patient questionnaires and formal education as more...
TRANSCRIPT

S29Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36
Medical care at this time is based largely on a paradigm known as a “biomedical model.”1-3 In this model, the causes, diagnosis, prognosis,
treatment, and outcomes of diseases are determined largely by physical or somatic variables (Table 1). Mind and body are distinct in the causation and outcomes of diseases. General health and the approach to disease are determined primarily, if not exclusively, by health professionals and the medical care system, with relatively little attention to the actions and behaviors of individual patients in health and disease. The use of a biomedical model has been spectacularly successful in medical and surgical advances in patient care over the last 50 years. Perhaps the most effective example is seen in antibiotic therapy of acute infectious diseases, in which a “cause” is identified through a microbiological culture, leading to rational treatment and a “cure,” if the host is intact. Similar successes, though not as dramatic, have been seen in pharmacologic treatment of hyperten-sion, gastroesophageal reflux and many other diseases, as well as surgical advances in coronary bypass, joint replace-ment and many conditions. A biomedical model also provides a primary foundation for understanding pathogenetic mechanisms in disease and advances in therapeutics. For example, biomedical research based on the discovery of rheumatoid factor in 19484 led to development of biological therapies for patients with rheumatoid arthritis (RA), which have provided major advances for rheumatologists and their patients. Further laboratory-based research according to a biomedical model clearly is a prerequisite to future advances in prevention and therapy of diseases.
Nonetheless, despite its critical importance to advances in medical care, a biomedical model has many limitations to understand health in general and the course and outcomes of chronic diseases, which account for most medical in-terventions at this time. A biomedical model presents an oversimplification, even in situations in which it appears most useful. For example, although an individual who has tuberculosis clearly has tubercle bacilli as a “cause,” the same dose of tubercle bacilli may initiate a wide spectrum of responses in different individuals, ranging from no disease to death. Therefore, even in the simplest case, one cannot identify a single “cause” of disease. How much more so is this seen in diseases in which “causes” have yet to be identified? A complementary approach to a biomedical model of health and disease may be termed a “biopsychosocial mod-el” (Table 1),1,5 in which mind and body are not independent in health and disease, particularly in the development and course of chronic diseases. In a biopsychosocial model, disease results from multifactorial “causes,” including external agents and events, internal genetic and dysregula-tory processes, and psycho-socio-economic variables rather than a single “cause” based on a “reductionist” approach. It is recognized that the patient history contributes to most di-agnoses as much or more than laboratory tests, radiographs, MRI scans, and other high technology information, and that 70% to 80% of encounters of patients with physicians are not explained by physical examination, imaging studies, or laboratory tests.6 A biopsychosocial model considers that health and disease outcomes are determined as much by the individual as by health professionals and the medical care system. Although the potential value of a biopsychosocial model is recognized by many observers, including many physi-cians, a biomedical model paradigm continues to dominate medical education, medical care, and medical policy.3,7,8
Patient Questionnaires and Formal Education as More Significant Prognostic Markers than Radiographs or Laboratory Tests for Rheumatoid Arthritis MortalityLimitations of a Biomedical Model to Predict Long-Term Outcomes
Theodore Pincus, M.D.
Theodore Pincus, M.D., is with the NYU Hospital for Joint Dis-eases, New York, New York.Correspondence: Theodore Pincus, M.D., 301 East 17th Street, New York, New York 10003; [email protected].
Pincus T. Patient questionnaires and formal education are more significant prognostic markers than radiographs or laboratory tests for rheumatoid arthritis mortality: limitations of a biomedical model to predict long-term outcomes. Bull NYU Hosp Jt Dis. 2007;65(Suppl 1):S29-36.

Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36S30
One explanation is the continued daily reinforcement of its value in clinical activities at acute-care oriented inpatient medical centers, the setting of more than 95% of medical education, training, and clinical research. In these settings, an acute somatic problem is a prerequisite to hospital admission. Health professionals are responsible for inter-ventions and results. The patient has a minimal role in the process and outcomes of care. Even the patient’s regular medications generally are administered by a nurse or aide (rather than by the patient) in an inpatient hospital. A second explanation for continued dominance of a biomedical model and limited attention to a biopsychoso-cial model may result from relatively few reports that both document the value of biopsychosocial data and include extensive rigorous biomedical data. Many concepts con-cerning assessment, prognosis, and outcomes according to a biopsychosocial model may be correct, but not necessarily (yet) supported by data from clinical care and other clinical research. However, recent clinical research concerning RA supports the potential value of a biopsychosocial model to explain the prognosis and course of disease in individual patients, using the rigorous statistical methods associ-ated with research conducted according to a biomedical model.2,9-21
Three observations concerning RA that are explained more effectively by a biopsychosocial model than by a biomedical model include:
1. RA is associated with increased mortality rates, al-though the acute causes of death are similar to those seen in the general population.9,10,22-24
2. Data from patients concerning functional status are of greater prognostic significance for premature death of patients with RA than currently available laboratory tests, radiographs, and other imaging data.10,12-15,17,18,25
3. Formal education level is also of greater prognostic significance for long-term mortality than laboratory or radiographic data.8,13,19-21,26
Some of the evidence to support these statements is sum-marized briefly below.
