the effect of chronic kidney disease (ckd) on the cardiovascular system lesley c. dinwiddie msn, rn,...
TRANSCRIPT

The Effect of The Effect of Chronic Kidney Disease (CKD) Chronic Kidney Disease (CKD) on the CardioVascular Systemon the CardioVascular System
Lesley C. DinwiddieLesley C. DinwiddieMSN, RN, FNP,CNNMSN, RN, FNP,CNN
February 24th, 2011February 24th, 2011

Thanks to the Cardinal Chapter
for giving me the opportunity to increase awareness about the under-diagnosed and under-treated public health threat that is Chronic Kidney Disease (CKD) plus CardioVascular Disease!

Disclosures
ICEER – Institute for Clinical Excellence, ICEER – Institute for Clinical Excellence, Education, and Research – nurse organized, Education, and Research – nurse organized, non-profit group promoting education about non-profit group promoting education about CKD CKD
Acknowledgement of Patricia McCarley, RN, Acknowledgement of Patricia McCarley, RN, MSN, NP, co-creator of this presentation. MSN, NP, co-creator of this presentation.
Consultant for Teleflex Medical, Hemosphere, Consultant for Teleflex Medical, Hemosphere, SurgPro, and Genentech – no conflicts of SurgPro, and Genentech – no conflicts of interest to disclose for this presentation.interest to disclose for this presentation.

Overall ObjectiveOverall Objective
Explain the scenario of chronic Explain the scenario of chronic kidney disease (CKD) and the effect kidney disease (CKD) and the effect of cardiovascular disease (CVD) in of cardiovascular disease (CVD) in the patient with chronic kidney the patient with chronic kidney disease. disease.

What is What is the the leading leading cause of cause of MortalityMortalityin our in our CKD CKD patient patient populatiopopulation? n?

Focused ObjectivesFocused Objectives
• Describe the link/the synergy between Describe the link/the synergy between patients with CKD and CVD.patients with CKD and CVD.
• Teach how to recognize patients at risk for Teach how to recognize patients at risk for CKD, review screening for CKD and CKD, review screening for CKD and assessment of eGFR.assessment of eGFR.
• Discuss factors related to progression and Discuss factors related to progression and slowing of progression of CKD and CVD.slowing of progression of CKD and CVD.
• Identify complications of CKD and strategies Identify complications of CKD and strategies to improve outcomes.to improve outcomes.

How you How you see this see this all all depends depends on your on your perspectperspective!ive!
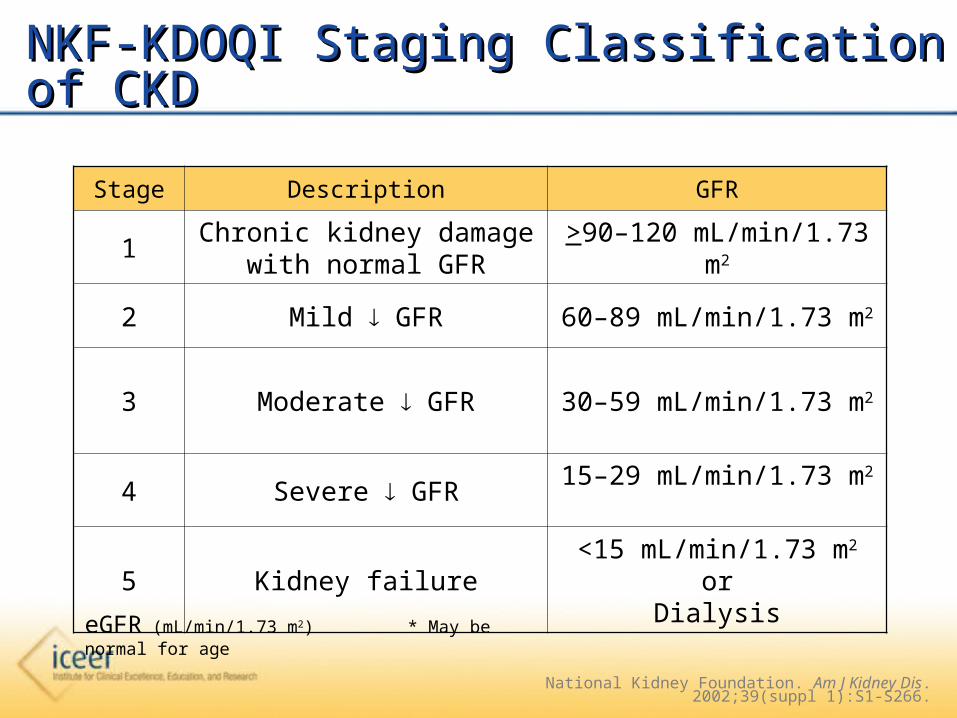
NKF-KDOQI Staging Classification of CKDNKF-KDOQI Staging Classification of CKD
Stage Description GFR
1Chronic kidney damage with
normal GFR>90–120 mL/min/1.73
m2
2 Mild GFR 60–89 mL/min/1.73 m2
3 Moderate GFR 30–59 mL/min/1.73 m2
4 Severe GFR15–29 mL/min/1.73 m2
5 Kidney failure<15 mL/min/1.73 m2
orDialysis
National Kidney Foundation. Am J Kidney Dis. 2002;39(suppl 1):S1-S266.
eGFR (mL/min/1.73 m2) * May be normal for age

• Mary is a 70 year old female with history of Mary is a 70 year old female with history of CKD, type 2 diabetes mellitus, twenty year CKD, type 2 diabetes mellitus, twenty year history of hypertension, CHF, hyperlipidemia, history of hypertension, CHF, hyperlipidemia, and CAD with recent history of MI and and CAD with recent history of MI and angioplasty.angioplasty.
• Patient presents to the officePatient presents to the office
• Chief complaint: “shortness of breath”Chief complaint: “shortness of breath”
CASE 1CASE 1

Assessment in the office:Assessment in the office: – BP 118/50 P-112 R-24 T-97.4 BP 118/50 P-112 R-24 T-97.4 – Alert & oriented x 3Alert & oriented x 3– No neck vein distention or apparent edemaNo neck vein distention or apparent edema– Lungs – crackles in basesLungs – crackles in bases– RRR, SEM III/VIRRR, SEM III/VI– No focal neurological deficitsNo focal neurological deficits– Meds: lisinopril, furosemide, clopidogrel, aspirin, Meds: lisinopril, furosemide, clopidogrel, aspirin,
isosorbide, carvedilol, glipizide, and rosiglitazone, isosorbide, carvedilol, glipizide, and rosiglitazone, atorvastatinatorvastatin
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

What are your differential diagnoses?What are your differential diagnoses?
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”
Does the fact that this patient has CKDDoes the fact that this patient has CKDaffect your choice of diagnoses?affect your choice of diagnoses?

• CARDIOVASCULAR DISEASECARDIOVASCULAR DISEASE
– MI MI
– ArrhythmiaArrhythmia
• CHFCHF
• AnemiaAnemia
• OTHEROTHER
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

Cardiovascular Disease ??Cardiovascular Disease ??
- MI - MI
- Arrhythmia- Arrhythmia
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”
Cardiovascular Disease ??Cardiovascular Disease ??
- MI - MI
- Arrhythmia- Arrhythmia
Patient with recent MI and Patient with recent MI and angioplasty and…… CKD. angioplasty and…… CKD.

