the thorax and lungs - dr. pedro...
TRANSCRIPT

The Thorax and Lungs
C H A P T E R
The Thorax and Lungs 66
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 209
ANATOMY AND PHYSIOLOGY
Study the anatomy of the chest wall, identifying the structures illustrated.Note that an interspace between two ribs is numbered by the rib above it.
Manubrium of sternum
Body of sternum
Xyphoid process
Costal angle
Costochondraljunctions
Suprasternal notch
Sternal angle
2nd costalcartilage
Cardiac notchof left lung
2nd rib
2nd ribinterspace

ANATOMY AND PHYSIOLOGY
210 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Suprasternal notchSternal angle
2nd rib
2
3
4
5
6
7
8
9
1011
12
2
3
4
5
6
7
8
9
11
Note that the costal cartilages of the first seven ribs articulate with the ster-num; the cartilages of the 8th, 9th, and 10th ribs articulate with the costalcartilages just above them. The 11th and 12th ribs, the “floating ribs,” haveno anterior attachments. The cartilaginous tip of the 11th rib can usually befelt laterally, and the 12th rib may be felt posteriorly. On palpation, costalcartilages and ribs feel identical.
Locating Findings on the Chest. Describe abnormalities of the chest intwo dimensions: along the vertical axis and around the circumference of the chest.
To make vertical locations, you must be able to count the ribs and interspaces.The sternal angle, also termed the angle of Louis, is the best guide: place yourfinger in the hollow curve of the suprasternal notch, then move your fingerdown about 5 cm to the horizontal bony ridge joining the manubrium to thebody of the sternum. Then move your finger laterally and find the adjacent 2ndrib and costal cartilage. From here, using two fingers, you can “walk down theinterspaces,” one space at a time, on an oblique line illustrated by the red num-bers below. Do not try to count interspaces along the lower edge of the ster-num; the ribs there are too close together. In a woman, to find the interspaceseither displace the breast laterally or palpate a little more medially than illus-trated. Avoid pressing too hard on tender breast tissue.

Posteriorly, the 12th rib is another possible starting point for countingribs and interspaces: it helps locate findings on the lower posterior chestand provides an option when the anterior approach is unsatisfactory. Withthe fingers of one hand, press in and up against the lower border of the12th rib, then “walk up” the interspaces numbered in red below, or fol-low a more oblique line up and around to the front of the chest.
The inferior tip of the scapula is another useful bony marker—it usually liesat the level of the 7th rib or interspace.
ANATOMY AND PHYSIOLOGY
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 211
2
3
4
5
6
7
8
9
101011
12
2
3
4
5
6
7
8
9
11
Spinous process of C7 Spinous process of T1
Inferior angleof scapula
7th rib
The spinous processes of the vertebrae are also useful anatomic landmarks.When the neck is flexed forward, the most protruding process is usually thevertebra of C7. If two processes are equally prominent, they are C7 and T1.You can often palpate and count the processes below them, especially whenthe spine is flexed.
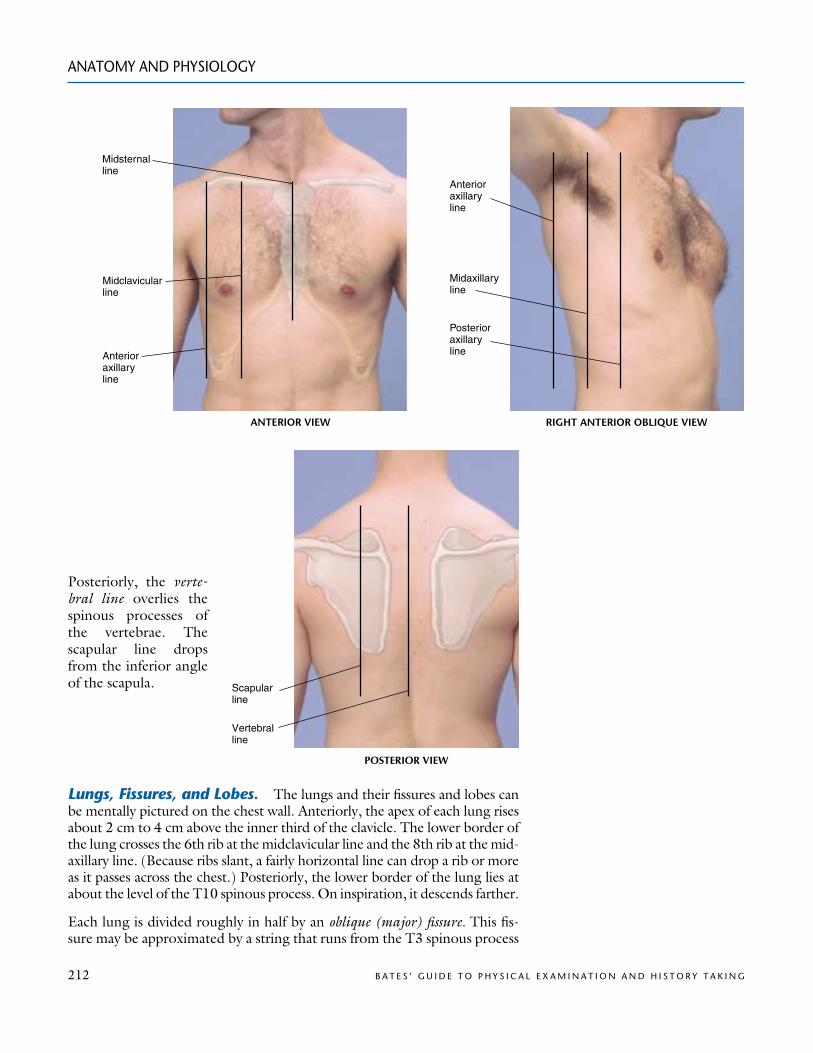
To locate findings around the circumference of the chest, use a series of verti-cal lines, shown in the next three illustrations. The midsternal and vertebrallines are precise; the others are estimated. The midclavicular line drops ver-tically from the midpoint of the clavicle. To find it, you must identify bothends of the clavicle accurately (see p. 469). The anterior and posterior axil-lary lines drop vertically from the anterior and posterior axillary folds, themuscle masses that border the axilla. The midaxillary line drops from theapex of the axilla.
ANATOMY AND PHYSIOLOGY
212 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Anterioraxillaryline
Posterioraxillaryline
Midaxillaryline
Midsternalline
Midclavicularline
Anterioraxillaryline
ANTERIOR VIEW RIGHT ANTERIOR OBLIQUE VIEW
Lungs, Fissures, and Lobes. The lungs and their fissures and lobes canbe mentally pictured on the chest wall. Anteriorly, the apex of each lung risesabout 2 cm to 4 cm above the inner third of the clavicle. The lower border ofthe lung crosses the 6th rib at the midclavicular line and the 8th rib at the mid-axillary line. (Because ribs slant, a fairly horizontal line can drop a rib or moreas it passes across the chest.) Posteriorly, the lower border of the lung lies atabout the level of the T10 spinous process. On inspiration, it descends farther.
Each lung is divided roughly in half by an oblique (major) fissure. This fis-sure may be approximated by a string that runs from the T3 spinous process
Scapular line
Vertebralline
POSTERIOR VIEW
Posteriorly, the verte-bral line overlies thespinous processes ofthe vertebrae. Thescapular line dropsfrom the inferior angleof the scapula.
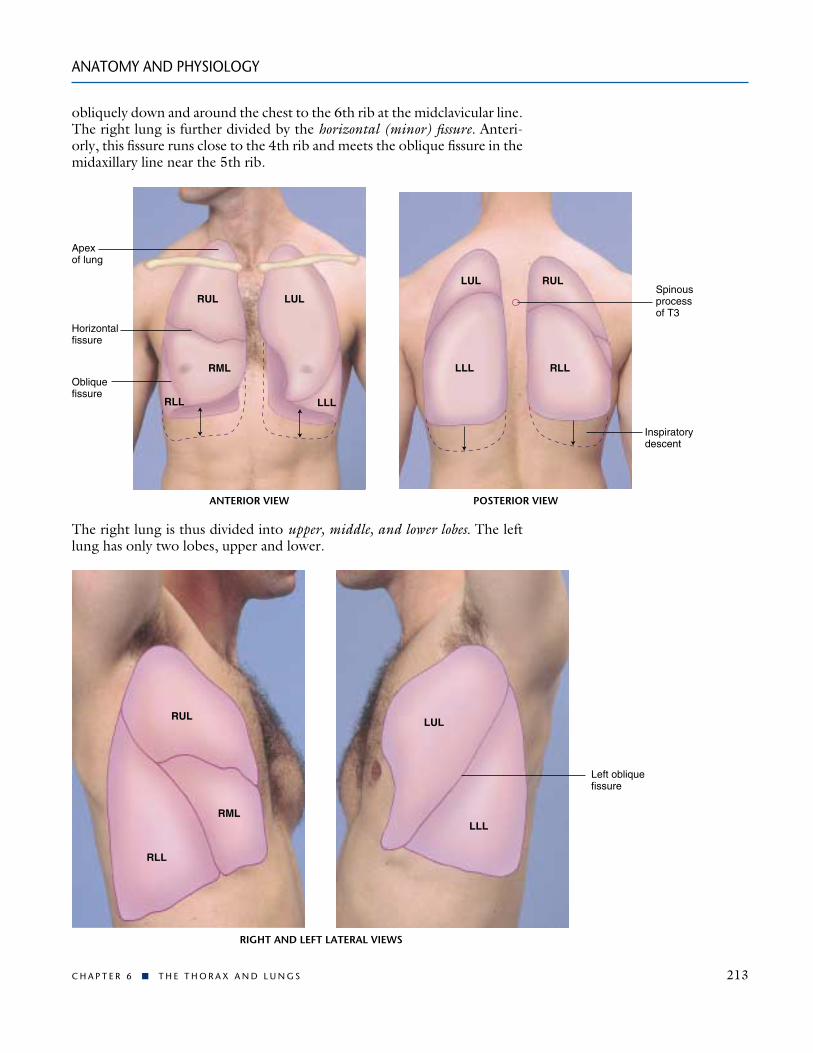
obliquely down and around the chest to the 6th rib at the midclavicular line.The right lung is further divided by the horizontal (minor) fissure. Anteri-orly, this fissure runs close to the 4th rib and meets the oblique fissure in themidaxillary line near the 5th rib.
ANATOMY AND PHYSIOLOGY
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 213
Apex of lung
Horizontalfissure
Obliquefissure
RUL
RML
RLL
LUL
LLL
LUL
LLL
RUL
RLL
Spinousprocessof T3
Inspiratorydescent
POSTERIOR VIEWANTERIOR VIEW
The right lung is thus divided into upper, middle, and lower lobes. The leftlung has only two lobes, upper and lower.
Left obliquefissure
LUL
LLL
RUL
RLL
RML
RIGHT AND LEFT LATERAL VIEWS