Premature Mortality in RAPremature mortality in RA was reported initially during the 1950s, but not widely appreciated until the 1980s.9,10,14,22,23 Recognition of this premature mortality in RA required longitudinal analysis of its natural history over 5 to 20 years, in which RA patients were found to have a shortened life span by 5 to 15 years, compared to individuals matched for age and sex in the general population (Fig. 1). One basis for limited recognition of premature mortality in RA in the past is that the acute attributed causes of death generally are similar to those in the general population (Table 2).9 Among 2262 deaths reported prior to 1986 from 13 sites in Western Europe and the US, 42% were attributed to cardiovascular disease, compared to 41% in the general US population. Although acute, attributable causes of death in patients with RA were higher for infection, renal disease, pulmonary disease, gastrointestinal disease, and RA itself, the overall pattern is similar to the general population (Table
Table 1 Biomedical and Biopsychosocial Model Summary
Biomedical Model Biopsychosocial Model
Cause Each disease has a single “cause” Disease etiology is multifactorial: external pathogens, toxins, and internal host milieu, genes, behavior, social support
Diagnosis Identified primarily through laboratory tests, A patient medical history provides 50% to 90% radiographs, scans; information from patients of of the information needed to make many, perhaps value primarily (or only) to suggest appropriate tests most, diagnoses
Prognosis Also established most accurately on the basis of Information provided by patients often is the most information from high technology sources, rather valuable data in establishing a prognosis than from a patient
Treatment Involves only actions of health professionals, Must involve patient, family, social structure e.g., medications, surgery
Outcome Health and disease outcomes are determined primarily Health and outcomes of chronic diseases are by decisions and actions of health professionals determined as much by actions of individual patients as by health professionals
Table 2 Attributed Causes of Death in 2262 RA Patients in 13 Series from Diverse Locales Compared to the General Population8
Attributed Cause Percent of Percent of 1977 of Death RA Deaths US Deaths
Cardiovascular Disease 42.1% 41.0%Cancer 14.1% 20.4%Infection 9.4% 1.0%Renal Disease 7.8% 1.1%Pulmonary Disease 7.2% 3.9%RA 5.3%GI Disease 4.2% 2.4%CNS Disease 4.2% 9.6%Accidents 1.0% 5.4%Miscellaneous 6.4% 15.2%Unknown 0.6%

S31Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36
2). At this time, there exists some understanding concerning a predisposition of patients with RA to cardiovascular and other comorbidities, so that premature death may be regarded as emerging from pathogenetic mechanisms in RA.27
Patient Questionnaires Rather Than Laboratory Tests, Radiographs, and Other High Technology Data are the Most Significant Prognostic Markers for Severe Long-Term Outcomes of Rheumatoid Arthritis, Including Premature Mortality and Work Disability In a traditional biomedical model, markers to predict disease outcomes are derived from data assessed by health profes-sionals: blood pressure, serum creatinine, cholesterol, a
mass on a chest radiograph, and many others. However, the most significant marker to predict premature mortality over 5 years in patients with RA is a score for functional capacity in activities of daily living on a patient questionnaire rather than a laboratory test, radiograph, or other high-technology information (Fig. 2A).10,12,14,15,17,18,25
In a study of patients who had an extensive baseline evaluation in 1973 and were reviewed 9 years later in 1982, patient responses regarding their capacity to perform usual activities, such as dressing, bathing, arising, and eating, were more effective at predicting mortality 9 years later than any known clinical measure, including data from the laboratory or radiographs. Patients with poor clinical status were 3 to 7.5 times more likely to die over the next 5 to 15
Figure 1 Survival of patients with rheumatoid arthritis versus expected survival in ten locales.
Figure 2 Nine to ten year survival ac-cording to quantitative markers in three chronic diseases.

Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36S32
years than patients with favorable clinical status (Table 3),18 risks at least as great as those seen in cardiovascular disease for blood pressure and cholesterol.18
Mortality rates in certain patients with severe RA over 5 to 10 years were in ranges seen in patients with cardiovascular and neoplastic diseases (Fig. 2).9,18,28-30 Patients who could perform fewer than 80% of activities of daily living “with ease,” according to a questionnaire (Fig. 2A), experienced 5-year survival of about 50%, in the range of patients with Stage IV Hodgkin’s disease30 (Fig. 2C) or three-vessel coro-nary artery disease (Fig. 2D).29 A smaller proportion of RA patients were in the poorest prognostic category compared to patients with cardiovascular or neoplastic diseases, and many patients with coronary artery disease and Hodgkin’s Disease were studied earlier in the disease course than the patients with RA. Nonetheless, certain patients with RA have a poor prognosis for survival comparable with relative risks of 3:1 for death comparable to elevated blood pressure, cholesterol, or smoking in cardiovascular disease (Table 3), recognized primarily through patient questionnaires. The observation that patient questionnaires are an optimal
prognostic marker for mortality in RA has been replicated in many studies.12-15,25,31 For example, a cohort of patients was established in 1985, designed to confirm and extend the ear-lier findings noted above that patient functional status was a significant predictor of mortality in patients with a baseline in 1973. The cohort with a 1985 baseline was assessed according to state-of-the-art measurements of clinical status, including a 68-joint count, Sharp radiographic score, and laboratory stud-ies to assess the shared epitope and in vitro rheumatoid factor production. In a review 5 years later, all clinical measures were found to indicate poorer status in patients who would not survive the 5-year period compared to survivors, as might be expected, although it may be regarded as an advance to express poor versus good clinical status in quantitative rather than qualitative, “Gestalt” terms (Table 4).31 The three independent predictors of mortality over 5 years in Cox regressions were age, co-morbidities, and functional status according to a modified health assessment question-naire (MHAQ) (Table 5).31 All subsequent studies of predic-tors of mortality in RA which include a patient self-report questionnaire indicate that questionnaire scores for physical function—rather than a joint count, radiographic score, or laboratory test—provide the most significant predictor among clinical measures over 5 years.10,13,15,17,18,31-33 Fur-thermore, patient questionnaire data are the most significant predictors of other severe long-term outcomes, including functional status,10,34 work disability,35-37 costs,38 and joint replacement surgery.39
Formal Education Level Predicts Morbidity and Mortality of Rheumatoid Arthritis, Independent of Race, Age, and Other Variables, Suggesting a Possible Role for Self-Management in a Biopsychosocial Model of Chronic DiseaseIn analyses of survival of RA patients in the cohort analyzed over 9 years from 1973 to 1982, a second significant predic-tor of morbidity and mortality was formal education level (Fig. 2B).19 Survival over 9 years was about 95% in patients with more than 12 years of education, compared to about 80% in patients with 9 to 12 years of formal education, and 65% in patients with fewer than 8 years of education (Fig. 2B).19 In addition, declines were seen in functional status
Table 3 Relative Risk of Death Over 12 to 15 Years in Rheumatoid Arthritis and Cardiovascular Disease, According to Baseline Severity Indicators
• Rheumatoid Arthritis (75 pts, 15 years)17
Functional status on patient questionnaire Less than vs. greater than 91.5% “with ease” 2.9:1 Number of involved joints Greater than vs. less than 18 joints 3.0:1• Cardiovascular disease (312,000 pts, 12 years)* Serum cholesterol Greater or equal to 245 vs. less than 182 mg/Dl 2.9:1 Systolic blood pressure Greater or equal to 142 vs. less than 118 mmHg 3.0:1 Diastolic blood pressure Greater or equal to 92 vs. less than 76 mmHg 2.9:1 Smoking Greater or equal to 26 vs. 0 cigarettes/day 2.9:1 Data adjusted for age, sex, education, disease duration*Neaton et al, Arch Int Med 152:56,1992.
