the california institute for mental health functional famiily therapy (fft) symposium april 28 –...
TRANSCRIPT

The California Institute for Mental Health
FUNCTIONAL FAMIILY THERAPY (FFT) SYMPOSIUM
April 28 – 29, 2010Sheraton Gateway Los Angeles Hotel
“The Core of FFT”
James F Alexander, Ph.D.University of Utah & FFT
Happy Birthday Mary

The Core of FFT
What is our “essence?” …
Our “character?” …
Our “mission?” …
What do we do? …(Actions speak louder than words!)

The Core of FFT (2)• Think “comedy”
• What is good comedy? What makes comedy “work?” Do we even “need” good comedy - or art or music or
poetry or fiction or sports and recreation for that matter?
• What does it take to create good comedy? Good art? Good fiction? A 2.42 ERA? A beautiful mural on a building in downtown LA? A meaningful mural on a
building in downtown
• Can everyone do it? - NO!
• Can we afford for only the “special few” to be able to do it? - NO!

The Core of FFT (2): What Is FFT?• First, FFT is a person – a person “doing” FFT √
• FFT is a “model;” a framework, a way to “think” and plan, and a guide or map with steps about what to do and when to do it √
• FFT also is a “model,” or framework, for training, monitoring, and maintaining quality > effectiveness; It is a system with feedback and internal correction built in, which also is available to others (yep – the old/new “transparency” thing ) √
• Doing FFT well is determined if not defined by our (and our client families’) ethnicity, religion, gender, social class, political beliefs, intelligence
… NOT !!!! …Influenced by? …. Yes. But determined by? NO!
• Doing FFT well is determined, if not defined by, our attitudes, our beliefs, our passion, our “heart,” and our stubbornness √
(selective! )
What Are These Beliefs? • Something about these people can change
• And I can do something to help that change to go in a positive direction
• I will do a better job if I follow a plan, a “model,” which has been shown to be effective (“efficacious”) with very troubled families often with great challenges like the ones we see
• I (yep, us …. Not just the families) am better off if I do this right!
(Not “make,” “force,” “insure,”)
Someone is watching, and cares!

Oh Yes …. And Then There is the “Doing” Part!
• “Style”– Relational / interpersonal sensitivity, ability to do what is
“right” for the other (not just what is “right”). (R&R: READ& REACT)– And to do it in a way that “matches”
• “Respectful” in a way that they experience as respectful and appropriate - for them!
• Reaches out to them in the domains in which they “live” / exist, can experience productively, and function:
• Specifically, “match” them in terms of “where they are”– Affect, Behavior, Cognitions (ABC’s)
» Centro De La Familia family based Gang Prevention program for girls» Fathers? (Directors’ attitudes & gender preference)
• And “Substance”– Techniques …. Embedded in Phases …. And with structuring skills
GENERALIZATIONGENERALIZATION Eco/Multi- Eco/Multi-
systemic systemic Linking Linking
BEHAVIOR CHANGE
Sessions1 2 3 4 5 6 7 >>>> End
ENGAGEMENT
Pre-Treat-ment
Post-Treat-ment
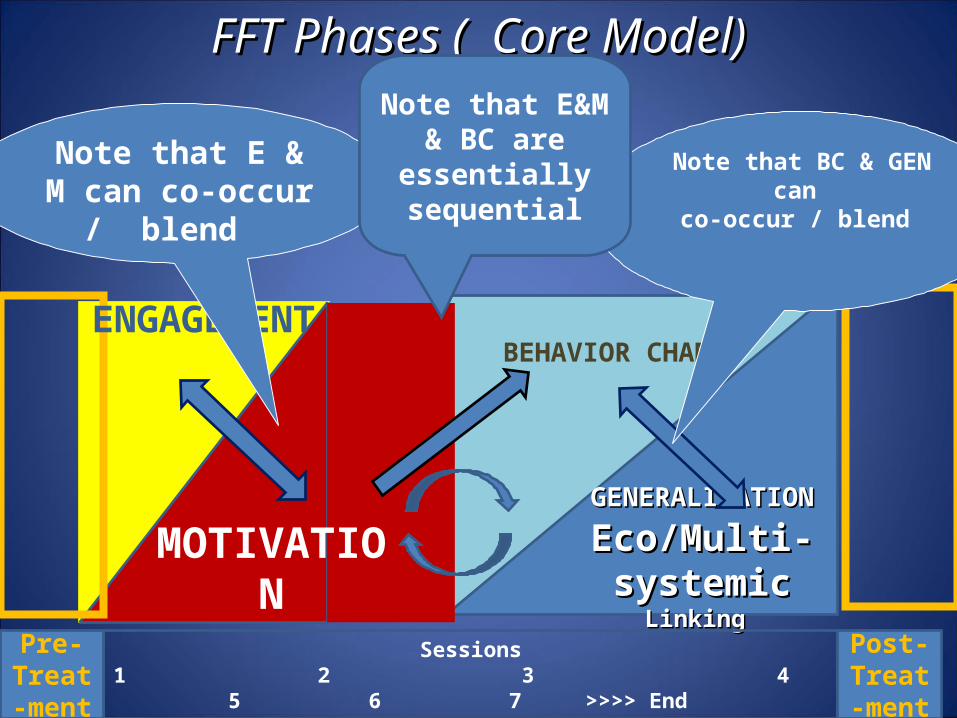
Note that E & M can co-occur / blend
Note that BC & GEN can co-occur / blend
FFT Phases ( Core Model)FFT Phases ( Core Model)
MOTIVATION
Note that E&M & BC are essentially
sequential

