the stepped wedge cluster randomised trial workshop: session 2
TRANSCRIPT

Introduction: what is the SW-CRT?
Defining features, common variations, and some salient
examples
Karla Hemming
30/08/2016

Why do we need another method of
evaluation?

Evaluation of policy and service delivery
interventions
• The Matching Michigan Study– Secular trend
– Intervention effect
• The Oregon Experiment – Randomised
– No primary outcome
• Mexican universal health
insurance– 74 matched clusters
– Staggered implementation

Evidence based policy interventions
Working constraints
• Stakeholder’s desires
• Pragmatic limitations
• A priori beliefs
How the SW-CRT can help
• All clusters ultimately get
intervention
• Sequential roll out
• Robust evaluation

What is the SW-CRT?

The Stepped Wedge Cluster Randomised Trial
Example 1: A cross-sectional SW-CRT
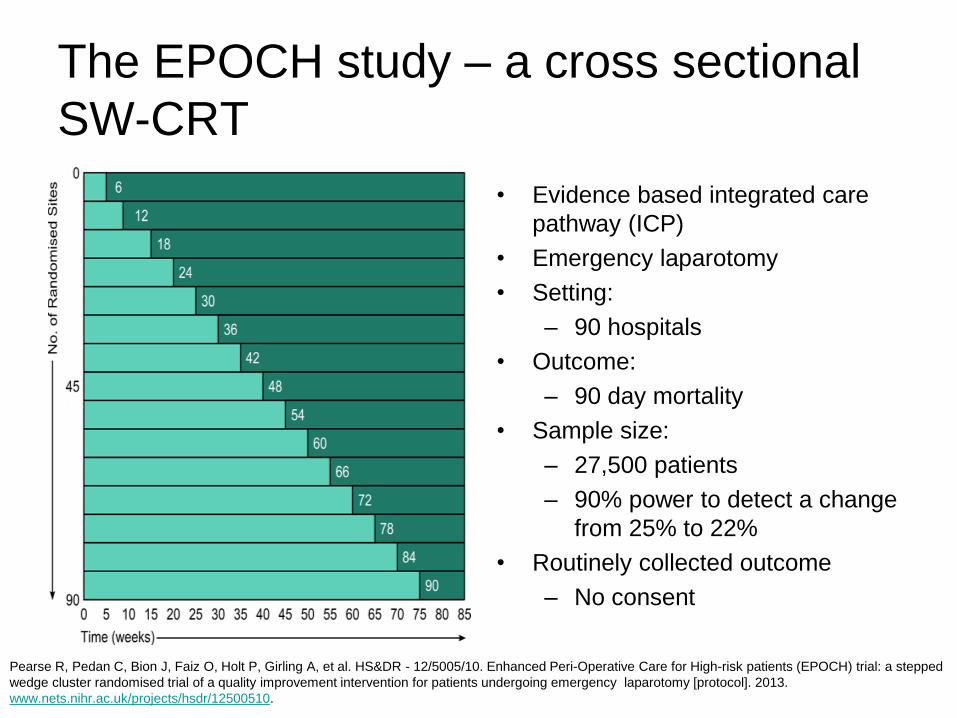
The EPOCH study – a cross sectional
SW-CRT
• Evidence based integrated care
pathway (ICP)
• Emergency laparotomy
• Setting:
– 90 hospitals
• Outcome:
– 90 day mortality
• Sample size:
– 27,500 patients
– 90% power to detect a change
from 25% to 22%
• Routinely collected outcome
– No consent
Pearse R, Pedan C, Bion J, Faiz O, Holt P, Girling A, et al. HS&DR - 12/5005/10. Enhanced Peri-Operative Care for High-risk patients (EPOCH) trial: a stepped
wedge cluster randomised trial of a quality improvement intervention for patients undergoing emergency laparotomy [protocol]. 2013.
www.nets.nihr.ac.uk/projects/hsdr/12500510.

Example 2: A cohort SW-CRT

Depression management– a cohort
SW-CRT
• Structural multidisciplinary approach
to depression management
• Participants – Residents who provided informed consent
• Setting:– 33 units within nursing homes (Dementia /
Somatic)
• Outcome:– Depression prevalence
• Sample size:– 793 patients
– 80% power to detect a 30 to 40% reduction
in prevalence (circa 20-30%)
• Outcome– Questionnaire (Cornell scale for
depression)
Leontjevas R, Gerritsen DL, Smalbrugge M, Teerenstra S, Vernooij-Dassen MJ, Koopmans RT. A structural multidisciplinary approach to depression
management in nursing-home residents: a multicentre, stepped-wedge cluster-randomised trial. Lancet. 2013 Jun 9;381(9885):2255-64. doi:
10.1016/S0140-6736(13)60590-5. Epub 2013 May 2. PubMed PMID: 23643110.