Table 4 Predicting Mortality in RA: Most Baseline Measures Are Worse in Patients Who Will Die Over a 5-Year Period29
Mean Baseline Values Alive Dead P Value
Age (years) 55.1 65.5 < 0.001ARA Functional Class (1-4) 2.2 2.6 < 0.001Number of Comorbidities 1.1 2.1 < 0.001Walking Time (sec) 10.8 16.8 < 0.001ESR (mm/hr) 33.8 48.3 0.004mHAQ Score (0-3)* 0.98 1.32 0.005Learned Helplessness (1-4) 2.41 2.55 0.007Global Self-Report (1-4) 2.6 3.0 0.01Number of Extra-Articular Features 0.2 0.5 0.02Duration of Disease (years) 9.1 12.7 0.03Years of Education 10.8 9.4 0.03Joint Count (0-66) 12.8 15.9 0.04Radiographic Score (0-4) 1.2 1.4 0.20Log RF Titer (0-12) 2.7 2.9 0.28Pain Score (0-10) 5.40 5.19 0.68
*Data changed from 1-4 in original report to 0-3 here reflects change in scoring since 1999.31
S33Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36
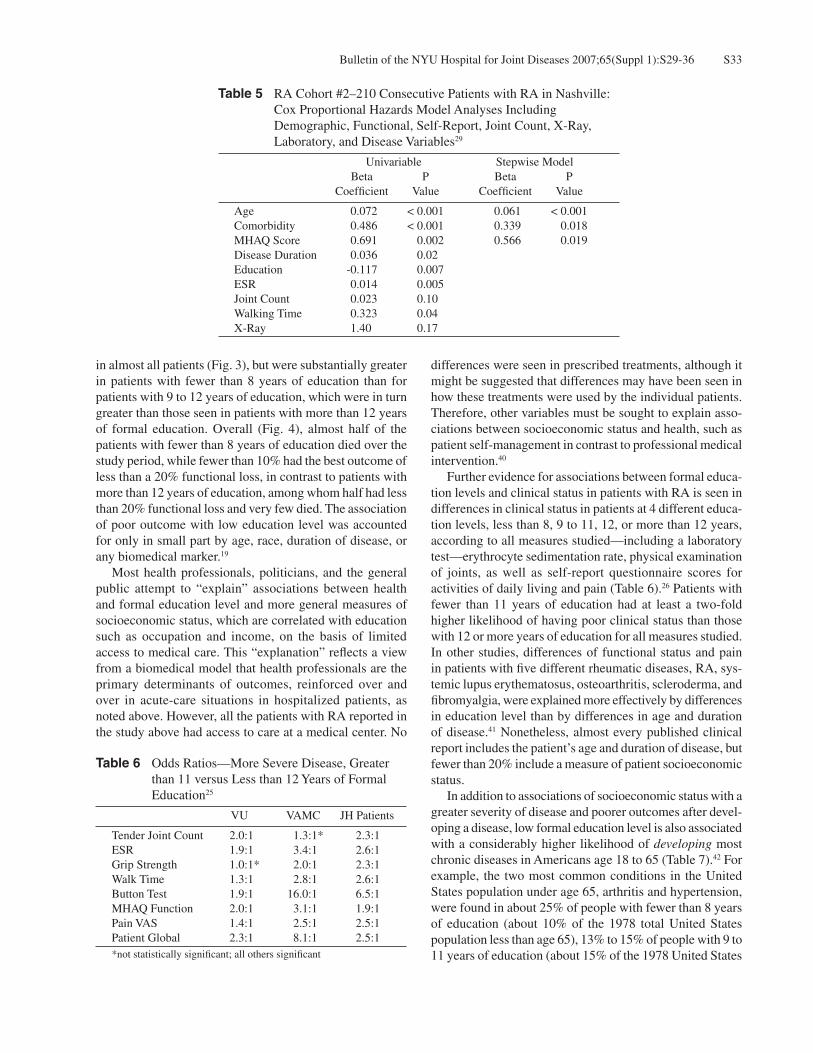
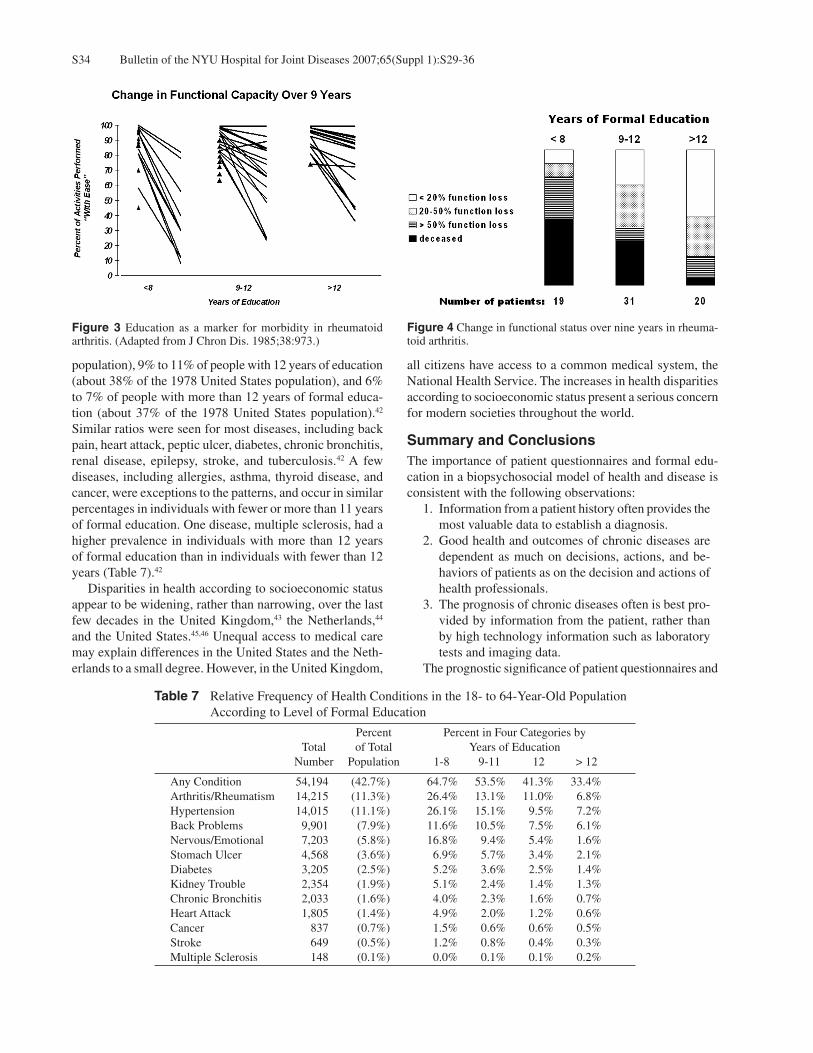
in almost all patients (Fig. 3), but were substantially greater in patients with fewer than 8 years of education than for patients with 9 to 12 years of education, which were in turn greater than those seen in patients with more than 12 years of formal education. Overall (Fig. 4), almost half of the patients with fewer than 8 years of education died over the study period, while fewer than 10% had the best outcome of less than a 20% functional loss, in contrast to patients with more than 12 years of education, among whom half had less than 20% functional loss and very few died. The association of poor outcome with low education level was accounted for only in small part by age, race, duration of disease, or any biomedical marker.19
Most health professionals, politicians, and the general public attempt to “explain” associations between health and formal education level and more general measures of socioeconomic status, which are correlated with education such as occupation and income, on the basis of limited access to medical care. This “explanation” reflects a view from a biomedical model that health professionals are the primary determinants of outcomes, reinforced over and over in acute-care situations in hospitalized patients, as noted above. However, all the patients with RA reported in the study above had access to care at a medical center. No
differences were seen in prescribed treatments, although it might be suggested that differences may have been seen in how these treatments were used by the individual patients. Therefore, other variables must be sought to explain asso-ciations between socioeconomic status and health, such as patient self-management in contrast to professional medical intervention.40
