the edema syndromes - budapest nephrology...
TRANSCRIPT

THE EDEMA SYNDROMESTHE EDEMA SYNDROMES

SOME COMMON EDEMA STATESSOME COMMON EDEMA STATES
Primary renalPrimary renalNa retentionNa retention
acute GNacute GN
Arterial Arterial UnderfillingUnderfilling
systolic failuresystolic failure
pericardial constrictionpericardial constriction
late cirrhosislate cirrhosis
IVC and/or lymphatic occlusionIVC and/or lymphatic occlusion
third space disordersthird space disorders
ControversialControversial
early cirrhosisearly cirrhosis
early early nephrosisnephrosis

NaNa++ BALANCEBALANCEQUANTITATIVE DILEMMASQUANTITATIVE DILEMMAS
VariableVariable FeNaFeNaNaNa++
(mEq)(mEq) (%)(%)
~ 3000~ 3000Total body NaTotal body Na++
~ 2200~ 2200extracellularextracellular
(140 mEq/L) (180 L/24 hrs)(140 mEq/L) (180 L/24 hrs)
Filtered Na load/24 hoursFiltered Na load/24 hours(P(PNaNa) X (GFR)) X (GFR) ~ 25000 ~ 25000
~ 1%~ 1%NaNa++ intake/24 hrsintake/24 hrs(~ 5(~ 5--6 gm)6 gm)
240240


THE EDEMA ODYSSEYTHE EDEMA ODYSSEYI. SOME EARLY LANDMARKSI. SOME EARLY LANDMARKS
1. 1. ““In heart failure . . . in consequence of low arterialIn heart failure . . . in consequence of low arterialpressure, the loss of fluids by the kidney ispressure, the loss of fluids by the kidney isdiminished. The ultimate result is diminished. The ultimate result is hydremichydremic plethora.plethora.””
Starling, 1896Starling, 1896

THE EDEMA ODYSSEYTHE EDEMA ODYSSEYI. SOME EARLY LANDMARKSI. SOME EARLY LANDMARKS
1. Starling (1896): 1. Starling (1896): ““hydremichydremic plethoraplethora””
2. 2. TigerstedtTigerstedt and Bergmann (1898): a saline extractand Bergmann (1898): a saline extractfrom kidneys, termed from kidneys, termed reninrenin,, raised raised b.pb.p..

THE EDEMA ODYSSEYTHE EDEMA ODYSSEYI. SOME EARLY LANDMARKSI. SOME EARLY LANDMARKS
1. Starling (1896): 1. Starling (1896): ““hydremichydremic plethoraplethora””
2. 2. TigerstedtTigerstedt and Bergmann (1898): and Bergmann (1898): reninrenin
3. 3. ““The kidneys react to changes in the volume ofThe kidneys react to changes in the volume ofthe circulating bloodthe circulating blood””((arterial receptors were implicit in Petersarterial receptors were implicit in Peters’’ argument)argument)
Peters (1935)Peters (1935)

THE EDEMA ODYSSEYTHE EDEMA ODYSSEYTHE CARDIAC EDEMA DEBATE: 1935THE CARDIAC EDEMA DEBATE: 1935--1945 1945
4. Harrison (1935) : backward failure4. Harrison (1935) : backward failure
““DyspneaDyspnea and edema . . . can both be accountedand edema . . . can both be accountedfor by the backfor by the back--pressure theory and are notpressure theory and are notexplicable on any other basisexplicable on any other basis””
Harrison (1935)Harrison (1935)

HARRISONHARRISON’’S S ““BACKWARD FAILUREBACKWARD FAILURE””DIASTOLIC DYSFUNCTIONDIASTOLIC DYSFUNCTION
DiastolicDiastolicdysfunctiondysfunction
Left
Ven
tric
ular
Pre
ssur
eLe
ft V
entr
icul
ar P
ress
ure
Left Ventricular VolumeLeft Ventricular Volume

