the difficult doctor or the doctor with difficulties simon willcock august 2008
TRANSCRIPT

THE DIFFICULT DOCTORor
THE DOCTOR WITH DIFFICULTIES
Simon Willcock
August 2008
NicholasNicholas

Nicholas is an Advanced Registrar working in your regional town practice for a year . He is 28 years old. He has had an average record of achievement in his studies and previous terms.
He has been regularly calling in sick, and did not turn up for a rostered Saturday morning shift. His explanation is that he forgot. The front desk staff says that he has been difficult – uncooperative and argumentative.
What could be happening to Nicholas?
Is Nicholas a bad doctor? Should we institute any measures, and if so
what options do we have?

Anxiety
Lack of support
Depression
Substance use
Family problems
Unhappy with career choice
IncompetenceFinancial problems
What could be happening to Nicholas?

After talking to Nicholas you find that he and his wife are living in a one bedroom apartment.
He has a new baby and his wife is suffering from post natal depression.
He is struggling to support his wife emotionally.
Why didn’t Nicholas ask for help?
“Doctors should cope”“Admitting you can’t cope equals
incompetence”Loss of control / loss of facePersonality factorsAssessment / progression

What makes a good doctor?
Organises time well and can work to a schedule
Pays great attention to detail
Hardworking Self sacrificing Ethical Can lead a team and
takes responsibility Confident in ones skill
Pre-occupied with details rules and lists
Perfectionist Devoted to work Over-conscientious and
concerned with ethical and moral values – inflexible
Reluctant to delegate to others
Shows rigidity and stubbornness
(Unable to discard worn out objects) (Overly thrifty)
OBSESSIVE COMPULSIVE PERSONALITY TRAIT

IPDEQ Subscale Frequencies Time 1
PARANOID n %NO 107 97.3YES 3 2.7
SCHIZOIDNO 91 82.7YES 19 17.3
DISSOCIALNO 100 90.9YES 10 9.1
IMPULSIVENO 100 90.9YES 10 9.1
BORDERLINENO 107 97.3YES 3 2.7
HISTRIONICNO 69 62.7YES 41 37.3
ANANKASTICNO 36 32.7YES 74 67.3
ANXIOUSNO 98 89.1YES 12 10.9
DEPENDENTNO 105 95.5YES 5 4.5
Total 110 100.0

Internal Stresses (personal characteristics)
Personality and coping styles in the caring professions
High achievers
Self denying
Obsessive
Prone to depression
(good for patients, bad for self-care)

Doctor’s health statistics
Heart disease Smoking related illness Motor vehicle accidents Liver disease Depression Anxiety suicide
Less than population Less than population 2x population 3x population 3x population >3x population >3 times population

Doctors as an at risk group?
Doctors are more likely to: be alcoholic – alcoholism is the major cause of
impairment in doctors over 50 be drug addicted – drug use is the major reason for
referral to the Medical Board for impairment be stressed be anxious or depressed commit suicide
These are powerful indicators of poor self care

