the role of public health in school fruit scheme – slovene...
TRANSCRIPT
The role of Public Health in School Fruit Scheme –
Slovene experience
DG AGRI, Management Committee, 'SFS'Brussels, 11 December 2007
Mojca Gabrijelčič BlenkušNational Institute of Public Health of the R of Slovenia
With the contribution of:Ministry of Agriculture, Forestry and Food of the R of Slovenia
Ministry of Education and Sport of the R of SloveniaMinistry of Health of the R of Slovenia
I. Role of Public Health
II. Working together
III. National school mealprogram and “Apple”project - Slovenia
IV. Conclusions
Presentation outline

I. Role of Public Health

Food and
health
Diets determine nutritional status
Nutritional status determines healthBalanced diets are essential to good healthUnsafe foods generate disease
Source: FAO presentation to WHO meeting, Paris, June 2007

Lost years of healthy life in Europe 2000
Source: Food and health in Europe 2004, The world health report 2000Sec. source: WHO presentation, 2006
Diseases with major nutritional determinants (F/V play major role)
41%
Other diseases
21%
Diseases in which nutrition plays a role 38%
CVD 61%
Diabetes mellitus 5%
Malignant neoplasms32%
Nutrition deficiencies 2%

Agriculture policies and practices
Agriculture policiesand agricultureproduction practices
Influence what farmers choose to grow
Could influence what consumers choose to eat
Source: FAO presentation to WHO meeting, Paris, June 2007
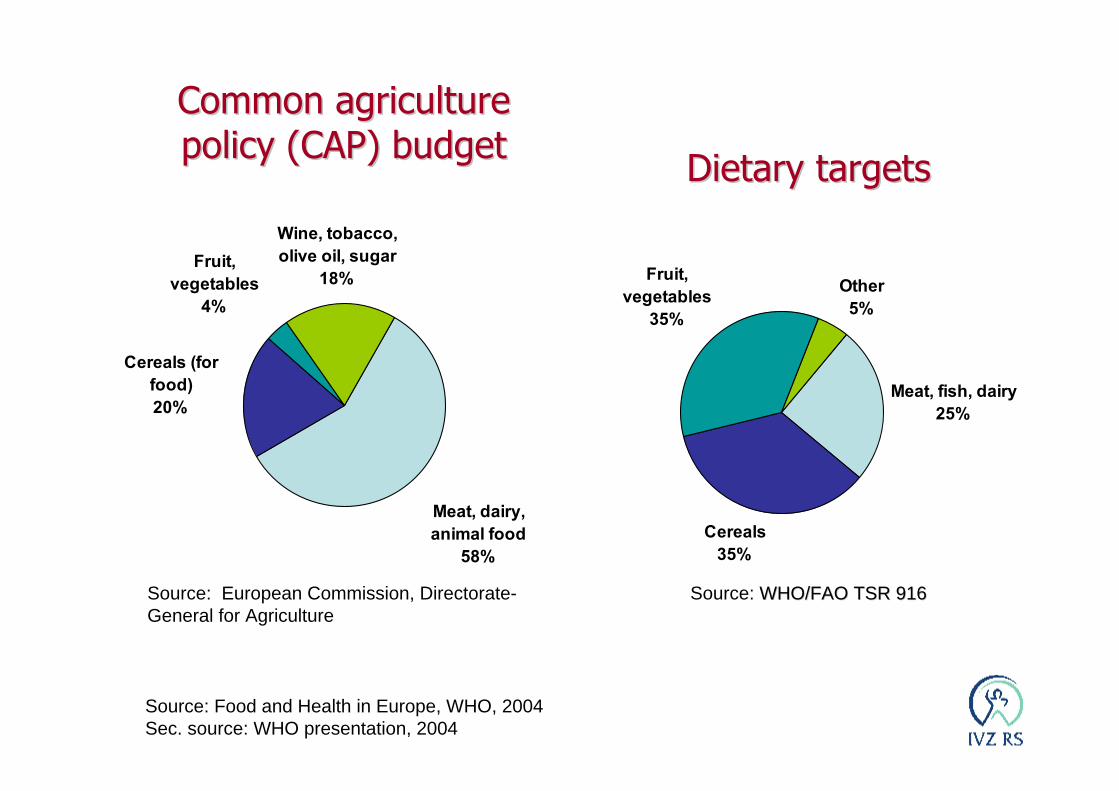
Fruit, vegetables
4%
Wine, tobacco, olive oil, sugar
18%
Cereals (for food)20%
Meat, dairy, animal food
58%
CommonCommon agricultureagriculturepolicypolicy (CAP) budget(CAP) budget
Source: European Commission, Directorate-General for Agriculture
Meat, fish, dairy25%
Cereals35%
Fruit, vegetables
35%
Other5%
DietaryDietary targetstargets
Source: Food and Health in Europe, WHO, 2004Sec. source: WHO presentation, 2004
Source: WHO/FAO TSR 916WHO/FAO TSR 916

