the thrill of victory, the agony of defeat: lessons from ... · 10/29/2012 1 the thrill of victory,...
TRANSCRIPT

10/29/2012
1
The Thrill of Victory, TheAgony of Defeat:
Lessons from 35 Years ofNeuro-Ophthalmic Practice
William T. Shults, MDPortland, Oregon
“Experience is just the name we giveour mistakes”
Oscar Wilde
“Some people make the same mistakeover and over again and call itexperience”
Herb Fred, MD
10/29/2012
2
“Listen to the patient, he’s trying to tell youwhat’s wrong with him.”
Eugene Stead, MD
“The final diagnosis is often as dependenton an accurate history as on a clinicalexamination”
Sir Gordon Holmes
Iatrogenic Papilledema
MT, 43 yr-old Latino, 10 yr hx of peptic ulcer 9/2/71: Surgery for obstruction → stormy post-
op course requiring hyperalimentation viacatheter in R subclavian vein
Developed headaches, diplopia and blurredvision soon afterwards → cerebral edema 2°
water retention! “This is all due to that thing they stuck in my
chest”
Iatrogenic Papilledema
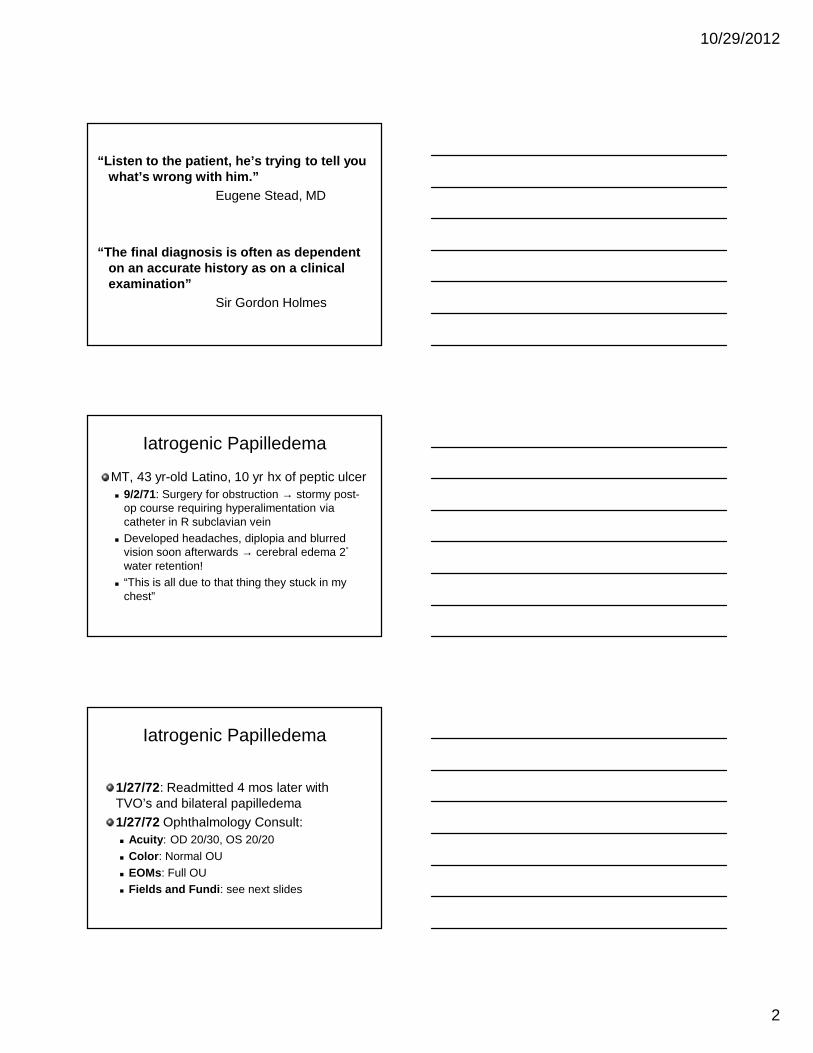
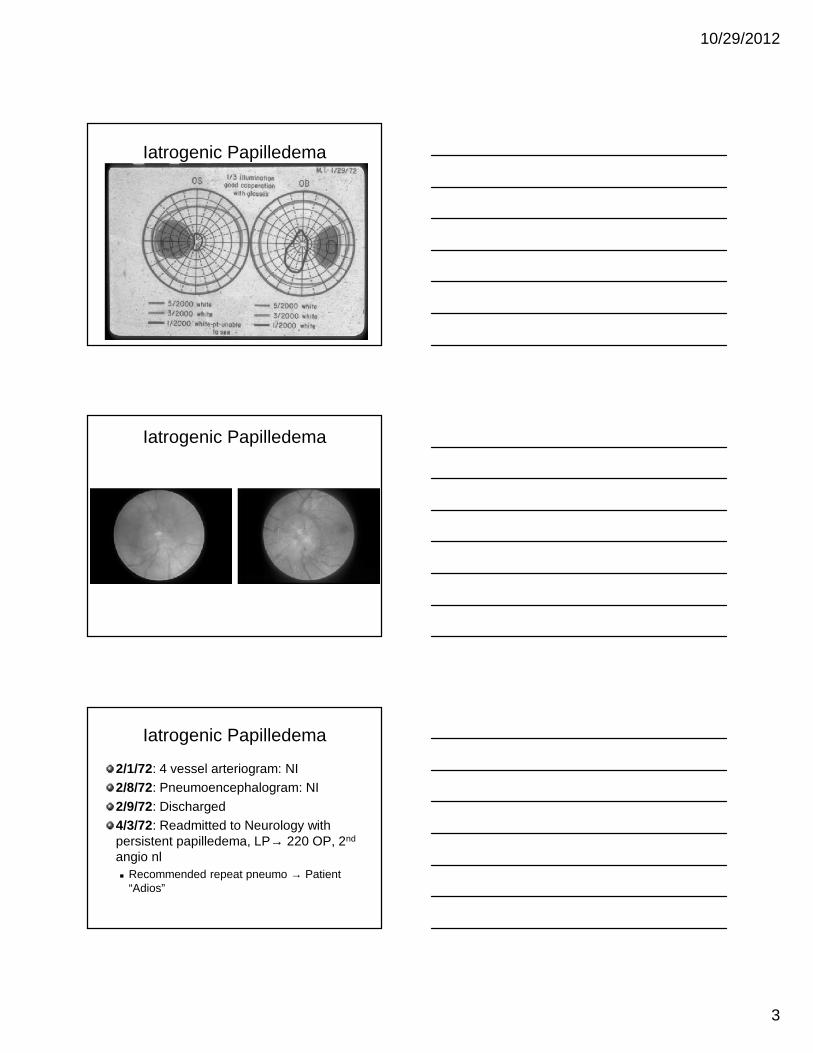
