thoracoabdominal aortic aneurysm - …intensivistenopleiding.org/downloads-25/files/taaa.pdf ·...
TRANSCRIPT
Thoracoabdominal aortic aneurysm
Patient (1)
• ♀ - 69
• PMH: 2013 - MVP, aortic root replacement with biological valve (Perimount) and subtotal aortic arch replacement
• Analysis for oppressive chest complaints reveals large thoracoabdominal aortic aneurysm


Underlying disease?• Marfan
• Ehlers-Danlos
• Turner’s syndrome
• Polycystic kidney disease
• Loeys-Dietz syndrome
• Syphilis / arteritis
• Traumatic injury

Risk factors for rupture?• In total 80% will rupture (10 - 20% 5-year survival)
• Higher age and COPD increase rupture risk
• For aneurysm ∅ > 6 cm annual rupture risk 7%
• For aneurysm ∅ > 7 cm 43% will rupture
• Incidence CAD < 30% in contrast to AAA (> 70%)

Indications for repair
• All symptomatic aneurysms regardless of size should be repaired (pain/pressure)
• However in 95% no heralding symptoms
• Rupture
• Acute dissection with malperfusion/ other life-threatening complication
• Symptomatic aneurysm (pain or compression other organs)
• Enlargement ≥ 1 cm/year
• Absolute size > 6.5 cm or > 6.0 cm with connective tissue disorder

Repair strategies
• Open
• Endovascular
• Hybrid
• Cardiovascular risk factors
• Spirometry - most open repairs require single lung ventilation
• Pre-existing renal function (AKI most important risk factor for early postoperative mortality)
• CTA with 3-D reconstruction
Preoperative workup

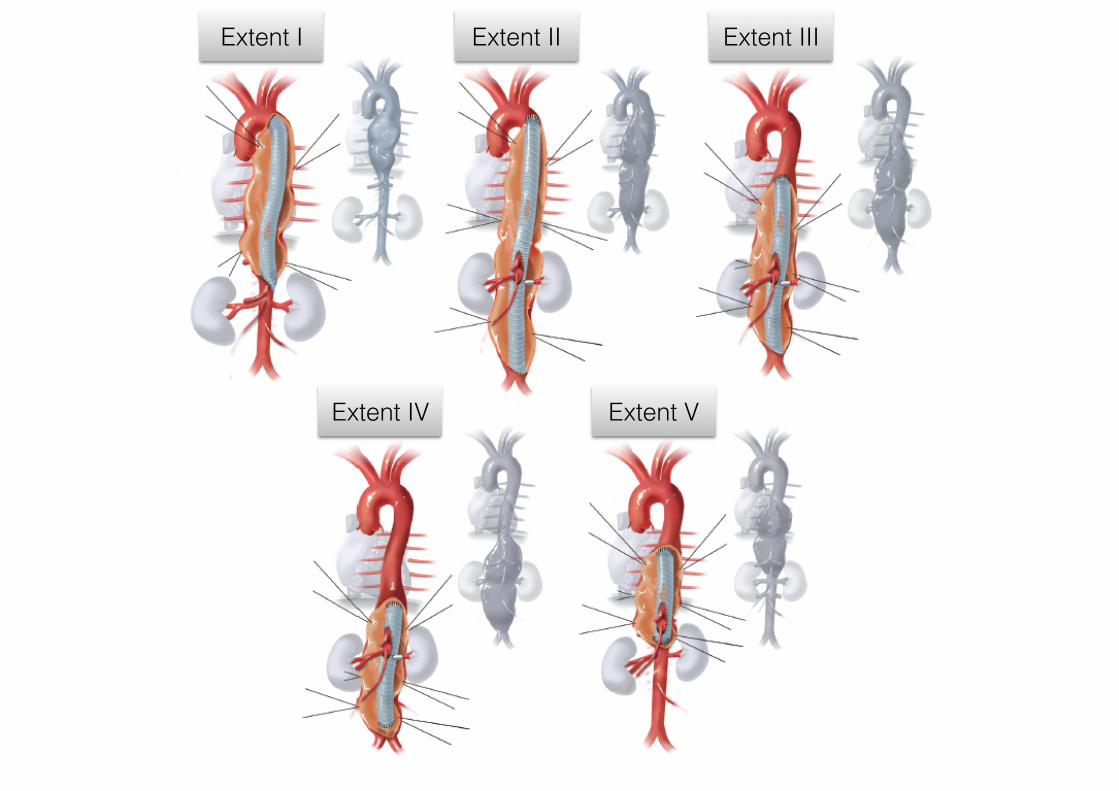
Modified Crawford classification
Extent I Extent II Extent III Extent IV Extent V