Cardiovascular Outcomes WorsenCardiovascular Outcomes Worsenwith CKD Progressionwith CKD Progression
0
10
20
30
40
50
60
Composite EndPoint
Death From CVCauses
Reinfarction CHF Stroke Resuscitation
CHF = congestive heart failure; CV = cardiovascular.
Est
imat
ed E
vent
Rat
e (%
)E
stim
ated
Eve
nt R
ate
(%) P<0.001
75 60-74 45-59<45
eGFR (mL/min/1.73 m2)
VALLIANT TRIAL
3-Yr Follow-Up by eGFR Levels3-Yr Follow-Up by eGFR Levelsin Post-MI Patientsin Post-MI Patients
Anavekar et al. N Engl J Med. 2004; 351:1285-1295.
N = 14,527

• MI symptoms in patients with CKD:• 4,482 patients seeking care for AMI -
community wide study involving 11 medical centers in Worchester, MA during 4 study years (1997, 1999, 2001, 2003)
Sosnov, J et al. AJKD. 2006.47(3); 378-384.
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”
Patients with CKD were less likely
to report chest pain, arm pain, shoulder pain,
while being more likely to report shortness of breath

Prevalence of IHD Prevalence of IHD in the General Population and CKD in the General Population and CKD
CVCVDiseaseDisease
General General PopulationPopulation
CKDCKD
IschemicIschemicHeart Heart
DiseaseDisease
8 - 13%8 - 13% 15 % (transplant)15 % (transplant)
40% (CKD stage 5)40% (CKD stage 5) Sarnak et al. Circulation. 2003. 108;2154.
IHD admissions are 2-2.5 times higher in the IHD admissions are 2-2.5 times higher in the CKD population CKD population USRDS, 2004 Annual Report
MI remains in our diagnosesMI remains in our diagnoses

CVD and CKD – MorbidityCVD and CKD – Morbidity
• Cardiac arrhythmia admission rates are 2 Cardiac arrhythmia admission rates are 2 times as common in CKD populationtimes as common in CKD population
• 269 patients with stable CHF 269 patients with stable CHF - longer PQ and QRS intervals were - longer PQ and QRS intervals were inversely related to eGFR (cardiac-event inversely related to eGFR (cardiac-event free survival rate 51% in pts with CKD vs free survival rate 51% in pts with CKD vs 81% in those without CKD) 81% in those without CKD)
USRDS, 2004 Annual Report
Bruch, C et al. Int J of Cardiol. 2007. 118(3):375-380.

Cardiovascular Disease ??Cardiovascular Disease ?? MI or arrhythmiaMI or arrhythmia
• Shortness of breath – YESShortness of breath – YES
Exam reveals - RRRExam reveals - RRR• MI – possible – must continue to consider MI – possible – must continue to consider
in the differential and evaluate furtherin the differential and evaluate further
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

VASCULAR SYSTEMVASCULAR SYSTEM
Large veinsElastic/conducting
arteries
Muscular/distributing arteries
Arterioles
Capillaries
Venules
Post-capillary venules
VeinsNode
Lymphatics
Heart
WABeresford

Congestive Heart Failure?Congestive Heart Failure?
Cardio-Renal Syndrome* – “ A syndrome in which Cardio-Renal Syndrome* – “ A syndrome in which the heart the heart OROR kidney fails to compensate for the kidney fails to compensate for the functional impairment of the respective organ, functional impairment of the respective organ, resulting in a vicious cycle that will ultimately result resulting in a vicious cycle that will ultimately result in decomposition of the entire circulatory system.” in decomposition of the entire circulatory system.”
Boerrigter,G. Current Heart Failure Rep. 2004: 1(3); 113-120.
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”
CRS “occurs through multiple mechanisms that demonstrate the CRS “occurs through multiple mechanisms that demonstrate the
complex interaction between the two organs”complex interaction between the two organs”
Elhassan and Schrier 2010 ASN Kidney NewsElhassan and Schrier 2010 ASN Kidney News
Congestive Heart Failure?Congestive Heart Failure?
““A pathologic condition where combined cardiac and A pathologic condition where combined cardiac and renal dysfunction amplifies progression of the renal dysfunction amplifies progression of the individual organ to astounding morbidity and individual organ to astounding morbidity and mortality.”mortality.”
Bongartzr, Eur Heart J,
2995
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”
““A Fatal Dance of Two Noble Organs”A Fatal Dance of Two Noble Organs” Burl, D, UCDavis,
2008.

The Cardiorenal Syndrome: The Cardiorenal Syndrome: Which Came First—Which Came First—the Chicken or the Egg?the Chicken or the Egg?
By Elwaleed Elhassan, MD, and Robert Schrier, MD
http://www.asn-online.org/publications/kidneynews/archives/2010/sep/KN_sep2010.pdf

Classification and Pathophysiology of CRS• Acute cardiorenal syndrome (type 1) - Acute worsening of heart function leading to kidney injury and/or dysfunction
• Chronic cardiorenal syndrome (type 2) -Chronic abnormalities in heart function leading to kidney injury and/or dysfunction
• Acute renocardiac syndrome (type 3) -Acute worsening of kidney function leading to heart injury and/or dysfunction
http://www.asn-online.org/publications/kidneynews/archives/2010/sep/KN_sep2010.pdf

Classification and Pathophysiology of CRS
• Chronic renocardiac syndrome (type 4) - Chronic kidney disease leading to heart injury, disease, and/or dysfunction
• Secondary cardiorenal syndrome (type 5) - Systemic conditions leading to simultaneous injury and/or dysfunction of heart and kidney
http://www.asn-online.org/publications/kidneynews/archives/2010/sep/KN_sep2010.pdf

High Prevalence of CKD in High Prevalence of CKD in Patients Patients Hospitalized with Acute Hospitalized with Acute Decompensated HFDecompensated HF
0
5
10
15
20
25
30
35
40
45
50
eGFR <90 60-89 30-59 15-29 < 15eGFR <90 60-89 30-59 15-29 < 15ml/min/1.73mml/min/1.73m22
Per
cen t
of
Pa t
i en t
sP
erc e
n t o
f P
a ti e
n ts
N = 118,465N = 118,465
Heywood, JT et al. J Card Fail. 2007. Aug 13(6); 422-230.
ADHEREADHERE Acute Decompensation Heart Failure National Registry
Cardiorenal Cardiorenal SyndromeSyndrome

Prevalence of LVH in the General Prevalence of LVH in the General Population and CKDPopulation and CKD
CVDisease
General Population
CKD
LVH(ECHO)
8 - 13% 25 – 50% (stage 2 – 4) 75- 85% (stage 5)
Sarnak, M et al. Circulation. 2003: 108(17) 2154-2169
Patient has long history of hypertension – LVH often Patient has long history of hypertension – LVH often the intermediate step resulting in impaired LV filling, the intermediate step resulting in impaired LV filling, increased ventricular stiffness, and CHFincreased ventricular stiffness, and CHF
Congestive Heart Failure?Congestive Heart Failure?

Congestive Heart Failure?Congestive Heart Failure?
• Patients with CKD have volume 10 - 30% Patients with CKD have volume 10 - 30%
increase in volume in absence of edema increase in volume in absence of edema Palmer, BF, N Eng J of Med, 2002: 347; 1256-1261
•Common LIFE THREATENING DX!!!Common LIFE THREATENING DX!!!
(CHF admissions 5x higher in CKD)(CHF admissions 5x higher in CKD) USRDS, 2004 Annual Report
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

Congestive Heart Failure?Congestive Heart Failure?• Rosiglitazone may aggravate edema and CHFRosiglitazone may aggravate edema and CHF
O’Connor AS, Schelling JR. Am J Kid Dis. 2005. 46(4):766-773
• Volume overload not clearly evident on exam Volume overload not clearly evident on exam • Lungs with evidence of possible fluid so CHF Lungs with evidence of possible fluid so CHF still in differentialstill in differential
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

Anemia secondary to GI bleed or CKD?Anemia secondary to GI bleed or CKD?
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

Central Nervous SystemCentral Nervous System• FatigueFatigue• DepressionDepression• Impaired cognitive functionImpaired cognitive function
Gastrointestinal SystemGastrointestinal System• AnorexiaAnorexia• NauseaNausea
Vascular systemVascular system• Low skin temperatureLow skin temperature• Pallor of skin, mucous Pallor of skin, mucous membranes and conjunctivaemembranes and conjunctivae
Immune SystemImmune System• Impaired T-cell anImpaired T-cell an macrophage function macrophage function
Cardiorespiratory system• Exertional dyspnea• Tachycardia, palpitations• Cardiac enlargement, hypertrophy• Increased pulse pressure, systolic ejection murmur• Risk of cardiac failure
Ludwid H, et al Semin Oncol 1998, 25(Suppl 7); 2-6.
Anemia Signs and SymptomsAnemia Signs and Symptoms
Genital TractGenital Tract• Menstrual problemsMenstrual problems• Loss of libidoLoss of libido

Pathophysiologic Consequences of Anemia in Pathophysiologic Consequences of Anemia in CKD: Effects on the CV SystemCKD: Effects on the CV System
Reduced HemoglobinReduced Hemoglobin
Reduced O2 DeliveryReduced O2 Delivery
Increased Cardiac WorkoutIncreased Cardiac Workout
Dilated Cardiomyopathy - Dilated Cardiomyopathy -
LVHLVH
Ischemic Heart DiseaseIschemic Heart Disease
Congestive Heart Failure
Angina Pectoris
Myocardial InfarctionAdapted from Metivier et al Nephrol, Dial, Transpl. 2000; 15 Suppl 3: 14-18.

