the relationship between night eating syndrome and … · the relationship between night eating...
TRANSCRIPT

1
Author: Aldawood Fahad A
Title: The Relationship between Night Eating Syndrome and Body Mass Index Among
College Students
The accompanying research report is submitted to the University of Wisconsin-Stout, Graduate School in partial
completion of the requirements for the
Graduate Degree/Major: MS Food and Nutritional Sciences
Research Adviser: Sally Dresdow BA, MBA, DBA
Submission Term/Year: Fall, 2012
Number of Pages: 44
Style Manual Used: American Psychological Association 6th edition
I understand that this research report must be officially approved by the Graduate School and that an electronic copy of the approved version will be made available through the University Library website
I attest that the research report is my original work (that any copyrightable materials have been used with the permission of the original authors), and as such, it is automatically protected by the laws, rules, and regulations of the U.S. Copyright Office.
My research adviser has approved the content and quality of this paper. STUDENT:
NAME: Fahad A Aldawood DATE: 12/17/2012
ADVISER:
NAME: Sally Dresdow DATE: 12/17/2012
----------------------------------------------------------------------------------------------------------------------------- ---- This final research report has been approved by the Graduate School.
Director, Office of Graduate Studies: DATE:

2
Aldawood, Fahad, A. The Relationship between Night Eating Syndrome and Body Mass
Index Among College Students
Abstract
Night eating syndrome (NES) is a relatively new eating disorder and there are no formal
diagnosis criteria or definitions established for this condition yet. It was thought that NES was
suspected of contributing to the worsening of obesity. Therefore, a full understanding of NES
could help in the management and prevention of obesity. The purpose of this research was to
investigate the relationship between NES and body mass index (BMI) among the University of
Wisconsin-Stout students during the fall semester of the academic year of 2012. The data were
collected through an electronic self-administered survey. There were 99 subjects included in this
research in which 41 subjects were males and 58 were females.
An average night eating (NE) score to reflect the severity of NES signs and symptoms
was calculated for every subject. BMI had a weak positive correlation with the average NE
score. Furthermore, BMI was not a significant predictor of NES. However, there was a
difference between males and females in average NE scores that were close to a statistical
significance and male subjects were significantly heavier than female subjects. The findings of
this study suggest further research on NES among young adults is needed.

3
Acknowledgement
Upon the completion of this research, I would like to express my gratitude where it is
due. First, I would like to thank and praise my god, Allah who did not leave me on my own for a
single second and I pray that he will continue supporting and protecting my beloved and me.
Secondly, I want to thank my parents and my family, particularly my mother and brothers who
stood by my side tirelessly through this task and many others. Thirdly, I would like to thank my
research adviser Dr. Sally Dresdow who generously shared her knowledge and wisdom with me
until the end. I also would like to thank Dr. Carol Seaborn for her significant contribution to this
research. In addition, I would like to thank Ms. Susan Greene and her staff for helping me
during the data analysis stage. Last but not least, I want to thank all my friends for their support
and encouragement throughout the wonderful years I spent in this fine institution.
4
Table of Contents
.................................................................................................................................................... Page
Abstract ............................................................................................................................................2
List of Tables ...................................................................................................................................6
Chapter I: Introduction ....................................................................................................................7
Statement of the Problem .....................................................................................................8
Purpose of the Study ............................................................................................................8
Definition of Terms..............................................................................................................8
Assumptions of the Study ....................................................................................................9
Limitations of the Study.......................................................................................................9
Methodology ........................................................................................................................9
Chapter II: Literature Review ........................................................................................................10
Definitions of Night Eating Syndrome ..............................................................................10
Prevalence and Classification of Night Eating Syndrome .................................................11
Night Eating Syndrome Associations with Psychological Stress ......................................16
Night Eating Syndrome Association with Obesity ............................................................18
Effectiveness of Certain Antidepressants in Treating Night Eating Syndrome .................19
Conclusions ........................................................................................................................20
Chapter III: Methodology ..............................................................................................................22
Subject Selection and Description .....................................................................................22
Instrumentation ..................................................................................................................23
Data Collection .................................................................................................................24
Data Analysis .....................................................................................................................24

5
Limitations ........................................................................................................................25
Chapter IV: Results ........................................................................................................................26
Survey Response ................................................................................................................26
Item Analysis .....................................................................................................................26
Demographics .......................................................................................................27
Average NE scores ................................................................................................28
BMI and average NE scores .................................................................................29
Figure 1: Scatter Plot showing the Relationship Between Subjects’ BMI and Subjects’
Average NE Scores ...........................................................................................................30
Conclusions ........................................................................................................................30
Chapter V: Discussion ...................................................................................................................31
Limitations .........................................................................................................................33
Conclusions ........................................................................................................................34
Recommendations ..............................................................................................................35
References ......................................................................................................................................36
Appendix A: Institutional Review Board Memo ...........................................................................39
Appendix B: Survey .......................................................................................................................40
Appendix C: Consent to Participate in UW-Stout Approved Research ........................................44

6
List of Tables
Table 1: Prevalence of Night Eating Syndrome According to Narrow and Broad Definitions
Among Different types of Subjects................................................................................................13
Table 2: Demographic Characteristics of Subjects Including BMI and Average NE Scores ........27
Table 3: Differences Among Males and Females As A Result of Two-Sample t Tests .........................................................................................................28

7
Chapter I: Introduction
Obesity is one of the most prevalent consequences of an unhealthy increase in body fat
(Medlineplus, n.d.). According to Ogden and Carroll (2010), 33.9% of the adults in the United
States of America (USA) population are obese, and the prevalence of obesity among children
and adolescents in the USA is 18.1%. The study of the development of obesity could help the
national and international efforts in the management and prevention of obesity. The development
of obesity can be attributed to a variety of contributing factors such as family history, sedentary
lifestyle, and overeating of unhealthy food.
Overeating is a significant contributing factor in the development of obesity. Overeating
means that people would consume more energy than what their body needs. It is a contributing
factor to obesity and can be observed as a symptom of certain eating disorders such as Binge
Eating Disorder (BED) and Night Eating Syndrome (NES). NES is the problem of interest in
this research.
According to Medlineplus (n.d.), BED occurs when the patient loses control and
consumes unusually large amounts of foods in a very little time. On the other hand, NES is a
relatively new condition and there is not a formal definition of the condition or diagnostic criteria
at this point in time. Several studies have established different definitions for NES. For
example, Rand, Macgregor and Stunkard (1997) used a broader definition of NES that describes
the condition as the presence of morning anorexia, evening hyperphagia, insomnia, evening
tension and/or feeling upset. While other researchers use a more specific definition of NES that
defines the condition as the consumption of 50% or more of total energy intake after 7:00 pm
(Colles, Dixon & O'Brien, 2007).

8
NES in research papers has been studied with obesity in mind. Therefore, researchers
utilize the Body Mass Index (BMI) of their subjects as one method to diagnosis obesity.
Usually, a patient with a BMI of 30 or greater is thought to be obese (Body Mass Index, n.d.).
According to Tholin et al. (2009), NES was found to be significantly more prevalent among
subjects with greater BMI.
Statement of the Problem
Existing research indicates that NES is correlated with obesity or contributes to the
worsening of obesity (Striegel-Moore et. al., 2008). Therefore, understanding NES is extremely
important to the treatment of obese patients with NES and to the prevention of obesity among
non-obese patient with NES.
Purpose of the Study
The purpose of this study was to investigate the relationship between NES and the Body
Mass Index (BMI) among the students of the University of Wisconsin-Stout during the Fall
semester of 2012.
Research Objectives
The main objective of this study is to evaluate the relationship between NES and BMI
among the students of the University of Wisconsin-Stout. Another objective of this study is to
find out how prevalent NES is among the students at the University of Wisconsin-Stout.
Definition of Terms
The following are the definition of the terms that are commonly mentioned in this
investigation.
Binge eating disorder (BED). BED is a condition that occurs when the patient loses
control and consumes unusually large amounts of foods in a very little time (Binge Eating, n.d.)

