the neuropsychology of reading disordersworldowiki.wikispaces.com/file/view/feiffer-dyslexia.pdf ·...
TRANSCRIPT
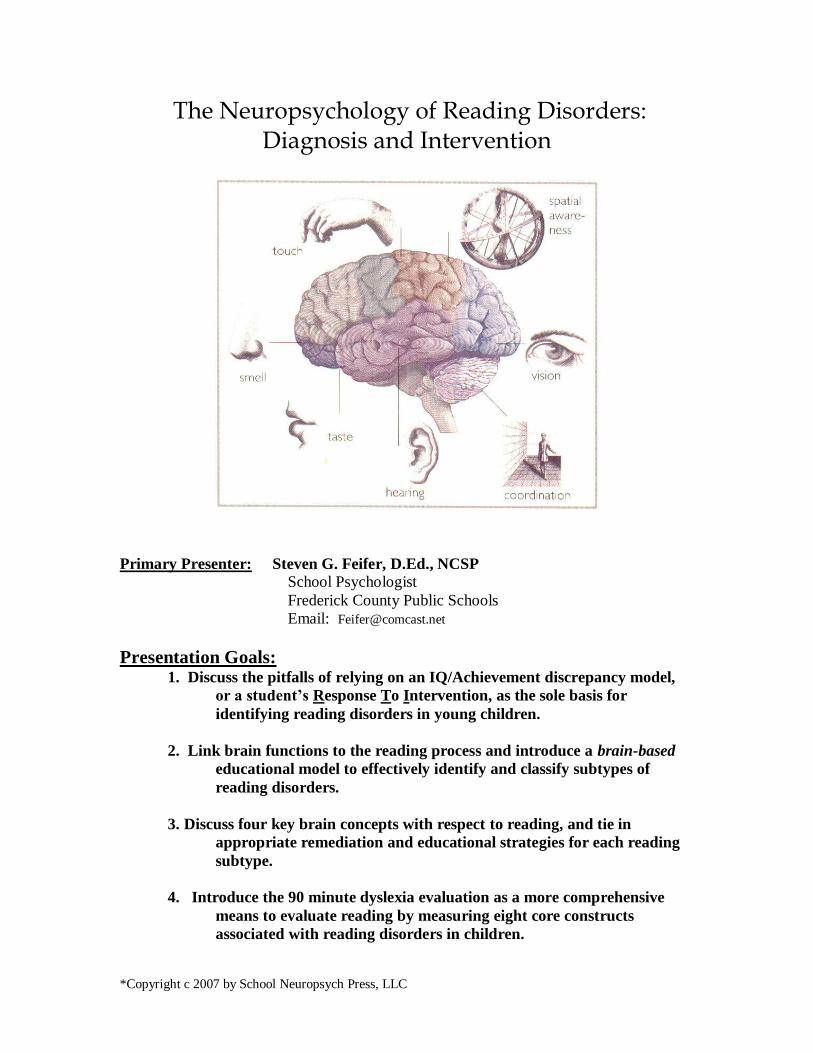
The Neuropsychology of Reading Disorders: Diagnosis and Intervention
Primary Presenter: Steven G. Feifer, D.Ed., NCSP School Psychologist
Frederick County Public Schools
Email: [email protected]
Presentation Goals: 1. Discuss the pitfalls of relying on an IQ/Achievement discrepancy model,
or a student’s Response To Intervention, as the sole basis for
identifying reading disorders in young children.
2. Link brain functions to the reading process and introduce a brain-based
educational model to effectively identify and classify subtypes of
reading disorders.
3. Discuss four key brain concepts with respect to reading, and tie in
appropriate remediation and educational strategies for each reading
subtype.
4. Introduce the 90 minute dyslexia evaluation as a more comprehensive
means to evaluate reading by measuring eight core constructs
associated with reading disorders in children.
*Copyright c 2007 by School Neuropsych Press, LLC
Neuropsychology of Reading Disorders
Page 2
5 Pitfalls of Aptitude/Achievement Discrepancies
1. There is no universal agreement on what the discrepancy should be.
2. It remains unclear as to which IQ score should be used to establish a
discrepancy.
3. A discrepancy model of reading disabilities precludes early identification.
4. Intelligence is more a predictor of school success, and not necessarily a
predictor of successful reading.
5. A discrepancy model promotes a “wait and fail” policy forcing intervention to
come after the fact.
ALTERNATIVE ASSESSMENT METHODOLOGIES
Reauthorization of IDEA:
* President Bush signed the IDEA bill into law in December, 2004.
* States may opt out of using a discrepancy model to identify learning
disabilities, and replace by using a Response-To-Intervention
model.
* Gives school districts flexibility to craft a policy whereby students who
do not respond to scientifically-based early reading programs may
be considered eligible for special education services.
* Requires districts with significant over-identification of minority
students to consider eliminating IQ testing and establish
procedures to reduce disproportional representation in special ed.
Developmental Dyslexia: The term refers to an inability to acquire functional reading
skills despite the presence of normal intelligence and exposure to adequate
educational opportunities. This term is often synonymous with the term
"learning disabled", and assumed to represent 5 to 10 percent of all school-aged
children.

Neuropsychology of Reading Disorders
Page 3
Six Components of an Effective RTI Model
(1)Universal Screening - for all students a minimum of three times per year.
(2)Baseline Data - using curriculum-based measurement as primary data gathering
means.
(3)Measurable Terms - define problem areas numerically.
(4)Accountability Plan – monitor fidelity of selected intervention.
(5)Progress Monitoring – how, where, and when intervention results will be
measured and recorded.
(6)Data Based Decision Making – ongoing analysis of data to drive future
intervention decisions.
RESPONSE TO INTERVENTION MODEL
FIVE COMMON MYTHS ABOUT RTI
Neuropsychology of Reading Disorders
Page 4
COMMON MYTHS ABOUT RTI
(1)The outcome and intent of RTI is identification” - The intent of RTI is to utilize
evidenced based instruction and data based decision making.
(2)“Tier IV is only special education” - the last tier is simply the most intense level of
intervention.
(3)“RTI is only for pre-referral decision making” - RTI is a model for assisting all
learners, not just weeding out candidates for special education.
(4) “RTI is best used to distinguish LD students from students not achieving due to
poor instruction” – The main benefit of RTI is prevention.
(5) “RTI is only beneficial for reading” – RTI has just as much research
documenting its effectiveness for behavioral concerns.
Curriculum-Based Measurement – an assessment of reading fluency by selecting a
random probe from the student’s basal reader, and the median number of words read
correctly in one minute is recorded. Multiple measures in 3-minute intervals are
administered throughout the year, instead of relying upon lengthy standardized tests.
RTI ADVANTAGES AND DISADVANTAGES
Advantages: * Better ecological validity than norm referenced testing.
* Quicker and cheaper than norm referenced testing.
* Allows for earlier intervention opportunities.
