the who/ unicef comprehensive strategy to reduceapps.searo.who.int/pds_docs/b4314.pdfworld health...
TRANSCRIPT



Measles and Rubella Surveillance and Outbreak Investigation Guidelines

© World Health Organization 2009
All rights reserved.
Requests for publications, or for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – can be obtained from Publishing and Sales, World Health Organization, Regional Office for South-East Asia, Indraprastha Estate, Mahatma Gandhi Marg, New Delhi 110 002, India (fax: +91 11 23370197; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the informa-tion contained in this publication. However, the published material is being distributed without war-ranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
This publication does not necessarily represent the decisions or policies of the World Health Orga-nization.
Printed in India
WHO Library Cataloguing-in-Publication data
World Health Organization, Regional Office for South-East Asia.
Measles & rubella surveillance &outbreak investigation guidelines.
1. Measles – epidemiology – immunology - mortality - prevention and control. 2. Rubella – epidemiology - immunology - prevention and control. 3. Rubella Syndrome, Congenital – epidemiology – diagnosis. 4. Rubella Virus - isolation and purification. 5. Measles Virus - isolation and purification. 6. Epidemiologic Surveillance. 7. Disease Outbreaks. 8. Guidelines
ISBN: 978-92-9022-350-4 (NLM classification: WC 500)

Measles and Rubella Surveillance and Outbreak Investigation Guidelines iii
Contents
Abbreviations .................................................................................v
1. Introduction ............................................................................ 1
2. Measles control in South-East Asia Region - Status, Goals and Strategies ................................................... 3
2.1 Integrated disease surveillance .......................................5
2.2 Integrating rubella/ congenital rubella syndrome control with measles mortality reduction ........................8
3. The epidemiologic and clinical basis of measles surveillance ............................................................................. 9
3.1 Epidemiology .....................................................................9
3.2 Clinical presentation ........................................................10
4. Measles: standard definitionsand case classification ............ 13
4.1 Case definition measles surveillance ..............................13
4.2 Case classification ..........................................................14
4.3 Interpretation of results in recently vaccinated patients ..........................................................................15
5. Measles surveillance in countries targeting measles mortality reduction and which have not yet conducted catch-up measles immunization campaigns .......................... 17
5.1 Establishing surveillance systems to report clinically suspected measles cases (aggregate reporting) ............18
5.2 Regular data analysis and identifying measles outbreaks .......................................................................19
6. Measles surveillance in countries targeting measles mortality reduction and which have conducted catch-up measles immunization campaigns .......................... 21
6.1 Strengthening surveillance systems to report clinically suspected measles cases .................................22
6.2 Linelisting clinically suspected measles cases ...............23
6.3 Laboratory confirmation of as many cases as possible ..........................................................................24
6.4 Regular data analysis and identifying measles outbreaks .......................................................................24

Measles and Rubella Surveillance and Outbreak Investigation Guidelinesiv
7. Outbreak investigation and response in countries targeting measles mortality reduction .................................. 25
7.1 Definition of measles outbreak in countries/provinces of large countries targeting measles mortality reduction ........................................................................25
7.2 Steps for conducting investigations of a suspected measles outbreak in endemic and low incidence areas targeting mortality reduction: ........................................27
7.3 Immunization response to measles outbreaks ...............36
7.4 Ensuring effective community involvement and public awareness ...........................................................42
8. Monitoring and evaluation in countries/provinces of large countries targeting measles mortality reduction ......... 43
8.1 Immunization coverage indicators for all countries .......44
8.2 Disease incidence and surveillance performance indicators .......................................................................44
9. Measles surveillance, outbreak detection and response in countries targeting elimination ......................................... 47
9.1 Indicators for monitoring progress towards elimination and targets for elimination ...........................................47
9.2 Definitions specific to measles elimination ....................50
9.3 Operationalizing measles surveillance in countries targeting elimination ......................................................50
10. Rubella and congenital rubella syndrome (CRS) surveillance 57
10.1 The epidemiologic and clinical basis of rubella surveillance ........................................................58
10.2 Recommended types of surveillance ..............................62
11. Role of laboratories in measles and rubella surveillance ...... 65
11.1 Collection, shipment and testing of specimens ..............66
11.2 Measles and rubella laboratory network ........................71
References .................................................................................. 75

Measles and Rubella Surveillance and Outbreak Investigation Guidelines v
Abbreviations
AFP Acute Flaccid Paralysis
CRS Congenital Rubella Syndrome
EPI Expanded Programme of Immunization
EWARS Early Warning and Reporting Systems
GAVI Global Alliance for Vaccines and Immunization
GIVS Global Immunization Vision and Strategy
IgM Immunoglobulin M
IgG Immunoglobulin G
IHR International Health Regulations
IMCI Integrated Management of Childhood Illness
ITAG Immunization Technical Advisory Group
IU International Unit
MCV Measles Containing Vaccine
PHEIC Public Health Emergency of International Concern
RI Routine Immunization
RNA Ribose Nucleic Acid
SIA Supplementary Immunization Activity
SEAR South-East Asia Region
SSPE Subacute Sclerosing Panencephalitis
TCG Technical Consultative Group
UNICEF United Nations Children’s Fund
VPD Vaccine Preventable Disease
WHO World Health Organization


Introduction
In May 2005, the fifty eighth World Health Assembly adopted the WHO/UNICEF Global Immunization Vision and Strategy (GIVS). GIVS called upon countries to reduce global measles deaths by 90% by 2010 as compared to 2000 estimates(1). In 2007, the South-East Asia Regional Strategic Plan for Measles Mortality Reduction, 2007-2010 was endorsed by the Regional Technical Consultative Group (TCG) for Vaccine Preventable Diseases at their twelfth meeting in New Delhi(2).
A cornerstone of sustainable measles mortality reduction is good quality surveillance. Until now Member countries have either strengthened measles surveillance within the integrated disease surveillance system or improved measles surveillance by building on the high quality Acute Flaccid Paralysis (AFP) surveillance infrastructure established for polio eradication. The focus of measles surveillance in many Member countries has been on aggregate data reporting and outbreak investigations which
Chapter 1

Measles and Rubella Surveillance and Outbreak Investigation Guidelines2
has provided valuable information for planning and evaluating measles immunization strategies.
Many Member countries are now observing a marked decrease in the number of measles outbreaks. Improved measles surveillance and successful immunization campaigns have helped to unearth the previously unrecognized rubella burden in several countries. However, a significant number of suspected measles cases continue to be reported throughout the Region(3). Efforts towards upgrading measles surveillance to case-based surveillance in all countries will be necessary to fully understand the regional measles and rubella epidemiology and to target immunization strategies.
The purpose of this document is to provide a framework for Member countries to:
Regularly collect information on measles cases reported in health •
facilities;
Use that information to investigate outbreaks;•
Ensure appropriate public health response to measles outbreaks; and•
Provide the basic principles for rubella and congenital rubella •
syndrome (CRS) surveillance.
The focus and intensity of measles surveillance will depend on national goals and the success of measles supplementary immunization activities. Accordingly, measles surveillance can be classified into three broad groups:
Countries/provinces of large countries targeting measles mortality •
reduction and which have not conducted catch-up measles immunization campaigns (Chapter 5) and where the disease is endemic;
Countries/provinces of large countries targeting measles •
mortality reduction and which have conducted catch-up measles immunization campaigns (Chapter 6) and where the disease incidence is low; and
Countries targeting measles elimination (Chapter 9).•
Chapter 7 outlines the steps for suspected measles outbreak investigation and response.
The guidelines are intended for national and sub-national level programme managers. They could adapt these guidelines according to local needs.

Measles control in South-East Asia Region - Status, Goals and
Strategies
Despite the availability of a safe, effective, and relatively inexpensive measles vaccine for over 40 years, measles remained a leading cause of childhood mortality especially for children living in developing countries(4).According to global estimates of mortality, 136,000 measles deaths (almost 69% of estimated global deaths) occurred in countries of the WHO South East Asia Region (SEAR) in 2007. Even though routine immunization coverage in the Region increased from 61% in 2000 to 73% in 2007, the Region as a whole achieved a modest 42% reduction in the estimated measles deaths during that period(5).
Four countries in the Region, Bhutan, DPR Korea, Maldives and Sri Lanka are implementing measles elimination strategies. Bangladesh, Indonesia, Myanmar, Nepal and Timor-Leste are implementing plans for sustainable mortality reduction(6). India
Chapter 2

Measles and Rubella Surveillance and Outbreak Investigation Guidelines4
outlined a national strategic plan for measles morality reduction in 2005 by strengthening measles surveillance building upon the strengths of the acute flaccid paralysis surveillance system and is planning to provide a second measles immunization opportunity(7).
Recently, countries of the Region, have seen a substantial improvement in the detection, investigation and case management of measles outbreaks
(8)owing to the expansion of Acute Flaccid Paralysis (AFP) surveillance and improvement in surveillance of other vaccine preventable diseases. Information from outbreak investigations have helped to identify susceptible groups and targeted supplemental immunization campaigns. Improved measles surveillance has also helped to uncover the previously unrecognized rubella disease burden in Bangladesh, Bhutan, Maldives and Nepal(9, 10).
The overall goal of the South-East Asia regional strategic plan for 2007-2010 is to reduce the number of measles deaths by 90% in 2010 relative to 2000 estimates.
The specific objectives of the regional plan are to:
Achieve at least 90% Measles Containing Vaccine (MCV1) •
coverage at the national level, and at least 80% MCV1 coverage in all districts by 2010;
Conduct case-based measles surveillance within an integrated •
vaccine preventable disease surveillance system in countries that have conducted measles catch-up campaigns;
Achieve full investigation and appropriate clinical case •
management of all measles outbreaks by all Member countries by 2009; and
Provide a second opportunity for measles immunization to •
eligible children in all Member countries by 2010 with at least 90% coverage.
Over the next few years, efforts towards sustaining measles mortality reduction will include strategies on improving routine immunization services, attaining high quality integrated surveillance with laboratory support and closing the immunity gap through supplementary immunization activities. Additionally, measles mortality reduction strategies in the Region should integrate rubella/ congenital rubella syndrome (CRS) control whenever possible.
Although the regional goal is sustainable measles mortality reduction, countries that have already reached a low incidence of measles are encouraged to accelerate and intensify the implementation of immunization and surveillance strategies with a view towards measles elimination.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 5
2.1 Integrated disease surveillance
The routine reporting of communicable diseases (e.g. the disease notification system) is the backbone of measles surveillance. It is essential to maintain high quality measles and rubella surveillance within an integrated vaccine preventable disease (VPD) surveillance system. Where possible, countries should continue to build on the well established polio eradication networks. Surveillance data needs to be used to develop and refine both routine and supplemental measles immunization activities. The key components for each stage of measles surveillance based on country goals are summarized in Table 1 below.
Table 1: Summary framework for measles surveillance
Source of Data
Key Components
Country Goals
Mortality Reduction Elimination
Not completed catch-up
campaigns
Completed catch-up
campaigns
Few cases detected
Patients coming
to health facilities
Reporting Type Aggregate data Case-based data
Case-based data
Serology N/a As many cases as possible All cases
Virus Isolation N/a In some cases All cases
Data transmission Summary table Line list
Case investigation
report
Desired Information
Number of cases by
location and age
Age, sex, location,
vaccination status,
outcome & serology
Age, sex, location,
vaccination status,
outcome, serology&
investigation of all epi-links
Outbreak Investigation
Reporting Type Case-based data
Case-based data
Case-based data
Suspected outbreaks
Increase in the expected number of
cases
5 per 100 000 population in one month
≥ 1 case
Serology At least 5 cases
At least 5 cases ≥ 1 case
Virus IsolationOptional as per
programme needs
In some outbreaks All outbreaks
Data transmission Line list Line list Line list
Measles and Rubella Surveillance and Outbreak Investigation Guidelines6
2.1.1 Countries/provinces of large countries targeting measles mortality reduction and which have not yet conducted catch-up measles immunization campaigns.
Measles surveillance in these countries should provide information that is most useful for documenting disease burden and guiding programme activities. Accordingly, these areas need to have an integrated VPD surveillance system that should be able to detect suspected measles outbreaks. The focus of measles surveillance in these areas would be to:
Establish and operationalize surveillance systems to understand •
measles epidemiology;
Assess the impact of Routine Immunization (RI); and•
Acquire data for planning supplementary immunization activities.•
Activities include:
Continuing routine monthly/weekly reporting of aggregated •
data of clinical measles cases by age group and immunization status;
Tracking potential measles outbreaks based on the above •
data;
Investigating and documenting outbreaks of measles and •
instituting weekly reporting when outbreaks take place and identifying reasons for the outbreaks;
Investigating any reports or rumours of measles cases occurring •
in the community.
During all suspected measles outbreaks, confirming five to ten •
initial cases and identifying measles virus from a few cases for genotyping.
Further details on surveillance can be found in Chapter 5 of these guidelines.
2.1.2 Countries/provinces of large countries targeting measles mortality reduction and which have conducted catch-up measles immunization campaigns.
Once a successful measles catch-up campaign has been conducted, measles incidence should immediately decline. However, outbreaks can still occur because of accumulation of susceptible children due to missing routine immunization and the uneven efficacy of measles vaccine for younger children. The focus of measles surveillance should be to:

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 7
Identify high-risk populations;•
Determine when the next outbreak may occur due to build-up •
of susceptible persons;
Determine where measles virus is circulating or may circulate •
(i.e. high-risk areas); and
Assess the surveillance system using performance indicators.•
Activities include:
Initiating case investigation for every suspected measles case.•
Collecting as many serum specimens as possible from suspected •
measles cases reporting to health facilities.
Sending linelist of cases to the next level.•
Identifying and tracking potential measles outbreaks.•
During outbreaks, collecting blood specimens from five to ten •
suspected cases for confirming the outbreak and collecting urine or nasopharyngeal swabs for virus isolation and genotyping.
Further details on surveillance can be found in Chapter 6 of these guidelines.
2.1.3 Countries targeting measles elimination
Countries achieving and maintaining immunization coverage goals with MCV1 and a second opportunity of measles vaccination in all districts and nationally should raise their surveillance standards to monitor progress towards measles elimination. This includes case-based surveillance and also meeting desired surveillance performance standards for reporting rate, laboratory confirmation, viral detection and adequacy of investigation.
Activities include:
Implementing case-based surveillance with laboratory confirmation •
for every suspected measles case including completing a case investigation form and transmission of information to the next administrative level.
Investigating and confirming all outbreaks by collecting blood •
specimens from the first five to ten reported cases.
Collecting urine/nasopharyngeal specimens from five to ten cases •
from suspected measles outbreaks for virus isolation and genetic characterization.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines8
Further details on surveillance can be found in Chapter 9 of these guidelines.
2.2 Integrating rubella/ congenital rubella syndrome (CRS) control with measles mortality reduction
Evidence of disease burden due to rubella is emerging from countries that have not yet provided rubella immunization. Countries can determine rubella disease burden and initiate immunization strategies. There are several options:
Including rubella and CRS as notifiable diseases and integrating •
them with the surveillance of other vaccine preventable diseases;
Identifying rubella outbreaks through serological confirmation •
of all suspected measles outbreaks. Investigating and following outbreaks to find out possible increase in the incidence of CRS in the areas;
Establishing sentinel surveillance for CRS at neonatology units, •
Ear, Nose and Throat (ENT) units, ophthalmology units and cardiology units;
Conducting sero-surveys for women of childbearing age to find •
out rubella susceptibility; and
Reviewing records of disability registers in paediatric, neonatology, •
ENT, cardiology, ophthalmology and obstetrics to identify suspected CRS cases.
The countries that have already started immunization against rubella should integrate rubella surveillance with measles surveillance. This will help to ensure that all potential rubella cases and outbreaks are investigated and quantify the impact of rubella immunization.

The epidemiologic and clinical basis of measles surveillance
3.1 Epidemiology
The measles virus is one of the most infectious agents causing human disease. The virus is an exclusive human pathogen and has no animal reservoir or vector. Transmission is by respiratory droplets or direct contact. When the measles virus is introduced into a non-immune population, nearly 100% of individuals will become infected and develop a clinical illness. In areas with tropical climate, most cases of measles occur during the dry season and in areas with temperate climate the peak is during the late winter and early spring(11).
The measles virus is an enveloped, RNA virus of the genus Morbillivirus belonging to the Paramyxoviridae family with only one known serotype. It is inactivated rapidly in sunlight, heat or extremes of pH, but remains viable over long periods when stored between –20°C and –70°C.
Chapter 3

Measles and Rubella Surveillance and Outbreak Investigation Guidelines10
3.2 Clinical presentation
The average interval from exposure to onset of rash is 14 days (range 7–18 days). Patients are contagious two to three days before the rash until one to two days after the onset of the rash. Following inhalation of virus-containing droplets, measles virus infects the nasopharyngeal epithelium and soon extends to cells of the reticuloendothelial tissues. Five to seven days after exposure, the infection is spread through the bloodstream to the skin, conjunctivae and respiratory tract. Viraemia peaks towards the end of the incubation period when patients develop the prodromal symptoms of high fever, cough, coryza and conjunctivitis. The typical maculopapular rash appears three to four days after the prodrome with a high fever peaking at 39°C to 40°C. The rash spreads from the face and neck to the trunk and extremities fading after about three days. The onset of the rash is often accompanied by bluish-white lesions on the oral mucosa called Koplik’s spots, which are pathognomonic for measles. Patients normally improve by the third day of rash and fully recover 7–10 days from the onset of the disease.
Figure 1: Clinical course of measles
Measles can be more accurately diagnosed clinically in areas where the disease is endemic and a patient presents with a history of febrile respiratory illness for two to four days followed by a maculopapular rash and Koplik’s spots. However, in areas of low measles prevalence, laboratory confirmation is critical to differentiate “true” measles cases from other rash illnesses such as rubella, roseola infantum, scarlet fever etc. The measles-specific IgM antibody assay is a highly sensitive and specific test used for laboratory confirmation of clinically diagnosed cases. The assay becomes positive shortly after the onset of the rash and remains positive for up to four weeks following measles infection (Figure 2).