9
Body mass index (BMI). BMI is a tool that is used to determine whether an individual’s
weight is under weight, normal weight, overweight, or obese. BMI is calculated by dividing the
weight in kilograms on the squared height in meters (Body Mass Index, n.d.).
Evening hyperphagia. Excessive food consumption in the evening.
Insomnia. Is a condition that happens when the patient is having difficulty to sleep or
stay sleeping (Insomnia, n.d.)
Morning anorexia. Is a condition when the patient loses his/her appetite in the morning.
Assumptions of the study
This investigation assumes that the survey will be distributed to all of the University of
Wisconsin-Stout students during spring semester of 2012 by email. In addition, this investigation
assumes that all the participants will answer the survey questions honestly and report facts
accurately.
Limitations of the study
This investigation might be limited by a small sample size. Another limitation might be
due to technical malfunctioning during the electronic survey distribution.
Methodology
In this research, the investigator developed an electronic survey that collected
demographic information from subjects such as age, weight, height and gender. In addition,
there were 13 items in the survey that were drawn from the night eating questionnaire (NEQ) in
order to assess the severity of NES signs and symptoms among subjects (Marshall et al., 2004).
The data were analyzed and several statistical procedures were applied to identify differences
between the two genders and to investigate the relationship between NES and BMI among the
subjects.

10
Chapter II: Literature Review
Night eating syndrome (NES) is one of a group of diseases referred to as eating disorders.
However, NES is highly suspected of causing obesity or contributing to the worsening of obesity
(Striegel-Moore et. al., 2008). Therefore, understanding NES is extremely important to the
treatment of obese patients with NES and to the prevention of obesity among non-obese patient
with NES.
This chapter explored research studies including two studies that investigated NES
prevalence and another study that used latent class analysis in order to classify NES to different
subtypes (Striegel-Moore et al., 2008). In addition, three studies were also included in this
chapter that investigated the association between NES and certain psychological features as well
as the relationship between obesity and NES among obese and non obese subjects (Calugi, Dalle
Grave & Marchesini, 2009; Colles et al., 2007; Marshall et al., 2004). Finally, the effectiveness
of the antidepressant Sertraline in the treatment of NES was also discussed in this chapter
(O’Reardon et al., 2006).
Definitions of NES and its Correlates in the Literature
The review by Birketvedt et al. (1999) reported that NES was first described by Stunkard
and his colleagues in 1955 as an eating disorder that involved morning anorexia, evening
hyperphagia and insomnia. Across the literature, different definitions of NES were used.
However, these definitions can be integrated into three categories, which were the broadest, the
broad and the narrow definitions of NES. One broader definition of NES was the presence of
morning anorexia, evening hyperphagia, insomnia, evening tension and/or feeling upset, (Rand
et al., 1997). A broad definition of NES was stated that 25% or more of a person’s daily food
intake was done after the evening meal and during the night (Tholin et al., 2009). The most

11
narrow definition of NES was that 50% or more of total energy intake was consumed after 7:00
pm (Colles, Dixon & O'Brien, 2007).
With different NES definitions, different and sometimes conflicting findings of NES
prevalence and other correlates have been reported. For instance, Rand et al. (1997) reported
that NES prevalence was 1.5% in the general US population after surveying a sample of 2,097
participants for NES using the broader definition. In the other hand, Tholin et al. (2009) reported
that NES prevalence was 2.5% among men and 1.7% among women who were included in a
twin study in Sweden with a sample of 21,741 participants using the narrow and broad definition
of NES. The study had also reported a positive correlation between NES and higher BMI where
other studies found conflicting results (Striegel-Moore et al., 2006).
Many studies indicated that formal diagnostic criteria and a standard definition for NES
have not been established (Striegel-Moore et al., 2006; Calugi, Dalle Grave & Marchesini, 2009;
Colles et al., 2007). In addition, NES was found to be associated with obesity and depression in
certain studies (Calugi, Dalle Grave & Marchesini, 2009; Colles et al., 2007). As reviewed by
Birketvedt et al. (1999), obesity, nocturnal snacking, stress and poor outcomes upon attempting
to lose weight seemed to be among the possible causes of NES while other studies emphasized
the role of certain hormones in the etiology of NES.
Prevalence and Classification of NES
NES could be an important contributor to the development of the obesity epidemic and
there is a need for a large sample from the population to accurately identify NE symptoms and
prevalence. Therefore, Tholin et al. (2009) conducted a cross sectional population based twin
study in Sweden in order to investigate NES prevalence and its relationship with BMI, BED and

12
sleep related problems. The sample size was 21,741 Swedish twins aging from 20 to 47 years
old with an average BMI of 24.6 for males and 23.1 for females.
The subjects answered a web-based questionnaire that included questions on
demographics, medical history, depression, sleep patterns and other data. The questionnaire
included questions that were targeted to identify NE according to the broad and narrow
definitions mentioned earlier and to investigate NES symptoms. The investigators had excluded
a subset of 7,242 subjects on the basis of their answers to the questions that would identify
people who ate at night due to reasons irrelevant to NE.
As shown in Table 1, Tholin et al. (2009) classified the prevalence of NE on the basis of
three factors gender, BMI and NES definition. It was found that NE highest prevalence was
among obese men, obese women, non-obese men and non-obese women respectively. On the
other hand, the prevalence of NE according to the broad definition was remarkably higher than
NE prevalence according to the narrow definition regardless of the subjects’ gender or obesity.
Furthermore, the investigators found the odds ratio of broadly defined NE among obese men and
women when compared to a same sex normal weight group were 2.47 for obese men and 2.80
for obese women, which could support the hypothesis of including NE as a major risk factor for
obesity. The investigators had analyzed the data again after excluding the mentioned subset and
reached similar findings.

13
Table 1
Prevalence of NES According to the Narrow and Broad Definitions Among Different Types of
Subjects
Type of Subjects Prevalence of NES according
to the broad definition
Prevalence of NES according to
the narrow definition
Men 4.6% 2.5%
Obese Men 8.4% 4.6%
Women 3.4% 1.7%
Obese Women 7.5% 4.5%
Tholin et al. (2009) concluded that NE was found to be more common in men than
women. NE was also found to be more common in obese men and women that non-obese men
and women, which could mean that NE might contribute to the development of obesity. The
study had a large sample size, which strengthens its findings when compared to other studies
with a relatively much smaller sample size. In contrast, the study relied on self-reported
questionnaire, which might be a potential source of bias because subjects might under report
their food consumption.
In the USA, Striegel-Moore et al. (2006) conducted a cross-sectional study to examine
the prevalence and correlates of NES. The sample was drawn from public databases of the
participants of the National Health and Nutrition Examination Survey (NHANES III), and was
drawn between 1988 and 1994. The participants of Continuing Survey of Food Intakes by
Individuals (CSFII) that was conducted from 1994 to 1996 were also part of the sample. The
study included 18,402 subjects who were 13 years and older, 47.5% were men, race, gender,