GENERALIZATIONGENERALIZATION, , Eco/Multi- systemic Linking Eco/Multi- systemic Linking
BEHAVIOR CHANGE
Sessions
Pre-Treat-ment
Post-Treat-ment
FFT Unique Components and FFT Unique Components and Phase Strategy Phase Strategy
MOTIVATION
RelationalAssessment&
Matching
ENGAGEMENT
MOTIVATION
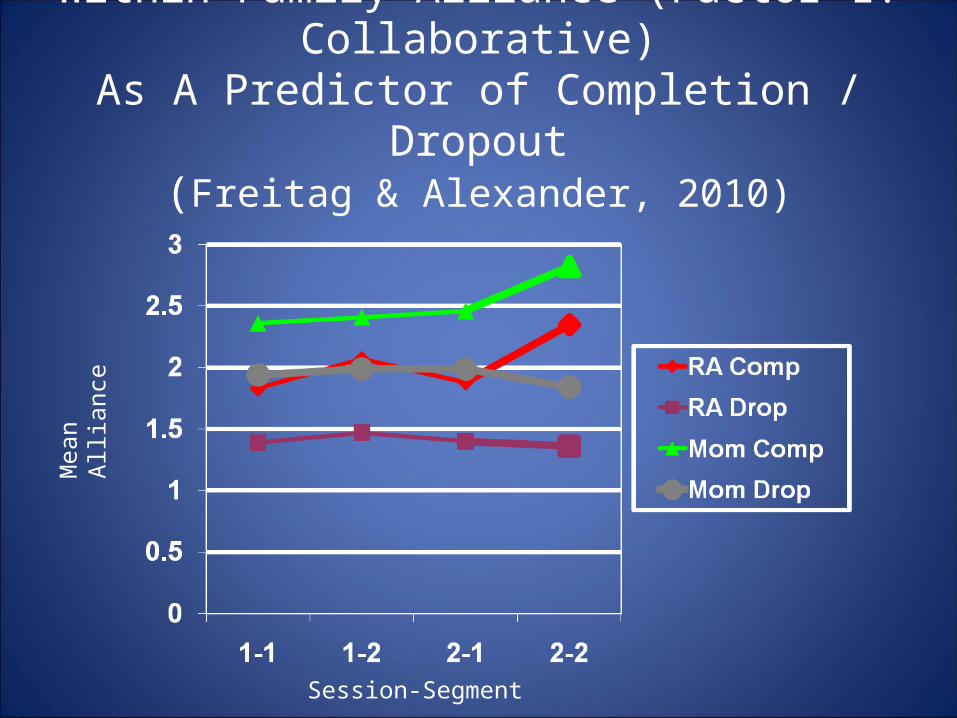
Within Family Alliance (Factor 1: Collaborative)As A Predictor of Completion / Dropout
(Freitag & Alexander, 2010)
Mea
n Al
lianc
e
Session-Segment

