tfessd contribution to improved accountability and...
TRANSCRIPT
Green and Inclusive Development: Harnessing TFESSD Knowledge
Presented by Amadeus Kamagenge, TASAF Management Unit
Kunduchi Beach Hotel and Resort, Dar es Salaam, Thursday, 17 November 2011
TFESSD contribution to Improved Accountability and Delivery of
CB-CCT Pilot in TASAF

Outline
Country overview and policy context
Overview of TASAF
Features of the Community Based-CCT Pilot
Using CSC to enhance accountability in CB-CCT
Mobile phone transfers
Concluding remarks

TF095119, Community-Based Conditional Cash Transfers (CB-CCT) with Mobile Phone Banking
Community score cards and focus groups financed by TFESSD were aimed at improving and evaluating processes that were also implemented by CB-CCT under TASAF.
The mobile phone transfers component also funded by TFESSD was aimed at reducing the potential for leakage of funds as well as the administrative burden placed on communities and local government authorities.

Tanzania Country Overview and Policy Context

Country profile Tanzania is a low income
country with a population estimated at 41 million people.
Total area: 945,000 km2 Average GDP growth: about
7% per annum. Per capita income of US$
400 per annum. The poor in Tanzania are overwhelmingly rural (84% of
the poor), and overwhelmingly dependent on agriculture as their primary source of income (74%).
Policy context
Providing adequate social protection and rights to the vulnerable and needy groups is one among six goals of Cluster II on Improvement of Quality of Life and Social Well-being of a five-year the National Strategy for Growth and Poverty Reduction (MKUKUTA).
The National Social Protection Framework (NSPF) targets the poor and vulnerable groups living far below the poverty line and those with special needs, e.g. orphans, vulnerable children, unemployed youth, poor widows , single mothers, people with disabilities, poor elderly and people living with HIV and AIDS.
The NSPF gives priority to the needs of those who are unable to sufficiently address the risks associated with poverty and vulnerability.

Overview of the Tanzania Social Action Fund (TASAF)

TASAF Program Overview
The Tanzania Social Action Fund (TASAF) was established in 2000 following successful implementation of a pilot in 1999.
TASAF is part of Government of Tanzania’s Strategy for reducing poverty and improving livelihoods by stimulating economic activity at the community level.
TASAF is a nationwide CDD operation that finances small scale economic and social infrastructures and delivers social assistance to poor and vulnerable groups contributing to social capital and development at local level.
TASAF Program Overview ….
TASAF also provides support to and helps build capacity of the district and village councils as well as community management committees.
TASAF-I was completed in 2005. The second phase started in 2005. TASAF-II is now under implementation and its completion has been extended to is 2013.
The PDO of TASAF-II is to improve access of beneficiary households to enhanced socio-economic services and income generating opportunities.

Overview of the Community-Based Conditional Cash Transfer (CB-CCT ) Pilot

Rationale for a conditional transfer Inadequate utilization by extremely poor households
of social infrastructure (esp. health facilities and schools) put in place through TASAF.
Orphans constitute about 11 percent of children under 18yrs.
Grand parents are care givers of a big number children, since 5.7 percent of adults are estimated to be infected with HIV.
Elderly are about 2.0 million, many elderly have been left to seek alternative livelihood mechanisms, and for the poorest households there are few options.

Specific objectives Increase primary school attendance of most vulnerable children (MVCs) by
using CCT as an incentive. Increase health visits of orphans and vulnerable children 0-5 years and
vulnerable elderly (60+ years) by using CCT as an incentive. Develop operational modalities for the community-driven delivery of a CCT
programme through TASAF-II operation. Test the effectiveness of the community-based CCT model against centralized
CCT programmes. Inform government policy on the best modalities to deliver support to MVCs
and vulnerable elderly.
Development Objective To test how a conditional cash transfer (CCT) program could be implemented through a social fund using a community-driven development (CDD) approach, and what incentive framework may need to be in place to achieve results.

Target population Most Vulnerable Children Old person
Most Vulnerable children: • One parent or both parents deceased, or abandoned children, or • Having one or two chronically ill parents (e.g. HIV/AIDS), or • Chronically ill children despite having two parents alive
Elderly: • Elderly with no caregivers • Poor health • Very poor
• Community based targeting • Proxy means testing
Eligibility criteria
Targeting mechanism
Program area and coverage Two regions and three district councils
Dodoma Region: Chamwino District Council
Pwani Region: Bagamoyo District Council Kibaha District Council
80 TASAF-I villages: 40 phase one (treatment) 40 phase two (control)
4,998 beneficiary households 13,081 individual beneficiaries

Benefit size and delivery mechanism Size of transfer ranges from US$6 minimum to $18 maximum
depending on the number of people in the household. US$ 3/month for children (50% of food poverty line) US$ 6/month for elderly (100% of food poverty line) Payments are made bimonthly (every two months). Funds are routed to the communities through district councils. The
community management committees make payments to individual beneficiary households.
Plans are underway to leverage other modern mechanism, like bio metrics technology, commercial banks, incl. ATMs and mobile phone transfers, e.g. Airtel Money, Tigo Pesa, Zantel Z-Pesa, Vodacom MPESA, etc.