* Emphasis on discrepancy from peer performance, not IQ.
* Evaluation hi-lights reading, not bureaucratic categories
* Linked to a problem solving model (Shinn, 2002).
Disadvantages: * Not a diagnostic approach.
* Does not assess many other aspects of reading such as
comprehension.
* Does not address the core aspects of reading as put forth by
the National Reading Panel (2000).
* Does not answer the most important question: Why?

Neuropsychology of Reading Disorders
Page 5
NATIONAL READING PANEL (2000)
NATIONAL READING PANEL CONCLUSIONS
Kindergarten through 1st grade
(1) The younger the child, the better the outcome.
(2) The “at-risk” child responds best to small group instruction (3:1), with
phonological awareness training being combined with explicit phonics
instruction.
(3) Highly trained teachers achieve the best results.
(4) Frequency of instruction (4-5 days per week) was more effective than sporadic
instruction (2 days per week).
(5) Gains were maintained in most children at long-term follow up.
(6) The following characteristics of the child were associated with poor outcome:
a) attention or behavioral concerns
b) low socioeconomic status
c) poor verbal skills
d) poor rapid naming skills
COMPREHENSION
LANGUAGE
FLUENCY
PHONICS
PHONEMIC AWARENESS
Neuropsychology of Reading Disorders
Page 6
NATIONAL READING PANEL CONCLUSIONS
2nd
through 6th
grades
(1) Readers at this age respond to explicit phonological instruction with improved
word reading, the gains were not as strong as with younger children.
(2) These readers were less responsive to explicit phonics, though did better in one-
to-one or small group instruction.
(3) More intensive work for a longer duration was required.
(4) Spelling and fluency did not improve very well, though some improvement was
noted with reading comprehension.
(5) Gains were maintained in most children at long-term follow up.
(6) Computer instruction served as an effective aid, but was not effective by itself.
(7) The following characteristics of the child were associated with poor outcome:
a) attention or behavioral concerns
b) low socioeconomic status
c) poor verbal skills
d) poor rapid naming skills
NEUROPSYCHOLOGY: A BRAIN/BEHAVIORAL
APPROACH
Evolution of Reading: * Encompassed just the past 5000 to 6000 years
* Approximately 1/3rd
of world's population illiterate
* Human beings seem pre-wired to acquire sound/symbol
language code.
* Some estimates suggest 75% of children will learn to read
in spite of methodology (Mather, 1992).
* 20 % of children need a specific method (e.g. Alphabetic
Phonics)
* 5 % may never acquire this skill at a functional level
Neuropsychology: An analysis of learning and behavior which examines brain-behavior
relationships. The underlying assumption is that the brain is the seat of ALL behavior;
therefore, knowledge of cerebral organization should be the key to unlocking the mystery
behind most cognitive tasks.

Neuropsychology of Reading Disorders
Page 7
GENERAL BRAIN STRUCTURES
Brain: * Weighs approximately 1400 grams ( 3 pounds)
* 100 billion cells comprised of neurons (gray matter) and glial cells
(white matter)
* Each neuron makes contact with as many as 10,000 other neurons.
* The firing rate of a neuron ranges from a few to several hundred per
second.
* Makes up less than 2 percent of body weight, though uses up 25 percent
of oxygen supply and 70 percent of glucose.
* DNA evidence suggests human brain has been evolving for
approximately 5 million years.
Neocortex: Frontal Lobes - organizes and arranges information leaving the brain.
Parietal Lobes - responsible for sensory and tactile functions.
Temporal Lobes – houses acoustically based information and language
Occipital Lobes - visual processing centers of the brain.
Parietal Lobe Frontal Lobe
Temporal Lobe
Occipital Lobe
Neuropsychology of Reading Disorders
Page 8
4 KEY BRAIN CONCEPTS WITH RESPECT TO READING
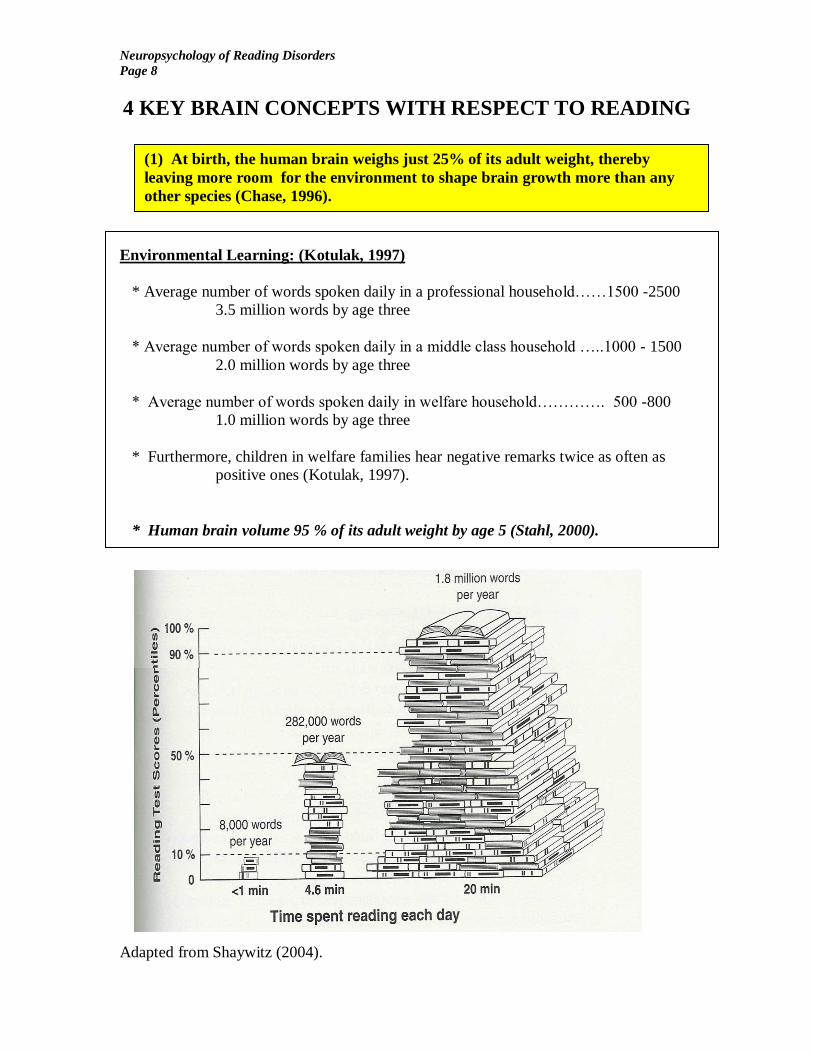
Environmental Learning: (Kotulak, 1997)
* Average number of words spoken daily in a professional household……1500 -2500
3.5 million words by age three
* Average number of words spoken daily in a middle class household …..1000 - 1500
2.0 million words by age three
* Average number of words spoken daily in welfare household…………. 500 -800
1.0 million words by age three
* Furthermore, children in welfare families hear negative remarks twice as often as
positive ones (Kotulak, 1997).
