the use of computed tomography to determine femoral...
TRANSCRIPT
49 BulletinoftheHospitalforJointDiseases Volume63,Numbers1&2 2005
Abstract
Computed tomography is used to assess whether ideal femo-ral component size in knee arthroplasty can be made more accurately. Ideal femoral component size was measured on radiography, computed tomography, and by direct measurement of 20 cadaver femora and analyzed statistically. There was no significance between the tomographically anticipated ideal femoral component size and ideal femoral size values (Wilcoxon W 388.5; p 0.565). There was difference between radiographi-cally anticipated ideal femoral size and ideal femoral size values (Wilcoxon W 324.5; p 0.020). Anticipating the ideal femoral size can be made more precisely with computed tomography than radiographs in cadaver femora. Anticipating the ideal femoral component size by computed tomography may solve the problems in “in-between sizes.” Future total knee designs may be manufactured in more anatomic sizes.
Componentsizingisoneofthefactorsaffectingtheoutcomeinkneearthroplasty.1,2Inthetibiaandpa-tellaitisrelativelysimple.However,femoralsizing
hasaspecificfunction,which is itseffectonflexionand
extensiongaps.3Duringpreoperativeplanning, templatesareusedforanticipatingthefemoralcomponentsizefromradiographs.Howevermagnificationofbonystructuresinradiographs may mislead the surgeon.4 Definite femoralsizing ismadeby instruments during theoperation. It ismadebyreferencingeithertheposteriorfemoralcondyle(posteriorreferencing)oranteriorfemoralcondyle(anteriorreferencing).Theposteriorreferencesystemistherecom-mendedmethodforpreventingcomplications.3 Scans obtained in computed tomography (CT) aredescribed as scout-views and used for measurement ofdistancesandangleswithsoftwareprograms.5Precisemea-surementsinbonystructuresandimplantsizemeasurementscanbedonereliablyindentalsurgeryusingthequantitativepropertiesofCT.6Therefore,insearchofamoresensitiveandreliabletoolforpreoperativefemoralsizing,ananalysisoftheefficacyofusingCTmaybeuseful.
Materials and MethodsTwentycadaverfemurs(10rightand10left)wereincludedinthestudy.
Step 1Directtruelateralradiographsofthefemurweretakenpayingspecialattentiontotheconjunctionofthecon-tours of the posterior femoral condyles (PFC) on oneanother.7Theradiographicsettingswereasfollows:40kW,2.5mAs,44ms.Thedistancebetweenthebeamandthefemurwas1meter.Thesameoperator(MU)identi-fied the landmarks and made the measurements. ThemostposteriorpointofthePFCandtheanteriorfemoralcortexsuperiortoanteriorfemoralcondyle(AFC)weredetermined.Atangentlinetoanteriorfemoralcortexwasdrawn passing through theAFC.A perpendicular linefromthePFCtothetangentlinewasdrawnanditslengthwasdetermined inmillimetersbya rulerdesigned for
The Use of Computed Tomography to Determine Femoral Component SizeA Study of Cadaver Femora
Murad Uslu, M.D., Baris Ozsar, M.D., Tuba Kendi, M.D., Simay Kara, M.D., Ibrahim Tekdemir, M.D., and O. Sahap Atik, M.D.
Murad Uslu, M.D., is anAssociate Professor at the KirikkaleUniversity Medical Center, Department of Orthopaedics andTraumatology,Ankara,Turkey.BarisOzsar,M.D.,isaresidentintheDepartmentofOrthopaedicsandTraumatologyatKirikkaleUniversityMedicalCenter,Ankara,Turkey.TubaKendi,M.D.,isanAssistantProfessorintheDepartmentofRadiologyandRadio-diagnosticsatKirikkaleUniversityMedicalCenter,Ankara,Turkey.SimayKara,M.D.,isanAssociateProfessorintheDepartmentofRadiologyandRadiodiagnosticsatKirikkaleUniversityMedi-calCenter,Ankara,Turkey. IbrahimTekdemir,M.D.,ProfessorintheDepartmentofAnatomyattheAnkaraUniversityMedicalCenter,Ankara,Turkey.O.SahapAtik,M.D.,isaProfessorintheDepartmentofOrthopaedicsandTraumatologyatGaziUniversityMedicalCenter,Ankara,Turkey.Correspondence: Murad Uslu, M.D., Ozdoya Sitesi No 25,AlacaatliKoyu,Cayyolu,Ankara,06530Turkey.

