the optic chiasm
TRANSCRIPT
Handbook of Clinical Neurology, Vol. 102 (3rd series)Neuro-ophthalmologyC. Kennard and R.J. Leigh, Editors# 2011 Elsevier B.V. All rights reserved
Chapter 7
The optic chiasm
DESMOND KIDD *
Department of Neuro-ophthalmology, Royal Free Hospital and Royal Free and University CollegeHospital Medical School, London, UK
INTRODUCTION
The optic chiasm is formed when the optic nerves cometogether in order to allow for the crossing of fibers fromthe nasal retina to the optic tract on the other side. Thisenables visual inputs from the nasal half of the contralat-eral eye and the temporal half of the ipsilateral eye to beprocessed by the occipital lobe, vital for visual processing.
ANATOMY
The optic chiasm lies above the sphenoid bone, over thediaphragma sellae (Fig. 7.1); anatomical variations arecommon and can influence the presenting visual symp-toms and signs in chiasmal disorders. In the majority ofcases (79% of a series of 125 autopsy cases) the chiasmis situated overlying the diaphragma sellae (Schaeffer,1924), prefixed when lying above the tuberculum sellaeor within the sulcus chiasmatis (17% of cases), and post-fixed when it lies above or even behind the dorsumsellae (4%) (Bergland et al., 1968).
The intracranial optic nerves rise from the canal tothe chiasm at an angle of 15–45�. The pia mater is con-tiguous with that of the nerves and that of the anteriortracts. The chiasm lies posterosuperiorly within the wallof the third ventricle and anteriorly with the cerebro-spinal fluid within the chiasmatic cistern (Fig. 7.1).Above lies the hypothalamus and below the pituitarygland. The infundibulum of the pituitary lies immedi-ately posteriorly and the mamillary bodies behind this,medial to the two optic tracts.
The internal carotid arteries lie to either side and theanterior communicating artery lies directly above; aneur-ysms of the anterior communicating artery or first seg-ment of anterior cerebral artery may therefore compressthe chiasm.
*Correspondence to: Desmond Kidd, MD FRCP, Consultant NRoyal Free Hospital and Royal Free and University College Ho
Tel: 00 44 2078 302868, Fax: 00 44 2074 726829, E-mail: d.kidd@
It is well known that fibers from the nasal retinacross within the chiasm; the ratio of crossed touncrossed fibers within the chiasm is 53:47 (Kupferet al., 1967). This crossing is of necessity very precise;only fibers from the temporal retina pass to the ipsilat-eral lateral geniculate nucleus, and only those from thenasal retina pass contralaterally. Those that cross doso as soon as they enter the chiasm and maintain theirrostral to caudal position within the chiasm. Thosethat are uncrossed continue in the lateral chiasm intothe ipsilateral tract. Fibers from the macula on eachside, which account for the majority of fibers withinthe chiasm (Hoyt and Luis, 1969), are found morecentrally and caudally than other fibers.
Rarely the chiasm may fail to develop (achiasmia).Patients studied have associated midline developmentaldisorders but intact fields; the visual-evoked potentialcharacteristically is monocular (Sami et al., 2005).
BLOODSUPPLY
The blood supply is variable, but in general comes fromfeeder vessels arising from branches of the anteriorcommunicating artery, anterior cerebral, posterior com-municating, posterior cerebral and basilar arteries(Wollschlaeger et al., 1971). The dorsal parts are sup-plied by branches of the internal carotid arteries andthe more ventral parts from the posterior circulation.There is considerable collateral supply, with the resultthat infarction of the chiasm is very rare indeed.
VISUAL FIELDDEFECTS INCHIASMALDISORDERS
A careful study of the bilateral visual field defectacquired in chiasmal lesions can provide important
eurologist and Head, Department of Neuro-ophthalmology,spital Medical School, Pond Street, London NW3 2QG, UK.
medsch.ucl.ac.uk

Fig. 7.1. T1-weighted (A) axial and (B) coronal magnetic
resonance images showing the position and immediate
relationship of the chiasm to adjacent anatomical structures.
A
B
C
D
E
F
GFig. 7.2. Visual field defects seen in chiasmal disorders.
(A) Ipsilateral central field defect and contralateral junctionalscotoma in a lesion involving the anterior angle of the chi-
asm; (B) also at the anterior angle, when only the crossing
macular fibers are affected; (C) bitemporal hemianopia when
the body of the chiasm is affected; (D, E) bitemporal upper
and lower quadrantinopia when the lesion compresses the
chiasm from below and above respectively; (F) bitemporal
hemianopic scotomas when a lesion involves the posterior
angle of the chiasm; (G) a noncongruous hemianopia occurs
when the tract is affected.
186 D. KIDD
information on the nature and in particular the site ofthe causative lesion. Traditionally field defects havebeen divided anatomically into the anterior angle, thebody, the posterior angle, and the lateral aspect of thechiasm (Fig. 7.2).
The anterior angle
Lesions that involve the anterior angle of the chiasm,the point at which the optic nerve passes into and formsthe chiasm, may show a junctional scotoma (Traquair,1949) since there is at this point separation of the
crossing and uncrossed fibers. If the lesion is not largethis will result in an ipsilateral monocular central fielddefect (from the optic nerve) and a small contralateralupper temporal homonymous field defect frominvolvement of the crossing fibers anteriorly. If thenerve itself is not affected as well, the defect willbe monocular and temporal, since only the crossingfibers are affected; if only the macular fibers areinvolved then the defect is a midline-obeying temporalscotoma. This defect may be very small and can be

IC CHIASM 187
missed with kinetic perimetry; it is, however, usuallypicked up using static perimetry.
Wilbrand’s knee is said to be an extension of thecrossing fibers from retinal ganglion cells locatednasal and inferior to the fovea into the ipsilateral dis-tal optic nerve; the contralateral field defect ariseswith involvement of these fibers. Horton (1977), how-ever, has stated that Wilbrand identified an artifactualstate in the examination of enucleated eyes. Nonethe-less, the importance of the identification of a smallasymptomatic contralateral defect in the presence ofa symptomatic monocular defect greatly encouragesthe examining physician to proceed with haste to imag-ing studies rather than diagnose an inflammatoryoptic neuropathy incorrectly.
THE OPT
Fig. 7.3. (A, B) Goldmann field showing bitemporal hemianopia
Fig. 7.15).
The body of the chiasm
Lesions that affect the body of the chiasm produce thetypical bitemporal hemianopia (Fig. 7.3). This may affectthe whole hemifield, upper or lower quadrants, andperipheral or central areas. The macula is usually, butnot always, split. In general, central visual acuity is unaf-fected. Clearly it is possible that the field defects are notthe same in each eye, since of course the causative lesionmay exert a greater effect on one side than the other.Complete defects tend only to occur in the case oftrauma. When the peripheral fields are affected, thedefect progresses in a clockwise direction in the rightand counterclockwise in the left (Cushing and Walker,1915). Lesions compressing from above cause the lower
caused by a lesion involving the body of the chiasm (shown in