14
ethnicity, age, type of day (weekday or weekend) and BMI were the main correlates of interest in
this study. In addition, three definitions of NES were utilized and compared in the this study
where the first definition of NES was “consuming 25% of the total daily calories between 7:00
pm and 4:59 am” (Striegel-Moore et al., 2006, p. 141). The second definition was “consuming
50% of the total daily calories between 7:00 am and 4:59 am” (Striegel-Moore et al., 2006, p.
141) and the third definition was “consuming anything between 11:00 pm and 4:59 am”
(Striegel-Moore et al., 2006, p. 141).
Striegel-Moore et al. (2006) reported that according to the first definition of NES, it was
found that more than 30% of all subjects had NES, however, prevalence rates according to the
second and third NES definitions were slightly lower among the CSFII participants which can be
attributed to the type of the day in which 36.1% of NHANES III participants provided their food
diaries on weekend days compared to 30.7% of CSFII participants which led the authors to
conclude that NES according to the first and second definitions could occur 1.2 to 1.4 times more
on weekends than weekdays. In addition, NES per the first and third definitions was 1.2 to 1.6
more present among young adults (18 to 30 years old) than any other age group of the
participants of both surveys.
In contrast to Tholin’s et al. (2009) findings, Striegel-Moore et al. (2006) found a
significant inverse relationship between BMI and NES per the first NES definition among the
participants of one of the surveys. This conclusion seemed to be consistent with Marshall et al.
(2004) and Tholin et al. (2009) in assuming a particular role of NES in the development of
obesity where a significant portion of Marshall et al. (2004) subjects reported that NES
manifestation was prior to the development of obesity. On the other hand, the reliance on a
single day food record and the inability of both surveys to investigate other significant features

15
of NES were among the limitations of Striegel-Moore et al. (2006) that hinders the ability to
assert a definitive relationship between BMI and NES.
Latent class analysis (LCA) is a method used to classify diseases into subtypes and
categories. According to Striegel-Moore et al. (2008), LCA had been used with NES where an
LCA based questionnaire was administered to 8,250 NHANES-III respondents aging from 15 to
39 years old in an exploratory study. They examined the possibility of classifying NES on the
basis of its symptoms into subtypes and examined the relationship between NES and mood
disorders, as well as compared the food intake of NE patients with non NE subjects.
The subjects underwent a medical examination to collect anthropometric information,
they also completed the diagnostic interview schedule in order to detect certain psychological
disorders including NES. The subjects also completed a 24 hours food recall. Then, they were
assigned to two groups the night eaters (NE) and the non-NE, where NE group were those who
were identified with NES (n= 2,068). The non-NE group (n= 6,182) were used as a comparison
group. The NES definition used in the study was eating 50% or more of total daily kilocalories
after 7:00 pm or any eating after 11:00 pm. The NE group underwent LCA that included major
NES symptoms such as depression, skipping breakfast, obesity, anorexia and sleeping
disturbances.
Striegel-Moore et al. (2008) found the NE group had a significantly higher food intake,
higher sodium intake, higher prevalence of depression, and higher prevalence of skipping
breakfast than the comparison group This presented the possible susceptibility of NES patients to
morbid obesity and hypertensive disorders which was consistent with the assumptions of
Marshall et al., 2004, Tholin et al., 2009, and Striegel-Moore et al., 2006.

16
The findings of Striegel-Moore et al. (2008) indicated that NES could be categorized into
four classes on the basis of depression and time of food intake. These categories were
significantly different among the NE group members. The four classes were non-depressed late
night eaters, non-depressed evening eaters, depressed late night eaters, and depressed evening
eaters respectively. Where the first and third group included those who consumed most of their
daily kilocalories after 11:00 pm. While the second and fourth group included those who
consumed most of their daily kilocalories after 7:00 pm.
To conclude, time of food intake and depression seemed to be the best factors in
classifying NES as a condition in which Striegel-Moore et al. (2008) reported NES patients
seemed to have unhealthy dietary habits that might exacerbate their condition if not treated.
NES Associations with Psychological Stress
NES is a relatively new condition and exploring the significance of the relationship
between NES and its most observable symptoms is extremely important in order to address NES
properly and produce a sound and accurate define the condition. Therefore, Colles et al. (2007)
conducted a cohort study on 431 subjects aging between 18 to 70 years old in order to explore
the relationship between NES, obesity, BED and psychological distress.
Colles et al. (2007) administered various measurements to collect data from subjects
including an NES screening survey followed by interviews for validating the NES diagnosis
according to the narrow definition. The Beck Depression Inventory (BDI) was used to assess
depression symptoms and the Questionnaire on Eating and Weight Pattern Revised (QEWP-R)
was also used for BED assessment. A self-report questionnaire to collect various anthropometric
and demographic information was also included. The study found a significant positive
correlation between NES prevalence and a higher BMI score which indicated a significant

17
association between NES and obesity. This finding contradicts the findings of Striegel-Moore et
al. (2006). In addition, the subjects who were identified with NES and BED had significantly
higher scores on the BDI than subject with only NES (20.80 and 13.90 respectively) thus
indicating that NES and BED together were significantly associated with more depressive
symptoms. However NES alone was not significantly associated with depression, which asserted
the importance of controlling the overlap between NES and BED in order to yield accurate
findings on the association of NES with depression.
Obesity was significantly associated with NES (Marshall et al., 2004; Tholin et al., 2009;
Colles et al., 2007). Additional investigation of the correlation of psychological problems with
NES could be relevant to establishing accurate diagnostic criteria for NES. To address this
relationship, Calugi, Dalle Grave and Marchesini (2009) conducted a cross-sectional
observational study on 266 subjects aging from 25 to 65 years old with a BMI of 35 or greater.
The purpose of the study was to explore the relationship between metabolic disorders and
psychological features of NES in moderately to severely obese subjects.
Calugi et al., (2009) conducted direct interviews and performed laboratory assessments
with subjects to collect data. In addition, a NE questionnaire and BDI were administered to
identify depression symptoms as well as NES according to the broad definition. Subjects who
were identified with NES had undergone an interview to validate a NES diagnosis. Twenty-
seven subjects were identified with NES and they had significantly higher BDI scores than non-
NE participants. This indicated a significant association between NES and depression in obese
subjects where depression was more prevalent among NES patients than non-NES subjects
without the influence of BED symptoms.

18
The findings of Calugi et al., (2009) among obese subjects could imply that a depressed
mood and NES could be major obstacles toward successful and sustainable weight loss regimen,
they also were inconsistent with Colles et al. (2007) findings. However, the history of NES and
its impact on depression and past weight loss attempts among the subjects was not adequately
considered in the study design by Colles et al. (2007). In addition, the participants were patients
of a medical center and were not selected from the general population, which might hinder the
ability to generalize the findings of the study and negatively influenced its implications for
practice.
NES Associations with Obesity
As previously mentioned, NES was found to be more common among obese patients
(Tholin et al., 2009). However, Marshall et al. (2004) reported that the condition was usually
studied among obese patients, which indicate that there was inadequate literature on NES among
non-obese patients. Therefore, Marshall et al. (2004) conducted a study to compare the
characteristics of obese subjects with NES and non-obese subjects with NES. The study
included 101 subjects who identified themselves as NES patients and were divided into three
groups. The first group consisted of forty obese subjects with a BMI greater than 30, the second
group were forty subjects with a BMI less than 25 and third group were 21 subjects who had a
BMI greater than 30. The first and second groups responded to the Night Eating Questionnaire
(NEQ) on a website. While the third group was subject to a personal interview that included nine
of the 14 items NEQ in order to verify NES diagnosis.
Marshall et al. (2004) compared the first group with the third group and found no
significant differences. However, the second group had significantly younger age, more
awakening at night, more frequent eating and more food cravings than the first group. In