EDEMAEDEMATHE CARDIAC EDEMA DEBATE: 1935THE CARDIAC EDEMA DEBATE: 1935--1945 1945
5. 5. ““The signs of a marked decrease in cardiacThe signs of a marked decrease in cardiacoutput . . . may be similar to that of shockoutput . . . may be similar to that of shock””
Stead and Ebert (1942)Stead and Ebert (1942)
6. Warren and Stead (1944)6. Warren and Stead (1944)
observation: CHF patients gain weightobservation: CHF patients gain weightbefore venous pressure risesbefore venous pressure rises
conclusion: conclusion: ““In congestive failure the cardiacIn congestive failure the cardiacoutput is inadequate . . . and theoutput is inadequate . . . and thekidneys are no longer able tokidneys are no longer able toexcrete saltexcrete salt””

WARREN AND STEADWARREN AND STEAD’’S S ““FORWARD FAILUREFORWARD FAILURE””PUMP FAILUREPUMP FAILURE
CHFCHFnormalnormal
Left
Ven
tric
ular
Pre
ssur
eLe
ft V
entr
icul
ar P
ress
ure
Left Ventricular VolumeLeft Ventricular Volume
THE EDEMA ODYSSEYTHE EDEMA ODYSSEYHORMONES AND EDEMA: 1945HORMONES AND EDEMA: 1945--1950 1950
7. 7. ““ReninRenin increases with a low cardiac outputincreases with a low cardiac outputdue to a decrease in blood available to thedue to a decrease in blood available to thekidney.kidney.””
A. J. Merrill (1946)A. J. Merrill (1946)
8. 8. LeutscherLeutscher (1950): (1950): ““The preliminary observations . . .The preliminary observations . . .indicate sodiumindicate sodium--retaining factors in the urine ofretaining factors in the urine ofsome cardiac or some cardiac or nephrosisnephrosis patientspatients””

THE EDEMA ODYSSEYTHE EDEMA ODYSSEYVOLUME RECEPTORS VOLUME RECEPTORS
9. The 9. The GauerGauer--Henry reflex (1947Henry reflex (1947--51):51):positive pressure breathing: positive pressure breathing: antidiuresisantidiuresisnegative pressure breathing: water negative pressure breathing: water diuresisdiuresis
conclusion: nonconclusion: non--osmotic ADH release driven byosmotic ADH release driven byleft left atrialatrial stretch receptor releasestretch receptor release
10. 10. HyponatremiaHyponatremia following following mitralmitral commisurotomycommisurotomy
THE EDEMA ODYSSEYTHE EDEMA ODYSSEYVOLUME RECEPTORS VOLUME RECEPTORS
11. Epstein (1953): 11. Epstein (1953): ““Circulating states in which kidneysCirculating states in which kidneystend to retain sodium are characterized by inadtend to retain sodium are characterized by inadequateequatefilling of the arterial tree.filling of the arterial tree.””
12. Homer Smith (1957): 12. Homer Smith (1957): ““Volume receptors are involvedVolume receptors are involvedin sodium conservation . . . Where these receptoin sodium conservation . . . Where these receptors arers arelocated is moot (the Cheshire cat hypothesis).located is moot (the Cheshire cat hypothesis).””

BARORECEPTORS: HOMER SMITHBARORECEPTORS: HOMER SMITH’’S S CHESHIRE CATCHESHIRE CAT
High SensitivityHigh Sensitivity Lower SensitivityLower Sensitivity IntrarenalIntrarenal HepaticHepatic
Portal veinPortal veinsinusoidalsinusoidal
? significance? significance
low pressure areaslow pressure areas
left atriumleft atriumthoracic veinsthoracic veins
high pressure areashigh pressure areas
carotid sinuscarotid sinusaortic archaortic arch
JGA JGA
HemodynamicHemodynamic changeschangesNa avidityNa avidity

DEPLETIONDEPLETIONTHE VOLUME REPLETION CASCADETHE VOLUME REPLETION CASCADE
AngiotensinAngiotensin IIII CatecholaminesCatecholamines
CNSCNS AldosteroneAldosterone
ThirstThirst Na retentionNa retentionHypoperfusionHypoperfusion
ADHADH
WaterWaterretentionretention
REPLETIONREPLETION
AtriopeptinAtriopeptin PGEPGE22NitricNitricOxideOxide
EndothelinsEndothelins

