thymus - humsc.net
TRANSCRIPT

▪ So here we see the thymus, it's one of the most important organs of the
immune system, the thymus lies behind the sternum, superior to the heart,
and it is the largest during childhood, and it becomes to get smaller with
age.
▪ Also, we have the spleen, which one of the important filters of the blood for
the invading foreign pathogens or antigens.
▪ Also, we have the lymph nodes which is present in multiple locations in the
human body.
▪ Also, we have the Peyer’s patches in the small intestine, we have the
appendix in the cecum, and we have the lymphatic vessels.
Thymus
Peyer’s
patches
(small
intestine)
Appendix
(cecum)
Lymph
nodes
Spleen
Lymphatic
vessels
Adenoid
Tonsils
Blood
capillary Interstitial
fluid
Lymphatic
vessel
Tissue
cells
Masses of
defensive cells Lymph
nodes

SCIENTIFIC TEAM 1 – الفريق العلمي
❖ Classification of Allograft Rejection: There are 2 types of allogeneic
reactions:
▪ Host versus graft reaction (HVGR): Conventional organ transplantation
▪ Host versus graft reaction (HVGR) which is the reaction seen in
conventional organ transplantation, in which the immune system of the host
attacks the graft and may result in rejection
▪ Graft versus host reaction (GVHR)
• Bone marrow transplantation
• Immune cells transplantation
▪ Graft versus host reaction (GVHR) which is commonly seen in bone marrow
and stem cells transplantations, in which the immune cells of the graft
attacks the host’s tissue
❖ Host Versus Graft Reaction (HVGR)
Host versus graft reaction have 3 types:
▪ Hyperacute rejection سريع جدا
▪ Acute rejection
▪ Chronic rejection
❖ 1. Hyperacute Rejection
▪ Occurrence time: Occurs within minutes to hours after host blood vessels
are anastomosed to graft vessels.
▪ It includes thrombotic occlusion of the graft vessels , ischemia ,
denaturation , necrosis
بسم الله الرحمن الرحيم
الأسود: كلام الدكتور ✓
السلايد الأزرق: ✓
ممكن تشوفوا بنفس السطر أسود وأزرق ، هاد معناه انه الدكتور عم بقرأ -
.. بس بطريقة ثانية لأنه الجملة بتكون لحالها مش مفهومة السلايد

SCIENTIFIC TEAM 2 – الفريق العلمي
▪ Pathology: Thrombotic occlusion of the graft vasculature, ischemia,
denaturation, necrosis
▪ Mechanisms:
- 1. Preformed antibodies
• Antibody against ABO blood type antigen
• Antibody against vascular endothelial cells (VEC) antigen
• Antibody against HLA antigen
ن العضو المراد نقله و المستلم له فإن هناك HLA antigensحتى لو تم فحص ال ▪ لمعرفة التوافق بي
ة ات كثي احتمالية لعدم التوافق لوجود متغي
- 2. Complement activation: Endothelial cell damage
- 3. Platelet activation: thrombosis, vascular occlusion, ischemic damage
❖ 2. Acute Rejection
▪ Occurrence time: Occurs within days to 2 weeks after transplantation, 80-
90% of cases occur within 1 month
▪ Pathology
– Acute humoral rejection: Acute vasculitis manifested mainly by
endothelial cell damage
▪ Its pathology results from acute humoral reaction in which antibodies are
formed against endothelial cells resulting in damaging them resulting in
acute vasculitis.
– Acute cellular rejection: Parenchymal cell necrosis along with infiltration of
lymphocytes and MΦ
▪ Also, from acute cellular reaction attacking parenchymal cells leading to
their necrosis and infiltration of macrophages and neutrophils,
▪ Mechanisms

SCIENTIFIC TEAM 3 – الفريق العلمي
▪ Vasculitis
– IgG antibodies against alloantigen son endothelial cell
– CDC complement dependent cytotoxicity
▪ vasculitis → from Ig G antibodies attacking endothelial allogeneic antigens
and complement dependent cytotoxicity by membrane attack complex MAC
on endothelial cells resulting in lysis.
▪ Parenchymal cell damage
–Delayed hypersensitivity mediated by CD4+Th1
–Killing of graft cells by CD8+Tc
▪ parenchymal cells damage → type 4 hypersensitivity:
1) CD4+ T cells → cytokines → Macrophage activation →
produce lysozymes and oxygen free radicals and →
complement activation
2) CD8+ direct killing of these cells
❖ 3. Chronic Rejection
▪ Occurrence time: Develops months or years after acute rejection reactions
have subsided
▪ Pathology: Fibrosis and vascular abnormalities with loss of graft function
▪ Mechanisms
• Not clear
• Extension and results of cell necrosis in acute rejection
• Chronic inflammation mediated by CD4+T cell/MΦ
• Organ degeneration induced by non-immune factors
▪ Its mechanism is unclear but thought to be mediated by type 4
hypersensitivity through macrophages activation and CD4+ cells , also may
be due to non-immune factors causing degeneration, and as an extension
and results from acute reaction after it subsided.