19
accordance with (Marshall et al., 2004; Tholin et al., 2009; Striegel-Moore et al., 2006)
assumptions, The study findings indicated the potential role of NES in the development of
obesity, as Napolitano, Head, Babyak and Blumenthal (2001), reported that NES patients
developed obesity a younger age than non NES obese patients. In addition, 52% of the third
group in the study said they had NES before they developed obesity.
On the other hand, Marshall et al. (2004) relied on self-reported data, which might limit
the ability to generalize its findings. The study attributed the insomnia that usually accompany
NES patients to the decreased concentration of melatonin and other hormones among NES
patients which led the authors to recommend the use of certain antidepressants to treat NES
among non obese patient to be as effective as among obese NES patient because of the strong
similarity between the first and the second group in the study (Marshall et al., 2004).
Effectiveness of Certain Antidepressants in Treating NES
According to O’Reardon et al. (2006), several treatments had been suggested for NES
including phototherapy, progressive muscular relaxation and selective serotonin reuptake
inhibitors (SSRIs) such as sertraline. However, further research is required to investigate the
effectiveness of each treatment. O’Reardon et al. (2006) conducted a randomized placebo
controlled study for eight weeks on 34 participants aging 18 years or older to evaluate the
efficacy of sertraline in treating NES. Several procedures were administered for data collection
including a structured clinical interview for NES diagnosis, food diaries and eating disorders
exam to detect other eating disorders.
The subjects were randomly assigned to two groups where the first group (n= 17)
received 50mg/day sertraline and the second group (n=17) received placebo (O’Reardon et al.,
2006). During the study, anthropometric measurements were recorded and NE Symptoms Scale

20
(NESS) was administered to measure NE severity. The Clinical Global Impression scale (CGI)
was also administered to assess the improvement and severity of NES symptoms. The results
indicated that Sertraline group had significantly lower CGI and NESS scores than the placebo
scores for weeks four, six and eight. These finding indicated that sertraline (with no behavioral
or psychological intervention) was effective in improving NES symptoms. The small sample
size and the short duration of study were among the limitations toward confirming the positive
long-term effects of sertraline in treating NES.
Conclusions
Across the reviewed literature, this chapter explored the prevalence and classification of
NES as well as the significance of NES association with obesity and psychological distress along
with the effectiveness of sertraline in treating NES. The findings of Striegel-Moore et al. (2008)
suggested that time of food intake and depression played significant roles in the diagnosis,
classification and prevalence of NES. Thus, they should be included upon establishing diagnosis
criteria for NES.
The management of depression and obesity should constitute a significant part of NES
treatment as they were found to be highly associated with NES and vise versa where NES was
repeatedly suggested as an important factor in the development of obesity (Marshall et al., 2004;
Tholin et al., 2009; Colles et al.; 2007). In addition, even with non-obese NES patients,
sertraline could produce significant benefits with NES and its long-term effects should be
carefully monitored when treating NES (O’Reardon et al., 2006).
Several studies investigating NES had indicated some areas for further research such as
controlling and investigating the common overlapping between NES and BED (Striegel-Moore
et al., 2006), accurate definition and investigation of other NES characteristics and supporting

21
the continuous efforts toward the development of standard diagnostic criteria of NES. In
addition, the impact of genetic and endocrine factors on the etiology of NES as well as the
efficacy of other intervention strategies for NES treatment and prevention were indicated for
further research as well.

22
Chapter III: Methodology
NES was believed to be a relatively new eating disorder and it, at this point, has no
formal definition or diagnostic criteria. However, NES is suspected of causing obesity or
contributing to the worsening of obesity (Striegel-Moore et al., 2008). Therefore, understanding
NES is extremely important to the treatment of obese patients with NES and to the prevention of
obesity among non-obese patient with NES. This research was intended to evaluate the
relationship between NES and BMI among the students of the University of Wisconsin-Stout. In
this chapter, subject selection methods along with a detailed description of the instrument used to
collect the data were discussed. In addition, data collection procedures, data analysis and the
limitations related to sampling, data collection and statistical analysis are addressed in this
chapter.
Subject Selection and Description
Subject recruitment for this research was carried out after the approval of the University
of Wisconsin-Stout Institutional Review Board for the Protection of Human Subjects in Research
(Appendix A). The investigator asked the University of Wisconsin-Stout office of Planning,
Assessment, Research and Quality (PARQ) to provide a randomly selected sample of 924
university students emails during the fall semester of 2012. Then, the survey (Appendix B) was
distributed to the subjects via email that contained an implied consent (Appendix C), which was
stated that when subjects submit their surveys, they gave their implied agreement to participate
in this research. In addition, it was impossible to identify subjects if they decided not to
participate.

23
Instrumentation
The data were collected through a survey that was created using Qualtrics. The survey
was distributed to 924 randomly chosen University of Wisconsin-Stout students through email
and it was a self-administered questionnaire that contained 21 items. Four questions of the
survey collected demographic information such as age, gender, weight and height. An additional
four questions asked subjects whether they were following a weight loss diet, had a condition
that affected their eating such as diabetes or hypertension and whether they were pregnant,
breastfeeding or working night shifts. These four questions were the exclusion criteria because
all of these conditions might have affected the subjects’ food intake particularly at night, which
could have negatively influenced the research findings.
The remaining 13 items of the survey were drawn from the Night Eating Questionnaire
(NEQ), which was well known to be valid and reliable in assessing the severity of NES
symptoms (Marshall et al., 2004). The 13 items from NEQ were self administered questions
concerning NES symptoms such as percentage of calories consumed at night, morning appetite,
troubled sleeping, night snacking, level of feeling depressed, and how much awareness and
control the subjects have over NES. As mentioned earlier, the survey was distributed to 924
randomly chosen students via email during the fall semester of 2012.
Data Collection
The 21 items survey was administered to 924 randomly chosen students. An implied
informed consent was obtained from subjects by submitting their responses. The data collected
from subjects included gender, age groups, weight, height and BMI was calculated from these
data by dividing the weight in kilograms on the squared height in meters. Subjects who met the
exclusion criteria by being pregnant, breastfeeding, night shift workers or having a condition that

24
affected eating were excluded from research. In addition, the subjects responses to the 13 items
from NEQ were collected and a score ranging from zero to four was calculated based on the
responses to each of the 13 NEQ items and given to each subject where acquiring score of four
represented very severe NES symptoms and acquiring a score of zero represented very mild NES
symptoms
Data Analysis
After collecting the data, appropriate descriptive statistics were run. In addition, BMI
was calculated for each subject by dividing subject’s height in meters squared on subjects weight
in kilograms. Subjects with a BMI below 18.5 were considered underweight, while subjects with
a BMI between 18.5 and 24.9 were considered normal weight subjects. Moreover, subjects with
a BMI from 25 to 29.9 were considered overweight subjects and subjects with a BMI of 30 or
more were considered obese subjects.
The scores of each subject on each of the 13 NEQ items were added together and an
average overall score ranging from zero to four was calculated for each subject. Then, Pearson’s
correlation was calculated between the two variables of average overall NE scores and subjects
BMI to investigate the relationship between NES and BMI. Furthermore, subjects were divided
into two group, the first group was subject who had an overall NE average score below two,
while the second group were those with an average NE score of two or more. Then a two-
sample t test was conducted to investigate the difference between the two groups.
Subjects were classified into two groups again on the basis of their BMI, where the first
group had a BMI of 24.9 or lower and the second group had a BMI of 25 or higher, then another
two sample t test was conducted to investigate whether there was a significant difference in the
average NES score between overweight and normal weight subjects.

25
As for gender, subjects were also classified according to their gender where a two-sample
t test was applied to investigate the difference in average NE scores between male and female
subjects.
Limitations
Reporting weight can be a sensitive topic for some participants especially for young
females. Thus, under-reporting of body weight might be a limitation of this investigation.
As for the survey, there were not any known surveys specifically designed for the
purposes of this investigation. Hence, the items included in the survey might be inadequate to
accurately detect NES. In addition, the majority of the survey questions were multiple-choice
questions, which might limit the participants’ options to report the data accurately and thus the
survey validity could be affected.
As mentioned earlier, the survey was distributed electronically. However, technical issues
related to the University of Wisconsin-Stout network or students’ email settings might have
limited the survey availability and functionality. In addition, timing is very important in which
the survey could be distributed during a busy time for the participants, which might lead to
ignoring the survey or filling it out inaccurately.

