the radiological diagnosis asbestosis - thorax
TRANSCRIPT

Thorax (1960), 15, 103.
THE RADIOLOGICAL DIAGNOSIS OF ASBESTOSISBY
ROGER WILLIAMS* AND P. HUGH-JONESFrom the Department of Medicine, Postgraduate Medical School of London
(RECEIVED FOR PUBLICATION DECEMBER 21, 1959)
The recognition of different pneumoconioses isusually based on a history of exposure to a givendust together with the presence of characteristicchanges in the chest radiograph. This implies thatthe radiological appearances are reasonablyspecific. Moreover, if they are to be used not onlyfor clinical diagnosis but also for compensationpurposes, and for the study of the disease inrelation to factors such as environmental condi-tions or the changes in lung function, then theradiographic appearances need to be recognizedand graded with little variation between differentobservers.
In asbestosis the changes described as beingcharacteristic are a ground-glass mottling of thelung fields, especially in the lower parts, togetherwith pleural thickening and a shaggy border to theheart (Fig. 1). Unfortunately no satisfactoryclassification of these changes has been producedand the international classification applicable toother pneumoconioses is not easily applied toasbestosis (International Labour Organization,1959).During an investigation into the significance of
lung function changes in asbestosis (Williams andHugh-Jones, 1960) it became necessary to try andrelate the results of lung function tests to anindependent assessment of the degree of change inthe patient's radiograph. The study described inthis paper was therefore made in order todetermine not only the specificity of the radio-logical changes in asbestosis but to see to whatextent their diagnosis and grading were affected byobserver variability.
DESCRIPTION OF STUDYA set of 53 films was chosen from the following
subjects:(1) Thirty-eight patients with asbestosis, who were
the first 38 cases in the series used for lung functionstudies and included certified cases (21), patients whohad had prolonged exposure to asbestos dust but hadno symptoms and whose radiographs had previously
*Present address: Medical Unit, Royal Free Hospital, Gray's InnRoad, London, W.C.1.
been regarded as clear (10), and a number who hadbeen referred because of atypical clinical or radio-logical changes (7).
(2) Six normal subjects.(3) Nine patients with other chronic respiratory
diseases (four with chronic bronchitis and emphysema,three with sarcoidosis, and two with coalworkers'pneumoconiosis).They were arranged in random order, names and
identification numbers being obscured by a mask.The films were viewed on separate occasions by
two panels of observers. On the first occasion thepanel of five observers (A to E) consisted of threechest physicians and one radiologist from Hammer-smith Hospital together with a visiting Americanradiologist. Two of the physicians had had specialexperience in the development of similar trials incoalworkers' pneumoconiosis. On the second occasionthe panel consisted of six senior medical officers ofthe pneumoconiosis medical panels (observers F toK). The films were read " blind," the only informa-tion given to the observers being that the films werefrom normal subjects and from patients withasbestosis, and the other chronic pulmonary fibrosis
_ 05;. \.
FIG. 1.-Classical radiological changes of asbestosis with ground-glass mottling of the lung fields, shaggy border to the heart, andpleural thickening.
on 24 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.103 on 1 June 1960. Dow
nloaded from
ROGER WILLIAMS and P. HUGH-JONES
>:W..ht
| E E ..-
I j C..l ..l ..., y.....X.
....
:..t.......> .
....
'H..
.::>..:
previously mentioned. Each observer recorded hisanswer to the following questions:
(1) Whether the film was normal.
(2) If abnormal, whether the changes seen were
consistent with asbestosis or were more likely to bedue to some other pulmonary fibrosis.