ANATOMY AND PHYSIOLOGY
214 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Locations on the Chest. Be familiar with general anatomic terms usedto locate chest findings, such as:
Supraclavicular—above the claviclesInfraclavicular—below the claviclesInterscapular—between the scapulaeInfrascapular—below the scapulaBases of the lungs—the lowermost portionsUpper, middle, and lower lung fields
You may then infer what part(s) of the lung(s) are affected by an abnormalprocess. Signs in the right upper lung field, for example, almost certainlyoriginate in the right upper lobe. Signs in the right middle lung field later-ally, however, could come from any of three different lobes.
The Trachea and Major Bronchi. Breath sounds over the tracheaand bronchi have a different quality than breath sounds over the lungparenchyma. Be sure you know the location of these structures. The tra-chea bifurcates into its mainstem bronchi at the levels of the sternal angleanteriorly and the T4 spinous process posteriorly.
The Pleurae. The pleurae are serous membranes that cover the outersurface of each lung, the visceral pleura, and also line the inner rib cage andupper surface of the diaphragm, the parietal pleura. Their smooth opposingsurfaces, lubricated by pleural fluid, allow the lungs to move easily within therib cage during inspiration and expiration. The pleural space is the potentialspace between visceral and parietal pleurae.
POSTERIOR VIEWANTERIOR VIEW
Trachea
Left mainbronchus
Right mainbronchus
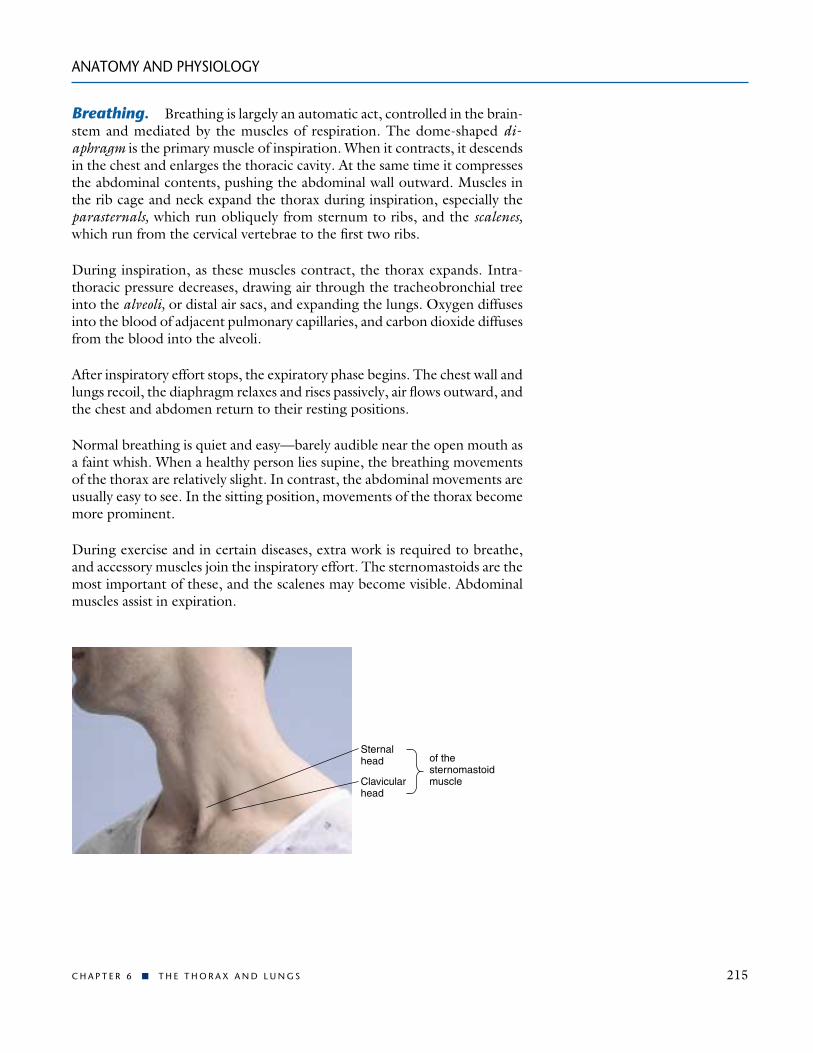
Sternalhead
Clavicularhead
of thesternomastoidmuscle
Breathing. Breathing is largely an automatic act, controlled in the brain-stem and mediated by the muscles of respiration. The dome-shaped di-aphragm is the primary muscle of inspiration. When it contracts, it descendsin the chest and enlarges the thoracic cavity. At the same time it compressesthe abdominal contents, pushing the abdominal wall outward. Muscles inthe rib cage and neck expand the thorax during inspiration, especially theparasternals, which run obliquely from sternum to ribs, and the scalenes,which run from the cervical vertebrae to the first two ribs.
During inspiration, as these muscles contract, the thorax expands. Intra-thoracic pressure decreases, drawing air through the tracheobronchial treeinto the alveoli, or distal air sacs, and expanding the lungs. Oxygen diffusesinto the blood of adjacent pulmonary capillaries, and carbon dioxide diffusesfrom the blood into the alveoli.
After inspiratory effort stops, the expiratory phase begins. The chest wall andlungs recoil, the diaphragm relaxes and rises passively, air flows outward, andthe chest and abdomen return to their resting positions.
Normal breathing is quiet and easy—barely audible near the open mouth asa faint whish. When a healthy person lies supine, the breathing movementsof the thorax are relatively slight. In contrast, the abdominal movements areusually easy to see. In the sitting position, movements of the thorax becomemore prominent.
During exercise and in certain diseases, extra work is required to breathe,and accessory muscles join the inspiratory effort. The sternomastoids are themost important of these, and the scalenes may become visible. Abdominalmuscles assist in expiration.
ANATOMY AND PHYSIOLOGY
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 215

Changes With Aging
As people age, their capacity for exercise decreases. The chest wall becomesstiffer and harder to move, respiratory muscles may weaken, and the lungslose some of their elastic recoil. The speed of breathing out with maximaleffort gradually diminishes. Skeletal changes associated with aging may ac-centuate the dorsal curve of the thoracic spine, producing kyphosis and in-creasing the anteroposterior diameter of the chest. The resulting “barrelchest,” however, has little effect on function.
THE HEALTH HISTORY
216 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
See Table 6-1. Chest Pain, pp. 234–235.
Angina pectoris, myocardial infarction
Pericarditis
Dissecting aortic aneurysm
Bronchitis
Pericarditis, pneumonia
Costochondritis, herpes zoster
Reflux esophagitis, esophagealspasm
Cervical arthritis, biliary colic, gastritis
Complaints of chest pain or chest discomfort raise the specter of heart disease,but often arise from structures in the thorax and lung as well. To assess thissymptom, you must pursue a dual investigation of both thoracic and cardiaccauses. Sources of chest pain are listed below. For this important symptom,you must keep all of these in mind.
! The myocardium
! The pericardium
! The aorta
! The trachea and large bronchi
! The parietal pleura
! The chest wall, including the musculoskeletal system and skin
! The esophagus
! Extrathoracic structures such as the neck, gallbladder, and stomach.
This section focuses on pulmonary complaints, including general questionsabout chest symptoms, dyspnea, wheezing, cough, and hemoptysis. For
EXAMPLES OF ABNORMALITIES
Common or Concerning Symptoms
! Chest pain! Dyspnea! Wheezing! Cough! Blood-streaked sputum (hemoptysis)
THE HEALTH HISTORY

health history questions about exertional chest pain, palpitations, orthop-nea, paroxysmal nocturnal dyspnea, and edema, see Chapter 7, The Cardio-vascular System.
Your initial questions should be as broad as possible. “Do you have any dis-comfort or unpleasant feelings in your chest?” As you proceed to the full his-tory, ask the patient to point to where the pain is in the chest. Watch for anygestures as the patient describes the pain. You should elicit all seven attri-butes of this symptom (see p. 27) to distinguish among the various causesof chest pain.
Lung tissue itself has no pain fibers. Pain in lung conditions such as pneu-monia or pulmonary infarction usually arises from inflammation of the ad-jacent parietal pleura. Muscle strain from prolonged recurrent coughing mayalso be responsible. The pericardium also has few pain fibers—the pain ofpericarditis stems from inflammation of the adjacent parietal pleura. (Chestpain is commonly associated with anxiety, too, but the mechanism remainsobscure.)
Dyspnea is a nonpainful but uncomfortable awareness of breathing that is in-appropriate to the level of exertion. This serious symptom warrants a full ex-planation and assessment, since dyspnea commonly results from cardiac orpulmonary disease.
Ask “Have you had any difficulty breathing?” Find out when the symptomoccurs, at rest or with exercise, and how much effort produces onset. Be-cause of variations in age, body weight, and physical fitness, there is no ab-solute scale for quantifying dyspnea. Instead, make every effort to determineits severity based on the patient’s daily activities. How many steps or flights ofstairs can the patient climb before pausing for breath? What about work suchas carrying bags of groceries, mopping the floor, or making the bed? Hasdyspnea altered the patient’s lifestyle and daily activities? How? Carefullyelicit the timing and setting of dyspnea, any associated symptoms, and re-lieving or aggravating factors.
Most patients with dyspnea relate shortness of breath to their level of activ-ity. Anxious patients present a different picture. They may describe difficultytaking a deep enough breath, or a smothering sensation with inability to getenough air, along with paresthesias, or sensations of tingling or “pins andneedles” around the lips or in the extremities.
Wheezes are musical respiratory sounds that may be audible both to the pa-tient and to others.
Cough is a common symptom that ranges in significance from trivial toominous. Typically, cough is a reflex response to stimuli that irritate re-
THE HEALTH HISTORY
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 217
A clenched fist over the sternumsuggests angina pectoris; a fingerpointing to a tender area on thechest wall suggests musculoskele-tal pain; a hand moving fromneck to epigastrum suggestsheartburn.
Anxiety is the most frequent cause of chest pain in children;costochondritis is also common.
See Table 6-2, Dyspnea, pp. 236–237.
Anxious patients may haveepisodic dyspnea during both restand exercise, and hyperventilation,or rapid, shallow breathing. At other times they may have frequent sighs.
Wheezing suggests partial airway obstruction from secre-tions, tissue inflammation, or aforeign body.
See Table 6-3, Cough and Hemoptysis, p. 238.
EXAMPLES OF ABNORMALITIES

ceptors in the larynx, trachea, or large bronchi. These stimuli includemucus, pus, and blood, as well as external agents such as dusts, foreignbodies, or even extremely hot or cold air. Other causes include inflamma-tion of the respiratory mucosa and pressure or tension in the air passagesfrom a tumor or enlarged peribronchial lymph nodes. Although coughtypically signals a problem in the respiratory tract, it may also be cardio-vascular in origin.
For complaints of cough, a thorough assessment is in order. Ask whether thecough is dry or produces sputum, or phlegm. Ask the patient to describe thevolume of any sputum and its color, odor, and consistency.
To help patients quantify volume, a multiple-choice question may behelpful . . . “How much do you think you cough up in 24 hours; a tea-spoon, tablespoon, a quarter cup, half cup, cupful?” If possible, ask thepatient to cough into a tissue; inspect the phlegm and note its character-istics. The symptoms associated with a cough often lead you to its cause.
Hemoptysis is the coughing up of blood from the lungs; it may vary fromblood-streaked phlegm to frank blood. For patients reporting hemoptysis,assess the volume of blood produced as well as the other sputum attributes;ask about the related setting and activity and any associated symptoms.
Before using the term “hemoptysis,” try to confirm the source of the bleed-ing by both history and physical examination. Blood or blood-streaked ma-terial may originate in the mouth, pharynx, or gastrointestinal tract and iseasily mislabeled. When vomited, it probably originates in the gastrointesti-nal tract. Occasionally, however, blood from the nasopharynx or the gastro-intestinal tract is aspirated and then coughed out.
HEALTH PROMOTION AND COUNSELING
218 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Cough is an important symptom ofleft-sided heart failure.
Dry hacking cough in Mycoplasmalpneumonia; productive cough in bronchitis, viral or bacterialpneumonia
Mucoid sputum is translucent,white, or gray; purulent sputum isyellowish or greenish.
Foul-smelling sputum in anaerobiclung abscess; tenacious sputum incystic fibrosis
Large volumes of purulent sputumin bronchiectasis or lung abscess
Diagnostically helpful symptomsinclude fever, chest pain, dyspnea,orthopnea, and wheezing.
See Table 6-3, Cough and Hemop-tysis, p. 238. Hemoptysis is rare ininfants, children, and adolescents; itis seen most often in cystic fibrosis.
Blood originating in the stomach isusually darker than blood from therespiratory tract and may be mixedwith food particles.
HEALTH PROMOTION AND COUNSELING
EXAMPLES OF ABNORMALITIES
Important Topics for Health Promotion and Counseling
! Tobacco cessation