26
Chapter IV: Results
This research project investigated the relationship between NES and BMI among the
University of Wisconsin-Stout students during the fall semester of 2012. As mentioned earlier,
NES is new eating condition for which there is no formal definition or diagnostic criteria for at
this time (Striegel-Moore et al., 2008). Therefore, an electronic survey was developed in order
to collect demographic data from subjects. In addition, there were 13 items in the survey that
were drawn from another study (Marshall et al., 2004) for the purpose of evaluating the severity
of NES signs and symptoms among subjects. Data were collected electronically through
submission of surveys by subjects into Qualtrics. In this chapter, data analysis and the results of
this research were discussed including some demographic data on subjects as well as a two
sample t tests to detect any differences among subjects average NES scores with regards to age,
gender and BMI. In addition, the results of Pearson’s correlation and regression to evaluate how
significantly BMI can predict subjects’ average NES scores were also reported in this chapter.
Survey Response
The survey was distributed to 924 students. Subjects who had a chronic condition that
affected their eating and subjects who were following a weight loss diet as well as subjects who
did not complete the entire survey were excluded from the study. In addition, subjects who were
pregnant, breastfeeding or working the night shift were also excluded from the study.
Item Analysis
Only 99 subjects’ data were analyzed out of 198 subjects recruited for this research. The
subjects excluded from the study (n=99) because they met one or more exclusion criteria that
included pregnancy, breastfeeding, any chronic condition that affects eating habits, following a
weight loss diet, working night shifts and incomplete surveys.

27
Demographics. The demographic data analyzed included age, gender, height and
weight. Overall, there were more female subjects (n=58) in this research than male subjects
(n=41) where males and females constituted 41% and 59% of all subjects included in this study
respectively. Table 2 shows that 77% of the subjects (n=99) were in the age group of 18 to 24
years old where females (n=47) represent nearly 62% of the subjects in that age group. Female
subjects represented 67% of the 31 to 35 age group and the 36 to 40 age group. On the other
hand, Table 2 also indicated that male subjects represented 64% of the 25 to 30 years age group.
Table 2
Demographic Characteristics of Subjects (n=99) Including BMI and Average NES Score.
Subjects Characteristics Male Subjects Female Subjects Total
Gender 41 (41%) 58 (59%) 99 (100%)
Age
Group
18 - 24 years old 29 (29%) 47 (48%) 76 (77%)
25 - 30 years old 7 (7%) 4 (4%) 11 (11%)
31 - 35 years old 1 (1%) 2 (2%) 3 (3%)
36 - 40 years old 1 (1%) 2 (2%) 3 (3%)
41 years old and older 3 (3%) 3 (3%) 6 (6%)
Height (cm) (M, SD) (176.93, 7.40) (165.91, 7.31) (170.48, 9.12)
Weight (Kg) (M, SD) (79.04, 16.18) (66.07, 17.30) (71.44, 17.95)
BMI (M, SD) (25.34, 5.41) (23.92, 5.52) (24.50, 5.50)
Average NE Score (M, SD) (1.28, 0.50) (1.15, 0.40) (1.20, 0.45)
As shown in table 2, height and weight data were collected from subjects in feet and
inches, and then height was converted to centimeters. Weight data were also was collected in
28
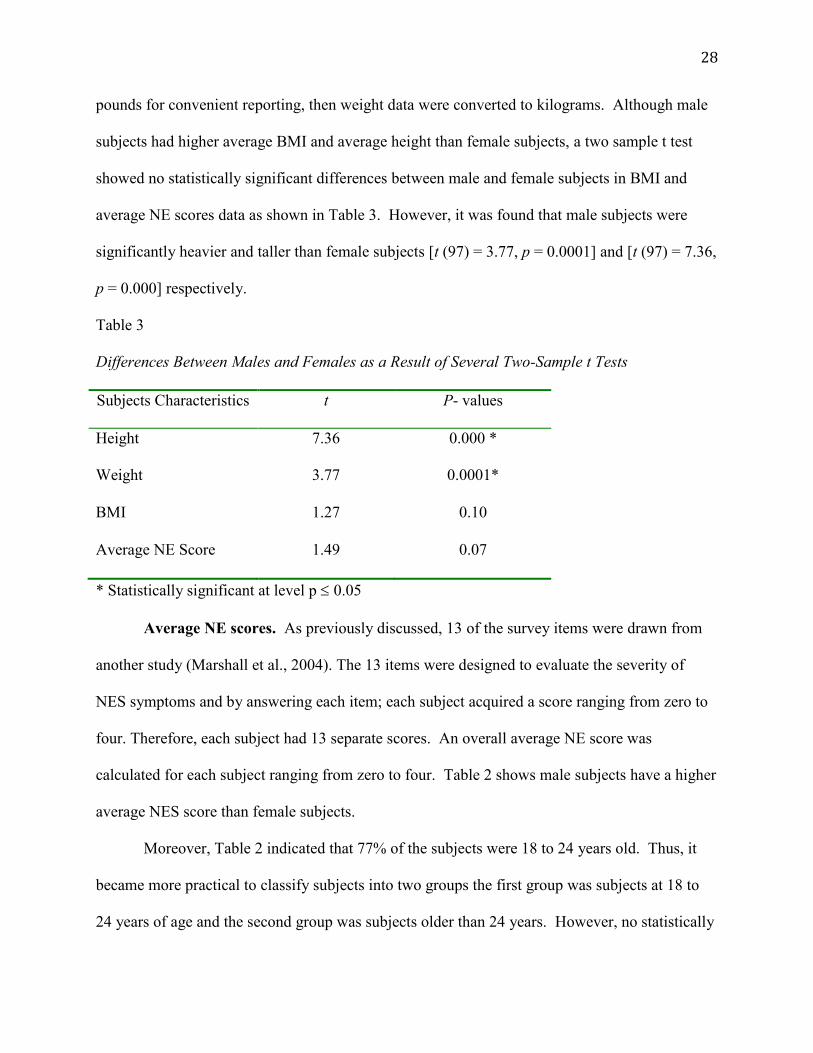
pounds for convenient reporting, then weight data were converted to kilograms. Although male
subjects had higher average BMI and average height than female subjects, a two sample t test
showed no statistically significant differences between male and female subjects in BMI and
average NE scores data as shown in Table 3. However, it was found that male subjects were
significantly heavier and taller than female subjects [t (97) = 3.77, p = 0.0001] and [t (97) = 7.36,
p = 0.000] respectively.
Table 3
Differences Between Males and Females as a Result of Several Two-Sample t Tests
Subjects Characteristics t P- values
Height 7.36 0.000 *
Weight 3.77 0.0001*
BMI 1.27 0.10
Average NE Score 1.49 0.07
* Statistically significant at level p 0.05
Average NE scores. As previously discussed, 13 of the survey items were drawn from
another study (Marshall et al., 2004). The 13 items were designed to evaluate the severity of
NES symptoms and by answering each item; each subject acquired a score ranging from zero to
four. Therefore, each subject had 13 separate scores. An overall average NE score was
calculated for each subject ranging from zero to four. Table 2 shows male subjects have a higher
average NES score than female subjects.
Moreover, Table 2 indicated that 77% of the subjects were 18 to 24 years old. Thus, it
became more practical to classify subjects into two groups the first group was subjects at 18 to
24 years of age and the second group was subjects older than 24 years. However, no statistically

29
significant differences were found between the two groups in average NES scores [t (97) = -
0.89, p = 0.19].
BMI and average NE scores. Another two-sample t test showed no statistically
significant differences between males’ and females’ average NES score as reported in Table 3 [t
(97) = 1.49, p = 0.07]. Subjects were classified into two groups according to their BMI where
the normal weight group were subjects with a BMI of 24.9 or lower and the overweight group
were subjects with a BMI of 25 or higher. Then, a two-sample t test indicated no statistically
significant differences between the overweight and normal weight group in average NE scores [t
(97) = - 1.31, p = 0.10] which indicated a slight if any effect at all of BMI on average NES
scores.
A regression analysis was run and it indicated that the subjects’ BMI was not a
statistically significant predictor of average NE score [F (1,97) = 2.56, p = 0.11]. However,
Pearson’s correlation coefficient was calculated to investigate the association between subjects’
BMI data and their average NE score and there was a weak positive correlation between the two
variables (r = 0.16). In addition, Figure 1 showed that the relationship between BMI and
average NE score which tended to be positive, but not enough to generate a statistical
significance which indicated that a larger sample size might reveal a stronger and perhaps a
statistically significant association between BMI and average NE scores.