Example 3 – the Gambia hepatitis
study

The Gambia hepatitis study
• Step lengths 10 to 12 weeks
• National coverage after 4 years
• Geographically defined areas
• Study started 1980s
– 30 year follow-up
• Vaccine
– efficacy against hep B
• Main outcome
– liver disease
• Vaccine rolled out
– national infant
vaccination schedule

Is the SW-CRT the right design for my
trial?
• Pragmatic considerations
– Does it allow a randomised evaluation which otherwise would
not be possible?
• Logistical considerations
– Allows sequential role out
• Efficiency
– Minimise number clusters / participants / observations
• Duration
– Will it necessarily extend the trial?
– Time between exposure and follow-up

Word of caution …
• Lack of concealment
of allocation
– Risk of selection bias
• Avoid individual
patient recruitment
– Routinely collected
outcome data
Chalmers:
“Although one of the reasons that the streptomycin trial has become iconic is …
random number tables …. it was because successful concealment of allocation”
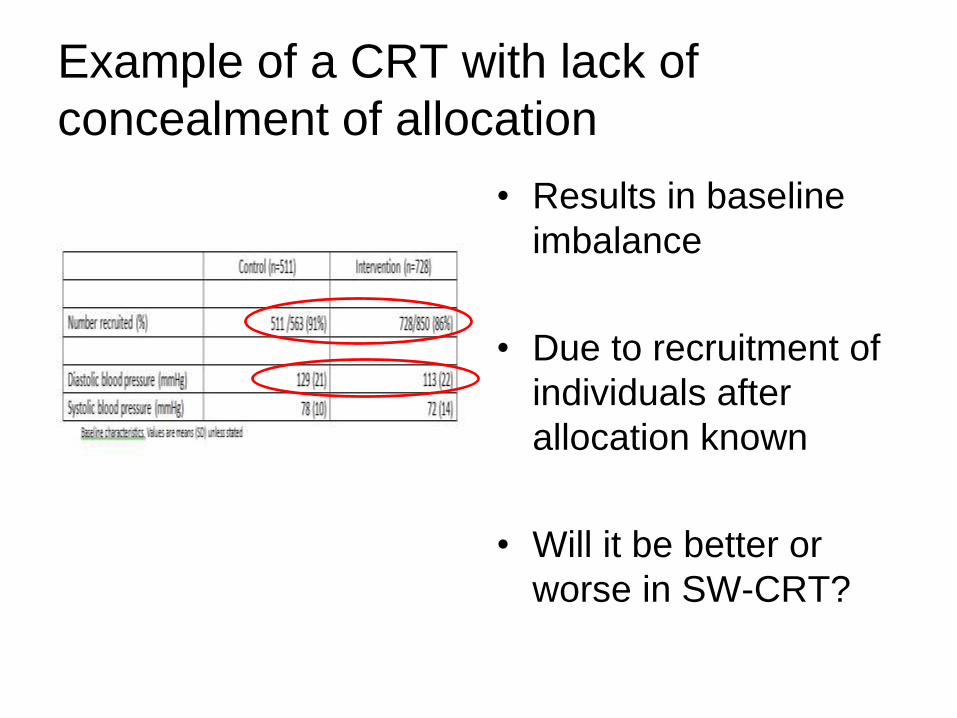
Example of a CRT with lack of
concealment of allocation
• Results in baseline
imbalance
• Due to recruitment of
individuals after
allocation known
• Will it be better or
worse in SW-CRT?

Variations to the common design
• More than two treatment comparisons
• Hybrid designs – mixtures of parallel designs and stepped studies
• Transition periods
• Multiple levels (i.e. clustering within clustering)
• Repeated measures (cohort designs)
To follow….
• What sample size do I need?
• What is the most efficient design?
• How to extend the design to all for more than two treatments?
• How do I analyse a SW-CRT?

Summary
• SW-CRT a pragmatic study design which reconciles the need for
robust evaluations with political or logistical constraints.
• Unbiased design when:
– No individual patient recruitment (routinely collected outcome)
• Efficient design when:
– Higher the ICC (process outcomes)
– Limited number of clusters
• Design and analysis
– Appropriate consideration of time effects in power and analysis

References 1 (methodology)
• Mdege ND, Man MS, Brown CATN, Torgerson DJ. Systematic review of stepped wedge cluster
randomized trials shows that design is particularly used to evaluate interventions during routine
implementation. Journal of Clinical Epidemiology 2011; 64:936–948.
• Hemming K, Haines TP, Chilton PJ, Girling AJ, Lilford RJ. The stepped wedge cluster randomised
trial: rationale, design, analysis, and reporting. BMJ. 2015 Feb 6;350:h391. doi: 10.1136/bmj.h391.
PubMed PMID: 25662947.
• Hussey MA, Hughes JP. Design and analysis of stepped wedge cluster randomized trials.
Contemp Clin Trials. 2007;28(2):182-91.

References 2 (motivating examples)
• Bion J, Richardson A, Hibbert P, Beer J, Abrusci T, McCutcheon M, et al. ‘Matching Michigan’: a
2-year stepped interventional programme to minimise central venous catheter-blood stream
infections in intensive care units in England. BMJ Qual Saf2013;22:110-23
• Baicker K, Taubman SL, Allen HL, Bernstein M, Gruber JH, Newhouse JP, Schneider EC, Wright
BJ, Zaslavsky AM, Finkelstein AN; Oregon Health Study Group, Carlson M, Edlund T, Gallia C,
Smith J. The Oregon experiment--effects of Medicaid on clinical outcomes. N Engl J Med. 2013
May 2;368(18):1713-22. doi: 10.1056/NEJMsa1212321. PubMed PMID: 23635051; PubMed
Central PMCID: PMC3701298.
• King G, Gakidou E, Imai K, Lakin J, Moore RT, Nall C, Ravishankar N, Vargas M, Téllez-Rojo
MM, Avila JE, Avila MH, Llamas HH. Public policy for the poor? A randomised assessment of the
Mexican universal health insurance programme. Lancet. 2009 Apr 25;373(9673):1447-54. doi:
10.1016/S0140-6736(09)60239-7. Epub 2009 Apr 7. PubMed PMID: 19359034.