Fig. 7.5. Illustration of the mechanism of postfixational
blindness in bitemporal hemianopia. Unshaded area , area
of binocular vision; light shading , area of monocular
vision; dark shading , area of blindness.
KIDD
field to be affected first and the defects are less congru-ous; those from below affect the upper fields first andtend to be more congruous in appearance.
The posterior angle of the chiasm
Lesions within the posterior aspect of the body ofthe chiasm produce bitemporal hemianopic scotomas(Larmande and Larmande, 1977). These may be con-fused with centrocecal scotomas (Fig. 7.4), but the for-mer will not be associated with significant reduction invisual acuity, whereas the latter will. More posteriorlyplaced lesions will also involve the optic tract, with theresult that the field defect will be predominantly oneof a homonymous hemifield defect.
The lateral aspect of the chiasm
Involvement of this area by compression leads to ahomonymous hemifield defect on the contralateralside.
VISUAL SYMPTOMS
When lesions damage chiasmal fibers there is a progres-sive loss of central visual acuity and a noticeable dim-ming of the temporal visual fields.
Patients may also notice a disturbance of depth per-ception at fixation which is due to crossing of the twoblind hemifields after the point of fixation in conver-gence (Fig. 7.5). Hence an object that is seen at adistance to be behind another will disappear when theeyes focus on the object in front.
“Hemifield slide” is a phenomenon in which patientscomplain of difficulty reading and notice a doubling,loss, or vertical deviation of words on a horizontal line
188 D.
Fig. 7.4. Goldmann field showing a field defect associated with a
Fig. 7.10).
(see Chapter 9). Normally there is an overlap betweenthe temporal field on one side and the nasal field onthe other to allow fusion, which helps to stabilize ocularalignment, with the result that the image is single andclear. Patients with minor phoric deviations of the eyes
lesion involving the posterior angle of the chiasm (shown in

IC CHIASM 189
will lose this overlap and therefore develop tropia, withthe result that minor horizontal or vertical misalignmentoccurs, leading to distortion or even doubling.
Those whose lesions involve not only the chiasm butalso the cavernous sinus or orbital apex may have ocu-lar motor pareses leading to diplopia and trigeminalsensory loss or pain.
Some patients with chiasmal syndromes may rarelycomplain of photophobia; the mechanism by which thiscomes about is not clear.
THE OPT
NEURO-OPHTHALMIC SIGNS
When a chiasmal lesion leads to optic nerve fiber atro-phy, “band” or “bow-tie” atrophy is observed, in whichatrophy is more evident in the nasal and temporal sidesof the disc and relatively spared in the superior andinferior sectors (Unsold and Hoyt, 1980) (Fig. 7.6). Thisis due to involvement of only those fibers arising nasalto the fovea (associated therefore with the bitemporalhemianopia) being affected and passing into the nervefrom these sections of the disc.
Tumors of the diencephalon and sellar region maybe associated with seesaw nystagmus, a rhythmicsynchronous alternating rotation of the eyes, in whichone eye elevates and intorts whilst the other simulta-neously depresses and extorts. In the case of parasellarlesions the brainstem fibers associated with the intersti-tial nucleus of Cajal are involved, and so the lesionmust also affect these fibers in order to cause thesyndrome.
Fig. 7.6. (A, B) Photographs of the optic fundus showing bow-tie
adenoma of the pituitary gland (shown in Fig. 7.13B).
DISEASESTHATMAYAFFECTTHECHIASM
Inflammatory diseases
GRANULOMATOUS INFILTRATION
Sarcoidosis
Sarcoidosis is an autoinflammatory disorder of uncertainetiology in which granulomatous inflammation developsleading to tissue destruction and fibrosis. It is thought thatsome 10% of cases arise within or also involve the centralnervous system. The neurological disorder is a meningeal-based inflammatory infiltration (Kidd and Beynon, 2003).The anterior visual pathway may be involved at any loca-tion; granulomas may arise within the disc, the optic nerveitself is involved most commonly, in which an intrinsiclesion may develop leading to the clinical syndrome ofan optic neuritis (Frohman et al., 2003; Koszman et al.,2008; Figs 7.7 and 7.8), or an optic perineuritis may arise.Compression by an inflammatory mass at the orbital apexand, much less commonly, at the cavernous sinus (Zareiet al., 2002) may occur and be associated with ophthalmo-paresis and trigeminal neuropathy. The tracts may also beaffected (Frohman et al., 2003).
Involvement of the chiasm comes about by thedevelopment of an inflammatory mass within thepituitary gland (Guoth et al., 1998). This arose in 1 in14 patients in one series (Chen and McLeod, 1989) and4 in 100 in my own personal series. Patients present withsymptoms of hypopituitarism and with visual fielddefects in keeping with a chiasmal problem. Pain is
atrophy of both discs in a patient with a large chromophobe

Fig. 7.7. (A, B) T1-weighted sagittal magnetic resonance images showing enlargement and enhancement of the pituitary gland
and stalk in sarcoidosis.
Fig. 7.8. T1-weighted coronal (A) and axial (B) magnetic resonance images showing enhancement of the hypothalamus and
pituitary stalk in sarcoidosis.
190 D. KIDD
uncommon and the syndrome appears to be indistin-guishable from pituitary adenoma both on clinical andon radiological grounds (see Fig. 7.7). There are isolatedreports of pituitary sarcoid arising within an adenoma(Rubin et al., 2001) and associated with a Rathke’s cleftcyst (Cannavo et al., 1997); whether or not these arerelated or coincidental is unclear.
It should be stressed that the majority of pati-ents with sarcoid who present with hypopituitarismhave involvement of the hypothalamus or the pitui-tary stalk rather than the anterior pituitary itself (seeFig. 7.8).
ANCA-positive vasculitis
ANCA-positive vasculitis is a granulomatous inflam-matory disorder with features of arteriolar and venularperivasculitis which affects the lungs, skin, eyes, andkidneys. Neurological involvement arises as a hyper-trophic pachymeningitis, as an isolated inflammatorymass, or as a central or peripheral manifestation ofinflammatory perivasculitis (Seror et al., 2006).
In one series 3 out of 6 cases had pituitary involve-ment, the majority of cases presenting with diabetesinsipidus and not with a mass lesion. A recent review

IC
of the literature cited 22 cases published (Yong et al.,2008), of which 80% showed pituitary enlargement,although this was sufficient to cause visual impairmentin only 1 case. The pituitary stalk was thickened and thehigh magnetic resonance signal usually seen onT1-weighted images was absent in all those with diabe-tes insipidus. Another case was fulminating and treat-ment was not associated with visual improvement(McIntyre and Perros, 2007).
LYMPHOCYTIC INFILTRATION
Idiopathic optic chiasmitis
This uncommon condition may be diagnosed whenother infective and inflammatory causes discussedabove have been ruled out. A recent series from Indiana(Kawasaki and Purvin, 2009) showed 20 patients, 60%of whom were female; 40% presented with monocularvisual loss but with evidence of chiasmal field defects,the remainder showing bitemporal hemianopia. Painwas not noted in this series.
Magnetic resonance imaging (MRI) revealedchiasmal swelling with or without enhancement in 12of 15 cases (Fig. 7.9), and white-matter lesions wereseen elsewhere in 6 of 15 cases. In follow-up, 6 of 15had developed multiple sclerosis, including 3 in whomimaging of the brain initially was considered to benormal. Visual outcome following treatment was a nor-mal acuity in 3 of 17, the remainder having improved toa degree with residual visual impairment, which wasmodest in the majority of cases.
THE OPT
Fig. 7.9. T1-weighted (A) sagittal magnetic resonance image
idiopathic chiasmitis; (B) coronal MRI showing considerable enh
and Valerie Purvin.)
It seems to this author that idiopathic chiasmitis isnot really a separate disease entity, merely the descrip-tion of a clinical syndrome that appears idiopathic atoutset but that may evolve into a more widespreadinflammatory neurological disorder over time.
An optic chiasmitis has also occasionally been seenin other systemic inflammatory diseases, for examplesystemic lupus erythematosus (Frohman et al., 2001).
Multiple sclerosis
The chiasm may be involved in multiple sclerosis; earlyreports (Traquair, 1925; Sacks and Melen, 1975; Spectoret al., 1980; Beck et al., 1983; Newman et al., 1991) high-lighted the clinical syndrome of a subacute unilateral orbilateral visual loss typical of an optic neuritis in whichchiasmal-type field defects were seen. MRI showsswelling of the chiasm and often enhancement.
I have seen a patient who presented with a bilateralUhthoff phenomenon with normal vision in between;the field defects were seen to enlarge with exercise.The patient went on to develop a slowly progressiveform of multiple sclerosis with visual loss, ataxia, andspasticity.
Lymphocytic hypophysitis
This uncommon condition is more common in women (bya factor of 5:1) and often occurs in the late stages of preg-nancy or the early postpartumperiod (Tubridy et al., 2001;Kidd et al., 2003; de Bellis et al., 2008). Patients presentwith headache, then signs of an expanding sellar lesion
CHIASM 191
(MRI) showing enlargement of the body of the chiasm in
ancement of the same lesion. (Courtesy of Drs Aki Kawasaki