KEY FACTORS IN EDEMA STATESKEY FACTORS IN EDEMA STATES
PRECIPITATING FACTORSPRECIPITATING FACTORS MANDATORY REQUIREMENTMANDATORY REQUIREMENT
Deranged Starling ForcesDeranged Starling Forces
Arterial Arterial UnderfillingUnderfilling
Altered Volume/Capacitance RatioAltered Volume/Capacitance Ratio
Primary Renal NaPrimary Renal Na++ AvidityAvidity
steadysteady--statestate
positive Napositive Na++ balancebalance

DERANGED STARLING FORCESDERANGED STARLING FORCESTHE STARLING EQUATIONTHE STARLING EQUATION
J = J = KKff ((∆∆ P P -- σσ ∆∆ ππ) ) vvThe equationThe equation
The termsThe terms JJvv = flow= flow
σσ = solute reflection coefficient= solute reflection coefficient((σσ = 0 : wholly permeable solute)= 0 : wholly permeable solute)((σσ = 1 : wholly impermeable solute)= 1 : wholly impermeable solute)
KKff = capillary permeability= capillary permeability∆∆ P = hydrostatic pressureP = hydrostatic pressure∆∆ ππ = = oncoticoncotic pressurepressure

DERANGED STARLING FORCESDERANGED STARLING FORCESσσ DISORDERSDISORDERS
SyndromeSyndrome
ARDSARDS
RhabdomyolysisRhabdomyolysis
BurnsBurns
Cyclical edemaCyclical edemasyndromesyndrome
AbnormalityAbnormality
leaky pulmonaryleaky pulmonarycapillariescapillaries
leaky muscleleaky musclecapillariescapillaries
leaky capillariesleaky capillariesloss of loss of cutaneouscutaneous
barrierbarrier
generalized capillarygeneralized capillaryleakleak
Net NaNet Na+ + BalanceBalance
++
varies c magnitude ofvaries c magnitude offluid sequestrationfluid sequestration
massive Namassive Na++ losseslosses
++

KEY FACTORS IN EDEMA STATESKEY FACTORS IN EDEMA STATES
PRECIPITATING FACTORSPRECIPITATING FACTORS MANDATORY REQUIREMENTMANDATORY REQUIREMENT
Deranged Starling ForcesDeranged Starling Forces
Arterial Arterial UnderfillingUnderfilling
Altered Volume/Capacitance RatioAltered Volume/Capacitance Ratio
Primary Renal NaPrimary Renal Na++ AvidityAvidity
steadysteady--statestate
positive Napositive Na++ balancebalance

SOME COMMON EDEMA STATESSOME COMMON EDEMA STATESPrimary renalPrimary renalNa retentionNa retention
acute GNacute GN
Arterial Arterial UnderfillingUnderfilling
systolic failuresystolic failure
pericardial constrictionpericardial constriction
late cirrhosislate cirrhosis
IVC and/or lymphatic occlusionIVC and/or lymphatic occlusion
third space disordersthird space disorders
ControversialControversial
early cirrhosisearly cirrhosis
early early nephrosisnephrosis

STARLING DERANGEMENTS (STARLING DERANGEMENTS (∆∆ P) WITH P) WITH ARTERIAL UNDERFILLINGARTERIAL UNDERFILLING
THE HEART FAILURE SYNDROMESTHE HEART FAILURE SYNDROMESFeaturesFeatures↓↓ contractility and EFcontractility and EF↑↑ endend--diastolic volumediastolic volume
demand > performancedemand > performance↓↓ volume/capacitance ratiovolume/capacitance ratio
↓↓ compliance and fillingcompliance and fillingnormal EFnormal EF““flashflash”” pulmonary edemapulmonary edema
LowLow--output Failureoutput Failure
HighHigh--output Failureoutput Failure
Diastolic failureDiastolic failure

LOW AND HIGH OUTPUT HEART FAILUREREDUCED ECV, BUT FOR DIFFERENT REASONS
ARTERIESVEINS
Normal
Lowoutputfailure
highoutputfailure

