editorial temmuz 2018 web.pdf · spontaneous pneumothorax in a patient with birt-hogg-dube syndrome...
TRANSCRIPT

ISSUE 3 JULY 2018 VOLUME
19Official Journal of the Turkish Thoracic Society
www.turkthoracj.org
EditorialAirway Clearance and VaccinationAslı Görek Dilektaşlı and Zeynep Pınar Önen; Bursa, Ankara, Turkey
Original ArticlesThe Efficacy of Physiotherapy in BronchiectasisBilge Üzmezoğlu et al.; Ankara, Edirne, Hatay
Allergen-Exposure Avoidance Scale and Inhaler Use Scales’ Reliability and Construct ValidityDöndü Şanlıtürk and Sultan Ayaz Alkaya; Tokat, Ankara, Turkey
Diagnosis of Chest Diseases in Refugees and Turkish CitizensŞerif Kurtuluş et al.; Şanlıurfa, Eskişehir, Turkey
Factors Affecting Influenza Vaccination among COPD PatientsSongül Özyurt et al.; Rize, Turkey
Bronchoscopy High-Frequency Jet VentilationAtefeh Abedini et al.; Tehran, Iran
Violation of Tobacco Law by Drivers in IzmirErdem Erkoyun et al.; İzmir, Turkey
The Turkish Sleep Apnea DatabaseYüksel Peker et al.; İstanbul, İzmir, Ankara, Turkey; Lund, Sweden; PA, USA
ReviewReview of Bronchoscopic Lung Volume Reduction ProceduresAşkın Gülşen; Borstel, Lübeck, Germany
Case ReportsSpontaneous Pneumothorax in a patient with Birt-Hogg-Dube SyndromeEngin Karaman et al.; Denizli, Turkey
Tuberculoma in a Child with SLE-NephritisHeda Melinda Nataprawira et al.; Bandung, Indonesia
Letter to the EditorPseudo-Authorshipİbrahim Onur Alıcı; İzmir, Turkey
EISSN 2149-2530 Indexed in
PubMed and
Web of Science

A-I
EDITORSOğuz KILINÇDepartment of Chest Diseases, Dokuz Eylül University School of Medicine, İzmir, Turkey
Metin AKGÜNDepartment of Chest Diseases, Atatürk University School of Medicine, Erzurum, Turkey
ASSOCIATE EDITORSMehmet BAYRAMDepartment of Chest Diseases, Bezmialem Vakıf University School of Medicine, İstanbul, Turkey
Ufuk ÇAĞIRICIDepartment of Chest Surgery, Ege University School of Medicine, İzmir, Turkey
Begüm ERGANDepartment of Chest Diseases, Dokuz Eylül University School of Medicine, İzmir, Turkey
Aslı GÖREK DİLEKTAŞLIDepartment of Chest Diseases, Uludağ University School of Medicine, Bursa, Turkey
Zuhal KARAKURTRespiratory Intensive Care Unit, Süreyyapaşa Chest Diseases and Surgery Training and Research Hospital, İstanbul, Turkey
Zeynep Pınar ÖNENDepartment of Chest Diseases, Ankara University School of Medicine, Ankara, Turkey
Özge YILMAZDepartment of Pediatrics, Celal Bayar University School of Medicine, Manisa, Turkey
BIOSTATISTICAL CONSULTANTAhmet Uğur DEMİRDepartment of Chest Diseases, Hacettepe University School of Medicine, Ankara, Turkey
PUBLICATION COORDINATORHasan BAYRAMDepartment of Chest Diseases, Koç University School of Medicine, Gaziantep, Turkey
Türk Toraks Derneği adına sahibi / Owner on behalf of the Turkish Thoracic Society: Hasan Bayram • Yayın türü / Publication Type: Yerel süreli / Local periodical • Yayın tarihi / Publication Date: Temmuz 2018 / July 2018 • Türk Toraks Derneği tarafından yayınlanmaktadır / Published by Turkish Thoracic Society, Turan Güneş Bulvarı Koyunlu Sitesi No: 175/19 Oran-Ankara, Turkey (+90 312 490 40 50)
Publisherİbrahim KARA
Publication DirectorAli ŞAHİN
Finance and Administration Zeynep YAKIŞIRER
Deputy Publication DirectorGökhan ÇİMEN
Editorial DevelopmentGizem KAYAN
Publication CoordinatorsBetül ÇİMENÖzlem ÇAKMAKOkan AYDOĞANMerve SAĞLAMERİrem DELİÇAY
Project AssistantsBüşra PARMAKSIZEcenur ASLIMCansu ASLAN
Graphics DepartmentÜnal ÖZERDeniz DURAN
ContactAddress: Büyükdere Cad. No: 105/9 34394 Mecidiyeköy, Şişli-İstanbulPhone: +90 212 217 17 00Fax: +90 212 217 22 92E-mail: [email protected]
ISSUE 3 JULY 2018 VOLUME
19Official Journal of the Turkish Thoracic Society