Despite declines in smoking over the past several decades, more than 27% ofAmericans age 12 and older still smoke.* All adults, pregnant women, par-ents, and adolescents who smoke should be counseled regularly to stopsmoking. Smoking has been definitively linked to significant pulmonary,cardiovascular, and neoplastic disease, and accounts for one out of every fivedeaths in the United States.† It is considered the leading cause of preventabledeath. Nonsmokers exposed to smoke are also at increased risk for lung can-cer, ear and respiratory infection, asthma, low birthweight, and residentialfires. Smoking exposes patients not only to carcinogens, but also to nicotine,an addictive drug. Be especially alert to smoking by teenagers, the age groupwhen tobacco use often begins, and by pregnant women, who may continuesmoking during pregnancy.
The disease risks of smoking drop significantly within a year of smoking ces-sation. Effective interventions include targeted messages by clinicians, groupcounseling, and use of nicotine-replacement therapies. Clinicians are advisedto adopt the four “As”:
! Ask about smoking at each visit.
! Advise patients regularly to stop smoking in a clear personalized message.
! Assist patients to set stop dates and provide educational materials for self-help.
! Arrange for follow-up visits to monitor and support progress.
HEALTH PROMOTION AND COUNSELING
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 219
Preview: Recording the Physical Examination—The Thorax and Lungs
Note that initially you may use sentences to describe your findings; lateryou will use phrases. The style below contains phrases appropriate formost write-ups. Unfamiliar terms are explained in the next section, Techniques of Examination.
“Thorax is symmetric with good expansion. Lungs resonant. Breathsounds vesicular; no rales, wheezes, or rhonchi. Diaphragms descend 4 cm bilaterally.”
OR
“Thorax symmetric with moderate kyphosis and increased anteroposterior(AP) diameter, decreased expansion. Lungs are hyperresonant. Breathsounds distant with delayed expiratory phase and scattered expiratorywheezes. Fremitus decreased; no bronchophony, egophony, or whis-pered pectoriloquy. Diaphragms descend 2 cm bilaterally.”
* Substance Abuse and Mental Health Services Administration, 1999 National Household Survey.www.samhsa.gov/hhsurvey/content/1999. Accessed 8/13/01.† Centers for Disease Control and Prevention. Cigarette Smoking: Attributable Mortality and Years ofPotential Life Cost—United States. MMWR 42: 645–649, 1993.
EXAMPLES OF ABNORMALITIES
Suggests chronic obstructive lungdisease
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
220 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
See Table 3-12, Abnormalities inRate and Rhythm of Breathing (p. 93). Prolonged expiration sug-gests narrowed lower airways.
TECHNIQUES OF EXAMINATION
It is helpful to examine the posterior thorax and lungs while the patient issitting, and the anterior thorax and lungs with the patient supine. Proceedin an orderly fashion: inspect, palpate, percuss, and auscultate. Try to visu-alize the underlying lobes, and compare one side with the other, so the pa-tient serves as his or her own control. Arrange the patient’s gown so that youcan see the chest fully. For women, drape the gown over each half of the an-terior chest as you examine the other half. Cover the woman’s anterior chestwhen you examine the back.
With the patient sitting, examine the posterior thorax and lungs. The pa-tient’s arms should be folded across the chest with hands resting, if possible,on the opposite shoulders. This position moves the scapulae partly out ofthe way and increases your access to the lung fields. Then ask the patient tolie down.
With the patient supine, examine the anterior thorax and lungs. The supineposition makes it easier to examine women because the breasts can be gen-tly displaced. Furthermore, wheezes, if present, are more likely to be heard.(Some authorities, however, prefer to examine both the back and the frontof the chest with the patient sitting. This technique is also satisfactory).
For patients unable to sit up without aid, try to get help so that you can ex-amine the posterior chest in the sitting position. If this is impossible, roll thepatient to one side and then to the other. Percuss the upper lung, and aus-cultate both lungs in each position. Because ventilation is relatively greaterin the dependent lung, your chances of hearing wheezes or crackles aregreater on the dependent side.
Initial Survey of Respiration and the Thorax
Even though you may have already recorded the respiratory rate when youtook the vital signs, it is wise to again observe the rate, rhythm, depth, and ef-fort of breathing. A normal resting adult breathes quietly and regularly about
Combining clinician and group counseling with nicotine replacement ther-apy is especially effective for highly addicted patients.
Relapses are common and should be expected. Nicotine withdrawal, weightgain, stress, social pressure, and use of alcohol are often cited as explanations.Help patients to learn from these experiences: work with the patient to pin-point the precipitating circumstances and develop strategies for alternativeresponses and health-promoting behaviors.
EXAMPLES OF ABNORMALITIES
14 to 20 times a minute. An occasional sigh is to be expected. Note whetherexpiration lasts longer than usual.
Always inspect the patient for any signs of respiratory difficulty.
! Assess the patient’s color for cyanosis. Recall any relevant findings from ear-lier parts of your examination, such as the shape of the fingernails.
! Listen to the patient’s breathing. Is there any audible wheezing? If so, wheredoes it fall in the respiratory cycle?
! Inspect the neck. During inspiration, is there contraction of the sterno-mastoid or other accessory muscles, or supraclavicular retraction? Is thetrachea midline?
Also observe the shape of the chest. The anteroposterior (AP) diameter may in-crease with aging.
Examination of the Posterior Chest
INSPECTIONFrom a midline position behind the patient, note the shape of the chest andthe way in which it moves, including:
! Deformities or asymmetry
! Abnormal retraction of the interspaces during inspiration. Retraction ismost apparent in the lower interspaces. Supraclavicular retraction is oftenassociated.
! Impaired respiratory movement on one or both sides or a unilateral lag(or delay) in movement.
PALPATIONAs you palpate the chest, focus on areas of tenderness and abnormalities inthe overlying skin, respiratory expansion, and fremitus.
Identify tender areas. Carefully palpate any area where pain has been re-ported or where lesions or bruises are evident.
TECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 221
Cyanosis signals hypoxia. Club-bing of the nails (see p. 110) inchronic obstructive pulmonarydisease (COPD) or congenitalheart disease
Audible stridor, a high-pitchedwheeze, is an ominous sign of airway obstruction in the larynx ortrachea.
Inspiratory contraction of the sternomastoids at rest signals severe difficulty breathing. Lateraldisplacement of the trachea inpneumothorax, pleural effusion, or atelectasis
The AP diameter also may increasein COPD.
See Table 6-4, Deformities of theThorax (p. 239).
Retraction in severe asthma, COPD,or upper airway obstruction.
Unilateral impairment or lagging of respiratory movement suggestsdisease of the underlying lung orpleura.
Intercostal tenderness over in-flamed pleura
Bruises over a fractured rib
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
222 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Test chest expansion. Place your thumbs at about the level of the 10th ribs,with your fingers loosely grasping and parallel to the lateral rib cage. As youposition your hands, slide them medially just enough to raise a loose fold ofskin on each side between your thumb and the spine.
Ask the patient to inhale deeply. Watch the distance between your thumbsas they move apart during inspiration, and feel for the range and symmetryof the rib cage as it expands and contracts.
Feel for tactile fremitus. Fremitus refers to the palpable vibrations transmit-ted through the bronchopulmonary tree to the chest wall when the patientspeaks. To detect fremitus, use either the ball (the bony part of the palm atthe base of the fingers) or the ulnar surface of your hand to optimize the vi-bratory sensitivity of the bones in your hand. Ask the patient to repeat thewords “ninety-nine” or “one-one-one.” If fremitus is faint, ask the patientto speak more loudly or in a deeper voice.
Use one hand until you have learned the feel of fremitus. Some cliniciansfind using one hand more accurate. The simultaneous use of both hands tocompare sides, however, increases your speed and may facilitate detection ofdifferences.
Causes of unilateral decrease ordelay in chest expansion includechronic fibrotic disease of the underlying lung or pleura, pleuraleffusion, lobar pneumonia, pleuralpain with associated splinting, andunilateral bronchial obstruction.
Fremitus is decreased or absentwhen the voice is soft or whenthe transmission of vibrationsfrom the larynx to the surface ofthe chest is impeded. Causes in-clude an obstructed bronchus;COPD; separation of the pleuralsurfaces by fluid (pleural effusion),fibrosis (pleural thickening), air (pneumothorax), or an infil-trating tumor; and also a verythick chest wall.
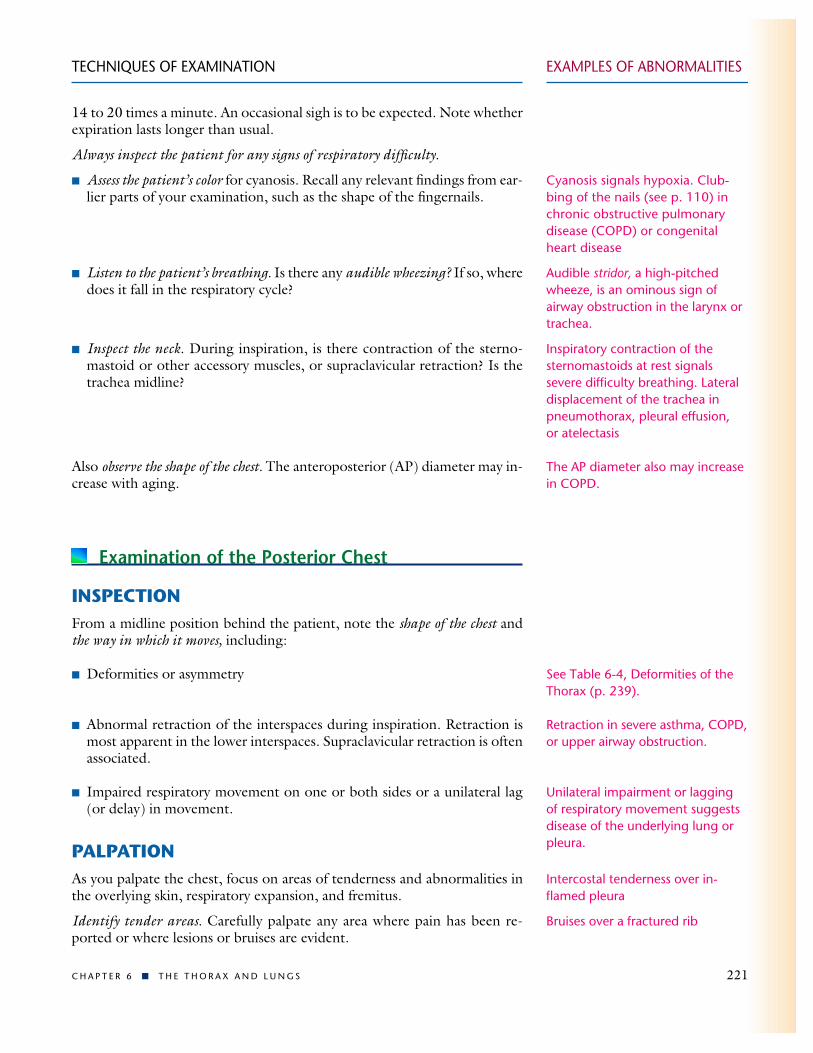
Assess any observed abnormalities such as masses or sinus tracts (blind, in-flammatory, tubelike structures opening onto the skin)
Although rare, sinus tracts usuallyindicate infection of the underlyingpleura and lung (as in tuberculosis,actinomycosis).

Palpate and compare symmetric areasof the lungs in the pattern shown inthe photograph. Identify and locateany areas of increased, decreased, orabsent fremitus. Fremitus is typicallymore prominent in the interscapulararea than in the lower lung fields,and is often more prominent on theright side than on the left. It dis-appears below the diaphragm.
Tactile fremitus is a relatively roughassessment tool, but as a scoutingtechnique it directs your attentionto possible abnormalities. Later inthe examination you will check anysuggested findings by listening forbreath sounds, voice sounds, andwhispered voice sounds. All theseattributes tend to increase or de-crease together.
PERCUSSIONPercussion is one of the most important techniques of physical examination.Percussion of the chest sets the chest wall and underlying tissues into mo-tion, producing audible sound and palpable vibrations. Percussion helps youestablish whether the underlying tissues are air-filled, fluid-filled, or solid. Itpenetrates only about 5 cm to 7 cm into the chest, however, and thereforewill not help you to detect deep-seated lesions.
The technique of percussion can be practiced on any surface. As you prac-tice, listen for changes in percussion notes over different types of materialsor different parts of the body. The key points for good technique, describedfor a right-handed person, are as follows:
! Hyperextend the middle fingerof your left hand, known as thepleximeter finger. Press its distalinterphalangeal joint firmly onthe surface to be percussed. Avoidsurface contact by any other partof the hand, because this dampensout vibrations. Note that thethumb, 2nd, 4th, and 5th fingersare not touching the chest.
! Position your right forearm quiteclose to the surface, with the handcocked upward. The middle fingershould be partially flexed, relaxed,and poised to strike.
TECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 223
1 1
2
3
2
3
4 4
LOCATIONS FOR FEELING FREMITUS

! With a quick sharp but relaxedwrist motion, strike the pleximeterfinger with the right middle fin-ger, or plexor finger. Aim at yourdistal interphalangeal joint. Youare trying to transmit vibrationsthrough the bones of this joint tothe underlying chest wall.
Strike using the tip of the plexorfinger, not the finger pad. Yourfinger should be almost at rightangles to the pleximeter. A shortfingernail is recommended toavoid self-injury.
! Withdraw your striking fingerquickly to avoid damping the vi-brations you have created.
In summary, the movement is at thewrist. It is directed, brisk yet relaxed,and a bit bouncy.
TECHNIQUES OF EXAMINATION
224 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Percussion Notes. With your plexor or tapping finger, use the lightestpercussion that produces a clear note. A thick chest wall requires heavier per-cussion than a thin one. However, if a louder note is needed, apply morepressure with the pleximeter finger (this is more effective for increasing per-cussion note volume than tapping harder with the plexor finger).
When percussing the lower posterior chest, stand somewhat to the side ratherthan directly behind the patient. This allows you to place your pleximeterfinger more firmly on the chest and your plexor is more effective, making abetter percussion note.
When comparing two areas, use the same percussion technique in both areas.Percuss or strike twice in each location. It is easier to detect differences inpercussion notes by comparing one area with another than by striking repet-itively in one place.