* Human brain volume 95 % of its adult weight by age 5 (Stahl, 2000).
Adapted from Shaywitz (2004).
(1) At birth, the human brain weighs just 25% of its adult weight, thereby
leaving more room for the environment to shape brain growth more than any
other species (Chase, 1996).

Neuropsychology of Reading Disorders
Page 9
4 KEY BRAIN CONCEPTS WITH RESPECT TO READING
Fast Facts: * Prenatal malnutrition causes more permanent harm than postnatal
malnutrition because it slows the proliferation rate of cells (Byrnes,
2001). Postnatal malnutrition hinders cell connections and
myelination process. Enriching diet can ameliorate the problem.
* More synapses present in brain by age 6 than any other time
(Stahl,2000).
* 83 percent of dendritic sprouting occurs after birth (Berninger &
Richards, 2002)
* Ectopias represent misplaced clusters of neurons along the left
perisylvan regions modulating rapid sound and symbol processing.
Ectopias may be related to prenatal alcohol and nicotine
consumption, as well as genetic scripts. These focal malformations
have been found in fMRI studies of the dyslexic brain (Galaburda
& Cestnick, 2003).
STAGES OF BRAIN DEVELOPMENT:
I. Proliferation - cells proliferate and divide in the developing fetus from
an inside to outside fashion. The cortex overproduces neurons, with
production ending by 7th
prenatal month – maybe 1 trillion formed at a
rate of 250,000 cells per minute (Byrnes, 2001).
II. Migration - cells migrate to appropriate location in the brain.
a) Aggregation - cells cluster into nuclei, like thalamus.
b) Arborization - thickening of dendrites as cells
interconnect.
III. Differentiation - First 2 or 3 years postnatally, neurons continue to
subdivide forming an overabundance of synapses. This
overproduction appears to help children recover from brain
damage more easily than adults (plasticity).
Pruning - many more neurons create synaptic connections and functional circuits than
are needed. For maximum efficiency on a task, cell death or axonal
retraction is essential. Perhaps 50 to 90% eventually die (apoptosis)
leaving the mature brain with 100 billion neurons.
Auditory Pruning - every child is born with the ability to discriminate all sounds.
However, based upon exposure to cultural specific dialects, a child
becomes tuned to only sounds from host language. Explains why
children born in another country continue to have foreign accents if
brought to the United States past age five.
(2) Prenatal factors have been linked to brain development, as proteins are
crucial in forming latticework of synaptic connections between brain cells.
Neuropsychology of Reading Disorders
Page 10
4 KEY BRAIN CONCEPTS WITH RESPECT TO READING
SUMMARY: There are certain windows of opportunity for learning based upon the
developing nervous system, brain growth spurts, and subsequent myelination. Sensory
experiences are essential for teaching brain cells their jobs, and after a certain critical
period, brain cells lose their opportunity to learn their jobs (Kotulak, 1997). For instance:
Vision: * If a child does not process visual experiences by age two, the sense of
sight may never develop properly.
Hearing: * If a child does not hear words by age 10, it becomes increasingly
difficult to discriminate among the sounds of a language.
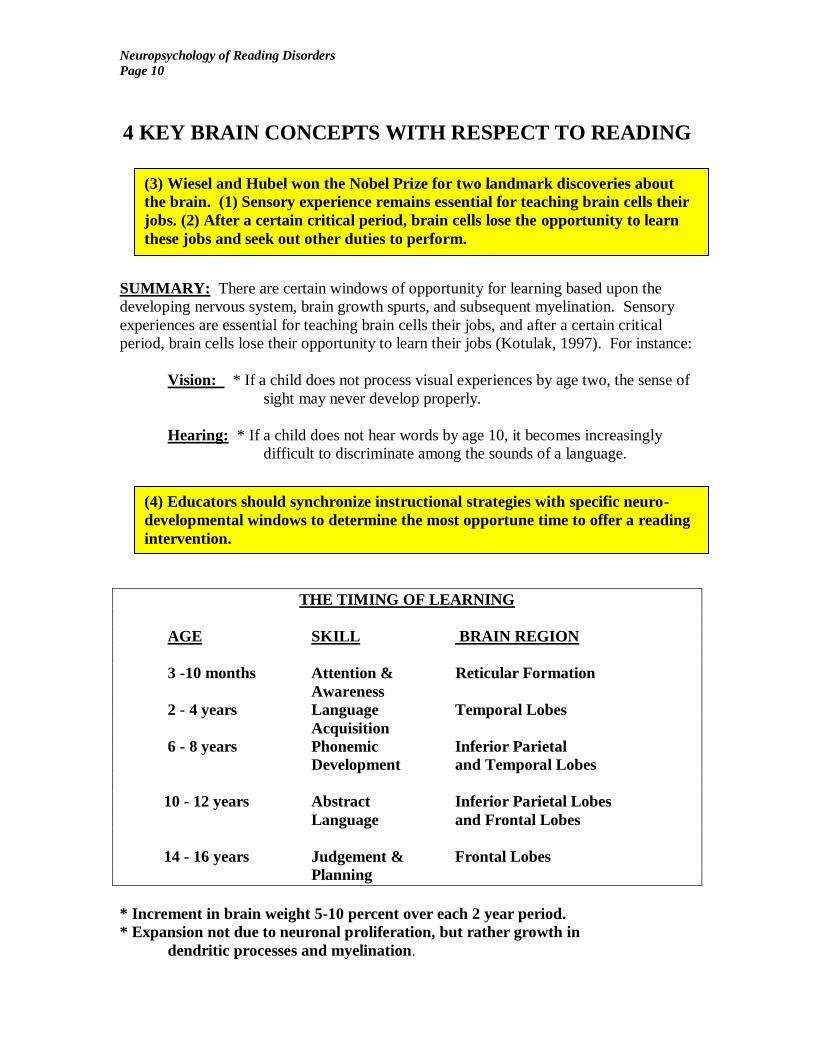
THE TIMING OF LEARNING
AGE SKILL BRAIN REGION
3 -10 months Attention & Reticular Formation
Awareness
2 - 4 years Language Temporal Lobes
Acquisition
6 - 8 years Phonemic Inferior Parietal
Development and Temporal Lobes
10 - 12 years Abstract Inferior Parietal Lobes
Language and Frontal Lobes
14 - 16 years Judgement & Frontal Lobes
Planning
* Increment in brain weight 5-10 percent over each 2 year period.
* Expansion not due to neuronal proliferation, but rather growth in
dendritic processes and myelination.
(3) Wiesel and Hubel won the Nobel Prize for two landmark discoveries about
the brain. (1) Sensory experience remains essential for teaching brain cells their
jobs. (2) After a certain critical period, brain cells lose the opportunity to learn
these jobs and seek out other duties to perform.
