the evolving landscape of rural health -...
TRANSCRIPT

Brock Slabach, MPH, FACHE
Senior Vice President for Member Services
National Rural Health Association
May 25, 2016
The Evolving Landscape of Rural Health
Oklahoma Rural Health Conference

Improving the health of the 62 million who call rural America home.
NRHA is non-profit
and non-partisan.

National Rural Health Association Membership

Destination NRHA Plan now to attend these upcoming events.
Quality Clinical Conference – Jul. 13-15, 2016 • Oakland, CA
RHC/CAH Conference – Sept. 20-23, 2016• Kansas City, MO
Policy Institute—February 6-9, 2017• Washington, DC
Annual Conference—May 9-12, 2017• San Diego, CA
Rural Hospital Innovation Summit—May 9-12, 2017• San Diego, CA
Visit RuralHealthWeb.org for details and discounts.
4

A History (short) of Rural Health
• War on Poverty in the 60’s
• Community Health Centers, created in the War on Poverty
• Rural Health Clinics –38 Years Old (1978), 4,100 nationwide
• Result of PPS 1983: 440 hospital closures
• Policy Response 1992-2003:
– State Office of Rural Health (SORH
– Medicare Dependent Hospitals (MDH)
– Critical Access Hospital (CAH) 1997
– Medicare Rural Flexibility Program (1997)
– Low-Volume Hospital (LVH) Adjustment (2003 and 2010)
• Patient Protection and Affordable Care Act (ACA) 2010
• Medicare Access and Chip Reauthorization Act (MACRA) 2015


Rural Hospital Closures: 1983-97

We’re not finished yet…
Rural differentiation:
“Rural Americans are older, poorer and sicker than their urban
counterparts… Rural areas have higher rates of poverty,
chronic disease, and uninsured and underinsured, and millions
of rural Americans have limited access to a primary care
provider.” (HHS, 2011)
Disparities are compounded if you are a senior or minority in rural America

We’re not finished yet…
Health Equates to Wealth:
People who live in wealthy areas like San Francisco,
Colorado, or the suburbs of Washington, D.C. are likely to be
as healthy as their counterparts in Switzerland or Japan, but
those who live in Appalachia or the rural South are likely to be
as unhealthy as people in Algeria or Bangladesh.
--University of Washington, July, 2013
Rural counties have the highest rates of premature death, lagging
far behind other counties, RWJF Report, March, 2016
Rural counties have had the highest rates of premature death for many
years, lagging far behind other counties. While urban counties continue to
show improvement, premature death rates are worsening in rural counties.

18 have closed in 2015, Already Ten closed in 2016
CLOSED
Closure Analysis
• Most closures in South
• Annual number of closures increasing
• Most are CAHs and PPS hospitals (vs MDH and
SCH)
• Most are in states that have not expanded Medicaid
• Patients in affected communities are probably
traveling between 5 and 28 more miles to access
inpatient care
• Most hospitals closed because of financial problems --Sheps Center for Rural Health, University of
North Carolina, 2016

2015 Rural Hospital Financial Status
Rural Hospital Financial Status
Provider Type Profitable Switch Unprofitable Total
CAH 358 27 917 1302
Medicare
Dependent
54 7 138 199
Sole Community 94 2 156 252
Standard Rural
PPS
52 1 101 154
1312 1907 69%
Source: iVantage Health Analytics