GENERALIZATIONGENERALIZATION, , Eco/Multi- systemic Eco/Multi- systemic Linking Linking
BEHAVIOR CHANGE
Sessions
Pre-Treat-ment
“ “Generic,” Major Syndrome Specific,Generic,” Major Syndrome Specific,** or Context Specific or Context Specific**** Matching & Techniques Matching & Techniques
*Adol Substance Abuse, Adol PTSD, Sex Offender, Gangs, “mental *Adol Substance Abuse, Adol PTSD, Sex Offender, Gangs, “mental health”health”
**Child Welfare. Integrated Reentry**Child Welfare. Integrated Reentry
Post-Treat-ment
MOTIVATION
RelationalAssessment&
Matching
ENGAGMENT
MOTIVATION

The Complete FFT Dissemination Model Phases
PretreatmentPretreatmentSystem Integration System Integration
PhasePhase
PosttreatmentSystem Integration
Phase
FFT CW Direct TreatmentFFT CW Direct Treatment PhasesPhases
- - EngagementEngagement- MotivationMotivation- Relational > BehavioralRelational > Behavioral AssessmentAssessment- Behavior Change- Behavior Change- Generalization / Ecosystemic - Generalization / Ecosystemic Integration Integration
The Youth / Family “Management” or Support System(s): The Youth / Family “Management” or Support System(s): Child Welfare, Mental Health, Justice, Drug Court, Welfare, EducationalChild Welfare, Mental Health, Justice, Drug Court, Welfare, Educational
Boosters, Boosters, Maintenance of Maintenance of links w/ Youth links w/ Youth Mgt Systems, Mgt Systems, Positive closePositive close
Referral, Preparation,Pretreatment
Linking w/ Youth Mgt
Systems
* Based on Alexander et al, 1983; Barton et al, 1985; Waldron et al, 2001 * Based on Alexander et al, 1983; Barton et al, 1985; Waldron et al, 2001
AssessmentAssessment AssessmentAssessment AssessmentAssessment

Assessment by Phase - Generic
PretreatmentPretreatmentSystem Integration System Integration
PhasePhase
PosttreatmentSystem Integration
Phase
FFT CW Direct TreatmentFFT CW Direct Treatment PhasesPhases
- - EngagementEngagement- MotivationMotivation- Relational > BehavioralRelational > Behavioral AssessmentAssessment- Behavior Change- Behavior Change- Generalization / Ecosystemic - Generalization / Ecosystemic Integration Integration
The Youth / Family “Management” or Support System(s): The Youth / Family “Management” or Support System(s): Child Welfare, Mental Health, Justice, Drug Court, Welfare, EducationalChild Welfare, Mental Health, Justice, Drug Court, Welfare, Educational
Boosters, Boosters, Maintenance of Maintenance of links w/ Youth links w/ Youth Mgt Systems, Mgt Systems, Positive closePositive close
Referral, Preparation,Pretreatment
Linking w/ Youth Mgt
Systems
* Based on Alexander et al, 1983; Barton et al, 1985; Waldron et al, 2001 * Based on Alexander et al, 1983; Barton et al, 1985; Waldron et al, 2001
AssessmentAssessment AssessmentAssessment AssessmentAssessment
Evaluate Risk &
Protective Factors for
Triage; Assess already involved systemsRelational
Functions, Deficits &
strengths, safety & initial
treatment challenges
Skill deficits & challenges, short
and long term change goals (Behaviors, Emotions, & Cognitions)
Extra-family & Multiple system
challenges & positive
resources