A-II
INTERNATIONAL EDITORIAL BOARD
Ian M. AdcockCell and Molecular Biology Airways Disease Section, National Heart and Lung Institute, Imperial College London, United Kingdom Piergiuseppe AgostoniDepartment of Clinical Sciences and Community Health, Cardiovascular Section, Università di Milano, Milano, Italy M. Selim ArcasoyPulmonary, Allergy, and Critical Care Division, Department of Medicine, Columbia University New York, USA Philippe AstoulThoracic Oncology - Pleural Diseases - Interventional Pulmonology, Hôpital Nord - Chemin des Bourrely, Marseille, France Ülkü BayındırRetired Faculty Member, Ege University School of Medicine, İzmir, Turkey Dominique MA BullensDepartment of Immunology and Microbiology, KU Leuven Laboratory of Pediatric Immunology Division of Pediatrics, Leuven, Belgium Richard CasaburiRehabilitation Clinical Trials Center, Los Angeles Biomedical Research Institute at Harbor-UCLA Medical Center, Torrance, California, USA Turgay ÇelikelDepartment of Chest Diseases, Marmara University School of Medicine, İstanbul, Turkey Tansu Ulukavak ÇiftçiDepartment of Chest Diseases, Gazi University School of Medicine, Ankara, Turkey Lütfi ÇöplüDepartment of Chest Diseases, Hacettepe University School of Medicine, Ankara, Turkey Çağlar ÇuhadaroğluAcıbadem Maslak Hospital, İstanbul, Turkey
Andrew J. GhioUS Environmental Protection Agency Chapel Hill, North Carolina, USA İlhan İnciUniversity Hospital Zurich, Department of Thoracic Surgery, Zurich, Switzerland Oya İtilDepartment of Chest Diseases, Dokuz Eylül University School of Medicine, İzmir, Turkey A. Fuat KalyoncuDepartment of Chest Diseases, Hacettepe University School of Medicine, Ankara, Turkey Fazilet KarakoçDepartment of Child Chest Diseases, Marmara University Pendik Training and Research Hospital, İstanbul, Turkey Ali KocabaşDepartment of Chest Diseases, Çukurova University School of Medicine, Adana, Turkey Emel KurtDepartment of Chest Diseases, Osmangazi University School of Medicine, Eskişehir, Turkey Richard LightDivision of Allergy, Pulmonary, Critical Care, Vanderbilt University Medical Center, Nashville, USA Atul MalhotraPulmonary and Critical Care, University of California San Diego, La Jolla, California, USA Muzaffer MetintaşDepartment of Chest Diseases, Osmangazi University School of Medicine, Eskişehir, Turkey Zeynep MısırlıgilDepartment of Chest Diseases, Ankara University School of Medicine, Ankara, Turkey
Nesrin MoğulkoçDepartment of Chests Diseases, Ege University School of Medicine, İzmir, Turkey
Official journal of the Turkish Thoracic Society

