the relationship between the superior petrosal sinus and
TRANSCRIPT

J Neurosurg / Volume 119 / November 2013
J Neurosurg 119:1221–1225, 2013
1221
©AANS, 2013
The SPS is a small, narrow venous channel located at the junction between the middle and posterior cra-nial fossae. It is adjacent to many important intracra-
nial structures, and its vicinity to these structures makes it an important landmark for surgical approaches to the skull base. It originates in the CS and passes dorsolaterally to drain into the transverse-sigmoid junction. The sinus runs in the superior petrosal sulcus and begins from the postero-lateral base of the petrous ridge and travels at an anterome-
dial angle toward its apex, and is usually larger posteriorly and becomes smaller near its apex.23 This sinus travels in the attached margin of the tentorium cerebelli26 and re-ceives drainage from the cerebellum, the inferior cerebral veins, and the veins of the tympanic cavity.26,31
Since knowledge of such regional anatomy is impor-tant to the neurosurgeon, and the relationship of the SPS to the Meckel cave has not been stressed in the literature, the current study was undertaken.
The relationship between the superior petrosal sinus and the porus trigeminus: an anatomical study
Laboratory investigationR. Shane TubbS, M.S., P.a.-C., Ph.D.,1 MaRTin M. MoRTazavi, M.D.,1 Sanjay KRiShnaMuRThy, b.S.,1 KeTan veRMa, b.S.,1 ChRiSToPh j. GRieSSenaueR, M.D.,2 anD aaRon a. Cohen-GaDol, M.D., M.SC.3 1Pediatric Neurosurgery, Children’s Hospital, Birmingham; 2Division of Neurosurgery, Department of Surgery, University of Alabama at Birmingham, Alabama; and 3Goodman Campbell Brain and Spine, Department of Neurological Surgery, Indiana University School of Medicine, Indianapolis, Indiana
Object. During intracranial approaches to the skull base, vascular relationships are important. One relationship that has received scant attention in the literature is that between the superior petrosal sinus (SPS) and the opening of the Meckel cave (that is, the porus trigeminus).
Methods. Cadaver dissections were performed in 25 latex-injected adult cadaveric heads (50 sides). Specifically, the relationship between the SPS and the opening of the Meckel cave was observed. The goal was to enhance knowl-edge of the relationship between the SPS and the opening of the Meckel cave.
Results. Of the 50 sides, 68%, 18%, and 16% of SPSs traveled superior to, inferior to, and around the opening to the Meckel cave, respectively. In the latter cases, a venous ring was formed around the proximal trigeminal nerve. No sinus entered the Meckel cave. In general, the porus trigeminus was narrowed on sides found to have an SPS that encircled this region. Sinuses that traveled only inferior to the porus were in general smaller than sinuses that trav-eled superior or encircled this opening. No statistically significant differences were noted between the various sinus relationships and sex, age, or side of the head.
Conclusions. Knowledge of the relationship between the SPS and the opening of the Meckel cave may be useful to the skull base surgeon. Based on this study, some individuals may retain the early embryonic position of their SPS in relation to the trigeminal nerve.(http://thejns.org/doi/abs/10.3171/2013.4.JNS122062)
Key WoRDS • anatomy • skull base • superior petrosal sinus • neurosurgery • cadaver dissection
1221
Abbreviations used in this paper: CS = cavernous sinus; SPS = superior petrosal sinus.
This article contains some figures that are displayed in color on line but in black-and-white in the print edition.

R. S. Tubbs et al.
1222 J Neurosurg / Volume 119 / November 2013
MethodsCadaver dissections were performed in 25 formalin-
fixed latex-injected adult cadaveric heads (14 male and 11 female specimens) with a mean age at death of 73 years (range 39–90 years). Specifically, the relationship between the SPS and the opening of the Meckel cave was observed. Measurements of the SPS were made at this lo-cation with the aid of digital calipers. Statistical analysis was performed using Statistica for Windows, with signifi-cance set at p < 0.05.
