transforming end of life care in acute hospitals - plenary 2 - heidi smoult, care quality commission
TRANSCRIPT

1
The role of the CQC in improving EOLC
Heidi Smoult
Deputy Chief Inspector of Hospitals
Care Quality Commission
November 2015

Overview
• Our purpose and role as an independent regulator
• Our new approach to inspecting EOLC
• Ratings summaries in each key question so far
• Themes and key points in EOLC
• Overview of the thematic review in EOLC to address inequalities
2
3
Our purpose and role
Our purpose
We make sure health and social care services
provide people with safe, effective,
compassionate, high-quality care and we
encourage care services to improve
Our role
We monitor, inspect and regulate services to
make sure they meet fundamental standards
of quality and safety and we publish what we
find, including performance ratings to help
people choose care

4
We ask these questions of all services:
• Is it safe?
• Is it effective?
• Is it caring?
• Is it responsive?
• Is it well led?
4
Our New Approach

Our new approach to inspecting:
3 Phases
1. Pre-inspection: Selection of hospital location Planning PIR Recruitment of teams
2. Inspection: Larger team 8 core services 5 key questions Visits to clinical areas Staff focus groups Interviews with senior managers Announced and unannounced visits
3. Post-inspection: Report writing Confirmation of ratings Quality Summit
5

Core Services
• The following 8 core services will always be inspected for NHS inspections. Highlighted in red are the most commonly used in independent healthcare
1. Urgent and emergency services
2. Medical care, including frail elderly
3. Surgical care, including theatres
4. Critical care
5. Maternity and gynaecology
6. Children and young people
7. End of Life Care
8. Outpatients and diagnostic imaging
• We will also assess other services if there are concerns (e.g. from complaints or from focus groups)
6

Ratings
7
• We rate each service on each of the five key questions
• Safe? Effective? Caring? Responsive? Well led?
• 4 point scale: Outstanding
Good
Requires Improvement
Inadequate

EOLC Ratings - Overall
8

EOLC rating - Safe
9
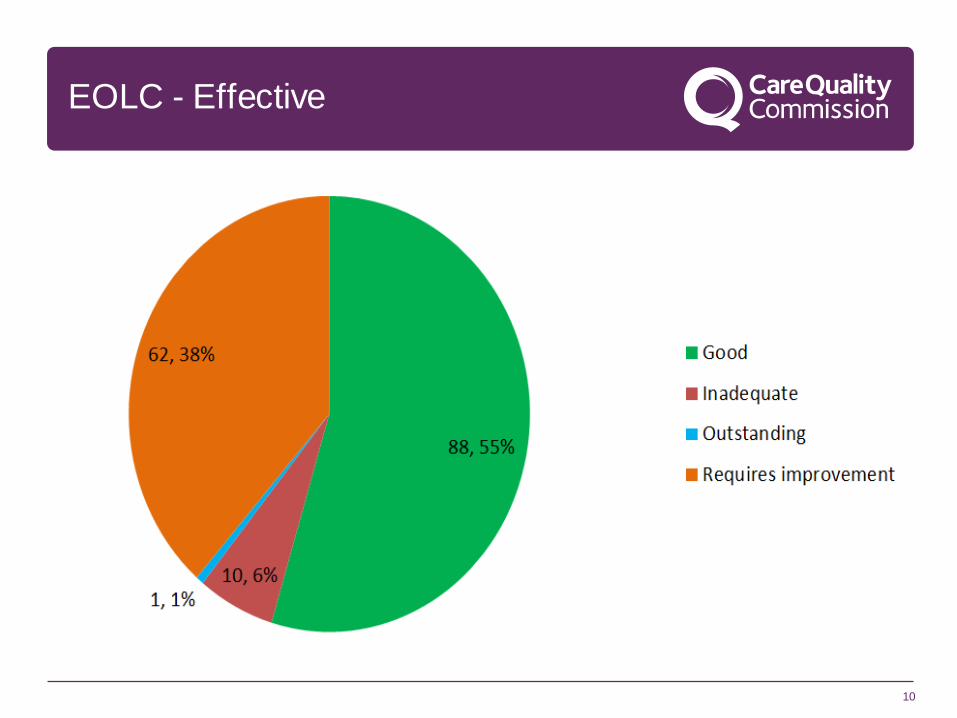
EOLC - Effective
10