Fig. 7.10. T1-weighted coronal magnetic resonance image
(unenhanced) showing a large pituitary mass due to lympho-
cytic hypophysitis.
192 D. KIDD
with visual impairment and endocrine hypofunction(Fig. 7.10). Occasionally hyperprolactinemia is seen. Theadenohypophysis is affected more often than theneurohypophysis, although isolated diabetes insipidusmay be seen. Many have other organ-specific autoim-mune diseases. Hypopituitarism arises as a consequenceof immune-mediated attack on the pituitary cells, ratherthan simply a compressive effect. MRI shows a symmet-rical intensely enhancing tissue mass within the pituitaryand there may be a dural tail (Sato et al., 1998). Thepathology of the lesion is one of intense infiltration bylymphocytes and plasma cells, often with lymphoid folli-cles, associated with evidence for necrosis of adjacentpituitary tissue. Antipituitary antibodies may be detected(Bensing et al., 2007), although the assays appear notyet to have clinical utility (de Bellis et al., 2008).
Treatment is often unnecessary if a hypophysec-tomy has been undertaken, and follow-up suggests alow risk of recurrence (presumably because allpituitary tissue has been removed). Those who arediagnosed clinically by supposition, or following pitui-tary biopsy, appear to respond well to treatment withcorticosteroids. The role of immunosuppression is notknown; there are case reports of a response to radio-therapy in patients who fail to improve with steroids(Selch et al., 2003).
HISTIOCYTIC INFILTRATION
Xanthomatous hypophysitis
This is a pathological description for another inflam-matory disorder of the pituitary in which cystic enlarge-ment of the gland is seen, containing yellow fluid.The pathological features are of a lymphocytic andhistiocytic infiltration of the gland. It is likely to be anincomplete form of the condition known as Erdheim–Chester disease, in which a histiocytic infiltration ofthe bones, lungs, and numerous other tissues may arise(Egan et al., 1999). Neurological complications occurmost commonly due to involvement of the sellar regionand orbit, but other areas may also be involved (Allenet al., 2004). This condition responds poorly to steroidsand immune suppression, and the fatality rate whenthe lungs and kidneys are involved is said to be around50% (Mills et al. 2008). Interferon-alpha may be helpful(Haroche et al., 2006).
Rosai–Dorfman disease is a rare histiocytic disorderof children and adults which presents with massivelymphadenopathy and infiltration of the nasopharynx,respiratory pathways, endocrine glands, bones, and skin.It may also involve the central nervous system (Kiddet al., 2006) in 4% of cases, in which a meningeal-basedinflammatory mass or multiple masses may arise whichsimulate meningiomas on imaging. Orbital and cavern-ous sinus masses may arise, and 3 cases of pituitaryinvolvement by mass lesions of the parasellar region havebeen published (Kelly et al., 1999; Woodcock et al., 1999;Kidd et al., 2006) (Fig. 7.11).
Mucoceles of the paranasal air sinuses
One report deals with a chiasmal visual field defect in apatient with a mucocele of the sphenoid sinus (Goodwinand Glaser, 1987).
Infections
TUBERCULOSIS (TB)
It is well known that TB may infiltrate the sellar region.Pituitary hypofunction and visual field defects mayarise as a result of the development of tuberculomawithin the pituitary, giving rise to a mass lesionwith chiasmal compression (Domingues et al., 2002)(Fig. 7.12) or to optochiasmal arachnoiditis, in which abasal tuberculous meningitis encroaches upon thatregion and induces visual loss, frequently in associationwith diabetes insipidus (Akhadder et al., 2001).
Patients may present with or without evidencefor TB elsewhere and may present subacutely or as anemergency (Sharma et al., 2003). Tuberculoma mass

Fig. 7.11. T1-weighted axial magnetic resonance image
showing a large suprasellar mass due to Rosai–Dorfman
disease.
Fig. 7.12. T1-weighted sagittal magnetic resonance image
showing enlargement and enhancement of the pituitary gland
and stalk in tuberculosis.
THE OPTIC
lesions are indistinguishable from other pituitarymass lesions (Akhadder et al., 2001), although it hasbeen suggested that thickening of the pituitary stalk ismore common in TB.
In optochiasmatic arachnoiditis imaging does notshow a mass lesion but perichiasmal enhancement(Silverman et al., 1995). The visual prognosis is oftengood (Hughes et al., 2008), although not always(Sharma et al., 2003).
Optochiasmatic arachnoiditis may occur in otherinfective meningeal processes such as syphilis, Pseudo-monas, staphylococcus, and streptococcus infections.
PITUITARY ABSCESS
One series noted that patients with pituitary abscessespresent with headache and visual loss mimicking a pitu-itary mass rather than signs of fever or meningitis;most cases were only diagnosed at surgery when apus-filled mass was opened (Vates et al., 2001). Treat-ment with antibiotics after surgery was helpful but themortality rate was 8% (Vates et al., 2001). Of 25 casesreported within the previous 5 years around half grewno organisms, whilst the majority of the remainderwere pyogenic organisms, fungi, or parasites (Dalanand Leow, 2008).
CRYPTOCOCCUS
Optic neuropathy is common in cryptococcal meningi-tis; a pathological study showed that the nerves and chi-asm were damaged as a result of direct infiltration bythe organism from the adjacent meninges (Cohenand Glasgow, 1993). There was no evidence for anassociated vasculitis.
The prognosis for visual recovery even with prompttreatment is very poor.
CYSTICERCOSIS
One series of 23 patients from the USA showed 4 caseswith chiasmal involvement; in 2 cases there was com-pression from the third ventricle on to the chiasm (seebelow) and in the other 2 cases there were intrasellarcysts causing compression from below (Chang andKeane, 2001).
VIRUSES
Isolated chiasmitis related to viral infections seemsrare, but has been reported with varicella-zoster virusand Epstein–Barr virus (Purvin et al., 1988; Grevenet al., 2001). It occurs more commonly alongside asevere syndrome in which the uveal tract, retina, andoptic nerve and chiasm may all simultaneously beaffected (Brazis and Miller, 2005).
CHIASM 193