ResultsOf the 50 sides, 68%, 18%, and 16% of SPSs trav-
eled superior to, inferior to, and around the opening to the Meckel cave (Figs. 1–4). In the latter cases, a venous ring was formed around the proximal trigeminal nerve. No sinus entered the Meckel cave. In general, the porus trigeminus was narrowed on the sides found to have an SPS that encircled this region. Sinuses that traveled only inferior to the porus were smaller in general than sinuses that traveled superior or encircled this opening. No petro-sal vein was found to empty into SPSs that were located below the Meckel cave. The mean diameter of the SPS at the level of the trigeminal nerve and when located above the Meckel cave was 2.1 mm; when located below it was
1.8 mm; and when found above and below it was 1.5 and 1.2 mm, respectively. No statistically significant differ-ences were noted between the various sinus relationships and sex, age, or side of the head. No intracranial pathol-ogy was observed in any specimen.
DiscussionEmbryonic Position of the SPS
The SPS is the last of the major adult sinuses to be formed and is derived from the metencephalic vein, which relates to the early development of the cerebellum.21,22 The SPS begins to appear in Stage 2 of development (14-mm embryo).14 At this point, the SPS rests between the trigeminal ganglion and the oculomotor and trochlear nerves.3,14 The more significant start of the development of the SPS occurs during Stage 3 (embryo 16–18 mm long).14 This stage is distinct because there is a sudden appearance of a large supraotic anastomosis, or cross-connection networking, linking the prootic and posterior rhombencephalic veins (Fig. 5).18 This new channel to-gether with the terminal part of the posterior rhombence-phalic veins forms the sigmoid sinus.3 At this stage, the SPS lies in the cavum epiptericum close to the anterior layer of dura mater forming the tentorium cerebelli.32 Its
Fig. 1. Schematic drawing of the developing fetus. Note the 3-pronged trigeminal nerve around the eye and the fetal arrangement of the precursor to the SPS traveling under the trigeminal nerve (gas-serian ganglion).
Fig. 2. Schematic drawing of the relationships (Types I–III) of the SPS to the porus trigeminus of the right skull base as found in our study.
J Neurosurg / Volume 119 / November 2013
Porus trigeminus and superior petrosal sinus
1223
role is to act as an anteriorly directed branch of the main prootic vein joining either the peritrigeminal vein or the termination of the anterior cerebral vein.3 At Stage 6 (90 mm long and approximately 60 days old), the SPS runs along the upper margin of the otic capsule and then above the trigeminal ganglion in the roof of the Meckel cave.14 As it joins the CS it lies above the trigeminal ganglion and above the oculomotor and trochlear nerves.3
The overall developmental process that occurs dur-ing this stage is as follows: the oculomotor and trochlear nerves and the SPS are close to the anterior dural fold and well in front of the otic capsule, from which they are separated by the trigeminal ganglion. As the temporal lobe expands and excavates the middle cranial fossa, it presses the anterior tentorial layer backward. This presses the oculomotor and trochlear nerves, the trigeminal gan-glion, and the SPS toward the otic capsule. This causes the nerves and the sinus to achieve their adult positions. Because of this, the SPS runs above the trigeminal gan-glion and below the oculomotor and trochlear nerves. The
expanded CS now protrudes toward the trigeminal gan-glion and receives the SPS.3 The connection of the SPS with the CS is a comparatively late event and, as shown in our study, is not constant.
Sinus-to-Nerve RelationshipsIn 1934, Coates4 conducted a study to clarify the re-
lationship between the SPS and the sensory root of the trigeminal nerve. In 8 of the cases, both the right and left sinuses passed over the cranial surface of the trigeminal nerve. In 3 cases, the left and right sinus passed under the nerve. Finally, in 3 cases, the sinus divided lateral to the root, meaning that a portion passed over the root and a portion passed under the root. These divisions were re-united at the CS. In the present study, we found that 68%, 18%, and 16% of SPSs traveled superior to, inferior to, and around the opening to the Meckel cave.
Endovascular Treatment and SurgeryEven though the SPS may not always be seen on an-
giograms, it can be obliterated with detachable coils, from distal to proximal.19 Endovascular therapy is often neces-sary to manage effectively the pathological entities in-volving this sinus, such as dural arteriovenous fistulas.2,6,7,
9,10,12,13,17,27,29
The venous anatomy of the skull base and its varia-tions are important in approaches to this region.1,15,20,25 Dolenc5 classified the CS region through the depiction of 10 triangles. The inferolateral triangle was defined as lines connecting the dural entry point of the trochlear nerve, the dural entry point of the abducent nerve, and the entry point of the petrosal vein into the SPS.11,13,23,24,33 The SPS also forms the superior boundary of the Traut-mann triangle, which is used for posterior petrosectomy approaches, and the medial border of the Kawase triangle (rhomboid; posteromedial triangle), which is used for an-terior petrosectomy.11,13,23,24,30
Approaches around the Meckel cave have been based on petrosal vein drainage types. Tanriover et al.28 classi-fied the drainage types of the petrosal vein. Type I com-
Fig. 3. Right-side cadaver dissection of the porus trigeminus, noting the Type I configuration of the SPS.
