the cardiac evaluation of the athlete daniel j. o’rourke, md, ms veterans affairs medical center...
TRANSCRIPT

The Cardiac Evaluation The Cardiac Evaluation of the of the AthleteAthlete
Daniel J. O’Rourke, MD, MSDaniel J. O’Rourke, MD, MS
Veterans Affairs Medical CenterVeterans Affairs Medical Center
Dartmouth-Hitchcock Medical Dartmouth-Hitchcock Medical CenterCenter

Competitive AthleteCompetitive Athlete
• ““One who participates in an One who participates in an
organized team or individual sport organized team or individual sport
requiring systematic training and requiring systematic training and
regular competition against others regular competition against others
while placing a high premium on while placing a high premium on
athletic excellence.”athletic excellence.”
Maron et al. Circulation 1996;94:850-867.

DemographicsDemographics
• 25 million children and young adults play 25 million children and young adults play
sports sports
• 4,000,000 high school (grades 9-12) athletes4,000,000 high school (grades 9-12) athletes
• 500,000 college athletes500,000 college athletes
• 5000 professional athletes5000 professional athletes


Scope of the ProblemScope of the Problem
Prevalence of athletic field deaths:Prevalence of athletic field deaths:
High school athletes: 1 in 300,000 High school athletes: 1 in 300,000
Older athletes: 1 in 15,000 healthy Older athletes: 1 in 15,000 healthy
male joggersmale joggers

U.S. Vital StatisticsU.S. Vital Statistics
CausesCauses Deaths per yearDeaths per year
AccidentsAccidents 13,96613,966 700x700x
HomicideHomicide 8,424 8,424 421x421x
SuicideSuicide 4,849 4,849 242x242x
CancerCancer 1,738 1,738 87x 87x
Congenital Heart Dz Congenital Heart Dz 981 981
49x49x
HIVHIV 609 609 30x 30x
SCD in the athleteSCD in the athlete 15-2515-25
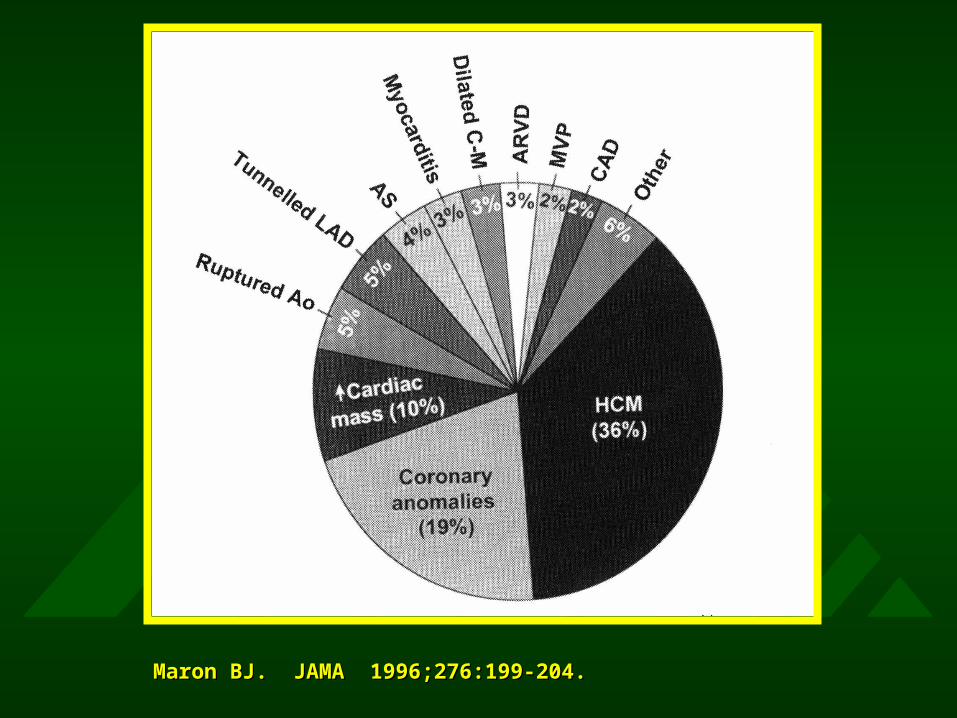
Maron BJ. JAMA 1996;276:199-204.Maron BJ. JAMA 1996;276:199-204.

Maron BJ. Circulation 1980;62:218-229.Maron BJ. Circulation 1980;62:218-229.

Gilman JK, Naccarelli GV. Curr Prob Cardiol Nov 1992.Gilman JK, Naccarelli GV. Curr Prob Cardiol Nov 1992.

Cardiac Evaluation of the Cardiac Evaluation of the AthleteAthlete
1. Primary Prevention of SCD 1. Primary Prevention of SCD (Screening)(Screening)
2. Secondary Prevention of SCD2. Secondary Prevention of SCD26th Bethesda Conference. 26th Bethesda Conference.
JACC. 1994;24:845-899.JACC. 1994;24:845-899.

ScreeningScreening
• Disease should be:Disease should be:• prevalentprevalent
• have significant M & Mhave significant M & M
• be treatablebe treatable
• Treatment results in a better Treatment results in a better
outcomeoutcome
• Good screening test must be availableGood screening test must be available
• Cost-benefit ratio should be favorableCost-benefit ratio should be favorable

ScreeningScreening
• Purpose:Purpose: to provide medical clearance to provide medical clearance for participation in competitive sports.for participation in competitive sports.
• Assumption:Assumption: intense training will intense training will increase the risk of sudden cardiac increase the risk of sudden cardiac death or disease progression in death or disease progression in trained athletes.trained athletes.
• Expected Outcome:Expected Outcome: to reduce the to reduce the risks associated with organized sports.risks associated with organized sports.