“Fruit and Vegetable”,at least 400 g/day
The group “fruit and vegetable” represents one of the key groups in human diet.
Sufficient intake of fruit and vegetable provides the body with:
- essential nutrients that increase the body’s antioxidative potential
- dietary fibre and micronutrients; The inclusion of fruit and vegetables into the
diet effectively reduces the energetic density of our meals.

WHO. World Health Report 2002

WHO. World Health Report 2002

Low FV intake leads to poor health and premature death
Increasing FV consumption in EU could decrease burden of:
• heart disease by 17-24%• selected cancers by up to 17 %• reduce total deaths by over 1 million people/year
Source: Pomerleau, Lock, McKee 2006

Approximately 5m school children in Europe are obese
22% of obese schoolchildren have significantly raised blood pressure
(1.1m in EU)34% of have significantly raised levels of insulin (1.7m
in Europe)25,000 children have type 2 diabetes
28% have early stage fatty liver disease(1.4m in Europe)
Increasing burden of disease in present children andadolescent and in futur adult population.
Source: IOTF
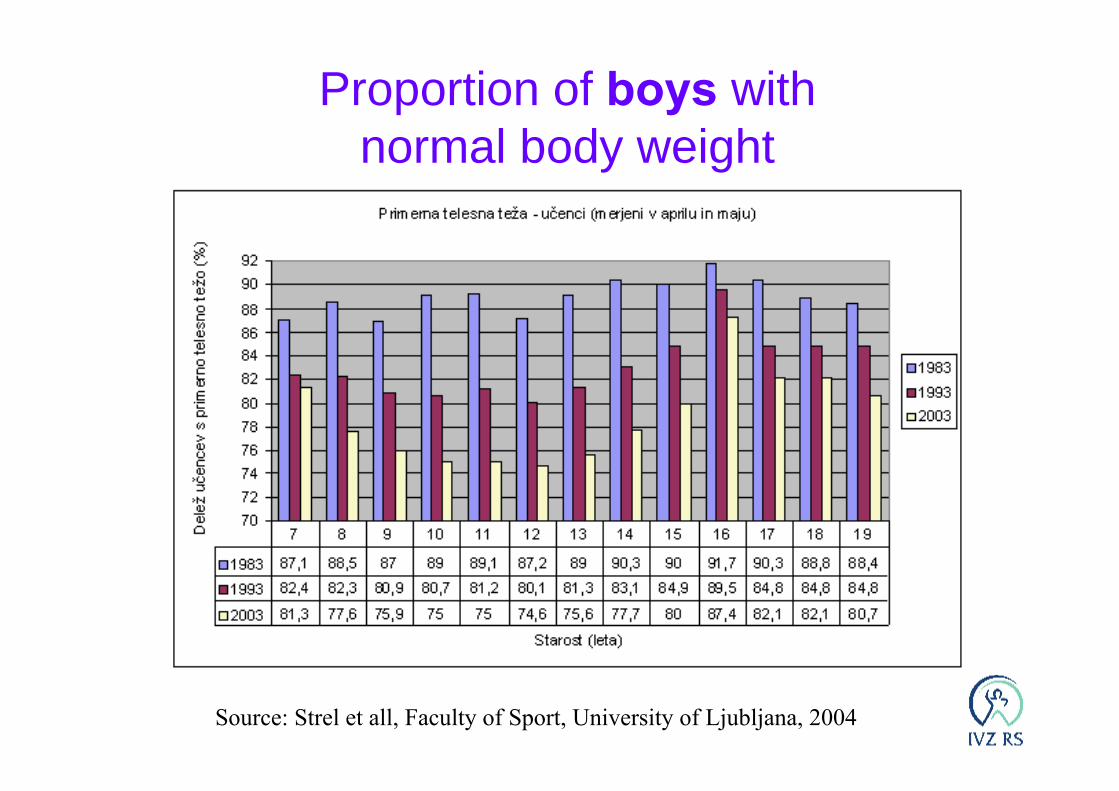
Proportion of boys withnormal body weight
Source: Strel et all, Faculty of Sport, University of Ljubljana, 2004