PATHOPHYSIOLOGY OF ARTERIAL PATHOPHYSIOLOGY OF ARTERIAL UNDERFILLINGUNDERFILLING
PATHOLOGIC SEQUENCEPATHOLOGIC SEQUENCE RESULT RESULT
HemodynamicHemodynamic response (minutes)response (minutes)
↑↑ Heart rateHeart rate↓↓ Capacitance (venous)Capacitance (venous)↑↑ Systemic resistanceSystemic resistance
(arterial)(arterial)
Renal Response (days)Renal Response (days)
NaNa++ avidityavidity
Local or systemic venousLocal or systemic venouspressure increasespressure increases
Reduced venousReduced venousarterial blood transferarterial blood transfer
Reduced effective Reduced effective circulating volumecirculating volume

HEART FAILURE: A SUICIDAL SYNDROMEHEART FAILURE: A SUICIDAL SYNDROME
““ ↓↓ filling . . . arterial treefilling . . . arterial tree””
NaNa++ avidityavidity
↑↑ preloadpreload
hemodynamichemodynamic changeschanges
↑↑ afterloadafterload
↑↑ end end -- diastolic volumediastolic volume
further further ↓↓ E. F. E. F.

PRINCIPAL SODIUMPRINCIPAL SODIUM--AVID SEGMENTSAVID SEGMENTSIN UNDERFILLINGIN UNDERFILLING
Normal Normal % Na Absorbed% Na Absorbed
60%60%
10%10%
5%5%
FactorsFactors↑↑ Na absorptionNa absorption
FFFFAA--IIIIcatecholscatechols
ADHADHaldoaldoANP resistance (?)ANP resistance (?)
ANP resistanceANP resistance
↑↑ TGFTGF
SegmentSegment
proximalproximal
late DCT; CCDlate DCT; CCD
IMCDIMCD

↓↓ ECV ECV
REDUCED ECV: GLOMERULAR AND HEMODYNAMIC REDUCED ECV: GLOMERULAR AND HEMODYNAMIC RESPONSERESPONSE
catecholaminescatecholamines AIIAII ADHADH endothelinendothelin II
↓↓↓↓ RBF, RBF, ↓↓ GFR GFR →→ ↑↑ FFFF
↑↑ net proximal absorptionnet proximal absorption
↓↓ distal Nadistal Na++ deliverydelivery
activation of JGA activation of JGA baroceptorsbaroceptors
reninrenin -- AIIAII

HH
HH++
ClCl
NaNa
NaNa
sugarssugarsamino acidsamino acidsPPii
2K2K
3Na3Na
[(Na) (3HCO[(Na) (3HCO33 )])]==
C. A.C. A.
GENERAL MODEL FOR PROXIMAL GENERAL MODEL FOR PROXIMAL TRANSPORTTRANSPORT
(HCO(HCO22 •• F)F)--


STARLING DERANGEMENTS (STARLING DERANGEMENTS (∆∆ P) WITH P) WITH ARTERIAL UNDERFILLINGARTERIAL UNDERFILLING
ACTIVATION OF TGFACTIVATION OF TGFNormalNormal
FiltrationFiltration
Proximal absorptionProximal absorption
Thick limb absorptionThick limb absorption
Macula Macula densadensa deliverydelivery
ReninRenin
↑↑ ATPATP↑↑ adenosineadenosine
increasesincreases
AA--IIII AA--IIII
reducesreduces

PRINCIPAL SODIUMPRINCIPAL SODIUM--AVID SEGMENTSAVID SEGMENTSIN UNDERFILLINGIN UNDERFILLING
Normal Normal % Na Absorbed% Na Absorbed
60%60%
10%10%
5%5%
FactorsFactors↑↑ Na absorptionNa absorption
AA--IIIIcatecholscatechols
ADHADHaldoaldo
ANP resistanceANP resistance
↑↑ TGFTGF
SegmentSegment
proximalproximal
late DCT; CCDlate DCT; CCD
IMCDIMCD