EXAMPLES OF ABNORMALITIES
Learn to identify five percussion notes. You can practice four of them on your-self. These notes differ in their basic qualities of sound: intensity, pitch, andduration. Train your ear to distinguish these differences by concentrating onone quality at a time as you percuss first in one location, then in another. Re-view the table below. Normal lungs are resonant.
TECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 225
While the patient keeps both arms crossed in front of the chest, percuss thethorax in symmetric locations from the apices to the lung bases.
Percuss one side of the chest and then the other at each level, as shown by thenumbers below. Omit the areas over the scapulae—the thickness of muscleand bone alters the percussion notes over the lungs. Identify and locate thearea and quality of any abnormal percussion note.
Relative Relative RelativeIntensity Pitch Duration Example of Location
Percussion Notes and Their Characteristics
* Distinguished mainly by its musical timbre.
Flatness
Dullness
Resonance
Hyperresonance
Tympany
Soft
Medium
Loud
Very loud
Loud
High
Medium
Low
Lower
High*
Short
Medium
Long
Longer
*
Thigh
Liver
Normal lung
None normally
Gastric air bubble orpuffed-out cheek
Pathologic Examples
Large pleural effusion
Lobar pneumonia
Simple chronic bronchitis
Emphysema, pneumothorax
Large pneumothorax
Dullness replaces resonance when fluid or solid tissue replacesair-containing lung or occupies the pleural space beneath yourpercussing fingers. Examples include: lobar pneumonia, in whichthe alveoli are filled with fluid andblood cells; and pleural accumula-tions of serous fluid (pleural effusion), blood (hemothorax), pus (empyema), fibrous tissue, or tumor.
Generalized hyperresonance maybe heard over the hyperinflatedlungs of emphysema or asthma,but it is not a reliable sign. Unilat-eral hyperresonance suggests alarge pneumothorax or possibly alarge air-filled bulla in the lung.
1
2
3
4
5
1
2
3
4
5
6 6
7 7
LOCATIONS FOR PERCUSSION AND AUSCULTATION

An abnormally high level suggestspleural effusion, or a high diaphragm as in atelectasis or diaphragmatic paralysis.
Sounds from bedclothes, papergowns, and the chest itself cangenerate confusion in auscultation.Hair on the chest may cause crack-ling sounds. Either press harder orwet the hair. If the patient is coldor tense, you may hear musclecontraction sounds—muffled, low-pitched rumbling or roaring noises.A change in the patient’s positionmay eliminate this noise. You can
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
226 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Identify the descent of the diaphragms, or diaphragmatic excursion. First, de-termine the level of diaphragmatic dullness during quiet respiration. Holdingthe pleximeter finger above and parallel to the expected level of dullness,percuss downward in progressive steps until dullness clearly replaces reso-nance. Confirm this level of change by percussion near the middle of the he-mothorax and also more laterally.
Resonant
Level ofdiaphragm
Dull
Locationand sequenceof percussion
Dull
Note that with this technique you are identifying the boundary between theresonant lung tissue and the duller structures below the diaphragm. You arenot percussing the diaphragm itself. You can infer the probable location ofthe diaphragm from the level of dullness.
Now, estimate the extent of diaphragmatic excursion by determining the dis-tance between the level of dullness on full expiration and the level of dull-ness on full inspiration, normally about 5 cm or 6 cm. This estimate doesnot correlate well, however, with radiologic assessment of diaphragmaticmovement.
AUSCULTATIONAuscultation of the lungs is the most important examining technique for as-sessing air flow through the tracheobronchial tree. Together with percus-sion, it also helps the clinician to assess the condition of the surroundinglungs and pleural space. Auscultation involves (1) listening to the soundsgenerated by breathing, (2) listening for any adventitious (added) sounds,and (3) if abnormalities are suspected, listening to the sounds of the patient’sspoken or whispered voice as they are transmitted through the chest wall.
Breath Sounds (Lung Sounds). You will learn to identify patterns ofbreath sounds by their intensity, their pitch, and the relative duration of theirinspiratory and expiratory phases. Normal breath sounds are:
EXAMPLES OF ABNORMALITIESTECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 227
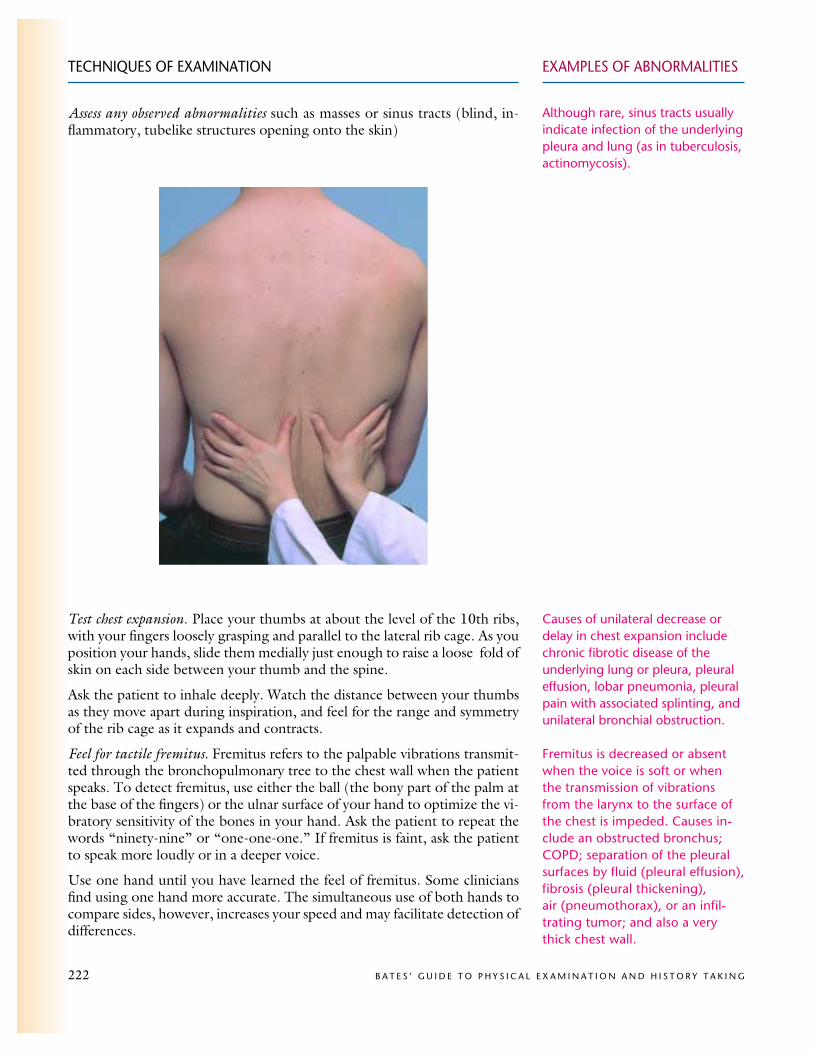
! Vesicular, or soft and low pitched. They are heard through inspiration,continue without pause through expiration, and then fade away about onethird of the way through expiration.
! Bronchovesicular, with inspiratory and expiratory sounds about equal inlength, at times separated by a silent interval. Differences in pitch and in-tensity are often more easily detected during expiration.
! Bronchial, or louder and higher in pitch, with a short silence between in-spiratory and expiratory sounds. Expiratory sounds last longer than inspi-ratory sounds.
The characteristics of these three kinds of breath sounds are summarized inthe table below. Also shown are the tracheal breath sounds—very loud,harsh sounds that are heard by listening over the trachea in the neck.
reproduce this sound on yourselfby doing a Valsalva maneuver(straining down) as you listen toyour own chest.
If bronchovesicular or bronchialbreath sounds are heard in loca-tions distant from those listed, sus-pect that air-filled lung has beenreplaced by fluid-filled or solid lungtissue. See Table 6-5, Normal andAltered Breath and Voice Sounds(p. 240).
Intensity of Pitch of LocationsDuration of Expiratory Expiratory Where HeardSounds Sound Sound Normally
Characteristics of Breath Sounds
* The thickness of the bars indicates intensity; the steeper their incline, the higher the pitch.
Vesicular*
Broncho-vesicular
Bronchial
Tracheal
Inspiratory soundslast longer thanexpiratory ones.
Inspiratory andexpiratory soundsare about equal.
Expiratory soundslast longer thaninspiratory ones.
Inspiratory andexpiratory soundsare about equal.
Soft
Intermediate
Loud
Very loud
Relatively low
Intermediate
Relatively high
Relatively high
Over most ofboth lungs
Often in the 1st and 2ndinterspacesanteriorly andbetween thescapulae
Over the manu-brium, if heardat all
Over the tracheain the neck
Listen to the breath sounds with the diaphragm of a stethoscope after in-structing the patient to breathe deeply through an open mouth. Use the pat-tern suggested for percussion, moving from one side to the other and com-paring symmetric areas of the lungs. If you hear or suspect abnormal sounds,auscultate adjacent areas so that you can fully describe the extent of any ab-normality. Listen to at least one full breath in each location. Be alert for pa-tient discomfort due to hyperventilation (e.g., light headedness, faintness),and allow the patient to rest as needed.

TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
228 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Note the intensity of the breath sounds. Breath sounds are usually louderin the lower posterior lung fields and may also vary from area to area. If thebreath sounds seem faint, ask the patient to breathe more deeply. You maythen hear them easily. When patients do not breathe deeply enough orwhen they have a thick chest wall, as in obesity, breath sounds may remaindiminished.
Is there a silent gap between the inspiratory and expiratory sounds?
Listen for the pitch, intensity, and duration of the expiratory and inspiratorysounds. Are vesicular breath sounds distributed normally over the chest wall?Or are there bronchovesicular or bronchial breath sounds in unexpectedplaces? If so, where are they?
Adventitious (Added) Sounds. Listen for any added, or adventitious,sounds that are superimposed on the usual breath sounds. Detection of ad-ventitious sounds—crackles (sometimes called rales), wheezes, and rhonchi—is an important part of your examination, often leading to diagnosis of car-diac and pulmonary conditions. The most common kinds of these soundsare described below:
Breath sounds may be decreasedwhen air flow is decreased (as byobstructive lung disease or muscu-lar weakness) or when the trans-mission of sound is poor (as inpleural effusion, pneumothorax, oremphysema).
A gap suggests bronchial breathsounds.
For further discussion and otheradded sounds, see Table 6-6, Ad-ventitious (Added) Lung Sounds:Causes and Qualities (p. 241).
DISCONTINUOUS SOUNDS (CRACKLES OR RALES) are intermittent,nonmusical, and brief—like dots in time
Fine crackles ( ) are soft, high pitched, and very brief (5–10 msec).
Coarse crackles ( ) are somewhat louder, lower in pitch, and not quite so brief (20–30 msec).
CONTINUOUS SOUNDS are > 250 msec, notably longer than crackles—like dashesin time—but do not necessarily persist throughout the respiratory cycle. Unlikecrackles, they are musical.
Wheezes ( ) are relatively high pitched (around 400 Hz or higher) and have a hissing or shrill quality.
Rhonchi ( ) are relatively low pitched (around 200 Hz or lower) and have asnoring quality.
Adventitious Lung Sounds
Crackles may be due to abnormalities ofthe lungs (pneumonia, fibrosis, earlycongestive heart failure) or of the air-ways (bronchitis, bronchiectasis).
Wheezes suggest narrowed airways, as inasthma, COPD, or bronchitis.
Rhonchi suggest secretions in largeairways.
If you hear crackles, especially those that do not clear after cough, listencarefully for the following characteristics. These are clues to the underlyingcondition:
! Loudness, pitch, and duration (summarized as fine or coarse crackles)
! Number (few to many)
Fine late inspiratory crackles thatpersist from breath to breath suggest abnormal lung tissue.

EXAMPLES OF ABNORMALITIES
! Timing in the respiratory cycle
! Location on the chest wall
! Persistence of their pattern from breath to breath
! Any change after a cough or a change in the patient’s position
In some normal people, crackles may be heard at the lung bases anteriorlyafter maximal expiration. Crackles in dependent portions of the lungs mayalso occur after prolonged recumbency.
If you hear wheezes or rhonchi, note their timing and location. Do theychange with deep breathing or coughing?
Transmitted Voice Sounds. If you hear abnormally located broncho-vesicular or bronchial breath sounds, continue on to assess transmitted voicesounds. With a stethoscope, listen in symmetric areas over the chest wall asyou:
! Ask the patient to say “ninety-nine.” Normally the sounds transmittedthrough the chest wall are muffled and indistinct.
! Ask the patient to say “ee.” You will normally hear a muffled long Esound.
! Ask the patient to whisper “ninety-nine” or “one-two-three.” The whis-pered voice is normally heard faintly and indistinctly, if at all.
Examination of the Anterior Chest
The patient, when examined in the supine position, should lie comfortablywith arms somewhat abducted. A patient who is having difficulty breathingshould be examined in the sitting position or with the head of the bed ele-vated to a comfortable level.
TECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 229
Clearing of crackles, wheezes, orrhonchi after cough suggests thatsecretions caused them, as inbronchitis or atelectasis.
Increased transmission of voicesounds suggests that air-filled lunghas become airless. See Table 6-5,Normal and Altered Breath andVoice Sounds (p. 240).
Louder, clearer voice sounds arecalled bronchophony.
When “ee” is heard as “ay,” an E-to-A change (egophony) is present, as in lobar consolidationfrom pneumonia. The qualitysounds nasal.
Louder, clearer whispered sounds are called whispered pectoriloquy.
Persons with severe COPD mayprefer to sit leaning forward, withlips pursed during exhalation andarms supported on their knees ora table.

TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
230 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
INSPECTIONObserve the shape of the patient’s chest and the movement of the chest wall.Note:
! Deformities or asymmetry
! Abnormal retraction of the lower interspaces during inspiration
! Local lag or impairment in respiratory movement
PALPATIONPalpation has four potential uses:
! Identification of tender areas
! Assessment of observed abnormalities
! Further assessment of chest expansion. Place your thumbs along each costalmargin, your hands along the lateral rib cage. As you position your hands,slide them medially a bit to raise loose skin folds between your thumbs.Ask the patient to inhale deeply. Observe how far your thumbs diverge asthe thorax expands, and feel for the extent and symmetry of respiratorymovement.
See Table 6-4, Deformities of theThorax (p. 239).
Severe asthma, COPD, or upperairway obstruction
Underlying disease of lung or pleura
Tender pectoral muscles or costalcartilages tend to corroborate, butdo not prove, that chest pain has amusculoskeletal origin.
! Assessment of tactile fremitus. Compare both sides of the chest, using theball or ulnar surface of your hand. Fremitus is usually decreased or absentover the precordium. When examining a woman, gently displace thebreasts as necessary.

