the environment by joseph d. brain*
TRANSCRIPT

Environmental Health PerspectivesVol 20,pp. 113-126, 1977
The Respiratory Tract and
the Environment
by Joseph D. Brain*
The primary determinants of pulmonary disease are environmental. The same thinness and delicacy ofthe air-blood barrier which allows rapid exchange of oxygen and carbon dioxide also reduce its effective-ness as a barrier to inhaled allergens, carcinogens, toxic particles, and noxious gases, and micro-
organisms. Adults breathe 10,000 to 20,000 liters of air daily. This volume of air contains potentiallyhazardous contaminating particles and gases. Future research should explore the diverse physiologicalmechanisms which prevent the accumulation and deleterious action of inhaled particles and gases. Sincemost pulmonary diseases are either initiated by or at least aggravated by the inhalation of particles andgases, the role of environmental factors in the development of respiratory disease is an area worthy ofcondnued support.
Functions of the RespiratorySystemHuman beings cannot live without producing ade-
quate amounts of energy, which is produced by ox-
idizing the organic molecules in food. Thus the con-
sumption of oxygen and the production of carbondioxide, a waste product of ATP synthesis, are in-dispensable to life. It follows that the human bodymust have an organ designed to exchange carbondioxide and oxygen between the circulating bloodand the atmosphere in sufficient volumes to sustainlife. Within the lungs are hundreds of millions ofalveoli which form a surface of approximately70 M2. Blood flowing through the lungs comes
within 1 am of gas contained in the alveoli. How-ever, the respiratory tract is faced with conflictingdemands. It must be an efficient organ of gas ex-
change, but it must also create a protective barrierwhich effectively excludes unwanted, harmfulagents.Three processes are essential for the transfer of
oxygen from outside air to the blood flowingthrough the lung: (1) ventilation, (2) perfusion, and(3) diffusion within the air spaces and across theair-blood barrier. Ventilation is the tidal process inwhich air is moved in bulk between the atmosphere
*Department of Physiology, Harvard School of PublicHealth, Boston, Massachusetts 02115.
and the lung. Perfusion is the action of the car-diovascular system in pumping blood throughoutthe lungs. Diffusion is the passive movement ofgases down a concentration gradient between thealveolar gas and pulmonary capillary blood.
In order to deliver the inhaled gas to the alveolarsurface uniformly, the lung has an elaborate dis-tribution system. After moving through the nasalcavity or through the mouth, air reaches the throator pharynx. Unless swallowing occurs, the epiglot-tis does not cover the larynx, and the gas passesthrough the larynx into the trachea. The tracheabranches into left and right bronchi, which branchrepeatedly until the alveoli are reached.Movement of air into the lungs is caused by the
action of the respiratory muscles which expand thechest wall so that the lungs till passively. At the endof a normal expiration, a large amount of gas re-mains in the lungs. Both the rate at which breathingoccurs (respiratory frequency) and the amount ofair coming in with each breath (tidal volume) arevariable and can be altered to match metabolic de-mands. The ventilation rate is adjusted by the brainto keep the concentration of oxygen and carbondioxide in the alveoli relatively constant.Although ventilation is essential, gas exchange
does not occur unless blood is uniformly distributedthroughout the lungs. The right side of the heartpumps venous blood which is high in carbon diox-ide and low in oxygen. The pulmonary blood ves-sels are highly branched, and a thin film of blood is
October 1977 113

spread just beneath the alveolar surface.The third requirement for gas exchange in the
lungs is diffusion. Diffusion is very effective oversmall distances. In the alveoli, the blood is sepa-rated from the air by two specialized layers of cells,which together are less than I Am thick. The gas-exchange capability of the lungs must be linked tothe needs of the whole body by means of the cir-culatory system and by the unique properties of theblood.
During the last decade, it has become obviousthat the lung also has many nonrespiratory func-tions; for example, the endocrine function of thepulmonary circulation has been emphasized. Thelungs metabolize vasoactive substances and may beinvolved in such complex humoral processes asblood pressure homeostasis. The endothelial cellsin the lung alter bradykinin, angiotensin-l, andprostaglandins of the E and F series. Preliminaryevidence also suggests that the lung may synthesizeprostaglandins E2, F2a, G2, and H2. Too few studiesinvolving the uptake and release of pharmacologicsubstances in the lung have been conducted onhuman beings, although there is substantial infor-mation from animal experiments.
The Lung as a Portal of Entry:Pathways of Toxic Materials fromthe Outer to the InnerEnvironmentThe respiratory tract is the most common route
of entry for toxic particles present in the work envi-ronment and the inhalation of particles in pollutedair by the general population is also of great con-cern. Furthermore, the major portal of entry forinfectious particles is the respiratory tract; inhaledparticles from tobacco smoke now represent themost important cause of emphysema, bronchitis,and lung cancer. This section briefly summarizesthe nature of particle deposition and clearance inthe respiratory tract. These principles have broadapplication to both toxic and therapeutic aerosolswhich are inhaled. Excellent reviews of this areaare readily available (1-3).
Deposition is the process that determines whatfraction of the inspired particulates will be caught inthe respiratory tract and thus fail to exit with theexpired air. It is likely that all particles deposit aftertouching a surface; thus the site of initial depositionis the site of contact. Distinct physical mechanismsoperate on particles suspended in the inspired air,causing them to move towards the surface of therespiratory tract: inertial forces, sedimentation,Brownian diffusion, interception, and electrostatic
forces.Inertia is the tendency of moving particles to
resist changes in direction and speed. Repeatedbreathing in the airways causes sudden changes inthe direction of air flow. However, because of in-ertia, particles tend to continue in their original di-rection, crossing air-flow streamlines and eventu-ally making contact with the airway walls. Gravityaccelerates falling bodies downward, and terminalsettling velocity is reached when viscous resistiveforces are equal and opposite in direction to gravita-tional forces. Respirable particles reach this con-stant terminal or sedimentation velocity in less than0.1 msec. Thus, particles are also removed as theirterminal velocity causes them to strike the airwaywalls or alveolar surfaces. Aerosol particles alsoundergo Brownian diffusion, a motion caused bycollisions of gas molecules with particles suspendedin the air. This motion causes the particles to crossstreamlines and thus increases the probability thatthey will deposit.The effectiveness of these deposition
mechanisms depends on: (1) the anatomy of the res-piratory tract, (2) the effective aerodynamicdiameters of the particles, and (3) the pattern ofbreathing. These factors determine the fraction ofthe inhaled particles that are deposited as well asthe site of deposition.The anatomy of the respiratory tract is important
since it is necessary to know the diameters of theairways, the frequency and angles of branching, andthe average distances to the alveolar walls. Fur-thermore, when considered with the volumetricflow rate, airway anatomy specifies the local linearvelocity of the air stream and the character of theflow as a significant change in the effective anatomyof the respiratory tract occurs when there is aswitch between nose and mouth breathing. Thereare inter- and intraspecies differences in lungmorphometry; even within the same individual, thedimensions of the respiratory tract vary with chang-ing lung volume, aging and pathological processes.The effective aerodynamic diameters of the par-
ticles affect the magnitude of forces acting on them.For example, while inertial and gravitational effectsincrease with increasing particle size, diffusion pro-duces larger displacements as particle size de-creases. This effective aerodynamic diameter is afunction of particle size, shape, and density. Hy-groscopic properties may also alter particle size bothwithin and without the respiratory tract. In order topredict deposition patterns, it is essential to de-scribe both the distribution and the mean ofaerodynamic diameters.The remaining factor affecting deposition is the
breathing pattern. Minute volume defines the aver-
Environmental Health Perspectives114
age flow velocity of the aerosol-containing air in thelung and the total number of particulates to whichthe lung will be exposed. Respiratory frequencywill affect the residence time of aerosols in the lungsand hence the probability of deposition by gravita-tional and diffusional forces. Changing lung volumewill alter the dimensions of the airways and paren-chyma.