Patient (2)
• Rapidly progressive TAAA ∅ 7.9 cm
• No underlying other disease (degenerative)
• Extent II
• Open repair
Patient (3)
• Preoperative ICU admission (28/11)
• Arterial line (right radial artery)
• Pulmonary artery catheter (PAP 29/13, CI 3.8)
• ELD (10 cm H2O)
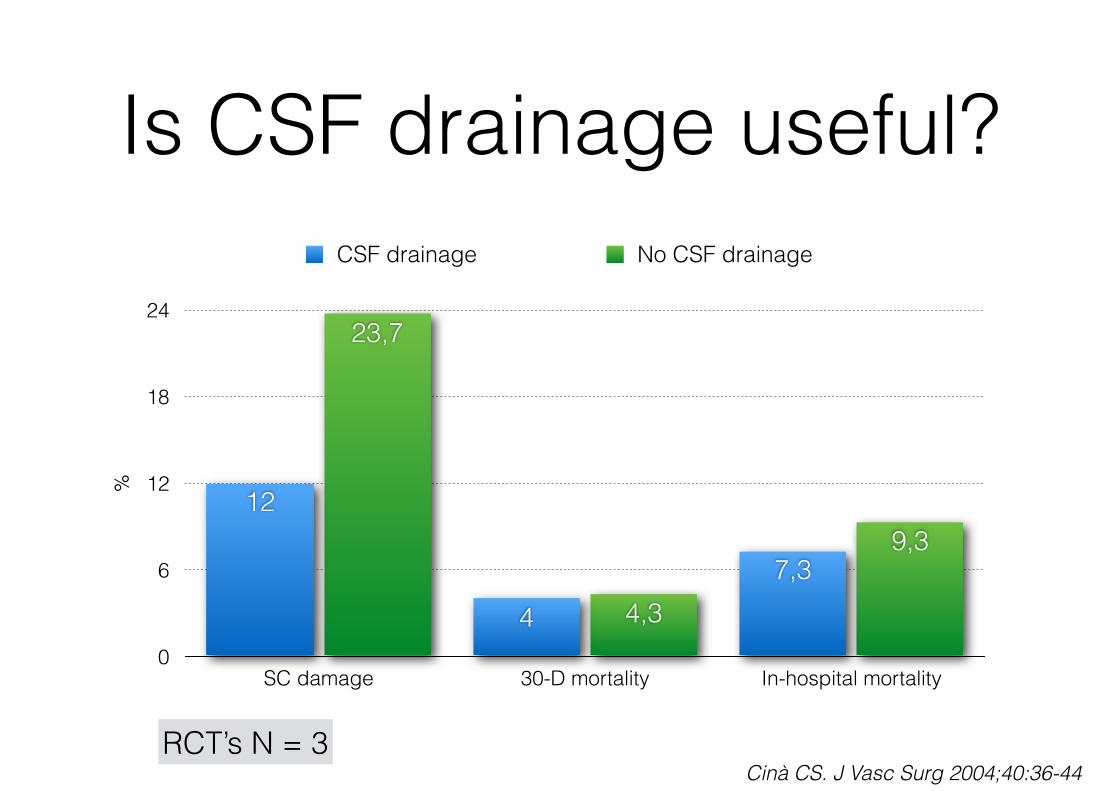
Is CSF drainage useful?%
0
6
12
18
24
SC damage 30-D mortality In-hospital mortality
9,3
4,3
23,7
7,34
12
CSF drainage No CSF drainage
RCT’s N = 3Cinà CS. J Vasc Surg 2004;40:36-44
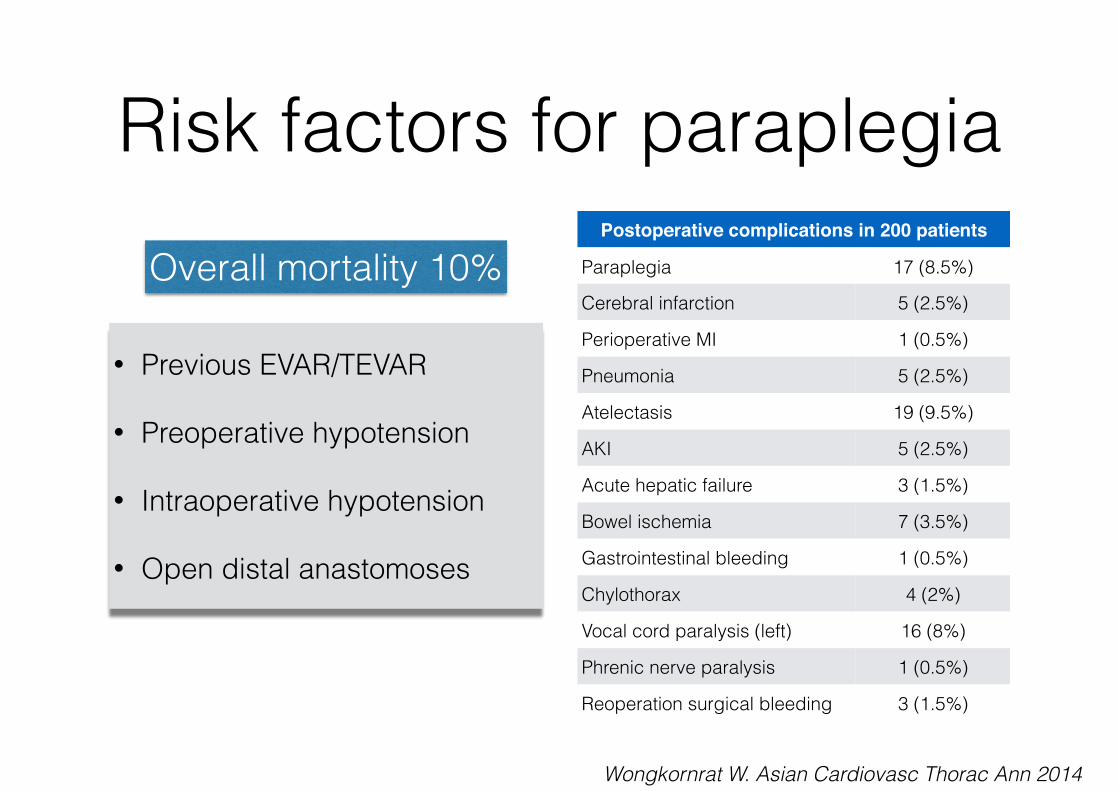
Risk factors for paraplegia
• Previous EVAR/TEVAR
• Preoperative hypotension
• Intraoperative hypotension
• Open distal anastomoses
Postoperative complications in 200 patients
Paraplegia 17 (8.5%)
Cerebral infarction 5 (2.5%)
Perioperative MI 1 (0.5%)
Pneumonia 5 (2.5%)
Atelectasis 19 (9.5%)
AKI 5 (2.5%)
Acute hepatic failure 3 (1.5%)
Bowel ischemia 7 (3.5%)
Gastrointestinal bleeding 1 (0.5%)
Chylothorax 4 (2%)
Vocal cord paralysis (left) 16 (8%)
Phrenic nerve paralysis 1 (0.5%)
Reoperation surgical bleeding 3 (1.5%)
Wongkornrat W. Asian Cardiovasc Thorac Ann 2014
Overall mortality 10%