Proportion of girls withnormal body weight
Source: Strel et all, Faculty of Sport, University of Ljubljana, 2004
Nutritional habits in children andadolescents in Slovenia
- To low intake of fruits and vegetables- Boys consume fruit and vegetables statisticaly
significant less regularly- The intake of fruit and vegetables decreases
with age- To often meals consist of energy-dense and
nutrient-poor foods- Number of daily meals is to low, with irregular
periodicity- No risk of not “being cool” if you decide for
healthy nutrition choices- Sedentary lifestyle is high and increasingSource: National Institute of public health - reports 2000, HBSC 2006

Summary of strenght of evidence on factors that might promote or protect against weight gain and obesity, WHO TRS 916
AlcoholIncresased eatingfrequency
Insufficient
Large portion sizesHigh proportion of foodprepared outside thehome
Protein contentof the diet
Low glycaemic index foodsPossible
Heavy marketing ofenergy dense foods andfast-food outletsHigh intake of sugars-sweetened soft drinks andfruit juicesAdverse socioeconomicconditions
Home and schoolenvironments thatsupport healthy foodchoices for childrenBreastfeeding
Probable
Sedentary lifestylesHigh intake of energydense, micronutrientpoor foods
Regular physical activityHigh dietary intake ofdietary fibre
Concincing
Increased riskNo relationshipDecreased riskEvidence
Limited evidence of cost-effectiveness
One economic modelling study from Norwegian Directorate of Health:– ‘providing a free school fruit programme to
all pupils grade 1-10 would be cost-effective if it resulted in a lifelong increase in mean fruit and vegetable consumption of only 2.5 g/day’
Source: Sælensminde, K. Frukt og grønnsaker i skolen Beregning avsamfunnsøkonomisk lønnsomhet. Oslo: Sosial-og helsedirektoratet; 2006Sec. source: LSHTM 2007
II. Working together

Health is created and lived by people within the settings oftheir everyday life; where they learn, work, play and love.
(Ottawa charter, 1986).
http://www.who.int/hpr/NPH/docs/ottawa_charter_hp.pdf
Most of determinants of ill-health or positive health are not under control of health sector

Amsterdam Treaty, Article 152: …a high level of human healthprotection shall be ensured bothin the definition andimplementation of all Communitypolicies and activities
Lisbon strategy (economic goals, for the first time supported bysocial cohesion goals)
Nutrition and physical activitypolicy documents (EC, WHO, FAO)
WHO Nutrition Friendly SchoolInitiative (NFSI)
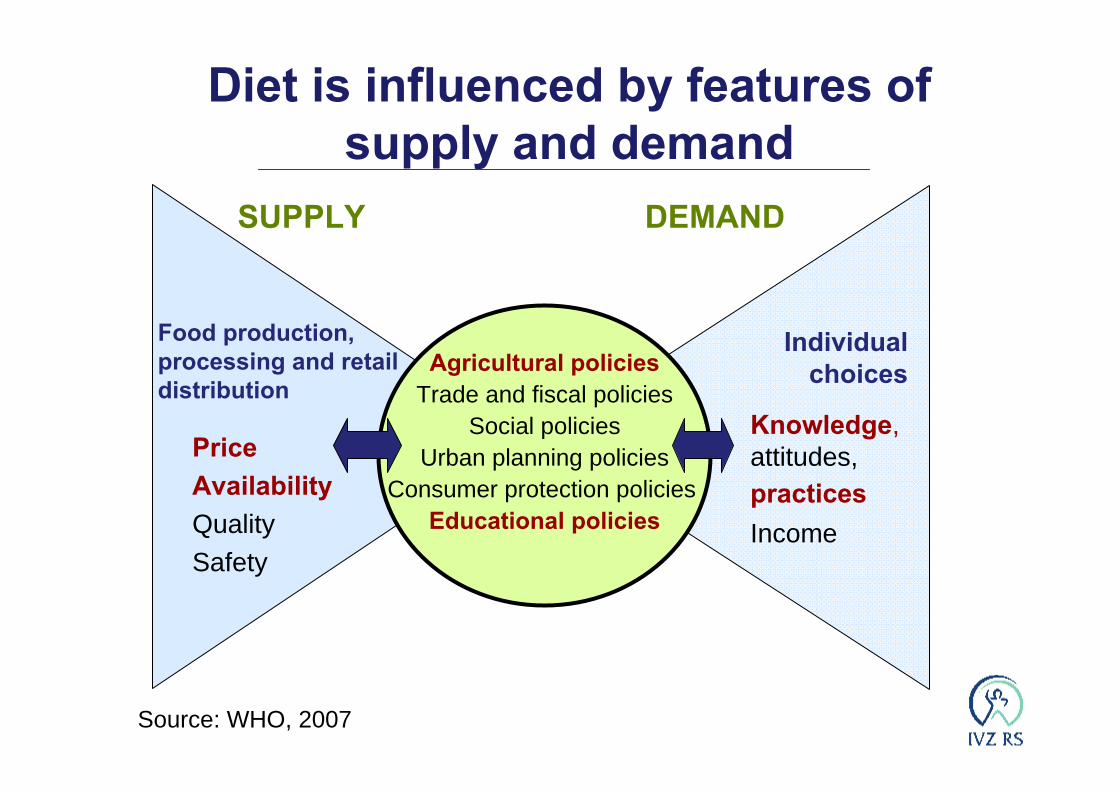
Agricultural policiesTrade and fiscal policies
Social policiesUrban planning policies
Consumer protection policiesEducational policies
Food production,processing and retail distribution
SUPPLY DEMAND
Individual choices
PriceAvailabilityQualitySafety
Knowledge,attitudes, practicesIncome
Diet is influenced by features of supply and demand
Source: WHO, 2007