Despite continuous exposure of the lung to par-ticulates characteristic of occupational and urbanenvironments, the surfaces of the respiratory tractare relatively free of foreign matter. Even the dis-eased and blackened lungs of miners who succumbto coal workers' pneumoconiosis, contain less than10% of the dust originally deposited there. Even inlungs seriously compromised by disease, the res-piratory system is still surprisingly efficient atcleaning itself. The healthy lung exhibits evengreater potency in the pursuit of cleanliness. This isthe result of a complex system of respiratory de-fense mechanisms which both prevents particleentry and removes particles that have been depo-sited. Clearance refers to the dynamic processesthat remove particulates from the respiratory tract;it is the output of particulates previously deposited.Highly soluble particles and gases dissolve rapidlyand are absorbed into the blood from the respira-tory tract. Their metabolism and excretion resemblethat of an intravenously injected dose of the samematerial.
Less soluble particles that deposited on themucus blanket covering pulmonary airways aremoved toward the pharynx by the cilia. Also pres-ent in this moving carpet of mucus are cells andparticles which have been transported from the non-ciliated alveoli to the ciliated airways. Similarly,particles deposited on the ciliated mucus mem-branes of the nose are propelled toward thepharynx. There, mucus, cells, and debris comingfrom the nasal cavities and the lungs meet, mix withsalivary secretions, and enter the gastrointestinaltract after being swallowed. Since the particles areremoved with half-times of minutes to hours, thereis little time for solubilization of slowly dissolvingmaterials. In contrast, particles deposited in thenonciliated compartments have much longer resi-dence times; there, small differences in in vivosolubility can have great significance.A number of factors can affect the speed of
mucus flow. They may be divided into twocategories: those affecting the cilia themselves andthose affecting the properties of the mucus. Thefollowing aspects of ciliary action may be affectedby environmental insult: the number of strokes perminute, the amplitude of each stroke, the timecourse and form of each stroke, the length of the
cilia, the ratio of ciliated to nonciliated area, and thesusceptibility of the cilia to intrinsic and extrinsicagents that modify their rate and quality of motion.The characteristics of the mucus are frequentlyeven more critical. The thickness of the mucuslayer and its rheological properties may undergowide variations.Many studies reported in the literature do not
characterize ciliary motility and the quantity of themucus separately. In most cases the interaction ofthe two processes, mucus transport, is the variablethat is measured. Most evidence suggests thatmucus secretion is a more sensitive process than isciliary activity. In many instances the quantity andrheological characteristics of the polymeric gelwhich constitutes mucus may be affected indepen-dently of any change in the cilia.Macrophages are usually credited with keeping
the alveolar surfaces clean and sterile. Alveolarmacrophages are large, mononuclear, phagocyticcells found on the alveolar surface. They do notform part of the continuous epithelial layer, whichis made up of pulmonary surface epithelial cells(type I pneumonocytes) and great alveolar cells(type II pneumonocytes). Rather, the alveolar ma-crophages rest on this lining. These cells are largelyresponsible for the normal sterility of the lung (4). Itis the phagocytic and lytic potential of the alveolarmacrophages that provides most of the known bac-tericidal properties of the lungs. Like other phago-cytes, alveolar macrophages are rich in lysosomes.The lysosomes attach themselves to thephagosomal membrane surrounding the ingestedpathogen. Then the lysosomal membranes becomecontinuous with the phagosomal membrane and thelytic enzymes kill and digest the bacteria. Amongthe hydrolases they are known to contain are pro-teases, deoxyribonuclease, ribonuclease, f3-glu-curonidase, and acid phosphatase. Although theseenzymes constitute an important aspect of thelung's defensive posture, when kept in a chronicallyactivated state, this digestive capacity may serve todamage pulmonary tissues. Release of lysosomalenzymes, particularly proteases, from activatedmacrophages and leukocytes may be involved in thedevelopment of emphysema. Release may occur asa consequence of cell death, cell injury, or exocyto-sis. Increased deposition of inert or infectiousparticles acts to recruit additional macrophages andthus the effect may be reinforced.Hence, our concern is also directed toward their
ability to ingest nonliving, insoluble dust and de-bris. Rapid endocytosis of insoluble particles pre-vents particle penetration through the alveolarepithelia and facilitates alveolar-bronchiolar trans-port. Schiller (5) and later Sorokin and Brain (6)
October 1977 115

found little evidence that macrophages laden withdusts can re-enter the alveolar wall; only free parti-cles appear to penetrate. Thus phagocytosis playsan important role in the prevention of the entry ofparticles into the fixed tissues of the lung. Onceparticles leave the alveolar surface and penetratethe tissues subjacent to the air-liquid interface (typeI and II cells, interstitial and lymphatic tissues),their removal is slowed. Particles remaining on thesurface are cleared with a biological half-time esti-mated to be twenty-four hours in humans, whileparticles that have penetrated into "fixed" tissuesare cleared with half-times ranging from a few daysto thousands of days. Therefore, the probability ofparticle penetration is critical in determining theclearance of particles from the non-ciliated regionsof the lungs.
Pathological processes, such as fibrosis, may alsoimpair particle clearance from these compartments.The probability of particle entry into a fixed tissuein which it would have a long biological half-time isreduced if the particle is phagocytized by a free cell.Therefore endocytosis emerges as a central themeof macrophage activity and the ability to quantitateendocytosis and to study variations in the rate ofendocytosis are essential to our understanding ofrespiratory defense mechanisms. Only then can therole of differing environmental conditions on en-docytosis be understood. Endocytosis has beenmuch studied, but most techniques which are avail-able measure phagocytosis in vitro. Attempts toquantitate phagocytosis in vivAo are considerablyless frequent. Hepatic macrophages have beenstudied as the major component of the reticuloen-dothelial system and the rate of disappearance ofvarious particulate materials from the circulation iswell described. In contrast, the rate at whichphagocytosis occurs in the living lung is not wellestablished. Serial sacrifice and visual observationcan give some clues, but other techniques to esti-mate endocytosis in vivo must be created.
During the last few years, it has become increas-ingly obvious that not all pulmonary macrophagesare alveolar macrophages. Another important sub-division of pulmonary macrophages is the airwaymacrophage. These mononuclear cells are presentin the conducting airways, both of large and smallcaliber. They may be present as passengers on themucus escalator, or they may be found beneath themucus lining, apparently adhering to the bronchialepithelium. These airway macrophages probablyrepresent the result of alveolar-bronchiolar trans-port of alveolar macrophages, although it has beensuggested that they are the product of direct migra-tion of cells through the bronchial epithelium.The third subdivision of pulmonary macrophages
is interstitial macrophages found in the variousconnective tissue compartments in the lung. Theseinclude alveolar walls, sinuses of the lymph nodesand nodules, and peribronchial and perivascularspaces. Conn,ective tissue macrophages have beenconsidered in some detail by Sorokin and Brain (6).All pulmonary macrophages are usually consideredto be relatives of monocytes and macrophagesthroughout the body. This extended family includesthe Kupffer cells of the liver, the free and fixed ma-crophages in the spleen, lymph nodes, bone marrow,the peritoneal macrophage of the serous cavity, andthe osteoclasts of bone.A major aspect of macrophage function of great
importance to environmental health is the fate ofthe pulmonary macrophage. Differences existamong the varying classes of pulmonary macro-phages and their fate must be considered sepa-rately. Although little is known about the latterstages of the life of the alveolar macrophage, thepossibilities are finite and easily enumerated.They may be subject to alveolar-bronchiolar trans-port mechanisms; they may enter the lymphatics orconnective tissue; or they may enter the circulation.Finally, it is also possible that some never leave thealveolar surface but persist for long periods of time,die there, and are then ingested and digested byyounger, more vigorous siblings.There is speculation about the mechanisms re-
sponsible for alveolar-bronchiolar transport but lit-tle supporting evidence exists. We do know thatmost particles deposited in alveoli are ingested byalveolar macrophages. Some of these cells find theirway to the bronchioles, and are then carried to thepharynx by ciliary action. Migration through alveo-lar pores, or other collateral pathways between ad-jacent bronchial paths cannot be excluded. How-ever, almost all of the macrophages are located onthe surfaces of alveoli or bronchi. Thus, it seemsunlikely that macrophages migrate to the bron-chioles by penetrating between alveolar cells or byemerging from lymphatic pathways.