(4) Educators should synchronize instructional strategies with specific neuro-
developmental windows to determine the most opportune time to offer a reading
intervention.
Neuropsychology of Reading Disorders
Page 11
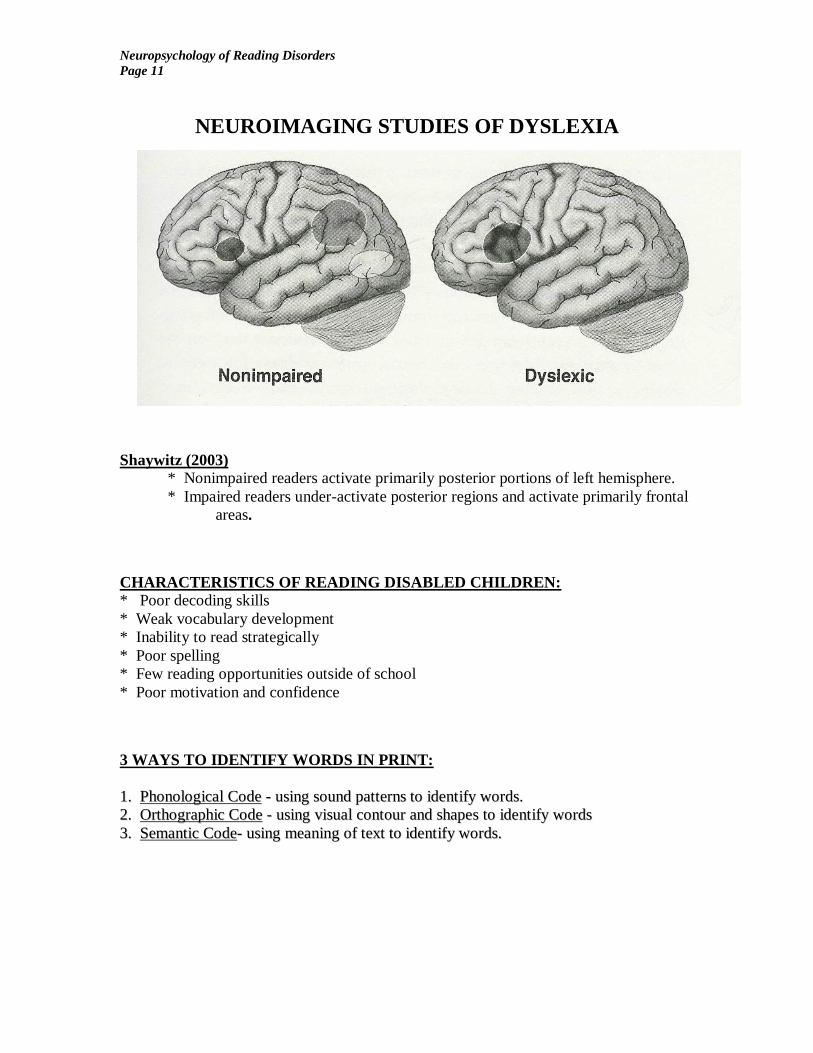
NEUROIMAGING STUDIES OF DYSLEXIA
Shaywitz (2003)
* Nonimpaired readers activate primarily posterior portions of left hemisphere.
* Impaired readers under-activate posterior regions and activate primarily frontal
areas.
CHARACTERISTICS OF READING DISABLED CHILDREN:
* Poor decoding skills
* Weak vocabulary development
* Inability to read strategically
* Poor spelling
* Few reading opportunities outside of school
* Poor motivation and confidence
3 WAYS TO IDENTIFY WORDS IN PRINT:
11.. PPhhoonnoollooggiiccaall CCooddee -- uussiinngg ssoouunndd ppaatttteerrnnss ttoo iiddeennttiiffyy wwoorrddss..
22.. OOrrtthhooggrraapphhiicc CCooddee -- uussiinngg vviissuuaall ccoonnttoouurr aanndd sshhaappeess ttoo iiddeennttiiffyy wwoorrddss
33.. SSeemmaannttiicc CCooddee-- uussiinngg mmeeaanniinngg ooff tteexxtt ttoo iiddeennttiiffyy wwoorrddss..

Neuropsychology of Reading Disorders
Page 12
SUBTYPES OF DYSLEXIA
1. Phonological Subtype - Great difficulty using phonological route in
reading, so visual route to lexicon used. There is little reliance
on letter to letter sound conversion. Instead, an over-reliance
on visual cues to determine meaning from print.
Anatomical Correlates: Left temporal-parietal cortex
Interventions: Similar to the National Reading Panel’s (2000) findings, there is
KEY BRAIN REGIONS IN DYSPHONETIC DYSLEXIA
Heschl’s Gyrus – auditory perception and discrimination (phonemic awareness).
Superior Temporal Gyrus – modulating the 44 phonemes of the English language.
Angular Gyrus – cross modal association area underlying mapping symbols to sounds.
Supramarginal Gyrus – cross modal association area underlying the spatial appreciation
and positioning of sounds.
Inferior Frontal Gyrus – end point for inner articulation region.
Dorsal Stream – all of the aforementioned structures involved in the ability to
phonologically assemble a word. A relatively slower paced
learning network.