194 D. KID
Tumors and cysts
PITUITARY ADENOMA
These constitute 10% of all intracranial tumors; theprevalence increases with age. Adenomas arise fromtissues within the anterior pituitary; functioning orsecreting adenomas secrete prolactin, somatotrophin,adrenocorticotropic hormone, and thyroid-stimulatinghormone. Most are microadenomas (measuring lessthan 10 mm in diameter), of which the majority willpresent with the effects of hormone hypersecretionand other incidental findings. Nonsecreting adenomas
Fig. 7.13. Pituitary adenoma: (A) T1-weighted coronal magnetic
noma with cystic change causing chiasmal compression. (B) T1-adenoma. (C) Thyroid-stimulating hormone-producing adenoma
with headache, visual loss, and a complete right-sided ophthalmo
are more likely to be large; they account for only 10%of cases and present with visual loss and headache(Wilson, 1992) (Fig. 7.13). Some 10–20% of pituitaryadenomas are identified incidentally on MRI brainscans (Aron and Howlett, 2000).
Prolactinomas account for 40% of pituitary tumorsand present with galactorrhea and amenorrhea; themajority (90%) are microadenomas (Schlechte, 2003),but macroadenomas can enlarge appreciably in preg-nancy (Kupersmith et al., 1994). The majority are treatedsuccessfully with dopamine agonists, and surgery evenfor large tumors is not required (Schlechte, 2003).
D
resonance image (MRI) showing a large chromophobe ade-
weighted sagittal MRI showing a large, predominantly cystic
. (D) Pituitary apoplexy: chromophobe adenoma presenting
plegia.

IC
It should be remembered that nonfunctioningmacroadenomas may induce a rise in prolactin levelsby the mechanism of compression on the pituitary stalk,leading to a loss of dopaminergic inhibition, and so toan increase in the prolactin level.
Corticotrope- and somatotrope-secreting tumorsproduce Cushing’s disease and acromegaly/giantismrespectively. The former are more likely to present withendocrine abnormalities but growth hormone-producingtumors may enlarge unnoticed until visual symptomsarise (Rivoal et al., 2000). The majority of cases aredue to pituitary tumors, but adrenocorticotropic hor-mone and growth hormone may be produced ectopicallyby lung carcinomas or by carcinoid tumors respectively.Cushing’s disease requires surgery and, since there is ahigh rate of tumor recurrence, postoperative radiother-apy. Treatment of growth hormone-producing tumorsis with somatostatin analogs.
Thyroid-secreting hormone-secreting tumors accountfor only 3% of cases and present either with thyrotoxicosisor with visual loss (25%) (Brucker-Davis et al., 1999). Theyare usually macroadenomas (see Fig. 7.13), and so treat-ment is surgical, although some respond to somatostatinanalogs since their receptors are present.
A headache disorder is a prominent feature of some34% of cases (Abe et al., 1998), and is more common inpatients with hyperprolactinemia and acromegaly (Levyet al., 2002). In one recent series 76% had featuresof migraine headache, 27% primary stabbing head-ache, and 9% had features of cluster headache orshort-lasting, unilateral, neuralgiform headache attackswith conjunctival injection and tearing (SUNCT) (Levyet al., 2005). The latter were more common in acromeg-aly and when the tumor involved the cavernous sinus.The pathogenesis of the headache disorder remainspoorly understood; early assumptions that it reflecteddural stretching or cavernous sinus involvement havebeen refuted (Levy et al., 2002). It was noted that49% had a family history of migraine, implying thatthey were already predisposed to a primary headachedisorder (Levy et al., 2005). Only half of the patientsnoted an improvement in headache with treatment,and use of cabergoline worsened the headache in 20%of those with prolactinoma (Levy et al., 2005).
Treatment
The risk of recurrence following transsphenoidal sur-gery in nonsecreting tumors is less than 10%, and higherfollowing transcranial surgery (Couldwell, 2004).
With the exception of corticotrope adenomas, radio-therapy is usually withheld until there is evidence oftumor recurrence; hypopituitarism inevitably occurs,but late radiation-associated optic neuropathy is un-common. The risk of oncogenesis leading to glioma,
THE OPT
meningioma, or sarcoma is considered to be exceedinglyrare (Jones, 1991).
Visual prognosis following surgery
This clearly depends on the size of the lesion, the dura-tion of compression, patient age, and visual acuity atthe time of surgery. In general an appreciable improve-ment occurs postoperatively, often within 24 hours(Powell, 1995). A slower improvement after 4 monthsextending to 3 years is less likely to proffer significantreduction in visual impairments. In prolactinoma visualimprovement also starts quickly following initiation ofdopamine agonist therapy; following radiotherapyrecovery is more gradual.
CRANIOPHARYNGIOMA
These are benign lesions that nonetheless can causeprominent and irreversible pituitary and hypothalamicdysfunction. They arise from squamous epithelium atthe junction of the infundibular stem and the anteriorpituitary, and are thought to be remnants of Rathke’spouch. There is a bimodal incidence, in childhoodand again in middle to late life, with clinical featuresof a sellar or hypothalamic lesion. They may be situatedabove or below the chiasm, and rarely within it(Brodsky et al., 1988). The lesions are cystic (Fig. 7.14)and often contain viscid, oily (“engine oil”) fluid.Cholesterol clefts, calcium, and keratin may also bepresent.
In children these lesions present with hypothalamicdysfunction and hydrocephalus, in adults with featuresof chiasmal dysfunction, optic nerve or tract signs, andophthalmoparesis.
The MR features vary with the composition of thelesion (Eldevik et al., 1996).
Surgery aims to provide debulking rather thanremoval, since surgery is often complicated by thedevelopment of hypothalamic dysfunction. Postopera-tive radiotherapy increases 10-year survival and maylead to prolonged remission, although recurrence iscommon (Manaka et al., 1985). Use of more modernradiotherapy techniques appears to improve survivalfurther (Kobayashi et al., 2005).
The visual prognosis following treatment depends,as before, on the presenting acuity and the nature ofthe lesion, and the presence of disc atrophy or papille-dema (McFadzean, 1989).
RATHKE’S CLEFT CYST
These benign cysts form in embryogenesis if the lumenof Rathke’s pouch does not close, giving rise to a cystsituated between the anterior and intermediate lobesof the pituitary. Most are asymptomatic and do not
CHIASM 195