Since some macrophages find their way to air-ways, we must ask how these cells move to themucus escalator. It is possible that macrophagesexhibit directed locomotion because of a concentra-tion gradient of a chemotactic factor. Thephenomenon of chemotaxis is well studied in vitro.This is particularly true for neutrophils, thoughmuch less so for macrophages. Little is knownabout the chemotactic behavior of alveolar ma-crophages and no observations of alveolar ma-crophage movement in situ have been made. Thereis also no evidence to suggest that other tropisms,such as geotropism, account for a purposeful mi-gration of macrophages. Little direct experimental
Environmental Health Perspectives116

evidence suggests that the fluid lining of the alveolarregion moves mouthward, but many investigatorsassume that it does.The direct entry of alveolar macrophages into
lymphatic pathways and connective tissue has oftenbeen suggested but rarely proved. The presence ofparticle-containing macrophages in these compart-ments is compelling evidence for manyinvestigators. However, the entry of alveolarmacrophages on the one hand and the entry of bareparticles which are subsequently ingested by con-nective tissue macrophages already present on theother cannot be readily distinguished. During alveo-lar clearance, some noningested particles may fol-low lymphatic or vascular channels from alveoliinto the peribronchial, perivascular, or subpleuraladventitiae and thus penetrate into the connectivetissue of the lung. They are then stored by residentmacrophages already present. This pathway may bemore common when conditions favor increasedlymphatic permeability (pulmonary edema). Then agreater number of particles might pass into thesevessels through clefts between endothelial cells, tobe carried along lymphatic drainage paths until fil-tered out by macrophages located farther along inlymphoid foci. Although inhaled particles can befound in connective tissue macrophages, we areaware of little evidence that implicates movementof surface macrophages into connective tissuecompartments. We cannot, however, totally ex-clude this possibility, however uncommon it may be.Yet such penetration may be of consequence to en-vironmental immunological lung disease since it pro-vides a pathway for antigens in or on alveolar mac-rophages to meet reactive lymphocytes in the con-nective tissue.When we consider the fate of airway macro-
phages, we should not assume that the particle-containing mononuclear cells in the airways arenecessarily the product of alveolar-bronchiolartransport. Some may be, but others may derivefrom blood monocytes which have migrated fromthe bronchial circulation directly to the airways. Al-ternatively, they may derive from local monocyticcell renewal systems (albeit undescribed) subjacentto the bronchial epithelium.Although the pulmonary macrophages are essen-
tial to host defense, the normal activity and move-ment of pulmonary macrophages may also causeharm. Because the macrophages are activelyphagocytic, inhaled toxic, radioactive, or car-cinogenic particles become concentrated withinpulmonary macrophages. What begins as a diffuseand relatively even exposure becomes highlylocalized and nonuniform. "Hot spots" are formed,and if thresholds for certain effects exist, these "hot
spots" of high dose may be of significance.Similarly, adherence of some airway macrophages
to the airway epithelium may increase airwayexposure to inhaled toxic materials. More im-portantly, perhaps, this close association with thebronchial epithelium can lead to transbronchialtransport of inhaled particles and subsequent rein-gestion by subepithelial connective tissue ma-crophages. These cells, like their relatives in thealveolar and airway compartments, also segregate,retain. and perhaps metabolize carcinogenic andother toxic particles.
Additional research needs to be carried out onthe structure and function of the pulmonary lym-phatics. Classically, removal of particulatesthrough these channels was often considered to bethe major route for the clearance of material fromthe lower respiratory tract. The importance of lym-phatic clearance was probably exaggerated for sev-eral reasons. Most of the early judgments werebased on morphological studies. Histological pro-cedures, however, usually washed away the parti-cles and cells being cleared via the airways, and sothe importance of this route was underestimated. Itis also difficult to draw quantitative conclusionsabout dynamic processes when only static observa-tions are available. The importance of a clearancepathway is a function not only of the number ofparticles in the pathway, but also of the rate atwhich the particles are moving. Yet, although ourestimate of the percentage of particles cleared viathe lymphatics has dropped, our appreciation of theimportance of those particles entering the lym-pathics has greatly increased. Because particles inlymphatics are cleared slowly, they attain great sig-nificance in the pathogenesis of many lung diseases.When months and years have passed after exposureto particles, these connective tissue burdens mayconstitute the major reservoir of retained particles.Too little is also known regarding the nature and
properties of the air-blood barrier and the potentialfor particles to penetrate it. The extent to which thepulmonary capillary bed serves as a protective filtereliminating debris, pathogens, and cells from thecirculating blood is not well described.
Little is known about the relative importance ofthese clearance pathways in health and disease.This lack is not without good reason. Difficult ex-perimental protocols would be necessary to accu-rately quantitate fractions carried by the differentclearance pathways. Theoretically, clearance bythe various routes could be measured by monitoringthe final common pathways for the airways, theblood vessels and the lymphatics, using various in-genious approaches. In the airways, a balance mustbe made for material deposited more proximally if
October 1977 117
alveolar clearance is to be measured. In the lym-phatic route, a single final pathway would have tobe rationalized surgically for many collateral open-ings into the bloodstream. Examination of lungwashings can be helpful in determining what part ofthe uncleared particle residues are lodged in alveolarmacrophages and what part remain in the connec-tive tissue. Further allowance must be made for thepossibility of crossover from one clearance path toanother, and it is important to separate the amountof material cleared by extracellular from thatcleared by cellular mechanisms. As yet few studieshave provided quantitative details sufficient to de-scribe and evaluate the complexities of alveolarclearance. It is also likely that the extent to whicheach pathway is used depends on the sizes, sol-ubilities, and chemical properties of the depositedparticles, as well as the time elapsed after the ex-posure and the degree of disease present.
Finally, it should also be remembered that depo-sition and clearance must be considered together. Ofprime importance is the mass of the toxic substancein the lung. The actual amount of a substance in therespiratory tract at any time is called the retention.When the exposure is continuous, the equilibriumconcentration (achieved when the clearance ratematches the deposition rate) is also the retention.Thus, the relative rate constants of deposition andclearance determine the equilibrium level; it is thislevel, or retention integrated over time, and theproperties of the particle that are presumably re-lated to the probability of a pathological response.
