the concept of damage control surgery dr. derek tl fung department of surgery queen elizabeth...
TRANSCRIPT

The Concept of Damage Control SurgeryDr. Derek TL FungDepartment of SurgeryQueen Elizabeth Hospital
Damage Control Surgery (DCS)
Multiple abdominal trauma
Thoracic injury
Vascular surgery
Orthopaedics
Abdominal sepsis

Originated in the US Navy, refers to the capacity of a ship to absorb damage and maintain mission integrity
Damage Control

In 1970s & 1980s, surgeons tended to perform complex and lengthy operation in multiple trauma case
Extensive resection
Extensive reconstruction
Aggressive resuscitation
Extracorporeal support

HistoryIdea originated from liver trauma
Pringle published a case series of packing liver injuries in 1908
Pringle JH. V. Notes on the Arrest of Hepatic Hemorrhage Due to Trauma. Ann Surg. 1908 Oct;48(4):541-9.
Calne in 1979 published a series of liver trauma patients whose abdomens were packed prior to transfer and definitive surgery at another centre
Calne RY, McMaster P, Pentlow BD. The treatment of major liver trauma by primary packing with transfer of the patient for definitive treatment. Br J Surg. 1979 May;66(5):338-9.

Stone et al.
Coagulopathy in trauma patient leads to exsanguination and mortality
In his series, 31 patients with major bleeding tendency
11 out of 17 patient who was managed with packing and staged re-laparotomy survived. 1 out of 14 patients with standard treatment survived
Stone HH, Strom PR, Mullins RJ. Management of the major coagulopathy with onset during laparotomy. Ann Surg. 1983 May;197(5):532-5.

Rotondo et al.Rotondo and co-workers published a further series and coined the phrase ‘damage control surgery’ in 1993
7-fold of improvement in survival in a subgroup of patient with major vascular injury and 2 or more visceral injuries if they were managed with damage control approach
10/13 (77%) survived with damage control surgery1/9 (11%) with traditional definitive laparotomy
Rotondo MF, Schwab CW, McGonigal MD, Phillips GR 3rd, Fruchterman TM, Kauder DR, Latenser BA, Angood PA. 'Damage control': an approach for improved survival in exsanguinating penetrating abdominal injury. J Trauma. 1993 Sep;35(3):375-82; discussion 382-3

Lethal Triad
Acidosis
Hypothermia
Coagulopathy

Hypothermia
Central thermoregulation lost
Metabolic activity
Cold IV fluid
Platelet dysfunction
Clotting factors kinetics disturbance
Cardiac dysfunction
Vasoconstriction
Hypoperfusion
Acidosis
Cardiac contractility
Dysrhythmias
Synergize with hypothermia in its detrimental effect on the coagulation cascade

Coagulopathy
Platelet dysfunction
Clotting cascade disturbed
Haemodilution
Uncontrolled bleeding from all cut surfaces


Principles of DCS
Quickly abort the vicious cycle by haemorrhage and contamination control
Minimize further trauma created by Surgeon
Restore normal physiology before definitive surgery in reoperation

Stages of Damage Control Surgery
1. Patient selection
2. Intraoperative stage
3. Critical care stage
4. Return to the operating theatre
5. Formal closure
Moore EE. Thomas G. Orr Memorial Lecture. Staged laparotomy for the hypothermia, acidosis, and coagulopathy syndrome. Am J Surg. 1996 Nov;172(5):405-10.

Stage 1: Patient Selection

Rotondo M, Zonies D. The damage control sequence and underlying logic. Surg Clin N Am 1997; 77: 761-777.