Rural Hospital Closures and Risk of Closures
35% Percent Vulnerable X
73
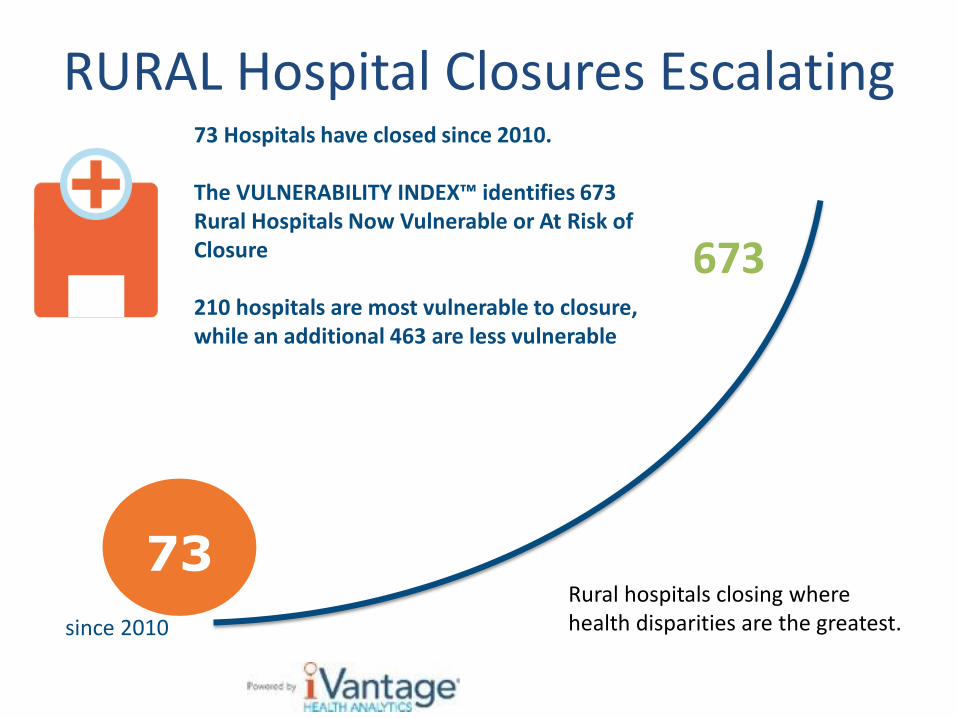
73 Hospitals have closed since 2010. The VULNERABILITY INDEX™ identifies 673 Rural Hospitals Now Vulnerable or At Risk of Closure 210 hospitals are most vulnerable to closure, while an additional 463 are less vulnerable
RURAL Hospital Closures Escalating
673
since 2010
73 Rural hospitals closing where health disparities are the greatest.

Rural Hospital Closures on the RiseThe rate of closure is six times higher in 2015 than in 2010
0
5
10
15
20
25
2010 2011 2012 2013 2014 2015 2016 2017
ClosuresAt this rate, 25% of rural hospitals will shut down in
less than 10 years .

The Impact of Rural Hospital Closures
The Vulnerability Index™ identifies 673 rural hospitals statistically
clustered in the bottom 2 tiers of performance.
673
NRHA Analysis of Rural Hospitals
Target solutions for three cohorts of rural hospitals:
• At high-risk of closure (n=210)
• Stable with strategically sound fundamentals
(n=1,437)
• High-performers or first movers (n=208)

Impact of Sequestration
7,200 jobs lost in rural hospitals and
communities (sustained over 10
years)
30 rural hospitals shifting from
profitable to unprofitable
-0.6% off the bottom line
$2.8 billion lost in rural Medicare
reimbursement (over 10 years)
2% cut

Impact of cuts in Bad Debt Reimbursement
2,000 rural healthcare jobs lost
$5.3 billion loss to GDP
(over 10 years)
2,600 rural community jobs lost
$1 billion lost in bad debt reimbursement
(over 10 years)
35% cut

Save Rural Hospitals Act, HR 3225
Rural hospital stabilization (Stop the bleeding)
Elimination of Medicare Sequestration for rural hospitals;
Reversal of all “bad debt” reimbursement cuts (Middle Class Tax Relief and Job Creation Act of 2012);
Permanent extension of current Low-Volume and Medicare Dependent Hospital payment levels;
Reinstatement of Sole Community Hospital “Hold Harmless” payments;
Extension of Medicaid primary care payments;
Elimination of Medicare and Medicaid DSH payment reductions; and
Establishment of Meaningful Use support payments for rural facilities struggling.
Permanent extension of the rural ambulance and super-rural ambulance payment.
Rural Medicare beneficiary equity. Eliminate higher out-of pocket charges for rural patients (total charges vs. allowed Medicare charges.)
Regulatory Relief
Elimination of the CAH 96-Hour Condition of Payment (See Critical Access Hospital Relief Act of 2014);
Rebase of supervision requirements for outpatient therapy services at CAHs and rural PPS See PARTS Act);
Modification to 2-Midnight Rule and RAC audit and appeals process.
Future of rural health care (Bridge to the Future)
Innovation model for rural hospitals who continue to struggle.