Correction of Anemia in PatientsCorrection of Anemia in Patientswith CKD and CHFwith CKD and CHF
N = 84 Before After P Value
Hgb (g/dl) 10.4 13.1 < 0.05
NYHA 3.89 2.53 < 0.05
VAS fatigue/ SOB index 8.6 2.8 < 0.05
No. of days Hospitalizations 3.38 0.16 < 0.05
.Silverberg, DS. Perit Dial Int . 200l.; 21Suppl3 ; S236-240.

Anemia secondary to GI Bleed or CKD?Anemia secondary to GI Bleed or CKD?
• Clopidogrel and aspirin – as high as 30 % incidence of bleeding - increased risk in elderly, women, and patients with reduced kidney function uptodate.com
Stool for occult blood negativeStool for occult blood negative
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

ANEMIAANEMIA
Adapted from: Harrison, FIn Principles of Internal Medicine. 1998:334.
Red blood cellsRed blood cells OO22 delivery delivery
ErythropoietinErythropoietinErythroidErythroidmarrowmarrow
IronIron
REREcellscells
X
Erythropoietin deficiency is the most Erythropoietin deficiency is the most common cause of anemia in CKD. common cause of anemia in CKD.
RE = reticuloendothelial

Anemia Starts Early in CKD and Anemia Starts Early in CKD and Worsens with Disease ProgressionWorsens with Disease Progression
†Kausz AT, et al. Dis Manage Health Outcomes. 2002;10(8):505-513.*Obrador GT, et al. J Am Soc Nephrol. 1999;10:1793-1800.
Pre
vale
nce
of
An
emia
(%
)P
reva
len
ce o
f A
nem
ia (
%)
14%20%
43%
62%8%
8%
15%
9%
17%
15%
10%
67.5%
5%
0%
20%
40%
60%
80%
100%
< 2 2-2.9 3-3.9 > 4 *Start of Dialysis(n=131,484)
Serum Creatinine Level (mg/dL)Serum Creatinine Level (mg/dL)
33%-36%33%-36%
30%-32.9%30%-32.9% < 30%< 30%N = 1,658†

Anemia and CHFAnemia and CHF

FINAL DIAGNOSESFINAL DIAGNOSES
•Anemia of CKDAnemia of CKD
•CHF secondary to anemiaCHF secondary to anemia
Labs: Troponin < Labs: Troponin < 0.03 µg/L0.03 µg/L
Hgb 8.2 g/dlHgb 8.2 g/dlChest X-ray - enlarged heart, pulmonary edemaChest X-ray - enlarged heart, pulmonary edema
CASE 1 – cc: “shortness of breath”CASE 1 – cc: “shortness of breath”

Brosius, FC et al. Circulation. 2006; .
“…proper management of CVD is different and more complex proper management of CVD is different and more complex
in patients with CKD”in patients with CKD”
CKD in CVDCKD in CVD

CVD Events, Hospitalization and Death are CVD Events, Hospitalization and Death are Common in CKDCommon in CKD
2.113.65
11.29
21.8
36.6
0
5
10
15
20
25
30
35
40
>60 45-59 30-44 15-29 < 15
Age-Standardized Age-Standardized Rate of Rate of
Cardiovascular Cardiovascular EventsEvents
(per 100 person-yr)(per 100 person-yr)
Estimated GFR (mL/min/1.73 m2)Go, et al., 2004
END Points:END Points:
CV Events, CV Events,
HospitalizationDeaHospitalizationDea
thth

Cardiovascular Disease is Cardiovascular Disease is Prevalent in CKDPrevalent in CKD
CVD CHF LVH
% M
ale
Pat
ient
s%
Mal
e P
atie
nts
CHD
Normal SCr (n=2591)
Elevated SCr (1.5–3.0 mg/dL n=246)
Culleton. Kidney Int. 1999;56:2214.
Framingham Heart Study

Chronic Kidney Disease is Chronic Kidney Disease is Prevalent in CVDPrevalent in CVD
0
20
40
60
CRCL< 60 < 60 60
23%
33%
45%
CAD = Coronary artery diseaseACS = Acute Coronary SyndromeCHF = Chronic heart failure
CAD = Coronary artery diseaseACS = Acute Coronary SyndromeCHF = Chronic heart failure
Ix, JH et al, JASN, 2003Anavekar, NS et al, NEJM, 2004
Shilpak, et al, JASN, 2004
Per
cent
of
Pat
ient
s w
ith
CK
DP
erce
nt o
f P
atie
nts
wit
h C
KD
CHFGFR < 60
DIG. In HF
ACSGFR < 60
VALLIANT
CADCRCL < 60
Heart and Soul
N=
68000 N=
14527 N=
431

• 37,173 individuals screened 2000-2003 in Kidney Early Evaluation Program (KEEP)
• Ave age 52.9, h/o DM, HTN, or CKD on survey
• Followed (max 47.7 months)
“Anemia, (decreased) eGFR, and microalbuminuria were independently associated with CVD, and when all 3 were present, CVD was common and survival was reduced.”
CKD and CVDCKD and CVD
McCullough, PA et al. Arch. Of Int Med. 2007. .
• 13,826 individuals screened between 1987 – 1990
(Atherosclerosis Risk in Community Study and the Cardiovascular Health Study)
• Ave age 57.6• Followed at 3 year intervals (average of 9.3 years)
• BP and Cr. were measured to track decline in kidney function
CVD and CKDCVD and CKD
Elsayed, E et al. 2007. Arch. Of Int Med. 2007. .
“Cardiovascular disease is independently associated with kidney function decline and with the development of kidney disease.”

Traditional Risk FactorsTraditional Risk Factorsfor Cardiac Diseasefor Cardiac Disease
TraditionalTraditional• HypertensionHypertension• DiabetesDiabetes• AgeAge• SmokingSmoking• DyslipidemiaDyslipidemia• ObesityObesity• InactivityInactivity• Family HistoryFamily History• LVHLVH
Sarnak. Am J Kidney Dis. 2000;35(suppl 1):S117Block. Am J Kidney Dis. 1998;131:607
Kitiyakara. Curr Opin Nephrol Hypertens. 2000;9:477