EXAMPLES OF ABNORMALITIESTECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 231
PERCUSSIONPercuss the anterior and lateral chest, again comparing both sides. The heartnormally produces an area of dullness to the left of the sternum from the 3rdto the 5th interspaces. Percuss the left lung lateral to it.
Dullness replaces resonance when fluid or solid tissue replacesair-containing lung or occupies thepleural space. Because pleural fluidusually sinks to the lowest part ofthe pleural space (posteriorly in asupine patient), only a very largeeffusion can be detected anteriorly.
The hyperresonance of COPD maytotally replace cardiac dullness.
1 1
2 23 3
11
22
33
44 55
66
LOCATIONS FOR FEELING FREMITUS
LOCATIONS FOR PERCUSSION AND AUSCULTATION
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
232 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
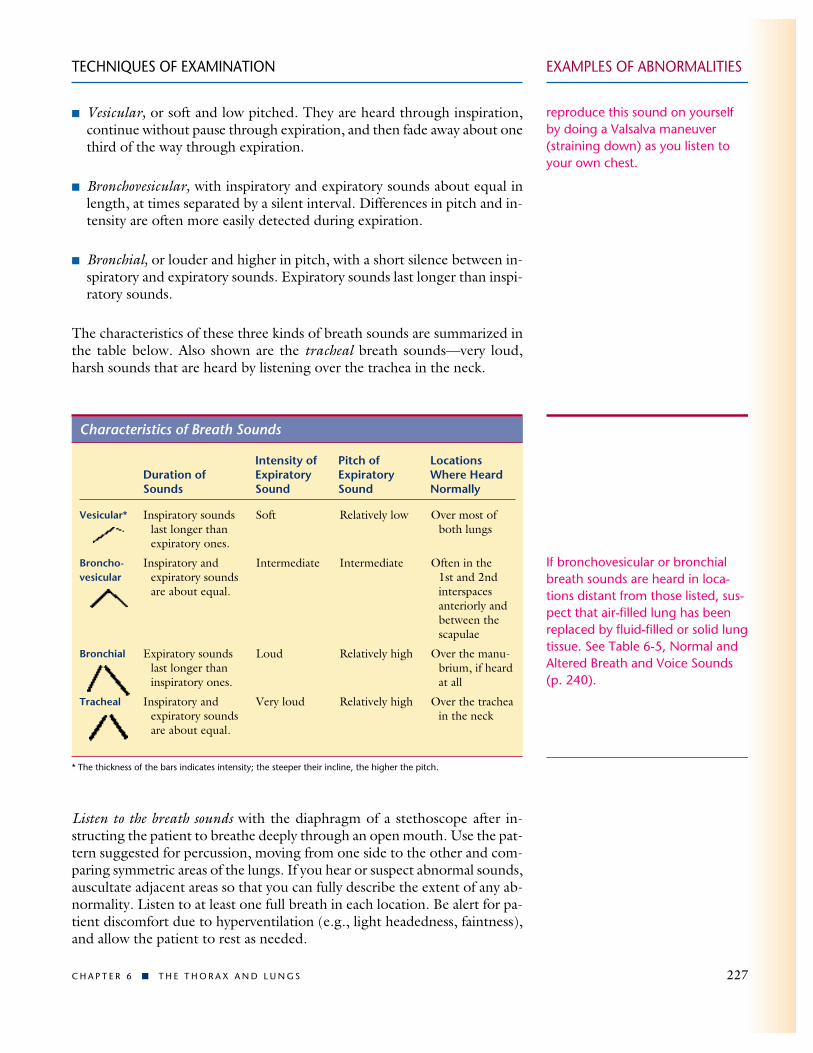
In a woman, to enhance percussion, gently displace the breast with your lefthand while percussing with the right.
The dullness of right middle lobepneumonia typically occurs behindthe right breast. Unless you dis-place the breast, you may miss theabnormal percussion note.
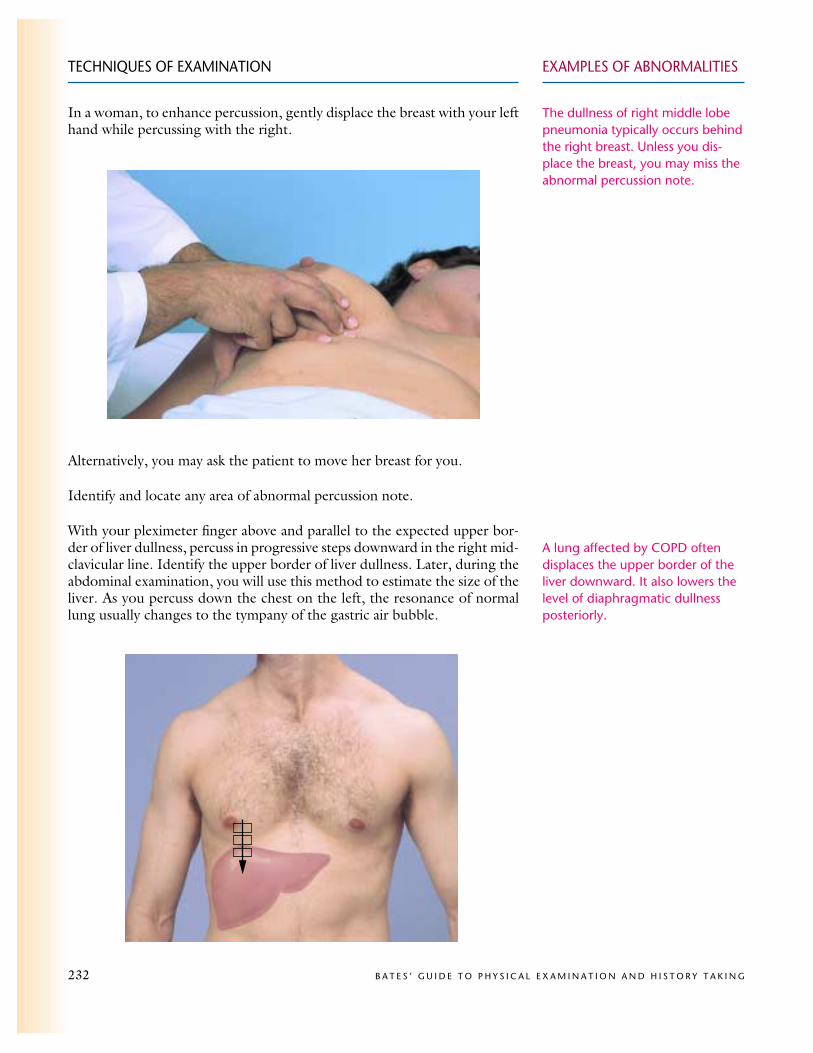
A lung affected by COPD oftendisplaces the upper border of theliver downward. It also lowers thelevel of diaphragmatic dullnessposteriorly.
Alternatively, you may ask the patient to move her breast for you.
Identify and locate any area of abnormal percussion note.
With your pleximeter finger above and parallel to the expected upper bor-der of liver dullness, percuss in progressive steps downward in the right mid-clavicular line. Identify the upper border of liver dullness. Later, during theabdominal examination, you will use this method to estimate the size of theliver. As you percuss down the chest on the left, the resonance of normallung usually changes to the tympany of the gastric air bubble.

EXAMPLES OF ABNORMALITIESTECHNIQUES OF EXAMINATION
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 233
AUSCULTATIONListen to the chest anteriorly and laterally as the patient breathes with mouthopen, somewhat more deeply than normal. Compare symmetric areas of thelungs, using the pattern suggested for percussion and extending it to adja-cent areas as indicated.
Listen to the breath sounds, noting their intensity and identifying any varia-tions from normal vesicular breathing. Breath sounds are usually louder inthe upper anterior lung fields. Bronchovesicular breath sounds may be heardover the large airways, especially on the right.
Identify any adventitious sounds, time them in the respiratory cycle, andlocate them on the chest wall. Do they clear with deep breathing?
If indicated, listen for transmitted voice sounds.
Special Techniques
Clinical Assessment of Pulmonary Function. A simple but infor-mative way to assess the complaint of breathlessness in an ambulatory pa-tient is to walk with the patient down the hall or climb one flight of stairs.Observe the rate, effort, and sound of the patient’s breathing.
Forced Expiratory Time. This test assesses the expiratory phase ofbreathing, which is typically slowed in obstructive pulmonary disease. Askthe patient to take a deep breath in and then breathe out as quickly and com-pletely as possible with mouth open. Listen over the trachea with the di-aphragm of a stethoscope and time the audible expiration. Try to get threeconsistent readings, allowing a short rest between efforts if necessary.
Identification of a Fractured Rib. Local pain and tenderness of oneor more ribs raise the question of fracture. By anteroposterior compressionof the chest, you can help to distinguish a fracture from soft-tissue injury.With one hand on the sternum and the other on the thoracic spine, squeezethe chest. Is this painful, and where?
See Table 6-6, Adventitious(Added) Lung Sounds: Causes andQualities (p. 241), and Table 6-7,Physical Findings in Selected ChestDisorders (pp. 242–243).
If the patient understands and cooperates in performing the test,a forced expiration time of 6 ormore seconds suggests obstructivepulmonary disease.
An increase in the local pain (distant from your hands) suggestsrib fracture rather than just soft tissue injury.

TABLE 6-1 ! Chest Pain
234 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Problem Process Location Quality Severity
CardiovascularAngina Pectoris
Myocardial Infarction
Pericarditis
Dissecting AorticAneurysm
PulmonaryTracheobronchitis
Pleural Pain
Gastrointestinal andother
Reflex EsophagitisDiffuse Esophageal SpasmChest Wall Pain
Anxiety
Temporary myocardialischemia, usually secondary tocoronary atherosclerosis
Prolonged myocardial ischemia,resulting in irreversible muscledamage or necrosis
! Irritation of parietal pleuraadjacent to the pericardium
! Mechanism unclear
A splitting within the layers ofthe aortic wall, allowing passageof blood to dissect a channel
Inflammation of trachea andlarge bronchi
Inflammation of the parietalpleura, as from pleurisy,pneumonia, pulmonaryinfarction, or neoplasm
Inflammation of the esophagealmucosa by reflux of gastric acid
Motor dysfunction of theesophageal muscle
Variable, often unclear
Unclear
Retrosternal or across theanterior chest, sometimesradiating to the shoulders,arms, neck, lower jaw, orupper abdomen
Same as in angina
Precordial, may radiate tothe tip of the shoulderand to the neck
Retrosternal
Anterior chest, radiatingto the neck, back, orabdomen
Upper sternal or on eitherside of the sternum
Chest wall overlying theprocess
Retrosternal, may radiateto the back
Retrosternal, may radiateto the back, arms, and jaw
Often below the leftbreast or along the costalcartilages; also elsewhere
Precordial, below the leftbreast, or across theanterior chest
Pressing, squeezing,tight, heavy,occasionallyburning
Same as in angina
Sharp, knifelike
Crushing
Ripping, tearing
Burning
Sharp, knifelike
Burning, may besqueezing
Usually squeezing
Stabbing, sticking,or dull, aching
Stabbing, sticking,or dull, aching
Mild to moderate,sometimes perceivedas discomfort ratherthan pain
Often but not alwaysa severe pain
Often severe
Severe
Very severe
Mild to moderate
Often severe
Mild to severe
Mild to severe
Variable
Variable
Note: Remember that chest pain may be referred from extrathoracic structures such as the neck (arthritis) and abdomen(biliary colic, acute cholecystitis). Pleural pain may be due to abdominal conditions such as subdiaphragmatic abscess.
TABLE 6-1 ! Chest Pain
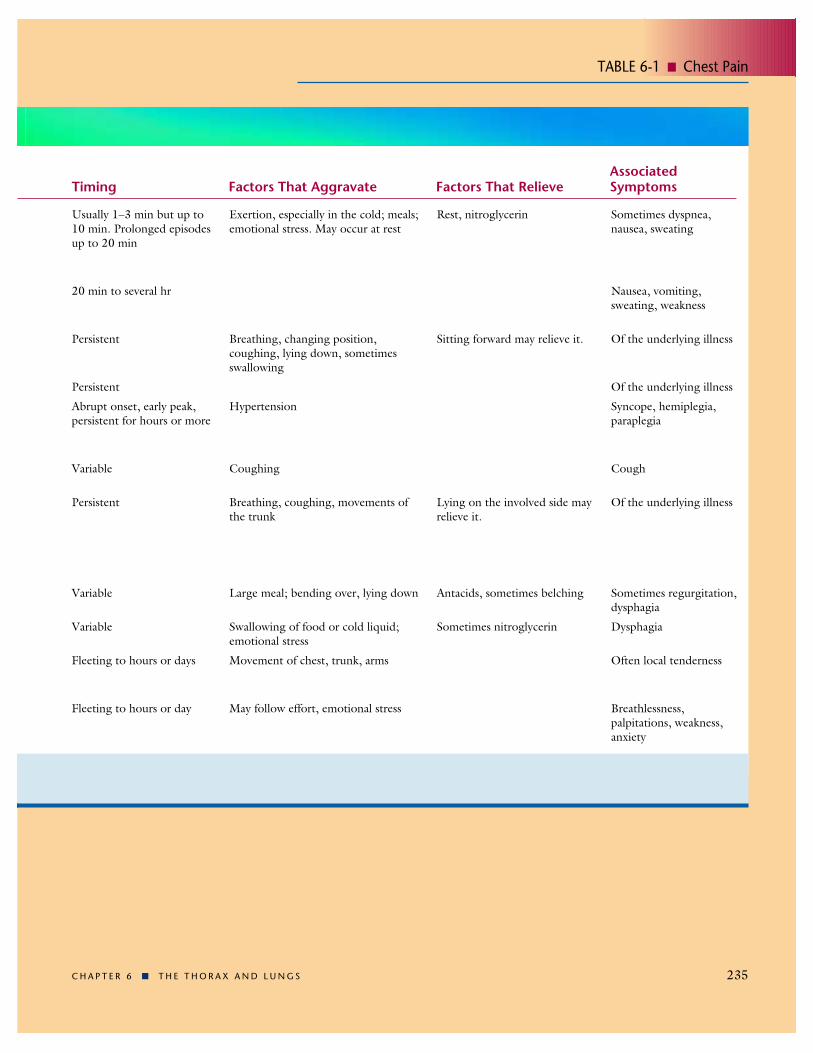
TABLE 6-1 ! Chest Pain
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 235
AssociatedTiming Factors That Aggravate Factors That Relieve Symptoms
Usually 1–3 min but up to10 min. Prolonged episodesup to 20 min
20 min to several hr
Persistent
Persistent
Abrupt onset, early peak,persistent for hours or more
Variable
Persistent
Variable
Variable
Fleeting to hours or days
Fleeting to hours or day
Exertion, especially in the cold; meals;emotional stress. May occur at rest
Breathing, changing position,coughing, lying down, sometimesswallowing
Hypertension
Coughing
Breathing, coughing, movements ofthe trunk
Large meal; bending over, lying down
Swallowing of food or cold liquid;emotional stress
Movement of chest, trunk, arms
May follow effort, emotional stress
Rest, nitroglycerin
Sitting forward may relieve it.
Lying on the involved side mayrelieve it.
Antacids, sometimes belching
Sometimes nitroglycerin
Sometimes dyspnea,nausea, sweating
Nausea, vomiting,sweating, weakness
Of the underlying illness
Of the underlying illness
Syncope, hemiplegia,paraplegia
Cough
Of the underlying illness
Sometimes regurgitation,dysphagia
Dysphagia
Often local tenderness
Breathlessness,palpitations, weakness,anxiety