Future Model:
Community Outpatient Hospital
• 24/7 emergency Services
• Flexibility to Meet the Needs of Your Community
through Outpatient Care: • Meet Needs of Your Community through a Community Needs
Assessment:
• Rural Health Clinic
• FFQHC look-a-like
• Swing beds
• No preclusions to home health, skilled nursing, infusions services
observation care.
• TELEHEALTH SERVICES AS REASONABLE COSTS.—For
purposes of this subsection, with respect to qualified outpatient services,
costs reasonably associated with having a backup physician available via
a telecommunications system shall be considered reasonable costs.”.
• “The amount of
payment for
qualified
outpatient
services is equal
to 105 percent of
the reasonable
costs of providing
such services.”
• $50 million in
wrap-around
population health
grants.
New Grants Available to CAHs
and Rural PPS Hospitals
• $12 million appropriated annually for Quality
Improvement and Compliance Grants.
• $15 million appropriated annually for rural
population health needs.
• $ 2 MILLION EMS GRANT FUNDING — to develop
EMS programs to meet community needs,
address workforce and funding problems.
• For COHs - $50 million in grant funding.

Rep. Sam Graves (R-MO) – 7-27-15 Rep Abraham, Ralph Lee [LA-5] - 11/18/2015 Rep Bustos, Cheri [IL-17] - 2/9/2016 Rep Clarke, Yvette D. [NY-9] - 1/5/2016 Rep Conaway, K. Michael [TX-11] - 2/12/2016 Rep Cramer, Kevin [ND] - 12/7/2015 Rep Farenthold, Blake [TX-27] - 11/16/2015 Rep Grothman, Glenn [WI-6] - 9/9/2015 Rep Harper, Gregg [MS-3] - 2/1/2016 Rep Hastings, Alcee L. [FL-20] - 10/28/2015 Rep Hinojosa, Ruben [TX-15] - 11/30/2015 Rep Huffman, Jared [CA-2] - 12/1/2015 Rep Kind, Ron [WI-3] - 10/2/2015 Rep Kirkpatrick, Ann [AZ-1] - 11/5/2015 Rep Loebsack, David [IA-2] - 7/27/2015 Rep Lucas, Frank D. [OK-3] - 2/3/2016 Rep Neugebauer, Randy [TX-19] - 11/16/2015 Rep Peterson, Collin C. [MN-7] - 10/22/2015 Rep Pocan, Mark [WI-2] - 11/16/2015 Rep Ribble, Reid J. [WI-8] - 11/17/2015 Rep Stewart, Chris [UT-2] - 9/28/2015 Rep Stivers, Steve [OH-15] - 2/11/2016 Rep Takai, Mark [HI-1] - 2/3/2016 Rep Thompson, Glenn [PA-5] - 2/23/2016 Rep Thornberry, Mac [TX-13] - 10/8/2015 Rep Walz, Timothy J. [MN-1] - 11/18/2015 Rep Williams, Roger [TX-25] - 12/3/2015 Rep Young, David [IA-3] - 9/30/2015

UNC Research Projects
• Prediction of Financial Distress among Rural Hospitals
• Geographic Variation in Risk of Financial Distress among Rural Hospitals
• CAH Financial Indicators Report: Summary of Indicator Medians by State