Risk Factors for Cardiac Risk Factors for Cardiac Disease in Patient with CKDDisease in Patient with CKD
TraditionalTraditional• HypertensionHypertension• DiabetesDiabetes• AgeAge• SmokingSmoking• DyslipidemiaDyslipidemia• ObesityObesity• InactivityInactivity• Family HistoryFamily History• LVHLVH
Non-Traditional (Kidney)Non-Traditional (Kidney)• GFR < 60 ml/minGFR < 60 ml/min• Proteinuria/hypoalbuminProteinuria/hypoalbumin• AnemiaAnemia• Inflammation Inflammation (( CRP) CRP)• Oxidative stressOxidative stress• HyperhomocysteinemiaHyperhomocysteinemia• Disorders of mineral Disorders of mineral
metabolismmetabolism• Fluid overloadFluid overload• Uremic toxinsUremic toxins• Electrolyte imbalanceElectrolyte imbalance• MalnutritionMalnutrition• Thrombogenic factorsThrombogenic factors
Sarnak. Am J Kidney Dis. 2000;35(suppl 1):S117Block. Am J Kidney Dis. 1998;131:607
Kitiyakara. Curr Opin Nephrol Hypertens. 2000;9:477
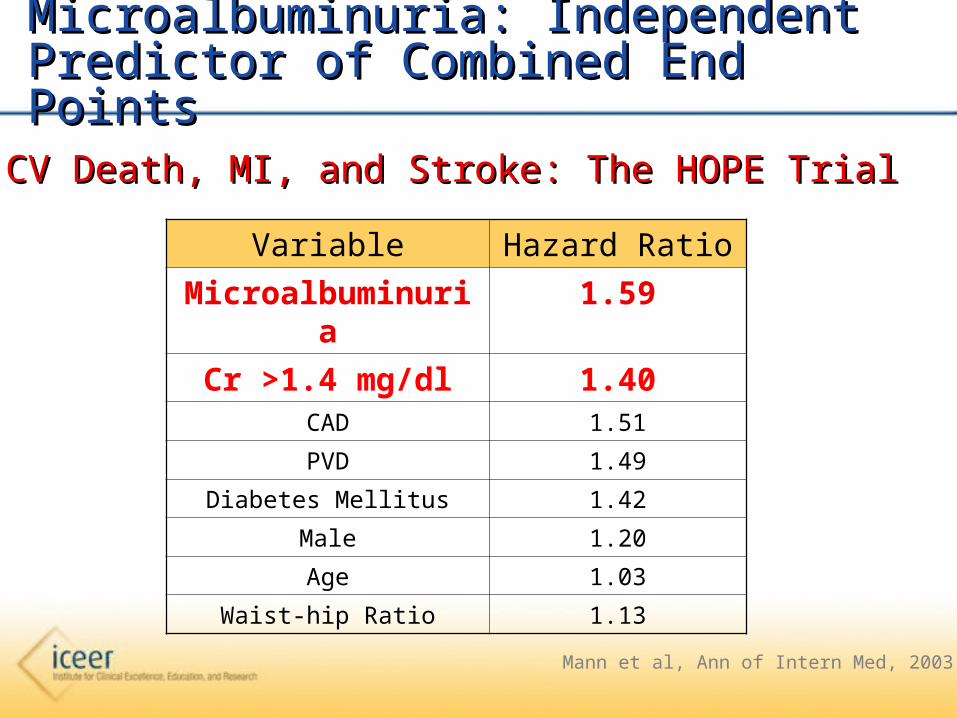
Microalbuminuria: Independent Predictor of Microalbuminuria: Independent Predictor of Combined End PointsCombined End Points
CV Death, MI, and Stroke: The HOPE TrialCV Death, MI, and Stroke: The HOPE Trial
Variable Hazard Ratio
Microalbuminuria 1.59
Cr >1.4 mg/dl 1.40CAD 1.51
PVD 1.49
Diabetes Mellitus 1.42
Male 1.20
Age 1.03
Waist-hip Ratio 1.13
Mann et al, Ann of Intern Med, 2003

Proteinuria is Associated withProteinuria is Associated withAdverse CV Outcomes – LIFE studyAdverse CV Outcomes – LIFE study
0
0.5
1
1.5
2
2.5
3
3.5
Composite EndPoint
CV Mortality All-causeMortality
Stroke MI
Adj
u ste
d H
azar
d R
atio
Adj
ust e
d H
azar
d R
atio
N= 7143
Watchtell et al, Ann of Intern Med, 2003
<2.2 mg/g>83.3 mg/g

AlbuminuriaAlbuminuria
• In a population-based study (subset n = 9000) the In a population-based study (subset n = 9000) the presence of albuminuria enhanced the presence of albuminuria enhanced the predictivepredictivevalue of ST-T segment changes in a restingvalue of ST-T segment changes in a restingECG for all-cause and CVD mortality. ECG for all-cause and CVD mortality.
• The impact of the presence of microalbuminuriaThe impact of the presence of microalbuminuriaon all-cause mortality was greater than other more on all-cause mortality was greater than other more traditional cardiac risk factors including traditional cardiac risk factors including hypertension, hypercholesterolemia, cigarette hypertension, hypercholesterolemia, cigarette smoking, obesity, and diabetessmoking, obesity, and diabetes..
Diercks et al, JACC, 2002
Prevend StudyPrevend Study
Microalbuminuria – CV Risk Factor?Microalbuminuria – CV Risk Factor?
• Despite the fact that the Framingham study Despite the fact that the Framingham study established in 1984 that proteinuria is an important established in 1984 that proteinuria is an important risk marker of CV mortality in the general risk marker of CV mortality in the general population, albuminuria has never been added to population, albuminuria has never been added to the list of important CV risk factors.the list of important CV risk factors.
• Confirmed by Arnlov et al, persons with normal Confirmed by Arnlov et al, persons with normal BP, without DM and normal GFR – BP, without DM and normal GFR – microalbuminuria is a strong predictor of CV microalbuminuria is a strong predictor of CV outcome.outcome.
Kannel, A Heart J,108,1984
Arnlov et al, Circulation, 2005

Albuminuria — So WHAT?Albuminuria — So WHAT?
LIFE STUDY LIFE STUDY
Reducing Proteinuria independent of BPReducing Proteinuria independent of BPdecreased CVD risk (endpoints CV mortality, stroke, MI)decreased CVD risk (endpoints CV mortality, stroke, MI) Ibsen, et al, Hypertension 45, 2005
PREVEND-IIPREVEND-II
Patients with albuminuria treated with fosinopril decreased Patients with albuminuria treated with fosinopril decreased CV events compared to patients on pravastatin CV events compared to patients on pravastatin
Asselbergs et al Circulation 110, 2004
RENAAL RENAAL
Patients treated with ARB showed significant decreased risk Patients treated with ARB showed significant decreased risk of CV endpoints with any decrease in albuminuria. of CV endpoints with any decrease in albuminuria.
deZeeuw, et al , KI, 2004.

Chronic Kidney Disease is a Risk FactorChronic Kidney Disease is a Risk Factorfor Cardiovascular Diseasefor Cardiovascular Disease
Sarnak et al. Circulation. 2003;108:2154-2169.

CASE 2CASE 2
Case:Case:– Diane, 63-year-old , 66-kg body weightDiane, 63-year-old , 66-kg body weight
– Hospitalized March & April,Hospitalized March & April,Hct 16%, GI work-up negative,Hct 16%, GI work-up negative,TransfusedTransfused
– May, Adm. with weaknessMay, Adm. with weaknessHct 27.5%, K+ 6.9 mg/dl,Hct 27.5%, K+ 6.9 mg/dl,Creatinine 1.3 mg/dlCreatinine 1.3 mg/dl
– Nephrology consultNephrology consult

CASE 2CASE 2
Case:Case:
– What if any level of kidney disease?What if any level of kidney disease?
NoneNone
Mild (GFR 60-90)Mild (GFR 60-90)Moderate (GFR 30- 60)Moderate (GFR 30- 60)Severe (GFR 15-30)Severe (GFR 15-30)Kidney failure (GFR <15)Kidney failure (GFR <15)

CASE 2
Use Prediction EquationMDRD formula (simplified)
Case:
– 63-year-old,non-African American, femaleSCr = 1.3 mg/dL
• Formula result:– eGFR= 44 mL/min/1.73m2
Stage 3 Moderate Kidney DiseaseStage 3 Moderate Kidney Disease

Estimate GFR from Prediction EquationsEstimate GFR from Prediction Equations
• Cockcroft-Gault equation (www.clinicalculator.com/english/nephrology/cockcroft/cc.htm)
CrCl (ml/min) = [(140 – age) x IBW
(kg)]/(72 x SCr) x (.85 if female)
• MDRD equation (www.kidney.org/professionals/kdoqi/gfr_calculator.cfm)
GFR (ml/min/1.73m2 ) = 186 x (SCr)-1.154 x (age)-0.203 x
x (0.742 if female) x (1.210) if African-American
Cockcroft, DW and Gault, MH.. Nephron. 1976; 16:31-41...Levey et al, J AM Soc Nephrol. 2000; 11:155A.
.

Serum Creatinine Is Inaccurate in Serum Creatinine Is Inaccurate in Predicting Kidney FunctionPredicting Kidney Function
Age Gender RaceSCr
(mg/dL)
eGFR (mL/min/1.73
m2)
CKD Stage
20 M B 1.3 91 1*
20 M W 1.3 75 2*
55 M W 1.3 61 2*
20 F W 1.3 56 3
40 F B 1.3 48 3
63(Case 2)
F W 1.3 44 3
B = black; W = all ethnic groups other than black;*With evidence of kidney damage. Duncan, L et al. Nephrol Dial Transplant. 2001; 16(5): 1042-1046
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266..