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 11
Figure 2: Measles virus infection and outcome(12)
Natural measles infection tends to induce higher antibody levels than does measles vaccination. Depending upon the titer of passively acquired maternal antibodies, young infants are usually protected against measles for several months. Maternal antibody protection decays by six to nine months of age, leaving infants increasingly susceptible to measles.
Most persons recover from measles without sequelae. Some complications are associated with measles due to transient suppression of cellular immunity, which is a characteristic feature of the disease. Frequent complications in children less than five years of age include otitis media (5% -15%) and pneumonia (5% -10%). In developing countries, persistent diarrhoea with protein-losing enteropathy may ensue, particularly in young infants.
Rare complications such as measles encephalitis occurs in approximately one per 1000 measles cases and subacute sclerosing panencephalitis (SSPE), a slowly progressive infection of the central nervous system may occur approximately in one per 100,000 measles cases several years after infection.
In developed countries, measles deaths are rare with case-fatality rates between 0.01% and 0.1%. In developing countries, case fatality rates are much higher and range between 5% and 15%. Malnutrition, vitamin-A deficiency and immunodeficient conditions (such as advanced HIV infection) can increase the risk of severe complications or death.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines12

Measles: standard definitions and case classification
4.1 Case definitions for measles surveillance(13)
Clinical case definition of suspected measles
Any person in whom a clinician suspects measles
or
Any person with:
fever, and•
generalized maculopapular (i.e. non-•
vesicular) rash, and
cough, coryza ( i .e. runny nose) or •
conjunctivitis (i.e. red eyes).
Laboratory criteria for diagnosis
Presence o f meas les -spec i f i c IgM •
antibodies
Chapter 4

Measles and Rubella Surveillance and Outbreak Investigation Guidelines14
Figure 3: Summary of classification of case
4.2 Case classification
Clinically confirmed measles: • Any person meeting the clinical case definition in whom a laboratory investigation is not conducted and does not have epidemiologic linkage to a laboratory confirmed case1
.
Laboratory confirmed measles: • A case that meets the clinical case definition and has laboratory confirmation of measles virus infection.
Epidemiologically confirmed measles:• A case that meets the clinical case definition and is linked epidemiologically2 to a laboratory confirmed or another epidemiologically confirmed case.
Discarded: • A suspected case that has been subjected to serology or virus identification but has not met any of the laboratory criteria for diagnosis, or a suspected case which has been linked
1 A suspected case in which laboratory investigations have equivocal results for measles specific IgM antibodies after being tested twice, should be classified as a clinically confirmed measles case.
2 Epidemiological linkage: A case that meets the clinical case definition and has contact with a lab-oratory-confirmed measles case whose rash onset was within the preceding 7-21 days or a case that lives in the same district or adjacent district where a measles outbreak has been laboratory confirmed and transmission is plausible.
IgM positive forrubella
Equivocal
IgM negative formeasles and rubella
Repeat blood test withfresh sample andclassify as above
Lab confirmedmeasles
Stillequivocal
Clinicallyconfirmed measles
Lab confirmedrubella
Discard
Clinically confirmedmeasles
Epidemiologicallyconfirmed measles
Epidemiologic link to labconfirmed measles case
Epidemiologic link to labconfirmed Rubella case
No epidemiologic link to labconfirmed measles/rubella
case
IgM positive formeasles
Epidemiologic link to otherdisease
Discard
Clinically suspectmeasles case
Adequate bloodSpecimen*
No adequateblood specimen
AND
*A single serum sample obtained at the first contact with the health care system within 28 daysafter onset is considered adequate for measles surveillance
Epidemiologicallyconfirmed rubella

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 15
epidemiologically to a confirmed case of another communicable disease.
A measles-related death is a death in an individual with confirmed (clinically, laboratory confirmed or epidemiologically) measles in which death occurs within 30 days of rash onset and is not due to other unrelated cause e.g., a trauma or chronic disease.
4.3 Interpretation of results in recently vaccinated
Natural measles infection and measles vaccine can stimulate an IgM response. If the suspected case has been vaccinated within six weeks before the onset of rash the interpretation of the results may be problematic because of the following:
Measles vaccine can cause fever in 5% and rash in approximately •
20% of vaccinees.
First-time vaccinees are expected to have detectable measles •
IgM after vaccination.
A mild rash lasting one to three days may occur approximately •
a week after vaccination.
Serological techniques cannot distinguish between immunity from •
a natural infection or an immunization.
Other medical conditions (rubella or dengue) can cause rash and •
fever in a person who has recently received measles vaccine.
The classification of cases with a positive measles IgM result and a recent history of measles vaccination is given in Table 2 below.
Table 2: Classification of cases with IgM-positive result and recent history of measles vaccination
Vaccination History Epidemiological Findings Final
Classification
History of measles vaccination within six weeks before onset of rash
Active search in community does not reveal evidence of measles transmission
No history of traveling to areas where measles virus is known to be circulating
Discarded
Active search in community reveals other laboratory-confirmed measles cases
Confirmed

Measles and Rubella Surveillance and Outbreak Investigation Guidelines16

Measles surveillance in countries targeting measles mortality
reduction and which have not yet conducted catch-up measles
immunization campaigns
In countries/ provinces of large countries where the disease is endemic and supplementary immunization activities (SIA) have not been conducted, the focus should be on gathering aggregate data, outbreak identification and investigation, and collecting specimens to identify the type and nature of the outbreak.
The key objectives for developing and/or strengthening surveillance at this stage are:
Monitor incidence and coverage in order to •
assess progress (i.e., decreasing incidence rate and increasing coverage);
Identify areas at high risk or with poor •
programme performance; and
Describe changes in epidemiology of measles •
in terms of age, immunization status and intervals between epidemics.
Chapter 5

Measles and Rubella Surveillance and Outbreak Investigation Guidelines18
Measles surveillance in areas where the disease is endemic can be operationalized by:
Establishing surveillance systems to report clinically suspected •
measles cases;
Analyzing data; and •
Identifying measles outbreaks.•
Figure 4: Aggregate measles surveillance
5.1 Establishing surveillance systems to report clinically suspected measles cases (aggregate reporting)
The surveillance system should be initially established at sites where clinically suspected measles cases are likely to seek treatment such as hospitals (inpatient and outpatient departments), health centres and clinics. Private medical practitioners and private hospitals are an important part of the medical infrastructure and should be included in the surveillance system.
Every reporting site should have one person and an alternate designated to monitor and report clinically suspected measles cases. Reporting sites should submit reports to the district surveillance focal person. As outlined in Figure 5, the district should report to the next level (regional/ national) and feedback on information acquired should be given to the lower levels. Wherever possible data should be collected through an existing surveillance system such as AFP or Early Warning and Reporting System (EWARS). Cases should be reported weekly or monthly with zero reporting when there are no cases. If the AFP surveillance system is used, the existing routine reporting forms should be modified to include measles data.
Identify suspected outbreaks
(an increase in the expected number of suspected measlescases being reported in a specific geographical area)
Establish surveillance to report clinicallysuspect measles cases (Aggregate)
Regular data analysis

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 19
Figure 5: Measles surveillance in endemic countries
5.2 Regular data analysis and identifying measles outbreaks
Data should be collected from all sources and reporting sites on a weekly or monthly basis and collated, merged and evaluated at the district level. A measles outbreak should be suspected if there is an increase in the expected number of suspected measles cases being reported in a specific geographical area.
Evaluating trends in recent years will help to identify whether a measles outbreak is imminent or whether there is continuation of an outbreak. If surveillance data from previous years is not available, local health-care workers could provide information about an increase in measles cases in a given area over a specific period of time.
When the data suggests measles outbreak, the affected areas should be visited and a rapid assessment performed to determine whether the reported cases are compatible with clinical case definition of measles.If the cases are compatible, the district health authorities and the outbreak coordination committee, based on the criteria laid by the national, state or provincial authorities should decide whether it is necessary to conduct a comprehensive measles outbreak investigation and response in the area. The details are outlined in Chapter 7, Outbreak investigation and response in countries targeting measles mortality reduction.
Health care facility(Routine reporting)
District Health Office(Outbreak investigation, collectspecimens, analysis, response)
Regional / National level(Guideline, supplies, lab investigation,
analysis, response)
Reporting
Feedback
Reporting Feedback
Feedback

Measles and Rubella Surveillance and Outbreak Investigation Guidelines20

Measles surveillance in countries targeting measles mortality reduction and which have
conducted catch-up measles immunization campaigns
In countries/provinces of large countries where the measles incidence is relatively lower and SIAs have been completed, the surveillance network should move towards case-based surveillance by improving reporting, collecting essential information on cases (linelist) and laboratory confirmation of as many cases as possible.
The goal of measles surveillance in these areas is to better define where the measles virus is circulating and identify accumulation of susceptibles in order to focus specific interventions.
Chapter 6
Measles and Rubella Surveillance and Outbreak Investigation Guidelines22
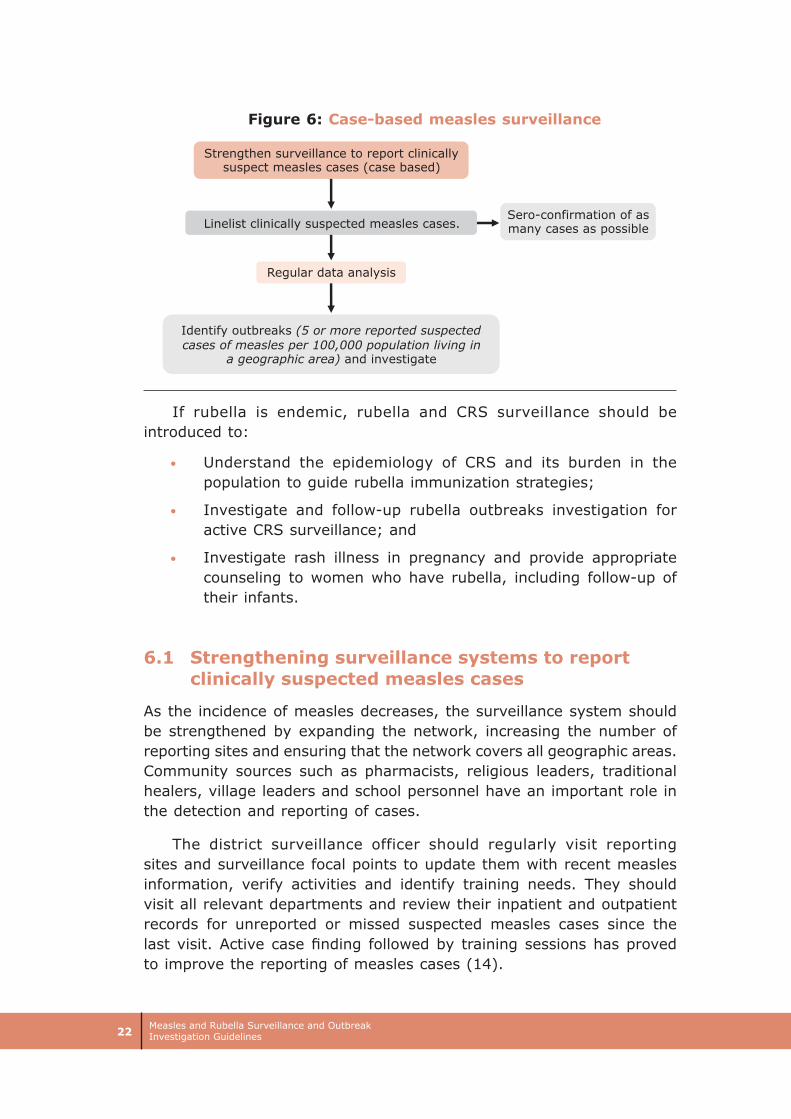
Figure 6: Case-based measles surveillance
If rubella is endemic, rubella and CRS surveillance should be introduced to:
Understand the epidemiology of CRS and its burden in the •
population to guide rubella immunization strategies;
Investigate and follow-up rubella outbreaks investigation for •
active CRS surveillance; and
Investigate rash illness in pregnancy and provide appropriate •
counseling to women who have rubella, including follow-up of their infants.
6.1 Strengthening surveillance systems to report clinically suspected measles cases
As the incidence of measles decreases, the surveillance system should be strengthened by expanding the network, increasing the number of reporting sites and ensuring that the network covers all geographic areas. Community sources such as pharmacists, religious leaders, traditional healers, village leaders and school personnel have an important role in the detection and reporting of cases.
The district surveillance officer should regularly visit reporting sites and surveillance focal points to update them with recent measles information, verify activities and identify training needs. They should visit all relevant departments and review their inpatient and outpatient records for unreported or missed suspected measles cases since the last visit. Active case finding followed by training sessions has proved to improve the reporting of measles cases (14).
Identify outbreaks (5 or more reported suspectedcases of measles per 100,000 population living in
a geographic area) and investigate
Linelist clinically suspected measles cases.
Strengthen surveillance to report clinicallysuspect measles cases (case based)
Sero-confirmation of asmany cases as possible
Regular data analysis

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 23
Figure 7: Measles surveillance in low incidence countries
Countries should adopt reporting systems suited to their existing surveillance system. Routine reports should be submitted to the district surveillance officer. As outlined in Figure 7, the district should report to the next level (regional/ national) and feedback provided to lower levels. Weekly reporting should gradually replace monthly reporting and include “zero measles case” reports.
6.2 Linelisting clinically suspected measles cases
As a requirement for case-based surveillance, reporting sites should send line lists to the district surveillance focal person of clinically suspected measles cases on Form A. The district should prepare a consolidated linelist from all sources and transmit it to the state/ province or national surveillance office. The linelist should include the following information:
Unique identifier; •
Date of onset of rash;•
Place of occurrence; •
Age; •
Vaccination status;•
Date of last vaccination;•
Laboratory confirmation; and•
Case classification. •
Every measles case that is investigated in this phase should be allotted a unique identification number (case id or epid number) and linelisted. The epid number should be able to capture information on the state/ province, district, year of onset of the rash and the serial number
Health care facility(Routine reporting)
District Health Office(Outbreak investigation, collectspecimens, analysis, response)
Regional / National level(Guidelines, supplies, lab investigation,
analysis, response)
Reporting
Feedback
Reporting Feedback
Feedback