Under Pressure…
Threats of more cuts and current issues…
• Helping Hospitals Improve Patient Care Act (H.R. 5273): SES and REACH
• OIG Challenges • Necessary Provider Report
• Swing Bed Report
• CMS Challenges • Exclusive Use of Provider-Based Clinics
• Re-certification Requirements for CAHs
• Opioid and Heroin Crisis
• MedPAC June Rural Report
• ACA Update
• JAMA Article on Rural Surgery
• EHR Meaningful Use

MedPAC upcoming report
Preserving access to emergency care in rural areas
(Jeff Stensland, Zach Gaumer)
• MedPAC will promote new model for rural communities
• Big change in MedPAC approach
• 24/7 emergency care services will be provided
Concerns: sustainability.
• Likely will be PPS reimbursement (with small grant)
• No cost-based funding
• Significantly limit the number of facilities to qualify
• MedPAC failed to notice that the negative 9% Medicare margins are impacting rural hospitals (blamed volume)

Is ACA Working?
CDC May 17, 2016: U.S. Uninsured Rate at 9.10%, Lowest in Eight-Year Trend
But let’s dive in closer…
“More than 1 million ObamaCare exchange customers have likely dropped out since open enrollment, Feb. 1”
State Case in Study: Colorado
• Colorado: Number of paying individuals has dropped 23% this year from last (150,769 to 115,890). Why?
• Co-Op failure - - covered 69,000 lives
• Premium increases Rate Hikes - Customers who don’t qualify for subsidies are paying 34% more for catastrophic and 21% for bronze
• Rather pay the penalty.

Opioid Crisis in Rural American
All states have demonstrated an increase in nonmedical prescription opioid
mortality during the past decade, however, the largest areas of abuse are
concentrated in states with large rural populations, such as Kentucky, West
Virginia, Alaska, and Oklahoma.

Rural Health Clinics (RHC)
• HCPCS Codes on RHC Claims April 1, 2016
• First Qualifying Visit List (QVL) was limited
• Second QVL was expanded to include a broad list of
procedure only codes…unable to bill procedures on
this list until October 1, 2016
• Stay tuned…the drama continues
• Don’t Forget: Annual Wellness Visits and Chronic
Care Management Reimbursement—Let us know of
billing issues on these codes
• Transforming Clinical Practice Initiative (TCPI): have
you joined a Practice Transformation Network
(PTN)?

CMS Star Rating Program
• CMS to allow 30 day preview of the July update starting May
6, 2016. Click here for link to see your hospital’s Star Rating.
Star
Rating
Number of hospitals
(percent of hospitals rated)
One Star 142 (4%)
Two Star 716 (20 %)
Three Star 1881 (52%)
Four Star 821 (23%)
Five Star 87 (2%)
Total Hospitals in Hospital Compare Data Set: 4604
Met Reporting Threshold: 3647 (79%)
Did not meet reporting threshold: 957 (21%)

CMS Star Rating System
Outcome Measures Process of Care Measures
Mortality (N=7, 22%
weight)
Safety of Care (N=8,
22% weight)
Readmissions (N=8,
22% weight)
Effectiveness of Care (N= 16, 4%
weight)
Timeliness of Care (N=7 , 4% weight)
Patient Experience (N=11, 22%
weight)
Efficient Use of Medical Imaging
(N=5, 4% weight)
To meet the minimum threshold to have a star rating calculated
hospitals must have at least three measures, in at least three groups,
with at least one outcome group.

CMS Star Rating System
“The idea that dying and being readmitted to
the hospital are equally important to patients
seems funny to me,”
Ashish Jha, M.D.
Harvard Medical School
JAMA Article on Rural Surgery
• Journal of the American Medical Association (JAMA) Released
May 17, 2016
• Conclusions and Relevance:
Among Medicare beneficiaries undergoing common
surgical procedures, patients admitted to critical access
hospitals compared with non–critical access hospitals had
no significant difference in 30-day mortality rates,
decreased risk-adjusted serious complication rates, and
lower-adjusted Medicare expenditures, but were less
medically complex.

