the opioid epidemic’s impact on the most vulnerable opioid epidemic’s impact on the most...
TRANSCRIPT

The Opioid Epidemic’s Impact on the Most VulnerableGINA CONNELLY MDTMC OBSTETRICSMEDICAL DIRECTOR; OBSTETRICS SERVICES; TUCSON MEDICAL CENTER
Illicit Drug Use in Pregnancy Opioid use during pregnancy has escalated, in parallel with the opioid
epidemic in the general population. Pregnant women who use opioids are at increased risk for pregnancy-
associated complications and death. Their infants are at risk for Neonatal Abstinence Syndrome
5.4% of pregnant women admit to using one or more illicit drug By age group
15-17: 14.6% 18-25: 8.6% 26-44: 3.2%
More women drink alcohol (9.4%) and smoke (15.4%) than all other drugs combined. 90% of women addicted to opioids smoke cigarettes
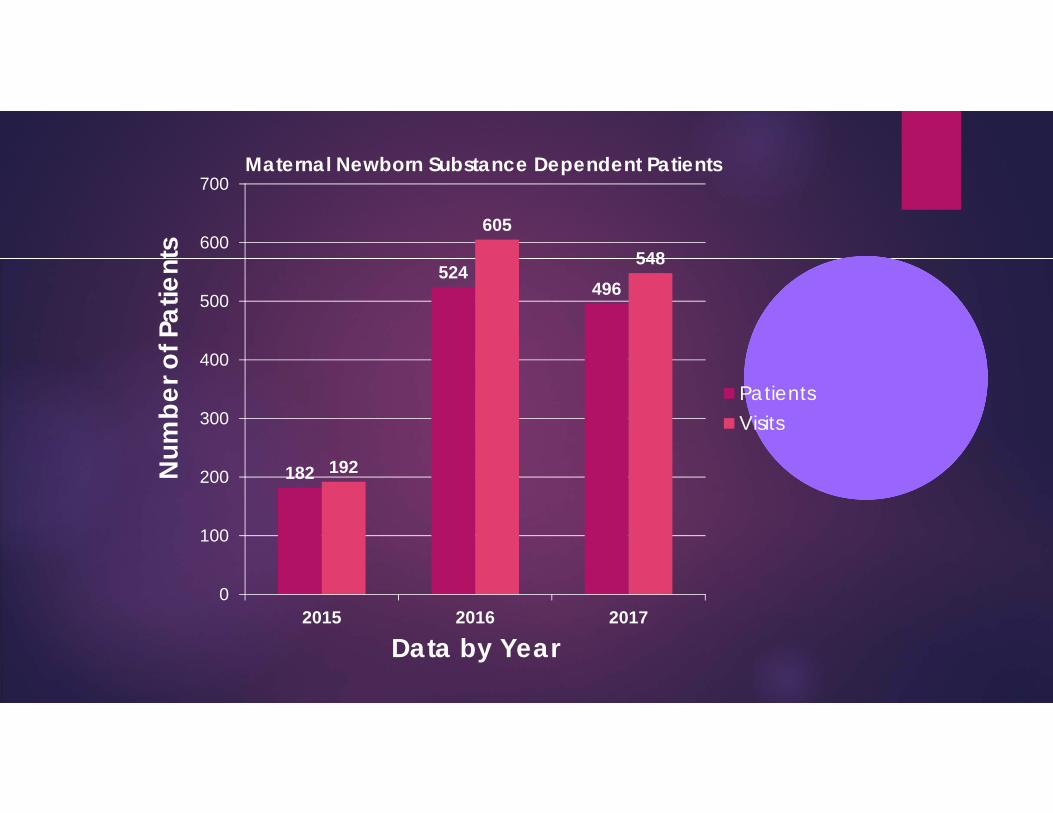
182
524496
192
605
548
0
100
200
300
400
500
600
700
2015 2016 2017
Num
ber o
f Pat
ient
s
Data by Year
Maternal Newborn Substance Dependent Patients
PatientsVisits

Illicit Drug Use and Pregnancy A drug’s effects on the fetus depend on
many things: How much? How often? Fetal response? When during pregnancy was it
used? First trimester
The early stage of pregnancy is the time when main body parts of the fetus form.
Second, Third trimester Interfere with the growth of
the fetus Increase preterm birth Increase in fetal death
Other confounding factors Other Medical Conditions Social Psychological