SCIENTIFIC TEAM 4 – الفريق العلمي
ح ▪ وري تشوفوه م 3على رسمة عن الأنواع ال هون الدكتور ببدأ يشر . 39:53ن الفيديو دقيقة فضن

SCIENTIFIC TEAM 5 – الفريق العلمي
❖ II. Graft Versus Host Reaction (GVHR)
▪ Graft versus host reaction (GVHR)
• Allogenetic bone marrow transplantation
• Rejection to host alloantigens
• Mediated by immune competent cells in bone marrow
▪ Graft versus host disease (GVHD)
• A disease caused by GVHR, which can damage the host
▪ Graft versus host reaction happens commonly in allogeneic bone marrow
transplantation, mediated by intact graft immune cells which recognize host
cells and antigens and attacking them. Graft versus host reaction results in
graft versus host disease
▪ Conditions:
• Enough immune competent cells in grafts
• Immunocompromised host
• Histocompatability differences between host and graft
❖ 1. Acute GVHD
▪ 10-100 days post-transplant
▪ Occur in 30-50% of allogenic transplant recipients
▪ Endothelial cell death in the skin, liver, and
gastrointestinal tract
▪ Rash (palms and soles), nausea, vomiting,
diarrhea, loss of appetite, jaundice, abdominal
pain, wtloss, and gastrointestinal hemorrhage.
▪ Symptoms are rash on palms and soles,
nausea, vomiting, diarrhea, loss of appetite,
jaundice, abdominal pain, weight loss and GI
hemorrhage.
SCIENTIFIC TEAM 6 – الفريق العلمي
▪ Graded I-IV (skin, liver, gut). Poor prognosis IV
▪ Mediated by mature T cells in the grafts
▪ The reaction is graded according to severity from I to IV where IV is the
severest ي الجلد و الكبد و القناة , وبحيث تجمع التصنيفات و تكون الهضمية,التصنيف يكون فن
هي الأعلى و الأشد. 10و 11و 12القيم
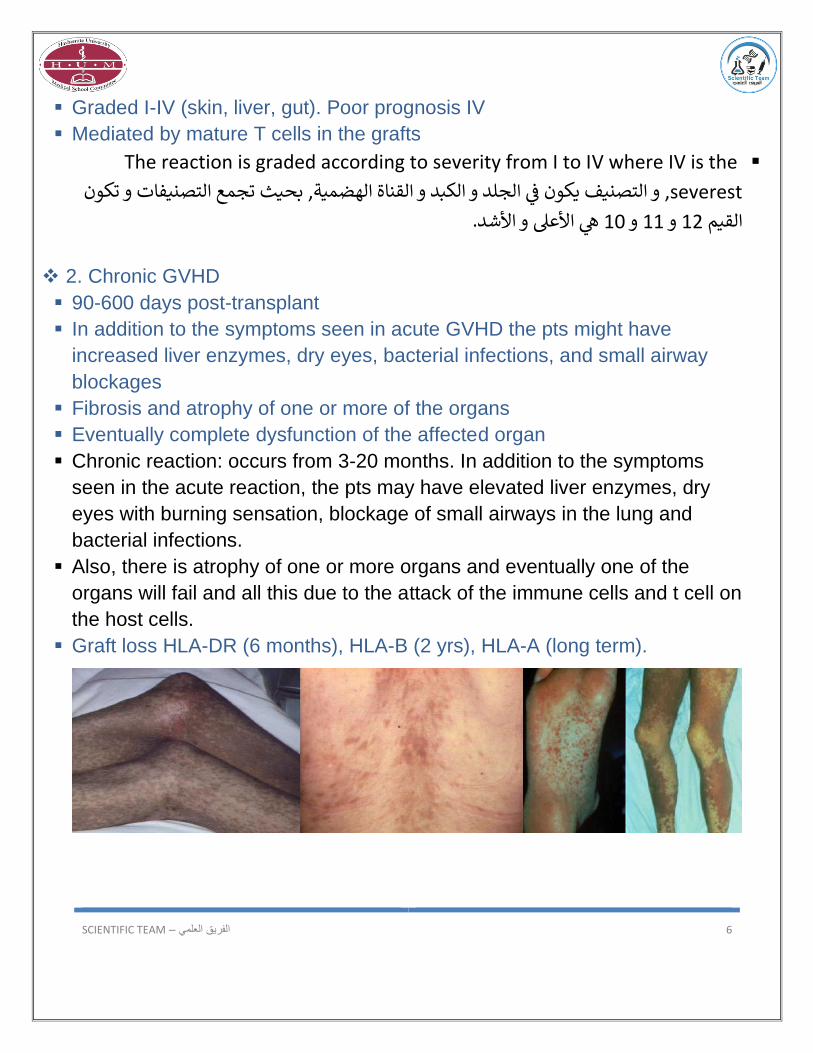
❖ 2. Chronic GVHD
▪ 90-600 days post-transplant
▪ In addition to the symptoms seen in acute GVHD the pts might have
increased liver enzymes, dry eyes, bacterial infections, and small airway
blockages
▪ Fibrosis and atrophy of one or more of the organs
▪ Eventually complete dysfunction of the affected organ
▪ Chronic reaction: occurs from 3-20 months. In addition to the symptoms
seen in the acute reaction, the pts may have elevated liver enzymes, dry
eyes with burning sensation, blockage of small airways in the lung and
bacterial infections.
▪ Also, there is atrophy of one or more organs and eventually one of the
organs will fail and all this due to the attack of the immune cells and t cell on
the host cells.
▪ Graft loss HLA-DR (6 months), HLA-B (2 yrs), HLA-A (long term).