Measles and Rubella Surveillance and Outbreak Investigation Guidelines24
of the case in that year. Countries may adopt case epid number codes suitable to their needs. One suggestion is given below:
MSL - COU - PR - DIS - YR - NUM
MSL denotes measles • case code
COU indicates country code, •
PR indicates the province (state) code, •
DIS indicates the district code, •
YR represents the year of rash onset (eg 09 for 2009) and •
NUM denotes the serial number of the case detected in the •
district in that year.
Therefore, MSL-COU- PR-DIS-09-001 will be the code of the first measles case (001) investigated in a country (COU) at a particular province/ state (PR) in a district (DIS) in 2009.
6.3 Laboratory confirmation of as many cases as possible
Efforts must be made in health facilities, to collect serum samples from as many suspected measles cases as soon as possible and sent to the laboratory for confirmation. During outbreaks, to avoid overwhelming the laboratory capacity, only 5 to 10 samples need to be laboratory confirmed. Details are given in Chapter 11 Role of laboratories in measles and rubella surveillance.
6.4 Regular data analysis and identifying measles outbreaks
When clinically suspected measles cases are reported, it is important to probe from the patient or relatives about the occurrence of similar cases in the neighbourhood. Routine measles data collected through passive surveillance as well as through the AFP/measles surveillance network should be collated and analyzed at the district and sub-district to identify clustering. The analysis should also include age distribution, vaccination status, geographic location and laboratory results.
A measles outbreak should be suspected if there are 5 or more reported suspected measles cases in one month per 100,000 population in a geographic area. Case mapping is important to identify clustering and the detection of suspected outbreaks. A site visit by the district health authorities and outbreak coordination committee will help decide if a full-scale outbreak investigation and response are warranted. Details are outlined in Chapter 7 Outbreak investigation and response in countries targeting measles mortality reduction.
Outbreak investigation and response in countries targeting measles mortality reduction(15)
7.1 Definition of measles outbreak in countries/provinces of large countries targeting measles mortality reduction
7.1.1 In countries/provinces of large countries targeting measles mortality reduction and which have not yet conducted catch-up measles immunization campaigns
A suspected measles outbreak is defined as "an increase in the expected number of suspected measles cases reported in a specific geographical area".
A substantial increase in incidence of suspected measles cases compared to non-epidemic years or incidence similar to incidence in an epidemic year
Chapter 7
Measles and Rubella Surveillance and Outbreak Investigation Guidelines26
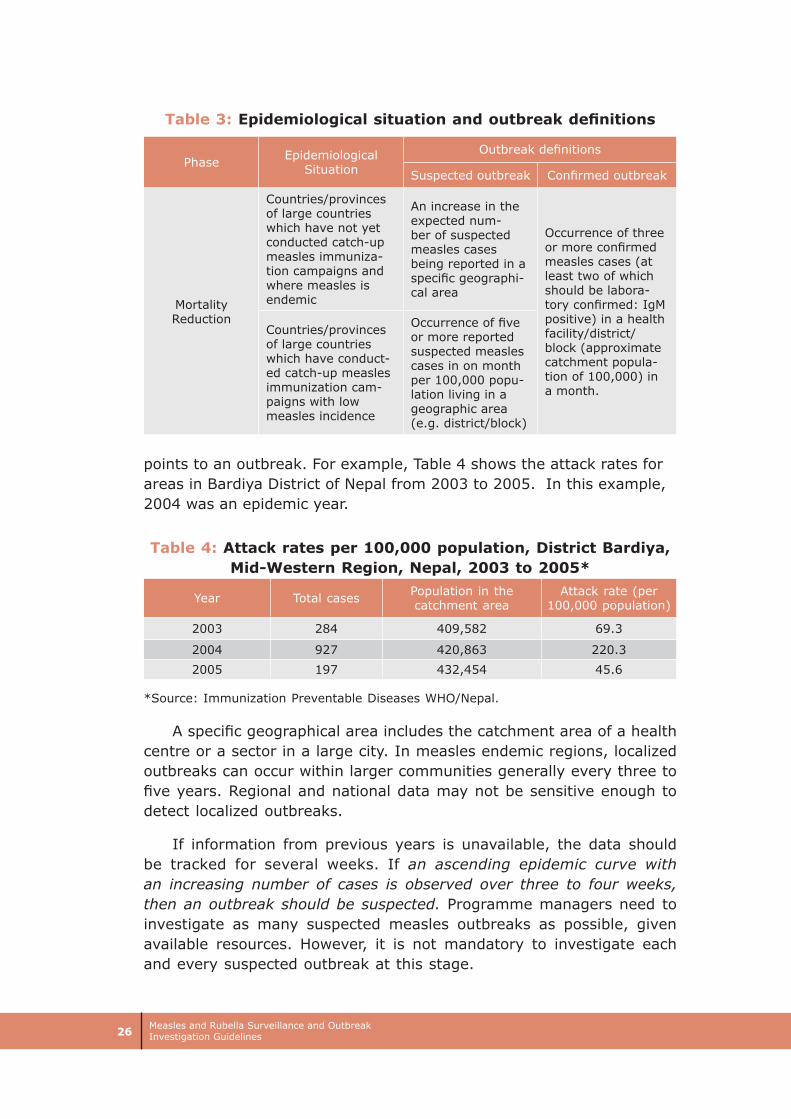
Table 3: Epidemiological situation and outbreak definitions
Phase Epidemiological Situation
Outbreak definitions
Suspected outbreak Confirmed outbreak
Mortality Reduction
Countries/provinces of large countries which have not yet conducted catch-up measles immuniza-tion campaigns and where measles is endemic
An increase in the expected num-ber of suspected measles cases being reported in a specific geographi-cal area
Occurrence of three or more confirmed measles cases (at least two of which should be labora-tory confirmed: IgM positive) in a health facility/district/block (approximate catchment popula-tion of 100,000) in a month.
Countries/provinces of large countries which have conduct-ed catch-up measles immunization cam-paigns with low measles incidence
Occurrence of five or more reported suspected measles cases in on month per 100,000 popu-lation living in a geographic area (e.g. district/block)
points to an outbreak. For example, Table 4 shows the attack rates for areas in Bardiya District of Nepal from 2003 to 2005. In this example, 2004 was an epidemic year.
Table 4: Attack rates per 100,000 population, District Bardiya, Mid-Western Region, Nepal, 2003 to 2005*
Year Total cases Population in the catchment area
Attack rate (per 100,000 population)
2003 284 409,582 69.3
2004 927 420,863 220.3
2005 197 432,454 45.6
*Source: Immunization Preventable Diseases WHO/Nepal.
A specific geographical area includes the catchment area of a health centre or a sector in a large city. In measles endemic regions, localized outbreaks can occur within larger communities generally every three to five years. Regional and national data may not be sensitive enough to detect localized outbreaks.
If information from previous years is unavailable, the data should be tracked for several weeks. If an ascending epidemic curve with an increasing number of cases is observed over three to four weeks, then an outbreak should be suspected. Programme managers need to investigate as many suspected measles outbreaks as possible, given available resources. However, it is not mandatory to investigate each and every suspected outbreak at this stage.
Measles and Rubella Surveillance and Outbreak Investigation Guidelines 27
A confirmed measles outbreak is defined as the occurrence of three or more confirmed measles cases (at least two of which should be laboratory confirmed; IgM positive) in a health facility/block/district (approximate catchment population of 100,000) in a month.
If laboratory confirmation is not possible, an outbreak may be documented through a sustained and progressive rise in clinically confirmed cases over a three-week period. In addition, hospitalization of a proportion of the suspected cases due to measles-related complications such as diarrhoea and respiratory infections (pneumonia, croup) can be used to distinguish measles from outbreaks of other infections, which usually have lower hospitalization and complication rates.
No specific threshold should be set for triggering an outbreak response. If an outbreak or potential outbreak is suspected, then response activities should start immediately.
7.1.2 In countries/provinces of large countries targeting mortality reduction and which have conducted catch-up measles immunization campaigns.
A suspected outbreak of measles is defined as the occurrence of five or more reported suspected cases of measles in one month per 100,000 population living in a geographic area (e.g., block/district). All measles outbreaks should be fully investigated.
A confirmed measles outbreak is defined as the occurrence of three or more confirmed measles cases (at least two of which should be laboratory confirmed: IgM positive) in a health facility/block/district (approximate catchment population of 100,000) in a month.
7.2 Steps for conducting investigations of a suspected measles outbreak in endemic and low incidence areas targeting mortality reduction:
7.2.1 Decision on outbreak investigation by outbreak coordination committee:
When surveillance systems are being initially established in the districts, a measles outbreak coordination committee should be formed. If a rapid response team or epidemic response team exists, it should coordinate the measles outbreak investigation. The committee should include representatives from appropriate stakeholders.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines28
The committee should meet periodically before anticipated outbreaks to coordinate, plan and review epidemic preparedness and response activities .The committee should:
Assess the supplies, equipment and resources available;•
Estimate and identify additional resources needed for a rapid •
outbreak response; and
Ensure the availability of staff and their training for outbreak •
investigation and response.
When a suspected outbreak is identified the outbreak coordination committee should:
Assign responsibilities to staff with clear tasks and lines of •
communication;
Communicate with the general public and the media;•
Analyze epidemiological information as the outbreak progresses ;•
Meet regularly to review data and monitor implemented •
measures;
Evaluate the response; and•
Produce a detailed report on the outbreak response activities •
and make specific recommendations on any changes to the vaccination strategies and programme
Figure 8: Key steps in measles outbreak investigations
Additionalcase Search
ImmunizationResponse
Vit A & CaseManagement
NotifyAuthorities
Dataanalysis
Decision on outbreak investigation byOutbreak Coordination Committee
Outbreakinvestigation
Serum Samplesfrom 5-10 cases
Dataanalysis
Confirming typeof outbreak

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 29
7.2.2 Investigating outbreaks and additional case search
If a measles epidemic affects a large geographical area, it is recommended that outbreaks be investigated only in a few locations, e.g. a rural area and an urban area, rather than every outbreak in every town. An increase in the number of cases may reflect an increase in reporting of other diseases, e.g. rubella.
Every measles outbreak that is investigated should be allotted a unique outbreak ID. The outbreak ID should be able to capture information on the province/state, district, year of onset of the first case in the outbreak and the number of outbreak in that year. Countries may adopt outbreak IDs suitable to their needs. One suggestion is given below:
MOB-COU-PR-DIS-YR-NUM
MOB indicates the measles • outbreak code
COU indicates the country code•
PR indicates the province or state code•
DIS indicates the district code•
YR indicates the two-digit year (eg 09 for 2009)•
NUM indicates the outbreak number for the year (001 for the •
first outbreak of the year)
The following is recommended for outbreak investigations:
Assign outbreak ID by district surveillance staff; •
Notify other health facilities in the area;•
Interview households and collect details on Form B;•
Provide Vitamin-A and clinically manage cases; and•
Collect specimens from 5-10 cases, complete laboratory request •
form (Form C), and ship them to the laboratory.
Following an outbreak investigation, the area should be visited periodically for additional case finding. A measles outbreak is considered to be over when there are no new suspected cases in the affected district or neighbouring districts for at least three weeks.
Measles outbreak is fully investigated if:
A house-to-house survey is conducted in the affected area;•
At least five suspected cases are serologically tested for measles/•
rubella IgM; and
Case investigation form or line list with basic epidemiologic data- •
geographic location, age, vaccination status for measles, date of last vaccination, date of rash onset and outcome of illness is completed.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines30
7.2.3 Measles case management
There is significant morbidity and mortality associated with measles. During an outbreak adequate case management is critical for reducing measles mortality. Even though there is currently no specific treatment for measles infection, the administration of vitamin-A to children with measles has been shown to decrease both the severity and the case-fatality for the disease. WHO recommends that vitamin-A be administered to all children with acute measles infection as per the schedule given in Table 5 (16).
Table 5: Vitamin A Schedule
Age Immediately on diagnosis Next day
< 6 months 50,000 IU 50,000 IU
6 – 11 months 100,000 IU 100,000 IU
> 12 months 200,000 IU 200,000 IU
Supportive treatment should be provided for all cases, including supplemental fluids (such as oral rehydration solution) and antipyretics. Antibiotics should be used for cases complicated by otitis media or pneumonia and nutritional therapy provided for children with malnutrition. Many children require four to eight weeks to fully recover their pre-measles nutritional status. Detailed guidance on measles clinical case management is available in the WHO integrated management of childhood illness (IMCI) protocol for treating measles complications and management of the child with a serious infection or severe malnutrition (http://www.who.int/child-adolescent-health/integr.htm).
7.2.4 Collecting and testing specimens
In all outbreaks, 5-10 serum specimens should be collected to confirm the type of outbreak. The samples should be collected within 28 days after the onset of the rash. Urine or nasopharyngeal specimens should be collected in order to type the virus and determine the source of the outbreak. The details of collecting and processing specimens are given in Chapter 11. Role of laboratories in measles and rubella surveillance.
7.2.5 Confirming the type of outbreak
Confirmed measles outbreak: is defined as the occurrence of three or more confirmed measles cases (at least two of which should be laboratory confirmed; IgM positive) in a health facility/block/district (approximate catchment population of 100,000) in a month.
Confirmed rubella outbreak: is defined as the occurrence of three or more confirmed rubella cases (at least two of which should be laboratory

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 31
confirmed; IgM positive) in a health facility/block/district (approximate catchment population of 100,000) in a month.
Mixed outbreak: If at least one case is positive for measles and at least one case is positive for rubella, the outbreak is designated mixed outbreak.
Discard: If the samples are negative for both measles and for rubella, the outbreak is designated discarded.
Figure 9: Confirming type of suspected measles outbreak
7.2.6 Data collection, collation, analysis and determining the cause of the outbreak
During an outbreak, data collection should be limited to basic information from each case (name, address, age, sex, immunization status, date of last vaccination, symptoms, date of rash onset, outcome), which is collated into an outbreak linelist (Form B). Any additional information on the population where the outbreak occurred that may help to identify risk factors for measles should be obtained if possible. This includes routine immunization coverage, SIA coverage, HIV prevalence and nutrition status. The data should be analyzed rapidly to determine the extent and severity of the outbreak, vaccine effectiveness, potential risk factors for measles infection, and possible causes of the outbreak such as vaccine failure or failure to vaccinate.
In countries/provinces of large countries targeting measles mortality reduction and which have not conducted a catch-up measles immunization campaigns, the descriptive analysis should include time, place and person (see examples below). The key information is data on the age and vaccination status of cases which will help to identify the populations at the highest risk, and guide the response activities.
Mixed outbreak
Confirmedmeaslesoutbreak
Confirmedrubella
outbreak
*IgM ELISA tests for measles and rubella are more sensitive between 4 and 28 daysafter the onset of rash
All samples negative formeasles and rubella IgM
Three or more confirmedmeasles cases (at least two ofwhich are measles IgM positive)
Three or more confirmed rubellacases (at least two of which are
rubella IgM positive)
At least one case is measlesIgM +ve AND at least one case
is rubella IgM +ve
Discard
Clinically suspectedmeasles outbreak

Measles and Rubella Surveillance and Outbreak Investigation Guidelines32
Time: An epidemic curve as shown in Figure 10 can help determine if the peak of the outbreak is over and also the magnitude of the outbreak. Weekly incidence rates can be used to compare different geographic areas and monitor the progression of the outbreak over time.
Figure 10: Measles cases by epidemiologic week
Figure11: Number of cases in blocks, 2008 District A
0
100
200
300
400
500
600
44 45 46 47 48 49 50 51 52 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Surveillance week numbers for 2008- 2009
Case
s
N=458

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 33
Place: As shown in Figure 11, mapping the extent of the outbreak can help identify the most affected areas and identify clustering of cases.
Person: The characteristics of the cases such as age distribution and immunization status as shown in Table 6 and Table 7 can help to decide programme response. Table 6 shows that in District A, 397 of 458 or 87% of measles cases occurred among children below 10 years and Table 7 shows that only 12% of children below five years were vaccinated.
Table 6: Age distribution of cases in outbreaks, 2008: District A
Year 2008 < 1 Year 1-4 Years 5-9 Years 10-15 Years
> 15 Years Total
Outbreak 1 12 88 55 29 4 188
Outbreak 2 8 56 23 11 0 98
Outbreak 3 3 17 15 5 0 40
Outbreak 4 9 68 43 11 1 132
Total 32 229 136 56 5 458
Table 7: Vaccination status of <5 years’ cases in outbreaks, 2008: District A
Year 2008 Vaccinated Unvaccinated Unknown Total
Outbreak 1 14 68 18 100Outbreak 2 10 49 5 64Outbreak 3 1 18 1 20Outbreak 4 6 66 5 77
Total 31 201 29 261
The quality and reliability of the surveillance system generating the data is an important element to consider when interpreting information. In measles endemic areas, the following information is essential for deciding response activities:
Case fatality rate (CFR)
The case fatality rate measures the proportion of deaths among cases1. CFR should be calculated for the community and hospitals separately. The CFR is an indicator of the severity of the outbreak. The CFR can be calculated as follows:
CFR = Number of cases who died of measles X100 Total number of measles cases
1 A measles-related death is a death of an individual with confirmed (clinically, laboratory-con-firmed or epidemiologically) measles in which death occurs within 30 days of rash onset and is not due to other unrelated cause e.g., a trauma or chronic disease.
Measles and Rubella Surveillance and Outbreak Investigation Guidelines34
In the community, the CFR may be underestimated, as many cases that die at home are not reported. In hospitals, the CFR may be high probably because only severe cases seek hospital care or due to poor case management.
If a more accurate estimate of the CFR is required, a community-based study should be conducted focusing on CFR estimates by age groups.
Additional data analysis in countries/provinces of large countries targeting measles mortality reduction and which have conducted catch-up measles immunization campaigns.
Additional data analysis to determine the attack rate and the vaccine efficacy using population data need to be done only for a few outbreaks in countries targeting measles mortality reduction and which have conducted catch-up measles immunization campaigns.
In low-incidence areas where measles SIAs have been conducted, additional information on the population will assist the programme in deciding the outbreak response. A community survey using Additional Form B could be used to collect population information from a few outbreak-affected areas.
Attack rate (AR)
The AR expresses the risk of disease in population in a given area since the beginning of the outbreak. If population data by age groups are available, age-specific attack rates can be calculated, which can help identify priority age groups for vaccination.
AR 0-11 months = Number of cases in children age 0 to 11 months X100 Total number of children aged 0 to 11 months
AR allows the comparison of risk of outbreak between different populations. For example; Table 8 shows the attack rates by village in Hosdurga Block of Chitradurga district in Karnataka, India, for the outbreak from January to April 2008. In this outbreak, Kenkere village had the highest attack rate but a fewer number of cases compared to two other villages (Madadakere and Lakkihalli) of the same block. Identifying the location of infection rather than place of treatment for suspected cases is important in order to follow the geographic spread and identifying areas of high risk.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 35
Table 8: Measles outbreak, Chitradurga district, Hosdurga block, India
MOB-IND-KA-CDG-08-002, Jan – Apr 2008*
Villages Population Cases Attack rate
Madadakere 2290 38 1.7
Kenkere 950 20 2.1
Sanna Kittadahalli 749 2 0.3
Dodda Kittadahalli 890 7 0.8
Lakkihalli 2458 22 0.9
Anchebarihatti 485 1 0.2
Nakikere 1526 3 0.2
Rangapanahatti Thanda 366 0 0.0
Total 9684 93 1.0*Source: NPSP: Government of India - WHO collaboration
Vaccine efficacy (VE)
The VE is estimated from outbreak and routine coverage data. The difference between attack rates among vaccinated persons (ARV) and those among the unvaccinated (ARU) is expressed as a fraction of the attack rate among unvaccinated persons (ARU):
VE = (ARU-ARV)/ARU
If there is a greater proportional reduction of illness in the vaccinated group as compared to the unvaccinated group, then there is greater VE.
Vaccine efficacy can be estimated by plotting the percentages of measles cases occurring in vaccinated individuals (PCV %) and the percentage of the population vaccinated (PPV %) on a normogram, which shows the relationship between PPV, PCV and VE (Figure 12)(17). For instance, if 60% of measles cases are in individuals vaccinated against measles and if vaccination coverage is 95%, vaccine effectiveness is close to 95%; if 30% of measles cases are in individuals vaccinated against measles and if vaccination coverage is 60%, vaccine effectiveness is about 70%.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines36
Figure 12: Relationship between percentage of cases vaccinated (PCV) and percentage of population vaccinated
(PPV) for seven values of vaccine efficacy (VE)
Notifying authorities
Health authorities and facilities at all levels should be notified of outbreaks and updated as frequently as possible. Once an outbreak has been laboratory confirmed, sub-district and district staff should report the information to the next administrative level using the outbreak investigation summary form (Form D)(14). Any additional supplies and technical support should be sought at this time.
Under the International Health Regulations (IHR 2005), a measles outbreak could be considered a Public Health Emergency of International Concern (PHEIC). Consequently, all measles outbreaks should be reported to the health authorities at the local, regional and national levels. The national health authority will decide if the measles outbreak should be considered a PHEIC and reported to WHO(18).
7.3 Immunization response to measles outbreaks
7.3.1 Assessing the risk of a large outbreak with high morbidity and mortality
As soon as an outbreak is suspected, the risk of a large outbreak with high morbidity and mortality must be assessed. This evaluation is needed
0
10
20
30
40
50
60
70
80
90
100
0 10 20 30 40 50 60 70 80 90 100
PPV %
PC
V%
ve=40
ve=50
ve=60
ve=70
ve=80
ve=90
ve=95
PCV = PPV - (PPV x VE)
1 - (PPV x VE)