The Lung As a Target OrganThe lung is more than an important portal of
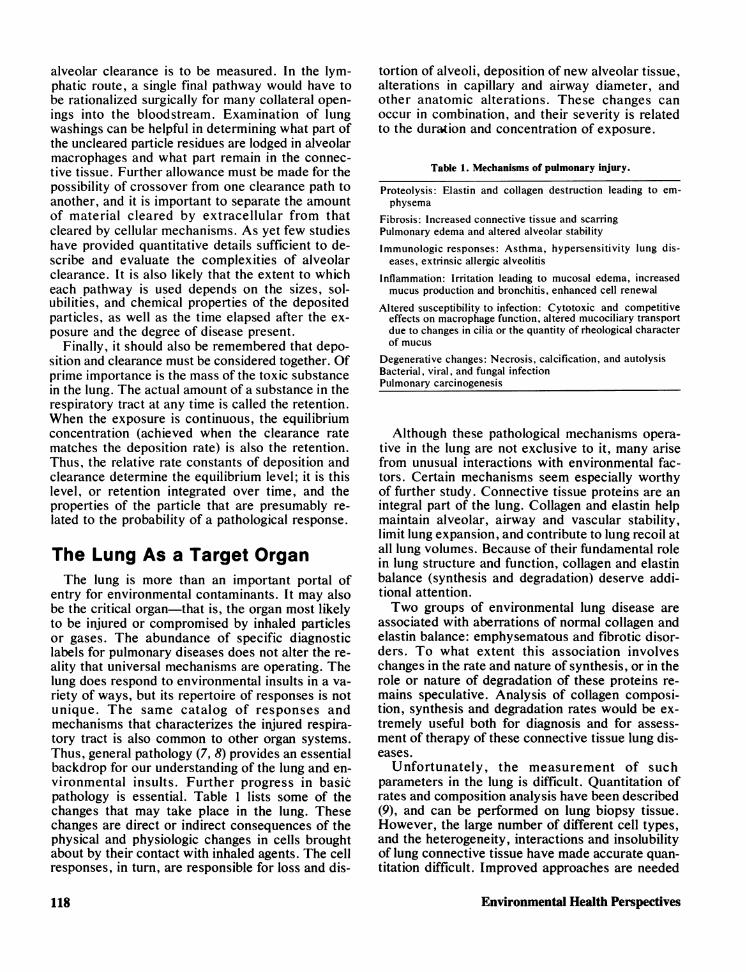
entry for environmental contaminants. It may alsobe the critical organ-that is, the organ most likelyto be injured or compromised by inhaled particlesor gases. The abundance of specific diagnosticlabels for pulmonary diseases does not alter the re-ality that universal mechanisms are operating. Thelung does respond to environmental insults in a va-riety of ways, but its repertoire of responses is notunique. The same catalog of responses andmechanisms that characterizes the injured respira-tory tract is also common to other organ systems.Thus, general pathology (7, 8) provides an essentialbackdrop for our understanding of the lung and en-vironmental insults. Further progress in basicpathology is essential. Table 1 lists some of thechanges that may take place in the lung. Thesechanges are direct or indirect consequences of thephysical and physiologic changes in cells broughtabout by their contact with inhaled agents. The cellresponses, in turn, are responsible for loss and dis-
tortion of alveoli, deposition of new alveolar tissue,alterations in capillary and airway diameter, andother anatomic alterations. These changes canoccur in combination, and their severity is relatedto the duration and concentration of exposure.
Table 1. Mechanisms of pulmonary injury.
Proteolysis: Elastin and collagen destruction leading to em-physema
Fibrosis: Increased connective tissue and scarringPulmonary edema and altered alveolar stabilityImmunologic responses: Asthma, hypersensitivity lung dis-
eases, extrinsic allergic alveolitis
Inflammation: Irritation leading to mucosal edema, increasedmucus production and bronchitis, enhanced cell renewal
Altered susceptibility to infection: Cytotoxic and competitiveeffects on macrophage function, altered mucociliary transportdue to changes in cilia or the quantity of rheological characterof mucus
Degenerative changes: Necrosis, calcification, and autolysisBacterial, viral, and fungal infectionPulmonary carcinogenesis
Although these pathological mechanisms opera-tive in the lung are not exclusive to it, many arisefrom unusual interactions with environmental fac-tors. Certain mechanisms seem especially worthyof further study. Connective tissue proteins are anintegral part of the lung. Collagen and elastin helpmaintain alveolar, airway and vascular stability,limit lung expansion, and contribute to lung recoil atall lung volumes. Because of their fundamental rolein lung structure and function, collagen and elastinbalance (synthesis and degradation) deserve addi-tional attention.Two groups of environmental lung disease are
associated with aberrations of normal collagen andelastin balance: emphysematous and fibrotic disor-ders. To what extent this association involveschanges in the rate and nature of synthesis, or in therole or nature of degradation of these proteins re-mains speculative. Analysis of collagen composi-tion, synthesis and degradation rates would be ex-tremely useful both for diagnosis and for assess-ment of therapy of these connective tissue lung dis-eases.
Unfortunately, the measurement of suchparameters in the lung is difficult. Quantitation ofrates and composition analysis have been described(9), and can be performed on lung biopsy tissue.However, the large number of different cell types,and the heterogeneity, interactions and insolubilityof lung connective tissue have made accurate quan-titation difficult. Improved approaches are needed
Environmental Health Perspectives118

and in vitro models of lung biochemical functionmay be very useful. Appropriate animal models ofemphysema and fibrosis could be exploited to quan-titate the rates of elastin and collagen synthesis anddegradation and to compare them to normal rates.In emphysema, further studies are needed to ex-amine the release of proteolytic enzymes fromleukocytes and macrophages, their effect on lungcells, and the protection afforded by serum and lungantiproteases. In fibrosis, investigations need to bepursued studying the role of lymphocytes, ma-crophages, fibroblasts and the effect of fibrogenicagents on the collagen balance and on the replica-tion and differentiation of each parenchymal celltype (10).
Attention to this kind of injury has increased be-cause of recent new knowledge about pulmonaryemphysema associated with inborn a,-antitrypsin-inhibitor deficiency in humans. Inbalances betweenproteolytic activity and its control or inhibitionhave important implications as a generalizedmechanism of lung injury in other pulmonary path-ological states caused by air pollution, or the inhala-tion of occupational dusts.Much more needs to be known regarding the na-
ture of the particles which trigger these connectivetissue diseases. Dust particles of appropriate sizeand shape may deposit on alveolar surfaces andstimulate production of excess collagen in the al-veolar membrane. Particle size, shape, and durabil-ity may be more important in fibrogenicity thanchemical characteristics. Asbestos, glass, and otherfibrous dusts all have been shown to stimulate col-lagen synthesis (11). Fibers over 5 ,mm in length aresometimes incompletely ingested by macrophages(12, 13), and this may result in macrophage death orrelease of mediators. Growth of fibroblasts in vitrohas been shown to require a solid supporting parti-cle of critical minimum dimensions (14).
In addition, there is some evidence that fibro-genesis may also occur as a two-step process (15).This would especially apply to highly fibrogenicparticles such as silica which are highly symmetri-cal in shape (5 um in diameter) and which are en-gulfed by macrophages following deposition. Silicahas not been shown to exert a direct stimulatoryeffect on fibroblasts. Rather, the interaction of aparticle with a macrophage is thought to release fac-tors which stimulate local production of collagen byfibroblasts. It is unlikely that macrophages differen-tiate into collagen synthesizing fibroblasts (16).