SCIENTIFIC TEAM 7 – الفريق العلمي
❖ Laboratory Studies:
There are many laboratory tests that must be done before transplantation:
▪ ABO and Rh blood typing
▪ ABO and Rh antigens compatibility because any incompatibility may result
in hyperacute reaction in blood transfusions.
▪ Crossmatching (Preformed antibodies)
▪ cross-matching: we take blood from the recipient and the donor and mix
them to see if there is any immunologic reaction, if the reaction happens
then it is due to preformed antibodies that may be formed in pregnancy by
mixture of one’s blood and his mother’s, like antibodies vs Rh antigen.
▪ Also, if one of them had transfusion blood previously. we test all of this by
crossmatching to detect any preformed antibodies.
▪ HLA typing
• HLA-A and HLA
• HLA-DR
▪ Lymphocytotoxicity test:
determine whether a patient already has any specific HLA antibodies, a lab
specialist will test a patient's blood (serum) against lymphocytes obtained
from a panel of about 100 blood donors.
ي حالة الـ ▪ against specific HLAالفحص هون رح يكون Lymphocytotoxicity testبالتالي فن
antibodiesكيف بنعرف انه هاي الـ ، specific HLA antibodies موجودة ولا لأ؟
lymphocytes obtained from a panel ofمن المريض ونخلطه مع serumرح نجيب الـ
about 100 blood donors .. واللىي بكون موجود عنا اوريدي بالمختير
اللىي HLA antigen رح يتفاعل مع الـ Recipient bloodبالـ Anti-HLA antigenهسا اذا عنا
. ن موجود بدم المانحي

SCIENTIFIC TEAM 8 – الفريق العلمي
ي إ Recipientشخص ال ـقبل ما نعمل عملية الزراعة بنفحص ال، عن Anti-HLA ABs عنده ذا فن
اللىي حكينا عنها ، القاعدة بتحكي : panel مع الـ Serumطريق انه بنخلط الـ
The more the reaction against these 100 blood donors, the higher rejection.
ي لو عملنا سكيل من ي تفاعل، و 0، بحيث انه 10ل ـ 0يعتن
ي ما فني التفاعل 10يعتن
%.. 100يعتن
ي الـ 2لو طلع التفاعل ي احتمالية 10-7بكون خفيف وضعيف، بينما لو طلع Rejectionيعتن
بالتالي فن
. Mismatch & rejectionأكير لأنه يصي عنا
▪ Mixed leukocyte reaction
▪ Screening for Presence of Preformed Antibodies to allogeneic HLA
ن بنفحص فيهم عن الـ Lymphocytotoxicity test شبيها بال ـهاي Anti-HLA Antigens، التنتي
❖ Identifying MHC Polymorphisms (Tissue typing)
▪ Tissue typing ensures that an organ from a donor will be
compatible with its recipient. The process starts with
identifying the unique human leukocyte antigens (HLAs)
for the organ donor and recipient, either from blood or
tissue.
Humanوجود على الـبكون م HLA MHC Complexالـ ▪
chromosome 6 ي عنا الـ + HLA-1 + HLA-Bاللىي هي HLA Class 1، وفن
HLA-C عنا الـ، وHLA Class 2 اللىي هيHLA-DP + HLA-DQ + HLA-DR
▪ Formerly determined by antibodies against MHC
molecules.
لطوها مع ، ويخRecipient ـمن ال Serumكانوا بالبدايات يعملوها عن طريق انهم ياخدوا الـ ▪
اللي MHC Antigensرح تتفاعل مع الـ Anti-HLA Antibodies، الفكرة انه اذا عنا donors الـ
، وزي ما حكينا كل ما زاد التفاعل بزيد احتمالية الرفض. Test Tubeموجودة بالـ