THE CD PRINCIPAL CELLTHE CD PRINCIPAL CELL
ATPaseATPaseNaNa2K2K
KK
ClCl
ClCl
KK
3Na3Na
HH22OO
amilorideamiloride
•• ADH, via ADH, via cAMPcAMP↑↑ ENaCENaC↑↑ AQPAQP22
•• Aldo, via nuclearAldo, via nuclearreceptorsreceptors↑↑ ENaCENaC
-- 20 mV20 mV -- 80 mV80 mV 0 mV0 mV

ENaCEpithelial Na Channel • Each α subunit :
amiloride-sensitiveNa channel
• β and γ subunits:↑surface delivery of ENaC
• Liddle's syndrome:β subunit mutation
• pseudohypoaldo I:α or β subunit mutation
• ARDS :α subunit mutation
News in Physiol. Sci.12:55, 1997

AQUAPORIN 2: AGRE'S HOURGLASS MODELAQUAPORIN 2: AGRE'S HOURGLASS MODEL
AgreAgre, , et al.et al.JBC JBC 269:14648, 1994269:14648, 1994

PRINCIPAL SODIUMPRINCIPAL SODIUM--AVID SEGMENTSAVID SEGMENTSIN UNDERFILLINGIN UNDERFILLING
Normal Normal % Na Absorbed% Na Absorbed
60%60%
10%10%
5%5%
FactorsFactors↑↑ Na absorptionNa absorption
AA--IIIIcatecholscatechols
ADHADHaldoaldo
ANP resistanceANP resistance
↑↑ TGFTGF
SegmentSegment
proximalproximal
late DCT; CCDlate DCT; CCD
IMCDIMCD
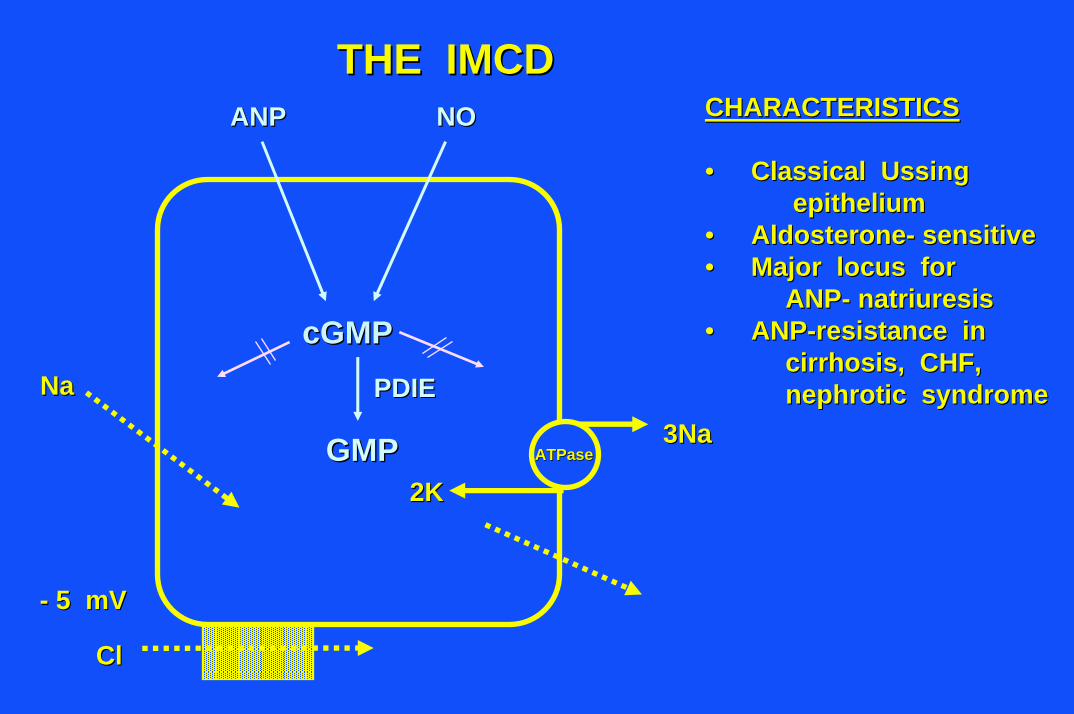
THE IMCDTHE IMCD
ATPaseATPase3Na3Na
2K2K
-- 5 mV5 mV
ClCl
NaNa
CHARACTERISTICSCHARACTERISTICS
•• Classical Classical UssingUssingepitheliumepithelium
•• AldosteroneAldosterone-- sensitivesensitive•• Major locus forMajor locus for
ANPANP-- natriuresisnatriuresis•• ANPANP--resistance inresistance in
cirrhosis, CHF,cirrhosis, CHF,nephroticnephrotic syndromesyndrome
cGMPcGMPPDIEPDIE
GMPGMP
ANPANP NONO