Senate Bill on EHR
Meaningful Use
• NRHA Supported Legislation introduced by Sens.
Thune and Alexander
• Provisions:
• Remove all or nothing approach to meaningful
use
• Set a 75% threshold for meeting objectives and
measures
• 90 Reporting Period in 2016 and later years
• Flexibility in applying hardship exceptions

• MACRA – MIPS and APMs • CMS Quality Measure Development Plan – NRHA Comments Submitted March 1
• Regulations expected around May (rule must be finalized by November 1)
• Healthcare Payment Learning & Action Network (HPCLAN) – NRHA Comments submitted March 7
• Patient Attribution
• Financial Benchmarking
• ACO – benchmarking regulation – comments were due March 28
• IPPS Rule 2016—NRHA Preparing Comment Letter • Two-midnight changes
• Medicare outpatient observation notice (MOON) requirements
• Next slide
Regulatory Update

Notification Procedures for
Outpatient Observation
• Implements the NOTICE Act effective August 6, 2016 for all
hospitals and CAHs as a condition of participation.
• Standardized written notice called the Medicare Outpatient
Observation Notice (MOON) explaining:
• the individual was an outpatient—not an inpatient
• the reason for outpatient status (i.e., the individual doesn’t currently need
inpatient services but requires observation to decide whether to admit or
discharge)
• the implications of receiving observation services as an outpatient (i.e.
cost-sharing and eligibility for skilled nursing facility care)
• Provide the explanations in plain language Include a blank for
additional information
• Include a dedicated signature area to acknowledge
receipt and understanding of the notice

Rural Innovation
Volume to Results: A major leap
Transformation to Population
Health Management
Novelty Trending Reality 2011 2013 2016

40
Payment Framework

41
2016
30%
85%
2018
50%
90%
Target percentage of payments in ‘FFS linked to quality’ and ‘alternative payment models’ by 2016 and 2018
2014
~20%
>80%
2011
0%
~70%
Goals Historical Performance
All Medicare FFS (Categories 1-4)
FFS linked to quality (Categories 2-4)
Alternative payment models (Categories 3-4)

MACRA of 2015: Quality
Payment Program
Incentivizes movement to alternative payment models
(APM) or Participate in MIPS
• APMs • Patient Centered Medical Homes
• Accountable Care Organizations
• Bundled Payments
• Episodes of Care
• Yet to be Invented
• Revenue Requirements • 2018-19 25% of Physician Revenues through APMs
• Receive 5% Fee Schedule Bonus
• Revenue threshold increases each year

MACRA of 2015: Quality
Payment Program
Merit-based Incentive Payment System (MIPS)
• Minimal FFS yearly increase next 10 years of 0.5%, then
0%
• MIPS (eventually -4% to +27% adjustment)—Based on
quality, resource use and clinical practice improvement
activities
• 41% payment difference between highest and lowest
performing physicians

44
The Health Care Payment Learning and Action Network (LAN) was launched to accelerate adoption and align methods of APMs
Medicare alone cannot drive sustained progress towards alternative payment models (APM)
Success depends upon a critical mass of partners adopting new models
More than 50 organizations have committed support, including AARP, Anthem, Humana, National Partnership for Women & Families, Partners Healthcare, Rite Aid, Walgreens, Walmart, States of MA and NY
Network Objectives
• Match or exceed Medicare alternative payment model goals across the US health system
-30% in APM by 2016 -50% in APM by 2018
• Shift momentum from CMS
to private payer/purchaser and state communities
• Align on core aspects of alternative payment design
4,800 registered participants + {
{

Work and Affinity Groups
Work Groups:
• APM Framework
• Clinical Episode Payments
• Population Based Payments
• Payment Reform Evaluation Hub
Affinity Groups:
• Consumer and Patient
• Purchasers/Employers
• State Engagement Group
NRHA Request:
• Rural Affinity Group