SCIENTIFIC TEAM 9 – الفريق العلمي
ي نسبة للتغي بالآلاف خصوصا انه عنا More specificبعد هيك صرنا ندور عأشياء تكون ▪لانه فن
ن بحيث انه نقدر نحدد بدقة لأنه حتى لو صار التغي ع HLA Class 2الـو HLA Class 1الـ نوعي
هو بسببه Amino acedوهاد ال ـ Amino acedمستوى نيوكليوتيد واحد رح يكون اله تأثي عال ـ
DNA testing by allele specific PCR, sequencing، لهيك صرنا نعمل Rejectionصي الـي
ن الـsequence ، ونقارن هاد الـPrimer to look for specific sequence، ونستعمل Donorبي
ن بالـ sequencing.. وممكن برضه نعمل Recipient والـ ن الـونقارن Alleleبجزء معي Donorبي
ي اللىي بصي حاليا وبكون أكير دقة وبقلل فرصة الـRecipient والـ .Rejectionوهاد الاشر
▪ Now by DNA testing: allele specific PCR, sequencing
❖ Mixed Lymphocyte Reaction:
، بنخلط Allele A & B from Recipientو Allele A from donorهون بكون عنا ▪
ن تاعون Lymphocytesالـ ن بس بنكون عاملي Allele A A from donorللـ Irradiationالتني
. Cell Proliferationوبعدها بنطلع على الـ -مثلا H5 thymidine باستخدام الـ-
▪ Strong Proliferation ---> High incompatibility
▪ Weak proliferation ---> Low incompatibility
▪ No proliferation ---> 100% compatibility
▪ Helps to identify any antigenic differences between donor and recipient
؟ ▪ ي )شوفوا الصورة تحت مهمة( شو يعتن
ما بالتالي Mismatchما بصي عنا Allele A from Recipient والـAllele A from donor اذا ال ـ -
وبالتالي ما بصي T Cell proliferation & differentiation & clonal expansionعنا بصي
.Reactionعنا

SCIENTIFIC TEAM 10 – الفريق العلمي
ي حال كان الـ - Activation & Proliferationرح يصي Recipient مختلف على الـ Alleleفن
ي دخل عليهم الـRecipient cells للـبالنسبة الهم لأنه Foreignواللىي بكون Allele A، يعتن
Mismatch نا ع بصي بالتاليCell proliferation & differentiation & clonal expansion
Incorporation in DNA of عن طريق انه بصي Irradiation خلال الـ Detectionوبصي الـ
newly formed proliferated cells للـ H5 thymidine فرصة اللىي حكينا عنه.. وبالتالي
.. بتكون عالية جدا Rejectionالـ

SCIENTIFIC TEAM 11 – الفريق العلمي
❖ Immunosuppressive Therapy
ي حال صار ال ـ ▪ما بهمنا كثي التفاصيل فقط ، شو العلاجات اللىي بنقدر نستخدمها؟ Rejectionفن
الاسماء ..
▪ Cyclosporine (CsA), FK506: Inhibit nuclear factor of activated T-cells
(NFAT) transcription factor
▪ Azathioprine, Cyclophosphamide: Block the proliferation of lymphocytes
▪ Ab against T cell surface molecules: Anti-CD3 mAb ---- Deplete T cells
▪ Anti-inflammatory agents: Corticosteroids ---- Block the synthesis and
secretion of cytokines
❖ Induction of Immune Tolerance
ي طريقة لأنه نخدع جهاز المناعة والجسم ونخليه يفهم انه هاي ال ـ ▪ self-organsهي Organsفن
ونقلل التفاعل ضدها، عن طريق:
▪ Inhibition of T cell activation:
• Soluble MHC molecules
Availability of the T cellsمعناته رح نخفف من الـ Soluble MHC moleculesلما نعطي ▪
that is going to target the graft ورح يرتبط عدد كبي جدا منها مع الـ Soluble MHC
molecules بالتالي رح يقل عدد الـ T cellsاللىي مع الـGraft.
• CTLA4-Ig
حكينا أول Activation of T cellلما يبدأ الـ ▪
signal ن الـ انه T Cellوالـ MHCيصي ارتباط بي
Receptor، وال ـ signalي انه ال ـلازم يرتبط B7الثانن
.Co-stimulatorوسميناها CD28مع الـ
عن Inhibition of signal 2فاحنا هون بنعمل ▪
بنخليها CD4ترتبط مع الـ B7طريق انه بدل ما ال ـ
Inhibatoryوبتتحول إل CTLA-4 ترتبط مع الـ
effect بدلstimulatory effect.