(3) If the film was considered to be consistent withasbestosis they were asked to record:
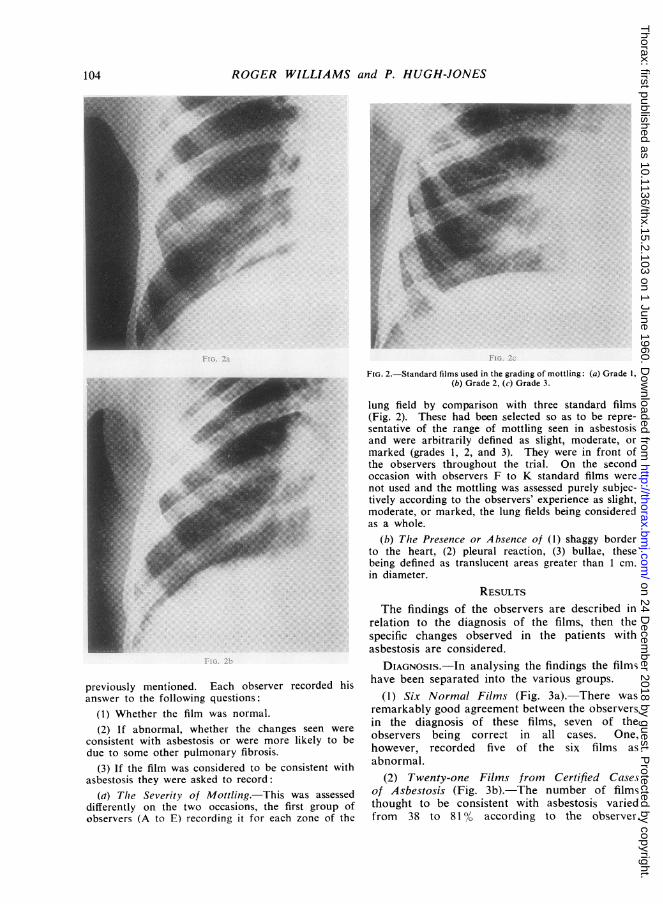
(a) The Severity of Mottling. This was assesseddifferently on the two occasions, the first group ofobservers (A to E) recording it for each zone of the
FIG. 2.-Standard films used in the grading of mottling: (a) Grade 1,(b) Grade 2, (c) Grade 3.
lung field by comparison with three standard films(Fig. 2). These had been selected so as to be repre-sentative of the range of mottling seen in asbestosisand were arbitrarily defined as slight, moderate, ormarked (grades 1, 2, and 3). They were in front ofthe observers throughout the trial. On the secondoccasion with observers F to K standard films werenot used and the mottling was assessed purely subjec-tively according to the observers' experience as slight,moderate, or marked, the lung fields being consideredas a whole.
(b) Tlhe Presence or Absence of (1) shaggy borderto the heart, (2) pleural reaction, (3) bullae, thesebeing defined as translucent areas greater than 1 cm.in diameter.
RESULTSThe findings of the observers are described in
relation to the diagnosis of the films, then thespecific changes observed in the patients withasbestosis are considered.
DIAGNOSIS.-In analysing the findings the filmshave been separated into the various groups.
(1) Six Normal Films (Fig. 3a). There wasremarkably good agreement between the observersin the diagnosis of these films, seven of theobservers being correct in all cases. One,however, recorded five of the six films asabnormal.
(2) Twenty-one Films from Certified Casesof Asbestosis (Fig. 3b). The number of filmsthought to be consistent with asbestosis variedfrom 38 to 81% according to the observer.
104
on 24 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.103 on 1 June 1960. Dow
nloaded from

RADIOLOGICAL DIAGNOSIS OF ASBESTOSIS
Although this gives some idea of the disagreementbetween the observers it does not show the fullpicture. For instance, observers D and H bothrecorded asbestosis in the same number of cases,yet only 10 of these 14 were the same films. Infact there were only two films in this group inwhich all 11 observers agreed on the presence ofchanges consistent with asbestosis. In Table I
TABLE IFILMS FROM 21 CERTIFIED CASES OF ASBESTOSISGROUPED ACCORDING TO NUMBER OF OBSERVERS
AGREEING WITH DIAGNOSIS
No. of Observers Agreeing on No. ofDiagnosis of Asbestosis Films
11 210 19 58 27 46 25 14 13 12 21 0
Total .. 21
the findings have been arranged to show the levelof agreement between the observers. It can beseen that if instead of complete agreement thefindings of the majority of the observers, i.e., sixor more, are considered, then the number of filmsdiagnosed as asbestosis is only increased to 16.The wide divergence of opinion seen in many
of the films in this group is illustrated by thefindings in Case 17 of the main series, where twoof the observers thought the film was normal,seven considered it was abnormal but showed no
/00
90
- 70
60
B50
~4
830
20
0
0,
ABCDEFGHI/JK A
(a) OBSERVERS
Normal/ E
AsbestosisE
(b)
FIG. 3.-The frequency of diagnosis of (a) normal films in six normalsubjects, (b) asbestosis in 21 certified cases.