Silica and asbestos have the added disadvantageof being cytotoxic to alveolar macrophages. Withina few minutes they can cause lysis of cells by directinteraction with the plasma membrane, or, if suc-cessfully ingested, in several hours cause rupture of
secondary lysosomes, releasing lysosomal hy-drolases into the cytoplasm (17). The resulting deadmacrophages can become focal points for further fi-brogenesis. In addition, the particles are releasedanew on the alveolar surface to cause more irritation.The responses of the lung to inhaled antigens and
allergens and the general area of environmental al-lergic respiratory disease is emerging as an impor-tant area of basic investigation. Advances in thisarea may help to identify hyperreactors to a numberof industrially important materials, such as toluenediisocyanate (TDI), cotton dust, molds (Farmer'sLung and Bagassosis) and proteins causing a vari-ety of forms of extrinsic allergic alveolitis. Im-munological research addressed to the interactionof these inhaled materials, connective tissue, pul-monary cells and the lymphatic and vascular sys-tems in the lung holds promise. Little is knownabout the degradation of proteins deposited on therespiratory tract surfaces. No doubt, in many in-stances macrophages and pulmonary clearance de-fend the body against excessive antigenic stimula-tion. However, there may also be circumstanceswhen clearance pathways may cooperate with theimmune system and preserve and present im-munogenic molecules to the immune system. Thusthe issue of how and when pulmonary macrophageseither suppress or enhance the immunogenicity ofantigens must be confronted.
It is known that several organic dusts can inducean immune response in bronchial or alveolar tis-sues. The type I and type III allergic reactions aremost commonly seen (18, 19). The type I response,often termed immediate hypersensitivity, occurswhen an inhaled antigen reacts with cell-sensitizingreagenic antibody (IgE). Cells of the bronchial wallmay be sensitized by this antibody, and react toproduce histamine, slow reacting substance ofanaphylaxis, and bradykinin. In persons sensitizedto a specific inhaled antigen, bronchoconstriction,mucosal edema, excessive secretions, andeosinophil infiltration occur.The type III, or Arthus reaction, is characterized
by formation of a complex between an antigen and aprecipitating antibody in the presence of comple-ment. Tissue damage occurs from inflammatory re-sponses caused by deposition of these complexesalong capillary basement membranes. The complexis phagocytized by leukocytes and causes them torelease their lysosomes. In addition, histamine maybe released from mast cells producing local edema.It is unknown whether antigens cross the alveolarand capillar membranes to react with circulating an-tibodies, or if lymphocytes and other reactive cellson the alveolar and bronchiolar surfaces are re-sponsible for the initial antibody-antigen reaction.
October 1977 119

The site of action of TDI and the active compo-nents of cotton dust need to be better described.
Particles inducing hypersensitivity pneumonitistend to be derived from fungal, bacterial, or serumprotein sources. Examples are the fungusThermnoactinomytes vulgaris in Farmer's Lung,Bacillius subtilis in detergent workers' lung and birdfanciers' disease (20-22).Neoplastic responses to inhaled particles is
another area of major and growing concern. Al-though smoking has been determined to be themajor cause of respiratory carcinogenesis, otherfactors, especially industrially produced agents, aregaining strong epidemiologic support. Asbestosishas been correlated with bronchogenic carcinoma,as well as mesothelioma of the pleura andperitoneum (22). In addition, a synergistic effect be-tween asbestos and cigarette smoking may cause asubstantially increased risk (23). Other agents im-posing an increased risk are the polycyclic aromatichydrocarbons, radioisotopes, chromates, and com-pounds involved in nickel refining (24-27).
Further study on the role of modifying influencesis of particular importance. The pathogeneticmechanisms just discussed are in no way isolatedfrom important host variables. Dose-responsecurves for interactions with environmental agentsare altered by many characteristics of the exposedorganism and its immediate environment. Some fac-tors known to be important include: developmentalaspects, aging; genetic factors (AHH inducibilityand lung cancer, a,-antitrypsin deficiency, non-specific airway reactivity); sexual differences;species differences; interactions; circadianrhythms; effects of pre-existing disease ("the sensi-tive individual"); nutritional status; drugs; exerciseand altered ventilation; tolerance and adaptation;and metabolic transformations.
Additional resear-ch concerning the effect ofthese variables on the respiratory tract and otherorgan systems is desirable.
Detection and Quantitationof Lung InjuryAn essential aspect of research on environmental
lung diseases relates to improved determination ofdose-response curves. We need to know with pre-cision to what the respiratory tract is being ex-posed. We must be able to measure lung damagewith similar precision and sensitivity.
It is now more widely appreciated that it is essen-tial to specify the mass, particle size, and solubilityof inhaled particles. The ICRP lung model (2, 28)emphasized the importance of these parameters indetermining burdens of particulates in the respira-
tory tract. It also provided a common frameworkwhich can be used in summarizing experimentaldata. But there are still major problems in quantitat-ing the pulmonary dose. The relative merits of in-tratracheal and inhalation exposures have recentlybeen discussed (29). Switching from nose to mouthbreathing and the effects of exercise are largely un-explored. Systematic descriptions of species differ-ences are also essential. Although many specieshave been used for studies in aerosol deposition, weare unaware of any published systematic descrip-tion of the differences between commonly usedlaboratory animals. It is difficult to abstract such adescription from the literature because so many dif-ferent kinds of animals and aerosols have been usedin various combinations.The lung responds to environmental injury in
many ways. This diversity in response is matchedby a dazzling array of possible tests designed todetect and quantitate lung damage. Table 2 listssome of the approaches which commonly have beenused.Almost all these approaches demand further re-
finement and many have serious limitations. Forexample, one of the major problems with pulmo-nary function tests is that they are rarely specific.Measurements of airway resistance reflect not onlydirect alterations in the airway but may also reflectparenchymal changes. For example, if the paren-chyma becomes weakened by emphysema, supportfor the airways is diminished. They become morecollapsible and airway resistance may increase.Similarly, compliance measurements do not exclu-sively reflect changes in the pulmonary paren-chyma. If airway obstruction occurs, then theparenchyma served by the airway will largely beexcluded and the lung will appear to be stiffer.
Further refinements are also needed for betterhistologic, histochemical and morphometricanalysis of lung damage. Various fixation proce-dures have been used for the fixation of lung tissue.The main criteria are to preserve optimally the pul-monary parenchyma in accordance with the desiredgoal (examination of ultrastructure, investigation ofacellular alveolar lining layer, application of his-tochemistry). Techniques exist which permit cuttingsections of whole lungs for pathologic examination.These sections were originally intended for study-ing the pathology of coal workers' pneumoconiosis,and for comparison with radiological examinationsduring the individuals'lives.In addition to evaluatingthe lung sections qualitatively, quantitative mor-phometric methods (30) have been developed toassay the degree of tissue damage.
It would be desirable to identify enzymes or otherfactors released from damaged lung into serum
Environmental Health Perspectives120
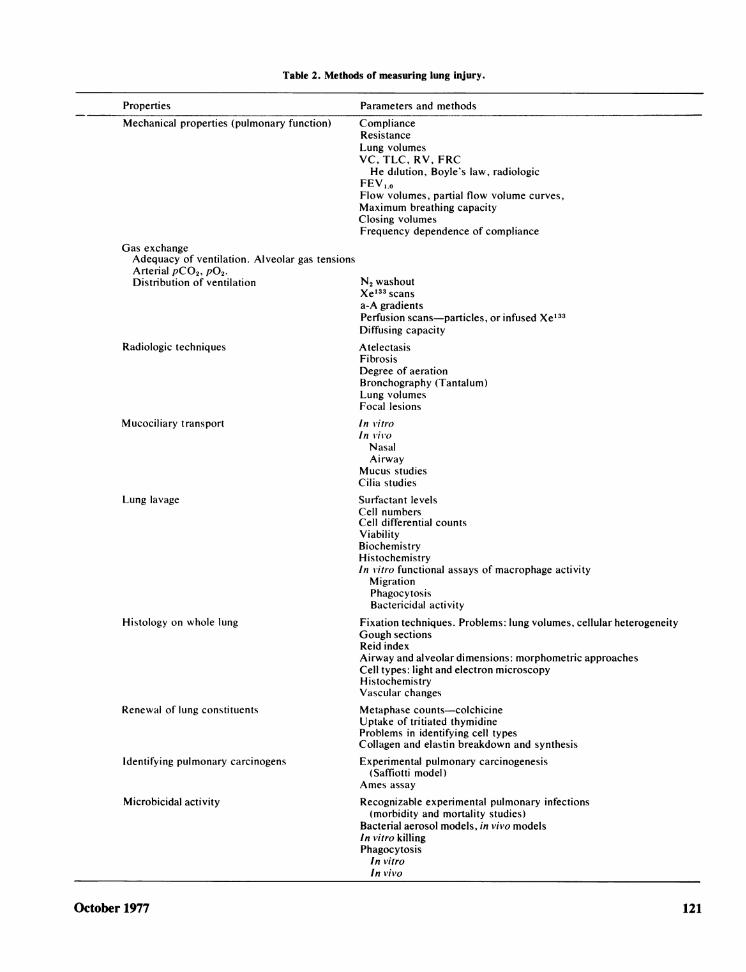
Table 2. Methods of measuring lung injury.