EOLC ratings - Caring
11

EOLC ratings - Responsive
12
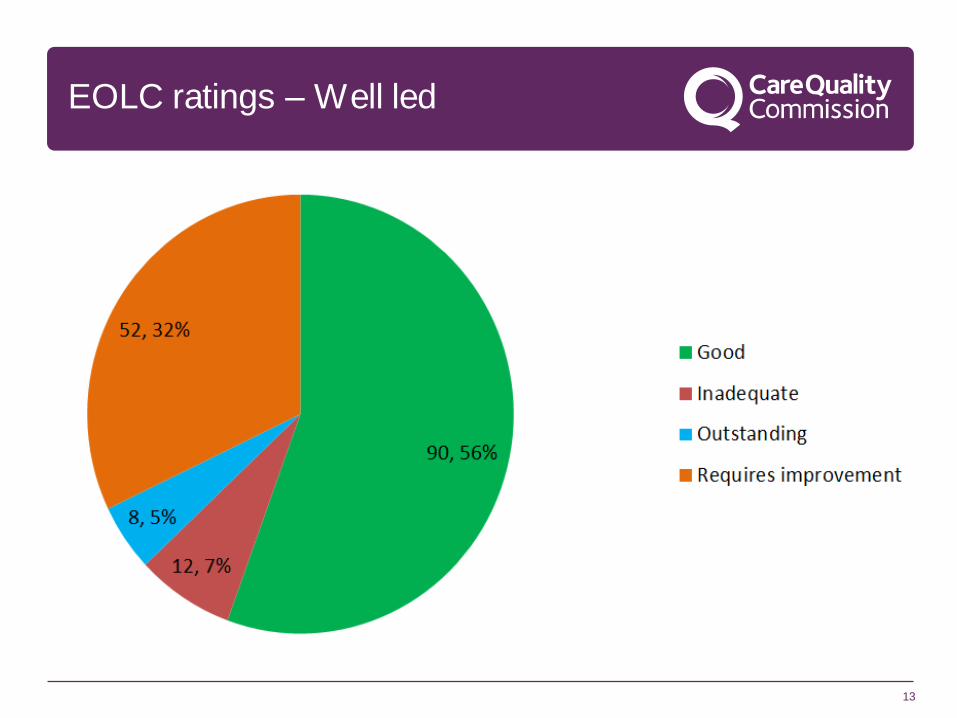
EOLC ratings – Well led
13

Hospital ratings grid
14

Themes & key points – Well Led
15
• Many trusts simply do not give EOLC sufficient priority at all levels.
• We often find there is no board level leadership or that it is tokenistic.
• Ward level leadership may be clearer, but there is often no trust wide
leadership group for EOLC; such time allocated in job plans or specific
operational oversight.
• Limited vision or strategy (and very rarely any firm goals or milestones)
• Poor governance. For example; which wards have the most patients
identified on EOLC pathway and do those wards with lower numbers
identify patients well? Was the care individualised?
• We often see poor links with the community, to plan care & manage rapid
discharges.
• Lack of a plan and resourcing to train staff on EOLC

Themes & key points – Responsive
16
• Our findings on this are variable, as some do this very well
Key points:
• Are they able to nurse dying patients in side rooms if this is their choice?
• Are they able to support relatives who want to stay overnight?
• How quickly can they discharge patients? This varies from hours to days.
• Is there a good chaplaincy service to meet the spiritual needs of patients?
• Is there any dedicated service to support relatives?
• How responsive is the bereavement service?
• How responsive is the mortuary service?
• Is there any access to care/follow up for relatives some time after death?
These aspects can be separated into three time periods - before death,
immediately after death and later.