In figures from 1996 (Lawrence J) Male doctors – 1.5 to 3.4 times the suicide rate
for the population Female doctors – 2.5 to 5.7 times
Over represented areas• Anaesthetics• Psychiatry• General practice• Emergency Medicine
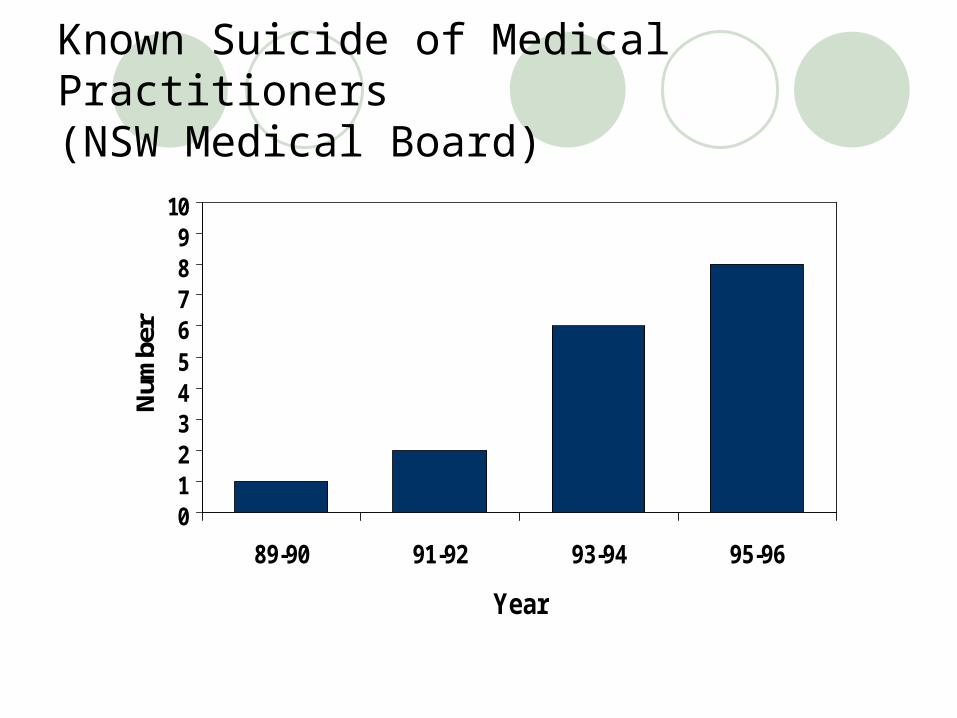
Known Suicide of Medical Practitioners(NSW Medical Board)
0123456789
10
89-90 91-92 93-94 95-96
Year
Num
ber
Hume and Wilhelm 1994 Intern StudyPrince of Wales / Prince Henry Hospitals
Showed 17% reported having sought help for previous emotional problems
During intern year 8%reported seeking help - anxiety, depression and eating disorders
During the year 4% had ‘often’ considered life was not worth living and 3% had entertained (but not acted on) suicide plans
72% reported ‘often experiencing significant and distressing episodes of anger.

Performance and Competence
Look below the surface of performance distracters Most students and young doctors are there
to try and do a good job Look out for those whose behaviour
changes suddenly Would Nicholas’ friends have noticed a
change in his behaviour?

What resources do you have to help Nicholas?
Supportive colleaguesAccess to professional assistance e.g. GP,
psychologist, psychiatristGeneral PractitionerMedical Benevolent AssociationDHAS

What if Nicholas’ attendance or attitude fail to improve?
SupportProgression

Robert

Robert is a 25 year old student in Med 4, doing a long placement in your practice. He has always been one of the top students and has great reports from the clinical school.
He is undertaking an honours project in cardiothoracic surgery. He is a good sportsman, plays first grade rugby for the university and is an accomplished musician. His father is the professor of surgery at a leading university. Everyone says he is going to be a great doctor.
It has been reported that he was rude to a patient who complained about his manner and he got into a brawl at the local club.

You’ve organised to meet with Robert to discuss these issues.
What will you do to prepare for this interview?

When Robert comes to see you he breaks down in tears and says he is leaving the medical program because he will never be a good doctor

Anxiety
Lack of support
Depression
Substance use
Family problemsInterpersonal problems
Unhappy with career choice
IncompetenceFinancial problems
What could be happening to Robert
Stress and Burnout

Concepts of Stress , Distress and Impairment
We all experience stress
We may become distressed
If we are distressed for long, we may become impaired
IS STRESS A MENTAL ILLNESS?
No! - Some stress is good
Better Reduced
Perf. Perf.
Performance
Stress

Coping well Distressed Impaired(? 15-30%) (1-3%)
External(Environmental)
factors
Internal(Personal)
factors

External Stresses
Assessment
Workload
Family expectations
Exams, options, honours
Vocational issues – length of time, limited choices
Relationship issues
Family problems – children and parents
Financial problems
The work environment – low morale, aggression and bullying, traumatic experiences – the elective term

Signs of “distress”
Depression (and anger)
Burnout
Changes in behaviour e.g. drinking more, taking risks
Relationship problems (family, patients, staff)
Financial problems
Withdrawal

What is Burnout?
“The origin of burnout is in occupations where large amounts of time are spent
with the problems of others” (Heiter and Maslach, 1988)

3 Dimensions of Burnout
Emotional exhaustion
Depersonalisation
Reduced feelings of Personal Accomplishment

Medical Practitioners and Burnout
Medical practitioners as a group tend to have “moderate” levels of burnout across all 3 dimensions
There are times when burnout levels are generally increased
e.g. internship

Change in Reported Burnout over Time (T1=early final medical student year, T6= late internship year)
Access Time
654321
Mea
n B
urno
ut S
core
with
95%
CI
30
20
10
0
MBI Subscale
Emotional Exhaustion
Depersonalisation

2. Is burnout inevitable?

Burnout Prevalence
(Willcock et al – 2000 study of GMP graduates)
Midway through final medical student year (Time 1), 27.7% of participants met criteria for burnout (either high DP score (>=10) or high EE score(>=27)).
This level of burnout then gradually increased to 74.7% by mid way through the internship year (Time 5).