50 Bulletinofthe HospitalforJointDiseases Volume63,Numbers1&2 2005
accuratemeasurementwithregardtothemagnificationpropertyofradiography(TemplateforOsteonics®Series7000 Total Knee, Printed in U.S.A, Osteonics Corp.,1994).Themeasurementsforeachfemurwererecordedasthe“radiographicallyanticipatedidealfemoralsize”(RAIFS)(Fig.1).
Step 2FemurswereplacedinthecenterofthegantryoftheCTmachineandlateralscansofthefemurweretakenpayingspecial attention toconjunctionof thecontoursof thePFCononeanotherandplacing the femoralcondylesin the center of the CT gantry. The scans were taken
withthefollowingsettings:120kvp,50mA,matrix512andlength500mm.Thesameoperator(TK)identifiedthe landmarks and made the measurements.The mostposterior point of the PFC and the anterior femoralcortexsuperiortoanteriorfemoralcondyle(AFC)weredetermined.A tangent line to anterior femoral cortexwas drawn passing through theAFC.A perpendicularline from the PFC to tangent line was drawn and itslength was determined in millimeters by CT process-ing.The measurements for each femur were recordedasthe“tomographicallyanticipatedidealfemoralsize”(TAIFS)(Fig.2).
Step 3Thefemoralsizingandanteriorfemoralresectionwasmade by using the total knee instrumentation system
Figure 1Directlateralradiographyofthedistalfemur.•Ante-riorfemoralcondyle(AFC).*Posteriorfemoralcondyle(PFC).Intermittantline:tangentlinetoanteriorfemoralcortexpassingthroughtheAFC.StraightlineperpendicularlinefromthePFCtothetangentline.Measurementofradiographicallyanticipatedidealfemoralsize(RAIFS)withregardtothemagnificationpropertyofradiographybyaruler.
Figure 2CTofdistalfemur.•Anteriorfemoralcondyle(AFC).*Posteriorfemoralcondyle(PFC).Intermittantline:tangentlinetoanteriorfemoralcortexpassingthroughtheAFC.StraightlineperpendicularlinefromthePFCtothetangentline.Measurementoftomographicallyanticipatedidealfemoralsize(RAIFS)byCTprocessing.
Figure 3Anteriorfemoralresectionwithpos-terior referencing.The stylus was lowered tothelateralanteriorcortexandatthispointtheindicatedsizewasnottakenintoconsiderationandtheresectionwasmadefromwhereverthestyluspointed.