Fig. 7.14. Craniopharyngioma: (A) T1-weighted sagittal scan showing a cystic suprasellar lesion arising above and behind the
chiasm. (B) T2-weighted coronal magnetic resonance image showing the same lesion compressing the chiasm forwards.
196 D. KIDD
enlarge. Patients with symptoms are predominantlyfemale and present in middle life with visual loss dueto chiasmal compression, headache, and hypopituita-rism (Voelker et al., 1991). They are difficult to diag-nose with certainty on MRI as there are usuallyfeatures of craniopharyngioma or pituitary adenomaand the diagnosis is usually made at surgery. Treat-ment is with endoscopic transsphenoidal drainageand marsupialization. Visual improvement occurspostoperatively in 70% of cases (El Mahdy andPowell, 1998); those with poor preoperative acuitiesdo less well.
EPIDERMOID CYSTS
When these cysts arise from the suprasellar region theypresent in the same way as a pituitary adenoma orcraniopharyngioma, with visual loss and hypothalamicdysfunction (Mtanda et al., 1986). It is rarely possibleto remove them in their entirety owing to their propen-sity to be adherent to the surrounding tissues, andrecurrence therefore is common, although the rate ofgrowth of these lesions is exceedingly slow. They arelined by stratified squamous epithelium; enlargementoccurs due to progressive exfoliation from the epithe-lium of keratinous material, which is laid down in alamellar pattern.
DERMOID CYSTS
These are also rare and similar to epidermoids except thatthe cyst is lined by pilosebaceous structures leading to theformation of hair. Whilst epidermoids are often laterallyplaced, dermoids tend to arise in midline structures.
Rupture of these cysts is associated with a chemicalmeningitis and seizures; those in the suprasellar regionmay therefore present with an apoplectic disordersimilar to pituitary adenomas.
RARE CHORISTOMAS IN THE SELLAR REGION
Occasionally cystic lesions also arise in the optic nerve,chiasm, or tract. The lesions are found to be composedof muscle and adipose tissue (Zimmerman et al., 1983).
SUPRASELLAR ARACHNOID CYSTS
These arise relatively frequently and present with signsof compression of the underlying structures, and occa-sionally upward compression leading to hypothalamicdysfunction and hydrocephalus. It is difficult withimaging to differentiate these from other cystic lesionssuch as Rathke’s cleft cyst (Rao et al., 2008), and thediagnosis is often only made at surgery; treatment iswith incision and fenestration of the cyst with a low riskof recurrence.
THE OPTIC
CHORDOMA
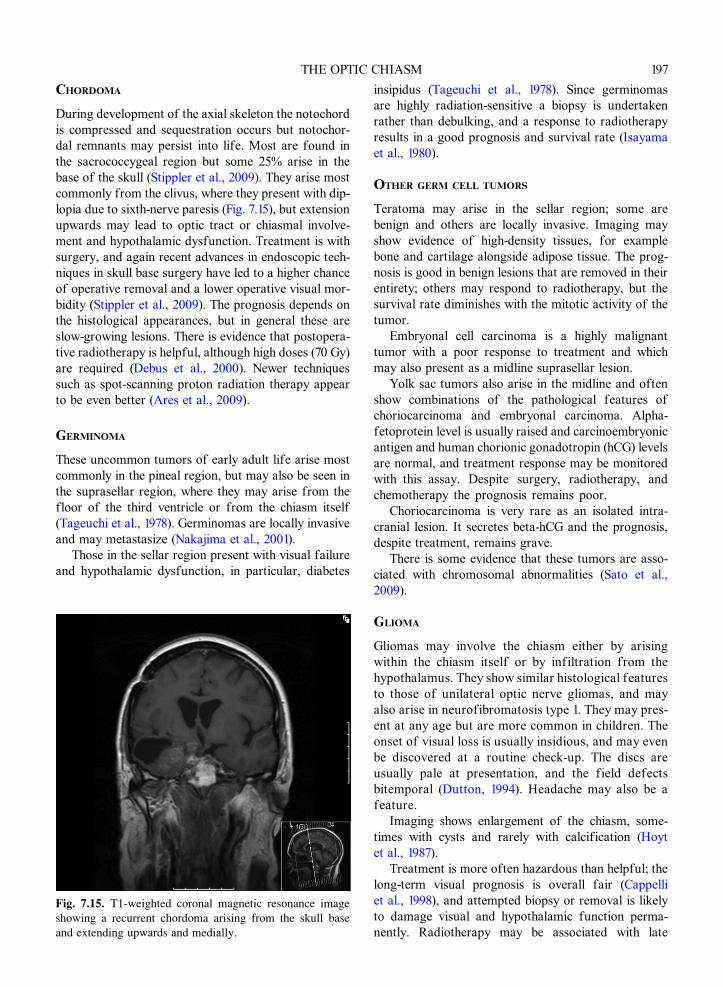
During development of the axial skeleton the notochordis compressed and sequestration occurs but notochor-dal remnants may persist into life. Most are found inthe sacrococcygeal region but some 25% arise in thebase of the skull (Stippler et al., 2009). They arise mostcommonly from the clivus, where they present with dip-lopia due to sixth-nerve paresis (Fig. 7.15), but extensionupwards may lead to optic tract or chiasmal involve-ment and hypothalamic dysfunction. Treatment is withsurgery, and again recent advances in endoscopic tech-niques in skull base surgery have led to a higher chanceof operative removal and a lower operative visual mor-bidity (Stippler et al., 2009). The prognosis depends onthe histological appearances, but in general these areslow-growing lesions. There is evidence that postopera-tive radiotherapy is helpful, although high doses (70 Gy)are required (Debus et al., 2000). Newer techniquessuch as spot-scanning proton radiation therapy appearto be even better (Ares et al., 2009).
GERMINOMA
These uncommon tumors of early adult life arise mostcommonly in the pineal region, but may also be seen inthe suprasellar region, where they may arise from thefloor of the third ventricle or from the chiasm itself(Tageuchi et al., 1978). Germinomas are locally invasiveand may metastasize (Nakajima et al., 2001).
Those in the sellar region present with visual failureand hypothalamic dysfunction, in particular, diabetes
Fig. 7.15. T1-weighted coronal magnetic resonance image
showing a recurrent chordoma arising from the skull base
and extending upwards and medially.
insipidus (Tageuchi et al., 1978). Since germinomasare highly radiation-sensitive a biopsy is undertakenrather than debulking, and a response to radiotherapyresults in a good prognosis and survival rate (Isayamaet al., 1980).
OTHER GERM CELL TUMORS
Teratoma may arise in the sellar region; some arebenign and others are locally invasive. Imaging mayshow evidence of high-density tissues, for examplebone and cartilage alongside adipose tissue. The prog-nosis is good in benign lesions that are removed in theirentirety; others may respond to radiotherapy, but thesurvival rate diminishes with the mitotic activity of thetumor.
Embryonal cell carcinoma is a highly malignanttumor with a poor response to treatment and whichmay also present as a midline suprasellar lesion.
Yolk sac tumors also arise in the midline and oftenshow combinations of the pathological features ofchoriocarcinoma and embryonal carcinoma. Alpha-fetoprotein level is usually raised and carcinoembryonicantigen and human chorionic gonadotropin (hCG) levelsare normal, and treatment response may be monitoredwith this assay. Despite surgery, radiotherapy, andchemotherapy the prognosis remains poor.
Choriocarcinoma is very rare as an isolated intra-cranial lesion. It secretes beta-hCG and the prognosis,despite treatment, remains grave.
There is some evidence that these tumors are asso-ciated with chromosomal abnormalities (Sato et al.,2009).
GLIOMA
Gliomas may involve the chiasm either by arisingwithin the chiasm itself or by infiltration from thehypothalamus. They show similar histological featuresto those of unilateral optic nerve gliomas, and mayalso arise in neurofibromatosis type 1. They may pres-ent at any age but are more common in children. Theonset of visual loss is usually insidious, and may evenbe discovered at a routine check-up. The discs areusually pale at presentation, and the field defectsbitemporal (Dutton, 1994). Headache may also be afeature.
Imaging shows enlargement of the chiasm, some-times with cysts and rarely with calcification (Hoytet al., 1987).
Treatment is more often hazardous than helpful; thelong-term visual prognosis is overall fair (Cappelliet al., 1998), and attempted biopsy or removal is likelyto damage visual and hypothalamic function perma-nently. Radiotherapy may be associated with late
CHIASM 197