Properties
Mechanical properties (pulmonary function)
Gas exchangeAdequacy of ventilation. Alveolar gas tensionsArterial pCO2, P02.Distribution of ventilation
Radiologic techniques
Mucociliary transport
Lung lavage
Histology on whole lung
Renewal of lung constituents
Identifying pulmonary carcinogens
Microbicidal activity
Parameters and methods
ComplianceResistancel1ung volumesVC, TLC, RV, FRCHe dilution, Boyle's law, radiologic
FEV ,OFlow volumes, partial flow volume curves,Maximum breathing capacityClosing volumesFrequency dependence of compliance
N2 washoutXe'33 scansa-A gradientsPerfusion scans-particles, or infused Xe'33Diffusing capacityAtelectasisFibrosisDegree of aerationBronchography (Tantalum)Lung volumesFocal lesions
In VitroIn vivoNasalAirway
Mucus studiesCilia studies
Surfactant levelsCell numbersCell differential countsViabilityBiochemistryHistochemistryIn *vitro functional assays of macrophage activity
MigrationPhagocytosisBactericidal activity
Fixation techniques. Problems: lung volumes, cellular heterogeneityGough sectionsReid indexAirway and alveolar dimensions: morphometric approachesCell types: light and electron microscopyHistochemistryVascular changes
Metaphase counts-colchicineUptake of tritiated thymidineProblems in identifying cell typesCollagen and elastin breakdown and synthesisExperimental pulmonary carcinogenesis
(Saffiotti model)Ames assay
Recognizable experimental pulmonary infections(morbidity and mortality studies)
Bacterial aerosol models, in vivo modelsIn vitro killingPhagocytosis
In vitroIn vivo
October 1977 121

which could be sampled. Unfortunately, currentlyno biochemical parameters are known which clearlyindicate the presence of toxic lung damage. It thusbecomes important to obtain more complete knowl-edge about the biochemical events leading to celldeath or to repair and pulmonary cell proliferation.Only then will we understand the mechanisms ofresponse and perhaps obtain useful indicators oflung damage.Techniques for sampling directly from the lung
are also desirable. Improved biopsy techniqueswhich can be used for repeated sampling from liveanimals need to be developed. Lung lavage both insacrificed animals and in isolated segments of livinganimals is also a valuable approach (see Table 2).For example, research on pulmonary macrophagesoften depends on our ability to isolate pure popula-tions of macrophages from the lungs of animals andman. Alveolar macrophages represent a relativelyhomogeneous cell population accessible by lunglavage. However, success in isolating pulmonarymacrophages depends on the particular subclassesinvolved, and, unfortunately, not all categories ofpulmonary macrophages can be recovered with thesame ease and purity. To our knowledge, no inves-tigator has been able to prepare a pure suspensionof interstitial pulmonary macrophages. Techniquesfor dissolving the lung and liberating individual cellsare being developed and intensive efforts are un-derway with regard to separation of isolated lungcells. However, interstitial macrophages are lessnumerous and little is known about the existence ofunique physical or chemical properties which couldbe exploited in separating these cells. Conceivably,their tendency to attach themselves to glass or somespecific surface receptor could be exploited. If alung which has been washed to eliminate airwayand alveolar macrophages, was dispersed, presum-ably those cells attaching to glass represent arelatively enriched population of interstitial macro-phages.
Improved assays for identifying pulmonary car-cinogens also need to be developed. One approachis to administer the suspected material to a labora-tory animal by intratracheal instillation. Saffioti (31)has developed such an approach, and it has beenfirequently imitated. An alternative to experimentalcarcinogenesis has been implemented by Ames etal. (32). This test operates under the working hy-pothesis that carcinogens are also mutagens. Using'an in vitro bacterial test system (Salmonellatyphimurium) Ames et al. have been able to detectknown classes of mutagens at very low con-centrations. The Ames assay is based on the use ofcontrolled mutation of the bacterial strain for de-tecting mutagens by a highly sensitive and con-venient back mutation test. The relatively small
genome (approx. 4 x 106 base pairs), the largenumber of organisms exposed (approx. 109 perplate), and positive selection of mutants are some ofthe advantages of this system. In addition, manychemical carcinogens become powerful mutagensthrough in vivo metabolic activation, so addition ofvarious cell suspensions to the test culture isanother important feature.
ConclusionsPollutants characteristic of occupational and
urban environments, bacteria, viruses, and other in-fectious particles, allergens, and antigens all maycause or aggravate pulmonary disease (Table 3).Furthermore, the magnitude of these effects isstrongly influenced by the number of particles depo-sited, their site of deposition, and especially theirultimate fate. Thus, environmental factors representa major area of concern. Death rates for lung cancerand pulmonary emphysema have been steadily in-creasing over the last half century. Chronic nons-pecific pulmonary disease has become a leadingcause of death and disability in adult males.Cigarette smoking is the major cause of thisepidemic, but community air pollution and industrialexposures are also a major significance.
RecommendationsIt is important to realize that factors within the
laboratory environment may influence the responseof animals to inhaled particles and vapors. Suchdiverse influences as dietary components and con-taminants, caging conditions, (bedding, cleanliness,crowding, lighting, temperature), nutritional defi-ciency, disease, as well as such factors as insec-ticides and pesticides which are used to keep animalfacilities insect- or pest-free must be better under-stood and quantified.The properties of the bronchial epithelium may
be critical in relation to the development of lungdisease. The epithelium is both a surface that canrespond, and a barrier which is occasionallycrossed. A great deal is known about the epitheliallining of the gastrointestinal tract and its relation-ship to the movement of particles, molecules,electrolytes, and water. Similar information oughtto be gathered about the bronchial epithelium.