(a) OBSERVERS (b)
FIG. 4.-The frequency of diagnosis of (a) normal films, (b) asbestosisand other pulmonary diseases in 10 patients exposed to asbestosdust but whose radiograph had previously been reported as clear.
changes consistent with asbestosis, and only oneagreed with the diagnosis of asbestosis previouslymade by the pneumoconiosis medical panel. Itwas of interest therefore to find that the patientdid have definite functional evidence of thedisease.
(3) Ten Films from Patients Exposed toAsbestos Dust but Radiologically ReportedClear (Fig. 4).-The observers differed widely inthe assessment of these films, the numberregarded as normal varying from 10 to 80%. Itmight be expected that the films of some of thesepatients would show early changes though perhapsthese might not be sufficiently marked to beregarded as abnormal. In fact the number offilms thought to show changes consistent withasbestosis varied from 0 to 50%. There were nofilms in this group in which there was completeagreement of opinion between the observers.
(4) Seven Films from Patients with QuestionableDiagnosis of Asbestosis Because of AtypicalClinical or Radiological Changes (Fig. 5a).-Itwas to be expected that there would be particulardifficulty in assessing the radiological appearancesin this group. In only one case did a majority ofobservers agree on the presence of changesconsistent with asbestosis. The majority of theifims were considered to be abnormal, though therewas one film which was thought to be normal byfour of the 11 observers..
(5) Ten Films from Patients with OtherPulmonary Diseases (Fig. 5b).-The main pointof interest in considering the findings in thisgroup was the number of films which were thought
105
on 24 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.103 on 1 June 1960. Dow
nloaded from

ROGER WILLIAMS and P. HUGH-JONES
/°°r90-
Z 70
J 60k8 50
40
030
20
/0
* Asbestosis
(a) OBSEVEfS (b)
FIG. 5.-The frequency of diagnosis of asbestosis in (a) seven patientsin whom the diagnosis had been questioned on atypical clinicalor radiological findings, (b) 10 patients with other pulmonarydiseases.
to show changes consistent with asbestosis. Thesevaried from 0 to 60% according to the observer.
THE SPECIFIC RADIOLOGICAL FEATURESMOrrLING. This will be described separately
for the two groups of observers since it was
assessed in a different way.
First Occasion (Observers A to E).-Standardfilms were used and each zone of the lung field wasconsidered separately. This was done to determinewhich part of the lung was mainly affected inasbestosis and whether there was a differencebetween the two sides. Pendergrass (1938) at one
time thought that the changes began more oftenon the left side than on the right and progressedmore on that side. The results showed that,although there was a considerable difference ofopinion between the observers on the individualcases, in the majority a higher grade of mottlingwas recorded in the lower zones than in the midzones. In only a few cases were grade 1 (slight)changes recorded in the upper zones and thesealways had moderate or marked changes in themid and lower zones. There appeared to be littledifference between the two sides. For instance,observer B, who was one of the most consistentobservers, recorded in the 29 films which he con-
sidered to show mottling that it was equal inseverity on the two sides in 18. In the other 10it was more marked on the right side in six andon the left side in five. It seemed justified, there-fore, in attempting to consider the film as a wholeto derive a total score for each film by addingtogether the grade recorded in each zone and then
placing the film in one of the following categoriesaccording to the total score obtained:
l~~~~~Total Score Category
0 Absent1 -4 Slight5-8 ModerateOver 9 Marked
The frequency with which mottling was foundin the 38 films of the patients who had beenexposed to asbestos and number in each categoryare shown in Fig. 6. It is apparent that observerE not only diagnosed mottling in a greater numberof cases but also placed more in the categorymarked. This figure does not, however, show
40 M k st
ru Marked moderate
30[
K-202
/0
A B C D E F G H / J KOB$RVERS
FjIG. 6.-Frequency of diagnosis of mottling and the number in eaclicategory in 38 patients who had been exposed to asbestos dust.