Fig. 4. Right-side cadaver dissection of the porus trigeminus, noting the Type II configuration of the SPS.
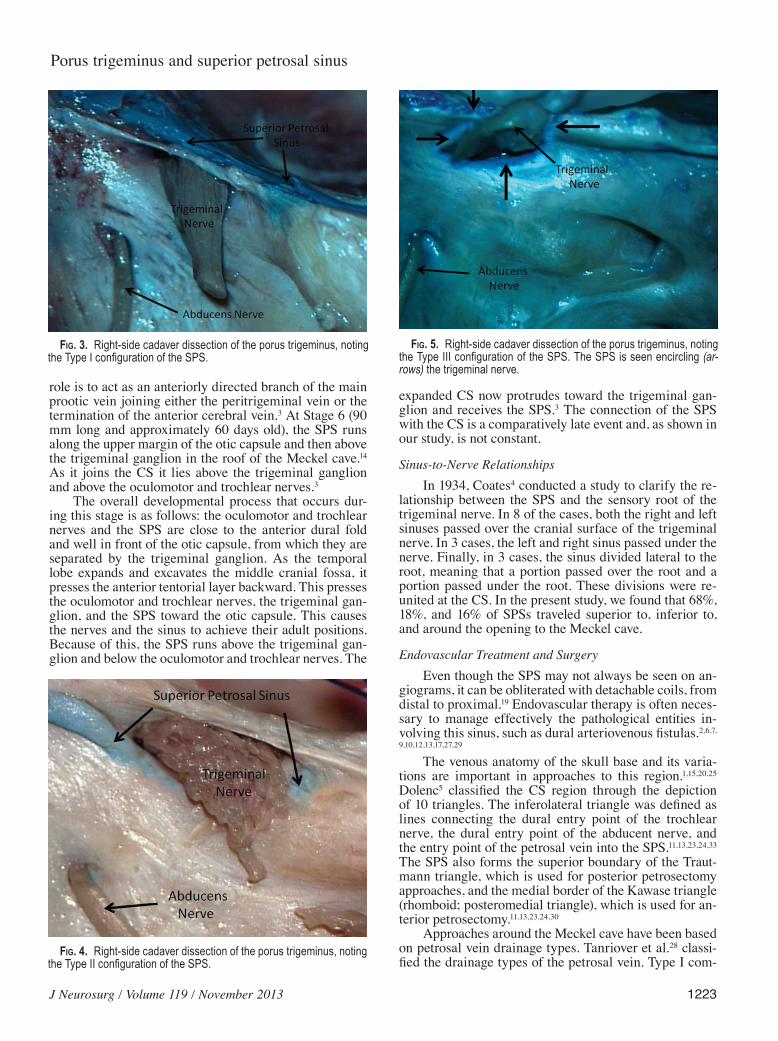
Fig. 5. Right-side cadaver dissection of the porus trigeminus, noting the Type III configuration of the SPS. The SPS is seen encircling (ar-rows) the trigeminal nerve.

R. S. Tubbs et al.
1224 J Neurosurg / Volume 119 / November 2013
plexes called for a subtemporal transtentorial approach, with or without anterior extradural petrosectomy, because the petrosal vein drained into the SPS posteriorly and near the porus acusticus. In Types II and III, the petrosal vein drained into the SPS near the Meckel cave, mak-ing the working space in a subtemporal transtentorial ap-proach smaller, and making alternative approaches such as a retrosigmoid suprameatal approach more desirable. A detailed preoperative MR venogram or a venous-phase CT angiogram demonstrating the site of entry of the su-perior petrosal venous complex into the SPS might be helpful in assessing the unique drainage patterns prior to subtemporal transtentorial and retrosigmoid suprameatal approaches.8,16,24,28 Interestingly, such classifications have not taken into consideration the position of the SPS rela-tive to the Meckel cave. If the sinus were in an inferior position in relation to the trigeminal nerve, drainage of regional veins might take a variable route into this sinus. Therefore, tumors or arteriovenous malformations of this specific area may have drainage that is considered un-common.