Further evidence for associations between formal educa-tion levels and clinical status in patients with RA is seen in differences in clinical status in patients at 4 different educa-tion levels, less than 8, 9 to 11, 12, or more than 12 years, according to all measures studied—including a laboratory test—erythrocyte sedimentation rate, physical examination of joints, as well as self-report questionnaire scores for activities of daily living and pain (Table 6).26 Patients with fewer than 11 years of education had at least a two-fold higher likelihood of having poor clinical status than those with 12 or more years of education for all measures studied. In other studies, differences of functional status and pain in patients with five different rheumatic diseases, RA, sys-temic lupus erythematosus, osteoarthritis, scleroderma, and fibromyalgia, were explained more effectively by differences in education level than by differences in age and duration of disease.41 Nonetheless, almost every published clinical report includes the patient’s age and duration of disease, but fewer than 20% include a measure of patient socioeconomic status. In addition to associations of socioeconomic status with a greater severity of disease and poorer outcomes after devel-oping a disease, low formal education level is also associated with a considerably higher likelihood of developing most chronic diseases in Americans age 18 to 65 (Table 7).42 For example, the two most common conditions in the United States population under age 65, arthritis and hypertension, were found in about 25% of people with fewer than 8 years of education (about 10% of the 1978 total United States population less than age 65), 13% to 15% of people with 9 to 11 years of education (about 15% of the 1978 United States
Table 5 RA Cohort #2–210 Consecutive Patients with RA in Nashville: Cox Proportional Hazards Model Analyses Including Demographic, Functional, Self-Report, Joint Count, X-Ray, Laboratory, and Disease Variables29
Univariable Stepwise Model Beta P Beta P Coefficient Value Coefficient Value
Age 0.072 < 0.001 0.061 < 0.001Comorbidity 0.486 < 0.001 0.339 0.018MHAQ Score 0.691 0.002 0.566 0.019Disease Duration 0.036 0.02Education -0.117 0.007ESR 0.014 0.005Joint Count 0.023 0.10Walking Time 0.323 0.04X-Ray 1.40 0.17
Table 6 Odds Ratios—More Severe Disease, Greater than 11 versus Less than 12 Years of Formal Education25
VU VAMC JH Patients
Tender Joint Count 2.0:1 1.3:1* 2.3:1ESR 1.9:1 3.4:1 2.6:1Grip Strength 1.0:1* 2.0:1 2.3:1Walk Time 1.3:1 2.8:1 2.6:1Button Test 1.9:1 16.0:1 6.5:1MHAQ Function 2.0:1 3.1:1 1.9:1Pain VAS 1.4:1 2.5:1 2.5:1Patient Global 2.3:1 8.1:1 2.5:1*not statistically significant; all others significant
Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36S34
Figure 3 Education as a marker for morbidity in rheumatoid arthritis. (Adapted from J Chron Dis. 1985;38:973.)