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 37
to determine susceptibility and potential spread in both affected and neighbouring areas as well as the appropriate vaccination response to control the outbreak.
Approximately 15% of children vaccinated at nine months of age and 5%–10% of those vaccinated at 12 months of age fail to seroconvert and are not protected after vaccination. In Table 9, district M has a population of 500,000 and 12,500 births per year and illustrates the build-up of susceptible children. If 80% of children aged one year receive measles vaccination through routine health services and assuming 85% vaccine effectiveness, only 8,500 children (12,500 x 80% x 85%) or 68% in each birth cohort will be protected against measles and 4,000 children (32%) will remain susceptible to measles. Thus, 4,000 children will be added each year to the pool of measles-susceptible children. As a general guide, an outbreak is likely to occur when the pool of susceptible children reaches the size of one birth cohort. In this example, an outbreak is likely to occur in district M after three to four years.
Table 9: Accumulation of susceptible children with each successive birth cohort over a four year period in district M
with 80% coverage / vaccine effectiveness of 85%
Year Cumulative No. of live births
Cumulative No. children protected against measles
Cumulative No. children susceptible
to measles
1 12,500 8,500 4,000
2 25,000 17,000 8,000
3 37,500 25,500 12,000
4 50,000 34,000 16,000
To evaluate the risk of further transmission, morbidity and mortality, the following factors should be taken into consideration:
Population characteristics such as size, density, movement, and •
setting;
Under five mortality rates;•
Nutritional and vitamin-A status;•
HIV prevalence;•
Period of the year: seasonal outbreaks or holidays, festivals and •
social events that would increase opportunities for spread;
Cases reported and comparison with previous years; and•
Access to health services.•

Measles and Rubella Surveillance and Outbreak Investigation Guidelines38
7.3.2 Conducting appropriate vaccination activities
District-level outbreak coordination committees need to determine the appropriate vaccination activities under the following broad principles:
As soon as an outbreak is suspected the two steps mentioned below (selective vaccination activities and reinforcement of routine vaccination) should be taken concurrently. Further, as soon as the outbreak is confirmed, the district outbreak coordination committee should review risk assessment results and accordingly decide whether to continue with the selective vaccination activities or to carry out a non-selective vaccination campaign.
Selective vaccination activities
Enhance social mobilization activities to inform the affected •
communities about the suspected outbreak, which specific age-group of previously unvaccinated children is targeted for measles vaccination and where parents should bring their at-risk children for vaccination.
Vaccinate all children (six to 59 months of age) presenting to a •
health facility or an outreach vaccination site without a history of measles vaccination (either written or verbal). Children receiving measles vaccine before the age of nine months must be revaccinated after the age of nine months (with at least a one-month interval between the doses).
Ensure sufficient supplies: Use stock management records to •
determine available quantity and location of vaccine, AD syringes and other supplies (e.g. cold chain equipment and Vitamin-A) that are immediately available for use. Estimate and request the additional supplies needed so that activities are not interrupted due to supply stock-outs.
Reinforcement of routine vaccination
A measles outbreak provides an opportunity to identify routine immunization programme weaknesses causing the outbreak and a chance to correct them. As soon as a measles outbreak is suspected, without waiting for the laboratory confirmation of the suspected measles cases, the following steps to reinforce routine vaccination should be taken:
District staff, health facility staff and partners should • rapidly identify priority areas within the affected district (e.g. communities with low vaccination coverage and high risk of morbidity and mortality);

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 39
Jointly work on strengthening the available district immunization •
workplans;
Locate health centres conducting immunization sessions that •
may need additional staff or vaccine supplies; and
Organize corrective measures such as additional outreach services •
to communities with a high proportion of unreached children.
Non-selective mass vaccination activity
As soon as the outbreak is confirmed, and if the risk assessment results indicate that there is a high risk of a large measles outbreak, then the capacity to carry out a high quality, large-scale immunization campaign should be rapidly evaluated by:
Evaluating the availability of staff and financial resources (both •
internal and external) for the operational and logistical aspects of the campaign; and
Evaluating if the vaccine and other supplies can be made available •
at the time needed.
If there is sufficient capacity (human and financial resources, vaccine and other supplies), to carry out a safe and timely vaccination campaign, then a mass vaccination campaign should be carried out in the targeted areas (affected and neighbouring areas as determined by the risk assessment). However, if the outcome of the assessment does not indicate a mass vaccination response, then selective immunization of unimmunized children presenting to health facilities as outlined above should be continued and the number of reported cases closely followed to monitor the progression of the outbreak.
For the non-selective mass vaccination response, the timing, target age group and area for vaccination should be defined as outlined below. An accelerated micro-planning exercise should be performed to determine the bundled vaccine, logistics, staffing and communication needs for the campaign. Existing country or regional guidelines for conducting mass measles vaccination campaigns should be used.
Timing of intervention and target population
Once the decision to intervene has been made, it is critical to act quickly to minimize the number of measles cases and deaths. Choosing the target population depends upon the susceptibility profile of the population. Key elements to consider are:

Measles and Rubella Surveillance and Outbreak Investigation Guidelines40
Routine vaccination coverage and coverage during SIAs in each •
birth cohort;
Age specific attack rates; and•
Absolute number of cases.•
For example, Table 10 shows the attack rates and population and number of cases during an outbreak in Khulna district in Bangladesh in 2005. The highest attack rate is in children < 1 year. Although the attack rate in the 5 – 9 year old age group is lower, the absolute number of cases in this age group is almost 35%. It is important to consider absolute numbers of cases and the potential at-risk population as well as the attack rate. In this example, the 5 – 9 year-old age group also may contribute to transmitting the disease to younger age groups and should be targeted for vaccination.
Table 10: Measles attack rates by age group in BANMSL3329205002 outbreak in Khulna District, Bangladesh, 2005*
Age group Population sur-veyed Cases AR %
< 1 year 144 23 16.0
1-4 years 482 73 15.1
5-9 years 774 107 13.8
10-14 years 765 73 9.5
>=15 years 3802 38 1.0
Total 5967 314 5.3
* Source: Expanded Program of Immunization: Government of Bangladesh
It is critical that the results from the outbreak investigation be used to develop and tailor an appropriate response. If the data suggest that older children are affected then the age group initially targeted for vaccination should be adjusted to include the older cohorts. Even if the attack rate is low in some age groups, especially in older age groups, they may represent a large number of cases and could potentially transmit the infection to younger age groups. Once the age group targeted for vaccination is determined, all children in that age group should be vaccinated, regardless of their vaccination status.
Target area
The response should target both outbreak-affected areas and adjacent areas in which the risk assessment shows a high risk of spread. As distinct from preventive SIAs (e.g., catch-up and follow-up campaigns) that target whole countries, provinces or states, campaigns in response to outbreaks should be more limited in scale.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 41
Health staff should pay particular attention to ensure that groups and areas with high likelihood of not being reached and at high risk for measles-related complications are reached during the vaccination activities, and any necessary supplemental measures such as the provision of vitamin-A are provided. These vulnerable groups and areas include:
Young children, particularly those under one year of age; •
Malnourished and vitamin-A deficient children;•
Infants and children of HIV-infected women, and other immuno-•
compromised children;
Certain ethnic and religious groups who may have poor access •
to immunization;
Populations with poor access to health care;•
Hospitals and other health facilities; and•
All children above six months of age who are attending hospitals •
(inpatients and outpatients) or who are visiting the hospital.
Children receiving measles vaccine before the age of nine months during a campaign must be revaccinated after the age of nine months (maintaining a one month interval between two doses) since the efficacy of vaccine administered before nine months of age is likely to be low. Strategies to ensure that these children receive a second dose of measles vaccine include the following:
Inform mothers at the time of vaccination that their child must •
be vaccinated again;
Notify health workers, non-governmental organizations, and the •
community about the need for these infants to receive a second dose.
Target coverage
Ideally, the target coverage (the proportion of the target population to vaccinate) should be 100%. However, this may not always be possible, given the available resources. Even if it is not possible to achieve 100% coverage, the intervention should be conducted. Once the vaccination activities are conducted, it is important to carry out rapid coverage monitoring to estimate the achieved coverage and identify potential groups of missed children and ensure they are vaccinated.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines42
7.4 Ensuring effective community involvement and public awareness
When an outbreak is confirmed there is likely to be widespread public concern and media attention. It is important to keep the public informed, to calm fear and encourage cooperation. Messages to the community should be clear and concise using local terminology, and should convey the following:
Existence of an outbreak and the benefits of measles •
vaccination;
Signs and symptoms of the disease;•
Encourage parents whose children have had a recent rash and •
fever illness to consult a health care facility;
Instruct parents to bring their children to a health facility/vaccine •
post for vaccination; and
Inform about locations and timings of health facility/vaccine •
posts.
Messages to the community can be transmitted by radio/television, newspapers, posters and fliers, meetings with health personnel, community, religious and political leaders, and presentations at markets, health centres and schools. The media are useful partners in keeping the public informed through regular press releases and conferences. Select and use a community spokesperson to serve as a focal person for the media. As soon as the outbreak has been recognized, release information to the media only through the spokesperson to make sure that the community receives clear and consistent information.
On a regular basis, meet with the spokesperson to give:
Frequent, up-to-date information on the outbreak and response; •
and
Clear and simple health messages that the media should use.•

Monitoring and evaluation in countries/provinces of large countries targeting measles
mortality reduction
For the Region, routine immunization coverage, measles incidence and outbreaks are monitored through Annual Regional EPI Reporting (Form F) and WHO/UNICEF Joint Reporting Forms. Countries should also send a monthly VPD reporting form (Form E) to the Regional Office. Linelists from low incidence countries need to be transmitted on a regular basis. Periodic analysis enables the Region to monitor for completeness and timeliness of measles reporting, outbreak investigations, monthly trends and laboratory performance. Furthermore, the annual SEAR EPI Managers and Immunization Technical Advisory Group (ITAG) meetings are forums for reviewing the status and progress of the vaccine preventable disease control activities in the Region.
Chapter 8

Measles and Rubella Surveillance and Outbreak Investigation Guidelines44
WHO and UNICEF provide assistance in monitoring existing national disease surveillance programmes in order to achieve sub-national targets. This includes supervision of the surveillance and laboratory activities, monitoring of the routine measles coverage, and the quality of SIAs through external monitors. The basic elements of measles surveillance should be part of EPI and Acute Flaccid Paralysis (AFP) surveillance reviews.
8.1 Immunization coverage indicators for all countries
The key immunization coverage indicators for measles control at national and district levels are given in Table 11 below.
Table 11: Measles immunization coverage indicators – SEA Region
Area/Level Vaccine type Indicator SEA Regional Target
National level
MCV1 and MCV2 Immunization coverage 90%
Supplementary Immunization Activities with
measles containing vaccine
Immunization coverage 90%
District level
MCV1
Percentage of districts with routine measles
coverage(<50%, 50-79%, 80-90%, 90%+)
All districts > 80%
MCV2
Percentage of districts with routine measles
coverage(<50%, 50-79%, 80-90%, 90%+)
All districts > 80%
Supplementary Immunization activities with
measles containing vaccine
Percentage of districts with SIAs coverage level (<80%; 80-90%, 90%+)
All districts > 90%
8.2 Disease incidence and surveillance performance indicators
The indicators depend on whether a country is collecting aggregate data or case-based data.
Countries collecting aggregated data
Annual number/incidence of reported measles cases and •
deaths.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 45
Annual number of reported rubella cases.•
Percentage of reported supected measles outbreaks fully •
investigated (target 100%).
Completeness of monthly VPD surveillance reports (target •
100%).
Timeliness of monthly VPD surveillance reports (target 80%).•
Percentage of adequate specimens sent to the laboratory (target •
80%).
Percentage of specimens with laboratory results within 14 days •
(target 80%).
Measles case fatality rates.•
Countries collecting case-based data
Annual incidence of measles cases (laboratory confirmed and •
epidemiologically linked) and deaths.
Annual national incidence of non-measles suspected measles •
cases (target more than 2 per 100,000 population).
Percentage of districts annually reporting at least one non-measles •
suspected measles case per 100,000 population (target at least 80% districts).
Annual number of reported rubella cases.•
Percentage of reported suspected measles outbreaks fully •
investigated (target 100%).
Completeness of monthly VPD surveillance reports (target •
100%).
Timeliness of monthly VPD surveillance reports (target 80%).•
Percentage of suspected measles cases tested in a proficient •
laboratory, any cases that are epidemiologically linked to a laboratory confirmed case are excluded from the denominator (target 80%).
Percentage of outbreaks tested for virus detection (target •
80%).
Percentage of specimens with laboratory results within 14 days •
(target 80%).
Measles case fatality rates•
Percentage of all suspected cases adequately• 2 investigated.
2 An adequate investigation includes at a minimum, collection of all the following data elements from the suspected measles cases: date of rash onset; date of specimen collection; vaccination status; age and district.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines46

Chapter 9
Measles surveillance, outbreak detection and response in
countries targeting elimination
Countries achieving and maintaining immunization coverage goals with MCV1 and a second opportunity of measles vaccination in all districts and nationally should raise their surveillance standards to monitor progress towards measles elimination. Priorities are to identify the final chains of transmission, monitor the measles epidemiology (age groups at risk, inter-epidemic period, immunization status) and accelerate immunization activities to avert potential outbreaks.
9.1 Indicators for monitoring progress towards elimination and targets for elimination
In countries with elimination goals, the surveillance system must be sensitive and specific to ensure the detection of measles virus. The surveillance system performance indicators and targets are outlined below.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines48
9.1.1 Surveillance performance indicators for countries targeting elimination
Reporting rate
Countries should report annually at least two non-measles •
suspected measles cases per 100,000 population. These cases must have been investigated and discarded as non-measles cases using laboratory testing in a WHO accredited laboratory and/or epidemiological linkage to another confirmed disease.
Administrative units with a population of a least 100,000 should •
report annually at least one non-measles suspected measles case in at least 80% of districts.
Laboratory confirmation: Specimens adequate for detecting measles IgM should be collected from at least 80% of suspected measles cases and laboratory tested in a WHO accredited laboratory. Any cases that are epidemiologically linked1 to a laboratory confirmed case of measles or other communicable disease should be excluded from the denominator.
Viral detection: Samples should be collected for virus detection from 80% of identified transmission chains (outbreaks) and tested in an accredited laboratory. The numerator is the number of transmission chains with sufficient samples for viral detection and the denominator is the number of transmission chains identified.
Adequacy of investigation: At least 80% of all reported suspected measles cases should have had an adequate investigation within 48 hours of notification. The numerator is the number of suspected measles cases for which an adequate2 investigation was carried out within 48 hours of notification, and the denominator is the total number of suspected measles cases.
9.1.2 Indicators for monitoring progress towards elimination and targets suggestive of having achieved elimination
Each of the following indicators has a target, the achievement of which would be suggestive of elimination. Because country-specific scenarios can
1 Epidemiological linkage: A case that meets the clinical case definition and has contact with a lab-oratory-confirmed measles case whose rash onset was within the preceding 7-21 days or a case that lives in the same district or adjacent district where a measles outbreak has been laboratory confirmed and transmission is plausible.
2 An adequate investigation includes at a minimum the collection of all of the following data ele-ments from each suspected measles case: name or identifiers, age (or date of birth), sex, date of rash onset, date of specimen collection, vaccination status, date of last vaccination, and district in addition to an investigation of all epidemiological links (as defined at the country/regional level).