TABLE 6-2 ! Dyspnea
236 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABLE 6-2 ! Dyspnea
Problem Process Timing
Left-Sided Heart Failure (left ventricular failure or mitral stenosis)
Chronic Bronchitis*
Chronic Obstructive PulmonaryDisease (COPD)*
Asthma
Diffuse Interstitial Lung Diseases(such as sarcoidosis, widespreadneoplasms, asbestosis, andidiopathic pulmonary fibrosis)Pneumonia
Spontaneous Pneumothorax
Acute Pulmonary Embolism
Anxiety With Hyperventilation
Elevated pressure in pulmonary capillarybed with transudation of fluid intointerstitial spaces and alveoli, decreasedcompliance (increased stiffness) of thelungs, increased work of breathing
Excessive mucus production in bronchi,followed by chronic obstruction ofairways
Overdistention of air spaces distal toterminal bronchioles, with destructionof alveolar septa and chronic obstructionof the airways
Bronchial hyperresponsiveness involvingrelease of inflammatory mediators,increased airway secretions, andbronchoconstriction
Abnormal and widespread infiltration ofcells, fluid, and collagen into interstitialspaces between alveoli. Many causes
Inflammation of lung parenchyma fromthe respiratory bronchioles to the alveoli
Leakage of air into pleural spacethrough blebs on visceral pleura, withresulting partial or complete collapse ofthe lung
Sudden occlusion of all or part ofpulmonary arterial tree by a blood clotthat usually originates in deep veins oflegs or pelvis
Overbreathing, with resultantrespiratory alkalosis and fall in thepartial pressure of carbon dioxide in the blood
Dyspnea may progress slowly, orsuddenly as in acute pulmonaryedema.
Chronic productive cough followedby slowly progressive dyspnea
Slowly progressive dyspnea; relativelymild cough later
Acute episodes, separated bysymptom-free periods. Nocturnalepisodes are common.
Progressive dyspnea, which varies inits rate of development with the cause
An acute illness, timing varies withthe causative agent
Sudden onset of dyspnea
Sudden onset of dyspnea
Episodic, often recurrent
*Chronic bronchitis and chronic obstructive pulmonary disease (COPD) may coexist.
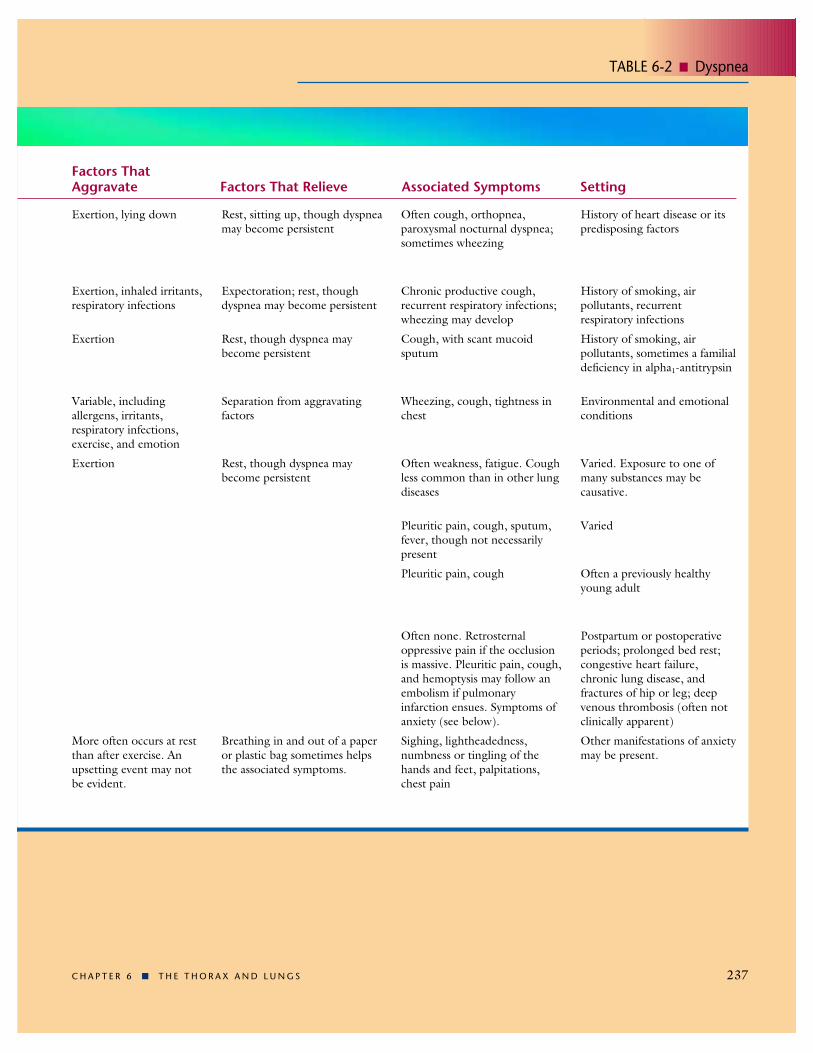
TABLE 6-2 ! Dyspnea
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 237
Factors ThatAggravate Factors That Relieve Associated Symptoms Setting
Exertion, lying down
Exertion, inhaled irritants,respiratory infections
Exertion
Variable, includingallergens, irritants,respiratory infections,exercise, and emotion
Exertion
More often occurs at restthan after exercise. Anupsetting event may not be evident.
Rest, sitting up, though dyspneamay become persistent
Expectoration; rest, thoughdyspnea may become persistent
Rest, though dyspnea maybecome persistent
Separation from aggravatingfactors
Rest, though dyspnea maybecome persistent
Breathing in and out of a paperor plastic bag sometimes helpsthe associated symptoms.
Often cough, orthopnea,paroxysmal nocturnal dyspnea;sometimes wheezing
Chronic productive cough,recurrent respiratory infections;wheezing may develop
Cough, with scant mucoidsputum
Wheezing, cough, tightness inchest
Often weakness, fatigue. Coughless common than in other lungdiseases
Pleuritic pain, cough, sputum,fever, though not necessarilypresent
Pleuritic pain, cough
Often none. Retrosternaloppressive pain if the occlusionis massive. Pleuritic pain, cough,and hemoptysis may follow anembolism if pulmonaryinfarction ensues. Symptoms ofanxiety (see below).
Sighing, lightheadedness,numbness or tingling of thehands and feet, palpitations,chest pain
History of heart disease or itspredisposing factors
History of smoking, airpollutants, recurrentrespiratory infections
History of smoking, airpollutants, sometimes a familialdeficiency in alpha1-antitrypsin
Environmental and emotionalconditions
Varied. Exposure to one ofmany substances may becausative.
Varied
Often a previously healthyyoung adult
Postpartum or postoperativeperiods; prolonged bed rest;congestive heart failure,chronic lung disease, andfractures of hip or leg; deepvenous thrombosis (often notclinically apparent)
Other manifestations of anxietymay be present.