Themes & key points – Caring
17
• We usually observe good care, but we only observe a very limited number of
patients approaching EOLC
• Does the hospital attempt to assess the care provided to people at the end
of life (e.g. Through surveys of bereaved relatives)?
• Talk to relatives but it can be too early to gain their view of the EOLC service
overall

Themes & key points – Safe & Effective
18
• Most trusts do not have any formal/routine process for identifying patients who are
likely to be nearing the end of life. This means it is much more difficult to assess their
needs and to plan their care.
• Advance care planning is inconsistent and often not ‘person centred’. Ceilings of care
should be agreed. This includes DNACPR, but goes wider (e.g. do they want
antibiotics if they develop an infection?).
• The size and composition of the specialist palliative care team may be inadequate for
the caseload.
• The team is often not staffed to provide a 7/7 service
• Specific EOLC competency training of ‘champions’ and ward staff is often limited
• In some places the proportion of all referrals to the SPCT team who have cancer is
still around 90%. This strongly suggests that non-cancer patients are missing out.
• Pain control may not be being adequately monitored.
19
Thematic review: Inequalities and
variation in EOLC
• Our thematic review programme expands the
understanding of quality of care beyond our existing
regulatory activity, and provides an authoritative voice
on priority issues.
• We prioritised End of Life care as a topic for a thematic
review in 2014 as part of our response to the review of
the Liverpool Care Pathway.
• We wanted to build on our strengthened focus on quality of End of Life Care in
inspection of registered services through looking at people’s experience of End of
life Care across services.
• We asked our stakeholders, including people who use services, what aspect of
EOLC we should focus on, and they said the differences in quality of care which
people experience due to diagnosis, age and other factors.
• Inequalities in people’s experience of end of life care, both between different
geographical areas and across different groups of people, are well-documented.
20
Inequalities and variation in EOLC:
our questions
1. What are the barriers to people from some groups getting good care at the
end of life?
• People with a diagnosis other than cancer
• Older people (over 75)
• People with dementia
• People from BAME groups
• Other groups of people who may have specific needs: people with
learning disabilities, people with mental health needs, LGBT
people, people who are homeless, prisoners, travellers and
Gypsies.
2. What good practice can others learn from at local level?
3. What action can national and local stakeholders take in the next five years
to address inequalities?

21
Inequalities and variation in EOLC:
our work streams
1. Data review: CCG profiles using national level data informed selection of a
sample of CCGs. We found limited data at CCG level on quality of EOLC.
2. CCG perspective: We asked a sample of 43 CCGs about EOLC in their
area, and how they meet the needs of the groups we have prioritised. We
found that almost all CCGs were making provision for EOLC, but a smaller
number were making specific provision for the needs of specific groups.
3. People’s experience: We ran an online survey earlier this year asking
people to share their experience of EOLC with us. We are now working with
National Council for Palliative Care, Race Equality Foundation and National
Voices to talk to people in local areas about the care they have experienced.
4. Local area fieldwork: We are visiting 18 local areas to talk to people with
experience of EOLC, and to commissioners and providers of EOLC about
how care across services meets people’s needs.

Next steps…..
• Review reports of NHS inspections in more detail and share themes with providers
• Review our guidance on EOLC, particularly in relation to safe and effective
• Consider how we can strengthen information in relation to our ‘caring’ key question
• Work closely with other key stakeholders to develop our process and drive improvements in EOLC
• Review the information from the thematic review in conjunction with acute hospital findings
22

Any questions?
23

Join our team
24
To join CQC and help to drive quality improvement through our inspection programme
Become an Inspector:
(Permanent or on Secondment) [email protected]
Become a Specialist Advisor:
(Clinician) [email protected]
Become an Expert by Experience:
(Patient or Carer) [email protected]