51 BulletinoftheHospitalforJointDiseases Volume63,Numbers1&2 2005
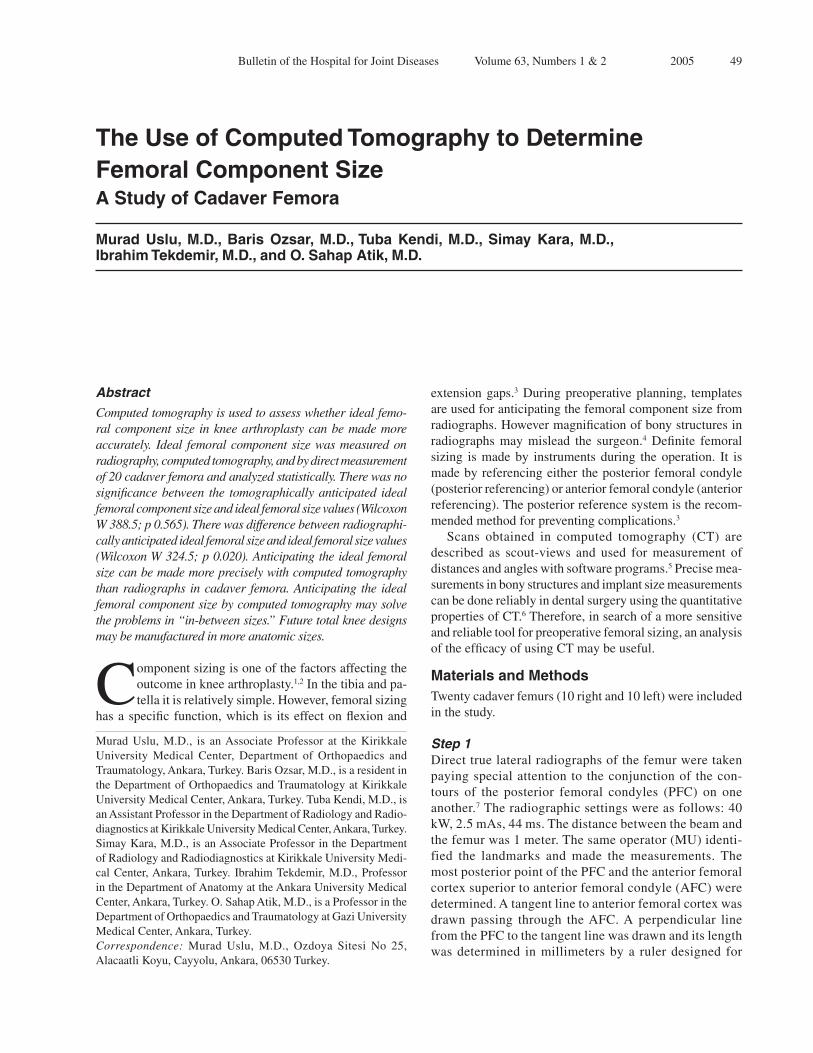
(Genesis2TotalKneeSystem,SmithandNephewInc.)by the authors (MU and BO). The femoral canal wasopenedwitha9.5mmdrillandan intramedullary rodwasplacedwithavalgusalignmentguideandthebushingpositionedtoeitherleftorrightside.Posteriorpaddlesofthevalgusalignmentguidewereincontactwiththeposteriorcondyles.Thefemoralsizingguideforposteriorreferencingwasattachedtothevalgusalignmentassem-bly.Thestyluswasloweredtothelateralanteriorcortexandanteriorfemoralresectionwasmade.Atthispointtheindicatedsizewasnottakenintoconsiderationandtheresectionwasmadefromwhereverthestyluspointed(Fig.3).ThedistancebetweentheanteriorcutsurfaceandthePFCwasmeasuredbydigitalcalipersandrecordedasthe“idealfemoralsize”(IFS)(Fig.4).