HIA Report to Ministry of HealthRecommendations can be summarized
in four main policy areas:- fruit and vegetables,- wine, - diary produce and - rural development.
Source: Lock K, Gabrijelčič Blenkuš M, Maučec Zakotnik J, Poličnik R. HIA on Food and Agricultural Policies in Slovenia. Report to Ministry of Health, 2003
Perception of HIA on foodand agriculture policies by
different stakeholdersMedical expert:
broader socio-economicdeterminants of health wereincluded
Agricultural expert: assessment was based on a relatively narrow medical concept
…expressed by agriculture expert: “Thus one should be well-versed and technically competent when dealing with inter-sector communication and work. Expert multidisciplinary competency is the key and we do not have enough of it. The fixation on medicine is very disturbing. Medical experts think that everything derives from it ... This disrupts normal work. The agricultural experts believe that they are untouchable because of the large portion of the budget and the money they possess”.
Qualitative evaluation conclusion: lack of multidisciplinary competence,more cooperation and discussion is needed!
Source: HIA effectivenes DG SANCO project, Who Observatory with Memberstates, research data 2006

Intersectoral working body for school nutrition was established in May 2007.Leading sector is education, agriculture and healthparticipating.
Ministers of health, education and family/social affairs are signing official obligation to take care for children andadoloescent health together, with harmonizedactivities (2007)
Source: Slovene NIPH, 2007

III. National school nutritionprogram and “Apple” project –
Slovene experience

National school nutrition programme1. All kindergartens in Slovenia offer breakfast, midmorning
snacks, lunches and afternoon snacks. Financing: Ministry of Education, local comunity, parents
2. Most primary schools offer breakfast, midmorning snacks, lunches and afternoon snacks. All primary schools offer at least two meals (midmorning snacks and lunches) every school day. Financing: Ministry of Education and Sport, local comunity(regular expenses), parents
3. Regretfully the situation in secondary schools is not as good, although is foreseen that the adopted guidelines could improve the current situation. Financing: Ministry of Education and Sport, parents
Source: Ministry of Education and Sport, 2007

Contents
1. Recommended energy and nutrientdaily intake for different age groups(2 – 18 years), with calculations fordifferent of meals
2. Periodicity of meals3. Recommended frequency of intake
for different food groups, fruit and/or vegetables part of every meal
4. List of food items/groups with limitedinclusion in daily meal
5. “Demo” seasonal menues
Vending machines for sweetened softdrinks in school buildings are not recommended.
Guidelines for healthy nutrition in kindergartens,
primary and secondary schools,
2005

National school nutrition programme
The main objectives are:- to provide a supportive environment for healthy choice in
schools, supporting better health status of school children- to support regular curricula with the elements of “hiden”
curricula- to support families and working mothers,- to reduce social inequalities and inequalities in health