SCIENTIFIC TEAM 12 – الفريق العلمي
Inhibitionبسبب انه صار Unresponsiveness toward the graftبالتالي بصي عنا
Activation of T cellلـل
• Anti-IL2R mAb
ه زي ما هو موضح بالصورة تأثي
▪ Th1 cytokines
• Anti-TNF-α,Anti-IL-2,Anti-IFN-γ mAb
IL-2 والـTNF-α زي الـ cytokinesرح تعطينا TH1، الـ Activationبنعرف انه لما يصي عنا ▪
رح يصي Anti-TNF-α,Anti-IL-2,Anti-IFN-γ، وبالتالي إذا أعطينا IFN-γ والـ
Inhibition of TH1 proliferation

SCIENTIFIC TEAM 13 – الفريق العلمي
▪ Micro chimerism
• The presence of a small number of cells of donor, genetically distinct from
those of the host individual
hybridization من اسمها فهي زي الـ ▪
ة من Hypersensitivityلما حكينا عن علاج الـ حكينا ممكن نعطي جرعات صغي
ي Toleranceومع الزمن ممكن يصي عنا Immunogenالـ .. وهون نفس الاشر
ن قليلة من ال ـ ي الـ Antigensوجود تراكي وبتعمل Micro chimerismبنسميها cells of donor فن
Induction of tolerance.
❖ Removal of T cells from Marrow Graft
▪ Methods to overcome GVHR:
GVHR : Graft Vs Host diseases
• Treat bone marrow to deplete T cells.
، T cellsحكينا انه المشاكل بتصي بسبب الـ ▪
قبل ما Bone marrowمن ال ـبالتالي لو شلناها
، GVHR نعطيها للمريض هاد رح يخفف الـ
، Magnetic Antibodiesبنشيلها عن طريق الـ
تبط مع الـ microbeadsبكون عنا ABsبيى
وبعدها T cellsبتقدر تحدد الـ ABsوبالتالي الـ
bone من الـ T cellsبنقدر نسحب الـ
marrowقبل ما يتم زراعته بالـRecipient .
• Use autologous bone marrow.
من المريض نفسه ونعمله معالجة بحسب ما تتطلب الحاجة bone marrowممكن ناخد ▪
ها Any recognition of any foreignونرجع نرجعله إياه بالتالي ما بصي عنا لانه بيعتير
Self-Antigen
• Use umbilical cord blood.
ي ▪ . Any recognition of any foreignما بصي عنا نفس الشر

SCIENTIFIC TEAM 14 – الفريق العلمي
، وجدوا انه بنقدر نعمل 2بالأطفال أقل من عمر Organ transplantلما نحكي عن ال ـ ▪
transplant حتى لو عندهمMismatch لأنه الـImmune system بكون عندهمIsn’t
mature enough بالتالي ممكن نعمل ،Graft ي شويةوبتكون نسبة Mismatchesحتى لو فن
ي فيهي بنلجأله بالحالات اللىي بكون صعب علينا نلافى
Completelyالنجاح جيدة، وهاد الاشر
matched ..
ي ! Completely matchedأما طبعا بالكبار لا ممنوع نعطي الا اشر
❖ Why is Fetus not Rejected?
تاعون الامرأة نفسها . ليه ما Antigensهو جسم موجود داخل الامرأة مختلف عن ال ـ Fetusالـ ▪
؟Rejectionبصي هون
▪ Placenta acts as a barrier or filter. It filters anti-MHC Abs.
▪ Trophoblast---outermost layer of fetal tissue---is in direct contact with
maternal blood. Trophoblast expresses weak or no MHC.
▪ Progesterone---hormone---immunosuppressive.
▪ Uterine epithelium and trophoblast* secrete cytokines that suppresses
TH1
▪ Spontaneous abortions are sometimes triggered by maternal immune
response against fetus بحالات قليلة جدا وهون بنعمل اجهاض .. .
.. 16 ديوالفي لهون وصلنا آخر رحلتنا مع
^^.. لا تنسونا من صالح دعائكم
حفظكم ورعاكم الله الله، أعانكم الله،وفقكم