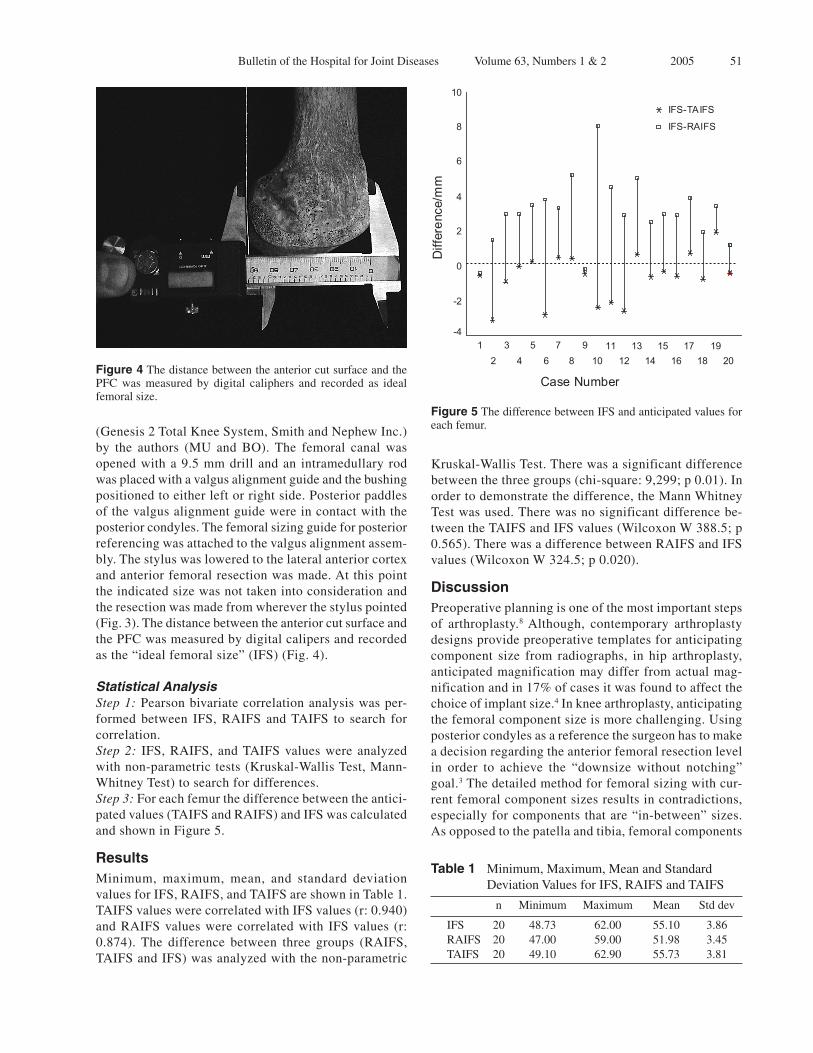
Statistical AnalysisStep 1:Pearsonbivariatecorrelationanalysiswasper-formed between IFS, RAIFS andTAIFS to search forcorrelation.Step 2: IFS,RAIFS,andTAIFSvalueswereanalyzedwithnon-parametrictests(Kruskal-WallisTest,Mann-WhitneyTest)tosearchfordifferences.Step 3:Foreachfemurthedifferencebetweentheantici-patedvalues(TAIFSandRAIFS)andIFSwascalculatedandshowninFigure5.
ResultsMinimum, maximum, mean, and standard deviationvaluesforIFS,RAIFS,andTAIFSareshowninTable1.TAIFSvalueswerecorrelatedwithIFSvalues(r:0.940)andRAIFSvalueswerecorrelatedwith IFSvalues (r:0.874). The difference between three groups (RAIFS,TAIFSandIFS)wasanalyzedwiththenon-parametric
Kruskal-WallisTest.Therewasasignificantdifferencebetweenthethreegroups(chi-square:9,299;p0.01).Inordertodemonstratethedifference,theMannWhitneyTestwasused.Therewasnosignificantdifferencebe-tweentheTAIFSandIFSvalues(WilcoxonW388.5;p0.565).TherewasadifferencebetweenRAIFSandIFSvalues(WilcoxonW324.5;p0.020).
DiscussionPreoperativeplanningisoneofthemostimportantstepsof arthroplasty.8Although, contemporary arthroplastydesignsprovidepreoperativetemplatesforanticipatingcomponent size from radiographs, in hip arthroplasty,anticipatedmagnificationmaydifferfromactualmag-nificationandin17%ofcasesitwasfoundtoaffectthechoiceofimplantsize.4Inkneearthroplasty,anticipatingthefemoralcomponentsizeismorechallenging.Usingposteriorcondylesasareferencethesurgeonhastomakeadecisionregardingtheanteriorfemoralresectionlevelin order to achieve the “downsize without notching”goal.3Thedetailedmethodforfemoralsizingwithcur-rentfemoralcomponentsizesresultsincontradictions,especiallyforcomponentsthatare“in-between”sizes.Asopposedtothepatellaandtibia,femoralcomponents
Table 1 Minimum,Maximum,MeanandStandardDeviationValuesforIFS,RAIFSandTAIFS
n Minimum Maximum Mean Stddev
IFS 20 48.73 62.00 55.10 3.86 RAIFS 20 47.00 59.00 51.98 3.45 TAIFS 20 49.10 62.90 55.73 3.81
Figure 4ThedistancebetweentheanteriorcutsurfaceandthePFC was measured by digital caliphers and recorded as idealfemoralsize.