Change in Burnout over Time
88838495103101N =
Access Time
6.005.004.003.002.001.00
95%
CI M
BI B
urno
ut E
mot
ional
Exha
ustio
n
28
26
24
22
20
18
16
1488838495103101N =
Access Time
6.005.004.003.002.001.00
95%
CI M
BI B
urno
ut D
eper
sona
lisat
ion
14
12
10
8
6
488838495103101N =
Access Time
6.005.004.003.002.001.00
95%
CI M
BI B
urno
ut P
erso
nal A
ccom
plish
men
t
41
40
39
38
37
36
35
Depersonalisation (Mean Diff T6-1, p<0.001)
Emotional Exhaustion (Mean Diff T6-1, p<0.001)
Personal Accomplishment (Mean Diff T6-1, p<0.001)

Correlations
Females were more likely to become emotionally exhausted, while males were more likely to exhibit depersonalisation
The higher the degree of emotional exhaustion, the higher the “assessed” term performance !

3. Is Burnout bad for you?
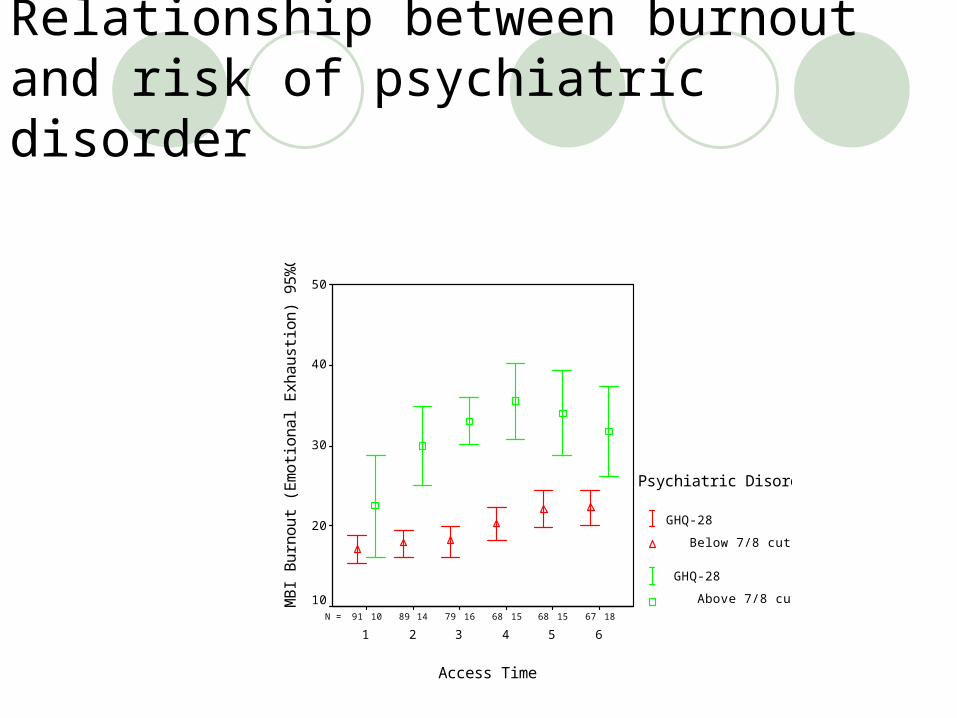
Relationship between burnout and risk of psychiatric disorder
181515161410 676868798991N =
Access Time
654321
MB
I B
urn
ou
t (E
mo
tion
al E
xha
ust
ion
) 9
5%
CI
50
40
30
20
10
Psychiatric Disorder
GHQ-28
Below 7/8 cut off
GHQ-28
Above 7/8 cut of