Support for studying the effects of air pollutionshould be continued. Such studies are essential indetermining mechanisms of biological response andas part of systematic studies of dose-response rela-tionships. They also may be used as animal models
Environmental Health Perspectives122

Table 3. Important agents producing environmental lung diseases.a
Type
Inorganic dustsFree silica
CrystallineAmorphous
SilicatesFibrousOther
Carbon"Inert" metals
Biological "dusts"Vegetable
Animal
Toxic chemicalsIrritant gases
Metallic fumes, vapors, oxidesand salts
PlasticsAerosols
Respiratory infectionsBacteria
Vi rus/rickettsiae
Fungi
Respiratory carcinogens
Consumer products
Tobacco products
Examples
Quartz, tridymite cristobaliteDiatomaceous earth, silica gel
Asbestos, sillimanite, talc, sericiteMica, Fuller's Earth, kaolin, cement dustCoal, graphite, carbon black, soot, charcoalIron, barium, tin
Moldy hay ("farmer's lung"), mushroom compost, bagasse (sugar cane), maplebark, B. siubtilis enzyme (detergents), malt, grain-weevil, cork, roof-thatch,lycoperdon, cotton, flax, hemp, jute, sisal, thermiophilic actinomycetes
Pigeons, parrots, buderigars, hens, pituitary snuff
Oxides of nitrogen (silo filler's disease) sulfur dioxide, ammonia, chlorine ozone,phosgene, carbon tetrachloride, hydrogen chloride, chlorinated camphrene,chloropicrin, "smoke"
Beryllium, silicide, mercury, cadmium, platinum, magnanese, zinc, vanadiumpentoxide, nickel, osmiumPolytetrafluoroethylene, toluene diisocyanate (TDI)Mineral oil, "cutting" oils, copper sulfate
Tuberculosis (miners, nurses, pathologists),Anthrax (wool, mohair, and alpaca workers)Glanders (grooming of horses, mules)Psittacosis (pet shops, turkey dressings, pigeons)Variola (smallpox handlers)Q fever (lab workers, abattoirs)Coccidiomycocis (irrigation, farm work, archeology)Histoplasmosis (poultry, pigeons, starlings)Cryptococcosis (pigeons)Arsenic, cobalt, nickel, hematite, uranium (pitch blends, "yellow cake") iso-propyl oil, gas retort fumes, chromates, asbestos, other silicates (talc)Hair spraysDeodorantsPaintsPesticidesCigarettesCigars and pipesMarijuana
"From Trieff and Corrigan (33).
for the effects of new products. Systematic expo-sure of animals to materials produced by technolog-ical advance would permit some assessment of theeffects of these materials.The effects of parameters which may modulate
the pulmonary response to atmospheric and indus-trial contaminants should be measured. The effectsof medications, altered physiological states, andconcurrent illness should be systematically ex-plored. Meteorologic variables (temperature, fog)and factors in the organism such as exercise, dis-
ease, or allergic states, adaptation, and presence ofother foreign chemicals should also be considered.Support for lung research is supplied by a number
of Federal agencies, such as NHLBI, EPA,NIOSH, ERDA, as well as NIEHS. Coordinationand integration among these different organiza-tions is frequently inadequate. Mechanisms shouldbe developed for finding out about each other'sgrant programs, contract programs, and in-houseresearch. Also, a published inventory of majorfacilities which are essential in health effects re-
October 1977 123

search would encourage more efficient use ofscarce and expensive resources. Sophisticated en-vironmental exposure chambers, for example, nowexist and might be made available to visiting scien-tists.A frequent response to environmental insult is
the deposition of fibrous connective tissue (a scar)usually known as pulmonary fibrosis or proteolysisand alveolar wall destruction leading to em-physema. These responses are common to anumber of inhaled particles and gases. Our under-standing of these diseases and appropriatestrategies for their prevention and control would behelped by a better understanding of the synthesisand degradation of collagen in the lung, since it isthe primary connective tissue protein. Similarstudies should be carried out with regard to pulmo-nar-y elastin.
Diseases such as bronchial asthma, Farmer'sLung, diffuse hypersensitivity pneumonitis, andsai-coidosis are all examples of pulmonary diseasescharacterized by immunologic abnormalities. Manyof the symptoms of asthma appear to be mediatedby various chemicals released from lung cells.Further reseai-ch is needed to define othermediators, to determine where and how they act,and to learn what environmental materials governtheir release.
Frequently important contributions to our under-standing of environmental disease have dependedupon the existence of appr-opriate animal models.These are most helpful when the animals react todisease as humans do. Additional research whichwill develop and exploit animal analogs of en-vironmental disease processes common to manshould be suppor-ted.New indices of exposure need to be developed.
Breath analysis may be exploited as an indicator ofexposure. Lung analysis at autopsy may also yielduseful information about retention levels of pollu-tants. Noninvasive approaches to intact animalsand people, such as whole body counting ofradioactive materials or the use of magnetic mea-surements as a possible index of asbestos exposure,should be exploited.More sensitive and specific indices of injury
should be developed. Early detection should be amajor goal especially when reversibility is possible.
For large segments of the population, industrialand atmospheric contaminants aggravate existinglung injury. More research is needed concerning theinfluence of disease states on the response to en-vironmental agents. Animal models of asthma, em-physema, lung cancer, and newborn and adult res-piratory distress syndrome all need to be better de-veloped and defined and then used in these kinds of
experiments. Similarly, such important agents as to-bacco and alcohol need to be studied in regard topossible synergistic action.
Pulmonary metabolism needs to be better de-scribed. We need to understand how environmentalcontaminants are either degraded or made moretoxic by the lung. The use of isolated cells, the iso-lated perfused lung, whole animals, and other testsystems can lead to improved understanding.
Species differences in lung structure, function,endemic disease, and susceptibility to environmen-tal agents need to be better determined. Compara-tive studies of the physiology, biochemistry, andmorphology of the lung should be encouraged inorder to provide a logical basis for understandingthe mechanisms of environmental influence andcomparing results in animals and man.
Pyrolysis products, either as a result of industrialprocesses or as a result of unwanted fires, causefrequent exposure. Better analysis of the chemicalcomposition of pyrolysis products and of their im-pact on the lung and other organs is needed.
Since so many diseases of the lung are poorlydiagnosed and/or treated, more emphasis needs tobe given to preventive strategies. The design ofadequate legislation, testing of new materials andespecially compliance with existing laws, all need tobe studied. Frequently, we are dealing with factorsinfluencing human behavior (i.e. use of protectiveequipment and safety strategies). Factors affectingindividual compliance need to be better understood.
All organisms undergo a normal developmentalsequence beginning with conception and leading todeath. The conditions of each developmental stagemay influence the response of the lung and of theorganism to environmental insult and should be bet-ter studied. Very young and very old animalsshould be exposed to both air pollutants and parti-cles and gases characteristic of industrial environ-ments. Age-related responses must be morethoroughly described.Chamber concentrations of pollutants do not
adequately define dose since deposition is influ-enced by exercise, circadian rhythms, level of activ-ity, and other factors. The effective dose is furthermodified by clearance pathways and by metabolicchanges which make the compounds more or lesstoxic. Whenever possible, the effective tissue doseat the site of action in the lung should be measured.The time course of damage, recovery, repair, and
adaptation to inhaled particles and vapors must bedescribed. This description is essential to an under-standing of mechanisms involved in damage. Thishistory also influences the design of experiments bypredicting optimal times for sampling.Our understanding of almost all environmental
Environmental Health Perspectives124

lung disease would be greatly enhanced by a morethorough knowledge of the cell biology andphysiology of the lungs. Important clues to thecause and prevention of environmental lung diseasehave frequently come from scientists working in un-related areas. Thus future progress in controllingenvironmental lung disease will depend in part onstrong support for basic research in a variety offields of science, as well as those fields directlyconcerned with the environment and the lung.Too little is known about what influences an
individual's decision to help or hinder his or herpulmonary health. Addictive cigarette smoking orcompliance with preventive strategies such as res-pirators are two examples. Research should focuson the mechanisms of motivation for self-help orself-destruction. Similarly, research should be sup-ported on the effectiveness of various educationcampaigns designed to influence human behavior.
Bronchial mucus is a major factor in the defensemechanisms of the lung as well as a componentcapable of response. The structure, synthesis,physical, chemical and rheological characteristicsof mucus and periciliary fluid need to be betterelucidated.