Figure 5ThedifferencebetweenIFSandanticipatedvaluesforeachfemur.
Case Number
20 19
18 17
16 15
14 13
12 11
10 9
8 7
6 5
4 3
2 1
Diff
eren
ce/m
m
10
8
6
4
2
0
-2
-4
IFS-TAIFS
IFS-RAIFS

52 Bulletinofthe HospitalforJointDiseases Volume63,Numbers1&2 2005
havebeenfoundtodifferinsizein6.7%ofpatientsbe-tweenrightandleftkneesofthesamepatientundergoingbilateral knee replacement.9 For those reasons severalinvestigatorshavelookedforabettermethodtoestimatemagnificationandbonemorphologyofthedistalfemur.Macherandcolleaguesdemonstratedthatbonemodelscreatedbyanalysisofthree-dimensionalultrasoundim-agesareusefulforthesimulationofkneereplacements.10Menschandassociatesdevelopednomogramsforprecisepreoperative morphologic evaluation.7 However, theclinical validity of these methods is controversial. Inthecurrentstudy,bothTAIFSandRAIFSvalueswerecorrelatedwithIFS.HoweverthecorrelationofIFSwashigherwithTAIFSthanRAIFS.Inaddition,therewasnostatisticaldifferencebetweentheTAIFSandIFSvalues(p0.565).Thecurrentstudydemonstratesthatanticipat-ingtheidealfemoralsizecanbemademorepreciselywithCTscansthanradiographsincadaverbonesandCTscanscanbeusedasanalternativemethodforpreopera-tivesizeanticipation. Currentkneearthroplastydesignsuseanteroposterior(AP) height in the production of knee prosthesis andmediolateral (ML)width iscalculatedwithanAP/MLratioof0.8:1.0.11Anteroposteriorheighthasakeyrolein femoral sizing.The femoral components come in aspectrumofsizesandanteroposteriorsizesusuallyvarybetween3mmand5mm.Howevercontemporarydesignsdonotprovidesurgeonswiththeidealfemoralsizeinallcases.Thesurgeonisusuallyexpectedtotailorthefemuraccordingtothesizeofthepre-manufacturedprosthesis.Thisprocessmayrevealcomplicationssuchasanteriorfemoralnotchingorpatellafemoraldisordersat“inbe-tweensizes.”3Sizeincrementsincontemporaryfemoraldesignsdonotseemtoprovideanidealfitofprosthesistofemurinallcases.Intraoperativemeasurementofdistalfemursrevealsthatthereisaneedtogeneratefemoralcomponentsizesthataremorelikelytofitacrossthewidevariationofcases.11PrecisepreoperativedeterminationofAPheightmaycontributetotheefficacyofpreoperativeplanningandservethispurpose. Radiographshaveaseriousmagnificationproblemthatcannotbeeasilystandardized.Thissituationarisesfromthefactthattheradiographicimageisnotanexactpictureofthebone,butratheraprojectionofthebone.Andthisprojectionismagnifiedbyseveralvariablesintheprocess,likeobjectfilmdistance,focalfilmdistance,and object size. The magnification ratio in standardlateral knee radiographswas found tobe3.8% inonestudy.7 However, the standard measurement templatesare manufactured with a magnification ratio of 10%.ThismaybeoneofthefactorscausingtherelativelypoorcorrelationbetweenRAIFSandIFSvalues.Additionally,sinceX-rayshaveadivergingprojectiongeometry,mag-nificationratiosofmedialandlateralcondylesinlateralradiographsdifferandmaketheradiographicassessment