Syndrome-Specific Specialization vs Syndrome-informed EM, BC, & Gen
• Adolescent substance abuse / use, Adolescent PTSD, Adolescent Sex Offender, Child Welfare, and Integrated Reentry all represent syndromes and contexts commonly encountered by many FFT therapists.
• As a result, FFT therapists responsible for the larger range of FFT referrals will be provided as many FFT-specific tools (knowledge & techniques – but only within their “scope of practice” abilities & training) as possible as we move into increasingly diverse treatment contexts.
• However, these syndromes and contexts also can represent specialty training tracks offered as packages to specific treatment systems (e.g., institutions with reentry / “aftercare” treatment responsibilities; Drug Courts, Child Welfare Systems, Mental Health systems specializing in PTSD, Dual Dx Depression / Anxiety). In this case, FFT therapists will be trained as teams providing specific FFT “packages.” This training will be more extensive, and will require manualized and evidence-informed versions of FFT, primarily during Behavior Change.

GRYD Risk & Protective Factor Domains (“Ecological Model”)
Youth
Family
Community, Neighborhood
Institutions

The Moment of Decision – Proximal and Distal Influences
Youth
Family
Community
Institutions
Peers?

The Moment of Decision: Proximal Influences
Youth
Family
Community
Institutions
Peers?
Attachment issues, Internal
sense of “security”
Identity, “Self Concept”
Behavioral Styles & Patterns, Skills
Self Regulation (self soothing,
emotional intelligence,
impulse control
“Internal” Representation of
Family, Community Peers, “Institutions” Biological Risk &
Protective Factors

The Moment of Decision: Proximal Influences
Youth
Attachment
“Self Concept”
Behavior Patterns, Skills
Self Regulation
“Internal “Representations of
Others
Biological R & P

Cancer Staging (as a metaphor) •Stage 1: Usually cancer is relatively small & contained ; seemingly easily treated “non aggressively”
•Stage 2: The tumor is larger than in stage 1 ... Sometimes spread into lymph nodes.
Aggressive Tx necessary, but with high long term outcomes
•Stage 3: cancer is larger ...started to spread … ...cancer cells in the lymph nodes in the area
• •Stage 4: cancer has spread from where it started
to another body organ. Very aggressive interventions necessary, but with low “success” rates nonetheless

Gang “Staging”•Stage 1: Risk / Protective factor ratio is low; seemingly easily treated “non aggressively;” low probability of gang entry under current conditions
•Stage 2: Risk / Protective factor ratio higher; low but discernable levels of gang-related behaviors
appear; attitudes positive re gangs
•Stage 3: Clear identification w/ gang mentality; aggression > violence; 1 major or several less serious but notable criminal behaviors;
•Stage 4: Major gang involvement, high offense rate, few or no protective factors, long duration of
criminal behaviors, violence and/or heavy economic integration.

What Are The Risk Factors? (GRYD)• Youth (10-15), four or more risk factors, highest risk
• Antisocial Tendencies– Isolates self, Unable to work as part of a socially acceptable group – Rebels against authority
• Impulsive Risk Taking– without first considering potential consequences. (“Impulsivity”) – experience s dangerous or illegal acts as thrilling (“Under-arousal?”)
• Neutralization (Rationalization; externalization; no guilt)– Justifies actions hurtful to others, – Consistent victimizing and manipulating others; rationalizing that it
is acceptable– Unable to show or feel remorse or accept responsibility
• Delinquency & Substance Abuse– Frequently involved in illegal behaviors connected to drug use
• Negative Peer Influence & Peer Delinquency– Associates w/ friends directly involved in illegal activities

What Are The Risk Factors (2)? • Critical Life Events
– a traumatic event – in combination with other risk factors may the “the last straw”
• Weak Parental Supervision– Lacks parental guidelines – street activities without the knowledge/ supervision of parents.– parents are often physically or emotionally absent
• Family Gang Influence– influential family members active in formal gang activity.– family values that affirm and accept gang involvement as normal
• • Personal” – ADHD, depression, anxiety, etc ( JFA)Separate “trait” /
genotype contributions from phenotype (contextually elicited & reinforced components.
• JFA Addition – school / vocational involvement; guilt is good, -parents permissive, - do as I say not do as I do. (not as big a problem) – are separate issues
•