Figure 4 Change in functional status over nine years in rheuma-toid arthritis.
population), 9% to 11% of people with 12 years of education (about 38% of the 1978 United States population), and 6% to 7% of people with more than 12 years of formal educa-tion (about 37% of the 1978 United States population).42 Similar ratios were seen for most diseases, including back pain, heart attack, peptic ulcer, diabetes, chronic bronchitis, renal disease, epilepsy, stroke, and tuberculosis.42 A few diseases, including allergies, asthma, thyroid disease, and cancer, were exceptions to the patterns, and occur in similar percentages in individuals with fewer or more than 11 years of formal education. One disease, multiple sclerosis, had a higher prevalence in individuals with more than 12 years of formal education than in individuals with fewer than 12 years (Table 7).42
Disparities in health according to socioeconomic status appear to be widening, rather than narrowing, over the last few decades in the United Kingdom,43 the Netherlands,44 and the United States.45,46 Unequal access to medical care may explain differences in the United States and the Neth-erlands to a small degree. However, in the United Kingdom,
all citizens have access to a common medical system, the National Health Service. The increases in health disparities according to socioeconomic status present a serious concern for modern societies throughout the world.
Summary and ConclusionsThe importance of patient questionnaires and formal edu-cation in a biopsychosocial model of health and disease is consistent with the following observations:
1. Information from a patient history often provides the most valuable data to establish a diagnosis.
2. Good health and outcomes of chronic diseases are dependent as much on decisions, actions, and be-haviors of patients as on the decision and actions of health professionals.
3. The prognosis of chronic diseases often is best pro-vided by information from the patient, rather than by high technology information such as laboratory tests and imaging data.
The prognostic significance of patient questionnaires and
Table 7 Relative Frequency of Health Conditions in the 18- to 64-Year-Old Population According to Level of Formal Education
Percent Percent in Four Categories by Total of Total Years of Education Number Population 1-8 9-11 12 > 12
Any Condition 54,194 (42.7%) 64.7% 53.5% 41.3% 33.4%Arthritis/Rheumatism 14,215 (11.3%) 26.4% 13.1% 11.0% 6.8%Hypertension 14,015 (11.1%) 26.1% 15.1% 9.5% 7.2%Back Problems 9,901 (7.9%) 11.6% 10.5% 7.5% 6.1%Nervous/Emotional 7,203 (5.8%) 16.8% 9.4% 5.4% 1.6%Stomach Ulcer 4,568 (3.6%) 6.9% 5.7% 3.4% 2.1%Diabetes 3,205 (2.5%) 5.2% 3.6% 2.5% 1.4%Kidney Trouble 2,354 (1.9%) 5.1% 2.4% 1.4% 1.3%Chronic Bronchitis 2,033 (1.6%) 4.0% 2.3% 1.6% 0.7%Heart Attack 1,805 (1.4%) 4.9% 2.0% 1.2% 0.6%Cancer 837 (0.7%) 1.5% 0.6% 0.6% 0.5%Stroke 649 (0.5%) 1.2% 0.8% 0.4% 0.3%Multiple Sclerosis 148 (0.1%) 0.0% 0.1% 0.1% 0.2%

S35Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36
formal education for long-term outcomes of RA suggests that a biopsychosocial model may be as informative as a biomedical model to describe patient prognosis and course. Possible implications of these findings might be that rheu-matologists should collect data concerning functional status using a questionnaire in all patients as a component of the infrastructure of routine care.47,48 Patient questionnaire data may be more appropriate for decisions to initiate aggressive biological therapies for RA, including methotrexate and biological agents, compared to quantitative joint counts or laboratory measures,49 particularly as erythrocyte sedimenta-tion rate (ESR) and C-reactive protein (CRP) are normal in 40% of patients with RA at presentation.50 Furthermore, the suggestion that associations between poor health and low socioeconomic status, manifested by low levels of formal education, result from limited access to medical care, widely advocated by medical societies and accepted by politicians and the general public, appears valid primarily in acute diseases. Data concerning associations of educational level with clinical status in RA have been interpreted to suggest that self-management is of great im-portance in outcomes of RA and other chronic diseases.40 If self-management explains these associations far more than limited access to medical care, treatment of disadvantaged patients with RA and other chronic diseases must include efforts to assist in self-management if these patients are to achieve more favorable outcomes.
References1. Engel GL. The need for a new medical model: a challenge
for biomedicine. Science. 1977;196:129-36.2. Pincus T, Callahan LF. Remodeling the pyramid or remodeling
the paradigms concerning rheumatoid arthritis—lessons from Hodgkin’s disease and coronary artery disease. J Rheumatol. 1990;17:1582-5.