ofimplantsizemoredifficult.7 ACTscan isascoutviewanda two-dimensionalprojectionofathree-dimensionalstructurelikearadio-graph.However,inCTtheradiationsourcemovesatafixeddistancetothecenteroftheobject,whichisattheintersectionofthesagittalandfrontalplanes.Magnifica-tioninthecentraltomographicplanehasbeenreportedas1:1.5ThehighlycorrelatedTAIFSvalueswithidealfemoralcomponentsizesfoundinthecurrentstudysup-portthatthemagnificationinCTscansisminimalundercontrolledconditions.ClinicalstudiesmustbecarriedoutinordertofurtherresearchtherelevanceandutilityofCTinfemoralsizing. Anterior referencingorcutting the femur in3de-grees flexion are alternatives to femoral sizing usingposterior referencing systems in “in-between sizes.”Howeverthesesolutionsbringtheirowncomplicationswith them.Anterior referencing may result in flexioninstability.3,9 Cutting the femur in 3 degrees flexionmayresult inpost-impingementintheposteriorcruci-atesubstitutingsystems.3Manufacturing the“betweensize”femoralcomponentsmayprovidemorecongruousfemoral component implantation. In such a situation,precisepreoperativeanticipationof femoralsizesmayprovideadvantagetothesurgeonandthepatient.
ConclusionPreoperativeanalysisofCTscansandanticipatingtheidealfemoralcomponentsizemorepreciselymayhelptosolvetheproblems inherent inpatients that require in-betweensizedimplants.Ifprecisepreoperativemethodsforanticipat-ingcomponentsizeandtheirclinicaluseimprove,futureimplantdesignsmaybemanufacturedinawiderrangeofanatomicsizes.
AcknowledgmentWethankCumhurBoratav,M.D.,forhiskindassistanceinthestatisticalstudyofthisarticle.
References 1. TownleyCO:Theanatomictotalkneeresurfacingarthroplasty.
ClinOrthop1985;192:82-96.2. PFSharkey,HozackWJ,RothmanRH,ShastriS,JacobyMS:
Whyaretotalkneearthroplastiesfailingtoday?ClinOrthop2002;404:7-13.
3. ScottRD:Femoralcomponentsizing:Betwixtandbetween.Orthopedics2002;25(9):955.
4. KnightJL,AtwaterRD:Preoperativeplanningfortotalhiparthroplasty:Quantitatingitsutilityandprecision.JArthro-plasty1992;7suppl:403-9.
5. ChidiacJJ,ShoferFS,Al-KutoubiA,LasterLL,GhafariJ:Comparison of CT scanograms and cepholometric radio-graphs in craniofacial imaging. Orthod Craniofacial Res2002;5(2):104-13.
6. DixonDR,MorganR,HollenderLG,RobertsFA,O’NealRB:Clinicalapplicationofspiraltomographyinanteriorimplant

53 BulletinoftheHospitalforJointDiseases Volume63,Numbers1&2 2005
placement:Casereport.JPeriodontol2002;73(10):1202-9.7. MenschJS,AmstutzHC:Kneemorphologyasaguidetoknee
replacement.ClinOrthop1975;112:231-41.8. LaskinRS:Misconceptionsintotalkneereplacement.Ortho-
pedics2002;25:953.9. BrownTE,DiduchDR,MoskalJT:Componentsizeasym-
metry inbilateral totalkneearthroplasty.AmJKneeSurg2001;14(2):81-4.
10. MacherC,LiebingM,LazovicD,OverhoffHM:Pilotstudyoftotalkneearthroplastyplanningbyuseof3-Dultrasoundimagevolumes.StudHealthTechnolInform2000;77:1175-9.
11. KRChin,DFDaiury,DZurakowski,RDScott:Intraopera-tivemeasurementsofmaleandfemaledistalfemursduringprimarytotalkneearthroplasty.JKneeSurg2002;15(4):213-7.