MAJOR ACTIONS OF ANPMAJOR ACTIONS OF ANP
•• ↓↓ Afferent arteriolar resistanceAfferent arteriolar resistance
•• ↓↓ Aldo effect in CCDAldo effect in CCD
•• ↓↓ IMCD NaIMCD Na++ absorptionabsorption

ANP RESISTANCEANP RESISTANCE
DisorderDisorder
Experimental CHFExperimental CHF
Experimental cirrhosisExperimental cirrhosis
Experimental Experimental nephrosisnephrosis
MechanismMechanism
↓↓ ANPANPAA densitydensity((AJP AJP 265:F119, 1993)265:F119, 1993)
↑↑ cGMPcGMP -- PDIEPDIE((AJPAJP 271:F3, 1996)271:F3, 1996)
↑↑ cGMPcGMP -- PDIEPDIE((AJPAJP 271:F3, 1996)271:F3, 1996)

SOME COMMON EDEMA STATESSOME COMMON EDEMA STATES
Primary renalPrimary renalNa retentionNa retention
acute GNacute GN
Arterial Arterial UnderfillingUnderfilling
systolic failuresystolic failure
pericardial constrictionpericardial constriction
late cirrhosislate cirrhosis
IVC and/or lymphatic occlusionIVC and/or lymphatic occlusion
third space disordersthird space disorders
ControversialControversial
early cirrhosisearly cirrhosis
early early nephrosisnephrosis

EDEMATOUS STATES: CIRRHOSISEDEMATOUS STATES: CIRRHOSIS
PRECIPITATING FACTORSPRECIPITATING FACTORS MANDATORY REQUIREMENTMANDATORY REQUIREMENT
Deranged Starling ForcesDeranged Starling Forces
Arterial Arterial UnderfillingUnderfilling
Altered Volume/Capacitance RatioAltered Volume/Capacitance Ratio
Primary Renal NaPrimary Renal Na++ AvidityAvidity
steadysteady--statestate
positive Napositive Na++ balancebalance

Classical Classical UnderfillingUnderfilling TheoryTheorySinusoidal Portal HypertensionSinusoidal Portal Hypertension
Lymph Formation > Lymph RemovalLymph Formation > Lymph Removal
AscitesAscites FormationFormation
Reduction of Plasma VolumeReduction of Plasma Volume
Activation of Activation of ReninRenin -- AngiotensinAngiotensin, , Sympathetic Nervous System and AVPSympathetic Nervous System and AVP
SecretionSecretion
SODIUM ANDSODIUM ANDWATER RETENTIONWATER RETENTION
OVERFLOW THEORYOVERFLOW THEORYSinusoidal Portal HypertensionSinusoidal Portal Hypertension
Hepatic PressureHepatic PressureReceptorsReceptors
PRIMARY SODIUM ANDPRIMARY SODIUM ANDWATER RETENTIONWATER RETENTION
Plasma Volume ExpansionPlasma Volume Expansion
AscitesAscites FormationFormation
CIRRHOSISCIRRHOSISUNDERFILLING VS. OVERFILLINGUNDERFILLING VS. OVERFILLING
MassryMassry and and GlassockGlassockTextbook of NephrologyTextbook of NephrologyEd. 3; Fig. 34Ed. 3; Fig. 34--44