NUTRITION IN SCHOOLS - PROVISIONS
Legal basis: All schools must provide at least one meal a dayProvision of school meals in primary schools:
- 1 job assignment of school nutrition organizerfor every 4,200 children
- 1 job assignment of chef for the preparation of snacks for every 400 children (approx. 410 kitchen employes)
- all primary schools in Slovenia have central or dispensing school kitchens
Participation of primary school pupils in individual meals:
breakfast: 3,5 %morning snack: 97 %lunch: 46 %afternoon snack: 6,5 %
Source: Ministry of Education and Sport, 2007
Morning meal/snack is part of the National programme, for which partial financing is provided by the Ministry of Education and Sport. All schoolchildren pay solely for the price of food, composing the meal.
Other meals such as lunch or breakfast are placed into the so called economic, but non profit programme.
Subsidising of school meal, for children and adolescentsfrom families with lower socioeconomic status,subsidies for school meals for pupils/students in 2006/07:
EUR 0.55 daily per pupil for 36,4% of pupilsEUR 0.85 daily per pupil for 32,8% of secondary
school students
Source: Ministry of Education and Sport, 2007

PROJECT “APPLE IN SCHOOL”
started 200425 primary chools25 secondary schools
selection criteriaparticipation in Slovenian network of Health Promotion Schools regional distribution of schools
Supported by Ministry of Education and Sportin cooperation with:
Ministry of Health and Institute of Public Health of the Republic of Slovenia andMinistry of Agriculture, Forestry and Food
Source: Ministry of Education and Sport, 2007

PROJECT “APPLE IN SCHOOL”
means of support funds for schools to buy apples (3 times a week)list of certain local producers (4 varieties of
apples)setting conditions that must be met by the
producers
obligations of each schoola contract with the selected providerplan of activities
- set specific goals- adequate supply of apples- adequate offer of apples to pupils- set cooperation of pupils, teachers and
parents- promotion and cooperation with local
communitySource: Ministry of Education and Sport, 2007
PLANING proces is described (for schools)- concrete, measurable goals- description of pupils/students participation- description of the distribution of apples- additional activities (link with regular curicula,
taste education, link with environmentaleducation …
- cooperation with parents, local comunity, local producers …
Source: NIPH

EVALUATION protocol is described (for schools)- observed changes- measurement of the observed changes- realization of the plan- satisfaction with the outcomes (children, teachers,
management, parents)- cooperation with the fruit providers- most successful approaches- recommendations
Source: NIPH

Main changes/outcomes proved by evaluation:
- increased consumption of apples among pupils- popularity of apples grew higher- apples occasionally replaced unhealthy foodd- increased awareness of the importance of healthy food among
pupils- inter-subject links and links with other projects and various
promotional activities- high motivation of pupils, parents and teachers- offered non-coercive way for:
- environmental education- learning about sustainable development- recognising the importance of biodiversity and
environment protection, - waste management (separate collection and composting)- importance of the inclusion and cohesion of all actors
Source: Ministry of Education and Sport, 2007

Administrative details
0,65108.23115 8660,6570.29510 8922006/07
0,64104.40016 3520,6470.61311 0602005/06
Budget /month/personin € *
Totalbudget(in €)
Secondaryschools
Budget/month/personin € *
Totalbudget(in €)
Primaryschools
* Apples have exclusively been purchased locallySource: Ministry of Education and Sport, 2007

IV. Conclusion

ConclusionsSFS may help curbing presently increasing trends
of excessive body weight and obesity in children and adolescents and ensure a long-term protection of children and adolescents against obesity.
MS should involve the Ministry of Agriculture as well as the Ministry of Education and the Ministry of Health (intersectoral collaboration).
Flexibility and sustainability of SFS shall beassured.
Education shall be part of the programes.It is essential to involve local comunity, specially local
producers, parents ant others.

ConclusionsSFS is an effective tool for ensuring equity in health.
The investment into SFS would be justified when compared with the disease burden, i.e.
- direct and - indirect disease-related costs and - the costs of lost opportunities as well as - all the consequences of a lower quality of life already
in childhood and particularly in later life.
Comprehensive approach to these issues would call for additional measures to counteract the adverse influences on children and adolescents’ dietary choices, such as e.g. measures to ban marketing of unhealthy food to children.

Intersectoral collaboration in partnerships
is a way forward