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 49
lead to misinterpretation of any one of the four indicators, the proposed indicators should not be used in isolation. These indicators are useful for providing general guidance and once targets have been achieved an in-depth review is recommended to confirm elimination.
Vaccination coverage
Countries should continuously monitor vaccination coverage to assess population immunity.
Vaccination coverage indicator: Vaccination coverage of both •
routine first dose (MCV1) and second dose (either routine second dose MCV2 or SIA coverage).
Vaccination coverage target: Achieving and maintaining at least •
95% coverage with both MCV1 and the second dose of measles vaccination in all districts and nationally.
Outbreak size
Monitoring outbreak size demonstrates that the chains of transmission are self-limited as a result of very high population immunity to measles. The outbreak-size indicator is intended to encourage countries to conduct thorough outbreak investigations. The outbreak size data can be misleading in the absence of thorough outbreak investigation that includes active case finding and epidemiological linked cases.
Outbreak size indicator: Monitoring of outbreak size of all •
outbreaks including outbreaks in closed settings and outbreaks where interventions have taken place to stop the outbreak.
Outbreak size target: At least 80% of outbreaks should have •
less than 10 confirmed measles cases.
Incidence
Incidence indicator: Measles incidence per million per year. The •
numerator should exclude measles cases confirmed as imported3.
Incidence target: Achieving a measles incidence of less than one •
confirmed measles case per million population per year excluding cases confirmed as imported.
Endemic measles virus strain(s)
Countries should try to detect all epidemiological links to importation and determine measles virus’ genetic sequence for all chains of transmission.
3 All import-related cases and sporadic or endemic measles cases that are not imported should be included.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines50
This data can be used to provide evidence of the absence of endemic measles transmission and confirm importation.
Endemic measles indicator: The number of endemic measles •
virus strains
Endemic measles target: Zero cases of measles caused by an •
endemic strain for at least 12 months.
9.2 Definitions specific to measles elimination
Elimination: The absence of endemic measles cases for a period of 12 months or more, in the presence of adequate surveillance.
Outbreak in countries that target elimination: One or more laboratory confirmed case of measles in a country that targets elimination is considered an outbreak.
Measles imported case: A case exposed outside the region/country during the 7 - 21 days prior to rash onset as supported by epidemiological and/or virological evidence.
Measles import-related cases are locally-acquired infections occurring as part of a chain of transmission originated by an imported case as supported by epidemiologic and/or virological evidence.
Chain of transmission: When two or more confirmed cases are temporally-related (with 7-21 days between rash and onset of cases), and are epidemiologically and/or genetically linked.
Endemic measles transmission in countries targeting elimination: The existence of continuous transmission of indigenous or imported measles virus that persists for a period of 12 months or more in any defined geographical area.
Re-establishment of endemic transmission: This is a situation in which epidemiological and laboratory evidence indicates the presence of a chain of transmission of laboratory-confirmed virus that continues uninterrupted for a period of 12 months or more.
9.3 Operationalizing measles surveillance in countries targeting elimination
In countries targeting elimination every suspected case should be investigated immediately as part of the case-based surveillance system with laboratory specimens collected from all cases. In the event of a

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 51
Serum/ urinesamples from all
cases
ProgrammeresponseLab test +ve
Confirmedmeasles or rubella
CaseData analysis
Enhancement ofsurveillance
Detect and notify all clinicallysuspect measles cases
Notifyauthorities
Investigate all clinicallysuspect measles cases
Outbreakinvestigation
Case management,Vitamin A supplementation andsearch for additional cases
suspected measles outbreak, 5 to 10 specimens should be collected for confirmation and urine or nasopharyngeal specimens should be collected for virus detection/genotyping and to characterize viral circulation and importation patterns. The key elements in operationalizing measles surveillance in countries targeting elimination are outlined in Figure 13:
Figure 13: Measles and rubella surveillance in countries targeting elimination
9.3.1 Enhanced surveillance
The network should ensure that all suspected measles cases are identified and notified. Case-based reporting and laboratory confirmation of every clinically suspected measles case is essential. Measles surveillance reporting sites need to be categorized and prioritized based on the case reporting patterns. Reporting should include weekly zero reporting even when no cases are detected. Active case finding in priority reporting sites should be systematically instituted and monitored.
9.3.2 Detection and notification of all clinically suspect measles cases
When a suspected case is detected, the district should be notified within 24 to 48 hours. The district should report to the state / province or

Measles and Rubella Surveillance and Outbreak Investigation Guidelines52
Summary steps in response to measles outbreaks in countries targeting elimination
Isolate in household and investigate suspected cases.•
Obtain appropriate blood specimens for confirmation, as well as •
specimens for viral detection/isolation.
Inform other health authorities.•
Assess coverage in affected and surrounding areas.•
Provide measles vaccine to unvaccinated persons.•
Enhance surveillance, including active case-searches for further •
suspected cases.
Analyze/summarize outbreak.•
national level within 24 to 48 hours of confirmation. Establishing a special “hot line” is recommended to convey information by the fastest means possible (telephone, telegram, aerogram, fax, SMS or email).
9.3.3 Investigation of all clinically suspected measles cases (20)
Whenever a patient is suspected of having measles, outbreak control measures and a detailed investigation should be initiated in the area of the patient’s residence without waiting for laboratory confirmation.
Health care provider responsibilities:
Obtain basic information, clinical data, a blood sample and urine •
or nasopharyngeal sample during the first contact (as this could be the only contact with the patient).
Inform the patient or parent that a district health officer/surveillance •
focal person will visit their home for additional information.
District health/surveillance focal person responsibilities:
Visit the family immediately and determine whether the case •
meets the clinical case definition for measles, assign a case epid number and complete the suspected measles/rubella case investigation form (Form G).
Collect specimens (if it has not been done already).•
Ask the family if the case has traveled or had close contact with •
individuals from other areas 7–21 days before the onset of the illness.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 53
Visit homes up to 1000 meters (1 km) away from the case or •
in the same block/neighbourhood and find out if similar cases occurred in the previous month.
Visit health facilities, local private doctors, laboratories, •
pharmacies, traditional healers, nurseries and schools in the area to see if there are any other similar cases.
Advise families to keep patients at home and the number of •
visitors to a minimum until the rash disappears.
Immunize all children in the target age group living in the •
neighbourhood who have not received two doses of measles vaccine.
Notify the neighbourhood and schools about the measles case in the •
area and encourage vaccination among unprotected children.
9.3.4 Management of measles cases
Clinical case management of every suspected or confirmed measles case is critical to reducing the immediate and long-term complications. The details are described in Chapter 7 Outbreak investigation and response in countries targeting measles mortality reduction.
9.3.5 Identification and investigation of outbreaks
A single laboratory confirmed measles case confirms a measles outbreak during measles elimination. The locality of the suspected measles case should be visited and outbreak control measures and detailed investigation initiated without waiting for laboratory confirmation. Additional cases must be searched. If additional cases are found, then each should be investigated and specimens collected for serology and virus isolation. The source of the infection should be epidemiologically linked whenever possible. In addition to the details described in Chapter 7, data analysis should focus on quality assurance and performance of the reporting system.
Information on suspected and confirmed measles cases, vaccination activities, and areas visited should be monitored and updated continuously during an outbreak. When no new cases are reported during a three-week period, despite the presence of enhanced surveillance, the outbreak may be considered to be at an end. At the end of an outbreak, a report should be prepared describing the outbreak, time, place and person analysis, control measures taken, issues identified, conclusions and recommendations. Virus isolation and genotyping should provide

Measles and Rubella Surveillance and Outbreak Investigation Guidelines54
information on the origin of the infection and evidence of importation or endemic transmission.
9.3.6 Collecting and testing of specimens
All chains of measles transmission should have at least one viral isolation and genetic analysis conducted at a WHO accredited laboratory. When sporadic cases are investigated the samples (serum and urine or nasopharyngeal specimens) need to be collected from each case and shipped to the laboratory (Form H). In an outbreak situation, serum samples need to be collected from only 5 to 10 suspected patients for testing (Form C). If the transmission chain continues over an extended period, further suspected patients should be sampled at intervals of two to three months.
9.3.7 Notification of health authorities
Health authorities at all levels should be notified of an outbreak using Form D. If a suspected case has traveled or had close contact with individuals from other areas of the country 7–21 days before the onset of the illness, the surveillance focal person(s) in those areas should be notified immediately. The public should be informed through the media about the outbreak and any control efforts.
9.3.8 Programme response
Health authorities should evaluate each case or outbreak and determine the surveillance and immunization response.
Surveillance response: As part of the response to a measles outbreak, surveillance should be intensified to search for additional suspected cases. All reporting sites should be notified of the suspected measles outbreak and be alerted to look for additional cases with daily calls or visits to schools, hospital emergency rooms, and selected pediatricians.
Immunization response: Epidemiological information collected during the outbreak investigation should be analyzed and an appropriate immunization response initiated. Vaccination within 72 hours of exposure may help to prevent the disease or mitigate severity.
Vaccination of previously unvaccinated persons should start immediately. All children nine months to 15 years of age without a history of measles vaccination should be vaccinated. If the outbreak is large and many cases are occurring in infants aged less than nine months, the age of routine vaccination should be decreased to six months. These infants

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 55
should be revaccinated when they reach nine months of age. All health workers must be vaccinated. Children hospitalized or attending outpatient clinics for any reason and who cannot provide written proof of measles vaccination should be vaccinated, if not contraindicated.
The focus of vaccination efforts should target pockets of susceptible infants and children. Gathering points such as schools, churches, and health posts may be chosen as mass vaccination sites. In addition, vaccination of adolescents and young adults residing or working in institutions, such as military bases, university dormitories, hospitals, religious centres and factories, should be considered.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines56

Rubella and congenital rubella syndrome (CRS) surveillance
As countries in the South-East Asia Region complete supplementary measles immunization campaigns and improve their surveillance systems, rubella has emerged as a disease of concern. To adequately understand the burden in the Region, rubella and CRS should be included in each country’s vaccine preventable diseases (VPD) surveillance systems. The focus of the surveillance system will depend on whether the national goal is CRS prevention or rubella and CRS elimination. The following are elements for establishing surveillance:
Include rubella and CRS on the list of •
notifiable diseases and integrate with other VPD surveillance;
Identify rubella outbreaks as part of the •
measles surveillance system. Ensure that serum samples are also tested for rubella in all suspected measles outbreaks where the samples are negative for measles;
Chapter 10

Measles and Rubella Surveillance and Outbreak Investigation Guidelines58
Investigate suspected rubella outbreaks and follow-up pregnant •
women in the rubella confirmed and mixed outbreaks for CRS; and
Establish sentinel surveillance for CRS at neonatal, paediatric, •
ophthalmology, cardiology, ENT and obstetric units.
10.1 The epidemiologic and clinical basis of rubella surveillance
Rubella is a mild illness but if acquired in early pregnancy can lead to CRS in infants. The major problems associated with CRS include deafness, blindness, heart disease, and mental retardation.
The rubella virus is an enveloped single stranded RNA virus with a single serotype belonging to the togavirus family and genus rubivirus. Humans are the only known host and transmission is by respiratory droplets. Viral replication occurs in the nasopharyngeal mucosa and local lymph nodes. The incubation period ranges from 12 to 23 days with an average of 18 days(19).
Figure 14: Serology after rubella virus infection(12)
Viraemia occurs five to seven days after exposure and leads to viral spread to different organs. In pregnancy the virus infects the placenta and developing fetus. Rubella virus can be found in nasopharyngeal samples from one week before to two weeks after rash onset with maximal shedding after one to five days. Infants with congenital rubella may excrete the virus for more than a year in pharyngeal secretions and urine.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 59
Antibodies are first detectable about 14-18 days after acquired rubella infection at about the time the maculopapular rash appears. A rise in IgM and IgG levels is observed, but IgM antibody levels wane fairly quickly and are undetectable by eight weeks, while IgG persists. Passively acquired maternal antibodies provide protection against rubella for the first few months of life and can affect immune response to the rubella vaccine.
The diagnosis of rubella requires laboratory confirmation, particularly under non-epidemic conditions. Serology is the preferred method for routine laboratory diagnosis. Presence of rubella IgM or demonstration of a significant rise in rubella IgG from paired acute and convalescent sera provide evidence of ongoing or recent rubella infection. Viral isolation is time consuming and costly and is not routinely used for diagnosis but is important for molecular surveillance purposes.
10.1.1 Clinical presentation
Acquired rubella is characterized by a transient, erythematous rash, conjunctivitis, coryza, postauricular/ suboccipital lymphadenopathy, low grade fever and nausea. Arthralgia and arthritis rarely occur in children, but may affect up to 70% of adults, particularly women. The rash that starts on the face and neck progresses down the body may be pruritic. It usually lasts between one and three days and is fainter than measles rash, doesn’t coalesce and may be difficult to detect on pigmented skin(20). Haemorrhagic manifestations, Guillain-Barrè syndrome and encephalitis are rare. Serological studies have shown that 20%-50% of all rubella infections are subclinical(19).
Congenital rubella infection and CRS are caused by infection in early pregnancy (from prior to conception to the first 10 weeks of gestation).Rubella infection may result in multiple fetal defects in up to 90% of cases, and often results in miscarriage or stillbirth. Fetal defects are rarely associated with maternal rubella infections after the 16th week of pregnancy, although sensorineural hearing deficit may occasionally occur up to week 20.
Natural rubella infection normally confers lifelong immunity. There have been rare cases of serologically documented re-infections either after earlier natural infection or after vaccination. Re-infection in pregnancy resulting in CRS has occasionally been reported in women with natural or vaccine-induced immunity, but the risk to the fetus is low.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines60
Table 12: Main clinical manifestations of congenital rubella(21)
GeneralFetal loss (spontaneous abortion and stillbirths)Low birth weightMicrognathia
Ears and central nervous systemSensorineural deafness: unilateral or bilateralCentral auditory deafnessMental retardationSpeech defects
Cardiovascular systemPatent ductus arteriosusPulmonary arterial stenosisVentricular septal defects
EyesRetinopathyCataracts: pearly, dense, nuclear; 50% bilateralMicrophthalmos
Transient neonatal manifestationsThrombocytopenia, +/- purpuraHepatospenomegalyMeningoencephalitisBody radiolucenciesAdenopathies
Late-emerging or developmentalLate-onset interstitial pneumonitis, age 3-12 monthsChronic diarrhoeaInsulin-dependent diabetes mellitus
Rubella standard case definitions(22)
Suspected rubella case:• Any patient of any age in whom a health personnel suspects rubella. Health personnel should suspect rubella when a patient presents with fever, maculopapular rash; and cervical, suboccipital or postauricular adenopathy or arthralgia/arthritis.
Clinical confirmation:• Rubella cannot be confirmed clinically: laboratory confirmation is required.
Laboratory confirmed rubella case:• A laboratory-confirmed case is a suspected case with a positive blood test for rubella-specific IgM. The blood specimen should be obtained within 28 days after the onset of rash.
Epidemiologically confirmed rubella case:• A patient with a febrile rash illness that is linked epidemiologically to a laboratory-confirmed rubella case.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 61
List A List B
Cataract(s)
Congenital Glaucoma
Congenital Heart Disease
Loss of Hearing
Pigmentary Retinopathy
Purpura
Splenomegaly
Microcephaly
Mental Retardation
Meningoencephalitis
Radiolucent Bone Disease
Jaundice (within 24hr post-delivery)
Confirmed rubella outbreak• is defined as the occurrence of three or more confirmed rubella cases (at least two of which should be laboratory confirmed; IgM positive) in a health facility/district/block (approximate catchment population of 100,000) in a month.
Congenital rubella syndrome (CRS) standard case definitions
Suspected CRS case:• Any infant less than one year of age in whom a health worker suspects CRS.
A health worker should suspect CRS when an infant aged 0-11 months presents with heart disease and/or suspicion of deafness and/or one or more of the following eye signs: white pupil (cataract), diminished vision, pendular movement of the eyes (nystagmus), squint, smaller eye ball (microphthalmus), or larger eye ball (congenital glaucoma).
A health worker should also suspect CRS when an infant’s mother has a history of suspected or confirmed rubella during pregnancy, even when the infant shows no signs of CRS.
Clinically confirmed CRS case:• Any infant in whom a qualified physician detects at least two of the conditions from list A or one from list A and one from list B:
Laboratory confirmed CRS case:• An infant with clinically-confirmed CRS who has a positive blood test for rubella-specific IgM.
100% of such infants are positive at the age of 0-5 months; 60% are positive at 6-11 months. Where special laboratory resources are available the detection of rubella virus in specimens from the pharynx or urine of an infant with suspected CRS provides laboratory confirmation of CRS (60% of such infants shed rubella virus at the age of 1-4 months; 30% at 5-8 months: 10% at 9-11 months).

Measles and Rubella Surveillance and Outbreak Investigation Guidelines62
Congenital rubella infection (CRI):• An infant who does not have clinical signs of CRS but who has a positive rubella-specific IgM test is classified as having congenital rubella infection (CRI).
If a mother has suspected or confirmed rubella in pregnancy her infant should have a rubella-specific IgM blood test.
10.2 Recommended types of surveillance
All countries that include rubella vaccine in their immunization services should conduct surveillance for CRS and rubella. In the CRS prevention stage, disease surveillance should focus on CRS case detection. In the CRS/rubella elimination phase (usually in conjunction with measles elimination), case-based surveillance should be conducted for febrile rash illness (23).Rubella surveillance activities should be based on the stage of the rubella immunization strategy. For countries with a functioning measles surveillance system, rubella outbreaks will be detected as part of measles outbreak investigations. These countries need to follow-up pregnancy outcomes for the period of the outbreak, assess the magnitude of the CRS problem and decide the programme response.
Minimum requirements in the CRS prevention stage
Monthly routine reporting of suspected CRS cases with zero •
reporting (clinical and laboratory analysis should be conducted for all suspected CRS cases in children less than one year old).
Monthly routine reporting of suspected rubella cases.•
Investigation of all febrile rash illnesses in pregnant women.•
For a suspected rubella outbreak, 5-10 cases should be tested for •
rubella specific IgM. Active CRS case finding should be initiated for children less than one year old. It should continue for nine months after the last reported case of rubella.
Minimum requirements in the CRS/ rubella elimination stage
Infants with CRS are likely to be seen at specialty facilities that do not normally participate in the immunization service or the routine communicable disease surveillance system, e.g. eye hospitals, ENT hospitals, cardiothoracic hospitals etc. The data requirement for the CRS/ rubella elimination stage has the same requirements as the CRS prevention stage, plus the following:

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 63
Monthly routine reporting of confirmed rubella cases with zero •
reporting.
Case investigation for all suspected measles and rubella cases •
regardless of age with laboratory analysis of each case for measles IgM followed by rubella IgM if negative.
Priority case investigation for pregnant women with febrile rash •
illness.
Passive surveillance of CRS cases
CRS cases are likely to be underreported in areas and among populations where a high proportion of births occur at home and where infant deaths may not be reported. However, all suspected CRS cases that present to the outpatient clinic, emergency room, special clinics (ophthalmology, ENT, cardiology, cardiac surgery) and inpatient ward in health care facilities should be identified, reported and investigated. The CRS case investigation form (Form I) (22) should be completed and serum specimen collected and shipped to the laboratory as described in Chapter 11, “Role of laboratories in measles and rubella surveillance”.
Active surveillance of CRS cases at major hospitals
The surveillance focal person for the district should visit the hospital periodically to review inpatient registers, outpatient registers, clinic records, and log books for any possible CRS cases with special attention to the neonatal, paediatric, ophthalmology, ENT, cardiology and obstetric units.
Investigation of rubella outbreaks
Rubella outbreaks are usually detected during a measles outbreak investigation. Once rubella has been identified particular attention should be paid to women of childbearing age with laboratory testing of suspected cases and antenatal follow-up as necessary.
For suspected cases with negative rubella-specific IgM specimens •
during the first six days after rash onset, a second blood specimen should be collected and tested for rubella-specific IgM.
For laboratory-confirmed rubella infection during pregnancy, the •
patient should be tracked in a rubella pregnancy register with counseling and medical follow-up.
Infants born to women with confirmed rubella infection during •
pregnancy should be tested for rubella-specific IgM immediately after birth.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines64
Rubella outbreaks may continue over two or more years and smaller outbreaks may lead to larger ones.
Recommended data analyses, presentations and reports
Aggregated data from routine reporting
Number of CRS cases and incidence rate per 1,000 live births •
by month, year, and geographic area.
Number of rubella cases and incidence rates by month, year, •
and geographical area.
Age-specific, sex-specific, and district-specific rubella incidence •
rates.
Rubella vaccine coverage rates by target group and geographical •
area per year.
Completeness/timeliness of monthly reporting for CRS and rubella •
cases.
Proportion of laboratory confirmed rubella outbreaks.•
Case-based data from case investigations
Number of CRS cases by sex, month, year, and geographic •
area.
District specific CRS incidence rates per 1000 live births per •
year.
Age-specific, sex-specific and district-specific rubella incidence rates.•
Final classification of all suspected cases of CRS and rubella.•
Rubella immunization status for mothers of CRS cases.•
Proportion of febrile rash illness cases with rubella-specific •
IgM–positive laboratory investigations.
Surveillance quality
The surveillance quality indicators are the completeness and timeliness of routine reporting, notification, clinical investigation and laboratory investigation. In countries with low-incidence or in the elimination phase, performance indicators for rubella case investigation should be linked to measles case investigation.