Lack of Prenatal Care 86% of pregnant opioid –using women report pregnancy was
unintended Establish late care
Missed opportunities for screening, diagnosis, and treatment of pregnancy and medical problems that can improve outcomes for mother and baby
Ashamed to seek care Legal ramifications
Users may not even realize that they are pregnant Misinterpret early signs of pregnancy as opioid withdrawal
Nausea, vomiting, abdominal cramping
Pregnant women are typically highly motivated to modify their behavior in order to help their unborn child. In a national survey from the United States, the mean rate of pregnancy-
related abstinence among users of illicit drugs was 57 percent.

Opioid Associated Maternal Complications Infections
Needle sharing Hepatitis B, C and HIV
Bacteremia/Sepsis
Cellulitis
Endocarditis
Sexually transmitted infections HIV, Syphilis, Gonorrhea, Chlamydia

Opioid Related Pregnancy Complications
6-fold increase in obstetrical complications Intra-amniotic infection Abruption Fetal passage of meconium
21-46% versus12-13%
Premature labor 28% versus 12%
Preeclampsia Postpartum hemorrhage Victims of violence

Opioid Associated Pregnancy Complications: Fetal
Recent study that opioids users had increased risk of congenital heart defects Observational and poor study, no
direct evidence
Decreased birthweight 2490g versus 3176g
Fetal growth restriction Placental Insufficiency
Flucuations in drug level causes placental changes that decrease nutrients to fetus
20% versus 4%
Fetal death Stillbirth
Miscarriage
Neonatal abstinence syndrome (NAS) Drug withdrawal syndrome that
opioid-exposed neonates may experience shortly after birth
Meconium passage

AZ: NAS and Other Drug Exposure
Neonatal Abstinence Syndrome (NAS): Symptoms
Yawning, stuffy nose, sneezing Vomiting Diarrhea Dehydration Sweating Fever or Unstable Temperature
Tremors Irritability(excessive crying) Sleep problems High-Pitched cry Tight muscle tone Hyperactive reflexes Seizures
Poor feeding and suck

Other Drugs with Associated with Neonatal Withdrawal Syndromes
SSRI-Poor Neonatal Adaption Syndrome10-30% chance of symptoms if taken in the last trimester of pregnancy
Non-narcotic withdrawal Alcohol, Barbiturates, Benzodiazepines, Hydroxyzine
Marijuana
No withdrawal but may have long term developmental effects
Cocaine
Symptoms at birth are of the drug toxicity, withdrawal may come later, usually shorter
Hesitant breathing at birthJitterinessSeizuresExaggerated startle reflexWeak cryIncreased motor activity
Poor self regulationHigher arousal Poor muscle toneHypoglycemia Jaundice

Withdrawal ScoringFinnegan Neonatal Abstinence Scoring
An objective numerical scoring system that permits standardized care if inter-rater reliability is verifiedDivided into three assessment groupingsWhen an infant scores a certain amount then medication is often initiatedAs scores stabilize, then the treatment doses are decreased

Which infants develop NAS that requires treatment?
VARIABLE!
If methadone alone:
Genetic basis
Longer the treatment and the higher the dose may correlate with severity but not predictable
If methadone + SSRI or benzodiazepines,
Prolong the withdrawal period
Early data suggest buprenorphine withdrawal is shorter
Heroin withdrawal is shorter than methadone, but the health consequences during pregnancy are worse

Long-Term Outcomes
Specific long term effects of isolated drugs are difficult to determine due to comorbid substance exposure and also environmental and medical risk factors
A variety of results of NAS studies:
minimal to no effect greater than the underlying drug use
effect during toddlerhood that then resolves
persistent effect
Motor effects (more tense, less active, and poor coordination) may recover or are more closely correlated to sociodemographic factors (SES status, nutrition-birthweight, head circumference at birth)
Behavioral effects include less social responsivity, short attention span, and poor social engagement

