive metastatic breast cancer. cancer Invest 24:187–191
20. AGO-Online—Mamma n.d 21. Wardley AM, Pivot X, Morales-Vasquez F, Zetina lM, De Fátima
Dias Gaui M, Reyes DO et al (2010) Randomized phase II trial of first-line Trastuzumab plus docetaxel and capecitabine compared with Trastuzumab plus docetaxel in HeR2-positive metastatic breast cancer. J clin Oncol Off J Am Soc clin Oncol 28:976–983
22. Marty M, cognetti F, Maraninchi D, Snyder R, Mauriac l, Tubiana-Hulin M et al (2005) Randomized phase II trial of the efficacy and safety of Trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-posi-tive metastatic breast cancer administered as first-line treatment: the M77001 study group. J clin Oncol Off J Am Soc clin Oncol 23:4265–4274
23. Swain SM, Kim S-B, cortés J, Ro J, Semiglazov V, campone M et al (2013) Pertuzumab, Trastuzumab, and docetaxel for HeR2-positive metastatic breast cancer (cleOPATRA study): overall survival results from a randomised, double-blind, placebo-con-trolled, phase 3 study. lancet Oncol 14:461–471
24. Boyraz B, Sendur MAn, Aksoy S, Babacan T, Roach ec, Kizilarslanoglu Mc et al (2013) Trastuzumab emtansine (T-DM1) for HeR2-positive breast cancer. curr Med Res Opin 29:405–414
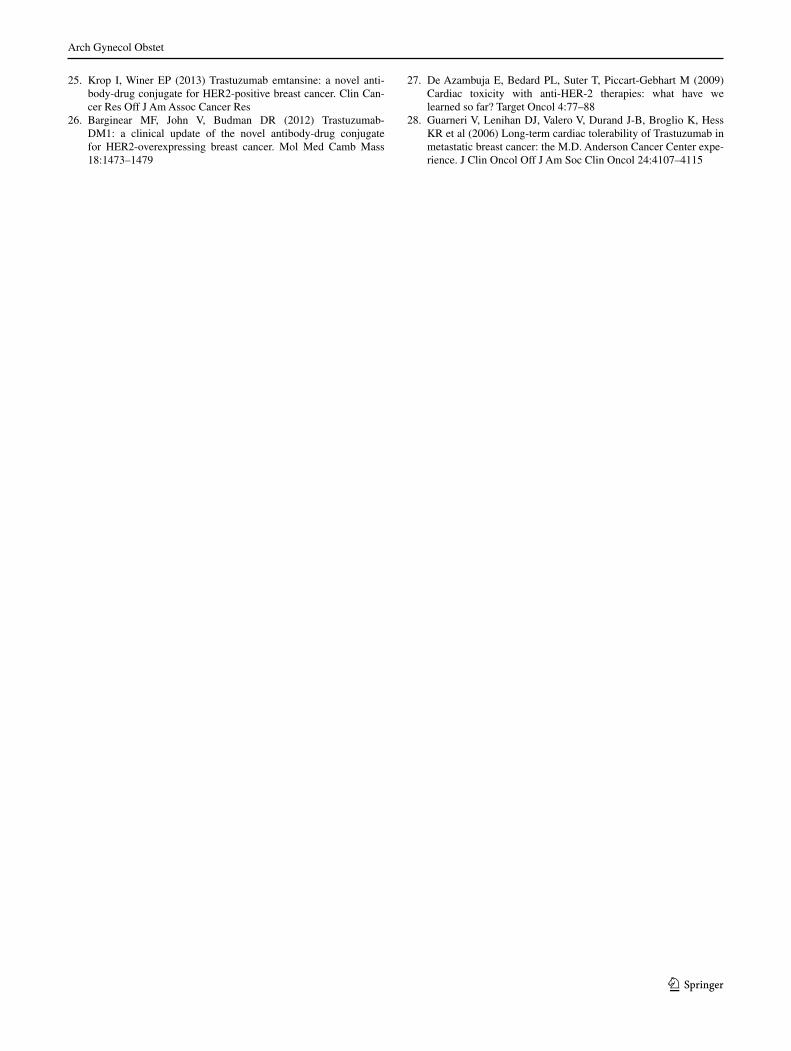
Fig. 3 Abdominal cT scan after 108 months (9 years) of treatment with Trastuzumab without any sign of liver metastasis (same patient as in Figs. 1, 2)
Arch Gynecol Obstet
1 3
25. Krop I, Winer eP (2013) Trastuzumab emtansine: a novel anti-body-drug conjugate for HeR2-positive breast cancer. clin can-cer Res Off J Am Assoc cancer Res
26. Barginear MF, John V, Budman DR (2012) Trastuzumab-DM1: a clinical update of the novel antibody-drug conjugate for HeR2-overexpressing breast cancer. Mol Med camb Mass 18:1473–1479
27. De Azambuja e, Bedard Pl, Suter T, Piccart-Gebhart M (2009) cardiac toxicity with anti-HeR-2 therapies: what have we learned so far? Target Oncol 4:77–88
28. Guarneri V, lenihan DJ, Valero V, Durand J-B, Broglio K, Hess KR et al (2006) long-term cardiac tolerability of Trastuzumab in metastatic breast cancer: the M.D. Anderson cancer center expe-rience. J clin Oncol Off J Am Soc clin Oncol 24:4107–4115