Role of laboratories in measles and rubella surveillance
The laboratory has two main functions in measles and rubella surveillance.
Monitor and verify virus transmission:•
Confirm clinical diagnosis. –
Identify measles and rubella virus –
genotypes.
Confirm individual measles or rubella –
suspected cases.
Monitor the population’s susceptibility •
profile:
– Determine key characteristics of measles and rubella cases.
Eva l ua te t he impac t o f mass –
campaigns.
Chapter 11

Measles and Rubella Surveillance and Outbreak Investigation Guidelines66
The timing of sample collection with respect to the onset of clinical signs is important for interpreting results and arriving at an accurate conclusion. The number, place and type of samples to be collected for measles/rubella IgM antibody detection and virus isolation should be in accordance with the phase of measles/rubella control and elimination.
11.1 Collection, shipment and testing of specimens
All specimens collected should be documented using the standardized laboratory request form to include the following as a minimum:
Unique identifying number (in an agreed format);•
In-house laboratory number (assigned by the laboratory);•
Patient’s name; •
Age (or date of birth in standard notation);•
Province (or state); •
Town/district;•
Date of last measles and/or rubella vaccination;•
Date of onset of rash;•
Specimen type;•
Date of specimen collection; and•
Date specimen sent to laboratory.•
Specimens for serology
Timing of collection of blood specimen for detection of IgM
While IgM ELISA tests for measles and rubella are more sensitive between days 4 and 28 after the onset of rash, a single serum sample obtained at the first contact with the health care system at any time within 28 days after onset is considered adequate for surveillance purposes (24).However, during the first 72 hours after rash onset, the false negative rate maybe as high as 30% for measles-specific IgM and 50% for rubella-specific IgM. For sporadic cases, a second serum sample may be required under the following circumstances:
IgM specific assay is negative for a specimen collected within •
four days of rash onset; and
IgM specific assay repeatedly gives an equivocal result.•

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 67
A second specimen for IgM testing may be collected anytime between 4 and 28 days after rash onset. Specimens collected 10-20 days after the first specimen was collected will permit the laboratory to not only retest for IgM, but also conduct IgG quantitative analysis if possible.
Specimen kit for blood collection:
5-ml vacutainer (non-heparinized) tube with a 23 gauge needle •
or sterile disposable syringe and needle;
Tourniquet;•
Sterilizing swabs;•
Serum storage vials;•
Specimen labels;•
Band-aid;•
Zip-lock plastic bags;•
Specimen referral form; and•
Cold box with ice packs,•
Collection procedures
Collect 5 ml of blood by venepuncture using aseptic precautions. •
If vacutainer is used, label the vacutainer tube. If syringe is used to collect blood, transfer the blood from the syringe to labeled sterile screw capped vials (label with the patient identification and collection date).
The blood should be kept at room temperature until there is •
complete clot formation.
The clotted blood can be stored at 4 to 8° C for up to 24 hours •
before the serum is separated.
Do not freeze whole blood.•
Transportation of blood samples to the measles laboratory
If vacutainer is used, the same can be shipped directly to the WHO accredited laboratory in cold chain.
If a syringe is used to collect the blood sample, there are two options available to ensure that the specimen reaches the WHO accredited measles laboratory in good condition.
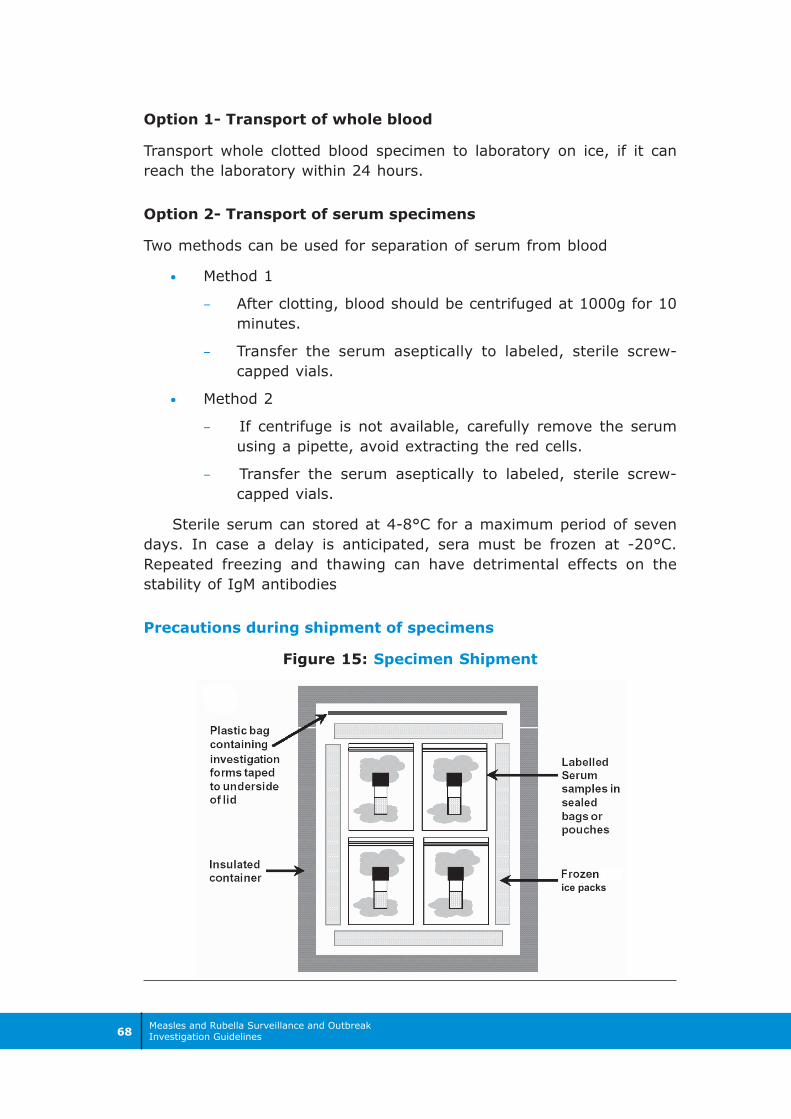
Measles and Rubella Surveillance and Outbreak Investigation Guidelines68
Option 1- Transport of whole blood
Transport whole clotted blood specimen to laboratory on ice, if it can reach the laboratory within 24 hours.
Option 2- Transport of serum specimens
Two methods can be used for separation of serum from blood
Method 1•
After clotting, blood should be centrifuged at 1000g for 10 –
minutes.
Transfer the serum aseptically to labeled, sterile screw- –
capped vials.
Method 2•
If centrifuge is not available, carefully remove the serum –
using a pipette, avoid extracting the red cells.
Transfer the serum aseptically to labeled, sterile screw- –
capped vials.
Sterile serum can stored at 4-8°C for a maximum period of seven days. In case a delay is anticipated, sera must be frozen at -20°C.Repeated freezing and thawing can have detrimental effects on the stability of IgM antibodies
Precautions during shipment of specimens
Figure 15: Specimen Shipment
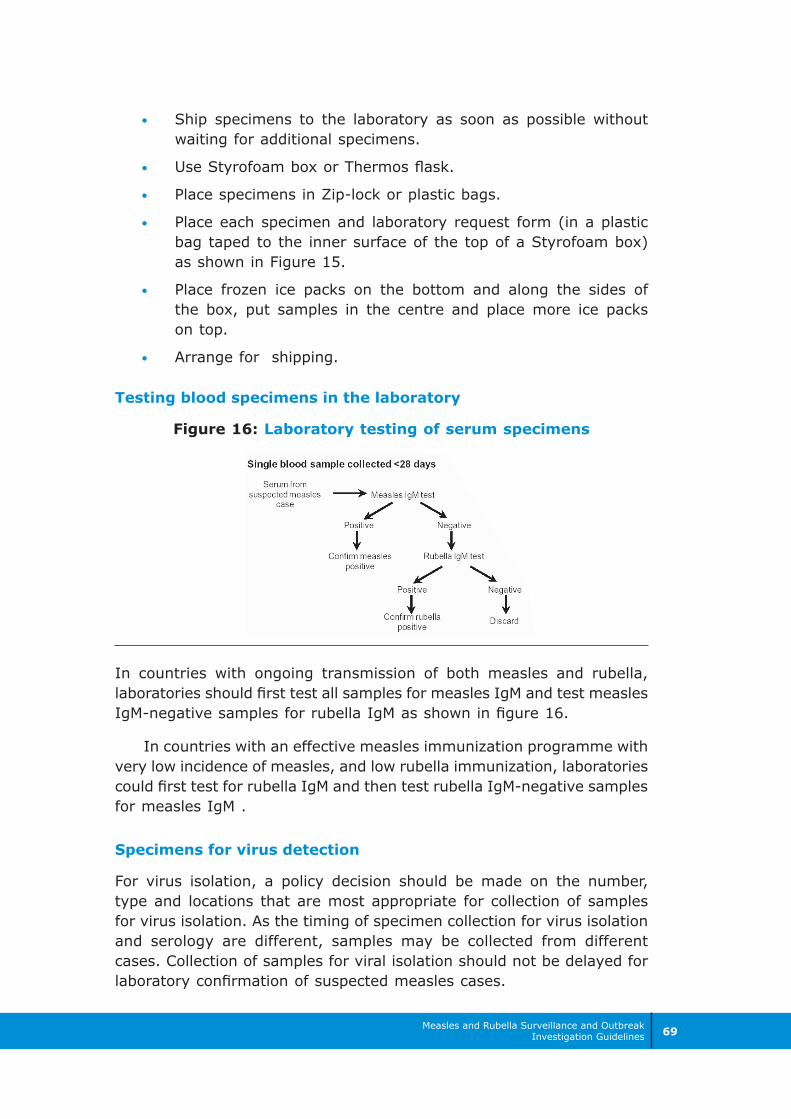
Measles and Rubella Surveillance and Outbreak Investigation Guidelines 69
Ship specimens to the laboratory as soon as possible without •
waiting for additional specimens.
Use Styrofoam box or Thermos flask.•
Place specimens in Zip-lock or plastic bags.•
Place each specimen and laboratory request form (in a plastic •
bag taped to the inner surface of the top of a Styrofoam box) as shown in Figure 15.
Place frozen ice packs on the bottom and along the sides of •
the box, put samples in the centre and place more ice packs on top.
Arrange for shipping.•
Testing blood specimens in the laboratory
Figure 16: Laboratory testing of serum specimens
In countries with ongoing transmission of both measles and rubella, laboratories should first test all samples for measles IgM and test measles IgM-negative samples for rubella IgM as shown in figure 16.
In countries with an effective measles immunization programme with very low incidence of measles, and low rubella immunization, laboratories could first test for rubella IgM and then test rubella IgM-negative samples for measles IgM .
Specimens for virus detection
For virus isolation, a policy decision should be made on the number, type and locations that are most appropriate for collection of samples for virus isolation. As the timing of specimen collection for virus isolation and serology are different, samples may be collected from different cases. Collection of samples for viral isolation should not be delayed for laboratory confirmation of suspected measles cases.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines70
The following are required for collection of specimens for virus isolation:
Sterile container for urine•
Throat swabs•
Virus transport medium/Virocult tubes•
Urine for measles virus isolation
Isolation of measles virus from a urine specimen is most successful if collected within five days after rash onset. A clean-catch 10 to 50ml urine specimen should be collected in a sterile container and stored at 4-8°C. Whole urine samples should be shipped within 24 hours of collection. DO NOT FREEZE whole urine specimens. If facilities are available, the specimen can be centrifuged at 500g (approximately 1500 rpm) at 4°C for five minutes, the supernatant should be discarded and the sediment re-suspended in 1ml viral transport medium (to be obtained from the laboratory). The re-suspended pellet may be stored at 4°C and shipped within 48 hours to a measles reference laboratory. If delay in shipment is anticipated the suspended pellet should be frozen at -70°C and shipped on dry ice in a well-sealed screw-capped vial.
Nasopharyngeal specimens for measles virus isolation
Nasopharyngeal specimens for virus isolation must be collected as soon as possible after the appearance of the rash. Nasopharyngeal specimens can be taken by aspiration, lavage or swabbing the mucous membranes.
Nasopharyngeal/ oropharyngeal swab is obtained by firmly rubbing the nasopharyngeal passage and back of the throat with sterile cotton swabs to dislodge epithelial cells (Figure 17). The swabs are placed in sterile viral transport medium in labelled, screw-capped tubes. (viral transport medium obtained from the laboratory can be stored at + 4°C for a month).
Shipment: Nasopharyngeal specimens should be transported on wet ice (4-8°C), and should arrive at the testing laboratory within 48 hours. If arrangements cannot be made for rapid shipment, swabs should be shaken in the virus transport medium and