No Definite Selection Criteria
Too Liberal Unnecessary staged operation
Too Strict Adverse physiological outcome established Too late to salvage
Experience, rapid surgical assessment and liaison with anesthetist are the keys in decision making
Stage 2: Intraoperative
Aim: Controlling Haemorrhage
Limiting contamination






Temporary Closure

- Risk of abdominal compartment Syndrome
- Ineffective Drainage
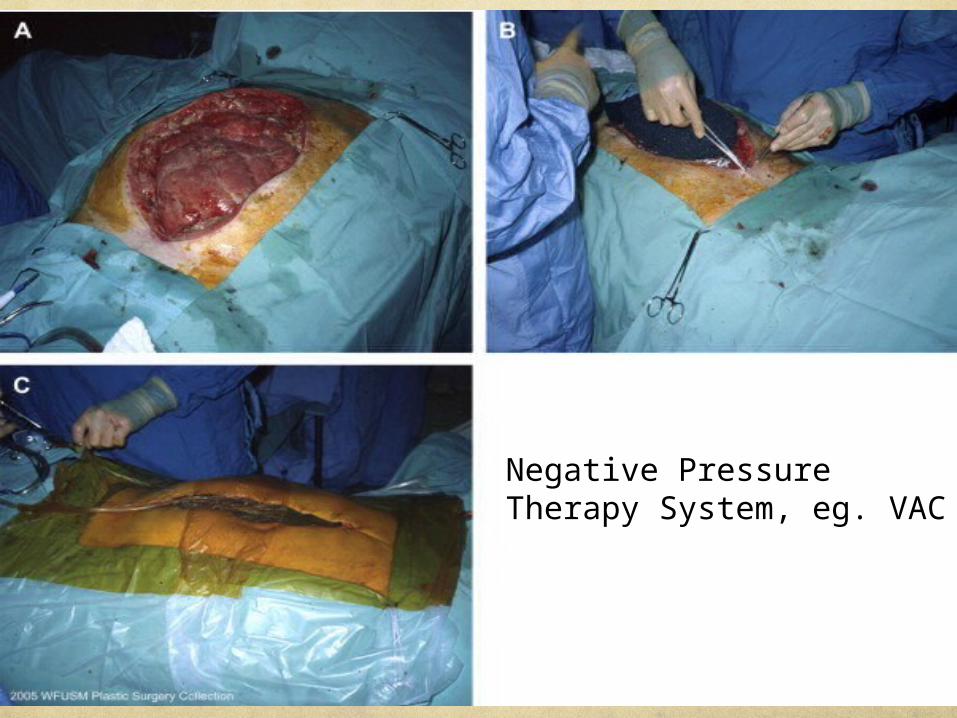
Negative Pressure Therapy System, eg. VAC
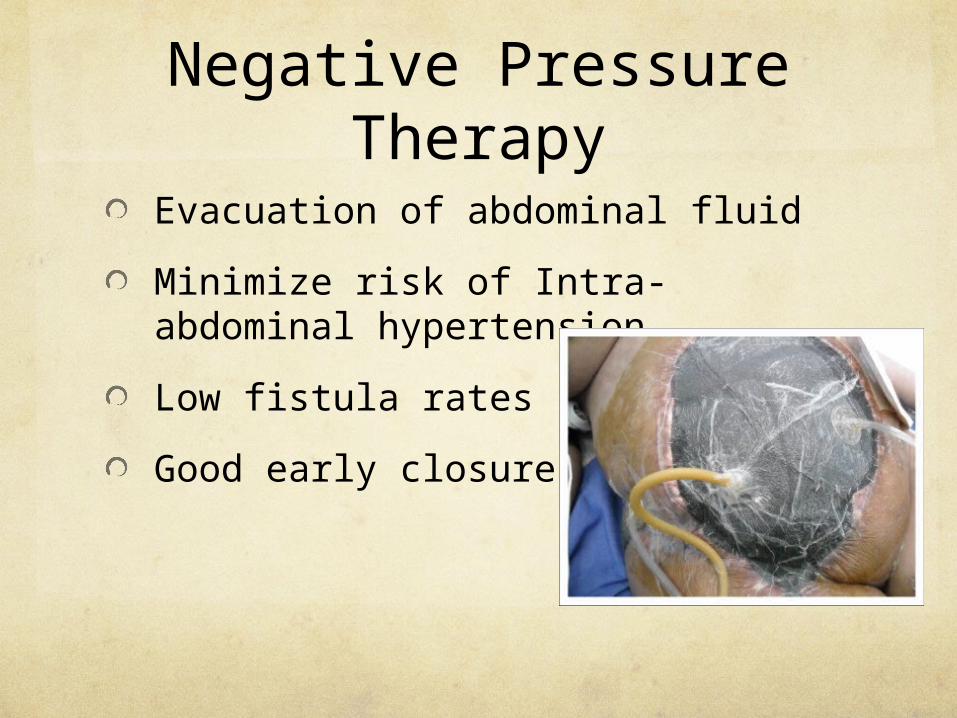
Negative Pressure Therapy
Evacuation of abdominal fluid
Minimize risk of Intra-abdominal hypertension
Low fistula rates
Good early closure rates