3. Pincus T. Challenges to the biomedical model: are actions of patients almost always as important as actions of health professionals in long-term outcomes of chronic diseases? (Editorial). Adv Mind Body Med. 2000;16:287-94.
4. Rose HM, Ragan C, Pearce E, Lipman MO. Differential ag-glutination of normal and sensitized sheep erythrocytes by sera of patients with rheumatoid arthritis. Proc Soc Exp Biol Med. 1948;68:1-6.
5. Engel GL. The biopsychosocial model: resolving the conflict between medicine and psychiatry. Resident Staff Physician. 1979;25:70-4.
6. Kroenke K, Mangelsdorff AD. Common symptoms in ambula-tory care: incidence, evaluation, therapy, and outcome. Am J Med. 1989;86:262-6.
7. Engel GL. How much longer must medicine’s science be bound by a seventeenth century world view? Psychother Psychosom. 1992;57(1-2):3-16.
8. Callahan LF, Pincus T. Education, self-care, and outcomes of rheumatic diseases: further challenges to the “biomedical model” paradigm. Arthritis Care Res. 1997;10:283-8.
9. Pincus T, Callahan LF. Taking mortality in rheumatoid arthri-tis seriously—predictive markers, socioeconomic status and
comorbidity. J Rheumatol. 1986;13:841-5.10. Pincus T, Callahan LF, Sale WG, et al. Severe functional de-
clines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years. Arthritis Rheum. 1984;27:864-72.
11. Pincus T. Long-term outcomes in rheumatoid arthritis. Br J Rheumatol. 1995;34:59-73.
12. Mitchell DM, Spitz PW, Young DY, et al. Survival, prognosis, and causes of death in rheumatoid arthritis. Arthritis Rheum. 1986;29:706-14.
13. Leigh JP, Fries JF. Mortality predictors among 263 patients with rheumatoid arthritis. J Rheumatol. 1991;18:1307-12.
14. Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum. 1994;37:481-94.
15. Sokka T, Hakkinen A, Krishnan E, Hannonen P. Similar pre-diction of mortality by the health assessment questionnaire in patients with rheumatoid arthritis and the general population. Ann Rheum Dis. 2004;63:494-7.
16. Yelin EH, Criswell LA, Feigenbaum PG. Health care utiliza-tion and outcomes among persons with rheumatoid arthritis in fee-for-service and prepaid group practice settings. JAMA. 1996;276(13):1048-53.
17. Söderlin MK, Nieminen P, Hakala M. Functional status predicts mortality in a community based rheumatoid arthritis population. J Rheumatol. 1998;25:1895-9.
18. Pincus T, Brooks RH, Callahan LF. Prediction of long-term mortality in patients with rheumatoid arthritis according to simple questionnaire and joint count measures. Ann Intern Med. 1994;120:26-34.
19. Pincus T, Callahan LF. Formal education as a marker for increased mortality and morbidity in rheumatoid arthritis. J Chronic Dis. 1985;38:973-84.
20. Pincus T, Callahan LF. Reassessment of twelve traditional paradigms concerning the diagnosis, prevalence, morbidity and mortality of rheumatoid arthritis. Scand J Rheumatol. 1989;18(Suppl 79):67-96.
21. Pincus T, Keysor J, Sokka T, et al. Patient questionnaires and formal education level as prospective predictors of mortality over 10 years in 97% of 1416 patients with rheumatoid ar-thritis from 15 United States private practices. J Rheumatol. 2004;31:229-34.
22. Cobb S, Anderson F, Bauer W. Length of life and cause of death in rheumatoid arthritis. N Engl J Med. 1953;249:553-6.
23. Allebeck P, Ahlbom A, Allander E. Increased mortality among persons with rheumatoid arthritis, but where RA does not appear on death certificate: eleven year follow-up of an epidemiological study. Scand J Rheumatol. 1981;10:301-6.
24. Isomäki HA. Mortality in patients with rheumatoid arthritis. In: Wolfe F, Pincus T (eds): Rheumatoid Arthritis: Pathogen-esis, Assessment, Outcome, and Treatment. New York: Marcel Dekker, 1994, pp. 235-246.
25. Wolfe F, Michaud K, Gefeller O, Choi HK. Predicting mor-tality in patients with rheumatoid arthritis. Arthritis Rheum. 2003;48:1530-42.
26. Callahan LF, Pincus T. Formal education level as a significant marker of clinical status in rheumatoid arthritis. Arthritis Rheum. 1988;31:1346-57.
27. Boers M, Dijkmans B, Gabriel S, et al. Making an impact on mortality in rheumatoid arthritis: targeting cardiovascular

Bulletin of the NYU Hospital for Joint Diseases 2007;65(Suppl 1):S29-36S36
comorbidity. Arthritis Rheum. 2004;50:1734-9.28. Gordon DA, Stein JL, Broder I. The extra-articular features
of rheumatoid arthritis: a systematic analysis of 127 cases. Am J Med. 1973;54:445-52.