1/27/72: Readmitted 4 mos later withTVO’s and bilateral papilledema1/27/72 Ophthalmology Consult: Acuity: OD 20/30, OS 20/20 Color: Normal OU EOMs: Full OU Fields and Fundi: see next slides
10/29/2012
3
Iatrogenic Papilledema
Iatrogenic Papilledema
Iatrogenic Papilledema
2/1/72: 4 vessel arteriogram: NI2/8/72: Pneumoencephalogram: NI2/9/72: Discharged4/3/72: Readmitted to Neurology withpersistent papilledema, LP→ 220 OP, 2nd
angio nl Recommended repeat pneumo → Patient
“Adios”
10/29/2012
4
Iatrogenic Papilledema
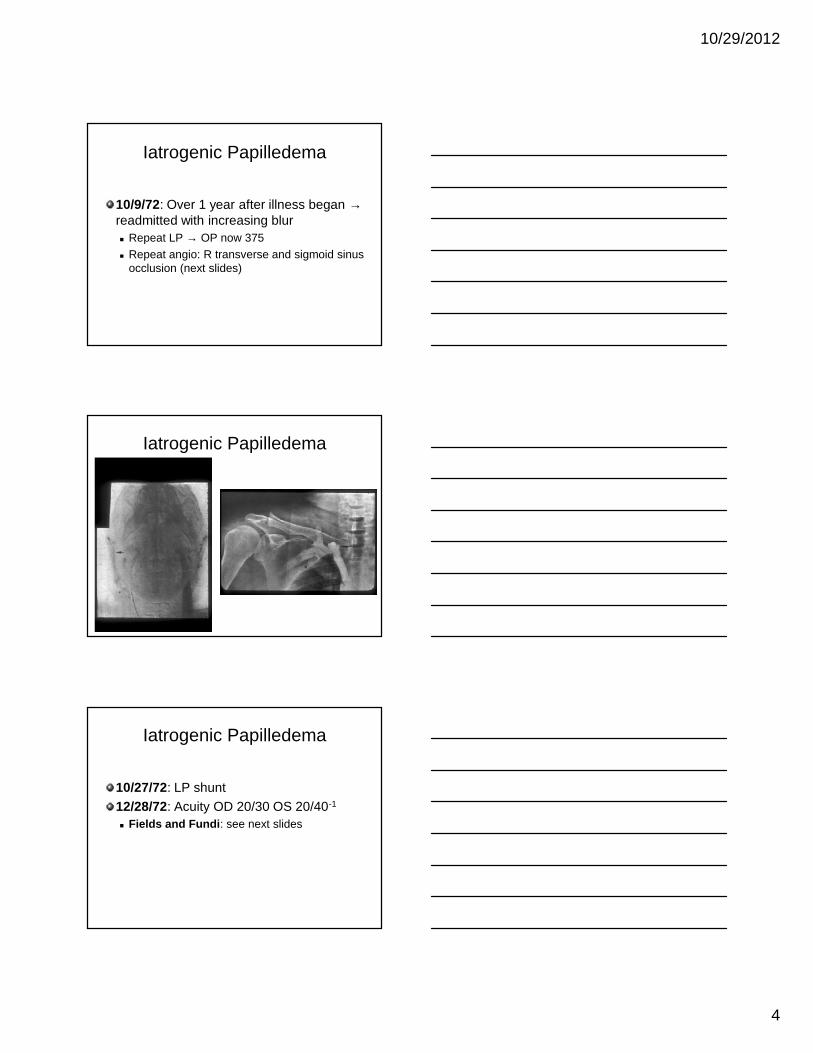
10/9/72: Over 1 year after illness began →readmitted with increasing blur Repeat LP → OP now 375 Repeat angio: R transverse and sigmoid sinus
occlusion (next slides)
Iatrogenic Papilledema
Iatrogenic Papilledema
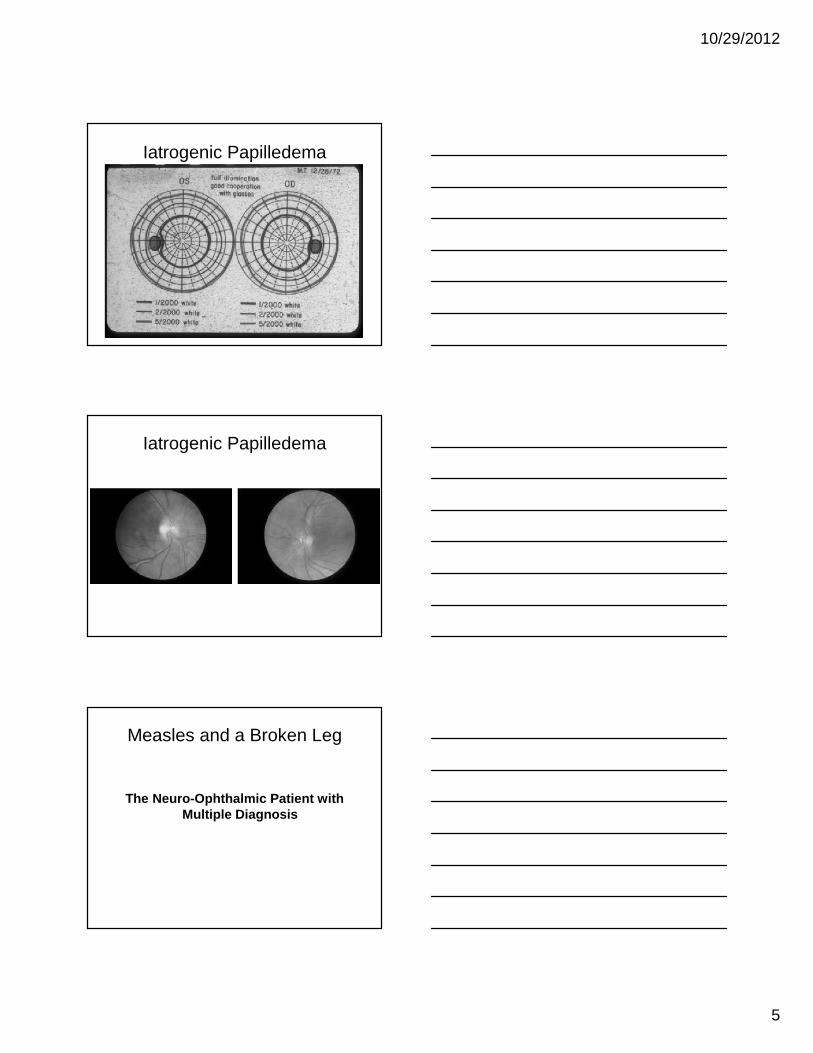
10/27/72: LP shunt12/28/72: Acuity OD 20/30 OS 20/40-1
Fields and Fundi: see next slides
10/29/2012
5
Iatrogenic Papilledema
Iatrogenic Papilledema
Measles and a Broken Leg
The Neuro-Ophthalmic Patient withMultiple Diagnosis