Stage 3: Critical Care Stage
Active rewarming
Correction of Acidosis
Correction of Coagulopathy
Monitor the need for early return to theatre
Ongoing surgical bleedingAbdominal compartment syndrome

Stage 4: Return to the Theatre
Timing:
24-48hrs later whenBase deficit < 4 mmol/LLactate of < 2.5 mmol/LCore temperature > 35 C INR < 1.25

Stage 4: Return to the Theatre
Definitive surgeryRemoval of packsAnastomoses or stomasVascular repairsSolid organ debridementPlacement of feeding tube
Stage 5: Formal ClosureMay not be feasible due to significant bowel edema or risk of abdominal compartment syndrome
30 - 80% closure rate in the 1st reoperationHirshberg A, Wall MJ, Mattox KL. Planned reoperation for trauma: a two-year
experience with 124 consecutive patients. J Trauma 1994;37(3):365– 9.
Hatch QM, Osterhout LM, Ashraf A, Podbielski J, Kozar RA, Wade CE, Holcomb JB, Cotton BA. Current use of damage-control laparotomy, closure rates, and predictors of early fascial closure at the first take-back. J Trauma. 2011 Jun;70(6):1429-36.
The highest closure rates are achieved during the first 7–10 days
Regner JL, Kobayashi L, Coimbra R. Surgical strategies for management of the open abdomen. World J Surg. 2012 Mar;36(3):497-510.