Because we appreciated an overall narrowing of the porus trigeminus in our cases found to have a venous ring, surgical access to the Meckel cave via a posterior fossa approach might be limited when this anatomy is present. Moreover, with a middle fossa approach to the Meckel cave, the surgeon may not visualize the inferior aspect of such a venous ring, which may predispose patients with this anatomy to venous injury. Last, intravascular venous access to the SPS may be derailed due to such venous rings as were identified in our study.
ConclusionsKnowledge of the relationship between the SPS and
the opening of the Meckel cave may be useful to the skull base surgeon. Based on our study, some individuals may retain the early embryonic position of their SPS in rela-tion to the trigeminal nerve, that is, inferior to the open-ing of the Meckel cave. Such a relationship should be con-sidered by the surgeon and by those who interpret cranial vascular imaging.
Disclosure
The authors report no conflict of interest concerning the mate-rials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript preparation include the following. Conception and design: Cohen-Gadol, Tubbs, Mortazavi. Acquisition of data: all authors. Analysis and interpreta-tion of data: all authors. Drafting the article: all authors. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Approved the final version of the manuscript on behalf of all authors: Cohen-Gadol. Study supervision: Tubbs.
References
1. Al-Mefty O, Fox JL, Smith RR: Petrosal approach for petro-clival meningiomas. Neurosurgery 22:510–517, 1988
2. Branco G, Takahashi A, Ezura M, Yoshida M, Yoshimoto T: Dural arteriovenous shunt involving the superior petrosal sinus: presentation and treatment by transvenous embolisa-
tion via the occipital and transverse sinuses. Neuroradiology 39:67–70, 1997
3. Butler H: The development of certain human dural venous si-nuses. J Anat 91:510–526, 1957
4. Coates AE: A note on the superior petrosal sinus and its relation to the sensory root of the trigeminal nerve. J Anat 68:428, 1934
5. Dolenc VV: Anatomy and Surgery of the Cavernous Sinus. New York: Springer-Verlag, 1989, pp 7–88
6. Gobin YP, Houdart E, Rogopoulos A, Casasco A, Bailly AL, Merland JJ: Percutaneous transvenous embolization through the thrombosed sinus in transverse sinus dural fistula. AJNR Am J Neuroradiol 14:1102–1105, 1993
7. Grisoli F, Vincentelli F, Fuchs S, Baldini M, Raybaud C, Le-clercq TA, et al: Surgical treatment of tentorial arteriovenous malformations draining into the subarachnoid space. Report of four cases. J Neurosurg 60:1059–1066, 1984
8. Hafez A, Nader R, Al-Mefty O: Preservation of the superior petrosal sinus during the petrosal approach. Technical note. J Neurosurg 114:1294–1298, 2011
9. Halbach VV, Higashida RT, Hieshima GB, Hardin CW, Pri-bram H: Transvenous embolization of dural fistulas involving the cavernous sinus. AJNR Am J Neuroradiol 10:377–383, 1989
10. Halbach VV, Higashida RT, Hieshima GB, Mehringer CM, Hardin CW: Transvenous embolization of dural fistulas involv-ing the transverse and sigmoid sinuses. AJNR Am J Neu roradiol 10:385–392, 1989
11. Inoue T, Rhoton AL Jr, Theele D, Barry ME: Surgical ap-proaches to the cavernous sinus: a microsurgical study. Neurosurgery 26:903–932, 1990
12. Kimura T, Shojima M, Koizumi T, Fukaya S, Ichikawa Y, Mori-ta A: Surgical treatment of a dural arteriovenous fistula in the superior petrosal sinus of an elderly patient with minimal sub-occipital craniotomy: case report. Neurol Med Chir (Tokyo) 49:465–467, 2009
13. Kiris T, Sankhla S, Lawton MT, Zabramski JM, Spetzler RF: Microsurgical anatomy of the cavernous sinus. BNI Q 12:4–14, 1996