Beyond the NurseryInfant Discharge Planning
All newborns should have a medical home (PCP) determined prior to discharge to allow flow of information on risk status, referrals, and follow upCare-givers with a substance abuse disorder are more likely to perceive care of a child as stressful and miss well child visitsEarly intervention services can positively impact drug exposed newborns at risk for developmental delayHome nurse visitation programs may reduce encounters for ingestions, injuries, and maltreatment; also can pick up behavioral problems in the children or parental stress

Detoxification in Pregnancy Associated with poor neonatal outcomes.
Early preterm birth or fetal demise The major reason not to attempt detoxification is that it is generally unsuccessful,
Relapse rates of 50% or more. If attempted, it is best to wait until the end of the first trimester
Limited data suggest that miscarriage rates may be higher in the first trimester. Robust evidence has demonstrated that maintenance therapy during pregnancy can
improve outcomes Opioid use during pregnancy can put infants at risk of Neonatal Abstinence
Syndrome Including MAT, prescription opioid use for pain, or non-medical opioid use However, NAS is both expected and treatable, and evidence has shown that it does not
lead to long-term complications ACOG continues to recommend use of Medication Assisted Therapy (MAT) as the
standard of care during pregnancy for women with opioid use disorders.

Opioid Substitution Therapy in Pregnancy Agent
1 g heroin 80 mg methadone
8 mg buprenorphine
Advantages Oral administration
Known dose and purity
Safe and steady availability
Improved maternal/fetal/neonatal outcomes
Opportunity to enter obstetrical care
Barriers to treatment Lack of health insurance
Incarceration
Mental Illness
Transportation
Childcare needs
Guilt about the effect of drugs on the fetus
Fear of legal consequences
Loss of custody of children

Benefits of Methadone Maintenance Have been demonstrated in the pregnant
population. Earlier and more-compliant prenatal care
Improved nutrition and weight gain
Fewer children in the foster system
Improved enrollment in substance abuse treatment and recovery programs
Remain opiate dependent, but generally become more functional
The goal of treatment is to provide sufficient dosing to prevent drug cravings, eliminate illicit use, and keep additional opiates from creating euphoria.
Goal of harm reduction, rather than elimination through abstinence.
The average dose needed to achieve clinical stability is between 80 and 120 mg daily. A dose lower than 60 mg is believed to be
insufficient to prevent drug-seeking behavior.
Due to the physiology of pregnancy, split daily dosing is sometimes recommended

Buprenorphine (Subutex)
Gaining recognition as a treatment for opioid addiction during pregnancy. Favored over buprenorphine/naloxone (Suboxone)
Lack of safety data regarding the combination product
May produce maternal and subsequently fetal hormonal changes.
Less autonomic withdrawal associated with buprenorphine Buprenorphine demonstrates favorable qualities similar to methadone
Decreasing drug cravings with daily dosing Additional benefit of being prescribed by specifically certified physicians as opposed
to federally funded clinics. This benefits patient autonomy and opiate maintenance. Controversial as there are many social and mental health benefits that are less available in
this model.

Comparison of Methadone/Buprenorphine
Jones et al , NEJM 2010;363(24):2320 Continued treatment to end of
pregnancy Methadone 82% Buprenorphine 67%
NAS Buprenorphine needed
less morphine: Shorter hospital stay: 10d
versus 17.5d Shorter treatment for NAS:
4.1 versus 9.9d
The 2010 MOTHER (Maternal Opioid Treatment: Human Experimental Research) Addiction 2012 Nov;107 Suppl 1:1-4 Buprenorphine was associated
with Significantly lower doses
of morphine for treatment of NAS
Shorter duration of treatment
Shorter hospital stay than methadone.

CASE PRESENTATION
A.A. is a 23yo G3P2 at 28 weeks of pregnancy Presents to the Emergency Room Friday evening at 11pm requesting
to “detox” from her heroin addiction Unplanned pregnancy No prenatal care Past medical history includes anxiety and depression for which she
stopped her medications when she found out she was pregnant Other children in foster care with a family member

PAPN: Polysubstance Abuse in Pregnancy and Newborn
Coordinate community resources in Tucson, Arizona Community wide effort to improve
patient care in women with polysubstance abuse in pregnancy with focus on opioid addiction Social Services
Community Treatment Programs
Physicians
Pharmacists
Successes Community wide drug
screening tool
Develop protocols for safe transition to methadone/subutex in ”off” hours.
Increase communication and entry into community treatment programs and prenatal care
Establish neonatal abstinence program