Heschl’s
Gyrus Superior Temporal Gyrus
Angular Gyrus
Supramarginal Gyrus
Inferior Frontal Gyrus
Neuropsychology of Reading Disorders
Page 13
PHONOLOGIAL DYSLEXIA INTERVENTIONS
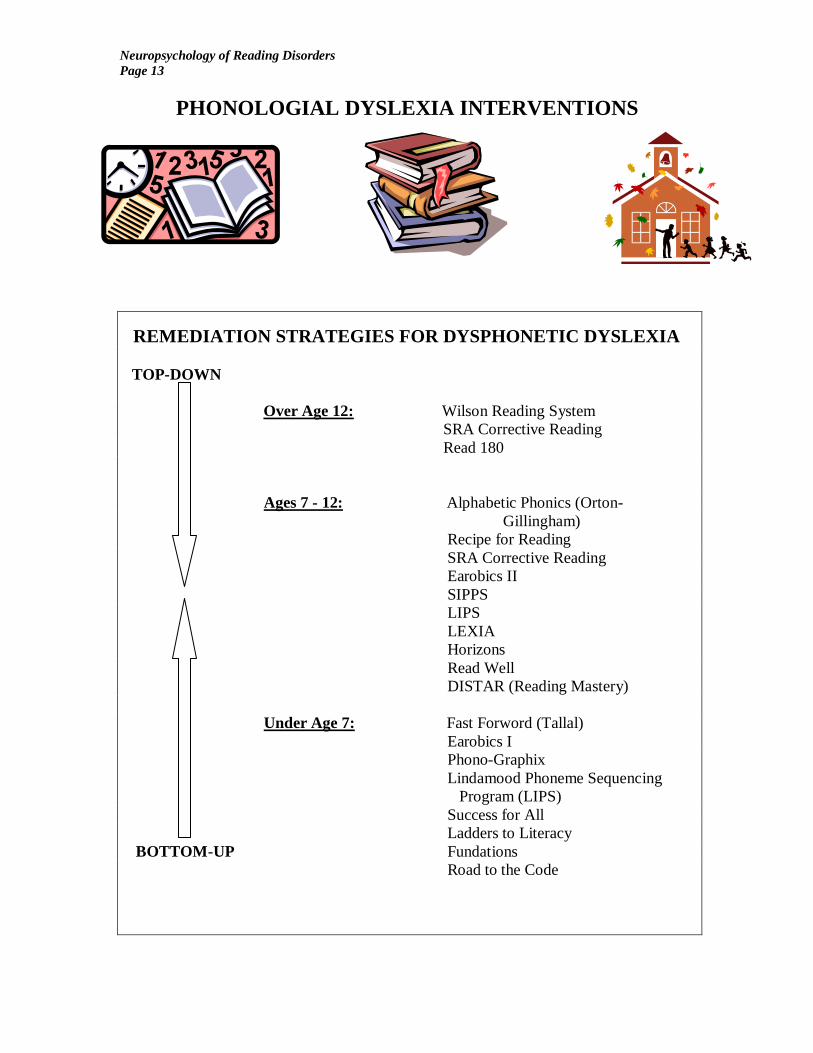
REMEDIATION STRATEGIES FOR DYSPHONETIC DYSLEXIA
TOP-DOWN
Over Age 12: Wilson Reading System
SRA Corrective Reading
Read 180
Ages 7 - 12: Alphabetic Phonics (Orton-
Gillingham)
Recipe for Reading
SRA Corrective Reading
Earobics II
SIPPS
LIPS
LEXIA
Horizons
Read Well
DISTAR (Reading Mastery)
Under Age 7: Fast Forword (Tallal)
Earobics I
Phono-Graphix
Lindamood Phoneme Sequencing
Program (LIPS)
Success for All
Ladders to Literacy
BOTTOM-UP Fundations
Road to the Code
Neuropsychology of Reading Disorders
Page 14
SURFACE DYSLEXIA 2. Surface Dyslexia - these children tend to over-rely on sound/symbol relationships as
the process of reading never becomes automatic. Words are broken down to individual
phonemes and read very slowly and laboriously, especially where phonemes and
graphemes are not in a 1 to 1 correspondence.
Error analysis of Surface Dyslexia:
Word Read as:
island ……………………… izland
grind ………………………. grinned
listen ……………………… liston
begin ……………………… beggin
lace ……………………….. lake
Structural Explanations for Surface Dysgraphia:
(1) Angular gyrus: Goldberg (1989) reasoned that some reading and writing
deficits may occur due to the disintegration of visual and spatial representations in
our brains. Areas of the occipital lobe (processing vision) and the parietal lobe
(processing spatial awareness) intersect in the inferior parietal region known as
the angular gyrus (interface of occipital and parietal lobes). In the left
hemisphere, this region of our brain allows for the appropriate visual-spatial
mapping of linguistic information.
(2) Insular Cortex - buried deep in the folds between parietal and temporal
lobes. PET studies have suggested involvement in automatizing the reading
process (Paulesu, et al, 1996) May serve as a “lexical checking” system to allow
readers to double check for unique spelling of phonologically consistent words
(Owen, Borowsky, & Sarty, 2004).
(3) Multiple Pathway Model (Shaywitz, 2003) - there are multiple pathways in
the brain which modulate various aspects of the reading process. The
occipital-temporal (Fusiform Gyrus) region automatically recognizes word
forms. Dyslexics tend to under-activate this region, also called ventral stream.
(4) Magnocellular pathway deficits have been linked to speed of temporal
lobe processing (Demb, Boynton, & Heeger 1997). Some studies suggest
27% fewer neurons in magnocellular pathways from retina to LGN to
occipital lobes (Livingstone, et al., 1991).
* Some studies have linked deficits in this circuitry affects up to 75 percent
of dyslexics (Ridder, Borting, Coope, McNeel, & Huang, 1997).
* Magno (large) cells are heavily mylinated meaning they have much higher
conduction velocities than parvo cells, which process color and fine
detail. Magno cells process visual motion, and motion sensitivity
correlates strongly with reading and orthographic processing (Stein,
2000).

Neuropsychology of Reading Disorders
Page 15
SURFACE DYSLEXIA INTERVENTIONS
Remediation Techniques: Under Age 7: Analytic or Embedded Phonics Approach
("top down" methodology)
Reading Recovery
Early Steps
Ages 7 - 12: Great Leaps program
Read Naturally
Quick Read
RAV-O
Over Age 12:…. Neurological Impress method
Wilson Reading System
Laubach Reading Series
Read 180
* Reversals: According to Stein (2000), most dyslexic children complain that
letters seem to jump around when reading. During the reading process, the eyes remain
fixated on an individual word for just 300msec before saccading to the next. Even during
these brief fixations, the eye moves approximately 1 degree, or the equivalent of 4 or 5
letters. The magnocellular system allows us to stabilize this movement, but many dyslexics
cannot, therefore transposing letters when reading. This unintended eye movement varies
in each eye, thus resulting in a high level of binocular instability. Since this instability
causes the line of sight for each eye to cross into an unintended visual field, the letters seem
to change places.
Neuropsychology of Reading Disorders
Page 16
MIXED DYSLEXIA
3. Mixed Dyslexia - severely impaired readers with characteristics of both
phonological deficits as well as visual/spatial deficits. These readers have
nousable key to the reading and spelling code. Very bizarre error patterns
observed.
Structural Explanations: (1) Some studies (Hynd, Hall, Novey, Eliopulos, Black, Gonzalez, & Edmonds,
Riccio, & Cohen, 1995) have suggested that the genu of the corpus callosum is
much smaller in dyslexic individuals. Duara et al. (1991) noted the most posterior
region of the corpus callosum, termed the splenium, (which maps directly to the
plana temporale) was actually larger in dyslexic men than controls.
(2) According to Bakker (1992), by the end of 1st grade there is a hemispheric
shift of reading mediated primarily by the left hemisphere. Mixed dyslexia may
reflect deficits in the ability of the brain to shift modes of operation.
(3) Multiple breakdowns in both the phonological route (superior temporal
gyrus) , the automatic word recognition route (fusiform gyrus), and the semantic
route (frontal lobes) may lead to mixed dyslexia.
(4) According to Pennington et al., (1999) the insular cortex, which has been
associated with the automatic retrieval of linguistic codes, is smaller in
dyslexics. Neuroimaging studies have demonstrated that dyslexics do not
activate this brain region when compared to controls (Corina, Richards, Serafini,
Richards, Steury, Abbott, Echelard, Maravilla, & Berninger, 2001).