KID
adverse effects such as necrosis, new tumors, andthe development of moyamoya disease (Lee, 2007).However, some are exophytic and therefore surgicallyaccessible.
Chemotherapy with vincristine, temozolamide, andplatinum agents has been shown to be helpful inchildren (Laithier et al., 2003).
Malignant optic nerve gliomas may also affect thechiasm (Fig. 7.16). These present with a much morerapidly evolving clinical syndrome and respond poorlyto treatment (Rudd et al., 1985). Metastasis to otherparts of the nervous system may occur (Murphyet al., 2003). The pathology of the lesion is verydifferent to that of the benign chiasmal glioma, andis more similar to glioblastoma multiforme (Hamiltonet al., 1973).
MENINGIOMA
These tumors are twice as common in women as in menand arise more frequently in the second half of life. Theytend to be benign and slow-growing but some may infil-trate the underlying tissues. The chiasm may be affectedby those that arise from the sphenoid wing, the clivus,and the olfactory groove (Cockerham et al., 2005), andprimary optic nerve sheath meningiomas may growbackwards to involve the chiasm (Dutton, 1992; Miller,2008). Tuberculum sellae or parasellar meningiomasare uncommon (Fig. 7.17), accounting for some 3% ofintracranial meningiomas. They may arise at any pointin relation to the chiasm, but are most common in theretrochiasmatic region. They present with progressivepainless loss of vision leading to the same visual field
198 D.
Fig. 7.16. Malignant glioma of the chiasm: (A) coronal T1-w
chiasm; (B) axial scan of the same lesion.
defects noted above, although rarely, when the chiasmis postfixed, the tumor may compress the optic nervesmedially, leading to compression by the internal carotidarteries laterally. When the chiasm is prefixed a tractopa-thy is more likely.
Treatment is with surgery, and not all can beremoved in their entirety; as such it may be advisablesimply to watch the tumor growth for a time, butworsening vision can result. Nonetheless, surgery car-ries with it significant morbidity, although this is dimin-ishing with new endoscopic endonasal techniques(Gardner et al., 2008). An improvement in visual acuityof modest proportions occurs in around two-thirds(de Divitiis et al., 2008).
In a series from Johns Hopkins (Chicani and Miller,2003) half of the patients followed had stable visionpostoperatively whilst the others deteriorated. Thiswas associated with radiographic evidence of tumorrecurrence in 39% after a mean of 10.7 years.
METASTATIC TUMORS
Metastasis to the sellar region has been reported with mostcarcinomas and also lymphoma and leukaemia.
Vascular disorders
CAVERNOMA
A recent series has found 40 cases published, in whichthe majority present acutely with visual loss due tobleeding. A total of 87% of those who under-went surgery showed an improvement in visual acuitypostoperatively (Crocker et al., 2008).
D
eighted scan showing enlargement and enhancement of the

Fig. 7.17. Meningioma: T1-weighted coronal magnetic resonance images (MRIs) showing (A) a tuberculum sellae meningi-
oma; (B) a medial sphenoid ridge meningioma extending on to the lateral body of the chiasm; and (C) T1-weighted axial
MRI showing cavernous sinus meningioma extending medially to involve the chiasm and with en plaque extension towards
the tentorium and anteriorly over the temporal surface. GAD: the scan was undertaken after injection of gadolinium, a paramag-
netic contrast agent.
THE OPTIC CHIASM 199
ARTERIOVENOUS MALFORMATIONS
Arteriovenous malformations may rarely arise withinthe chiasm and provoke a variety of syndromes, includ-ing transient bilateral visual obscurations, and fielddefects due to bleeding (Sibony et al., 1982).
ISCHEMIA
The extensive blood supply to the chiasm has beennoted above and for this reason ischemic infarction of
the chiasm is exceedingly rare. Ahmadi and colleagues(1984) reported a patient with very severe occlusiveinternal carotid artery disease in whom the chiasmalsyndrome was considered to be due to ischaemia.
Compression from hydrocephalus
A host of visual field defects has been seen inhydrocephalus, due to compression of the optic nerve,chiasm, and tract (Osher et al., 1978; Humphrey et al.,

Fig. 7.18. (A, B) Chiasmal compression from downward displacement of the third ventricle in hydrocephalus due to obstruction
by a lesion of the tegmentum.
200 D. KIDD
1982; Bogdanovic and Plant, 2000). When the thirdventricle presses downwards directly and symmetri-cally on to the chiasm a bitemporal hemianopia orupper quadrantinopia would be expected (Fig. 7.18).
Traumatic chiasmal syndrome
This usually develops in victims of motor accidents andis associated with skull and facial fractures. The fielddefect is a complete bitemporal hemianopia. In oneseries the prevalence of associated diabetes insipiduswas 37% (Hassan et al., 2002).
REFERENCES
Abe T, Matsumoto K, Kuwazawa J et al. (1998). Headache
associated with pituitary adenomas. Headache 38: 782–786.
Ahmadi J, Keane JR, McCormack GS et al. (1984). Ischemic
chiasmal syndrome and hypopituitarism associated with
progressive cerbrovascular occlusive disease. AJNR Am
J Neuroradiol 5: 367–372.
Akhadder A, El Hassani MY, Chakir N et al. (2001). Opto-
chiasmatic tuberculoma: complication of tuberculous
meningitis. Report of a case and review of the literature.
J Neuroradiol 28: 137–142.Allen TC, Chevez-Barrios P, Shetlar DJ et al. (2004). Pulmo-
nary and ophthalmic involvement with Erdheim–Chester
disease: a case report and review of the literature. Arch
Pathol Lab Med 128: 1428–1431.Ares C, Hug EB, Lomax AJ et al. (2009). Effectiveness and
safety of spot scanning proton radiation therapy for chor-
domas and chondrosarcomas of the skull base: first long-
term report. Int J Radiat Oncol Biol Phys 75: 1111–1118.Aron DC, Howlett TA (2000). Pituitary incidentalomas.
Endocrinol Metab Clin North Am 29: 205–221.
Beck RW, Schatz NJ, Savino PJ (1983). Involvement of the
optic chiasm, optic tract and geniculo-calcarine visual
system in multiple sclerosis. Bull Soc Belge Ophtalmol
208: 159–191.Bensing S, Hulting AL, Hoog A et al. (2007). Lymphocytic
hypophysitis: report of two biopsy-proven cases and
one suspected case with pituitary auto-antibodies.
J Endocrinol Invest 30: 153–162.
Bergland RM, Ray BS, Torack RM (1968). Anatomical varia-
tions in the pituitary gland and adjacent structures in 225
human autopsy cases. J Neurosurg 28: 93–99.
BogdanovicMD, Plant GT (2000). Chiasmal compression due
to obstructive hydrocephalus. J Neuroophthalmol 20:266–267.
Brazis PW, Miller NR (2005). Viruses (except retroviruses)
and viral diseases. In: NR Miller, NJ Newman (Eds.),
Walsh and Hoyt’s Clinical Neuro-ophthalmology. 6th
edn. Lippincott Williams and Wilkins, Philadelphia,
pp. 3115–3284.
Brodsky MC, Hoyt WF, Barnwell SL et al. (1988). Intrachias-
matic craniopharyngioma: a rare cause of chiasmal
thickening. J Neurosurg 68: 300–302.Brucker-Davis F, Oldfield EH, Skarulis MC et al. (1999).
Thyrotropin-secreting pituitary tumors: diagnostic criteria,
thyroid hormone sensitivity and treatment outcome in 25
patients followed by the National Institutes of Health.
J Clin Endocrinol Metab 84: 476–486.Cannavo S, Romano C, Buffa R et al. (1997). Granulomatous
sarcoidosis lesion of hypothalamic–pituitary region asso-
ciated with Rathke’s cleft cyst. J Endocrinol Invest 20:77–81.
Cappelli C, Grill J, Raquin M et al. (1998). Long term
follow up of 69 patients treated for optic pathway
tumors before the chemotherapy era. Arch Dis Child 79:
334–338.