the level of agreement between the observers onthe individual cases. In the 36 films in whichone or more of the observers recorded mottlingas present there was complete agreement on thecategory observed in nine cases only. In theremaining 27 films the level of disagreementbetween the observers can be seen from Table II,where the films have been arranged according to
TABLE IIRANGE OF EXTREME OPINIONS OF OBSERVERS A-E IN27 FILMS WITH DISAGREEMENT ON GRADE OF MOTTLING
Range of Range of Range ofOne Category Two Categories Three Categories
Extreme No. of Extreme No. of Extreme No. ofOpinions Films Opinions Films Opinions Films
Absent-slight 6 Absent- Absent tomoderate 2 marked .. 2
Slight- Slight-moderate 6 marked 4
Moderate- _marked.. 7
Totals .. 19 6 2
106
on 24 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.103 on 1 June 1960. Dow
nloaded from

RADIOLOGICAL DIAGNOSIS OF ASBESTOSIS
the extremes of the range of mottling recorded.It can be seen that in two films there was suchmarked disagreement that the same film wouldbe placed in any of the four categories accordingto the observer viewing the film. In six more therewas a range of opinion of two categories.Second Occasion (Observers F to K).-The films
were considered as a whole and the severity ofmottling assessed according to the individualobserver's own criteria of slight, moderate, ormarked change. It was decided not to use stan-dard films on this occasion since they are not atpresent used routinely by the pneumoconiosismedical boards. The frequency with whichmottling was recorded and the number in eachgrade are shown in Fig. 6. The number of filmsthought to show mottling varied from 21 to 33.Although this gives some idea of the disagreementbetween the observers it does not show the wholepicture. There was in fact complete agreementon the severity of mottling in three films only. Inthe others the range of mottling observed is shownin Table III, where the films have been groupedaccording to the extremes of the range of opinion
TABLE 11IRANGE OF EXTREME OPINIONS OF OBSERVERS F-K IN35 FILMS WITH DISAGREEMENT ON GRADE OF MOTTLING
Range of Range of Range ofOne Category Two Categories Three CategoriesExtreme No. of Extreme No. of Extreme No. ofOpinions Films Opinions Films Opinions Films
Absent-slight 10 Absent- Absent tomoderate 9 marked .. 7
Slight- Slight- _moderate 5 marked .. 1
Moderate- _marked.. 3
Totals .. 18 10 7
recorded. It is to be noted that in addition tothe 28 cases in which the range of opinion wasone or two categories there were seven with arange of three categories, i.e., the opinionsrecorded in these seven films varied from nomottling to marked mottling according to theobserver.SHAGGY HEART, PLEURAL REACTION, AND
BULLAE.-There was considerable disagreementbetween the observers on the presence or absenceof these signs. Some idea of this can be obtainedby comparing the number of films in which thesign is recorded as present by one or moreobserver with the number in which it was foundto be present by the majority, i.e., six or more.This is shown in Table IV. Although a shaggyborder to the heart was recorded as present by
H
TABLE IVDISAGREEMENT BETWEEN OBSERVERS IN DIAGNOSISOF SHAGGY HEART APPEARANCES, PLEURAL REACTION,
AND BULLAE
Shaggy Pleural BullaeHeart Reaction
Recorded as present by one ormore observers 25 29 30
Recorded as present by six ormore observers 3 15 6
one or other of the observers in 25 of the 38patients who had been exposed to asbestos, in onlythree of these did the majority agree on itspresence. Similarly there was marked disagree-ment on the presence or absence of bullae butbetter agreement with pleural reaction.
DISCUSSION
There were several surprising findings in thisstudy. One was the extent of the disagreementbetween the observers in the diagnosis of the filmsfrom the certified cases of asbestosis. Thesepatients had all been seen and certified by thepneumoconiosis medical panels and had initiallybeen selected by us as classical examples of thedisease. Yet when the same films were viewed inthe present trial the number thought to showchanges consistent with the diagnosis of asbestosisvaried from 40 to 80% approximately accordingto the observer. This study might be criticized onthe grounds that if the industrial history or physicalsigns of these patients had been known many ofthe films regarded as abnormal but not asbestosiswould have been correctly diagnosed. Never-theless it was emphasized at the beginning on bothoccasions that the decision was not whether thepatient did or did not have asbestosis but whetherthe changes seen in the radiographs were consistentwith this diagnosis. It is clear also that thediscrepancy of opinion was not due to poorselection of observers, as they all had specialexperience in this field and with one exceptionhad little difficulty in diagnosing the films fromthe normal subjects.The difficulties in the diagnosis of the early
radiological changes of asbestosis have beenemphasized repeatedly by Pendergrass since 1938,so that it was not surprising to find a differenceof opinion in the diagnosis of the films from thegroup of patients who had been exposed but inwhom previously the radiographs had beenregarded as clear. However, the extent of thisdisagreement was quite remarkable and it is clearthat little reliance can be placed on the presenceof radiological changes in the diagnosis of early
107
on 24 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.103 on 1 June 1960. Dow
nloaded from

ROGER WILLIAMS and P. HUGH-JONES
cases. Sander (1955) came to the same con-clusion. He describes a formal trial held by theair hygiene committee of the asbestos textileindustry in America in which sample films ofasbestosis of varying stages, including someessentially normal, were reviewed by eightexperienced physicians. They found that therewas no agreement on the borderline cases and thatit was impossible to define a first-stage case asthe same film would be called " essentiallynormal " one day and " first stage " the next dayby the same observer.