10/29/2012
6
Data Overload
KM, 31 year-old secretary 8/77: Developed transient
visual obscurations, OS withheadaches
Headaches cleared afterchiropractic manipulation,TVOs persisted
Data Overload
No history of exposure to steroids,nalidixic acid, lithium, tetracycline orexcess vitamin ANormal weightNeurologically healthyLong-standing right exotropia andamblyopiaIris colobomas (see next slides)
Data Overload

10/29/2012
7
Data Overload
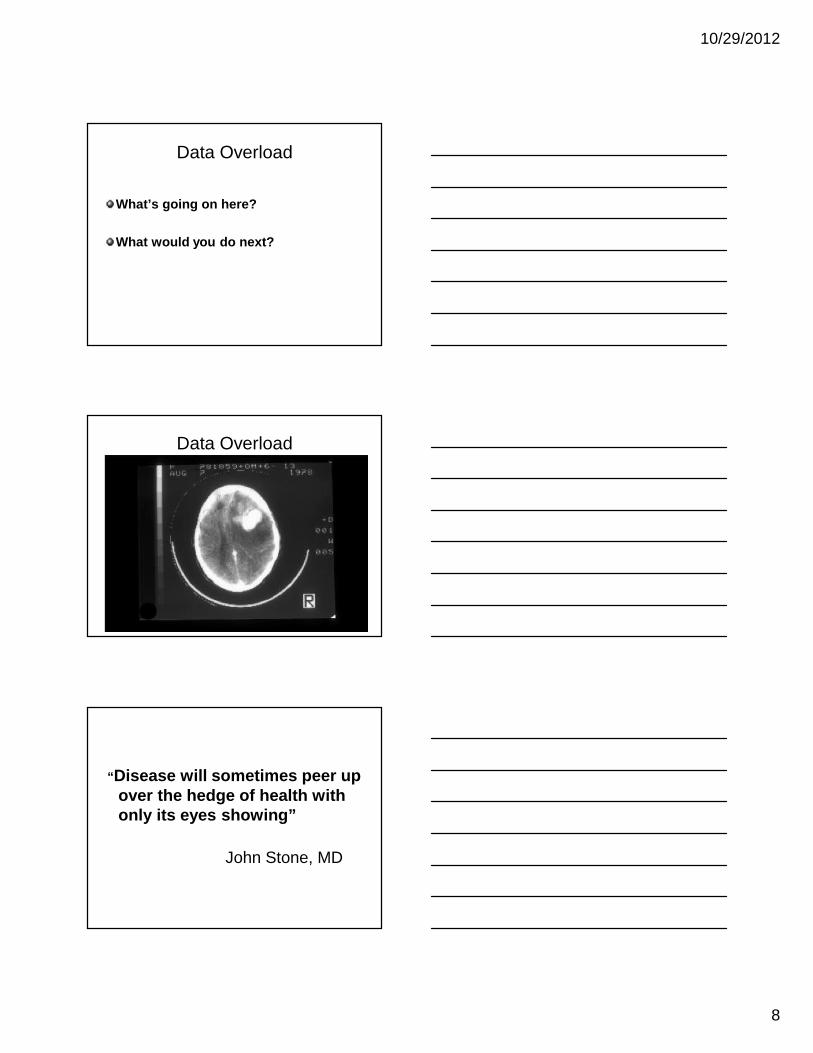
Examination (8/78): Acuity: OD HM; OS 20/30 Color: OD nil; OS 10/10 correct HRR Pupils: Right RAPD Fields and Fundi: see next slides
Data Overload
Data Overload
10/29/2012
8
Data Overload
What’s going on here?
What would you do next?
Data Overload
“Disease will sometimes peer upover the hedge of health withonly its eyes showing”
John Stone, MD

10/29/2012
9
Post Traumatic Vision Loss?
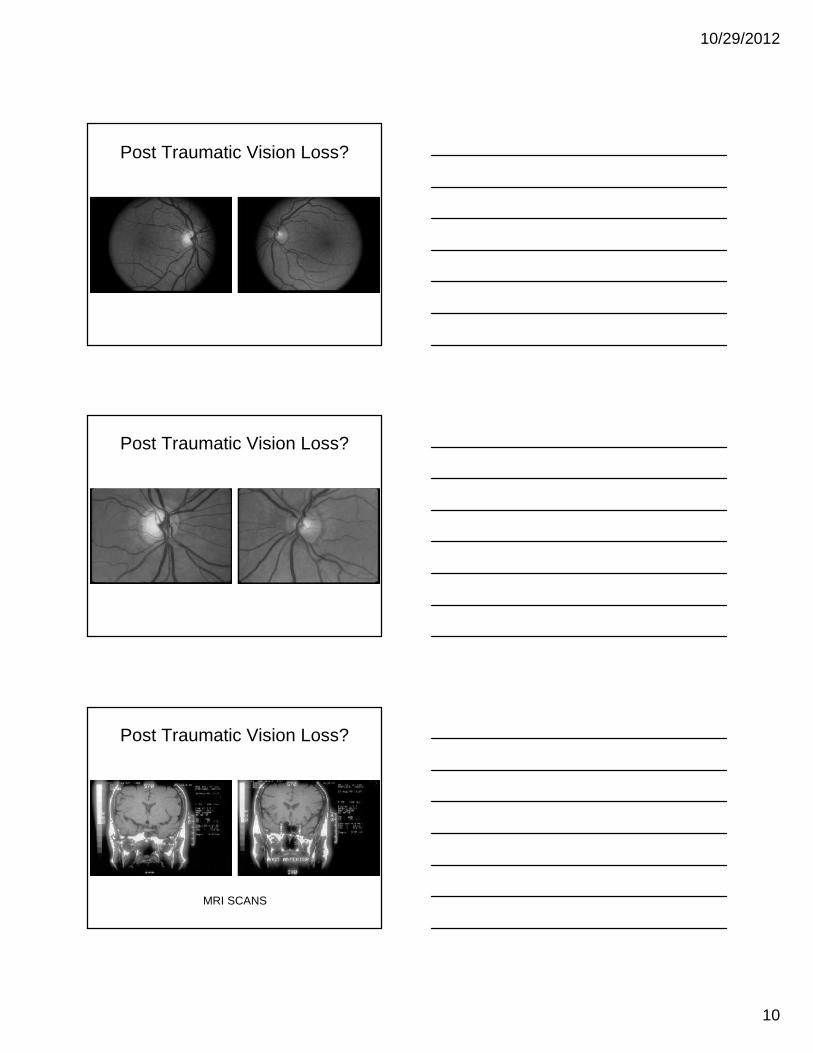
55 year old waitress 8/15/90 Rear-ended in MVA Struck forehead but no LOC Lost all vision in OD immediately after
accident VA gradually recovered over several days but
inferior nasal field defect persisted
Post Traumatic Vision Loss?
Examination (8/23/90): Acuity: OD 20/25+2, OS 20/20-2
Color: Normal Pupils: No RAPD! Fields and Fundi: see next slides
Post Traumatic Vision Loss?
10/29/2012
10
Post Traumatic Vision Loss?
Post Traumatic Vision Loss?
Post Traumatic Vision Loss?
MRI SCANS

10/29/2012
11
Post-traumatic Diplopia
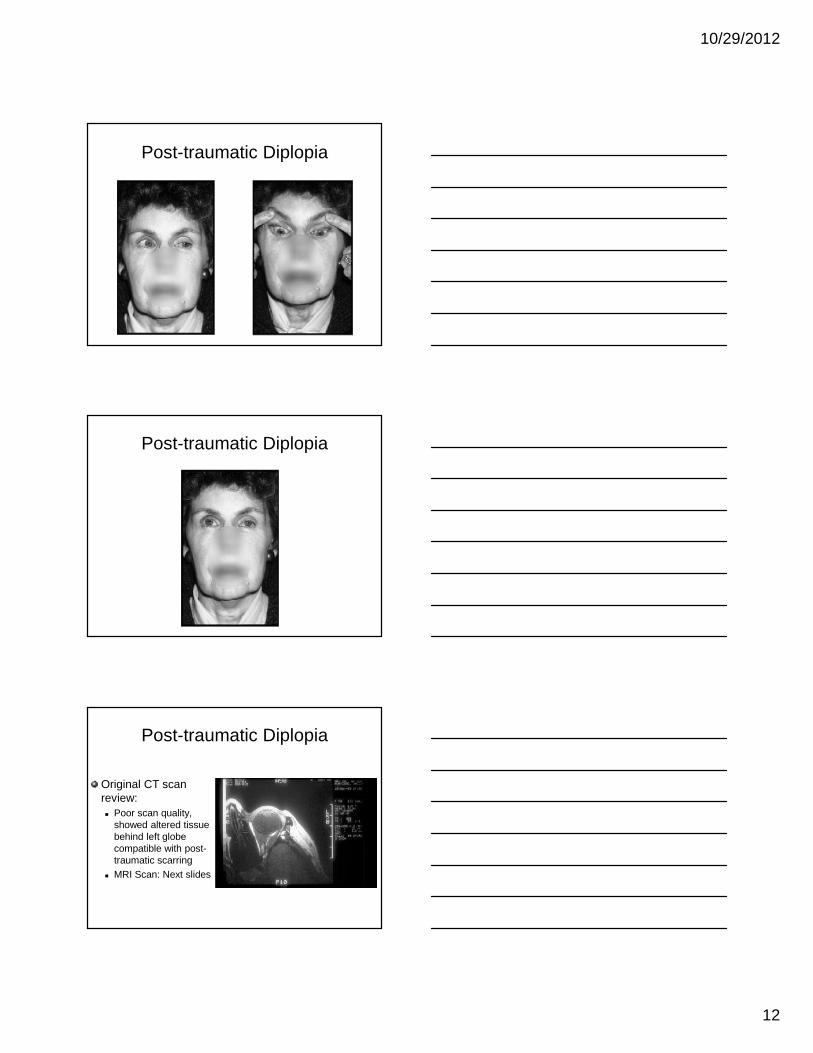
DR, 58 year old housewife 2/8/89: Involved in MVA with severe facial
trauma → right zygomatic fracture, bilateralorbital ecchymoses
Blepharoptosis noted OS sometime thereafter 3/89: Noted diplopia → Ill-defined impaired
ocular motility Tensilon test neg → referred
Post-traumatic Diplopia
Examination External: Narrowed palpebral aperture OS,
2mm enophthalmos on left Afferent package: Intact EOMs: Limited adduction, abduction,
elevation Forced ductions: Restricted
Post-traumatic Diplopia
10/29/2012
12
Post-traumatic Diplopia
Post-traumatic Diplopia
Post-traumatic Diplopia
Original CT scanreview: Poor scan quality,
showed altered tissuebehind left globecompatible with post-traumatic scarring
MRI Scan: Next slides