What is Chronic Kidney Disease?What is Chronic Kidney Disease?
Kidney damage (structural or functional*)Kidney damage (structural or functional*)
or GFR or GFR << 60 ml/min/1.73 m 60 ml/min/1.73 m22
for greater than 3 monthsfor greater than 3 months
* structural – i.e cysts, obstructionfunctional – hematuria, proteinuria
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266..

NKF-KDOQI Staging Classification of CKDNKF-KDOQI Staging Classification of CKD
Stage Description GFR
1Chronic kidney damage with
normal GFR>90–120 mL/min/1.73
m2
2 Mild GFR 60–89 mL/min/1.73 m2
3 Moderate GFR 30–59 mL/min/1.73 m2
4 Severe GFR15–29 mL/min/1.73 m2
5 Kidney failure<15 mL/min/1.73 m2
ordialysis
National Kidney Foundation. Am J Kidney Dis. 2002;39(suppl 1):S1-S266.
eGFR (mL/min/1.73 m2) * May be normal for age

CKD by Diagnoses (Simplified)CKD by Diagnoses (Simplified)
• Diabetic kidney disease• Non-diabetic kidney diseases
Vascular diseases (Hypertension)
Glomerular diseasesTubointerstitial diseasesCystic diseases
• Diseases in Transplant
… Always Pursue EtiologyNational Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1):S1-S266.

Eliminate Reversible CausesEliminate Reversible Causes
• May be superimposed on CKDMay be superimposed on CKD• Evaluate and correct potentially reversible Evaluate and correct potentially reversible causescauses
of a kidney injury:of a kidney injury:- Decreased renal perfusion – - Decreased renal perfusion –
hypovolemia, hypovolemia, hypotension, or drug hypotension, or drug induced (ACEi, ARB)induced (ACEi, ARB)
- Nephrotoxic agents- Nephrotoxic agents - Acute interstitial nephritis- Acute interstitial nephritis - Urinary tract obstruction- Urinary tract obstruction - Heart failure, liver disease- Heart failure, liver disease
- Other- Other
Schieppati, A et al. In: Primer on Kidney Disease. 2005: p.444.
Acute Renal Failure (ARF)Acute Renal Failure (ARF)

CKD IS A PROGRESSIVE DISEASECKD IS A PROGRESSIVE DISEASE
KidneyKidneyDamageDamage
22 33 44
120120 9090 6060 3030 1515
11StageStage 55
eGFReGFR
KidneyDamage
KidneyFailure
Mild KidneyFunction
Moderate KidneyFunction
Severe KidneyFunction
Timely evaluation and treatment may improve outcomesTimely evaluation and treatment may improve outcomes.

The Chronic Kidney Disease EpidemicThe Chronic Kidney Disease Epidemic
5.6 5.7
7.4
0.3 0.45*
0123456789
10
1 2 3 4 5
Mill
ions
of
People
eGFR = estimated glomerular filtration rate.*2003. Coresh et al. J Am Soc Nephrol. 2005;16:180-188; United States Renal Data System (USRDS) 2005 Annual Data Report. Available at: www.usrds.org; USRDS 2005 Annual Data Report. The data reported here have been supplied by the USRDS. The interpretation andreporting of these data are the responsibility of the author(s) and in no way should be seen as an official policy or interpretation ofthe U.S. government. Available at: www.usrds.org. Accessed December 6, 2005.
≥90 60-89 30-59 15-29 <15
CKD Stage
eGFR (mL/min/1.73 m2)
CKD Affects 12% of the US PopulationCKD Affects 12% of the US Population

CKD Patients Are More Likely CKD Patients Are More Likely to Die Than Progress to ESRDto Die Than Progress to ESRD
Percentage Who Remained Event-Free vs. Death vs.Percentage Who Remained Event-Free vs. Death vs.Developed ESRD During 5-Year Follow-UpDeveloped ESRD During 5-Year Follow-Up
10%20% 24%
46%
75%63%
64%
28%
15% 16% 10% 7%
20%
1%
0%
20%
40%
60%
80%
100%
Stage I Stage II Stage III Stage IV
% o
f P
atie
nts
DisenrolledEvent-freeRRTDied
Totals Stage 2-4Totals Stage 2-4
3.1% RRT3.1% RRT
24.9 % Die24.9 % Die
Keith D, et al. J Am Soc Nephrol. 2002;13:620A.
N= 27,000

Screening and Detection of CKDScreening and Detection of CKD
• WHO to screen? – identify risk factors • HOW to screen? - History
- Measure BP and glucose - Urinalysis – hematuria, proteinuria- Measure urinary albumin or protein excretion- eGFR - use prediction equation
• WHEN to screen?
Screening is the beginning of a complex Screening is the beginning of a complex management process for CKDmanagement process for CKD..
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.

Identify Risk Factors: Individual Predictors of Identify Risk Factors: Individual Predictors of New-Onset Kidney DiseaseNew-Onset Kidney Disease
0
1
2
3
4
5
BMI Smoking HTN Age Diabetes
Community Based Population N = 2585 Community Based Population N = 2585 Baseline Exam 1978-82; FU- 18 yrs.Baseline Exam 1978-82; FU- 18 yrs.
Fox et al JAMA, 2004; 291(7): 844-50.
Odd
s R
atio
Ris
k of
Dev
elop
ing
CK
D
WHO to screen?

• DiabetesDiabetes
• HypertensionHypertension
• Aging (>60 years old)*Aging (>60 years old)*• Racial-ethnic backgroundRacial-ethnic background
(African American, Native American, Asian American,(African American, Native American, Asian American,Pacific Islander, Latin American, Hispanic)Pacific Islander, Latin American, Hispanic)
• Family history of kidney diseaseFamily history of kidney disease
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.*Coresh, J et al, Am J Kidney Dis, 2003; 41(1):1-12..
WHO to screen?
Risk Factors for CKD - Early DetectionRisk Factors for CKD - Early Detection

Risk Factors for CKD - Early DetectionRisk Factors for CKD - Early Detection
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.Fox et al JAMA, 2004; 291(7): 844-50.
Mohanram, A et al. Kidney Int. 2004; 66: 1131-1138.Kurella, M et al. J Am Soc Nephrol. 2005; 16: 2134-2140.
• Tobacco UseTobacco Use
• Low Income/Education/ Low Income/Education/ Poor access to healthcarePoor access to healthcare
• UTI, Urinary stones, lower UTI, Urinary stones, lower UT obstructionUT obstruction
• Autoimmune diseaseAutoimmune disease
• ARF – recoveryARF – recovery
• NeoplasiaNeoplasia
• AnemiaAnemia
• Insulin resistanceInsulin resistance
• Reduced kidney massReduced kidney mass
• High-protein dietHigh-protein diet
• HyperlipidemiaHyperlipidemia
• AtherosclerosisAtherosclerosis
• ObesityObesity
• Nephrotoxin exposureNephrotoxin exposure
– NSAIDSNSAIDS
– Contrast dyeContrast dye
• Hazardous chemical or Hazardous chemical or environmental exposureenvironmental exposure
WHO to screen?
Brosius, FC et al. Circulation. 2006; .
“…“…all patients with CVD should be screened for CKD”all patients with CVD should be screened for CKD”
WHO to screen?

• History – clues (i.e. recent infections, symptoms during urination, skin rash, arthritis, heart failure, family history, medications)
• Blood pressure –high blood pressure is both a risk factor and an early complication, often first sign of kidney damage
• Abnormal serum glucose – early factor• Urinalysis – hematuria or proteinuria
Screening and Detection of CKDScreening and Detection of CKD
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.
HOW to screen?

Measure Urinary Albumin or Protein Excretion
• Untimed, “spot” urine for albumin- or protein-to-creatinine ratio (first-morning-void preferred)
• 24- hour urine collection for microalbumin, albumin, or protein acceptable (note: measure creatinine also to determine if collection is accurate)
• Advantages of random urine vs. 24 hour urine: lower cost and ease of collections
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1):S1-S266.
HOW to screen?HOW to screen?