It is impossible to draw any firm conclusionsregarding the value of standard films which wereused with thie first group of observers, as theexperiment was not repeated in the absence ofsuch films. Certainly there is considerableobserver variation even with their use, and it isdifficult to believe that they were of much valuein the diagnosis of borderline cases. It does seem,however, that with them a meaningful grading ofradiological change was obtained, for there wasa highly significant correlation (r= -0.74, P<0.001) between the grade of radiological mottlingand the degree of reduction in diffusing capacity(Williams and Hugh-Jones, 1960). Fletcher andOldham (1951) found with similar problems incoalworkers' pneumoconiosis that the use ofstandards enabled some but not all of theobservers to achieve a greater accuracy andconsistency in classification. The least experiencedobservers benefited most, though they tended tomake false diagnoses of abnormality in normalfilms when working with standards, whereas themore experienced observers found them of greaterhelp in the discrimination of normal films fromthose with slight abnormality than in theclassification of abnormal films. There is nodoubt that there was much greater disagreementwith the second group of observers in the assess-ment of radiological mottling. It is not justifiableto compare the findings on the two occasions, forthey were by different groups of observers, andit is impossible to assess the standards ofabnormality by which the films were judged onthe second occasion.
It is clear that the other radiological signs ofasbestosis, such as the shaggy heart appearanceand pleural reaction, are also subject to consider-able observer variation. It was of interest to findthat bullae, which are not usually regarded as oneof the classical features of the radiologicalchanges- in asbestosis, were present rather morefrequently than the shaggy heart appearance. It-is important to realize that differences in disagree-
ment represented not only the difficulty which theobservers found in detecting the various signs butalso reflect the degree to which these signs werepositive. For instance, the high level of disagree-ment in deciding on the presence or absence of ashaggy heart or bullae may in part be due to thefact that this group of films did not show thesesigns to a marked degree. On the other hand, itmay be equally due to the fact that the observersfound these signs particularly difficult to interpret.In the absence of any absolute opinion as to thepresence or absence of a particular change, it isimpossible to separate these two influences.
In conclusion it is apparent, from the observers'findings in the group of films from other pul-monary diseases, that the radiological appearancesin asbestosis are by no means specific, and may beconfused with such widely differing diseases aschronic bronchitis and emphysema, sarcoidosis, andother pneumoconioses. Presumably if other inter-stitial fibroses such as scleroderma, lymphangitiscarcinomatosa, xanthomatosis, or berylliumgranuloma had been included in this group theconfusion would have been even greater.
SUMMARYA trial was held to see if the radiological
changes in asbestosis were specific and to whatextent their diagnosis and grading were affected byobserver variation.Eleven experienced observers were asked to
read independently a series of 53 radiographswhich contained examples of asbestosis, otherpulmonary fibroses, and films from normalsubjects.The results showed that the radiological
appearances of asbestosis were quite unspecificexcept in some advanced cases and observervariability in grading asbestosis was great.The use of standard films both in the diagnosis
and grading of the radiological changes needsfurther trial.
We should like to thank the observers who tookpart in the trial, Dr. C. M. Fletcher for his constantinterest and advice, and Dr. J. C. McVittie, of theMinistry of Pensions and National Insurance, for hishelp in organizing the second part of the study.
REFERENCESFletcher, C. M., and Oldham, P. D. (1951). Brit. J. industr. Med., 8,
138.International LabourOrganization (1959). Occup. Safety Hlth, 9, 63.Pendergrass, E. P. (1938). In Silicosis and Asbestosis, ed. Lanza,
A. J., p. 174. Oxford University Press, London.Sander, 0. A. (1955). A.M.A. Arch. industr. Hlth, 11, 208.Williams, R., and Hugh-Jones, P. (1960). Thorax, 15, 109.
108
on 24 Decem
ber 2018 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.15.2.103 on 1 June 1960. Dow
nloaded from