10/29/2012
13
Post-traumatic Diplopia
Post-traumatic diplopia
8/89: Orbital biopsy by card carryingorbital surgeon. Biopsy negative
Now what?
Post-traumatic diplopia
Patient followed withstable motility findings3/90 developed“woody” firmnessbeneath left eyeMRI repeated

10/29/2012
14
Post-traumatic diplopia
Post-traumatic diplopia
RebiopsyDx: MetastaticCarcinoma of breast
Post-traumatic diplopia
References Mottow-Lippa L, Jakoblec FA, Iwamoto T:
Pseudoinflammatory metastatic breast carcinoma ofthe orbit and lids, Ophthalmology 88:575-580, 1981.
Manor RS, Enophthalmos caused by orbitalmetastatic breast carcinoma; ACTA Opthalmologica52:881-884,1974.
Cline RA, Rootman J: Enophthalmos: a clinicalreview. Ophthalmology 91:229-237, 1984.

10/29/2012
15
“Hindsight is an exact science.”
Fagan’s Rule on Past Prediction
Papilledema: True or False?
FD, 57 year old tool and dye maker Saw cornea consultant on 3/23/93 for RK pre-
op assessmentNoted to have asymptomatic bilateral disc edema→referred for neuro-ophthalmic consultation
No history of visual complaints of any kind
Papilledema: True or False?
No history of headache, obesity,intracranial bruits or exposure topseudotumorigenic drugsPast history: Hypertensive for 10 yearsHabits: Smokes 2 packs of cigarettes/day Recovering alcoholic

10/29/2012
16
Papilledema: True or False?
Examination: Acuity: OD 20/20, OS 20/20 with moderate
myopic Rx Color: OD 9/10, OS 9/10 correct with AOHRR Contrast: OD 1.50, OS 1.65, Pelli-Robson Pupils: no RAPD Fields and fundi: see next slides
Papilledema: True or False?
Papilledema: True or False?

10/29/2012
17
Papilledema: True or False?
MRI scan: NormalNeurology consult: No localizingabnormalitiesLumbar puncture: OP 140mm H2ONow what?
Papilledema: True or False?RK performed mid-April with 20/20 result OUAbout 1 month later noted abrupt loss ofcentral vision OSExamination on 6/2/1993: Acuity: OD 20/20-1, OS 20/50-3
Color: OD 10/10, OS 9/10 correct, AOHHR Contrast: OD 1.65, OS 1.35 Pupils: 0.3 log unit RAPD, OS Fields and fundi: see next slides
Papilledema: True or False?

10/29/2012
18
Papilledema: True or False?
Papilledema: True or False?
ANTERIOR ISCHEMIC OPTIC NEUROPATHYWITH PRESYMPTOMATIC DISC SWELLINGHayreh SS: Anterior ischemic optic neuropathy:V. Optic disc edema an early sign, ArchOphthalmology 99: 1030-1040, 1981.“Symptomless optic disc edema may precedethe vision loss in AION and could constitute theearliest sign of the disease.”
“The Second Cranial Nerve is Ours”Henry J. L. Van Dyk, MD

10/29/2012
19
Meningiomas: Importance ofProper Neuro-Imaging
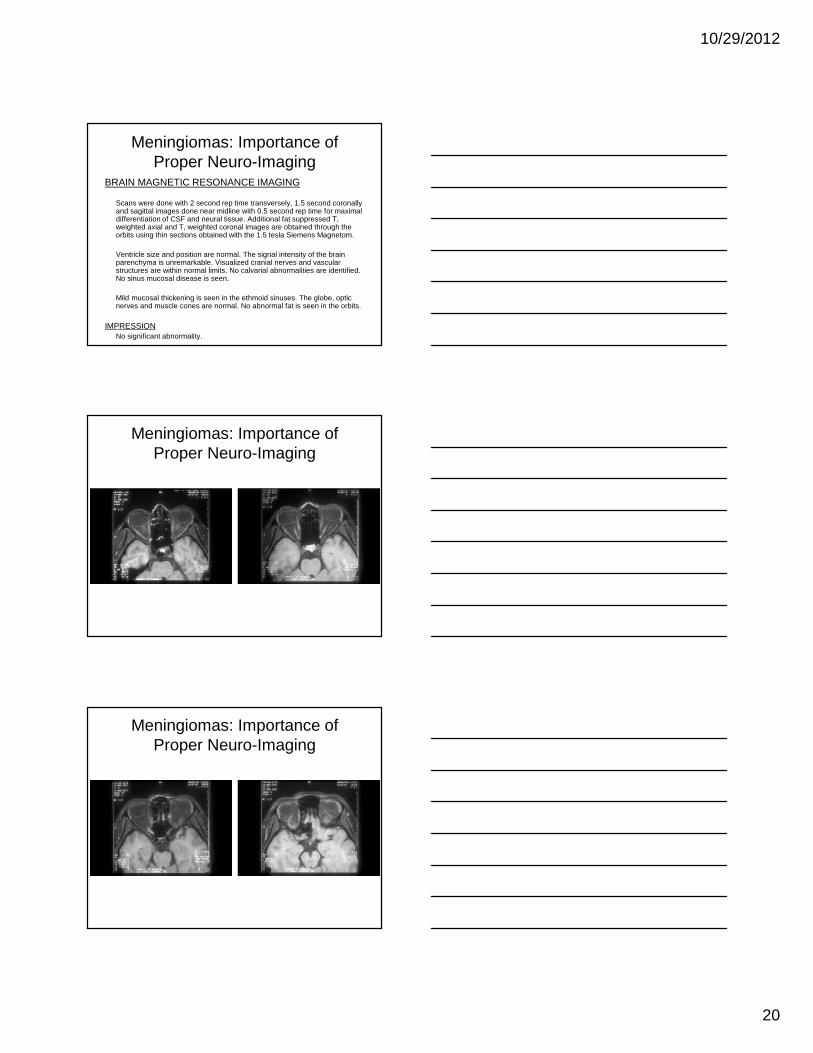
BC, 35 year old woman 3/97: “Smudged” area superonasal field,
reduced light brightness and color, ODVisual acuity: OD 20/20-1, OS 20/20Disc pallor noted OD, no RAPD
6/97: Acuity now OD 20/25, OS 20/20Visual fields: see next slide
Meningiomas: Importance ofProper Neuro-Imaging
Meningiomas: Importance ofProper Neuro-Imaging
MRI Scan: Done with standard angulation (rather than
reverse angulation in plane of the optic nerve) Thick slices Without Gadolinium
10/29/2012
20
Meningiomas: Importance ofProper Neuro-Imaging
BRAIN MAGNETIC RESONANCE IMAGING
Scans were done with 2 second rep time transversely, 1.5 second coronallyand sagittal images done near midline with 0.5 second rep time for maximaldifferentiation of CSF and neural tissue. Additional fat suppressed T,weighted axial and T, weighted coronal images are obtained through theorbits using thin sections obtained with the 1.5 tesla Siemens Magnetom.
Ventricle size and position are normal. The signal intensity of the brainparenchyma is unremarkable. Visualized cranial nerves and vascularstructures are within normal limits. No calvarial abnormalities are identified.No sinus mucosal disease is seen.
Mild mucosal thickening is seen in the ethmoid sinuses. The globe, opticnerves and muscle cones are normal. No abnormal fat is seen in the orbits.
IMPRESSIONNo significant abnormality.
Meningiomas: Importance ofProper Neuro-Imaging
Meningiomas: Importance ofProper Neuro-Imaging
10/29/2012
21
Meningiomas: Importance ofProper Neuro-Imaging
Meningiomas: Importance ofProper Neuro-Imaging
9/97: Referred for neuro-ophth consult Acuity: 20/15, OU Color: OD 4/10, OS 10/10, HRR Contrast: OD 1.35, OS 1.65 Pupils: 1.8 log unit RAPD, OD Fundus: Atrophic OD, Normal OS Repeat MRI: see next slides