30
Figure 1. A scatter plot showing the relationship between subjects’ BMI and average NE scores
Conclusion
Overall, 99 subjects were included in this research where 59% of the subjects
were females and 41% were males. As for age, 77% of the subjects were in the age group of 18
to 24 years. However, no statistically significant differences between males and females were
found in BMI and Average NE score. In addition, no statistically significant differences were
found between subjects in the 18 to 24 years age group and subjects in the other age groups in
average NE score. Moreover, overweight subjects and normal weight subjects were not
significantly different from each other in regards to the average NE score. Although there was a
weak positive correlation between BMI and average NE scores, BMI was not a statistically
significant predictor of average NE score.
0
0.5
1
1.5
2
2.5
3
0 20 40 60Subj
ects
' Ave
rage
NE
Sc
ores
Subjects' BMI data
Subjects' average NE scores and BMI data
average NES

31
Chapter V: Discussion
The purpose of this research was to investigate the relationship between NES and BMI
among the University of Wisconsin-Stout students during the fall semester of 2012. This chapter
served as a discussion of the findings of this research and the main conclusions of this paper
along with some of its limitations that were discussed in this chapter as well. Finally, this
chapter had also provided some recommendations for some of the areas where future research is
required.
The main objective of this research was to investigate the relationship between NES and
BMI. Although, the data analyzed in this research did not result in a statistically significant
association between NES and BMI, certain trends toward a positive correlation between NES
and BMI were noticed. But all these trends were not statistically significant. For instance, Figure
1 and Pearson’s correlation coefficient had both indicated a weak positive correlation between
NES and BMI. NES as variable was represented by the average NE score which was an average
total score calculated from the 13 scores of each NEQ item in the survey used in the study as a
data collection tool. These observations were consistent with the findings of (Marshall et al.,
2004; Tholin et al., 2009; Colles et al., 2007). However, Colles et al. (2007) indicated that the
overlapping between NES and BED could significantly impact the accuracy of such findings. On
the other hand, Striegel-Moore et al. (2006) found no significant associations between NES and
obesity and NES and male gender after testing for NES on the basis of several definitions for the
condition, which were applied on a very large sample.
The findings of this research showed that 77% of the subjects were in the 18 to 24 age
group, which made the findings of this research more representative of the 18 to 24 age group
than other age groups. To the investigator’s knowledge, there were no studies that focused on

32
this age group other than this research. Male subjects in this research were significantly heavier
and taller than female subjects and they had a higher average NE score than female subjects at (p
= 0.07) which are very close to a statistical significance. Such findings might imply an
association between the male gender and NES, which was reported by Colles et al. (2007) and
Tholin et al. (2009). However, Striegel-Moore et al. (2006) findings showed no association
between NES and the male gender. But Striegel-Moore et al. (2006) had reported an association
between NES and younger age. This could serve as a risk factor for NES and health education
efforts could include raising the awareness of young people to NES. This could be important for
those who were more likely to acquire an eating disorder and such education could help young
people avoid developing the condition at an early age.
In this research, 29.26% of male subjects were classified as overweight in which their
BMI values were larger than 24.9. While 19.51% of the male subjects were classified as obese
in which their BMI values exceeded 30. On the other hand, 20.69% of the female subjects were
classified as overweight, while only 6.90% of the female subjects were classified as obese as
their BMI values exceeded 30. Overall, 24.24% of all included subjects were classified as
overweight, while only 12.12% of all subjects were classified as obese. These findings are much
lower than the prevalence of obesity among adults in the USA, which is 33.9% (Ogden &
Carroll, 2010). The lower prevalence of obesity found in this research might be attributed to the
small sample size and possibly a higher education level of the subjects included in this study than
the national average. In addition, Striegel-Moore et al. (2008) findings suggested no association
between BMI and NES in which the investigators had reported that 15.65% of all subjects were
obese. However, there were no significant differences in the BMI data between subjects with
NES and subjects without NES. Similar to this research, Striegel-Moore et al. (2008) had

33
reported that the subjects were relatively at a younger age than most literature on NES. Marshall
et al. (2004) had also reported striking similarities between obese and non-obese NES patients
where the researchers suggested that NES might contribute to the development of obesity. These
findings might suggest that NES might progress in a bilateral fashion in which NES development
in non-obese young people could maximize the development of obesity. On the other hand, NES
development in obese and older subjects could be diagnosed as a complication of obesity.
Limitations
These research findings were limited by certain factors that could suppress the ability to
generalize the findings to a larger population. One of the key limitations in this research was the
inability to identify subjects with NES. The instrument used in this research was designed to
measure the severity NES signs and symptoms and it did not solely identify NES. Many studies
had used more than one instrument to validate NES diagnosis among subjects. For instance,
Calugi et al. (2009) had utilized the night eating syndrome inventory and history (NESHI) along
with NEQ to validate NES diagnosis. In addition, Colles et al. (2007) as well as Marshall et al.
(2004) had utilized an interview with a health care professional to validate NES diagnosis.
Another limitation of this study was the small sample size when compared to the
reviewed literature, which hindered the ability to produce a more generalized findings. However,
the busy life of college students might had a significant role in limiting the response rate of the
instrument used in this research. Moreover, Tholin et al. (2009) had excluded students from their
research and it was reported that the irregular lifestyle of students might lead to a higher food
intake during the nighttime for reasons other than NES. However, students along with others
who were excluded from the study (i.e. pregnant women, night workers) might constitute some
individuals with a high risk of developing NES and future research efforts should attempt to

34
include the commonly excluded subjects in NES study in order to improve the understanding and
the diagnosis of such condition. A third limitation of this research was the reliance on self-
reported data, which could potentially affect the validity and reliability of the findings in this
research.
Conclusions
The relationship between NES and BMI in this research was not statistically significant.
However, a weak positive association was found between NES and BMI among the subjects
included in this research. Although a statistically significant association was not established,
similar patterns were noticed in the findings of (Marshall et al., 2004; Tholin et al., 2009; Colles
et al., 2007). Furthermore, the findings if this research were also consistent with the findings of
Striegel-Moore et al. (2008) in which there were no statistically significant association between
NES and BMI.
Another conclusion of this research was that BMI did not appear to be a significant
predictor of average NE score [F (1,97) = 2.56, p = 0.11], which was also in accordance with the
findings of Striegel-Moore et al. (2008). In addition, the average NE scores did not significantly
differ between obese and non-obese subjects, which were consistent with findings of Marshall et
al. (2004). Tholin et al. (2009) had reported that male subjects were significantly more obese
than female subjects and which was quite similar to the findings of this research in which male
subjects were significantly heavier than female subjects [t (97) = 3.77, p = 0.0001]. Moreover,
Tholin et al. (2009) had also reported a higher NES prevalence among obese men than obese
women, however, this research had found a difference between male and female subjects in
average NE score that was close to a statistical significance [t (97) = 1.49, p = 0.07]. Overall,