PAPN Universal Screening Tool Multiple societies and agencies
consider screening for substance abuse a part of complete obstetric care and recommend asking all pregnant women about their use of alcohol and illicit drugs Universal screening
Substance users come from all economic strata, ages and races
Ideally, screening is performed at the initial prenatal visit
All Hospitals involved in development
In past 12 months, have you used the following? Please include onetime use. Yes No Last Used Frequency
Alcohol (beer, wine, liquor) Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Tobacco (Patch, Vape) Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Cannabis (marijuana, pot, grass, hash, spice, etc) *Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Cocaine (coke, crack, etc.) *Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Prescription stimulants (Ritalin, Concerta, Dexedrine, Adderall, Diet Pills, etc) Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Methamphetamine (Speed, Crystal Meth, Ice, etc) *Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Inhalants (Nitrous oxide, glue, gas, paint thinner, etc) Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Sedatives or Sleeping pills (Valium, Serepax, Ativan, Xanax, Librium, Rohypnol, GHB, etc)
Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Hallucinogens (LSD, Acid, Mushrooms, PCP, Special K, Ecstasy, Molly, Bath Salts, etc) *
Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Street Opioids (Heroin, Opium, etc * Never Once or Twice Daily Weekly Monthly
Amount used:____________________________
Prescription Opioids (Fentanyl, Oxycodone, [OxyContin, Percocet], Hydrocodone [Vicodin], Methadone, Buprenorphine, etc) *
Never Once or Twice Daily Weekly Monthly
Amount used:____________________________Script?
Other – Specify Never Once or Twice Daily Weekly Monthly
Amount used:____________________________

Risk Factors for Drug Testing Substance Abuse Indications for testing
Positive screening tool Previous positive drug test History of illicit drug use Monitoring compliance with methadone/subutex Pregnancy complications associated with drug use Frequent requests for prescription drugs of abuse Noncompliance with prenatal care

Universal Drug Laboratory Testing Generally still not recommended
because of the limitations of these tests
There is no consensus regarding when drug tests should be used in pregnant women or the best method for analyzing biological samples (urine, blood, hair, saliva) Urine drug testing is the most
common
Positive tests for illicit drugs can havelegal and economic implications.
Women should be informed of thepotential ramifications of a positivetest result and should give informedconsent prior to testing
Must have a plan to treat Random testing is unethical unless
patient: Unconscious Obvious signs of intoxication and
testingto provide approprtiatemedical interventions
Know State requirements for testingand reporting drug test results.

ACOG Toolkit on STATE LEGISLATION Pregnant women & drug abuse, dependence and addiction
If considering mandatory urine testing, Legislation should specify: Testing is permitted only with the patient’s consent and to
confirm suspected or reported drug use. Patient consent also applies to testing by hospitals when
pregnant women are admitted for labor and delivery. In the Medicaid program, a pregnant woman’s eligibility for
Medicaid should not be contingent on submitting to a mandatory urine drug test.
Similarly, reimbursement for prenatal, labor and delivery care should not be contingent on performance of urine drug testing.
Methadone Induction Team Sport
Patient agrees to long term treatment program and MAT therapy Physician and Pharmacy team initiate therapy under standardized
guidelines Social worker to identify outpatient program Outpatient program facilitates timely admission to care Obstetrical care is instituted All within a limited timeline
NASA
Neonatal Abstinence Syndrome AnnexSeparate area of the NICU so sights and sounds can be better regulated according to infant state
Parents know they are all in the same situation so less shame is felt
A group of nurses who self identified with personal interest in this population
Aromatherapy-lavender and peppermint oil
Neonatal massage, integration with pediatric therapies
Standardized protocol for medical and nutritional management

Preventing Pregnancy Risk Associated with Opioids
Types of Long Acting Reversible Contraception

Postpartum LARC The immediate postpartum period is a particularly favorable time for IUD
or implant insertion. 45% of women who planned on an IUD postpartum failed to return for
insertion Women who have recently given birth are often highly motivated to use
contraception, they are known not to be pregnant, and the hospital setting offers convenience for both the patient and the health care provider.
Postpartum LARC is now reimbursed by AHCCCS Not reimbursed by all commercial plans
In addition, women are at risk of an unintended pregnancy in the period immediately after delivery. In a study in which women were instructed to abstain from sexual
intercourse until 6 weeks postpartum, 45% of participants reported unprotected sex before that time.