TABLE 6-3 ! Cough and Hemoptysis
238 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABLE 6-3 ! Cough and Hemoptysis*
Problem Cough and Sputum Associated Symptoms and Setting
Acute InflammationLaryngitis
Tracheobronchitis
Mycoplasma and ViralPneumoniasBacterial Pneumonias
Chronic InflammationPostnasal Drip
Chronic Bronchitis
Bronchiectasis
Pulmonary Tuberculosis
Lung Abscess
Asthma
Gastroesophageal Reflux
NeoplasmCancer of the Lung
Cardiovascular DisordersLeft Ventricular Failure or Mitral Stenosis
Pulmonary Emboli
Irritating Particles,Chemicals, or Gases
Dry cough (without sputum), may becomeproductive of variable amounts of sputum
Dry cough, may become productive (asabove)
Dry hacking cough, often becomingproductive of mucoid sputum
Pneumococcal: sputum mucoid orpurulent; may be blood-streaked, diffuselypinkish, or rusty
Klebsiella: similar; or sticky, red, and jellylike
Chronic cough; sputum mucoid ormucopurulent
Chronic cough; sputum mucoid topurulent, may be blood-streaked or evenbloody
Chronic cough; sputum purulent, oftencopious and foul-smelling; may be blood-streaked or bloody
Cough dry or sputum that is mucoid orpurulent; may be blood-streaked or bloody
Sputum purulent and foul-smelling; may bebloody
Cough, with thick mucoid sputum,especially near end of an attack
Chronic cough, especially at night or earlyin the morning
Cough dry to productive; sputum may beblood-streaked or bloody
Often dry, especially on exertion or at night;may progress to the pink frothy sputum ofpulmonary edema or to frank hemoptysis
Dry to productive; may be dark, bright red,or mixed with blood
Variable. There may be a latent periodbetween exposure and symptoms.
An acute, fairly minor illness with hoarseness.Often associated with viral nasopharyngitis
An acute, often viral illness, with burningretrosternal discomfort
An acute febrile illness, often with malaise,headache, and possibly dyspnea
An acute illness with chills, high fever,dyspnea, and chest pain. Often is preceded byacute upper respiratory infection.
Typically occurs in older alcoholic men
Repeated attempts to clear the throat.Postnasal discharge may be sensed by patientor seen in posterior pharynx. Associated withchronic rhinitis, with or without sinusitis
Often longstanding cigarette smoking.Recurrent superimposed infections. Wheezingand dyspnea may develop.
Recurrent bronchopulmonary infectionscommon; sinusitis may coexist
Early, no symptoms. Later, anorexia, weightloss, fatigue, fever, and night sweats
A febrile illness. Often poor dental hygieneand a prior episode of impaired consciousness
Episodic wheezing and dyspnea, but coughmay occur alone. Often a history of allergy
Wheezing, especially at night (often mistakenfor asthma), early morning hoarseness, andrepeated attempts to clear the throat. Often ahistory of heartburn and regurgitation
Usually a long history of cigarette smoking.Associated manifestations are numerous.
Dyspnea, orthopnea, paroxysmal nocturnaldyspnea
Dyspnea, anxiety, chest pain, fever; factorsthat predispose to deep venous thrombosis
Exposure to irritants. Eyes, nose, and throatmay be affected.
*Characteristics of hemoptysis are printed in red.
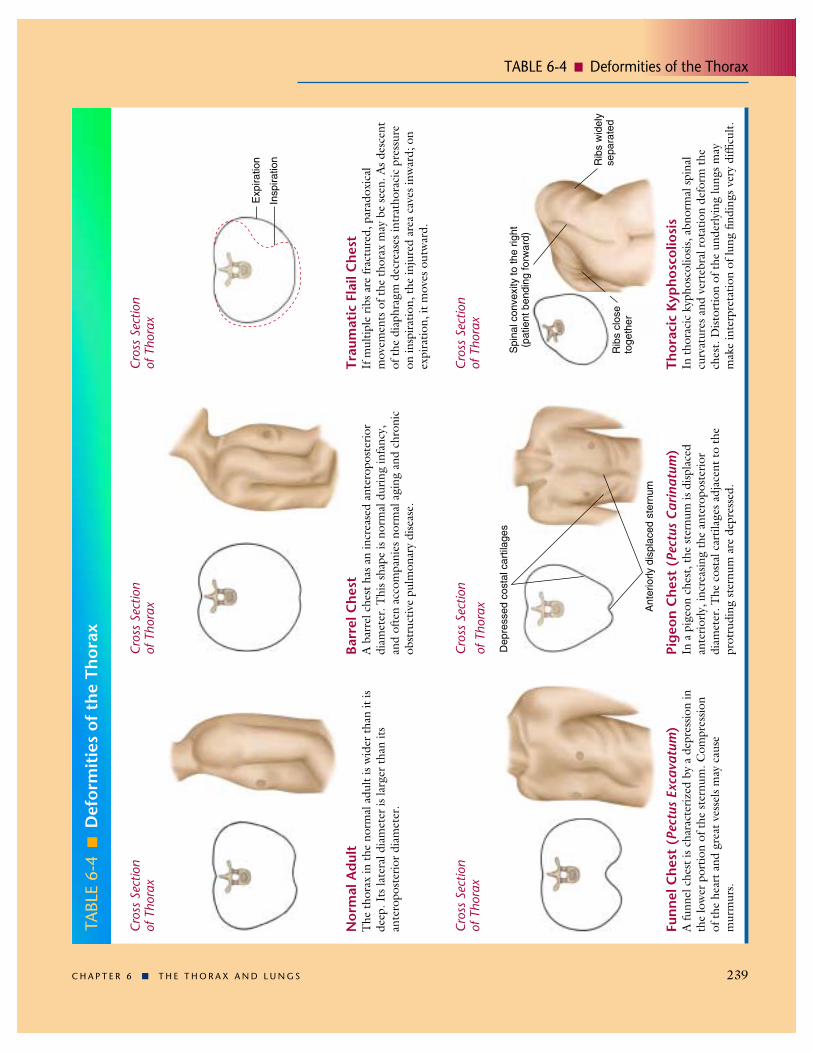
TABLE 6-4 ! Deformities of the Thorax
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 239
TABL
E 6-
4!
Def
orm
itie
s of
the
Tho
rax
Nor
mal
Adu
ltT
he th
orax
in th
e no
rmal
adu
lt is
wid
er th
an it
isde
ep. I
ts la
tera
l dia
met
er is
larg
er th
an it
san
tero
post
erio
r dia
met
er.
Barr
el C
hest
A b
arre
l che
st h
as a
n in
crea
sed
ante
ropo
ster
ior
diam
eter
. Thi
s sha
pe is
nor
mal
dur
ing
infa
ncy,
and
ofte
n ac
com
pani
es n
orm
al a
ging
and
chr
onic
obst
ruct
ive
pulm
onar
y di
seas
e.
Trau
mat
ic F
lail
Che
stIf
mul
tiple
ribs
are
frac
ture
d, p
arad
oxic
alm
ovem
ents
of t
he th
orax
may
be
seen
. As d
esce
ntof
the
diap
hrag
m d
ecre
ases
intr
atho
raci
c pr
essu
reon
insp
iratio
n, th
e in
jure
d ar
ea c
aves
inw
ard;
on
expi
ratio
n, it
mov
es o
utw
ard.
Exp
iratio
n
Insp
iratio
n
Cros
s Se
ctio
n of
Tho
rax
Cros
s Se
ctio
n of
Tho
rax
Cros
s Se
ctio
n of
Tho
rax
Funn
el C
hest
(Pe
ctus
Exc
avat
um)
A fu
nnel
che
st is
cha
ract
eriz
ed b
y a
depr
essio
n in
the
low
er p
ortio
n of
the
ster
num
. Com
pres
sion
of th
e he
art a
nd g
reat
ves
sels
may
cau
sem
urm
urs.
Pige
on C
hest
(Pe
ctus
Car
inat
um)
In a
pig
eon
ches
t, th
e st
ernu
m is
disp
lace
dan
terio
rly, i
ncre
asin
g th
e an
tero
post
erio
rdi
amet
er. T
he c
osta
l car
tilag
es a
djac
ent t
o th
epr
otru
ding
ster
num
are
dep
ress
ed.
Dep
ress
ed c
osta
l car
tilag
es
Ant
erio
rly d
ispl
aced
ste
rnum
Thor
acic
Kyp
hosc
olio
sis
In th
orac
ic k
ypho
scol
iosis
, abn
orm
al sp
inal
curv
atur
es a
nd v
erte
bral
rota
tion
defo
rm th
ech
est.
Dist
ortio
n of
the
unde
rlyin
g lu
ngs m
aym
ake
inte
rpre
tatio
n of
lung
find
ings
ver
y di
fficu
lt.
Cros
s Se
ctio
n of
Tho
rax
Cros
s Se
ctio
nof
Tho
rax
Cros
s Se
ctio
n of
Tho
rax
Rib
s w
idel
yse
para
ted
Spi
nal c
onve
xity
to th
e rig
ht(p
atie
nt b
endi
ng fo
rwar
d)
Rib
s cl
ose
toge
ther

TABLE 6-5 ! Normal and Altered Breath and Voice Sounds
240 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABL
E 6-
5!
Nor
mal
and
Alt
ered
Bre
ath
and
Voic
e So
unds
The
orig
ins o
f bre
ath
soun
ds a
re st
ill u
ncle
ar. A
ccor
ding
to le
adin
g th
eorie
s, tu
r-bu
lent
air
flow
in th
e ce
ntra
l airw
ays
prod
uces
the
trac
heal
and
bro
nchi
al b
reat
hso
unds
. As
thes
e so
unds
pas
s th
roug
h th
e lu
ngs
to th
e pe
riphe
ry, l
ung
tissu
e fil
-te
rs o
ut t
heir
high
er-p
itche
d co
mpo
nent
s an
d on
ly t
he s
oft
and
low
er-p
itche
dco
mpo
nent
s rea
ch th
e ch
est w
all,
whe
re th
ey a
re h
eard
as v
esic
ular
bre
ath
soun
ds.
Nor
mal
ly, t
rach
eal a
nd b
ronc
hial
soun
ds m
ay b
e he
ard
over
the
trac
hea
and
mai
n-st
em b
ronc
hi; v
esic
ular
bre
ath
soun
ds p
redo
min
ate
thro
ugho
ut m
ost o
f the
lung
s.
Whe
n lu
ng ti
ssue
lose
s its
air,
it tr
ansm
its h
igh-
pitc
hed
soun
ds m
uch
bett
er. I
f the
trac
heob
ronc
hial
tre
e is
open
, bro
nchi
al b
reat
h so
unds
may
rep
lace
the
nor
mal
vesic
ular
soun
ds o
ver a
irles
s are
as o
f the
lung
. Thi
s cha
nge
is se
en in
loba
r pne
u-m
onia
whe
n th
e al
veol
i fill
with
flui
d, r
ed c
ells,
and
whi
te c
ells—
a pr
oces
s ca
lled
cons
olid
atio
n.O
ther
cau
ses
incl
ude
pulm
onar
y ed
ema
or h
emor
rhag
e. B
ronc
hial
brea
th s
ound
s us
ually
cor
rela
te w
ith a
n in
crea
se in
tact
ile fr
emitu
s an
d tr
ansm
it-te
d vo
ice
soun
ds. T
hese
find
ings
are
sum
mar
ized
bel
ow.
Nor
mal
Air
-Fill
ed L
ung
Air
less
Lun
g, a
s in
Lob
ar P
neum
onia
Brea
th S
ound
sTr
ansm
itte
d V
oice
Sou
nds
Tact
ile F
rem
itus
Pred
omin
antly
ves
icul
ar
Spok
en w
ords
muf
fled
and
indi
stin
ctSp
oken
“ee
” he
ard
as “
ee”
Whi
sper
ed w
ords
fain
t and
indi
stin
ct, i
f hea
rd a
t all
Nor
mal
Bro
nchi
al o
r bro
ncho
vesic
ular
ove
r the
invo
lved
are
a
Spok
en w
ords
loud
er, c
lear
er (
bron
chop
hony
)Sp
oken
“ee
” he
ard
as “
ay”
(ego
phon
y)W
hisp
ered
wor
ds lo
uder
, cle
arer
(w
hisp
ered
pec
tori
loqu
y)
Incr
ease
d