Intraoperative monitoring• Insertion of double lumen endotracheal tube
• Central access with PA catheter for HD monitoring
• Arterial monitoring of upper and lower extremities with aortic clamping and left heart bypass
• Lumbar CSF drain in Extent I and II repair (IT pressure < 10 mmHg) - continue for 3 - 5 days
• Monitoring of SSEP/MEP with Extent II repair and hypothermic circulatory arrest
Circulatory support• LHB with decompression of the proximal circulation in
conjunction with distal perfusion through left atrial drainage via the left inferior pulmonary vein and arterial inflow distal to the aortic clamp site usually the iliac system
• Alternative is partial CP bypass by femoral vein canulation (advanced to RA) and same arterial inflow (includes membrane oxygenation)
• Circulatory arrest if proximal clamp is impossible with same canulation with total body retrograde perfusion

Additional measures to prevent ischemic injury
• Permissive or active systemic hypothermia (32 0C)
• Cold selective renal perfusion (4 0C)
• Reattachment of segmental arteries
• Sequential aortic clamping
• Selective visceral perfusion
Extent I Extent II Extent III
Extent IV Extent V

Operative procedure• 29/11 10.02 - 15.36 (24 mm Hemabridge from left SA until
aortic bifurcation with left-left bypass, CSF drainage, sequential aortic clamping, selective renal perfusion and IC artery reimplantation)
• left thoracophrenolaparotomy (retroperitoneal approach) - 4 tempi
• Period 1 - clamp distal LSA and T6 - E to E anastomosis native aorta and prosthesis
• Period 2 - clamp proximal prosthesis and T12 - reimplantation IC 10 (L/R)
• Period 3 - clamp distal reimplanted IC10 and infrarenal - reimplantation renal arteries and AMS/TC (single island)
• Period 4 - clamp infrarenal and above bifurcation - E to E anastomosis native aorta

Stage 1
Stage 2
Stage 3
Stage 4
Left-left bypass LUPV and LFA
Postoperative course• ICU return 29/11:16.00
• Stable hemodynamics (CI ≈ 3 l/min/m2, PAP 35/20, MAP > 85 - 90 mmHg)
• Paroxysmal AF (rate control - spontaneous SR)
• Sedation immediate stop - no SC damage
• Extubation 30/11: 08.00

Postoperative course
• Stable renal function (creatinine 47 - adequate diuresis)
• Restart oral intake 30/11
• Removal ELD 02/12
• Discharge home 12/12

OutcomeOpen TAAA repair (N)
30-D survival (%) AKI (%) Spinal cord
ischemia (%)
Crawford 1993 1509 92 9.0 15.5
Coselli 2007 2286 95 5.6 3.8
Safi 2005 355 93 2.1 1.3
Frederick JR. Ann Cardiothorac Surg 2012;1:277-285