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 71
removed. The medium or nasal aspirate should be centrifuged at 500g approximately 1500 rpm) at 4°C for five minutes. The resulting pellet should be re-suspended in cell culture medium. The suspended pellet and the supernatant are stored separately at -70°C and shipped to the testing laboratory on dry ice in well-sealed, screw-capped vials.
Alternate sampling: Oral fluids are easy to collect and non-invasive and have the added advantage that they can be used for viral genome detection and antibody detection. The decision to collect oral fluids should be taken in consultation with the programme managers and the laboratory.
Oral fluid is collected using special swab collection devices developed specially to collect crevicular fluid exuded from the interface between the gums and teeth. The swab should be used like a tooth brush and should be rubbed along the gums until the swab is thoroughly wet. It takes about a minute. The wet swab is placed in a clear transport tube that has an area to record the details of the specimens. Specific instructions given by the manufacturer of the swab should be followed. The sample should be kept refrigerated and transported on wet ice to the laboratory where possible though there is evidence that these samples are stable for up to one week at ambient temperature and are suitable for use where reverse cold chain is non-existent.
11.2 Measles and rubella laboratory network
The WHO Global measles/rubella Laboratory Network is organized in four levels
Sub-National Laboratories (SNL)• are established as the first or second administrative levels when the testing of specimens for measles may be beyond the capacity of a single national laboratory.
National Laboratories (NL)• are responsible for testing specimens from suspected cases by IgM enzyme-linked immunosorbent assay (ELISA) and report to the national programme managers.
Regional Reference Laboratories (RRL)• serve as reference laboratories for national laboratories in neighbouring countries and as national laboratories in their own countries. Each WHO Region may have up to three to four RRLs.
Global Specialized Laboratories (GSL)• are laboratories that set the technical standards for laboratory diagnosis. Their responsibilities extend to measles and rubella laboratories in all regions and countries.
Table 13 Outlines the role of the laboratories in the network
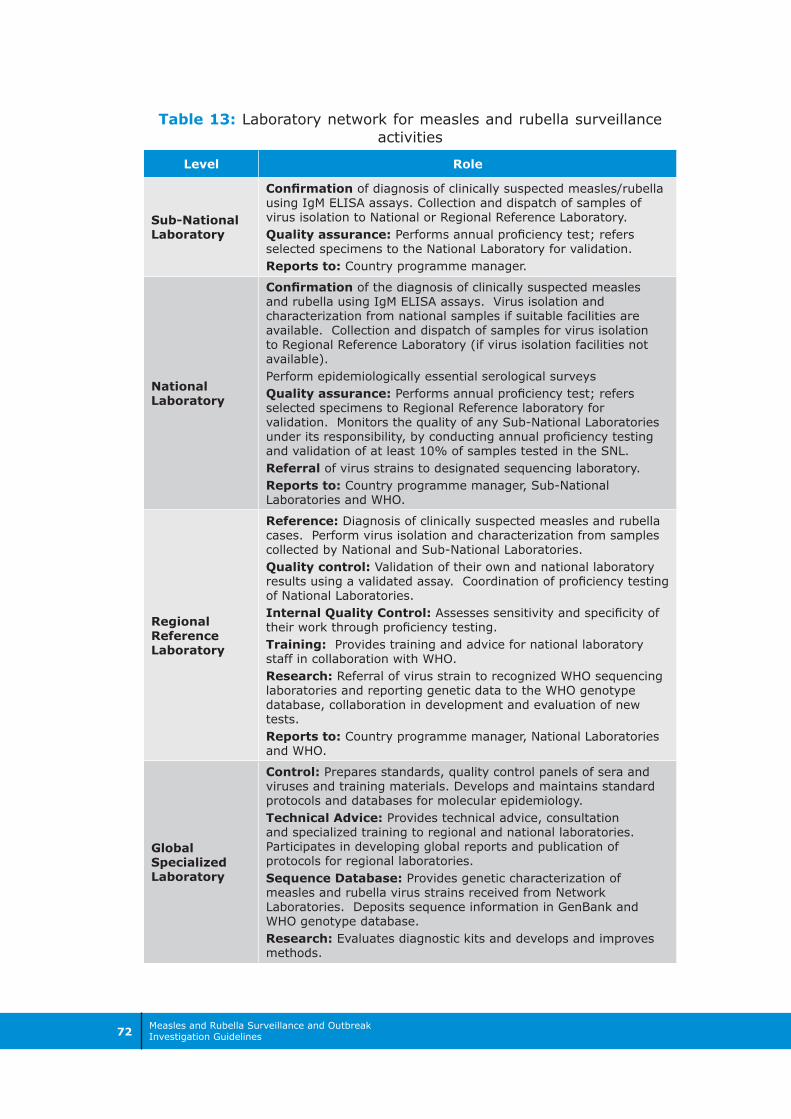
Measles and Rubella Surveillance and Outbreak Investigation Guidelines72
Table 13: Laboratory network for measles and rubella surveillance activities
Level Role
Sub-National Laboratory
Confirmation of diagnosis of clinically suspected measles/rubella using IgM ELISA assays. Collection and dispatch of samples of virus isolation to National or Regional Reference Laboratory.Quality assurance: Performs annual proficiency test; refers selected specimens to the National Laboratory for validation.Reports to: Country programme manager.
National Laboratory
Confirmation of the diagnosis of clinically suspected measles and rubella using IgM ELISA assays. Virus isolation and characterization from national samples if suitable facilities are available. Collection and dispatch of samples for virus isolation to Regional Reference Laboratory (if virus isolation facilities not available).Perform epidemiologically essential serological surveysQuality assurance: Performs annual proficiency test; refers selected specimens to Regional Reference laboratory for validation. Monitors the quality of any Sub-National Laboratories under its responsibility, by conducting annual proficiency testing and validation of at least 10% of samples tested in the SNL.Referral of virus strains to designated sequencing laboratory.Reports to: Country programme manager, Sub-National Laboratories and WHO.
Regional Reference Laboratory
Reference: Diagnosis of clinically suspected measles and rubella cases. Perform virus isolation and characterization from samples collected by National and Sub-National Laboratories.Quality control: Validation of their own and national laboratory results using a validated assay. Coordination of proficiency testing of National Laboratories.Internal Quality Control: Assesses sensitivity and specificity of their work through proficiency testing.Training: Provides training and advice for national laboratory staff in collaboration with WHO.Research: Referral of virus strain to recognized WHO sequencing laboratories and reporting genetic data to the WHO genotype database, collaboration in development and evaluation of new tests.Reports to: Country programme manager, National Laboratories and WHO.
Global Specialized Laboratory
Control: Prepares standards, quality control panels of sera and viruses and training materials. Develops and maintains standard protocols and databases for molecular epidemiology.Technical Advice: Provides technical advice, consultation and specialized training to regional and national laboratories. Participates in developing global reports and publication of protocols for regional laboratories.Sequence Database: Provides genetic characterization of measles and rubella virus strains received from Network Laboratories. Deposits sequence information in GenBank and WHO genotype database.Research: Evaluates diagnostic kits and develops and improves methods.

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 73
References
World Health Organization. GIVS : global immunization vision and (1) strategy: 2006-2015. Geneva: WHO, 2005. Document WHO/IVB/05.05. p.8. (http://www.who.int/immunization/givs/en/index.html - accessed 11 August 2009).
World Health Organization, Regional Office for South-East Asia. Twelfth (2) meeting of the SEAR technical consultative group for polio eradication and vaccine preventable diseases, 12-13 July 2007, New Delhi, India. New Delhi: WHO-SEARO, 2007. p.19. Document SEA-Polio-46.
World Health Organization, Regional Office for South-East Asia. SEAR 2008 (3) EPI fact sheet. New Delhi: WHO-SEARO, 2009 (http://www.searo.who.int/EN/Section1226/Section1229_13151.asp - accessed 11 August 2009).
Strebel P, Cochi S, Grabowsky M, Bilous J, Hersh BS, Okwo-Bele JM, (4) Hoekstra E, Wright P, Katz S. The unfinished measles immunization agenda. J Infect Dis. 2003 May 15;187 Suppl 1: S1-7.
Progress in global measles control and mortality reduction, 2000–2007. (5) Weekly epidemiological record. 2008; 83(40): 441-8. (http://www.who.int/wer/2008/wer8349.pdf - accessed 11 August 2009).
Sustainable Measles Mortality Reduction; Regional Strategic Plan 2007-(6) 2010 South-East Asia Region, July 2007
Ministry of Health and Family Welfare, Government of India. Measles (7) mortality reduction: India strategic plan 2005 – 2010. New Delhi.
World Health Organization, Regional Office for South-East Asia. SEAR, (8) 2007 measles EPI fact sheet. New Delhi: WHO-SEARO, 2007. (http://www.searo.who.int/vaccine/linkfiles/meavpd/mearub2007.pdf - accessed 11 August 2009).
World Health Organization, Regional Office for South-East Asia. Report (9) for Jul 1st to Sep 30th, 2007. Measles and rubella Quarterly Surveillance Bulletin. Vol. 1, No. 2 Published 07 November, World Health Organization, regional office for South-East Asia New Delhi. http://www.searo.who.int/vaccine/linkfiles/mslbulletin/measles_bulletin_q3_2007.pdf
World Health Organization, Regional Office for South-East Asia. Report for (10) Apr 1st to Jun 30th, 2007. Measles and Rubella Quarterly Surveillance Bulletin. 2007 Nov.; 1(1). (http://www.searo.who.int/vaccine/linkfiles/mslbulletin/measles_bulletin_q2_2007.pdf - accessed 11 August 2009).
Measles vaccines: WHO position paper. Weekly epidemiological record. 2004 (11) April 2; 79(14): 129–144. http://www.who.int/wer/2004/en/wer7914.pdf - accessed 11 August 2009).
WER:25,2008,83,225–232; http://www.who.int/wer/2008/wer8325.pdf(12)
World Health Organization. Module on best practices for measles (13) surveillance. Geneva: WHO, 2001. Document WHO/V&B/01.43. (http://www.who.int/vaccines-documents/DocsPDF01/www617.pdf - accessed 11 August 2009).
Measles and Rubella Surveillance and Outbreak Investigation Guidelines74
Field Guide - Measles Surveillance and Outbreak Investigation; September (14) 2006 Government of India Department of family welfare New Delhi
Word Health Organization. Response to measles outbreaks in measles (15) mortality reduction settings. Geneva: WHO, 2009. Document WHO/IVB/09.03. (http://whqlibdoc.who.int/hq/2009/WHO_IVB_09.03_eng.pdf - 11 August 2009).
Word Health Organization. Vitamin A supplements: a guide to their use in (16) the treatment and prevention of vitamin A deficiency and xerophthalmia. 2nd edition. Geneva: World Health Organization, 1997. (http://whqlibdoc.who.int/publications/1997/9241545062.pdf - accessed 11 August 2009).
Orenstein WA, Bernier RH, Dondero TJ, Hinman AR, Marks JS, Bart KJ, (17) Sirotkin B. Field-evaluation of vaccine efficacy. Bulletin of the World Health Organization. 1985; 63(6):1055–1068.
Word Health Organization. Revision of the international health regulations. (18) Geneva: WHO, 2005. Document WHA58.3. (http://www.who.int/gb/ebwha/pdf_files/WHA58/WHA58_3-en.pdf - accessed 11 August 2009).
Rubella vaccines: WHO position paper. Weekly Epidemiological Record. (19) 2000, 75(20): 161–172. (http://www.who.int/wer - accessed 11 August 2009).
World Health Organization. The immunological basis for immunization (20) series: module 11: rubella. Geneva: WHO, 2008. (http://whqlibdoc.who.int/publications/2008/9789241596848_eng.pdf - accessed 11 August 2009).
Cooper LZ. The history and medical consequences of rubella. Reviews (21) of infectious diseases. Rev Infect Dis. 1985 Mar-Apr; 7 Suppl 1:S2-10. And Dudgeon JA. Congenital rubella. Journal of pediatrics. 1975. 87(6): 1078—1086.
World Health Organization. WHO-recommended standards for surveillance (22) of selected vaccine-preventable diseases. Geneva: WHO, 2003. Document WHO/V&B/03.01. pp. 35-39. http://www.who.int/vaccines-documents/DocsPDF06/843.pdf - accessed 11 August 2009).
Cutts FT, Best J, Siqueira MM, Engstrom K, Robertson SE. Guidelines (23) for surveillance of congenital rubella syndrome and rubella: field test version, May 1999. Geneva, World Health Organization, 1999. Document WHO/V&B/99.22. (http://www.who.int/vaccines-documents/DocsPDF99/www9934.pdf - accessed 11 August 2009).
World Health Organization. Manual for the laboratory diagnosis of measles (24) and rubella virus infection. 2nd edition. Geneva: WHO, 2007. Document WHO/IVB/07.01. (http://www.who.int/immunization_monitoring/LabManualFinal.pdf - accessed 11 August 2009).

Annexes


Measles and Rubella Surveillance and Outbreak Investigation Guidelines 77
Genericlinelistforuseinroutinereportinginlowincidencecountries/provinces
Health
Facility:
District:
Note:
Ifdistrictsen
dsspecimen
sto
thelabo
ratory,u
sethesamecase
IDnu
mbe
rtoiden
tifythespecimen
.Form
described
onpage
23
* Exclude
dosesgiven14
days
before
onset.
**Indicate
howthevaccinationstatus
was
confirm
ed.i.e.,verballyor
was
avaccinationcard
seen
.
Outcome
A=alive
D=dead
Classification
Dateoflast
vaccination
Sourceof
vaccination
status
information**
Date
laboratory
specimen
taken
Resultsof
laboratory
testing
CASE
IDNum
ber
O=out-
patient
I=in-
patient
Nam
eVillage,Town,and
Neighbourhood
Sex
Dateof
Birth
Dateseen
athealth
facility
Dateonset
ofdisease
No.
vaccine
doses*
received
Form
ADate:

Measles and Rubella Surveillance and Outbreak Investigation Guidelines78
Gen
eric
line
listf
orus
edu
ring
mea
sles
outb
reak
sH
ealth
Faci
lity:
Out
brea
kid
:
Note:
Ifdistrictsen
dsspecimen
sto
thelabo
ratory,u
sethesamecase
IDnu
mbe
rtoiden
tifythespecimen
.Ex
clud
edo
sesgiven14
days
before
onset.
*** Indicate
howthevaccinationstatus
was
confirm
ed.i.e.,verballyor
was
avaccinationcard
seen
.
Dat
eof
Birt
h
Dat
eof
inve
stig
atio
nD
ate
onse
tof
dise
ase
No.
vacc
ine
dose
s*re
ceiv
edCA
SEID
Num
ber/
S.No
.
Villa
ge,T
own,
and
Nei
ghbo
urho
odSe
x
Out
com
eA
=aliv
eD
=dea
dN
K=N
otK
now
n
Cla
ssifi
catio
nD
ate
ofla
stva
ccin
atio
n
Sour
ceof
vacc
inat
ion
stat
usin
form
atio
n**
Dat
ela
bora
tory
spec
imen
take
n
Res
ults
ofla
bora
tory
test
ing
Form
BD
istr
ict:
Dat
e:
Form
desc
ribed
onpa
ge29
and
31
Nam
e

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 79
Nam
eoflocality:______________________________
Dateofsearch:________________
Search
done
by:__________________
District:______________________________________
Outbreakid_________________________
Fillup
informationofpersonssurveyed
TallyMark
Num
ber
TallyMark
Num
ber
TallyMark
Num
ber
Measles
Non-measles
Deathduetomeasles
Measles
Non-measles
Deathduetomeasles
Measles
Non-measles
Deathduetomeasles
Measles
Non-measles
Deathduetomeasles
Measles
Non-measles
Deathduetomeasles
Total
10-14years
4
>15years
Outbreakinvestigation:community
survey
1 5
<1year
21-4years
35-9years
Serial
Num
ber
Category
Num
berreceivedmeaslesvaccine
Unknownmeaslesvaccinationstatus
Age
Group
Num
bernotreceived
measlesvaccine
AddlFormB
Note:
Allpersonswho
presently
havemeaslesorintherecentpasthadmeaslesshouldbe
recorded
intheoutbreaklinelistformat.
Form
described
onpage
34

Measles and Rubella Surveillance and Outbreak Investigation Guidelines80
Add
ress
:___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
_State/
Prov
ince
:___
____
____
____
____
___
SubDistrict:_
____
____
____
__District:_
____
____
____
____
____
_Outbrea
kID:___
____
____
____
____
____
_
Years
Mon
ths
Mea
sles
Rub
ella
Datesp
ecim
ensse
nt:___
____
____
____
____
_
Nam
eof
person
send
ingthesp
ecim
ens:__
____
____
____
____
__
Add
ress
:___
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
____
Measles
labo
ratory
requ
esta
ndresu
ltform
foro
utbreaks
Dateof
rash
onse
tDateof
last
mea
sles
dose
Spec
imen
type
Spec
imen
colle
ction
date
Age
PartI:Caseinform
ation
Dateof
resu
ltTest
resu
ltSp
ecim
eniden
tification
numbe
rPa
tient
name
Sl.
No.
Form
C
Cas
eID
1 2 3 4 5 6 7 8 9 10
Form
describ
edon
page
29an
dpa
ge54
PartII:
tobe
filledou
tbyrece
ivinglabo
ratory
Datesp
ecim
ensrece
ived
:___
____
____
____
___
Rec
eiving
labo
ratory
name:__
____
____
____
___
Com
men
t:___
____
____
____
____
____
____
____
_
Sign
ature:
____
____
____
____
____
____
____
____

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 81
Outbreak ID: _______________________NotificationSource of notification: Weekly report / Active case search / Media / Other
Index case reported by:______________ Name of Surveillance focal person:___________________
Date of notification of index case: ______________ Designation:____________________
Village / Urban ward affected: _______________
Location of the outbreak
Health centre: ________________ Sub District: _______________________
District:______________________ State/ province: _______________________
Desk review: date________________________ findings________________________________________________________
Date/s of preliminary search:__________________________
Number of health facilities searched: ___________________
Number of areas* searched:__________________ Total number of clinically suspect measles cases:__________
Date of Outbreak Coordination Committee meeting: ____________________
Details of outbreak investigation
Date of pre outbreak investigation orientation:_______________________
Date of outbreak investigation From:________________ To:_______________
Number of health facilites involved:____________
Number of areas* involved:__________ Total population investigated:___________
Total number of measles cases:________ Total number of deaths due to measles:________
Date of onset of first case:________________ Date of onset of most recent case:__________
Laboratory investigation details
Date of lastmeaslesdose
Date ofSpecimencollectiontype
Date sentto lab
Datereceivedin lab
ResultMeasles/Rubella/Negative/Equivocal
Date ofResult
Note: * Areas are villages, urban units, named localities, towns or cities.
Preliminary investigation including desk review
Case ID
Form D Page 1/2Measles outbreak investigation summary
Sl.No.
12345678910
Age Sex

Measles and Rubella Surveillance and Outbreak Investigation Guidelines82
Dataanalysisofoutbreakinvestigation
OutbreakID:_________________________
Num
berof
measles
cases
received
measles
vaccine
Num
berof
measles
casesnot
received
measles
vaccine
Num
berof
measles
caseswith
unknown
vaccination
status
Num
berof
non-measles
received
measles
vaccine
Num
berof
non-measles
notreceived
measles
vaccine
Num
berof
non-measles
with
unknown
vaccination
status
Num
berof
deaths
dueto
measles
(Deathsmust
beincluded
incase
counts)
Total
population
Age
specific
attackrate
Age
wise
distributionof
measlescases(%)
Attackrate
amongnot
vaccinated
(ARU)
Attackrate
among
vaccinated
(ARV)
Vaccine
Efficacy(%)
CaseFatality
rate
(CFR)
AB
CD
EF
GH
=Sum(A:F)
J=
((A+B+C)/H)
*100
K=
(A+B+C)/(L+M+N)
*100
ARU=B/(B+E)
ARV
=A/
(A+D)
(ARU-ARV)/
ARU*100
CFR
=G/(A+B+C)
*100
<1year
1-4
years
5-9
years
10-14years
>=15years
Total
(L)
(M)
(N)
Any
otherrelevantdetails
Measlesoutbreakinvestigationsummary
Age
Group
Note:Colored
columns
tobe
completed
onlywhenpopulationdata(measlescasesandnoncases)iscollected.
Form
DPage
2/2
Form
described
onpage
36andpage
54