46
LAN Communications
https://publish.mitre.org/hcplan
Join work group affiliated communities to provide input on work group products [email protected] http://innovationgov.force.com/hcplan
Visit the LAN website to learn more and find resources

NRHA APM/DSR SIG
Alternative Payment Model/Delivery System Reform Special
Interest Group
• Leadership Team meets to review published rules and white
papers from the HCPLAN
• Daylong preconference at NRHAs Policy Institute
• Innovation Summit in Minneapolis May 10-13, 2016
• Dedicated APM/DSR Track at RHC/CAH Sept. 20-23, 2016
• Committed to spreading best practices on innovation

CMS RFI on Global Budgeting
Request for Information (RFI) from the Centers for Medicare and Medicaid Services Innovation (CMMI) Center:
• Population Health
• Next Generation Rural Payments: What’s after ACOs?
• Focused on Global Budgeting
• Submissions Were Due May 13, 2016
• NRHAs APM/DSR SIG Leadership Team drafted a response

49
Counties are ranked within states and split into quartiles with equal numbers of counties in each quartile

Adult Obesity Population View
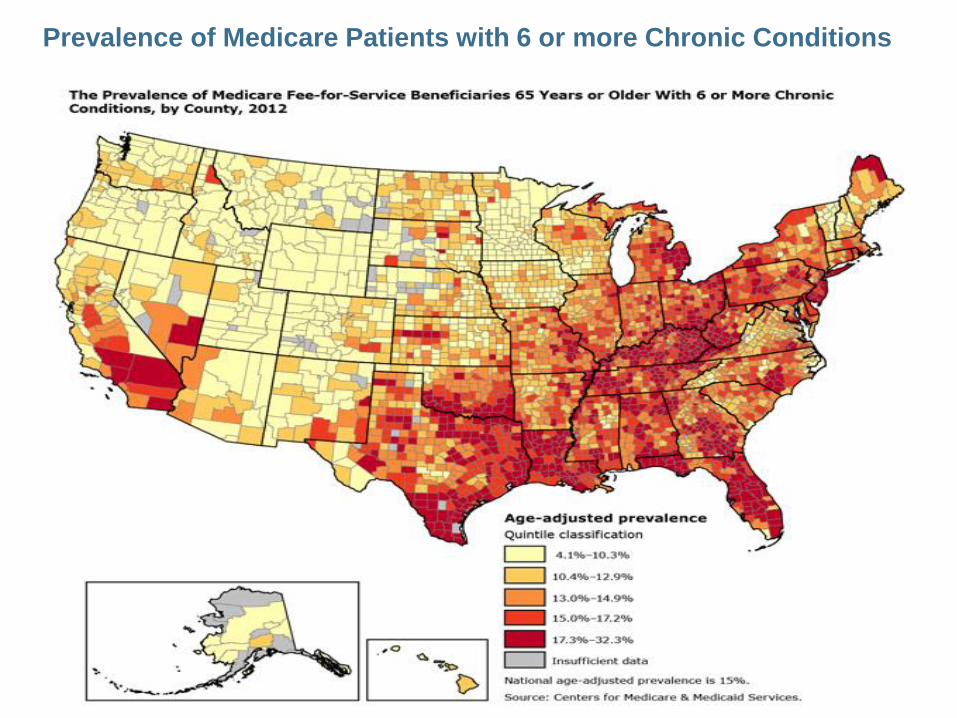
Prevalence of Medicare Patients with 6 or more Chronic Conditions

Chronic Disease
Growth Projections
Source: State of Healthcare 2010

53
County
Health
Rankings
Model

First Things First
Care Redesign
• PCMH
• Clinical Integration
• Care Management
• Post-acute Care
• EHR
• Data Analytics
Care redesign should not outpace
Changes in payment
New Payment Arrangements
• Care Transformation Costs
• Care Management Payments
• Shared Savings
• Episodes of Care Payments
• Global Payments
Population
Health
Transformation

Brock Slabach, MPH, FACHE
Senior Vice President for Member Services
National Rural Health Association
T H A N K Y O U