Studies aimed at identifying specific causativeagents in cigarette smoke should be continued. Thepresence of certain carcinogens, such as polycyclichydrocarbons and 210Po, have been suggested ashaving major importance. Animal experimentsshould be carried out with animals exposed tocigarettes with these materials selectively removed.Steps should be taken to determine whether low tarand nicotine cigarettes are less hazardous thanothers. The possibility that combinations of agentsrather than single components are responsible mustbe kept in mind. Research should not focus exclu-sively on carcinogenesis, but also on the manyother deleterious effects of cigarette smoke on therespiratory and cardiovascular systems. Aggressivesteps toward developing a safe cigarette should beundertaken.
Additional studies should be carried out to de-termine whether cigarette smoking has a synergisticaction with other materials in the production of em-physema, cancer, asthma, and other pulmonarydiseases. Such synergism seems to exist betweencigarette smoking and asbestos exposure as well asexposure to radon-daughters, which are found inuranium mines. Experiments of this sort should becarried out in animals as well as in humanepidemiological studies.Our knowledge of the effects of indoor climate is
limited. Widespread use of artificial ventilation,heating, and cooling of indoor air influence thelungs to a degree which is now uncertain. Building
materials may emit noxious substances into indoorair, or conversely may serve to reduce indoor airpollution through absorption on indoor surfaces.Additional studies are needed to ascertain the influ-ence of indoor climate on the lungs.The lung is composed of many different cell
types. Loss and replacement of these play an im-portant role in the response to environmental pol-lutants. Measurements of turnover rates of lungcells and the changes in these rates relative to en-vironmental insult require further study.
Because environmentally induced emphysema,chronic bronchitis, and lung cancer are usually ir-reversible by the time they are diagnosed, improvedtechniques and devices are needed to detect earlybiochemical, immunologic or physiologic abnor-malities associated with development of these dis-eases.
This material is drawn from a Background Document pre-pared by the author for the NIEHS Second Task Force forResearch Planning in Environmental Health Science. The Re-port of the Task Force is an independent and collective reportwhich has been published by the Government Printing Officeunder the title, "Human Health and Environment-Some Re-search Needs." Copies of the original material for this Back-ground Document, as well as others prepared for the report canbe secured from the National Technical Information Service,U.S. Department of Commerce, 5285 Port Royal Road, Spring-field, Virginia 22161.
These investigations were supported by grants ES 01016 and ES00002 from the National Institute of Environmental Health Sci-ences and Grant HL 19170 from the National Heart, Lung, andBlood Institute.
REFERENCES
1. Hatch, T. F., and Gross, P. Pulmonary Deposition and Re-tention of Inhaled Aerosols, Academic Press, New York,1964.
2. Brain, J. D., and Valberg, P. A. Models of lung retentionbased on the report of the ICRP Task Group. Arch. Envi-ron. Health 28: 1 (1974).
3. Lippman, M., et al. Effects of Inhaled Particles on Man andAnimals, Part I: Deposition, Retention, and Clearance. Na-tional Research Council, 1977.
4. Green, G. M., and Kass, E. H. The role of the alveolarmacrophage in the clearance of bacteria from the lung.J. Exp. Med. 119: 167 (1964).
5. Schiller, E. Inhalation, retention, and elimination of dustsfrom dogs' and rats' lungs with special reference to the al-veolar phagocytes and bronchial epithelium. In: InhaledParticles and Vapours, C. N. Davis, Ed., Pergamon Press,London, 1961.
6. Sorokin, S. P., and Brain, J. D. Pathways of clearance inmouse lungs exposed to iron oxide aerosols. Anat. Rec. 181:581 (1975).
7. Florey, H. W., General Pathology. Lloye-Luke, London, 4thed., 1970.
8. Robbins, S. L., and Angel, M. Basic Pathology. W. A.Saunders, Philadelphia, 1971.
9. Bradley, K., McConnel-Breul, S., and Crystal, R. G. Col-lagen in the human lung. J. Clin. Invest. 55: 543 (1975).
October 1977 125

10. Hance, A. J. The connective tissue of lung. Am. Rev. Resp.Dis. 112: 657 (1975).
11. Davis, J. M. G. In: Biological Effects of Asbestos. Int.Agency Res. Cancer, Lyons, 1973.
12. Allison, A. C. Effects of asbestos particles on macrophages,mesothelial cells and fibroblasts. In: Biological Effects ofAsbestos. Int. Agency Res. Cancer, Lyons, 1973.
13. Richards, R. J., Wusterman, F. S., and Dodgson, K. S. Thedirect effects of dusts on lung fibroblasts in vitro. Life Sci-ences 10: 1149 (1970).
14. Maroudas, N. D., O'Neill, C. H., and Stanteen, M. F.Asbestos induced tumours: fibroblast anchorage as a factorin carcinogenesis by fibres. Nature 244: 353 (1973).
15. Heppleston, A. G., and Styles, J. A. Activity of a ma-crophage factor in collagen formation by silica. Nature214: 521 (1967).
16. Allison, A. C. Pathogenic effects of inhaled particles andantigens. Ann. N. Y. Acad. Sci. 221: 2 (1974).
17. Allison, A. C., Harington, J. S., and Birbeck, M. An ex-amination of the cytotoxic effects of silica on macrophages.J. Exp. Med. 124: 141 (1966).
18. Bendixen, G. Classification of hypersensitivity in relation toclinical disease. Ann. Int. Med. 64: 668 (1966).
19. Rose, B., and Phills, A. The immune reaction in pulmonarydisease. Arch. Environ. Health 14: 97 (1967).
20. Pepys, J., et al. Farmer's lung. Thermophilic actinomycetesas a source of "farmer's lung hay" antigen. Lancet 2: 607(1963).
21. Pepys, J. Hypersensitivity Disease of the Lungs Due to Fungiand Other Organic Dusts. Monographs in Allergy, 4. S.Karger, Basel, 1969.
22. Selikoff, 1. J., Churg, J., and Hammond, E. C. Asbestosexposure and neoplasm. J. Amer. Med. Assoc. 188: 222(1964).
23. Selikoff, 1. J., Hammond, E. C., and Churg, J. Asbestosexposure, smoking, and neoplasia. J. Amer. Med. Assoc.204: 106 (1968).
24. Doll, R., et al. Mortality of gas workers-final report of aprospective study. Brit. J. Ind. Med. 29: 394 (1972).
25. Wagoner, J. K., et al. Cancer mortality patterns amongU. S. uranium miners and millers, 1950-1962. J. Natl. Canc.Inst. 32: 781 (1964).
26. Bidstrup, R. L., and Case, R. A. Carcinoma of the lung inworkmen in the bichromates producing industry in Great
Britain. Brit. J. Ind. Med. 32: 62 (1975).27. Pederson, E., Hogetver, A. C., and Andersen, A. Cancer
of the respiratory organs among workers at a nickel refineryin Norway. Int. J. Cancer 12: 32 (1973).
28. Task Group on Lung Dynamics. Deposition and retentionmodels for internal dosimetry of the human respiratory tract.Health Phys. 12: 173 (1966).
29. Brain, J. D., Sorokin, S. P., and Godleski, J. J. Structure,origin and fate of the macrophage. In: Respiratory DefenseMechanisms (Lung Biology in Health and Disease, Mono-graph 5), J. D. Brain, D. F. Proctor, and L. Reid, Eds.Marcel Dekker, New York, 1977.
30. Weibel, E. R. Morphological basis of alveolar-capillary gasexchange. Physiol. Rev. 53: 419 (1973).
31. Saffiotti, U., Cefis, F., and Kolb, L. H. A method for theexperimental induction of bronchiogenic carcinoma. CancerRes. 28: 104 (1968).
32. Ames, B. N., et al. An improved bacterial test system forthe detection and classification of mutagens and car-cinogens. Proc. Nat. Acad. Sci. 70(3): 782 (1973).
126 Environmental Health Perspectives