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 83
Dat
eR
epor
ted
Tota
lNum
bero
fRep
ortin
gU
nits
inC
ount
ry1
Num
bero
fUni
tsR
epor
ting
this
Mon
th1
Cas
esD
eath
sTe
sted
for
sero
logy
Sero
logy
+ve
mea
sles
Sero
logy
+ve
Rub
ella
Num
bero
fO
utbr
eaks
Num
bero
fca
ses
Num
bero
fO
utbr
eaks
Num
bero
fca
ses
Num
bero
fO
utbr
eaks
Num
bero
fca
ses
Col
umn:
12
34
56
78
910
1112
1314
1516
1718
1920
2122
2324
Janu
ary
Febr
uary
Mar
ch
Apr
il
May
June
July
Aug
ust
Sept
embe
r
Oct
ober
Nov
embe
r
Dec
embe
r
Tota
l
2AtLeast5bloodsamplesshouldbecollectedfromeachoutbreak.
Dat
ash
ould
been
tere
dan
dfo
rwar
ded
toSE
AR
OIV
DSu
rvei
llanc
eU
nit
byth
e15
thof
each
mon
th.Ea
chm
onth
lysu
bmis
sion
shou
ldin
clud
eup
date
dco
unts
fora
llpr
evio
usm
onth
s.
Num
bero
fC
ases
Adv
erse
Even
tsFo
llow
ing
Imm
uniz
atio
n(A
EFI)
Year
Mon
th
Agg
rega
teC
ase
Cou
nts
forO
ther
VPD
sFr
omA
llR
epor
ting
Sour
ces
Per-
tuss
isEn
ceph
-al
itis
Num
bero
fC
ases
Inve
s-tig
ated
Num
ber
ofD
eath
s
1ReportingcompletenessandtimelinesswillbedeterminedbythenumberofReportingUnitsreportingdatathismonth/totalnumberofReportingUnitsforthistimeperiod.
Lab
conf
irmed
Mix
edO
utbr
eaks
Rou
tine
Rep
ortin
gof
clin
ical
lysu
spec
tmea
sles
case
s
Cla
ssifi
catio
nof
Out
brea
ks2
Susp
ecte
dm
easl
esou
tbre
aks
Num
bero
fO
utbr
eaks
Num
ber
Inve
stig
ated
Num
ber
ofH
ospi
tal-
izat
ions
Lab
conf
irmed
Mea
sles
Out
brea
ksLa
bco
nfirm
edR
ubel
laO
utbr
eaks
Agg
rega
teR
epor
ting
ofVa
ccin
ePr
even
tabl
eD
isea
ses
from
Cen
tral
Leve
l
Mea
sles
&R
ubel
la Num
bero
fD
eath
s
Neo
-na
tal
Teta
nus
(NN
T)
Dip
h-th
eria
Num
ber
ofC
ases
ofA
EFI
Form
E
Form
desc
ribed
onpa
ge43
Cou
ntry
Electroniccopyofthisform
isavailablewith:
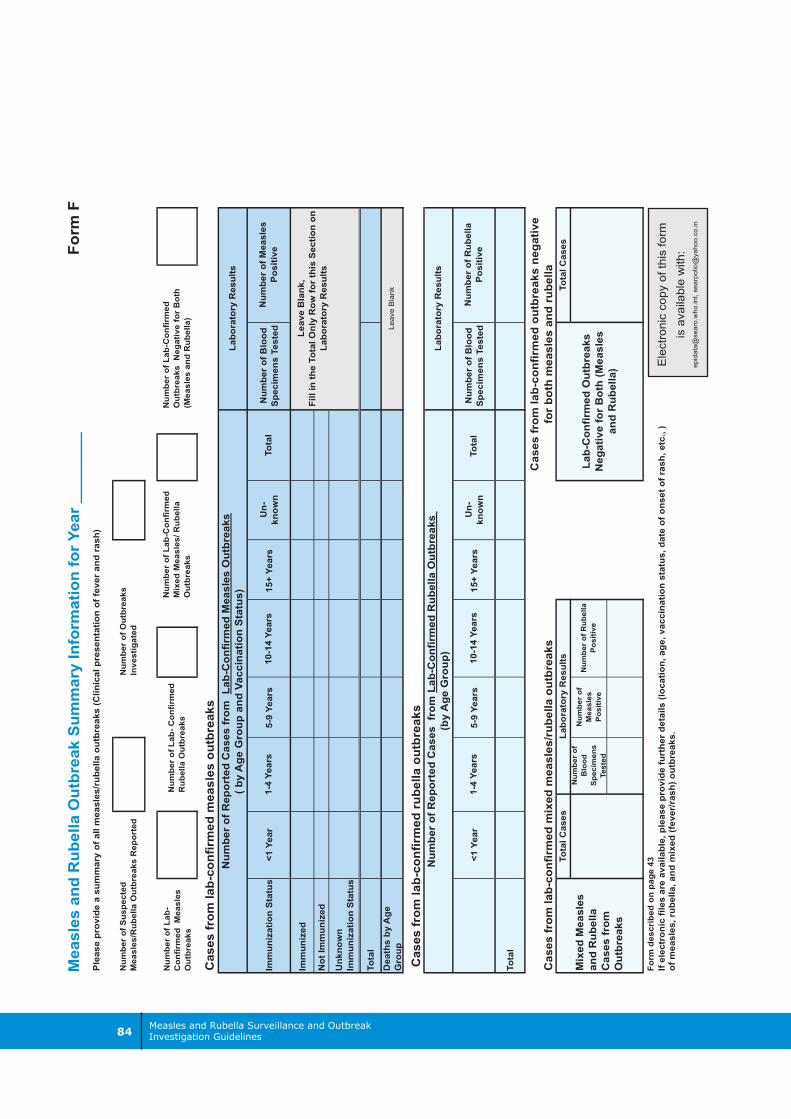
Measles and Rubella Surveillance and Outbreak Investigation Guidelines84
Num
berof
Lab-
Con
firmed
Measles
Outbreaks
ImmunizationStatus
<1Year
5-9Years
15+Years
Un-
know
nNum
berofBlood
SpecimensTested
Immunized
NotImmunized
Unknown
ImmunizationStatus
Total
Deathsby
Age
Group
<1Year
5-9Years
15+Years
Un-
know
nNum
berofBlood
SpecimensTested
Total
Num
berof
Blood
Specimens
Tested
Num
berof
Measles
Positive
Measles
andRubellaOutbreakSum
maryInform
ationforY
ear________
Pleaseprovideasummaryofallm
easles/rubellaoutbreaks(Clinicalpresentationoffeverandrash)
TotalC
ases
Cases
from
lab-confirmed
mixed
measles/rub
ellaou
tbreaks
Lab-Con
firmed
Outbreaks
NegativeforBoth(Measles
andRubella)
Cases
from
lab-confirmed
outbreaksnegative
forbo
thmeasles
andrubella
Cases
from
lab-confirmed
rubella
outbreaks
Num
berof
Suspected
Measles/Rub
ellaOutbreaks
Reported
Num
berof
Lab-Con
firmed
Outbreaks
NegativeforBoth
(Measles
andRub
ella)
Laboratory
Results
Num
berof
Lab-
Con
firmed
Rub
ellaOutbreaks
Num
berof
Lab-Con
firmed
Mixed
Measles/R
ubella
Outbreaks
Cases
from
lab-confirmed
measles
outbreaks
Num
berof
ReportedCases
from
Lab-Con
firmed
Measles
Outbreaks
(byAge
Group
andVaccinationStatus)
Total
Num
berof
Outbreaks
Investigated
Ifelectronicfiles
areavailable,please
providefurtherdetails
(location,age,vaccinationstatus,dateofonsetofrash,etc.,)
ofmeasles,rubella,and
mixed
(fever/rash)outbreaks.
Num
berofMeasles
Positive
10-14Years
Laboratory
Results
Num
berofRubella
Positive
1-4Years
Total
Num
berof
ReportedCases
from
Lab-Con
firmed
Rub
ellaOutbreaks
(byAge
Group
)
1-4Years
10-14Years
Mixed
Measles
andRub
ella
Cases
from
Outbreaks
TotalC
ases
Num
berof
Rub
ella
Positive
Laboratory
Results
LeaveBlank,
FillintheTotalO
nlyRow
forthisSectionon
Laboratory
Results
Leav
eB
lank
Form
F
Form
describ
edon
page
43E
lect
roni
cco
pyof
this
form
isav
aila
ble
with
:ep
idat
a@se
aro.
who
.int,
sear
polio
@ya
hoo.
co.in

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 85
Name of patient:________________________________________________________________Age (years):_______________________ Sex: M / FImmunized against measles ? YES / NO If yes, give date: ______/_____/_____Immunized against rubella ? YES / NO If yes, give date: ______/_____/_____Clinic where seen: _________________________________________________________________________________________________________________________________________Clinic record number: __________________________________________________________Address: ____________________________________________________________________________________________________________________________________________________________________________________________________________________________
Source :_________________________________________________________________________________________________________________________________________________Date of notificaton : ______/ _____/ ______Name of referring health worker :_________________________________________________Address of referring health worker :______________________________________________________________________________________________________________________________________________________________________________________________________Telephone number :___________________________________________________________
Fever? YES / NO If yes, date of onset: _____ / _____/ ____Generalized maculopapular(e.g. not vesicular) rash? YES / NO If yes, date of onset: _____/_____/______Duration:____________________________________________________________________
Conjuctivitis ? YES/ NO Coryza ? YES / NOCough ? YES / NO Lymph nodes swollen? YES / NOArthralgia/arthritis ? YES / NO Patient hospitalized for YES / NO
this illness ?If yes, name of hospital : _______________________________________________________________________________________________________________________________________________________________________________________________________________Pregnant ? YES / NO
If yes, due date : ____/ ____/ ____
If yes, where will delivery take place ? ____________________________________________
Notification
Clinical signs and symptoms
Form G Page 1/2Suspected measles/rubella case investigation form
Patient's identification Epid Number:

Measles and Rubella Surveillance and Outbreak Investigation Guidelines86
Epidemiological contact informationWas there contact with a suspected measles or rubella case in the month prior to rash onset ?_________ measles _________ rubella _________ no _________ unknownWas there a confirmed case of measles or rubell ain this area in the month prior to rashonset in this case?_________ measles _________ rubella _________ no _________ unknownTravel of the patient in the month prior to rash onset ?_________ Yes _________ no _________ unknownIf yes, describe where ?________________________________________________________Was patient in contact with a pregnant woman since developing symptioms ?_________ Yes _________ no _________ unknown
Date blood collected : _____/_____/_____Date serum sent to reference laboratory _____/____/______Name of reference laboratory : __________________________________________________Address ____________________________________________________________________Telephone __________________________________________________________________Measles IgM test result : Positive / Negative / Equivocal / Not DoneRubella IgM test result : Positive / Negative / Equivocal / Not DoneDengue IgM test result : Positive / Negative / Equivocal / Not DoneOther lab test resutls __________________________________________________________Date results received by investigator : _____/_____/_____Date patient informed of results : _____/_____/_____
______ laboratory-confirmed measles _________ laboratory-confirmed rubella______ Laboratory-confirmed dengue______ other ____________________________________________________________________ epidemiologically-confirmed _________ epidemiologically-confirmed
measles rubellaInvestigatorTitle : ______________________________________________________________________Address : ___________________________________________________________________Telephone : ________________________________ Date form completed ____/____/____
Laboratory tests
Final classification of case
Form G page 2/2Suspected measles /rubella caseinvestigation form (continued)
Form described in page 52
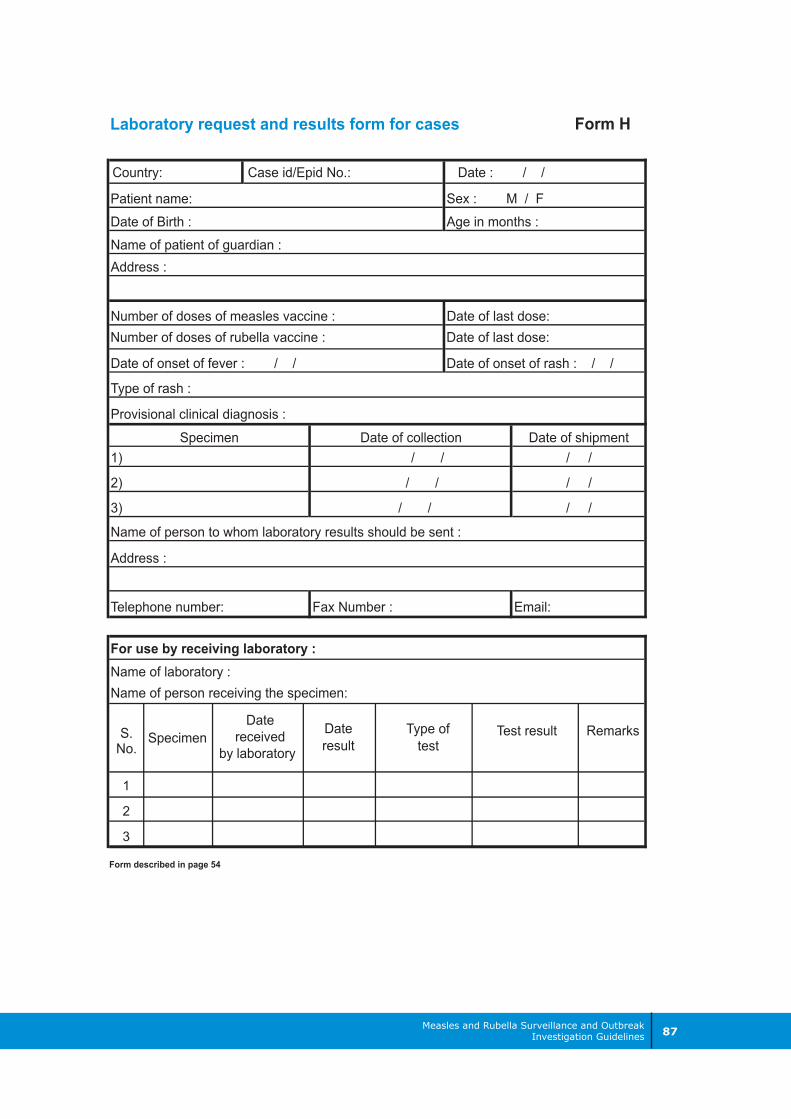
Measles and Rubella Surveillance and Outbreak Investigation Guidelines 87
Patient name:Date of Birth :
Date of onset of rash : / /
SpecimenDate
receivedby laboratory
Dateresult
Type oftest
Test result Remarks
For use by receiving laboratory :Name of laboratory :Name of person receiving the specimen:
Address :
Telephone number: Fax Number : Email:
Name of person to whom laboratory results should be sent :
1)
2)
3)
/ /
/ /
/ / / /
/ /
/ /
Specimen Date of collection Date of shipment
Date of onset of fever : / /
Type of rash :
Sex : M / FAge in months :
Name of patient of guardian :
Provisional clinical diagnosis :
Address :
Number of doses of measles vaccine : Date of last dose:
Country: Case id/Epid No.: Date : / /
Form HLaboratory request and results form for cases
Number of doses of rubella vaccine : Date of last dose:
Form described in page 54
S.No.
1
2
3

Measles and Rubella Surveillance and Outbreak Investigation Guidelines88
Sex: M / F Place infact delivered:______________________________________Hospital/clinic record number : __________________________________________________Name of mother: _____________________________________________________________Address: ____________________________________________________________________
Notified from :_____________________________________________________________________________________________________________________________________________Date of notificaton : ______/ _____/ ______Name of referring health worker :_________________________________________________Address of referring health worker :______________________________________________________________________________________________________________________________________________________________________________________________________Telephone number :___________________________________________________________
Group (a)Congenital heart disease : YES / NOIf yes, describe : ________________________________________________________________________________________________________________________________________
Cataract (s): YES / NO Glaucoma : YES / NOPigmentary retinopathy : YES / NO Hearing impairment: YES / NOGroup (b)Purpura : YES / NO Splenomegaly : YES / NOMicrocephaly : YES / NO Mental retardation : YES / NOMeningoencephalitis : YES / NO Radiolucent bone disese: YES / NOJaundice : YES / NOOther abnormalities : YES / NO
If yes, describle: ___________________________________________________________________________________________________________________________________________________________________________________________________________________Birth weight (grams): _____________________ if died, date of death: _____/_____/____Name of physician who examined infant: __________________________________________Address of Physician : ___________________________________________________________________________________________________________________________________Telephone : _______________________________ Date infant examined: ____/____/__
Infant's identification
Notification
Clinical signs and symptoms
Date of birth: ____/____/____Name of Child:_______________________________________________________________
Form I Page 1/2Congenital rubella syndrome caseinvestigation form

Measles and Rubella Surveillance and Outbreak Investigation Guidelines 89
Mother's age (years) ______________________ Number of previous pregnancies: ________Vaccinated against rubella ? YES / NO If yes, give date: ____/____/____
Travel during pregnancy ? YES / NO If yes, give month : __________________
If yes, describe where ____________________________________________________________________________________________________________________________________________________
Date blood collected : ____/____/____Date serum sent to rubella reference laboratory: ____/____/____Name of rubella reference laboratory: ____________________________________________Address: ___________________________________________________________________Telephone number :___________________________________________________________Type of IgM test (name of manufacturere) : ________________________________________Results : _________________________________________________________________________________________________________________________________________________________________________________________________________________________Date results received by investigator: ____/____/____Date family informed of results: ____/____/____
No laboratory test, but clinically consistent with CRS = Clnically-confirmed CRSPositive IgM + clinically-confirmed = Laboratory-confirmed CRSPositive IgM + no CRS manifestations = Congenital Rubella Infection (CRI)
Titles : _____________________________________________________________________Address : _________________________________________________________________________________________________________________________________________________________________________________________________________________________Telephone ; ________________________________ Date form completed; ____/____/____
Maternal history
Laboratory tests on infant
Investigator
Final classification of case
Maculopapular rash illness YES / NO If yes, give month : ________________with fever during pregnancy?If yes, was rubella laboratoryconfirmed in the mother?During the pregnancy was the mother exposedto any person (any age) withmaculopapular rashwith fever?
illness YES / NO If yes, give month: __________________
Form I page 2/2
Form described in page 63
Congenital rubella syndrome caseinvestigation form (continued)
YES / NO