35
BMI was not found to be significantly associated with NES, however, more controlled studies
with a larger sample sizes could reveal different findings.
Recommendations
NES was frequently studied among obese subjects who were relatively older adults.
However, certain studies had indicated the importance of studying the condition in younger
adults. For instance, Marshall et al. (2004) reported that the non-obese NES subjects were
significantly at a younger age than obese NES subjects. In addition, this research was conducted
among college students who were mostly in the age group of 18 to 24 years. According to
Napolitano et al. (2001), subjects with NES had developed obesity a younger age than non NES
obese subjects and 52% of the third group of subjects had reported developing NES before
obesity. Therefore, future research should also include non-obese subjects of young age more
often in order to initiate prevention and management efforts as early as possible.
On the other hand, Striegel-Moore et al. (2006) had indicated that the overlapping
between NES and BED had potential in confounding the findings of many studies investigating
NES. Therefore, future research on NES should strive to eliminate such overlapping in order to
produce more accurate findings. According to Birketvedt et al. (1999), certain endocrine and
genetic factors had potentially played a key role in the development and etiology of NES. Thus,
they should be researched more thoroughly in the future to accelerate the progression toward a
better understanding of the condition and consequently the establishment of formal diagnosis
criteria for NES. O’Reardon et al. (2006) had reported significant findings on using the
antidepressant Sertraline in the treatment of NES, however, the long term effects of Sertraline
should be further studied in the future to ensure the safety of subjects receiving long term
treatment of NES.

36
References
Allison, K., Wadden, T., Sarwer, D., Fabricatore, A., Crerand, C., Gibbons, L., & ... Williams, N.
(2006). Night eating syndrome and binge eating disorder among persons seeking bariatric
surgery prevalence and related features. Obesity (Silver Spring, Md.), 14 Suppl 277S-
282S. doi: 10.1038/oby.2006.286
Binge eating. (n.d.). Medlineplus. Retrieved February 10, 2012, from
http://www.nlm.nih.gov/medlineplus/ency/article/003265.htm
Birketvedt, G., Florholmen, J., Osterud, B., Dinges, D., Bilker, W., & Stunkard, A. (1999).
Behavioral and neuroendocrine characteristics of the night eating syndrome. Journal of
The American Medical Association, 282(7), 657-663. doi:10.1001/jama.282.7.657
Body mass index. (n.d.). Retrieved October 1, 2010, from:
http://www.cdc.gov/healthyweight/assessing/bmi
Calugi, S. S., Dalle Grave, R. R., & Marchesini, G. G. (2009). Night eating syndrome in class II–
III obesity metabolic and psychopathological features. International Journal of Obesity,
33(8), 899-904. doi:10.1038/ijo.2009.105
Colles, S. L., Dixon, J. B., & O'Brien, P. E. (2007). Night eating syndrome and nocturnal
snacking association with obesity, binge eating and psychological distress. International
Journal Of Obesity, 31(11), 1722-1730. doi:10.1038/sj.ijo.0803664
Insomnia. (n.d.). Medlineplus. Retrieved February 10, 2012, from
http://www.nlm.nih.gov/medlineplus/ency/article/000805.htm
Marshall, H. M., Allison, K. C., O'Reardon, J. P., Birketvedt, G., & Stunkard, A. J. (2004). Night
eating syndrome among nonobese persons. International Journal Of Eating Disorders,
35(2), 217-222. doi:10.1002/eat.10241

37
Napolitano, M. A., Head, S., Babyak, M. A., & Blumenthal, J. A. (2001). Binge eating disorder
and night eating syndrome psychological and behavioral characteristics. International
Journal Of Eating Disorders, 30(2), 193-203.
Obesity. (n.d.). Medlineplus. Retrieved March 8, 2012, from
http://www.nlm.nih.gov/medlineplus/ency/article/007297.htm
Ogden, C. L., & Carroll, M. D. (2010, June). Prevalence of overweight obesity and extreme
obesity among adults United States trends 1960–1962 through 2007–2008. Centers for
Disease Control and Prevention. Retrieved February 10, 2012, from
http://www.cdc.gov/nchs/fastats/overwt.htm
O’Reardon, J., Allison, K. C., Martino, N. S., Lundgren, J. D., Heo, M., & Stunkard, A. J.
(2006). A randomized placebo controlled trial of sertraline in the treatment of night
eating syndrome. The American Journal of Psychiatry, 163(5), 893-898. Retrieved from
http://ajp.psychiatryonline.org/article.aspx?articleID=96586
Rand, C. S., Macgregor, A. M., & Stunkard, A. J. (1997). The night eating syndrome in the
general population and among postoperative obesity surgery patients. International
Journal of Eating Disorders, 22(1), 65-69. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/9140737
Striegel-Moore, R., Franko, D., Thompson, D., Affenito, S., May, A., & Kraemer, H. (2008).
Exploring the typology of night eating syndrome. International Journal of Eating
Disorders, 41(5), 411-418. doi:10.1002/eat.20514
Striegel-Moore, R. H., Franko, D. L., Thompson, D., Affenito, S., & Kraemer, H. C. (2006).
Night eating prevalence and demographic correlates. Obesity Research, 14(1), 139-147.
doi:10.1038/oby.2006.17

38
Tholin, S., Lindroos, A., Tynelius, P., Åkerstedt, T., Stunkard, A. J., Bulik, C. M., & Rasmussen,
F. (2009). Prevalence of night eating in obese and non obese twins. Obesity (Silver
Spring), 17(5), 1050-1055. doi:10.1038/oby.2008.676

39
Appendix A
May 23, 2012 Fahad A Aldawood MSC Food and Nutritional Sciences UW-Stout RE: The Relationship between Night Eating Syndrome and Body Mass Index Among College Students Dear Fahad, The IRB has determined your project, "The Relationship between Night Eating Syndrome and Body Mass Index Among College Students” is Exempt from review by the Institutional Review Board for the Protection of Human Subjects. The project is exempt under Category 2 & 3 of the Federal Exempt Guidelines and holds for 5 years. Your project is approved from May 17, 2012, through May 16, 2017. Should you need to make modifications to your protocol or informed consent forms that do not fall within the exemption categories, you will need to reapply to the IRB for review of your modified study. If your project involved administration of a survey, please copy and paste the following message to the top of your survey form before dissemination:
If you are conducting an online survey/interview, please copy and paste the following message to the top of the form: “This research has been reviewed by the UW-Stout IRB as required by the Code of Federal Regulations Title 45 Part 46.” Informed Consent: All UW-Stout faculty, staff, and students conducting human subjects research under an approved “exempt” category are still ethically bound to follow the basic ethical principles of the Belmont Report: 1) respect for persons; 2) beneficence; and 3) justice. These three principles are best reflected in the practice of obtaining informed consent from participants. If you have questions, please contact Research Services at 715-232-1126, or [email protected], and your question will be directed to the appropriate person. I wish you well in completing your study. Sincerely,
Susan Foxwell Research Administrator and Human Protections Administrator, UW-Stout Institutional Review Board for the Protection of Human Subjects in Research (IRB) Cc: Dr. Sally Dresdow

40
Appendix B
“This research has been reviewed by the UW-Stout IRB as required by the Code of Federal Regulations Title 45 Part 46.”
By completing the following survey you agrees to participate in the research titled The Relationship between Night Eating Syndrome and Body Mass Index Among College
Students
Night Eating Questionnaire Q1 Please select your age group: 18 - 24 years old (1) 25 - 30 years old (2) 31 - 35 years old (3) 36 - 40 years old (4) 41 years old and older (5)
Q2 What is your gender? Male (1) Female (2)
Q3 Do you have any chronic condition that affects your eating (e.g. Diabetes, Hypertension, Celiac disease or other conditions) Yes (1) No (2)
If Yes Is Selected, Then Skip To End of Survey
Q4 Are you following a weight loss diet? Yes (1) No (2)
If Yes Is Selected, Then Skip To End of Survey
Q5 Are you pregnant or breastfeeding? Yes (1) No (2)
If Yes Is Selected, Then Skip To End of Survey