4 KEYS TO REMEDIATION
(1) Balanced Literacy - An eclectic and approach capitalizing on the particular strengths
of the child. Perhaps using a multi-sensory type of Orton-Gillingham program, coupled
with a fluency model such as Read Naturally, and the computerized models of Read 180.
Program depends upon the age, skill level, and neurodevelopmental profile of the child.
(2) Top Down Strategies – Often atypical development in various regions along the left
temporal-parietal cortices responsible for modulating the phonological aspect of reading,
and mapping these sounds to the visual word form association areas (Temple, 2002;
Shaywitz, et al, 2003; Noble & McCandliss, 2005).
(3) Socioeconomic Status - According to Noble and McCandliss (2005), socioeconomic
status (SES) is a very strong predictor of reading skills due primarily to the home literacy
environment. Therefore, schools need to provide more reading opportunities.
(4) Motivation and Confidence –Great Leaps, Read Naturally, and Neurological Impress
tend to give immediate feedback to students that they are improving, and can be used as a
confidence builder as well.
Neuropsychology of Reading Disorders
Page 17
READING COMPREHENSION
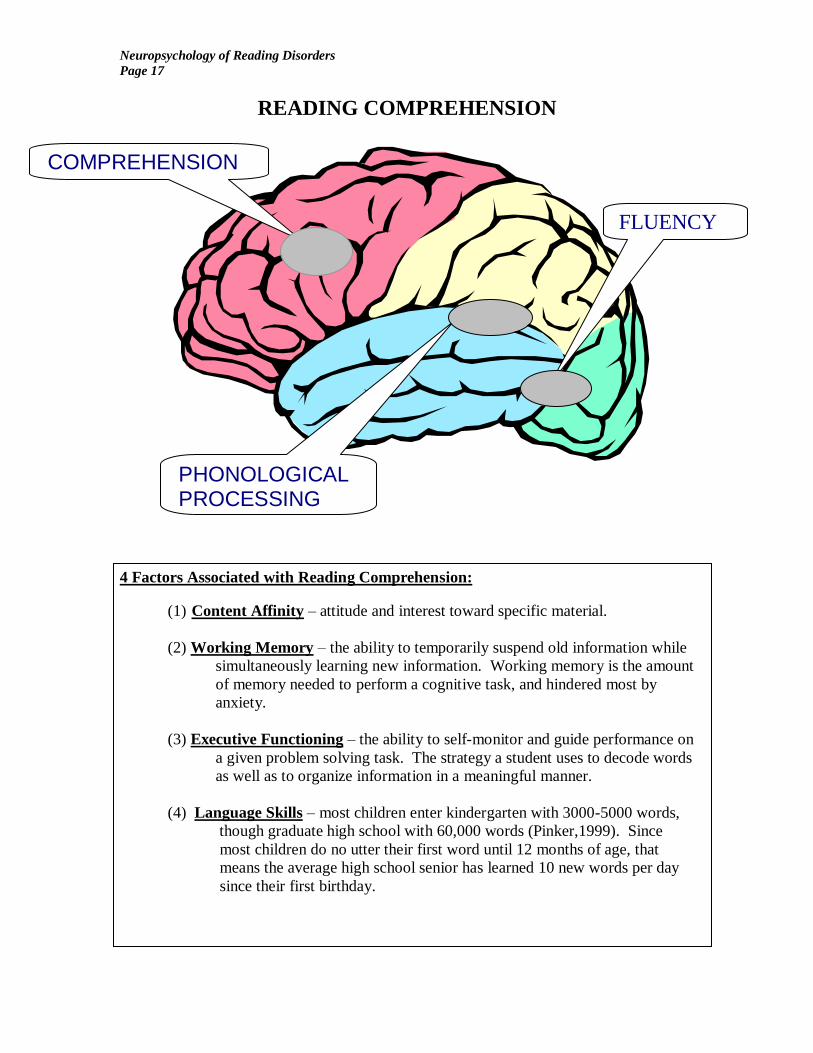
4 Factors Associated with Reading Comprehension:
(1) Content Affinity – attitude and interest toward specific material.
(2) Working Memory – the ability to temporarily suspend old information while
simultaneously learning new information. Working memory is the amount
of memory needed to perform a cognitive task, and hindered most by
anxiety.
(3) Executive Functioning – the ability to self-monitor and guide performance on
a given problem solving task. The strategy a student uses to decode words
as well as to organize information in a meaningful manner.
(4) Language Skills – most children enter kindergarten with 3000-5000 words,
though graduate high school with 60,000 words (Pinker,1999). Since
most children do no utter their first word until 12 months of age, that
means the average high school senior has learned 10 new words per day
since their first birthday.
COMPREHENSION
PHONOLOGICAL PROCESSING
FLUENCY
Neuropsychology of Reading Disorders
Page 18
READING COMPREHENSION INTERVENTIONS
(a) Stop and Start technique – the student reads a passage out loud, and every
30 seconds the teacher says “stop” and asks questions about the story.
Eventually the time interval is lengthened.
(b) Directional Questions – ask questions at the beginning of the text instead of
the end so students can become more directional readers.
(c) Story Maps – a pre-reading activity where graphic organizers are used to
outline and organize information prior to reading the text.
(d) Narrative retelling – have the child retell the story after reading it aloud.
(e) Read Aloud – reading out loud allows students to hear their own voices and
can facilitate working memory.
(f) Multiple Exposure – encourage students to skim the material upon reading
for the first time, with emphasis on chapter and text headings. Read for detail
on the second exposure of the text.
(g) Active Participation – encourage active reading by getting children in the
habit of note-taking or putting asterisks next to important material in the text.
(h) Create Questions – have students write their own test questions about the
material.
(i) Reduce Anxiety – anxiety inhibits working memory, and leads to ineffective
recall. Children who are anxious about reading out loud in front of their
classmates should be provided an opportunity to read in a “safety zone” in
class. This may also help to eliminate distractions as well.
(j) Medication Management – often students with attention-deficit-disorder
struggle with passage comprehension skills. Proper medication management
of the disorder can help foster better comprehension.
(k) Practice Terminology – practice defining new terms and concepts prior to
reading material with dense language. Vocabulary enrichment is often the key
to improving comprehension.
(l) Classroom Discussions – introduce new topic areas with general classroom
discussions to capture a student’s attention and interest prior to reading the
material.
(m) Sequencing Tasks – present random words out of sequence and have
children arrange them to make a sentence. Next, present sentences out of
sequence and have children arrange them to make a paragraph. Lastly,
present paragraphs out of sequence, and have children arrange them to make a
story. This type of organization drill will facilitate sequencing linguistic
material.
(n) Increase Fluency – for younger students, greater fluency allows for reading
to become a more automatic process, thereby freeing up cognitive resources to
concentrate on the passage itself, as opposed to mechanically decoding each
word in the passage.