10/29/2012
22
Meningiomas: Importance ofProper Neuro-Imaging
Meningiomas: Importance ofProper Neuro-Imaging
Meningiomas: Importance ofProper Neuro-Imaging

10/29/2012
23
Meningiomas: Importance ofProper Neuro-Imaging
The Definition of Neuro-Ophthalmology
RR, 78 year old man Three months of diplopia and one month of
dim vision in the left eye CT scan with contrast “normal” Referred for neuro-ophthalmology evaluation Visual fields, CT, MRI: see next slides
The Definition of Neuro-Ophthalmology

10/29/2012
24
The Definition of Neuro-Ophthalmology
CT SCANS
The Definition of Neuro-Ophthalmology
MRI SCANS
The Definition of Neuro-Ophthalmology
MRI SCANS

10/29/2012
25
“He who ignores the ancient Germanliterature will discover many new things.”
Simmons Lessell, MD
“Nihil Novum Sub Sole”(There is nothing new under the sun)
Wild & Crazy EOMs
JG, 60 year old farm machine shopoperator 1955: right 6th palsy, panhypopit → massive
sella → 3500 rads → hormone Rx 1955-1978: 6th palsy cleared, patient did well 5/78: MVA → Closed head trauma →
decreased acuity OD, no diplopia or motilitydeficits
CT Scan: large pituitary tumorCraniotomy: Incomplete removal → 3700 rads
10/29/2012
26
Wild & Crazy EOMs
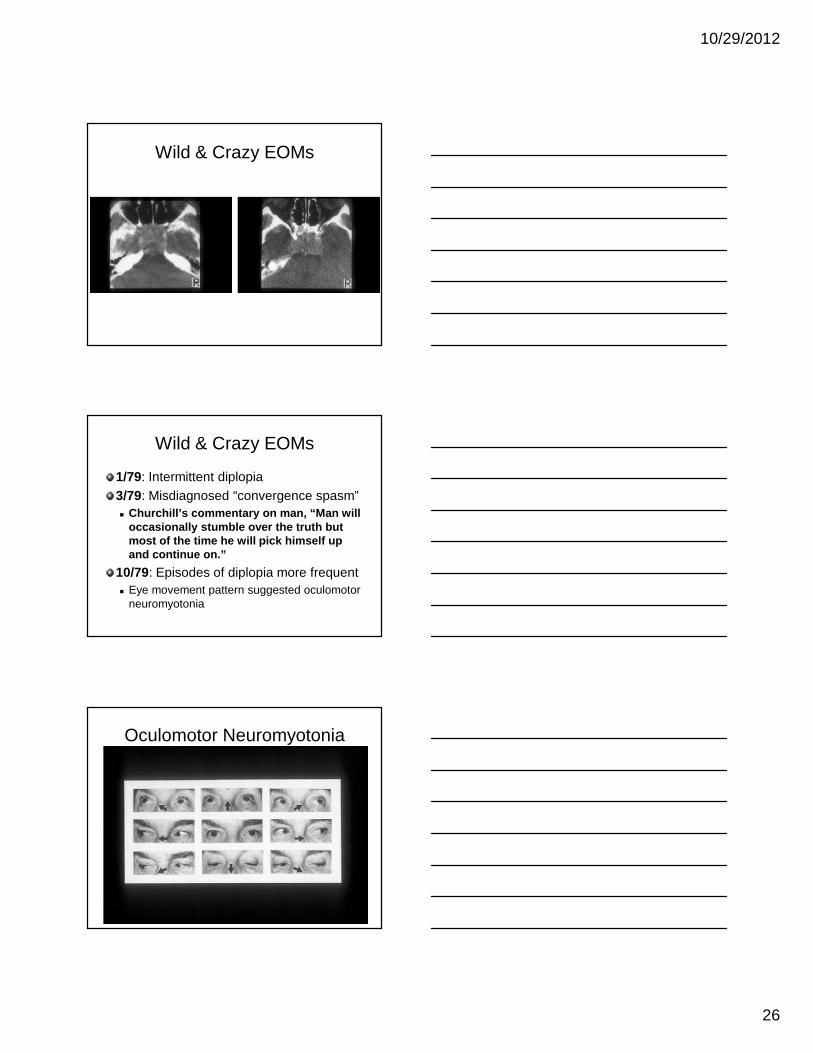
Wild & Crazy EOMs
1/79: Intermittent diplopia3/79: Misdiagnosed “convergence spasm” Churchill’s commentary on man, “Man will
occasionally stumble over the truth butmost of the time he will pick himself upand continue on.”
10/79: Episodes of diplopia more frequent Eye movement pattern suggested oculomotor
neuromyotonia
Oculomotor Neuromyotonia
10/29/2012
27
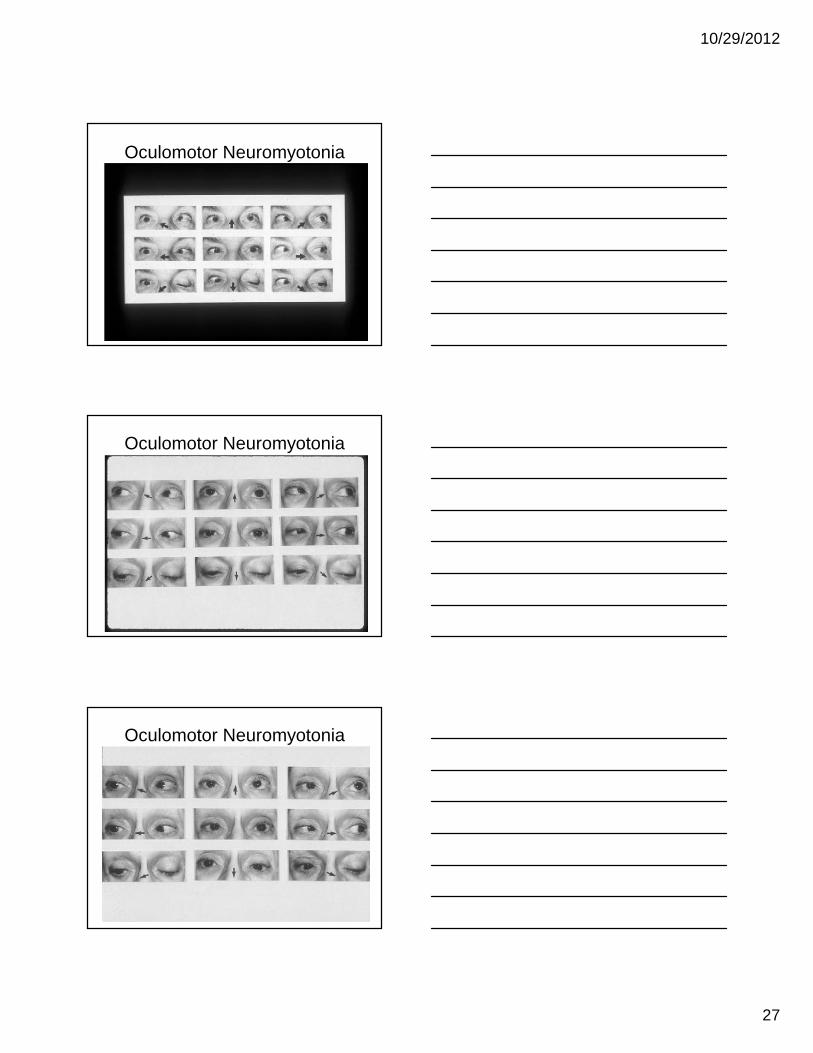
Oculomotor Neuromyotonia
Oculomotor Neuromyotonia
Oculomotor Neuromyotonia