Screening for Microalbuminuria, Screening for Microalbuminuria, Albuminuria or ProteinuriaAlbuminuria or Proteinuria
• Microalbuminuria:Microalbuminuria:
30 - 300 mg of albumin/g of creatinine (.03-.30)30 - 300 mg of albumin/g of creatinine (.03-.30)
• Macroalbuminuria:Macroalbuminuria:
>> 300 mg albumin/g of creatinine (.30) 300 mg albumin/g of creatinine (.30)
• Proteinuria: Proteinuria:
> 200 mg protein/g creatinine (.20)> 200 mg protein/g creatinine (.20)
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.National Kidney Foundation. Am J Kidney Dis.2007; 49(suppl 2): S1-S179.
HOW to screen?HOW to screen?

Glomerular Filtration Rate (GFR)Glomerular Filtration Rate (GFR)
• GFR – Best overall index of kidney GFR – Best overall index of kidney function in health and diseasefunction in health and disease
• Normal GFR varies according to Normal GFR varies according to age, sex, and body sizeage, sex, and body size
• Normal – 120 to 130 mL/min/1.73mNormal – 120 to 130 mL/min/1.73m22 in young adults, declines with agein young adults, declines with age
• Estimate GFR from prediction Estimate GFR from prediction equationsequations
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266..
HOW to screen?HOW to screen?

Screening and Detection of CKD
• Measure annually for microalbuminuria in patients at risk for CKD (including pts with CVD)
• Measure for microalbuminuria in patients with DM - at diagnosis for type 2 diabetes
- after 5 years for type 1 diabetes• Measure serum creatinine annually in patients at risk for CKD and calculate eGFR (automatic on many labs and required by law in some states)
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.www.cdc.gov/MMWR?PDF?wk/mm5610.pdf.
WHEN to screen?

KidneyKidneyDamageDamage
22 33 44
120120 9090 6060 3030 1515
11StageStage 55
eGFReGFR
KidneyKidneyDamageDamage
KidneyKidneyFailureFailure
MildMild KidneyKidneyFunctionFunction
ModerateModerate KidneyKidneyFunctionFunction
SevereSevere KidneyKidneyFunctionFunction
What Would Your Strategy Be What Would Your Strategy Be to Slow Progression of CKD?to Slow Progression of CKD?
Early Detectionof CKD
Delay progression
BP ControlTreat
Proteinuria
DM/BS control
Avoid Nephrotoxins
Prevent complications
Anemia
Malnutrition
Bone Disease
Acidosis
Treat co- morbidities
Cardiovascular disease
Hypertension
Diabetes
Prepare for RRTEducate patient
Select RRT modality
Determine access and initiate
dialysis in a timely fashion
Adapted from Pereira, B.. Kid Int. 2000;57:351-365.
Lifestyle
Treat Dyslipidemia
Targets for Treatment - CKDTargets for Treatment - CKD

• Hypertension is an independent Hypertension is an independent variable that predicts long-term variable that predicts long-term decline in kidney functiondecline in kidney function
• Proteinuria is also an independent Proteinuria is also an independent variable that predicts long-term variable that predicts long-term decline in kidney functiondecline in kidney function
• Both are targets to reduce CKD Both are targets to reduce CKD progressionprogression
National Kidney Foundation. Am J Kidney Dis. 2004; 43(suppl 1): S1-S290..
Delay Progression: Delay Progression: Targets: Hypertension and ProteinuriaTargets: Hypertension and Proteinuria

Lower Mean BP Results in Slower Rates of Lower Mean BP Results in Slower Rates of Decline in GFRDecline in GFR (Diabetics and Non-Diabetics)(Diabetics and Non-Diabetics)
9595 9898 101101 104104 107107 110110 113113 116116 119119
r = 0.69; P < 0.05
MAP (mmHg)
GF
R (
mL
/min
/yea
r)
130/85 140/90
UntreatedHTN
00
-2-2
-4-4
-6-6
-8-8
-10-10
-12-12
-14-14 Parving HH, et al. Br Med J. 1989. Moschio G, et al. N Engl J Med. 1996.Viberti GC, et al. JAMA. 1993. Bakris GL, et al. Kidney Int. 1996.Klahr S, et al. N Eng J. Med 1994. Bakris GL. Hypertension. 1997.Hebert L, et al. Kidney Int. 1994. The GISEN Group. Lancet. 1997.Lebovitz H, et al. Kidney Int. 1994.
Bakris GL, et al. Am J Kidney Dis. 2000;36(3):646-661.
Slide source: hypertensiononline.org

,
130/80 mm Hg DM/CKD130/80 mm Hg DM/CKD(JNC VII, NKF)(JNC VII, NKF)))
130/80 mm Hg 130/80 mm Hg or lower or lower (NKF)(NKF)))
Without Proteinuria
GOAL:GOAL: With Proteinuria
DelayDelay Progression: Progression: Targets: Hypertension and ProteinuriaTargets: Hypertension and Proteinuria
National Kidney Foundation. Am J Kidney Dis. 2004; 43(suppl 1): S1-S290.Chobanian et al, JAMA, 2003; 289: 2560-2572.
GOAL:GOAL: Proteinuria < 500 – 1000 mg/day Urine protein-to-creatinine ratio < .5 – 1.0

Delay Progression: Delay Progression: Targets: Hypertension and ProteinuriaTargets: Hypertension and Proteinuria
Weight LossWeight Loss 10 kg loss10 kg loss 5-20 mm Hg5-20 mm Hg
DASH DietDASH Diet Diet rich in fruit Diet rich in fruit vegetablesvegetables
8 –14 mm Hg8 –14 mm Hg
Low-sodium Low-sodium DietDiet
Restrict sodium Restrict sodium intakeintake
2 – 8 mm Hg2 – 8 mm Hg
Physical Physical ActivityActivity
30 minutes/day 30 minutes/day most daysmost days
4 – 9 mm Hg4 – 9 mm Hg
Moderate Moderate alcohol alcohol consumptionconsumption
2 drinks/day men 2 drinks/day men 1 1 drink/day/womendrink/day/women
2 – 4 mmHg2 – 4 mmHg
Lifestyle modificationsLifestyle modifications
Chobanian et al, JAMA. 2003; 289: 2560-2572.

Brenner. N et al. N Engl J Med. 2001;345:861.
0
5
10
15
20
25
30
% R
educt
ion in
Ris
k
Primary EndPoint
Doubling ofSCr
Progression toESRD
*
†**
* P = 0.02 † P =0.006**P =0.002
Renoprotection with ARBRenoprotection with ARB
16%
28%
25%
Type 2 Diabetes: RENAALType 2 Diabetes: RENAAL

CALM: Reductions from Baseline in Urinary CALM: Reductions from Baseline in Urinary Albumin: Creatinine Ratio (Week 24)Albumin: Creatinine Ratio (Week 24)
Change in Change in Urinary Urinary
Albumin: Albumin: Creatinine Creatinine Ratio, %Ratio, %
Candesartan 16 mg
Lisinopril
20 mg
Both
*P = 0.05 from baseline.†P < 0.001 from baseline.
–60
–50
–40
–30
–20
–10
0
*
†
†
Mogensen CE et al. BMJ.2000;321:1440–1444.

• At start up or change in ACE inhibitor/ARB dose, check creatinine and potassium within 2 weeks
• If eGFR decreases > 30% over 4 months then decrease or discontinue ACEi/ARB. Consider renal artery stenosis (RAS)
• IF K+ , dietary counseling, diuretics, HCO3 replacement, avoid herbals
Slow Progression: Slow Progression: Target: Hypertension and ProteinuriaTarget: Hypertension and ProteinuriaSlow Progression: Slow Progression: Target: Hypertension and ProteinuriaTarget: Hypertension and Proteinuria
Increased risk of side-effects in Increased risk of side-effects in patients with CKDpatients with CKD
National Kidney Foundation. Am J Kidney Dis. 2004; 43: S1-S290

• Avoid CCBs - Dihydropyridine, effective in lowering BP but can cause increased proteinuria
• Extreme caution with Aldactone and K+ sparing meds
• NSAIDS – block prostaglandin metabolism, ( renin - renin - aldosterone - aldosterone - K+) )
sodium retention, exacerbate volume overload, and nephrotoxicity
Slow Progression: Slow Progression: Target: Hypertension and ProteinuriaTarget: Hypertension and ProteinuriaSlow Progression: Slow Progression: Target: Hypertension and ProteinuriaTarget: Hypertension and Proteinuria
Increased risk of side-effects in Increased risk of side-effects in patients with CKDpatients with CKD
National Kidney Foundation. Am J Kidney Dis. 2004; 43: S1-S290

Slow Progression Slow Progression Target: Diabetic Kidney DiseaseTarget: Diabetic Kidney Disease
Complication RR(95% CI)
Risk Reducti
on
p Value
Cardiovascular
end point
0.47(0.24-0.73)
53% .008
Nephropathy 0.38(0.17-0.87)
61% .003
Retinopathy 0.42(0.21-0.86)
58% .02Gaede, et al, N Engl. J Med. 2003; 348(5): 383-393.