Implementation arrangement
• The Program is organized in a decentralized manner to facilitate greater autonomy and empowerment to local government structures and the community.
• The Program operates within the three spheres of Government, i.e. national, local government authority and village levels
• Community Management Committee (CMC) is responsible for day-to-day Program implementation management at the community level.
• Grant agreement was signed in September 2007. • Implementation of the Pilot commenced in September
2008, the first transfer was made in December 2009
Financing of the Pilot Program Government of the United Republic of Tanzania Government of Japan (Japan Social Development Fund) International Development Association (IDA) – supported
modest scale up Governments of Finland and Norway (Trust Fund for
Environmentally and Socially Sustainable Development -TFESSD) – supported impact evaluation and mobile phone study. Funding managed by WB.
Government of Spain (SIEF) – supported impact evaluation. Funding managed by WB.
Government of the United States of America (USAID) - to support impact evaluation (financing approved but funds not yet accessed)
Rapid Social Response Fund - Multi Donor Trust Fund (RSR-MDTF) – to support livelihood component (financing approved but funds not yet accessed)

How would the use Community Score Cards in CB-CCT enhance accountability?

Why use CSCs in the CB-CCT pilot? As pilot program, a need to ensure maximum
chance of success Critical success factors incl. transparency,
downward accountability, and ‘learning by doing’
‘Community-based’ administration requires need for decentralized monitoring.
A system for regular feedback to correct possible problems in implementation is required.
Cash transfers should be accompanied with greater voice of vulnerable and poor households
Therefore a strong case
for using participatory monitoring or
social accountability tool like CSC.
TASAF experience with CSC
strengths this case.
Using CSCs - points considered CSC is meant to be integrated in implementation of
CB-CCT– to promote accountability and get feedback
CSC it is part of the ‘treatment’ or ‘program’ being evaluated
CSC to provide information for process and impact evaluation
Linked to but separate from qualitative evaluation (latter looks at outcomes and impact, while CSC focuses mostly on inputs and outputs)
Emphasis was to use existing methodology and systems for running CSC within TASAF
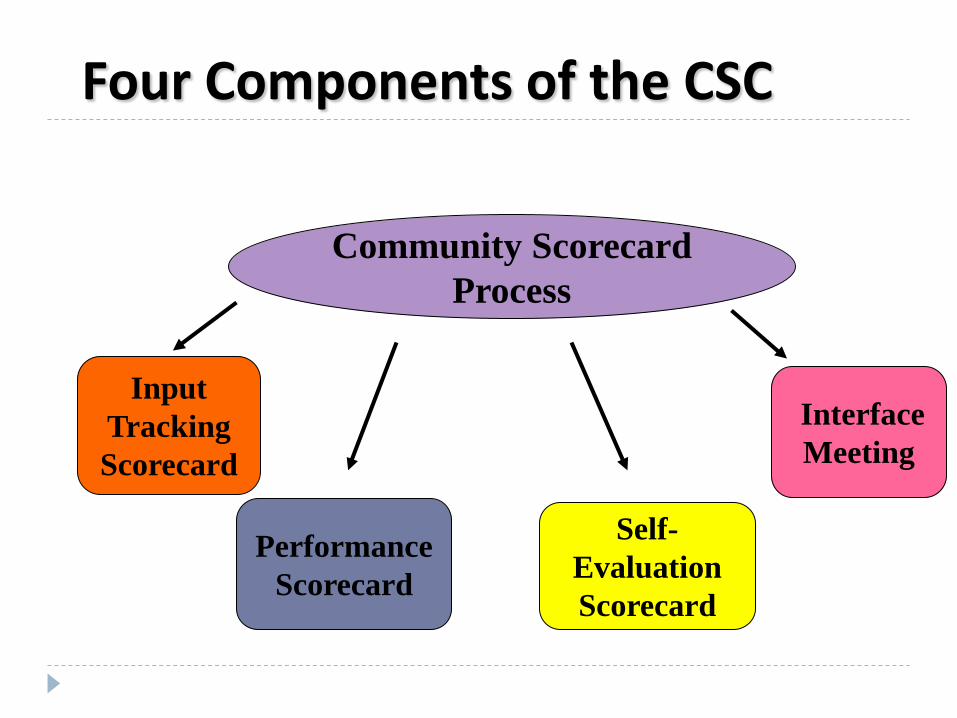
Four Components of the CSC
Input Tracking Scorecard
Performance Scorecard
Community Scorecard Process
Self-Evaluation Scorecard
Interface Meeting