10/29/2012
28
Oculomotor Neuromyotonia
History 1970 – Ricker and Mertens described a single
patient with brief periods of sustainedinvoluntary contraction of ocular musclesinnervated by the third nerve which theytermed oculomotor neuromyotonia
1972 – Pabst described a similar caseOcular EMG in both → neurogenic origin
Oculomotor Neuromyotonia
History 1986 – Shults et al described 6 patients, 4
with III nerve neuromyotonia and one eachwith IV and VI nerve neuromyotonia
1986 – Lessell et al added four casesemphasizing the association with radiationtherapy of skullbase neoplasms
“Sometimes it’s better to juststand there, not do something.”
Joel Glaser, MD

10/29/2012
29
Traumatic Abducens Palsy
27 year old womansustained a rightabducens palsy in anauto accident
Traumatic Abducens Palsy
January 19, 1977 21 days post injury
Traumatic Abducens Palsy
March 17, 1977 78 days post injury
10/29/2012
30
Traumatic Abducens Palsy
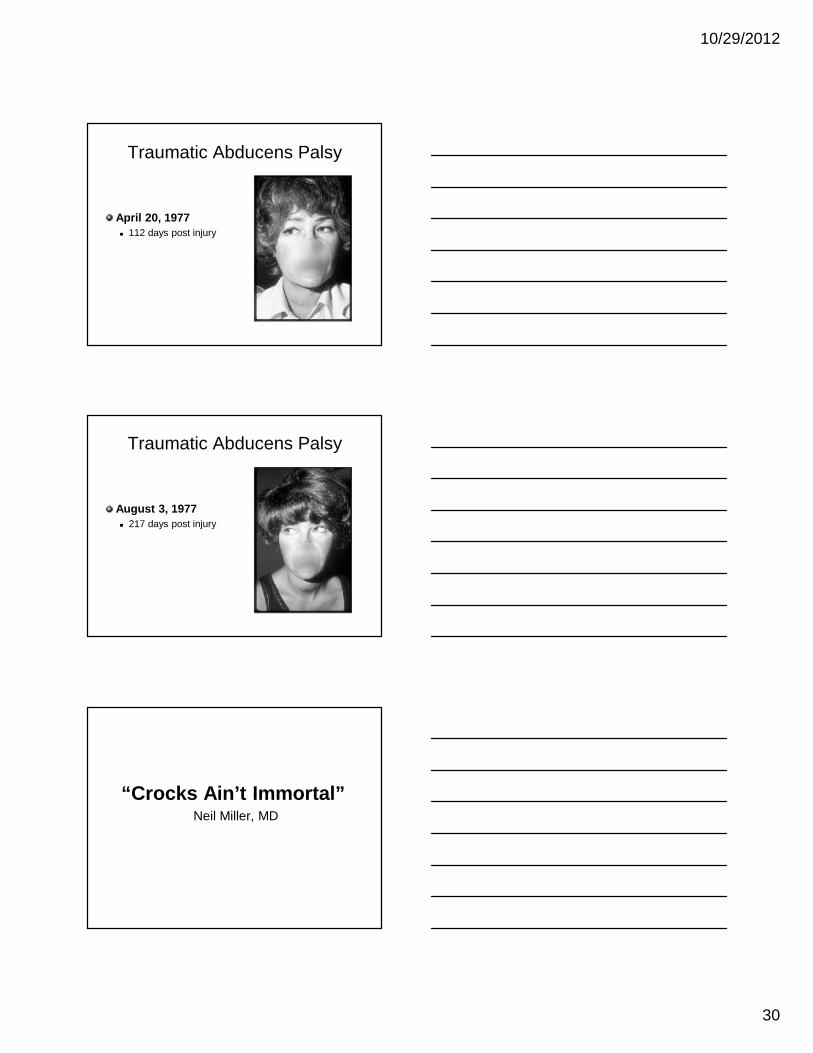
April 20, 1977 112 days post injury
Traumatic Abducens Palsy
August 3, 1977 217 days post injury
“Crocks Ain’t Immortal”Neil Miller, MD

10/29/2012
31
? Hysterical Visual Loss
PR, 59 year old housewife with a history ofsevere anxiety attacks 1987: Optometric exam showed acuity of 20/20 OU 1/91: Transient decrease in color vision OS 12/91: Further alteration of color perception (patchy
indistinctness) 4/92: Stopped driving
? Hysterical Visual Loss
5/92: Saw ophthalmologist because ofblurred vision Acuity: OD 20/200, OS CF @ 3ft IOP: OD 16, OS 17 GCF: Inferior loss OS Fundus: Temporal pallor, OS Referred to internist (no PE in 15 years) Internist referred to psychiatrist
? Hysterical Visual Loss
Psychiatrist diagnosed conversion hysteriaand placed on Xanax10/15/1992: Returned to ophthalmologistbecause of continuing visual failure Referred to neuro-ophthalmology

10/29/2012
32
? Hysterical Visual Loss
Neuro-ophthalmology exam: Acuity: OD CF @ 5ft, OS CF @ 7ft Color: 0/10 OU Contrast: unable Pupils: no RAPD Fundi: bilateral optic atrophy Visual fields: see next slide
? Hysterical Visual Loss
? Hysterical Visual Loss
MRI SCANS

10/29/2012
33
? Hysterical Visual Loss
? Hysterical Visual Loss
? Hysterical Visual Loss

10/29/2012
34
The Unlucky Resident
26 year old female medical resident 5/4/86:
Fell from bike at 35mph landing on left malareminenceUnconscious, left hemiparesisTaken to ER in central OregonFractured left zygoma and mandibleInitial CT normal
The Unlucky Resident
5/4/86 (continued): Left pupil dilated during repair of facial
fractures Repeat CT normal ICP monitoring line placed into right lateral
ventricle5/7/86: ICP line removed
The Unlucky Resident
5/8/86: Transferred to Portland Upon regaining consciousness noted
complete left homonymous hemianopsia5/14/86: Repeat CT normal
5/29/86: Referred for neuro-ophthalmology consult