THE OPTIC CHIASM 201
Chang GY, Keane JR (2001). Visual loss in cysticercosis:
analysis of 23 patients. Neurology 57: 545–548.Chen RC, McLeod JG (1989). Neurological complications of
sarcoidosis. Clin Exp Neurol 26: 99–112.
Chicani SF, Miller NR (2003). Visual outcome in surgi-
cally treated suprasellar meningiomas. J Neuroophthalmol
23: 3–10.
Cockerham KP, Kennerdell JS, Maroon JC et al. (2005).
Tumors of the meninges and related tissues: meningiomas
and sarcomas. In: NR Miller, NJ Newman (Eds.), Walsh
and Hoyt’s Clinical Neuro-Ophthalmology. 6th edn.
Lippincott Williams and Wilkins, Philadelphia, pp.
1486–1518.
Cohen DB, Glasgow BJ (1993). Bilateral optic nerve Crypto-coccus in sudden blindness in patients with acquired
immune deficiency syndrome. Ophthalmology 100:1689–1694.
Couldwell WT (2004). Transsphenoidal and transcranial sur-
gery for pituitary adenomas. J Neurooncol 69: 237–256.Crocker M, Desouzza R, King A et al. (2008). Cavernous
hemangioma of the optic chiasm: a surgical review. Skull
Base 18: 201–212.Cushing H, Walker CB (1915). Distortions of the visual fields
in cases of brain tumor. Brain 37: 341–400.Dalan R, Leow MK (2008). Pituitary abscess: our experience
with a case and a review of the literature. Pituitary 11:299–306.
de Bellis A, Ruocco G, Battaglia M et al. (2008). Immunolog-
ical and clinical aspects of lymphocytic hypophysitis. Clin
Sci (Lond) 114: 413–421.
Debus J, Sculz-Erntner D, Schad D et al. (2000). Stereotactic
fractionated radiotherapy for chordomas and chondrosar-
comas of the skull base. Int J Radiat Oncol Biol Phys 47:
591–596.DeDivitiis E, Esposito F, Cappabianca P et al. (2008). Tubercu-
lum sellae meningiomas: high route or low route? A series
of 51 consecutive cases. Neurosurgery 62: 556–563.Domingues FS, Marcondes de Souza J, Chagas H et al.
(2002). Pituitary tuberculoma: an unusual lesion of sellar
region. Pituitary 5: 149–153.
Dutton JJ (1992). Optic nerve sheath meningiomas. Surv
Ophthalmol 37: 167–183.Dutton JJ (1994). Gliomas of the anterior visual pathway.
Surv Ophthalmol 38: 427–452.Egan AJ, Boardman LA, Tazelaar HD et al. (1999). Erdheim–
Chester disease: clinical, radiological and histopathologi-
cal findings in five patients with interstitial lung disease.
Am J Surg Pathol 23: 17–26.Eldevik OP, Blaivas M, Gabrielsen TO et al. (1996). Cranio-
pharyngioma: radiologic and histologic findings and
recurrence. AJNR Am J Neuroradiol 17: 1427–1439.El Mahdy W, Powell M (1998). Transphenoidal management
of 28 symptomatic Rathke’s cleft cysts, with special refer-
ence to visual and hormonal recovery. Neurosurgery 42:7–17.
Frohman LP, Frieman BJ, Wolansky L (2001). Reversible
blindness resulting from optic chiasmitis secondary to sys-
temic lupus erythematosus. J Neuroophthalmol 21: 18–21.
Frohman LP, Guirgis M, Turbin RE et al. (2003). Sarcoido-
sis of the anterior visual pathway: 24 new cases.
J Neuroophthalmol 23: 190–197.Gardner PA, Kassam AB, Thomas A et al. (2008). Endoscopic
endonasal resection of anterior cranial base meningiomas.
Neurosurgery 63: 36–52.Goodwin JA, Glaser JS (1987). Chiasmal syndrome in sphe-
noid sinus mucocele. Ann Neurol 4: 440–444.Greven CM, Singh T, Stanton CA et al. (2001). Optic chiasm,
optic nerve, and retinal involvement secondary to vari-
cella-zoster virus. Arch Ophthalmol 119: 608–610.Guoth MS, Kim J, de Lotbiniere AC et al. (1998). Neurosar-
coidosis presenting as hypopituitarism and a cystic
pituitary mass. Am J Med 315: 220–224.
Hamilton AM, Garner A, Tripathi RC et al. (1973). Malignant
optic nerve glioma: report of a case with electron micro-
scopic study. Br J Ophthalmol 57: 253–264.
Haroche J, Amoura Z, Trad SG et al. (2006). Variability in
the efficacy of interferon-alpha in Erdheim–Chester dis-
ease by patient and site of involvement: results in eight
patients. Arthritis Rheum 54: 3330–3336.Hassan A, Crompton JL, Sandhu A (2002). Traumatic chias-
mal syndrome: a series of 19 patients. Clin Experiment
Ophthalmol 30: 272–280.Horton JC (1997). Wilbrand’s knee of the primate optic chi-
asm is an artefact of monocular enucleation. Trans Am
Ophthalmol Soc 95: 579–609.
Hoyt WF, Luis O (1969). The primate chiasm: details of the
visual fiber organisation studied by silver impregnation
techniques. Clin Neurosurg 17: 189–208.
Hoyt WF, Fletcher WA, Imes RC (1987). Chiasmal gliomas:
appearances and long term changes demonstrated by com-
puterized tomography. Prog Exp Tumor Res 30: 113–121.
Hughes EH, Petrushkin H, Sibtain NA et al. (2008). Tubercu-
lous orbital apex syndromes. Br J Ophthalmol 92:1511–1517.
Humphrey PRD,Moseley IF, Ross Russell RW (1982). Visual
field defects in obstructive hydrocephalus. J Neurol
Neurosurg Psychiatry 45: 591–597.Isayama Y, Takahashi T, Inoue M (1980). Ocular findings of
suprasellar germinoma: long term follow up after radio-
therapy. Neuroophthalmology 1: 53–61.Jones A (1991). Radiation oncogenesis in relation to treat-
ment of pituitary tumors. Clin Endocrinol 35: 379–397.Kawasaki A, Purvin VA (2009). Idiopathic chiasmal neuritis:
clinical features and prognosis. ArchOphthalmol 127: 76–81.
Kelly WF, Bradey N, Scoones D (1999). Rosai–Dorfman
disease presenting as a pituitary tumor. Clin Endocrinol
(Oxf) 50: 133–137.Kidd D, Beynon HLC (2003). Neurological complications of
systemic sarcoidosis. Sarcoidosis Vasc Diffuse Lung Dis
20: 85–94.Kidd D, Wilson PL, Unwin B et al. (2003). Lymphocytic
hypophysitis presenting in the first trimester of pregnancy.
J Neurol 250: 1385–1387.Kidd D, Revesz T, Miller NR (2006). Neurological complica-
tions of Rosai–Dorfman syndrome. Neurology 67:1551–1555.