Stages in the CSC process
Preparatory Groundwork
Community Gathering Input Tracking Scorecard Performance Scorecard
Interface Meeting
Feedback and Dialogue
Reform Accountability
Transparency Empowerment
Efficiency
Development
•Divide into focus groups •Information on entitlements/ budgets •Develop input indicators •Collect evidence on input use • “Transact Walk” • Record data
• Divide into focus groups • Develop performance indicators • Finalize indicators (5-8 max.) • Performance scoring by groups • Verify High/Low Scores • Record data
Self-Evaluation Scorecard

Changes are in the context of CSC
Monitoring performance of the CB-CCT program
Monitoring performance of participating schools and health facilities (alongside supply side capacity assessment)
Two application contexts:

Input tracking for the CB-CCT
Here the supply side data came from the MIS system for the CB-CCT.
Input tracking was a kind of mini-audit for things like – payments made, compliance records, timing, etc.
CSC covered a sample of beneficiary households and was triangulate with members of community management committee (CMC).

Example of input tracking matrix in CB-CCT context…
Input MIS Records
CMC Records Actual Remarks/
Comments
Cash Transfer - HH 1
Compliance Records
Timing of transfer
…

Community Performance Score Cards for CB-CCT Methodology used was the same as with CSC
already being done by TASAF Standardizing a set of indicators for comparing
over time was considered Allowance for some new community
determined indicators each time was made Focus groups of beneficiaries, non-beneficiaries
(but eligible), households who dropped out, elderly, MVC, women vs. men, etc.

Provider self-evaluation scorecards and interface meeting in CB-CCT
Here the ‘providers’ are effectively the CMCs
Also included district level staff Separate focus groups for schools and
health centers Interface meeting were conducted

CSCs for schools and health facilities
These were similar to those conducted from TASAF
This looked at how the schools and health centers are performing
It served as part of the supply side capacity assessment
It informed the impact evaluation (as a proxy variable for quality of facilities)

The Way Forward on CSC
Frequency – at least annual Timing – could be part of enrollment process Could also be timed with qualitative assessment Coverage – all treatment groups Implementation by TASAF through TMU Data to be incorporated within the MIS system as
well Incorporating in the overall budget of the
Program

Mobile phone transfers

Objectives and outputs
Identify companies with the potential for mobile phone transfers and having sufficient coverage in terms of cash-disbursing agents to be workable in CB-CCT program villages. Existing agents in program program
villages and/or nearby villages. Service providers that have service access
potential
Objectives and outputs
Examining the technology requirements of disbursing funds to individual beneficiaries of the CB-CCT program. Beneficiaries having phones and/or access to them Options and potential cost of providing phones to
beneficiaries without phones Explored cost-effective alternatives, including
providing a SIM card to beneficiaries that could be used at the agent’s office
Objectives and outputs
Calculated the costs of implementing mobile phone transfers for 5000 households, including both the additional costs associated with setting up such a system and the cost reductions that may be incurred as result of reduced administrative work (e.g., transport for CMC members)
Step by step plan to rollout the mobile phone transfers

Concluding Remarks

Achievements and lessons learned So far the Program has disbursed ten rounds of transfers. The tenth transfer amounted to a total of US$ 100,050.00 for
12,828 beneficiaries Total beneficiary households in the registry are 13,081 Total amount transferred to-date US$ 731,072.41 Supportive systems, including computerized MIS are in place and
operational. Communities have been able to undertake targeting, follow-up
compliance verification, make payment to the beneficiaries (collectively and individually) and make reconciliation of transferred funds.

Challenges as indicated by CSC and qualitative assessment The CSC and qualitative assessment indicated that
Proxy Means Test (PMT) model rejected many would-be beneficiaries in some villages.
Some villages are located very far away from town where commercial banks operate.
Ineffective mechanisms to handle grievance and complaints from beneficiaries.
Predictability of payment date on the part of community management committees and beneficiaries.
Compliance verification and disbursement of funds is taking long than earlier on expected.
Some villages which have low compliance rates and other show abnormal trend.

Way Forward informed by the studies
The PMT model has been revised to minimize exclusion error.
Studies informed Process evaluation undertaken to establish required adjustments in timing, personnel, forms, mechanisms incl. grievances mechanism.
Explore alternative and modern ways of transferring cash, monitoring compliance using mobile phones.
Follow up in villages that have shown low compliance rates and other show abnormal trend.
Implement support to livelihoods in treatment and control villages.
Studies informed the preparations for modest scale up under additional financing for TASAF-II
Studies have informed nationwide scale up under TASAF III Productive Social Safety Net (PSSN).
TFESSD contribution to Improved Accountability and Delivery of CB-CCT Pilot in TASAF
Thank you for your attention
Contact for details: [email protected]