TABLE 6-6 ! Adventitious (Added) Lung Sounds: Causes and Qualities
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 241
TABL
E 6-
6!
Adv
enti
tiou
s (A
dded
) Lu
ng S
ound
s: C
ause
s an
d Q
ualit
ies
Cra
ckle
sC
rack
les h
ave
two
lead
ing
expl
anat
ions
. (1)
The
y re
sult
from
a se
ries o
f tin
y ex
plos
ions
whe
n sm
all a
irway
s, de
flate
d du
ring
expi
ratio
n, p
op o
pen
durin
g in
spira
tion.
Thi
s mec
hani
sm p
roba
bly
expl
ains
the
late
insp
irato
ry c
rack
les o
f int
erst
itial
lung
dise
ase
and
early
con
gest
ive
hear
t fai
lure
. (2)
Cra
ckle
s res
ult f
rom
air
bubb
les
flow
ing
thro
ugh
secr
etio
ns o
r lig
htly
clo
sed
airw
ays d
urin
g re
spira
tion.
Thi
s mec
hani
sm p
roba
bly
expl
ains
at l
east
som
e co
arse
cra
ckle
s.
Whe
ezes
and
Rho
nchi
Stri
dor
Pleu
ral R
ub
Med
iast
inal
Cru
nch
(Ham
man
’s S
ign)
Insp
iratio
nE
xpira
tion
Late
insp
irat
ory c
rack
lesm
ay b
egin
in th
e fir
st h
alf o
f ins
pira
tion
but m
ust c
ontin
ue in
to la
te in
spira
tion.
The
y ar
eus
ually
fine
and
fairl
y pr
ofus
e, a
nd p
ersis
t fro
m b
reat
h to
bre
ath.
The
se c
rack
les a
ppea
r firs
t at t
he b
ases
of t
he lu
ngs,
spre
ad u
pwar
d as
the
cond
ition
wor
sens
, and
shift
to d
epen
dent
regi
ons w
ith c
hang
es in
pos
ture
. Cau
ses i
nclu
dein
ters
titia
l lun
g di
seas
e (s
uch
as fi
bros
is) a
nd e
arly
con
gest
ive
hear
t fai
lure
.
Earl
y ins
pira
tory
crac
kles
appe
ar so
on a
fter t
he st
art o
f ins
pira
tion
and
do n
ot c
ontin
ue in
to la
te in
spira
tion.
The
y ar
eof
ten
but n
ot a
lway
s coa
rse
and
are
rela
tivel
y fe
w in
num
ber.
Exp
irato
ry c
rack
les a
re so
met
imes
ass
ocia
ted.
Cau
ses
incl
ude
chro
nic
bron
chiti
s and
ast
hma.
Mid
insp
irat
ory a
nd ex
pira
tory
crac
kles
are
hear
d in
bro
nchi
ecta
sis b
ut a
re n
ot sp
ecifi
c fo
r thi
s dia
gnos
is. W
heez
es a
ndrh
onch
i may
be
asso
ciat
ed.
Whe
ezes
occ
ur w
hen
air fl
ows r
apid
ly th
roug
h br
onch
i tha
t are
nar
row
ed n
early
to th
e po
int o
f clo
sure
. The
y ar
e of
ten
audi
ble
at th
e m
outh
as w
ell a
s thr
ough
the
ches
t wal
l. C
ause
s of w
heez
es th
at a
re g
ener
aliz
ed th
roug
hout
the
ches
tin
clud
e as
thm
a, c
hron
ic b
ronc
hitis
, CO
PD, a
nd c
onge
stiv
e he
art f
ailu
re (
card
iac
asth
ma)
. In
asth
ma,
whe
ezes
may
be
hear
d on
ly in
exp
iratio
n or
in b
oth
phas
es o
f the
resp
irato
ry c
ycle
. Rho
nchi
sugg
est s
ecre
tions
in th
e la
rger
airw
ays.
Inch
roni
c br
onch
itis,
whe
ezes
and
rhon
chi o
ften
clea
r with
cou
ghin
g.
Occ
asio
nally
in se
vere
obs
truc
tive
pulm
onar
y di
seas
e, th
e pa
tient
is n
o lo
nger
abl
e to
forc
e en
ough
air
thro
ugh
the
narr
owed
bro
nchi
to p
rodu
ce w
heez
ing.
The
resu
lting
sile
nt ch
ests
houl
d ra
ise im
med
iate
con
cern
and
not
be
mist
aken
for i
mpr
ovem
ent.
A p
ersis
tent
loca
lized
whe
eze
sugg
ests
a p
artia
l obs
truc
tion
of a
bro
nchu
s, as
by
a tu
mor
or f
orei
gn b
ody.
It m
ay b
ein
spira
tory
, exp
irato
ry, o
r bot
h.
A w
heez
e th
at is
ent
irely
or p
redo
min
antly
insp
irato
ry is
cal
led
strid
or.I
t is o
ften
loud
er in
the
neck
than
ove
r the
ches
t wal
l. It
indi
cate
s a p
artia
l obs
truc
tion
of th
e la
rynx
or t
rach
ea, a
nd d
eman
ds im
med
iate
att
entio
n.
Infla
med
and
roug
hene
d pl
eura
l sur
face
s gra
te a
gain
st e
ach
othe
r as t
hey
are
mom
enta
rily
and
repe
ated
ly d
elay
ed b
yin
crea
sed
fric
tion.
The
se m
ovem
ents
pro
duce
cre
akin
g so
unds
kno
wn
as a
ple
ural
rub
(or p
leur
al fr
ictio
n ru
b).
Pleu
ral r
ubs r
esem
ble
crac
kles
aco
ustic
ally
, alth
ough
they
are
pro
duce
d by
diff
eren
t pat
holo
gic
proc
esse
s. T
he so
unds
may
be
disc
rete
, but
som
etim
es a
re so
num
erou
s tha
t the
y m
erge
into
a se
emin
gly
cont
inuo
us so
und.
Aru
b is
usua
lly c
onfin
ed to
a re
lativ
ely
smal
l are
a of
the
ches
t wal
l, an
d ty
pica
lly is
hea
rd in
bot
h ph
ases
of r
espi
ratio
n.W
hen
infla
med
ple
ural
surf
aces
are
sepa
rate
d by
flui
d, th
e ru
b of
ten
disa
ppea
rs.
A m
edia
stina
l cru
nch
is a
serie
s of p
reco
rdia
l cra
ckle
s syn
chro
nous
with
the
hear
t bea
t, no
t with
resp
iratio
n. B
est
hear
d in
the
left
late
ral p
ositi
on, i
t is d
ue to
med
iast
inal
em
phys
ema
(pne
umom
edia
stin
um).
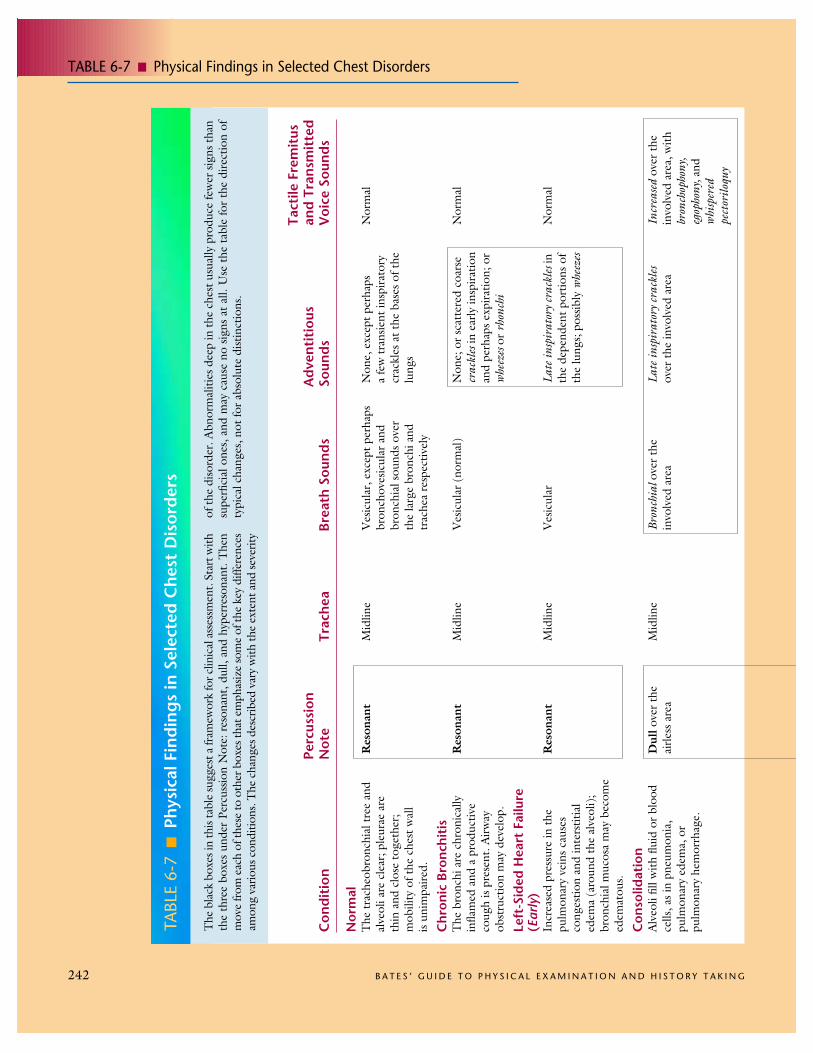
TABLE 6-7 ! Physical Findings in Selected Chest Disorders
242 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABL
E 6-
7!
Phys
ical
Fin
ding
s in
Sel
ecte
d C
hest
Dis
orde
rs
The
bla
ck b
oxes
in th
is ta
ble
sugg
est a
fram
ewor
k fo
r clin
ical
ass
essm
ent.
Star
t with
the
thre
e bo
xes
unde
r Pe
rcus
sion
Not
e: r
eson
ant,
dull,
and
hyp
erre
sona
nt. T
hen
mov
e fro
m e
ach
of th
ese
to o
ther
box
es th
at e
mph
asiz
e so
me
of th
e ke
y di
ffere
nces
amon
g va
rious
con
ditio
ns. T
he c
hang
es d
escr
ibed
var
y w
ith th
e ex
tent
and
seve
rity
of th
e di
sord
er. A
bnor
mal
ities
dee
p in
the
ches
t usu
ally
pro
duce
few
er si
gns t
han
supe
rfici
al o
nes,
and
may
cau
se n
o sig
ns a
t all.
Use
the
tabl
e fo
r th
e di
rect
ion
ofty
pica
l cha
nges
, not
for a
bsol
ute
dist
inct
ions
.
Tact
ile F
rem
itus
Perc
ussi
onA
dven
titi
ous
and
Tran
smit
ted
Con
diti
onN
ote
Trac
hea
Brea
th S
ound
sSo
unds
Voi
ce S
ound
s
Nor
mal
The
trac
heob
ronc
hial
tree
and
alve
oli a
re c
lear
; ple
urae
are
thin
and
clo
se to
geth
er;
mob
ility
of t
he c
hest
wal
lis
unim
paire
d.
Chr
onic
Bro
nchi
tis
The
bro
nchi
are
chr
onic
ally
infla
med
and
a p
rodu
ctiv
eco
ugh
is pr
esen
t. A
irway
obst
ruct
ion
may
dev
elop
.
Left
-Sid
ed H
eart
Fai
lure
(E
arly
)In
crea
sed
pres
sure
in th
epu
lmon
ary
vein
s cau
ses
cong
estio
n an
d in
ters
titia
led
ema
(aro
und
the
alve
oli);
bron
chia
l muc
osa
may
bec
ome
edem
atou
s.
Con
solid
atio
nA
lveo
li fil
l with
flui
d or
blo
odce
lls, a
s in
pneu
mon
ia,
pulm
onar
y ed
ema,
or
pulm
onar
y he
mor
rhag
e.
Res
onan
t
Res
onan
t
Res
onan
t
Dul
love
r the
airle
ss a
rea
Mid
line
Mid
line
Mid
line
Mid
line
Ves
icul
ar, e
xcep
t per
haps
bron
chov
esic
ular
and
bron
chia
l sou
nds o
ver
the
larg
e br
onch
i and
trac
hea
resp
ectiv
ely
Ves
icul
ar (
norm
al)
Ves
icul
ar
Bron
chia
l ove
r the
invo
lved
are
a
Non
e, e
xcep
t per
haps
a
few
tran
sient
insp
irato
rycr
ackl
es a
t the
bas
es o
f the
lung
s
Non
e; o
r sca
tter
ed c
oars
ecr
ackl
esin
ear
ly in
spira
tion
and
perh
aps e
xpira
tion;
or
whe
ezes
or r
honc
hi
Late
insp
irat
ory c
rack
les i
nth
e de
pend
ent p
ortio
ns o
fth
e lu
ngs;
poss
ibly
whe
ezes
Late
insp
irat
ory c
rack
les
over
the
invo
lved
are
a
Nor
mal
Nor
mal
Nor
mal
Incr
ease
dov
er th
ein
volv
ed a
rea,
with
bron
chop
hony
,eg
opho
ny, a
ndw
hisp
ered
pect
orilo
quy

TABLE 6-7 ! Physical Findings in Selected Chest Disorders
C H A P T E R 6 ! T H E T H O R A X A N D L U N G S 243
Ate
lect
asis
(L
obar
Obs
truc
tion)
Whe
n a
plug
in a
mai
nste
mbr
onch
us (
as fr
om m
ucus
or a
fore
ign
obje
ct)
obst
ruct
s air
flow
, affe
cted
lung
tiss
ueco
llaps
es in
to a
n ai
rless
stat
e.
Pleu
ral E
ffus
ion
Flui
d ac
cum
ulat
es in
the
pleu
ral s
pace
, sep
arat
es a
ir-fil
led
lung
from
the
ches
t wal
l,bl
ocki
ng th
e tr
ansm
issio
n of
soun
d.
Pneu
mot
hora
xW
hen
air l
eaks
into
the
pleu
ral
spac
e, u
sual
ly u
nila
tera
lly, t
helu
ng re
coils
from
the
ches
tw
all.
Pleu
ral a
ir bl
ocks
tran
smiss
ion
of so
und.
Chr
onic
Obs
truc
tive
Pulm
onar
y D
isea
se(C
OPD
)Sl
owly
pro
gres
sive
diso
rder
inw
hich
the
dist
al a
ir sp
aces
enla
rge
and
lung
s bec
ome
hype
rinfla
ted.
Chr
onic
bron
chiti
s is o
ften
asso
ciat
ed.
Ast
hma
Wid
espr
ead
narr
owin
g of
the
trac
heob
ronc
hial
tree
dim
inish
es a
irflow
to a
fluct
uatin
g de
gree
. Dur
ing
atta
cks,
airfl
ow d
ecre
ases
furt
her a
nd lu
ngs h
yper
infla
te.
Dul
love
r the
airle
ss a
rea
Dul
l to
flat
over
the
fluid
Hyp
erre
sona
ntor
tym
pani
ticov
er th
e pl
eura
lai
r
Diff
usel
yhy
perr
eson
ant
Res
onan
tto
diffu
sely
hype
rres
onan
t
Usu
ally
abs
entw
hen
bron
chia
l plu
g pe
rsist
s.E
xcep
tions
incl
ude
right
uppe
r lob
e at
elec
tasis
,w
here
adj
acen
t tra
chea
lso
unds
may
be
tran
smitt
ed.
Dec
reas
ed to
abs
ent,
but
bron
chia
l bre
ath
soun
dsm
ay b
e he
ard
near
top
ofla
rge
effu
sion.
Dec
reas
ed to
abs
ento
ver
the
pleu
ral a
ir
Dec
reas
ed to
abs
ent
Oft
en o
bscu
red
by w
heez
es
Usu
ally
abs
entw
hen
the
bron
chia
l plu
gpe
rsist
s. In
exce
ptio
ns, e
.g.,
right
upp
er lo
beat
elec
tasis
, may
be
incr
ease
d
Dec
reas
ed to
abs
ent,
but m
ay b
e inc
reas
edto
war
d th
e to
p of
ala
rge
effu
sion
Dec
reas
ed to
abs
ent
over
the
pleu
ral a
ir
Dec
reas
ed
Dec
reas
ed
May
be
shift
edto
war
d in
volv
edsid
e
Shift
ed to
war
dop
posit
e sid
e in
ala
rge
effu
sion
Shift
edto
war
dop
posit
e sid
eif
muc
h ai
r
Mid
line
Mid
line
Non
e
Non
e, e
xcep
t a p
ossib
lepl
eura
lrub
Non
e, e
xcep
t a p
ossib
lepl
eura
l rub
Non
e, o
r the
cra
ckle
s,w
heez
es, a
nd rh
onch
i of
asso
ciat
ed c
hron
icbr
onch
itis
Whe
ezes
, pos
sibly
crac
kles