202 D. KIDD
Kobayashi T, Kida Y, Mori Y et al. (2005). Long-term results
of gamma knife surgery for the treatment of craniopharyn-
gioma in 98 consecutive cases. J Neurosurg 103: 482–488.Koszman JJ, Rouleau J, Gaunt M et al. (2008). Neuro-
ophthalmic sarcoidosis: the University of Iowa experi-
ence. Semin Ophthalmol 23: 157–168.Kupersmith MJ, Rosenberg C, Kleinberg D (1994). Visual
loss in pregnant women with pituitary adenomas. Ann
Intern Med 121: 473–477.Kupfer C, Chumbley L, Downer JC (1967). Quantitative his-
tology of the optic nerve, optic tract and lateral geniculate
nucleus of man. J Anat 101: 393–401.Laithier V, Grill J, Le Deley MC et al. (2003). Progression-
free survival in children with optic pathway tumors:
dependence on age and the quality of the response to che-
motherapy – results of the first French prospective study
for the French Society of Pediatric Oncology. J Clin Oncol
21: 4572–4578.Larmande A, Larmande P (1977). l’Atteinte de genou poster-
ieur du chiasma. Rev Otoneuroophtalmol 49: 1–2.
Lee AG (2007). Neuroophthalmological management of
optic pathway gliomas. Neurosurg Focus 23: E1.LevyMJ, Jager HR, Matharu MS et al. (2002). Pituitary tumors
and headache: does size matter? Cephalalgia 22: 592.Levy MJ, Matharu MS, Meeran K et al. (2005). The clinical
characteristics of headache in patients with pituitary
tumors. Brain 128: 1921–1930.
Manaka S, Teramoto A, Takakura K (1985). The efficacy of
radiotherapy for craniopharyngioma. J Neurosurg 62:648–656.
McFadzean RM (1989). The visual prognosis in craniophar-
yngioma. J Neuroophthalmol 9: 337–341.McIntyre EZ, Perros P (2007). Fatal inflammatory hypophy-
sitis. Pituitary 10: 107–111.Miller NR (2008). Primary and secondary tumors of the optic
nerve and its sheath. In: D Kidd, NJ Newman, V Biousse
(Eds.), Neuro-Ophthalmology. Butterworth-Heinemann,
Philadelphia, pp. 215–223.
Mills JA, Gonzalez RG, Jaffe R (2008). Case records of the
Massachusetts General Hospital. Case 25-2008. A
43-year-old man with fatigue and lesions in the pituitary
and cerebellum. N Engl J Med 359: 736–747.Mtanda AT, Cruysberg JRM, Merx JL et al. (1986). The ocular
presentation of intracranial epidermoid tumors: a review of
37 cases from the literature. J Neuroophthalmol 6: 223–230.Murphy M, Timms C, McKelvie P et al. (2003). Malignant
optic nerve glioma: metastasis to the spinal neuroaxis.
J Neurosurg 98: 110.Nakajima T, Kunabe T, Jokura H et al. (2001). Recurrent ger-
minoma in the optic nerve: report of two cases. Neurosur-
gery 1: 214–218.Newman NJ, Lessell S, Wintertorn JMS (1991). Optic chias-
mal neuritis. Neurology 41: 1203–1210.
Osher RH, Corbett JJ, Schatz NJ et al. (1978). Neuro-ophthalo-
mological complications of enlargement of the third ventri-
cle. Br J Ophthalmol 62: 536–542.
Powell M (1995). Recovery of vision following transsphenoi-
dal surgery for pituitary adenomas. Br J Neurosurg 9:367–373.
Purvin V, Herr GJ, De Myer W (1988). Chiasmal neuritis as a
complication of Epstein–Barr virus infection. Arch Neurol
45: 458–460.Rao VJ, James RA, Mitra D (2008). Imaging characteristics
of common suprasellar lesions with emphasis on MRI
findings. Clin Radiol 63: 939–947.Rivoal O, Brezin AP, Feldman-Billard S et al. (2000). Gold-
man perimetry in acromegaly. A survey of 307 cases from
1951 through 1996. Ophthalmology 107: 991–997.Rubin MR, Bruce JN, Khandji AG et al. (2001). Sarcoidosis
within a pituitary adenoma. Pituitary 4: 195–202.
Rudd A, Rees JE, Kennedy P et al. (1985). Malignant optic
nerve gliomas in adults. J Clin Neuroophthalmol 238–243.Sacks JG, Melen O (1975). Bitemporal field defects in
presumed multiple sclerosis. JAMA 234: 69–72.Sami DA, Saunders D, Thompson DA et al. (2005). The
achiasmia syndrome: congenitally reduced chiasmal
decussation. Br J Ophthalmol 89: 1311–1317.Sato K, Takeuchi H, Kubota T (2009). Pathology of intracra-
nial germ cell tumors. Prog Neurol Surg 23: 59–75.
Sato N, Sze G, Endo K (1998). Hypophysitis: endocrinologic
and dynamic MR findings. AJNR Am J Neuroradiol 19:439–444.
Schaeffer JP (1924). Some points on the regional anatomy of
the optic pathway, with special reference to tumors of the
hypophysis cerebri; and resulting ocular changes. Anat
Rec 28: 243–279.
Schlechte JA (2003). Prolactinoma. N Engl J Med 349:2035–2041.
Selch MT, DeSalles AA, Kelly DF et al. (2003). Stereotactic
radiotherapy for the treatment of lymphocytic hypophysi-
tis. Report of two cases. J Neurosurg 99: 591–596.Seror R, Mahr A, Ramanoelina J et al. (2006). Central ner-
vous system involvement in Wegener granulomatosis.
Medicine (Baltimore) 85: 54–65.Sharma K, Pradhan S, Varma A et al. (2003). Irreversible
blindness due to multiple tuberculomas in the parasellar
cistern. J Neuroophthalmol 23: 211–212.Sibony PA, Lessell S, Wray S (1982). Chiasmal syndrome
caused by arteriovenous malformations. Arch Ophthalmol
100: 438–442.Silverman IE, Liu GT, Bilaniuk LT et al. (1995). Tuberculous
meningitis with blindness and perichiasmal involvement
on MRI. Pediatr Neurol 12: 65–67.Spector RH, Glaser JS, Schatz NJ (1980). Demyelinative
chiasmal lesions. Arch Neurol 37: 757–762.Stippler M, Gardner PA, Snyderman CH et al. (2009). Endo-
scopic endonasal approach for clival chordomas.
Neurosurgery 64: 268–277.Tageuchi J, Handa H, Nasgata I (1978). Suprasellar germi-
noma. J Neurosurg 49: 41–48.Traquair HM (1925). Acute retrobulbar neuritis affecting the
optic chiasm and tract. Br J Ophthalmol 9: 433–450.

THE OPTIC CHIASM 203
Traquair HM (1949). An Introduction to Clinical Perimetry.
6th edn. Kimpton, London.
Tubridy N, Molloy J, Saunders D et al. (2001). Postpartum
pituitary hypophysitis. J Neuroophthalmol 21: 106–108.
Unsold R, Hoyt WF (1980). Band atrophy of the optic nerve.
Arch Ophthalmol 98: 1637–1638.Vates GE, Berger MS, Wilson CB (2001). Diagnosis and
management of pituitary abscess: a review of 24 cases.
J Neurosurg 95: 233–241.Voelker JL, Campbell RL, Muller J (1991). Clinical, radio-
graphic and pathological features of synmptomatic
Rathke’s cleft cysts. J Neurosurg 74: 535–544.Wilson CB (1992). Endocrine-inactive pituitary adenomas.
Clin Neurosurg 38: 10–31.
Wollschlaeger PB, Wollschlaeger G, Ide CH et al. (1971).
Arterial blood supply of the human optic chiasm and
surrounding structures. Ann Ophthalmol 3: 862–864.Woodcock RW, Mandell JW, Lipper MH (1999). Sinus his-
tiocytosis of the suprasellar region: MR imaging findings
– a case report. Radiology 213: 808–810.Yong TY, Li JYZ, Amato L et al. (2008). Pituitary involve-
ment in Wegener’s granulomatosis. Pituitary 11: 77–84.Zarei M, Anderson JR, Higgins JN et al. (2002). Cavernous
sinus syndrome as the only manifestation of sarcoidosis.
Postgrad Med J 48: 119–121.Zimmerman LE, Arkfeld DL, Schenken JB et al. (1983).
A rare choristoma of the optic nerve and chiasm. Arch
Ophthalmol 101: 766–770.