29. Proudfit WL, Bruschke AVG, Sones FM Jr. Natural history of obstructive coronary artery disease: ten-year study of 601 nonsurgical cases. Prog Cardiovasc Dis. 1978;21:53-78.
30. Kaplan HS. Survival as related to treatment. In: Kaplan HS (ed): Hodgkin’s Disease. Cambridge: Harvard University Press, 1972, pp. 360-388.
31. Callahan LF, Pincus T, Huston JW III, et al. Measures of activ-ity and damage in rheumatoid arthritis: depiction of changes and prediction of mortality over five years. Arthritis Care Res. 1997;10:381-94.
32. Wolfe F, Kleinheksel SM, Cathey MA, et al. The clinical value of the Stanford health assessment questionnaire func-tional disability index in patients with rheumatoid arthritis. J Rheumatol. 1988;15:1480-8.
33. Callahan LF, Cordray DS, Wells G, Pincus T. Formal education and five-year mortality in rheumatoid arthritis: mediation by helplessness scale scores. Arthritis Care Res. 1996;9:463-72.
34. Wolfe F, Cathey MA. The assessment and prediction of functional disability in rheumatoid arthritis. J Rheumatol. 1991;18:1298-306.
35. Callahan LF, Bloch DA, Pincus T. Identification of work disability in rheumatoid arthritis: physical, radiographic and laboratory variables do not add explanatory power to demographic and functional variables. J Clin Epidemiol. 1992;45:127-38.
36. Wolfe F, Hawley DJ. The long-term outcomes of rheumatoid arthritis: work disability: A prospective 18 year study of 823 patients. J Rheumatol. 1998;25:2108-17.
37. Sokka T, Kautiainen H, Möttönen T, Hannonen P. Work dis-ability in rheumatoid arthritis 10 years after the diagnosis. J Rheumatol. 1999;26:1681-5.
38. Lubeck DP, Spitz PW, Fries JF, et al. A multicenter study of annual health service utilization and costs in rheumatoid arthritis. Arthritis Rheum. 1986;29:488-93.
39. Wolfe F, Zwillich SH. The long-term outcomes of rheumatoid arthritis: a 23-year prospective, longitudinal study of total joint replacement and its predictors in 1,600 patients with rheumatoid arthritis. Arthritis Rheum. 1998;41:1072-82.
40. Pincus T, Esther R, DeWalt DA, Callahan LF. Social conditions and self-management are more powerful determinants of health than access to care. Ann Intern Med. 1998;129:406-11.
41. Callahan LF, Smith WJ, Pincus T. Self-report questionnaires in five rheumatic diseases: comparisons of health status con-structs and associations with formal education level. Arthritis Care Res. 1989;2:122-31.
42. Pincus T, Callahan LF, Burkhauser RV. Most chronic diseases are reported more frequently by individuals with fewer than 12 years of formal education in the age 18-64 United States population. J Chronic Dis. 1987;40:865-74.
43. Marmot MG, McDowall ME. Mortality decline and widening social inequalities. Lancet. 1986;2:274-6.
44. Kunst AE, Looman CWN, Mackenbach JP. Socio-economic mortality differences in the Netherlands in 1950-1984: a regional study of cause-specific mortality. Soc Sci Med. 1990;31:141-52.
45. Feldman JJ, Makuc DM, Kleinman JC, Cornoni-Huntley J. National trends in educational differentials in mortality. Am J Epidemiol. 1989;129:919-33.
46. Pappas G, Queen S, Hadden W, Fisher G. The increasing dispar-ity in mortality between socioeconomic groups in the United States, 1960 and 1986. N Engl J Med. 1993;329:103-9.
47. Pincus T, Wolfe F. An infrastructure of patient questionnaires at each rheumatology visit: improving efficiency and docu-menting care. J Rheumatol. 2000;27:2727-30.
48. Pincus T, Yazici Y, Bergman M. Development of a multi-di-mensional health assessment questionnaire (MDHAQ) for the infrastructure of standard clinical care. Clin Exp Rheumatol. 2005;23:S19-28.
49. Pincus T, Huizinga TWJ, Yazici Y. N-of-1 trial of low-dose methotrexate and/or prednisolone in lieu of anti-CCP, MRI, or ultrasound, as first option in suspected rheumatoid arthritis? J Rheumatol. 2007;34:250-2.
50. Wolfe F, Michaud K. The clinical and research signifi-cance of the erythrocyte sedimentation rate. J Rheumatol. 1994;21:1227-37.
Disclosure StatementTheodore Pincus, M.D., has no financial or proprietary conflict of interest regarding the subject matter or materials discussed in the manuscript.