Neuropsychology of Reading Disorders
Page 19
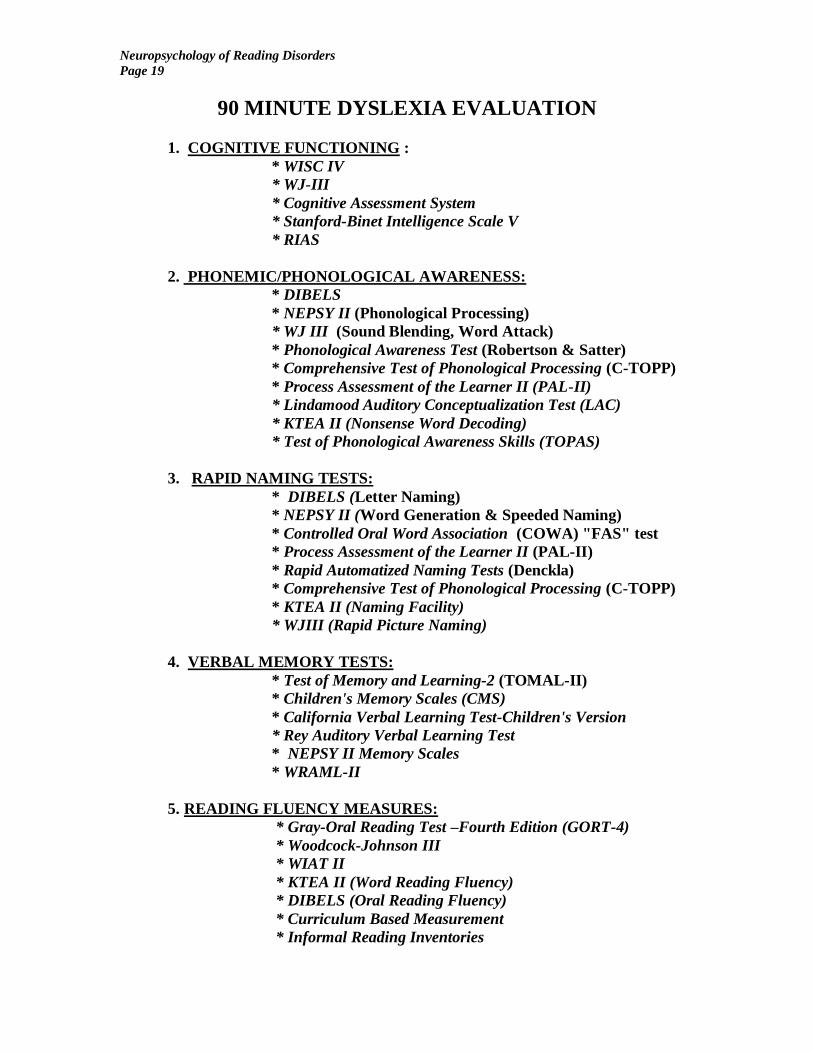
90 MINUTE DYSLEXIA EVALUATION
1. COGNITIVE FUNCTIONING :
* WISC IV
* WJ-III
* Cognitive Assessment System
* Stanford-Binet Intelligence Scale V
* RIAS
2. PHONEMIC/PHONOLOGICAL AWARENESS:
* DIBELS
* NEPSY II (Phonological Processing)
* WJ III (Sound Blending, Word Attack)
* Phonological Awareness Test (Robertson & Satter)
* Comprehensive Test of Phonological Processing (C-TOPP)
* Process Assessment of the Learner II (PAL-II)
* Lindamood Auditory Conceptualization Test (LAC)
* KTEA II (Nonsense Word Decoding)
* Test of Phonological Awareness Skills (TOPAS)
3. RAPID NAMING TESTS:
* DIBELS (Letter Naming)
* NEPSY II (Word Generation & Speeded Naming)
* Controlled Oral Word Association (COWA) "FAS" test
* Process Assessment of the Learner II (PAL-II)
* Rapid Automatized Naming Tests (Denckla)
* Comprehensive Test of Phonological Processing (C-TOPP)
* KTEA II (Naming Facility)
* WJIII (Rapid Picture Naming)
4. VERBAL MEMORY TESTS:
* Test of Memory and Learning-2 (TOMAL-II)
* Children's Memory Scales (CMS)
* California Verbal Learning Test-Children's Version
* Rey Auditory Verbal Learning Test
* NEPSY II Memory Scales
* WRAML-II
5. READING FLUENCY MEASURES:
* Gray-Oral Reading Test –Fourth Edition (GORT-4)
* Woodcock-Johnson III
* WIAT II
* KTEA II (Word Reading Fluency)
* DIBELS (Oral Reading Fluency)
* Curriculum Based Measurement
* Informal Reading Inventories

Neuropsychology of Reading Disorders
Page 20
90 MINUTE DYSLEXIA EVALUATION
6. VISUAL SPATIAL SKILLS:
* NEPSY II(Arrows, Design Copy)
* Jordan Left Right Reversal Test
* Bender Gestalt II
* Beery Visual Motor Integration Test (VMI)
* RIAS (NIX Index)
* Rey-Osterrieth Complex Figure Test
* WJ III (Spatial Relations, Visual Matching)
* SB V (Visual-Spatial Processing)
* KABC II (Gestalt Closure)
7. ATTENTION:
* Tea-CH
* NEPSY II (Auditory Attention and Response Set)
* CAS (Number Detection, Receptive Attention)
* WJIII (Numbers Reversed, Auditory Attention)
* KABC II (Number recall)
* Behavior Scales (ACTers, ADDES, Brown, BASC II,
Conners’)
8. EXECUTIVE FUNCTIONING:
* BRIEF
* Wisconsin Card Sort Test
* Delis-Kaplan Executive Functioning Scale(D-KEFS)
* NEPSY II Subtests
* Category Test
* Stroop Test
* Cognitive Assessment System
9. FAMILY HISTORY:
* Strong Genetic Component
* Chromosome 6 and 15 possible candidates.
* 40% of first degree relatives affected.
* Colorado Twin Study:
70% identical twins
48% fraternal twins

Neuropsychology of Reading Disorders
Page 21
References
Alexander, A. W. & Slinger-Constant, A. M. (2004). Current status of treatments for
dyslexia: A critical review. Journal of Child Neurology, 19 (10), 744-758.
Badian, N.A., McAnulty, G.B., & Duffy, F.H. (1990). Prediction of dyslexia in
kindergarten boys. Annals of Dyslexia, 40, 152-169.
Bakker, D.J. (1992). Neuropsychological classification and treatment of dyslexia. Journal
of Learning Disabilities, 25, 102-109.
Beitchman, J. H. & Young, A. R. (1997). Learning disorders: With a special emphasis on
reading disorders: A review of the past 10 years. Journal of the American Academy
of Child and Adolescent Psychiatry, 36(8), 1020-1030.