41
Q6 In the past 7 days, have you worked during the night time? Yes (1) No (2)
If Yes Is Selected, Then Skip To End of Survey
Q7 Please enter your height in feet and inches
Feet (1) Inches (2)
Q8 Please enter your weight in pounds:
Pounds (1)
Q9 In the past 7 days, how would you rate your food appetite in the morning: High (0) Moderate (1) Low (2) Very low (3) No appetite at all (4)
Q10 In the past 7 days, on average what time did you had your first meal of the day: 6:30 - 7:29 (0) 7:30 - 10:29 (1) 10:30 - 13:29 (2) 13:30 - 16:29 (3) 16:30 - 18:00 (4)
Q11 In the past 7 days, please estimate the percentage of food consumed after 7:00 pm from the total calories you consume per day: 0% (0) 1% - 25% (1) 26% - 50% (2) 51% - 75% (3) 76% - 100% (4)

42
Q12 In the past 7 days, how often did you had trouble sleeping: Never (0) Sometimes (1) Half the time (2) Usually (3) Always (4)
Q13 In the past 7 days, please estimate the number of times you awakened at night: Never (0) Once a month (1) Once a week (2) Once a night (3) More than once a night (4)
Q14 In the past 7 days, please estimate the number of times you were snacking at night Never (0) Sometimes (1) Half the time (2) Usually (3) Always (4)
Q15 Night Eating Syndrome is a condition that involve poor appetite in the morning, excessive eating in the evening, troubled sleeping, evening tension and/or feeling upset How would you estimate your level of awareness that you might have night eating syndrome: Unaware (0) Mostly unaware (1) Partially aware (2) Mostly aware (3) Completely aware (4)
Q16 In the past 7 days, how would you estimate the level of your feelings of sadness: Not at all (0) A little (1) Somewhat (2) Very much so (3) Extremely (4)
43
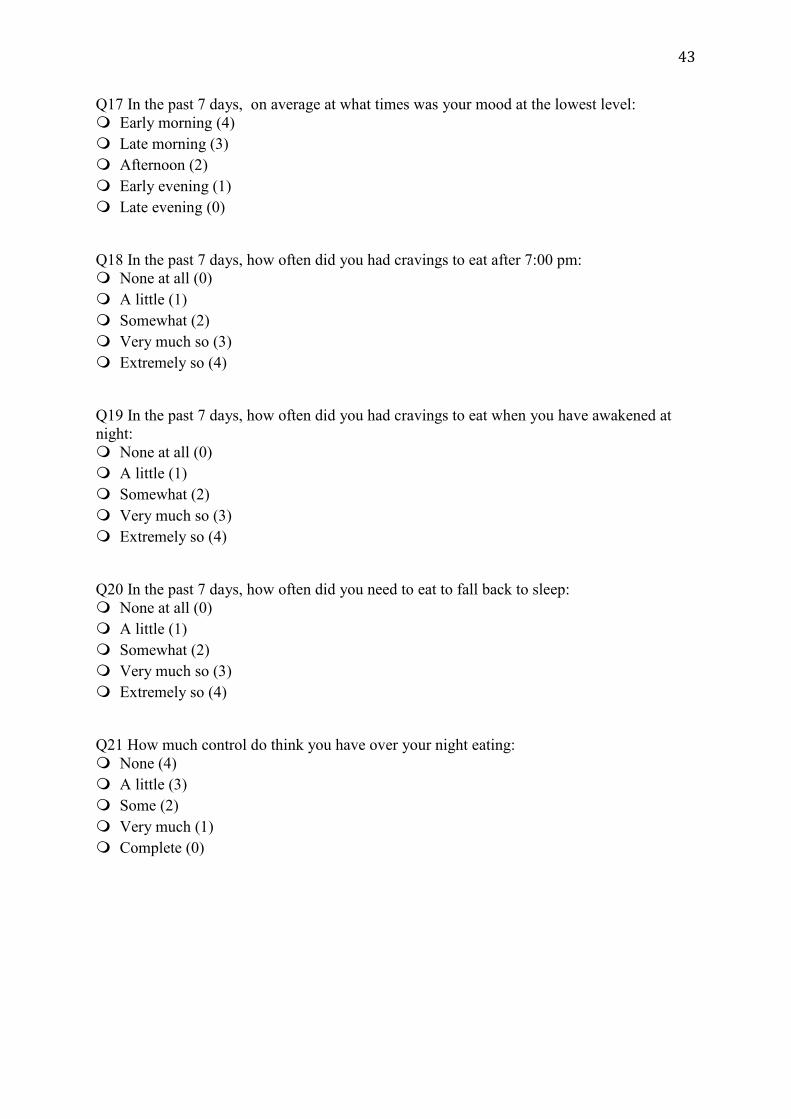
Q17 In the past 7 days, on average at what times was your mood at the lowest level: Early morning (4) Late morning (3) Afternoon (2) Early evening (1) Late evening (0)
Q18 In the past 7 days, how often did you had cravings to eat after 7:00 pm: None at all (0) A little (1) Somewhat (2) Very much so (3) Extremely so (4)
Q19 In the past 7 days, how often did you had cravings to eat when you have awakened at night: None at all (0) A little (1) Somewhat (2) Very much so (3) Extremely so (4)
Q20 In the past 7 days, how often did you need to eat to fall back to sleep: None at all (0) A little (1) Somewhat (2) Very much so (3) Extremely so (4)
Q21 How much control do think you have over your night eating: None (4) A little (3) Some (2) Very much (1) Complete (0)

44
Appendix C
Consent to Participate in UW-Stout Approved Research
Title: The Relationship between Night Eating Syndrome and Body Mass Index Among College Students Investigator Fahad A Aldawood [email protected] 715-254-5576
Research Sponsor Dr. Sally Dresdow [email protected] 715-232-3085
Description: The objective of this study is to investigate the relationship between night eating syndrome and body mass index among the University of Wisconsin-Stout students who are 18 years or older. Risks and Benefits: There are no major risks in this research and there are no direct benefits to any subject. A summary of results will be sent if requested. This research will help educate students about the association between night eating syndrome and obesity Time Commitment and Payment: The survey used in this research will take approximately 20 minutes to complete and there is no compensation or rewards for participation. Confidentiality: Your name will not be included in on any documents. We believe that you cannot be identified form any answers you provide. Right to Withdraw: Your participation in this research is entirely voluntary. You may choose not to participate without any adverse consequences to you. You have the right to stop the survey at any time. However, should you submit your survey and later wish to withdraw from the study, the data cannot be linked to you and cannot be withdrawn. IRB Approval: This study has been reviewed and approved by The University of Wisconsin-Stout's Institutional Review Board (IRB). The IRB has determined that this study meets the ethical obligations required by federal law and University policies. If you have questions or concerns regarding this study please contact the Investigator or Advisor. If you have any questions, concerns, or reports regarding your rights as a research subject, please contact the IRB Administrator. Investigator: IRB Administrator Fahad Aldawood Sue Foxwell, Director, Research Services [email protected] 152 Vocational Rehabilitation Bldg. 715-254-5576 UW-Stout Menomonie, WI 54751 Advisor: [email protected] Dr. Sally Dresdow [email protected] 715-232-3085 Statement of Consent: By completing the following survey you agree to participate in the project entitled, The Relationship between Night Eating Syndrome and Body Mass Index Among College Students