What can you do to help?
Recognise the symptomsEducation for studentsRealistic goalsPsychologistMentor / faculty independent support
person

LisaLisa

Lisa is a locum at your practice. Practice and hospital staff have noticed that she is keeping to herself. She has lost weight and doesn’t talk at all in practice meetings.
Her clothes look dishevelled at times. A few patients have refused to see her. Sometimes she can be seen just sitting alone staring blankly.
Anxiety
Lack of support
Depression
Substance use
Family problemsInterpersonal problems Unhappy with career choice
Incompetence
Financial problems
What could be happening to Lisa
Stress and Burnout
Physical illness
Serious mental illness – bipolar disorder or psychosis
Anorexia
Doctors and medical students are people too Physical Illness Psychological illness

Impairment
A doctor (or a student) is impaired if they suffer from any physical or mental illness which is likely to affect their capacity to work safely.
Impairment implies that the individual lacks insight into their own ability to work safely.

Illness likely to cause Impairment
Psychiatric illness Bipolar Depression Anxiety and OCD Eating disorders
AddictionPhysical illness and disability

Who would notice this behaviour?How should we encourage doctors or
students to report their concerns?
What can you do?
Remember what we are all here for – patient safety.
The key problem in impairment is lack of insight
Talk to someone – the person, your colleagues, DHAS, your indemnity organisation
DHAS? Refer to the Medical Board

Sarah

Sarah is a difficult student. She is unpopular with the other students and frequently complains about aspects of the course and the behaviour of other students. She often asks for ‘special consideration’ at exam time.
When counselled by sympathetic Faculty members she appears to lack insight and blames external factors. She has failed her last assessment but she is complaining to the Dean that the test was unfair.

Another student has complained that Sarah emailed other students very unpleasant information about a tutor and told them not to bother attending tutorials.
Sarah has been to the Associate Dean crying and saying other students don’t include her in their group and don’t value her opinion.
Anxiety
Lack of support
Depression
Substance use
Family problemsInterpersonal problems
Unhappy with career choice
Incompetence
Financial problems
What could be happening to Lisa
Stress and Burnout
Physical illness
Serious mental illness – bipolar disorder or psychosis
Anorexia
Personality problems‘the Disruptive Doctor’

ISSUES
Separating competency from conductSeparating support from progressionHow can this student be assisted to gain
competencyWhose responsibility is she?

Recognise the need for Behaviour management Performance and progression assessment Student support committee Documentation ++++ Everyone should be aware of decisions
Can one person do all of these roles?

Performance and support



The presenting behaviour is usually just the tip of the iceberg

Summary - 4 Basic Tasks
1. Diagnose the problem
2. Appropriate support
3. Manage performance
4. Manage unprofessional behaviour

Taking care of BASICs
BASIC
odyffectocialntellectosmos
New Jersey Medical Assoc. Physician Health Program

+ -Selfless Selfish

Nutrition avoid dehydration
minimise toxins
Exercise
Rest sleep is not a luxury
Recreation - “rest for mind and spirit”
Good Medical Care
Boundaries and Balance
B is for Body

A is for Affect
Mood Attitudinal and Emotional Health “Emotional Intelligence”
self awareness ability to manage emotions positively empathy delayed gratification, but not indefinitely!
Dealing with negative emotions

Emotional Sensitivity
Emotional Exhaustion
Psychological Distress
Personal Accomplishment
Personality Burnout Distress
Autoregressionp<0.0001 p<0.005
Predictor Model of Psychological Distress
Dependent Type Personality
Depersonalisation
Low Confidence In Coping Skills
Disability

S is for Social
Pay attention to your loved ones
“In and through community lies the salvation of the
world” (MS Peck)
Trust and take risks
Give and receive feedback
Support each other
Experience love and intimacy

I is for Intellect
Hobbies
Current events
Reading
Re-evaluate your worldview,
belief systems, ethical and
moral standards,
ideals and expectations
Deal with feelings of entitlement

C is for Cosmos
A personal sense
of meaning
and purpose
Spiritual Health
It is easy to lose perspective in the rigours of
daily medical practice
We need to keep the ability to experience awe,
wonder and surprise

BASIC
B A S I C
odyffectocialntellectosmos
Breathing Awake Satisfied Intelligible Continent
Into your 30’sInto your 30’s Into your 80’sInto your 80’s