10/29/2012
35
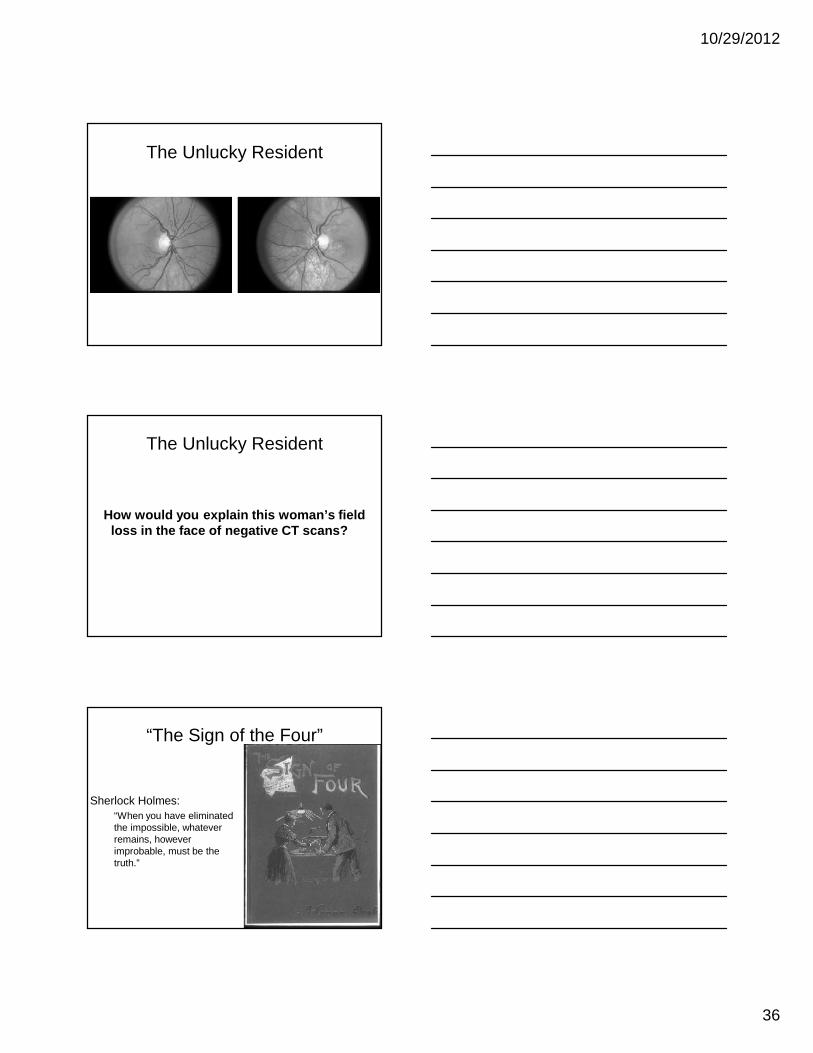
The Unlucky Resident
5/29/86 Examination: Acuity: 20/20 OU Color: normal Pupils:
Left efferent defectLeft afferent defect (0.6 log units)
Visual fields: see next slideTotal left homonymous defect
The Unlucky Resident
The Unlucky Resident
Fundoscopy: Mild temporal pallor OU Depigmentation and pigment clumping below
left disc See next slide
10/29/2012
36
The Unlucky Resident
The Unlucky Resident
How would you explain this woman’s fieldloss in the face of negative CT scans?
“The Sign of the Four”
Sherlock Holmes:“When you have eliminatedthe impossible, whateverremains, howeverimprobable, must be thetruth.”
10/29/2012
37
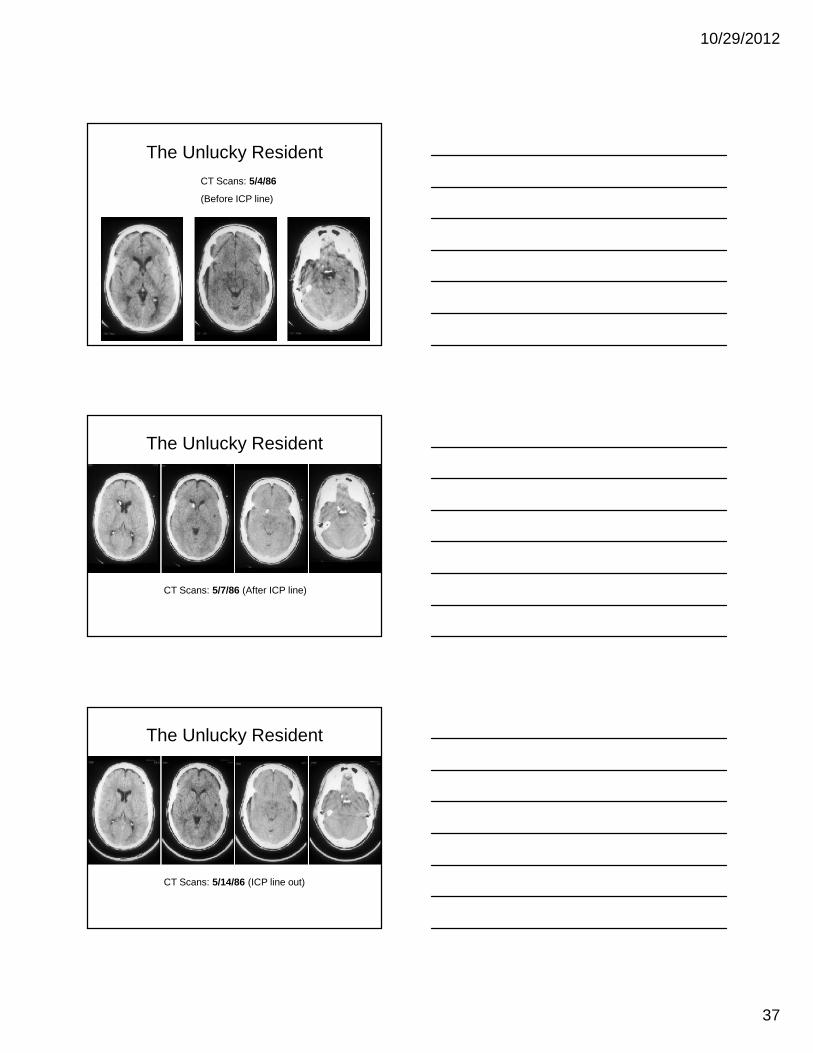
The Unlucky ResidentCT Scans: 5/4/86