Cause of SCD of Elite Cause of SCD of Elite AthletesAthletes
• Jim FixxJim Fixx ASCVDASCVD
• Len BiasLen Bias Cocaine Cocaine
• Reggie LewisReggie Lewis Focal MyocarditisFocal Myocarditis
• Flo HymanFlo Hyman Marfan’s - Aortic ruptureMarfan’s - Aortic rupture
• Hank GathersHank Gathers Hypertrophic Hypertrophic
CardiomyopathyCardiomyopathy
• Pete MaravichPete Maravich Hypoplastic Coronary Hypoplastic Coronary
ArteriesArteries

Fletcher GF. SCD in the Athlete. Futura Publishing, 1998.Fletcher GF. SCD in the Athlete. Futura Publishing, 1998.

Screening: H&PScreening: H&P
• HistoryHistory• Chest painChest pain
• SOBSOB
• Lightheadedness/Lightheadedness/SyncopeSyncope
• Excessive fatiguabilityExcessive fatiguability
• Family h/o cardiac dzFamily h/o cardiac dz
• Family h/o premature Family h/o premature deathdeath
• H/O murmurH/O murmur
• PalpitationsPalpitations
• Physical ExamPhysical Exam• Auscultate in Auscultate in
supine/standingsupine/standing
• Sinus bradycardia commonSinus bradycardia common
• Assess BP bilateral armsAssess BP bilateral arms
• Assess femoral pulsesAssess femoral pulses
• Signs of Marfan’sSigns of Marfan’s
• Functional murmur Functional murmur
commoncommon
• SS33 gallop common gallop common
Screening: ECGScreening: ECG
• Sinus bradycardiaSinus bradycardia
• Rightward axis Rightward axis
• First or second degree, type I AV First or second degree, type I AV
blockblock
• Incomplete RBBBIncomplete RBBB
• Ventricular hypertrophyVentricular hypertrophy
• Nonspecific ST-T changesNonspecific ST-T changes
Screening: Screening: EchocardiographyEchocardiography
• Bicuspid Ao valveBicuspid Ao valve
• Hypertrophic CMHypertrophic CM
• RV dysplasiaRV dysplasia
• Coronary Coronary
anomaliesanomalies
• Mitral Valve Mitral Valve
ProlapseProlapse
• ScreeningScreening• 4 studies4 studies• >5000 pts>5000 pts• No cases identifiedNo cases identified
• Cost is prohibitiveCost is prohibitive• $500,000 for each $500,000 for each
new case of HCM new case of HCM identifiedidentified
• >$1,000,000 per life >$1,000,000 per life savedsaved

Bruce BA et al. AJC 1980;46:371-Bruce BA et al. AJC 1980;46:371-378.378.
1 d ea th
P os it ive sc reen
1 0 0 h ig h risk p ts0 .7 7 % p er year
4 d ea th s
N eg ative sc reen
9 ,9 0 0 low ris k p ts0 .0 4 3 % p er year
E TT+
C R F sc reen
1 0 ,0 0 0 asx m en_ _ _ _ _S C D
0 .0 5 % p er year

AHA RecommendationsAHA Recommendations
• Careful, detailed history and physical exam Careful, detailed history and physical exam every 2 years by qualified care providers.every 2 years by qualified care providers.
• Intervening years, obtain an interim history.Intervening years, obtain an interim history.
• Selectively perform ETT in men (>40 yo) Selectively perform ETT in men (>40 yo) and women (>50 yo) having a high risk for and women (>50 yo) having a high risk for CAD who wish to begin regular physical CAD who wish to begin regular physical training.training.
• Develop a national standard for Develop a national standard for preparticipation medical evaluation.preparticipation medical evaluation.

Glover, Maron BJ. JAMA 1998;279:1817-1819.Glover, Maron BJ. JAMA 1998;279:1817-1819.

Glover, Maron BJ. JAMA 1998;279:1817-1819.Glover, Maron BJ. JAMA 1998;279:1817-1819.

Cummins RO et al. Circulation 1991;83:1832-1847.Cummins RO et al. Circulation 1991;83:1832-1847.


SummarySummary
• Sudden cardiac death (SCD) in the athlete is rare.Sudden cardiac death (SCD) in the athlete is rare.
• Identifying individuals at risk for SCD (i.e., primary Identifying individuals at risk for SCD (i.e., primary prevention) is very difficult.prevention) is very difficult.
• Guidelines for individuals with known Guidelines for individuals with known cardiovascular disease (i.e., secondary prevention) cardiovascular disease (i.e., secondary prevention) have been published -- 26th Bethesda Conference.have been published -- 26th Bethesda Conference.
SummarySummary
• A detailed history and physical exam should be A detailed history and physical exam should be performed on all athletes.performed on all athletes.
• Noninvasive testing should be used selectively.Noninvasive testing should be used selectively.
• Must educate the public about the limits of Must educate the public about the limits of screening and preventing SCD in the athlete. screening and preventing SCD in the athlete. It is not possible to achieve zero-risk in It is not possible to achieve zero-risk in competitive sports.competitive sports.
• Community efforts should focus on developing Community efforts should focus on developing and implementing systems of care that allows and implementing systems of care that allows for prompt response and treatment.for prompt response and treatment.