Slow Progression Slow Progression Target: Diabetic Kidney DiseaseTarget: Diabetic Kidney Disease
• Reduce BP to <130/80 mmHgReduce BP to <130/80 mmHg
• Use multiple antihypertensive drugs (ACE Use multiple antihypertensive drugs (ACE inhibitor, ARB, diuretic, CCB, beta-inhibitor, ARB, diuretic, CCB, beta-blocker)blocker)
• Maximal reduction of proteinuriaMaximal reduction of proteinuria
• Treat hyperlipidemia (LDL <100 mg/dL)Treat hyperlipidemia (LDL <100 mg/dL)
• Stop cigarette smokingStop cigarette smoking
American Diabetes Association. Diabetes Care 2008;31(suppl 1): S1-S42National Kidney Foundation. Am J Kid Dis. 2007; 49(suppl2): S1-S179.

Slow Progression Slow Progression Target: Diabetic Kidney DiseaseTarget: Diabetic Kidney Disease
• Insulin half-life prolonged with decreased GFR Insulin half-life prolonged with decreased GFR • Treatment cautions in CKD:Treatment cautions in CKD:
Adjust all agents to avoid hypoglycemiaAdjust all agents to avoid hypoglycemia
NoNo MetforminMetformin (eGFR < 40 ml/min/1.73m (eGFR < 40 ml/min/1.73m22) ) - lactic acidosis - lactic acidosis
SulfonylureasSulfonylureas accumulate in kidney failure accumulate in kidney failure (glipizide preferred agent) (glipizide preferred agent) GlitazoneGlitazones may aggravate edema and CHFs may aggravate edema and CHF
O’Connor, AS & Schelling, JR. Am J Kid Dis. 2005; 46(4): 766-773.American Diabetes Association. Diabetes Care 2008;31(suppl 1): S1-S41

Slow Progression:Slow Progression:Target: Avoid NephrotoxinsTarget: Avoid Nephrotoxins
• NSAIDs are potentially nephrotoxicNSAIDs are potentially nephrotoxic• Avoid other nephrotoxins Avoid other nephrotoxins
– iodinated radiocontrast, – iodinated radiocontrast, aminoglycosides, amphotericin B, aminoglycosides, amphotericin B, cyclosporin, tacrolimus, ?colascyclosporin, tacrolimus, ?colas
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.
• Prevention of contrast induced Prevention of contrast induced nephropathy - oral N-nephropathy - oral N-acetylcysteine (600 mg) before acetylcysteine (600 mg) before and after; sodium bicarbonate and after; sodium bicarbonate infusion (154 meq/L – infusion (154 meq/L – 3/mL/kg/hr 1 before and 6 hours 3/mL/kg/hr 1 before and 6 hours postpost
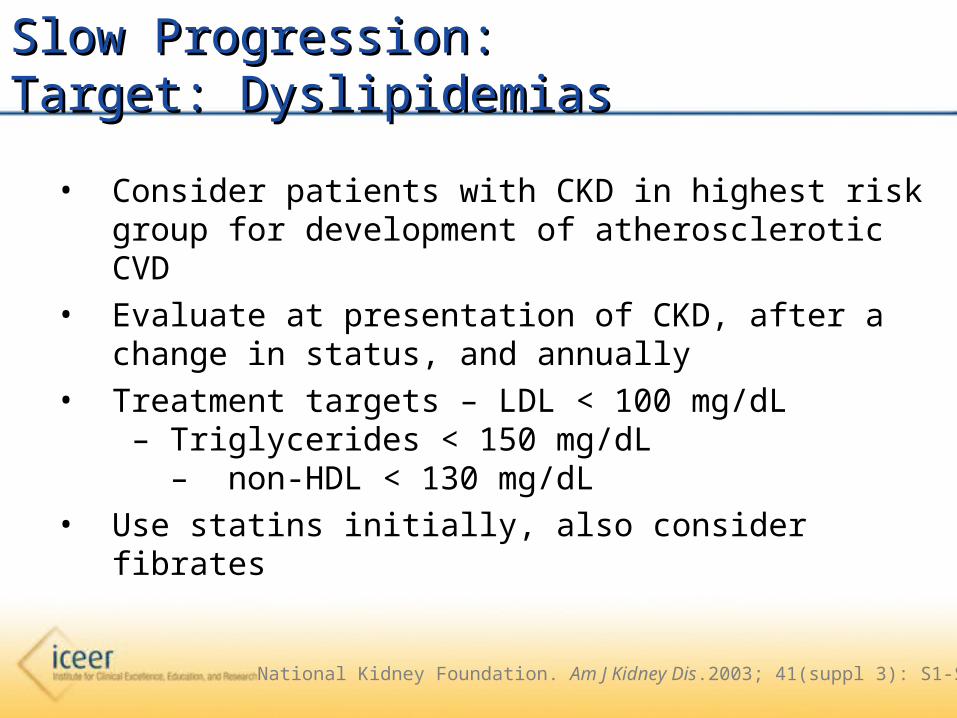
Slow Progression:Slow Progression:Target: DyslipidemiasTarget: Dyslipidemias
• Consider patients with CKD in highest risk group for development of atherosclerotic CVD
• Evaluate at presentation of CKD, after a change in status, and annually
• Treatment targets – LDL < 100 mg/dL – Triglycerides < 150
mg/dL – non-HDL < 130 mg/dL
• Use statins initially, also consider fibrates
National Kidney Foundation. Am J Kidney Dis.2003; 41(suppl 3): S1-S91.

Delay Progression:Delay Progression:Target: Lifestyle ChangesTarget: Lifestyle Changes
• Stop smoking
• Exercise
• Sodium restriction
2- 3 g/day of sodium
• Fluid restriction
• Potassium restriction – low K+ diet if elevated
• Consider dietary protein restriction:
– Microalbuminuria: 0.8 g/kg/day
– Decreasing GFR: 0.6 g/kg/day .
National Kidney Foundation. Am J Kidney Dis.2002; 39(suppl 1): S1-S266.

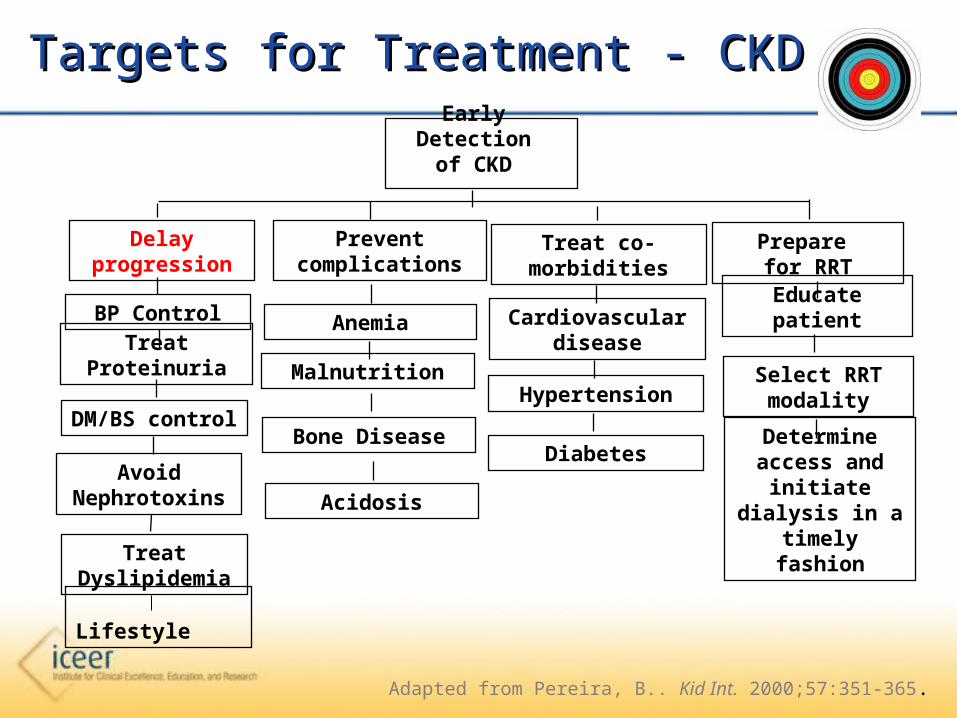
Early Detectionof CKD
Delay progression
BP ControlTreat
Proteinuria
DM/BS control
Avoid Nephrotoxins
Prevent complications
Anemia
Malnutrition
Metabolic Bone Disease
Acidosis
Treat co- morbidities
Cardiovascular disease
Hypertension
Diabetes
Prepare for RRTEducate patient
Select RRT modality
Determine access and initiate
dialysis in a timely fashion
Adapted from Pereira, B.. Kid Int. 2000;57:351-365.
Lifestyle
Treat Dyslipidemia
Targets for Treatment - CKDTargets for Treatment - CKD