(Before ICP line)
The Unlucky Resident
CT Scans: 5/7/86 (After ICP line)
The Unlucky Resident
CT Scans: 5/14/86 (ICP line out)
10/29/2012
38
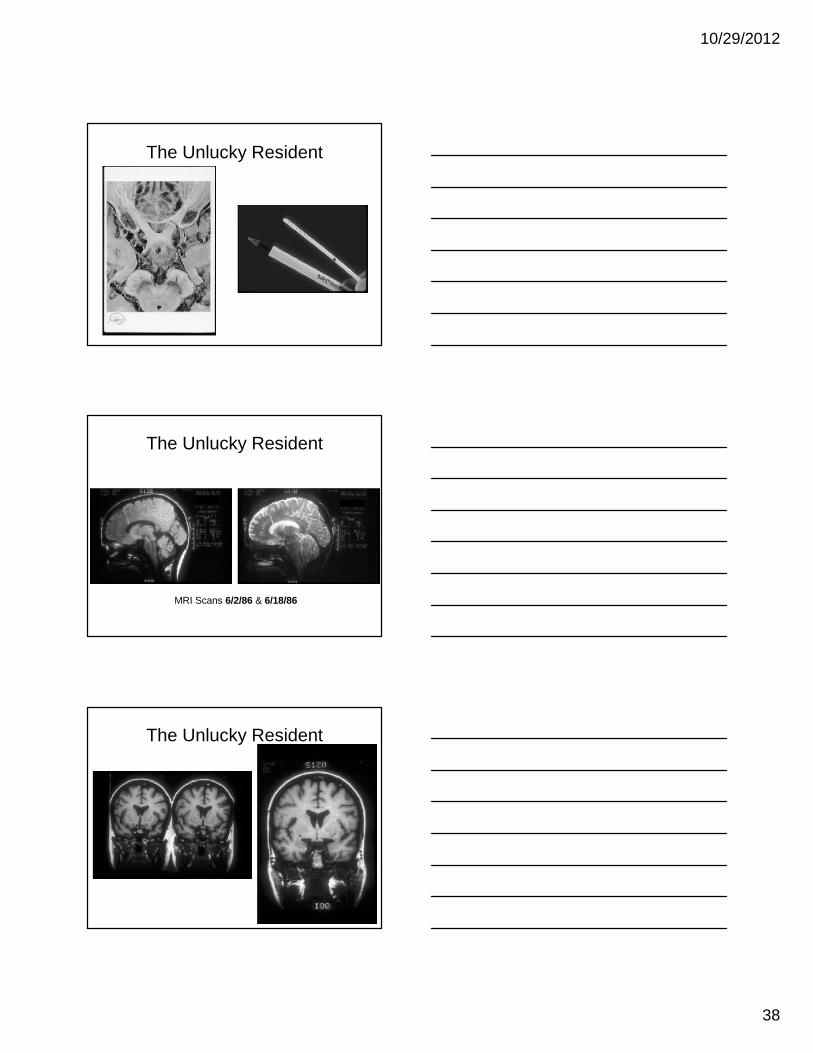
The Unlucky Resident
The Unlucky Resident
MRI Scans 6/2/86 & 6/18/86
The Unlucky Resident
10/29/2012
39
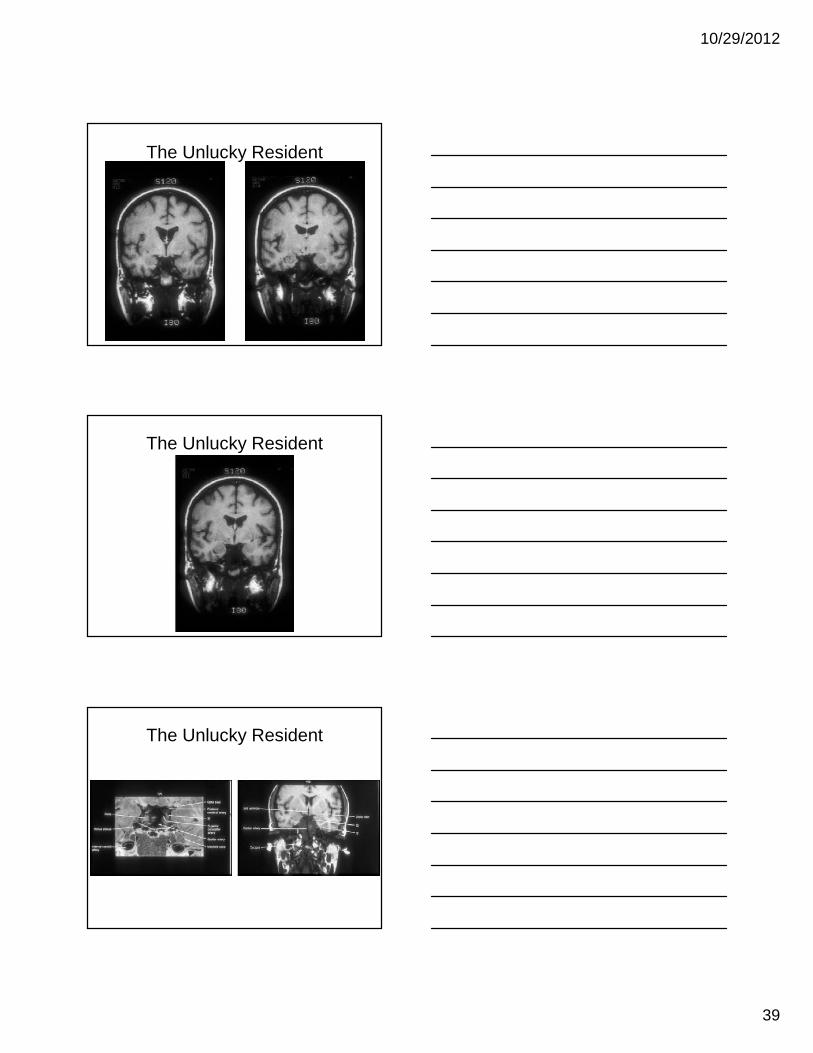
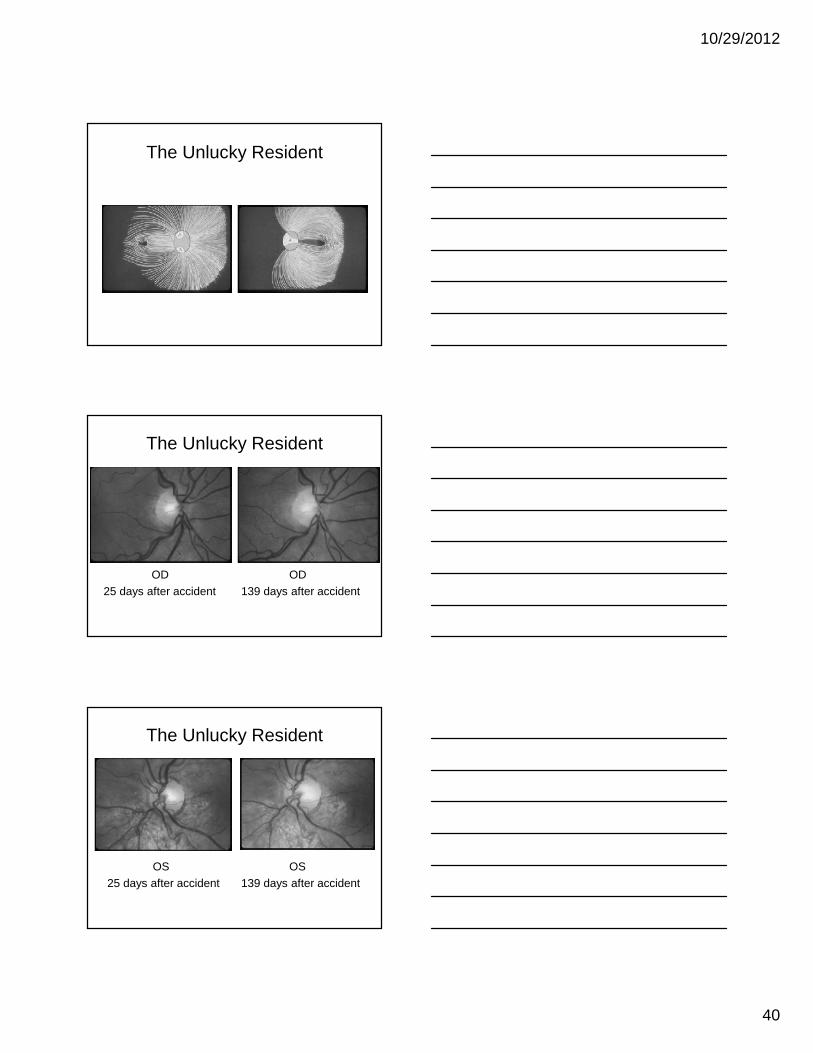
The Unlucky Resident
The Unlucky Resident
The Unlucky Resident
10/29/2012
40
The Unlucky Resident
The Unlucky Resident
OD25 days after accident
OD139 days after accident
The Unlucky Resident
OS25 days after accident
OS139 days after accident
10/29/2012
41
“Education neverends Watson. It is aseries of lessonswith the greatest forthe last.”
Sherlock Holmes