Berninger, V.W., & Richards, T.L. (2002). Brain literacy for educators and psychologists.
San Diego, CA: Academic Press.
Byrnes, J. P. (2001). Minds, brains, and learning: Understanding the psychological and
educational relevance of neuroscientific research. New York: Guilford Press.
Chase, C. H. (1996). Neurobiology of learning disabilities. Seminars in Speech and
Language, 17 (3), 173-181.
Corina, D., Richards, T., Serafini, S., Richards, A., Steury, K., Abbott, R., Echelard, D.,
Maravilla, K., & Berninger, V. (2001). fMRI auditory language differences
between dyslexic and able reading children. NeuroReport, 12, 1195-1201.
Demb, J.B., Boynton, G.M., & Heeger, D.J. (1997). Brain activity in visual cortex predicts
individual differences in reading performance. Proceedings from the National
Academy of Science, 94, 13363.
Duara, R., Kushch, A., Gross-Glenn, K., Barker, W.W., Jallad, B., Pascal, S.,
Loewenstein, D.A., Sheldon, J., Rabin, M., Levin, B., & Lubs, H. (1991).
Neuroanatomical differences between dyslexic and normal readers on
magnetic resonance imaging scans. Archives of Neurology, 48, 410-416.
Felton, R.H., Naylor, C.E., & Wood, F.B. (1990). Neuropsychological profile of adult
dyslexic. Brain and Language, 39, 485-497.
Flowers, L. (1993). Brain basis for dyslexia: A summary of work in progress. Journal of
Learning Disabilities, 26, 575-582.
Galaburda, A.M., & Cestnick, L. (2003). Developmental dyslexia. Review of Neurology,
36 (S.3-9).
Galaburda, A.M., Rosen, G.D., & Sherman, G.F. (1990). Individual variability in cortical
organization: Relationship to brain laterality and implications to function.
Neuropsychologia, 28, 529-546.

Neuropsychology of Reading Disorders
Page 22
Geschwind N., & Galaburda, A.M. (1985). Cerebral lateralization: Biological mechanisms,
associations, and pathology: III. A hypothesis and a program for research. Archives
of Neurology, 42, 634-654.
Goldberg, E. (1989). Gradiental approach to neocortical functional organization. Journal
of Clinical and Experimental Neuropsychology, 11, 4, 489-517.
Goldberg, E., & Costa, L. (1981). Hemispheric differences in the acquisition and use of
descriptive systems. Brain and Language, 14, 144-173.
Hynd, G.W., Hall, J., Novey, E.S., Eliopulos, R.T., Black, K., Gonzalez, J.J., Edmonds, J.E.,
Riccio, C., & Cohen, M. (1995). Dyslexia and corpus callosum morphology.
Archives of Neurology, 52, 32-38.
Hynd, G.W., Marshall, R.M., & Clikeman M.S. (1991). Developmental dyslexia,
neurolinguistic theory, and deviations in brain morphology. Reading and Writing:
An Interdisciplinary Journal, 3, 345-362.
Hynd, G.W., & Semrud-Clikeman, M. (1989). Dyslexia and brain morphology.
Psychological Bulletin, 106, 447-482.
Kotulak, R., (1997). Inside the Brain. Kansas City: Andrews McMeel Publishing.
Kolb, B. & Whishaw, I.Q. (1996). Fundamentals of human neuropsychology: fourth
edition. New York: W.H. Freeman and Company.
Lyon, G. R. (1996). Learning Disabilities. The Future of Children: Special Education for
StudentsWith Learning Disabilities, Vol. 6 (1), 54 - 73.
Mather, N. (1992). Whole language reading instruction for students with learning
disabilities: Caught in the cross fire. Learning Disabilities Research and Practice, 7,
87-95.
Moats, L. (2004). Relevance of neuroscience to effective education for students with
Reading and other learning disabilities. Journal of Child Neurology, 19(10), 840-
845.
McCarthy, R.A, & Warrington, E.K. (1990). Cognitive Neuropsychology: A clinical
introduction. New York: Academic Press, Inc.
Ogden, J. (1996). Phonological dyslexia and phonological dysgraphia following left and
right hemispherectomy. Neuropsychologia, 34 (9), 905-918.
Neuropsychology of Reading Disorders
Page 23
Owen, W. J., Borowsky, R., & Sarty, G. E. (2004). FMRI of two measures of
phonological processing in visual word recognition: Ecological validity matters.
Brain and Language, 90, 40- 46.
Paulesu, E., Frith, U., Snowling, M., Gallagher, A.,Morton, J., Frackowiak, R.S.J., Frith, C.
(1996). Is developmental dyslexia a disconnection syndrome? Brain, 119, 143-157.
Pennington, B., Filapek, P., Lefly, D., Churchwell, J., Kennedy, D., Simon, J., Filley, C.,
Gallaburda, A., Alarcon, M., & DeFries, J. (1999). Brain morphometry in reading
disabled twins. Neurology, 53, 723-729.
Pinker, S. (1994). The language instinct: How the mind creates language, New York:
Harper-Collins.
Posner, M.I., & Raichle, M.E. (1994). Images of the mind. New York: W. H. Freeman
Company.
Ridder, W.H., Borting, E., Cooper, M., McNeel, B., & Huang, E. (1997). Not all dyslexics
are created equal. Optometry and Vision Science, 74, 99-104.
Rourke, B.P. & Del Dotto J. (1994) Learning Disabilities: A neuropsychological
perspective. New York: Sage Publications.
Schultze, R.T., Cho, N.K., Staub, L. H., Kier, L.E., Fletcher, J.M., Shaywitz, S.E.,
Shankweler, D.P., Katz, L., Gore, J.C., Duncan, J.S., & Shaywitz, B.A.,(1994).
Brain morphology in normal and dyslexic children: The influence of sex and age.
Annals of Neurology, 35, 732-742.
Shaywitz, S. (1996). Dyslexia. Scientific America, 2-8.
Shaywitz, S. (2003). Overcoming Dyslexia.. New York: Alfred A. Knoff Publishers.
Shinn, M.R. (2002). Best practices in using curriculum-based measurement in a problem-
solving model. In A. Thomas & J. Grimes (Eds.) Best practices in school psychology
IV. Bethesda, Maryland. National Association of School Psychologists.
Siegal, L.S. (1992). An evaluation of the discrepancy definition of dyslexia. Journal of
Learning Disabilities, 25 (10), 618-629.
Stahl, S.M. (2000). Essential Psychopharmacology. New York: Cambridge University
Press.
Stein, J. (2000). The neurobiology of reading difficulties. prostaglandins, leukotrienes
and essential fatty acids, 63, 109 – 116.
Tallal, P., Miller, S., & Fitch, R. H. (1993). Neurobiological basis of speech. A case for the
preeminence of temporal speech. Annals of the New York Academy of Science,
682, 27-47.