CIRRHOSISCIRRHOSISOVERFILLINGOVERFILLING ARGUMENTS IN EARLY DISEASEARGUMENTS IN EARLY DISEASE
1.1. In In somesome experimental cirrhosis:experimental cirrhosis:NaNa+ + retention precedes retention precedes ascitesascites
2.2. In preIn pre--asciticascitic cirrhosis:cirrhosis:↑↑ cardiac outputcardiac output↑↑ blood volumeblood volume↑↑ splanchnicsplanchnic poolingpooling
3.3. In preIn pre--asciticascitic cirrhosis:cirrhosis:nlnl reninreninnlnl aldoaldo

CIRRHOSISCIRRHOSISKEY STRUCTURAL DERANGEMENTSKEY STRUCTURAL DERANGEMENTS
NormalNormal CirrhoticCirrhotic
Symmetrically placedSymmetrically placedhepatic lobuleshepatic lobules
Portal triad Portal triad →→ sinusoidsinusoid→→ central veincentral vein
Asymmetrically distributedAsymmetrically distributedregenerating nodulesregenerating nodules
Regenerating nodulesRegenerating nodulesno central veinno central veinsinusoidal compressionsinusoidal compression

CIRRHOSISCIRRHOSISCONSEQUENCES OF ABNORMAL REGENERATIVE CONSEQUENCES OF ABNORMAL REGENERATIVE
NODULESNODULES
high inflow resistancehigh inflow resistance
↓↓ portal / arterial flowportal / arterial flow
portal hypertensionportal hypertension
splanchnicsplanchnic poolingpooling
compression of adjacent sinusoidscompression of adjacent sinusoids
↑↑ intrasinusoidalintrasinusoidal pressurepressure
ascitesascites(a weeping liver)(a weeping liver)

SOME COMMON EDEMA STATESSOME COMMON EDEMA STATESPrimary renalPrimary renalNa retentionNa retention
acute GNacute GN
Arterial Arterial UnderfillingUnderfilling
systolic failuresystolic failure
pericardial constrictionpericardial constriction
late cirrhosislate cirrhosis
IVC and/or lymphatic occlusionIVC and/or lymphatic occlusion
third space disordersthird space disorders
ControversialControversial
early cirrhosisearly cirrhosis
early early nephrosisnephrosis

NEPHRITIC AND NEPHROTIC SYNDROMESNEPHRITIC AND NEPHROTIC SYNDROMESGENERAL FEATURESGENERAL FEATURES
Acute NephritisAcute Nephritis NephroticNephrotic SyndromeSyndrome
HematuriaHematuriaProteinuriaProteinuriaHypoalbuminemiaHypoalbuminemia↓↓ GFRGFRHypertensionHypertensionDilutionalDilutional anemiaanemia
++++++++++++
++++++++++++++++++++
++--
++--++++++++++++++++
++--++--++--

THE NEPHROTIC SYNDROMETHE NEPHROTIC SYNDROMETHE EDEMA CONTROVERSYTHE EDEMA CONTROVERSY
““UnderfillingUnderfilling””ProteinuriaProteinuria and and hypoalbuminemiahypoalbuminemia
Reduced effective volumeReduced effective volume
Activation of: Activation of: ReninRenin--angiotensinangiotensin systemsystem
Sympathetic nervous systemSympathetic nervous systemAVP secretionAVP secretion
Sodium and water retentionSodium and water retention
EDEMA FORMATIONEDEMA FORMATION
““OVERFILLINGOVERFILLING””Primary renal sodium retentionPrimary renal sodium retention
Increased plasma volumeIncreased plasma volumeand arterial pressureand arterial pressure
HypoalbuminemiaHypoalbuminemia
EDEMA FORMATIONEDEMA FORMATION
Adapted fromAdapted fromMassryMassry and and GlassockGlassockTextbook of NephrologyTextbook of NephrologyEd. 3; Fig. 34Ed. 3; Fig. 34--44

NEPHROTIC SYNDROMENEPHROTIC SYNDROMEARGUMENTS FAVORING PRIMARY RENAL Na AVIDITYARGUMENTS FAVORING PRIMARY RENAL Na AVIDITY
1.1. Congenital Congenital hypoalbuminemiahypoalbuminemia: generally edema: generally edema--freefree
2.2. NephroticNephrotic edema can resolve edema can resolve ⎯⎯cc hypoalbuminemiahypoalbuminemia
3.3. ↑↑ cGMPcGMP--PDIE levels; PDIE levels; ↓↓ ANP levels with edemaANP levels with edema
IMCD: putative locusIMCD: putative locusfor primary Na avidityfor primary Na avidity