Parting thoughts….. Opioid abuse in pregnancy is a significant problem affecting 2
patients – mother and newborn Developing standardized screening, more cases in pregnancy will
be identified and possible intervention started Establishing coordinated referral to treatment and prenatal care can
improve outcomes Coordinating community resources will empower us to more
efficiently treat the problem Mental health support Emphasis on contraception and planned pregnancy

References1. Gossop M, Green L, Phillips G, Bradley B. Lapse, relapse and survival among opiate addicts after treatment. A prospective follow-up study. Br J Psychiatry. 1989;154:348–353.2. Dashe JS, Jackson GL, Olscher DA, et al. Opioid detoxification in pregnancy. Obstet Gynecol. 1998;92(5):854–858.3. Rementeriá JL, Nunag NN. Narcotic withdrawal in pregnancy: stillbirth incidence with a case report. Am J ObstetGynecol. 1973;116(8):1152–1156.4. Zuspan FP, Gumpel JA, Mejia-Zelaya A, et al. Fetal stress from methadone withdrawal. Am J Obstet Gynecol. 1975;122(1):43–46.5 Luty J, Nikolaou V, Bearn J. Is opiate detoxification unsafe in pregnancy? J Subst Abuse Treat. 2003;24(4):363–367.6. Jones HE, O’Grady KE, Malfi D, Tuten M. Methadone maintenance vs. methadone taper during pregnancy: maternal and neonatal outcomes. Am J Addict. 2008;17(5):372–386.8. Burns L, Mattick RP, Lim K, Wallace C. Methadone in pregnancy: treatment retention and neonatal outcomes. Addiction. 207;102(2):264–270.9. McCarthy JJ, Leamon MH, Parr MS, Anania B. High-dose methadone maintenance in pregnancy: maternal and
neonatal outcomes. Am J Obstet Gynecol. 2005;193 (3 Pt 1):606–61010. Arunogiri S et al. Managing opioid dependence in pregnancy: a general practice perspective. Aust Fam Physician. 2013 Oct; 42(10):713-6. 11. Baldacchino A. Neurobehavioral consequences of chronic intrauterine opioid exposure in infants and preschool children: a systematic review and meta-analysis. BMC Psychiatry. 2014 Apr 8; 14:104. 12. Desai RJ. Increase in prescription opioid use during pregnancy among Medicaid-enrolled women. Obstet Gynecol. 2014 May; 123(5):997-1002. 13. Foder A et al. Behavioral effects of perinatal opioid exposure. Life Sci. 2014 May 28; 104(1-2):1-8. Fullerton CA et al. Medication-assisted treatment with methadone: assessing the evidence. Psychiatr Serv. 2014 Feb 1; 65(2):146-57. 14. Prasad, M . When opiate abuse complicates pregnancy. Contemporary Ob/Gyn. 2014, Feb 1.

References 15. Fischer G. Treatment of opioid dependence in pregnant women. Addiction 2000;
95:1141.
16. ACOG Committee on Health Care for Underserved Women, American Society of Addiction Medicine. ACOG Committee Opinion No. 524: Opioid abuse, dependence, and addiction in pregnancy. Obstet Gynecol 2012; 119:1070.
17. Johnson RE, Jones HE, Fischer G. Use of buprenorphine in pregnancy: patient management and effects on the neonate. Drug Alcohol Depend 2003; 70:S87.
18. Jones HE, Johnson RE, Jasinski DR, et al. Buprenorphine versus methadone in the treatment of pregnant opioid-dependent patients: effects on the neonatal abstinence syndrome. Drug Alcohol Depend 2005; 79:1.
19. Kakko J, Heilig M, Sarman I. Buprenorphine and methadone treatment of opiate dependence during pregnancy: comparison of fetal growth and neonatal outcomes in two consecutive case series. Drug Alcohol Depend 2008; 96:69.
20. Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure. N Engl J Med 2010; 363:2320.