14. Larsen WJ, Sherman LS, Potter SS, Scott WJ: Human Embryology, ed 3. Edinburgh: Churchill Livingstone, 2001
15. Miller DL, Doppman JL: Petrosal sinus sampling: technique and rationale. Radiology 178:37–47, 1991
16. Miyamoto N, Naito I, Takatama S, Shimizu T, Iwai T, Shimagu-chi H: Clinical and angiographic characteristics of cavernous sinus dural arteriovenous fistulas manifesting as venous in-farction and/or intracranial hemorrhage. Neuroradiology 51: 53–60, 2009
17. Mounayer C, Piotin M, Spelle L, Moret J: Superior petrosal sinus catheterization for transvenous embolization of a dural carotid cavernous sinus fistula. AJNR Am J Neuroradiol 23: 1153–1155, 2002
18. Mullan S, Mojtahedi S, Johnson DL, Macdonald RL: Embryo-logical basis of some aspects of cerebral vascular fistulas and malformations. J Neurosurg 85:1–8, 1996
19. Ng PP, Halbach VV, Quinn R, Balousek P, Caragine LP, Dowd CF, et al: Endovascular treatment for dural arteriovenous fis-tulae of the superior petrosal sinus. Neurosurgery 53:25–33, 2003
20. Ohata K, Haque M, Morino M, Nagai K, Nishio A, Nishijima Y, et al: Occlusion of the sigmoid sinus after surgery via the presigmoidal-transpetrosal approach. J Neurosurg 89:575–584, 1998
21. Padget DH: The cranial venous system in man in reference to development, adult configuration, and relation to the arteries. Am J Anat 98:307–355, 1956
22. Padgett BL, Walker DL: Enzymatic variants of influenza virus. I. Isolation and characterization of slowly reacting enzymatic variants of influenza B virus. J Exp Med 106:53–68, 1957
23. Rhoton AL Jr: The posterior fossa veins. Neurosurgery 47 (3 Suppl):S69–S92, 2000

J Neurosurg / Volume 119 / November 2013
Porus trigeminus and superior petrosal sinus
1225
24. Rhoton AL Jr: The temporal bone and transtemporal ap-proaches. Neurosurgery 47 (3 Suppl):S211–S265, 2000
25. Sakata K, Al-Mefty O, Yamamoto I: Venous consideration in petrosal approach: microsurgical anatomy of the temporal bridging vein. Neurosurgery 47:153–161, 2000
26. Standring S (ed): Gray’s Anatomy: The Anatomical Basis of Clinical Practice, ed 39. Edinburgh: Churchill Livingstone, 2005
27. Takahashi A, Yoshimoto T, Kawakami K, Sugawara T, Suzuki J: Transvenous copper wire insertion for dural arteriovenous malformations of cavernous sinus. J Neurosurg 70:751–754, 1989
28. Tanriover N, Abe H, Rhoton AL Jr, Kawashima M, Sanus GZ, Akar Z: Microsurgical anatomy of the superior petro-sal venous complex: new classifications and implications for subtemporal transtentorial and retrosigmoid suprameatal ap-proaches. J Neurosurg 106:1041–1050, 2007
29. Teng MM, Guo WY, Huang CI, Wu CC, Chang T: Occlusion of arteriovenous malformations of the cavernous sinus via the superior ophthalmic vein. AJNR Am J Neuroradiol 9:539–546, 1988
30. Tos M: Manual of Middle Ear Surgery. New York: Thieme, 1993
31. Tubbs RS, Menendez J, Loukas M, Shoja MM, Shokouhi G, Salter EG, et al: The petrosal nerves: anatomy, pathology, and surgical considerations. Clin Anat 22:537–544, 2009
32. Vidyasagar C: Persistent embryonic veins in arteriovenous malformations of the posterior fossa. Acta Neurochir (Wien) 48:67–82, 1979
33. Watanabe A, Nagaseki Y, Ohkubo S, Ohhashi Y, Horikoshi T, Nishigaya K, et al: Anatomical variations of the ten triangles around the cavernous sinus. Clin Anat 16:9–14, 2003
Manuscript submitted October 29, 2012.Accepted April 23, 2013.Please include this information when citing this paper: pub-
lished online May 24, 2013; DOI: 10.3171/2013.4.JNS122062.Address correspondence to: Aaron A. Cohen-Gadol, M.D.,
M.Sc., Goodman Campbell Brain and Spine, Indiana University De part ment of Neurological Surgery, 355 West 16th Street, Suite 5100, Indianapolis, Indiana 46202. email: [email protected].