Evidence

˜
DCS Vs Immediate and definitive repair (in patients with major abdominal trauma)
A total of 1523 studies were identified
A total of 1521 studies were excluded because they were not relevant to the review topic
Targets were not suffering from major abdominal trauma/ narrow spectrum
Not directly comparing DCS Vs definitive repair
Two studies were excluded because they were case-control studies. (Rotondo 1993, Stone 1983)
Cirocchi R, Abraha I, Montedori A. Damage control surgery for abdominal trauma. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD007438.
Evidence
No RCT, systemic review could not be done
Most of the studies were case series Different patient groups
Different methodology
Conclusion: Evidence is LIMITED.
Cirocchi R, Abraha I, Montedori A. Damage control surgery for abdominal trauma. Cochrane Database Syst Rev. 2010 Jan 20;(1):CD007438.
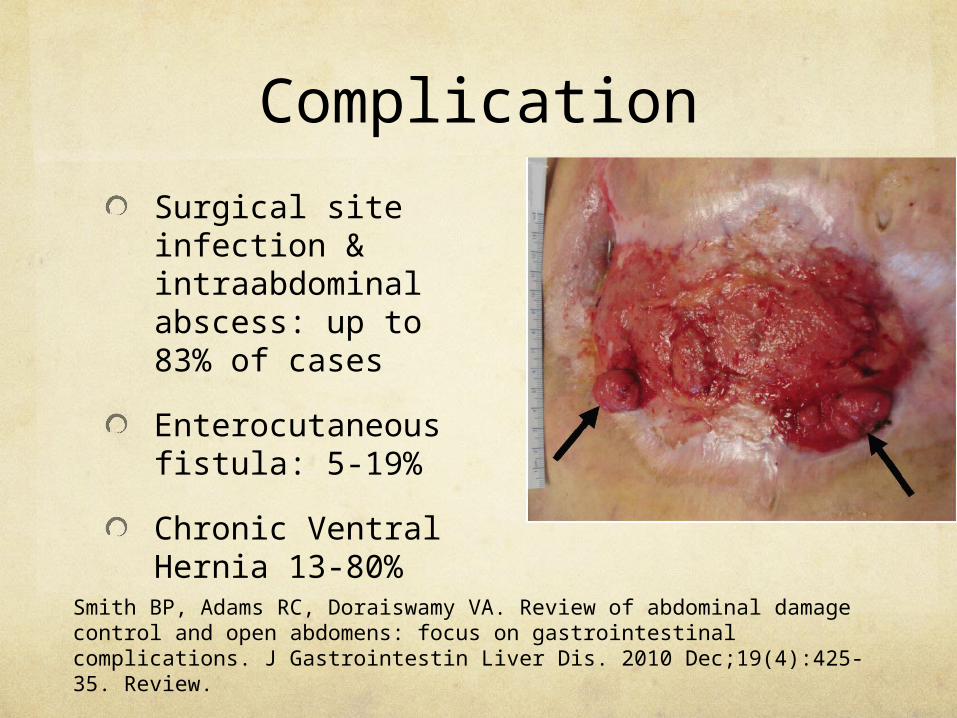
Complication
Surgical site infection & intraabdominal abscess: up to 83% of cases
Enterocutaneous fistula: 5-19%
Chronic Ventral Hernia 13-80%
Smith BP, Adams RC, Doraiswamy VA. Review of abdominal damage control and open abdomens: focus on gastrointestinal complications. J Gastrointestin Liver Dis. 2010 Dec;19(4):425-35. Review.

Overuse of DCS
Complications
Long intensive care unit stays
Increased use of blood products
Multiple operations
Higher hospital cost
Higa G, Friese R, O'Keeffe T, Wynne J, Bowlby P, Ziemba M, Latifi R, Kulvatunyou N, Rhee P. Damage control laparotomy: a vital tool once overused. J Trauma. 2010 Jul;69(1):53-9.
Hatch QM, Osterhout LM, Podbielski J, Kozar RA, Wade CE, Holcomb JB, Cotton BA. Impact of closure at the first take back: complication burden and potential overutilization of damage control laparotomy. J Trauma. 2011 Dec;71(6):1503-11.

Damage Control Resuscitation

Damage Control Resuscitation
Proactive early treatment to address the lethal triad (by rapid reversal of acidosis, prevention of hypothermia and coagulopathy) on admission to combat hospital.
Assumption that coagulopathy is actually present very early after injury
Holcomb J, Jenkins D, Rhee P et al. Damage Control Resuscitation: Directly Addressing the Early Coagulopathy of Trauma. J Trauma 2007; 62: 307-310.

Damage Control Resuscitation
Permissive HypotensionSatisfied with MAP = 50-60mmHg
Minimize dilution effect and hypothermia secondary to overzealous fluid replacement
Early use of blood product over isotonic fluid for volume replacement
Early correction of coagulopathy with components, ie. Massive transfusion protocol
PRBCs: FFP: Platelet = 1:1:1

Midwinter MJ. Damage control surgery in the era of damage control resuscitation. J R Army Med Corps. 2009 Dec;155(4):323-6.

Conclusion
Damage control surgery was an useful tool in handling patients with multiple injury, though high level of evidence is lacking
DCS is not without risk and complication, over-utilization may lead to more harm than benefit
With DCR integrating into DCS, the need of DCS may reduce as coagulopathy is corrected earlier
Thank You!