THE NEPHROTIC SYNDROMETHE NEPHROTIC SYNDROMEA CLINICAL SPECTRUMA CLINICAL SPECTRUM
1. 1. NephroticNephrotic syndrome is a clinical and syndrome is a clinical and hemodynamichemodynamicspectrum:spectrum:
↑↑ blood volumeblood volume ↓↓ or normal volumeor normal volumeolder patients younger older patients younger patientspatients
glomerularglomerular inflammationinflammation little inflammationlittle inflammation↓↓ GFR normal GFRGFR normal GFR↑↑ b. p. normal b. p.b. p. normal b. p.
↓↓ reninrenin/AII /AII nlnl or or ↑↑ aldoaldo..
2. Most 2. Most nephroticsnephrotics without without glomerularglomerular inflammationinflammationact act underfilledunderfilled..
THE NEPHROTIC SYNDROMETHE NEPHROTIC SYNDROMESOME GENERAL CONCLUSIONSSOME GENERAL CONCLUSIONS
1. Primary renal Na1. Primary renal Na++ retention occurs:retention occurs:ANP resistanceANP resistance? other factors? other factors
2. 2. ↓↓ albumin contributes to vascular/interstitialalbumin contributes to vascular/interstitialdistribution of accumulated fluiddistribution of accumulated fluid
3. 3. ↓↓ GFR: GFR: resemble nephritic syndrome resemble nephritic syndrome NL GFR: NL GFR: resemble resemble ““purepure”” nephrosisnephrosis

EDEMATOUS STATESEDEMATOUS STATES
PRECIPITATING FACTORSPRECIPITATING FACTORS MANDATORY REQUIREMENTMANDATORY REQUIREMENT
Deranged Starling ForcesDeranged Starling Forces
Arterial Arterial UnderfillingUnderfilling
Altered Volume/Capacitance RatioAltered Volume/Capacitance Ratio
Primary Renal NaPrimary Renal Na+ + AvidityAvidity
steadysteady--statestate
positive Napositive Na++ balancebalance

THE NEPHRITIC SYNDROMETHE NEPHRITIC SYNDROMEACUTE GN ACUTE GN →→ PRIMARY NaPRIMARY Na++ RETENTIONRETENTION
1. 1. GlomerularGlomerular InflammationInflammation↓↓ KKffNormal RPFNormal RPF
2. 2. ↓↓ GFR GFR ↓↓ axial delivery axial delivery ↑↑ proximal Naproximal Na++ absorptionabsorption
3. Continued Na3. Continued Na++ intake:intake:Plasma expansion Plasma expansion dilutionaldilutional edemaedemaHypertension edema; pulmonary cHypertension edema; pulmonary congestionongestion↑↑ ANPANP↓↓ reninrenin / / aldosteronealdosterone
↓↓ FFFF



SOME COMMON EDEMA STATESSOME COMMON EDEMA STATES
Primary renalPrimary renalNa retentionNa retention
acute GNacute GN
Arterial Arterial UnderfillingUnderfilling
systolic failuresystolic failure
pericardial constrictionpericardial constriction
late cirrhosislate cirrhosis
IVC and/or lymphatic occlusionIVC and/or lymphatic occlusion
third space disordersthird space disorders
ControversialControversial
early cirrhosisearly cirrhosis
early early nephrosisnephrosis

KEY FACTORS IN EDEMA FORMATIONKEY FACTORS IN EDEMA FORMATION
PRECIPITATING FACTORSPRECIPITATING FACTORS MANDATORY REQUIREMENTMANDATORY REQUIREMENT
Deranged Starling ForcesDeranged Starling Forces
Arterial Arterial UnderfillingUnderfilling
Altered Volume/Capacitance RatioAltered Volume/Capacitance Ratio
Primary Renal NaPrimary Renal Na++ AvidityAvidity
steadysteady--statestate
positive Napositive Na++ balancebalance