Disturbances of Ca++, PO4, PTH, and Vitamin D
Ca = calcium; CVD = cardiovascular disease; P = phosphorus; SHPT = secondary hyperparathyroidism.Courtesy of Kevin Martin, MB, BCh.
PTH
Bone Disease
FracturesBone pain
Marrow fibrosisErythropoietin resistance
Serum P1,25D
Calcitriol
Renal Failure
PTH
Systemic Toxicity
CVD HypertensionInflammationCalcification
Immunological
Ca++
Decreased Vitamin D Receptors and Ca-Sensing Receptors

Vascular Calcification and CKDVascular Calcification and CKD
Patient Without CKD
Intimal Calcification Secondary to
Atherosclerosis
Medial Calcification Secondary to CKD
Patients With CKD
Ca Deposition
Rib
Vertebra
EBCT Indicating Coronary Calcification
Raggi P. Clin Nephrol. 2000;54:325-333.
EBCT=electron beam computed tomography.

Pi Cbfa-1
SMC genes
NPC
PiNa Increasing Phosphate
Ca/P loadedmatrix vesicles
AP
alkaline phosphatase
calcium-binding proteinscollagen-rich ECM
Vascular Smooth Muscle Cell
Giachellli, CM, AJKD ,2001
Matrix Mineralization

EBCT Scores and EBCT Scores and Cardiovascular Risk Cardiovascular Risk in the General Populationin the General Population Mayo Clinic EBCT Guidelines
EBCT=Electron Beam Computed TomographyCV=Cardiovascular
Rumberger JA, Brundage BH, Rader DJ, Kondos G. Mayo Clin Proc. 1999;74:243-252.
EBCT Score
Plaque Burden
Implication for CV Risk
Recommendations
<10<10 MinimalMinimal LowLow Reassurance, Reassurance, educationeducation
11-10011-100 Definite, Definite, mildmild
ModerateModerate Counseling for Counseling for primary prevention; primary prevention; daily ASAdaily ASA
101-400101-400 Definite, Definite, moderatemoderate
Moderately Moderately highhigh
Institute risk Institute risk factor modification factor modification and secondary and secondary prevention prevention
>400>400 ExtensiveExtensive HighHigh Institute aggressive Institute aggressive risk factor risk factor modificationmodification

Risk of Cardiovascular Calcification Risk of Cardiovascular Calcification is Increased in Dialysis Patientsis Increased in Dialysis Patients
Mean total coronaryartery calciumscore*
Non-dialysis, no CAD (N=22)Non-dialysis, CAD (N=80)Dialysis (N=49)
Age (years)
0
500
1000
1500
2000
2500
28-39 40-49 50-59 60-69
High CV risk†
*Determined by electron beam
computed tomography (EBCT)CAD=Coronary Artery Disease
†
Braun J, Oldendorf M, Moshage W, Heidler R, Zeitler E, Luft FC. Am J Kidney Dis. 1996;27:394-401.

Framingham Heart Study: Coronary Artery Calcification (CAC) Increase as GFR Declines
*Median CAC (solid lines) and interquartile GFR ranges (boxes) are presented.•319 subjects (162men/157 women) from the Framingham Heart Study who were free of symptomatic cardiovascular disease•Coronary artery calcification (CAC) was evaluated by electron-beam computed tomography( EBCT)•Correlation was significant when adjusting for age, sex, body mass index, hypertension and total cholesterol

Treat Disorders of Bone andTreat Disorders of Bone andMineral MetabolismMineral Metabolism
• Check iPTH and (25)OH DCheck iPTH and (25)OH D22 levels annually starting levels annually starting
in stage 2 CKD in stage 2 CKD
• Treat low (25)OH DTreat low (25)OH D22 levels with ergocalciferol levels with ergocalciferol
50,000 IU q mon x 6, cholecalciferol 1000 IU/day50,000 IU q mon x 6, cholecalciferol 1000 IU/day• Treat iPTH with activated Vitamin DTreat iPTH with activated Vitamin D
• Monitor Ca and POMonitor Ca and PO44 levels and keep in normal levels and keep in normal
ranges for labranges for lab
National Kidney Foundation.. Am J Kidney Dis. 2003; 42(suppl 3): S1-S201.

Cardiovascular Disease Mortality General Cardiovascular Disease Mortality General Population vs. ESRD PatientsPopulation vs. ESRD Patients
Age (years)Age (years)
Ann
ual C
VD
Mor
talit
y (%
)A
nnua
l CV
D M
orta
lity
(%)
0.001
0.01
0.1
1
10
100
25-34 35-44 45-54 55-64 66-74 75-84 >85
Dialysis Female
Dialysis Black
Dialysis White
GP Male
GP Female
GP Black
GP White
Dialysis Male
Foley RN, et al. Am J Kidney Dis. 1998;32:S112-S119.
GP: General Population.GP: General Population.

Target: CardioprotectionTarget: Cardioprotection
Initiate cardioprotective Initiate cardioprotective measures at measures at
diagnosis of CKDdiagnosis of CKD. • Traditional risk-factor reductionTraditional risk-factor reduction
Control BP and blood sugars, treat dyslipidemias, stop Control BP and blood sugars, treat dyslipidemias, stop smoking, increase physical activity, and manage weight.smoking, increase physical activity, and manage weight.
• Nontraditional CKD-related risk factor reductionNontraditional CKD-related risk factor reductionDecrease proteinuria, treat anemia and mineral and bone Decrease proteinuria, treat anemia and mineral and bone disorders, control volume overload, and correct electrolyte disorders, control volume overload, and correct electrolyte imbalances.imbalances.
National Kidney Foundation. Am J Kidney Dis. 2002;39(suppl 1):S1-S266.

KidneyKidneyDamageDamage
22 33 44
120120 9090 6060 3030 1515
11StageStage 55
eGFReGFR
KidneyKidneyDamageDamage
KidneyKidneyFailureFailure
MildMild KidneyKidneyFunctionFunction
ModerateModerate KidneyKidneyFunctionFunction
SevereSevere KidneyKidneyFunctionFunction
Primary Care, Endocrinologist, CardiologistPrimary Care, Endocrinologist, Cardiologist
NephrologistNephrologist
Early Recognition of CKD and Collaboration Early Recognition of CKD and Collaboration between Cardiology and Nephrologybetween Cardiology and Nephrology
Adapted from K/DOQI Guidelines For Bone Metabolism and Disease 2003, Bone Care market research .

CKD and CVDCKD and CVDHave One, Screen for the Other!!!Have One, Screen for the Other!!!
•Pts with CVD have increased risk for CKD and should be screened annually.
•Aggressively manage CVD and CKD risk factors and slow progression of two diseases.

Thank You! You are not just Nephrology Nurses – you are RNs who interact with our patients’ families, the public and other RNs who care for our CKD patients long before either they, or we, know they have CKD!You cancan make a difference!