Dilşad MunganDepartment of Chest Diseases, Ankara University School of Medicine, Ankara, Turkey Gökhan M. MutluDivision of Pediatric Critical Care Medicine, Nortwestern University, Chicago, USA Gül ÖngenDepartment of Chest Surgery, İstanbul University Cerrahpaşa School of Medicine, İstanbul, Turkey Kent E. PinkertonUniversity of California, Davis, Center for Health and the Environment, Davis, USA Kannan RamarDivision of Pulmonary and Critical Care Medicine, Center for Sleep Medicine, Mayo Clinic, Rochester, MN, USA Joseph RocaInstituto de Biología Molecular de Barcelona, CSIC, Baldiri Reixac, Barcelona, Spain Israel RubinsteinSection of Pulmonary, Critical Care, Sleep and Allergy Medicine, Department of Medicine, College of Medicine, University of Illinois at Chicago, Chicago, Illinois, USA
Abdullah SayınerDepartment of Chest Diseases, Ege University School of Medicine, İzmir, Turkey Z. Toros SelçukDepartment of Chest Diseases, Hacettepe University School of Medicine, Ankara, Turkey Nadja TrillerDepartment of Pulmonary Medicine, University Pulmonary Clinic Golnik, Golnik, Slovenia Haluk TürktaşDepartment of Chest Diseases, Gazi University School of Medicine, Ankara, Turkey E. Sabri UçanDepartment of Chest Diseases, Dokuz Eylül University School of Medicine, İzmir, Turkey Karlman WassermanRespiratory and Critical Care Physiology and Medicine, Los Angeles Biomedical Research Institute Harbor-UCLA Medical Center, Torrance, California, USA Mark WoodheadHonorary Clinical Professor of Respiratory Medicine, Department of Respiratory Medicine, Manchester Royal Infirmary, Manchester, England
A-III
Official journal of the Turkish Thoracic Society

A-IV
AIMS AND SCOPE
Turkish Thoracic Journal (Turk Thorac J) is the double-blind, peer-reviewed, open access, international publication or-gan of Turkish Thoracic Society. The journal is a quarterly publication, published on January, April, July, and October and its publication language is English.
Turkish Thoracic Journal started its publication life following the merger of two journals which were published under the titles “Turkish Respiratory Journal” and “Toraks Journal” until 2007. Archives of both journals were passed on to the Turkish Thoracic Journal.
The aim of the journal is to convey scientific developments and to create a dynamic discussion platform about pul-monary diseases. With this intent, the journal accepts articles from all related scientific areas that address adult and pediatric pulmonary diseases, as well as thoracic imaging, environmental and occupational disorders, intensive care, sleep disorders and thoracic surgery. Clinical and research articles, reviews, statements of agreement or disagreement on controversial issues, national and international consensus reports, abstracts and comments of important interna-tional articles, interesting case reports, writings related to clinical and practical applications, letters to the editor, and editorials are accepted.
The editorial and publication processes of the journal are shaped in accordance with the guidelines of the International Committee of Medical Journal Editors (ICMJE), World Association of Medical Editors (WAME), Council of Science Editors (CSE), Committee on Publication Ethics (COPE), European Association of Science Editors (EASE), and National Informa-tion Standards Organization (NISO). The journal is in conformity with the Principles of Transparency and Best Practice in Scholarly Publishing (doaj.org/bestpractice).
Turkish Thoracic Journal is indexed in PubMed Central, Web of Science - Emerging Sources Citation Index, Scopus, EMBASE, EBSCO, CINAHL, Gale/Cengage Learning, ProQuest, DOAJ, and TUBITAK ULAKBIM TR Index.
Processing and publication are free of charge with the journal. No fees are requested from the authors at any point throughout the evaluation and publication process. All manuscripts must be submitted via the online submission sys-tem, which is available at www.turkthoracj.org. The journal guidelines, technical information, and the required forms are available on the journal’s web page.
All expenses of the journal are covered by the Turkish Thoracic Society. Potential advertisers should contact the Editorial Office. Advertisement images are published only upon the Editor-in-Chief’s approval.
Statements or opinions expressed in the manuscripts published in the journal reflect the views of the author(s) and not the opinions of the Turkish Thoracic Society, editors, editorial board, and/or publisher; the editors, editorial board, and publisher disclaim any responsibility or liability for such materials.
All published content is available online, free of charge at www.turkthoracj.org. Printed copies of the journal are distrib-uted to the members of the Turkish Thoracic Society, free of charge.
Turkish Thoracic Society holds the international copyright of all the content published in the journal.
Editors in Chief: Prof. Oğuz KILINÇProf. Metin AKGÜNAddress: Turan Güneş Bulvarı, Koyunlu Sitesi No: 175/19 Oran, Ankara, TURKEYPhone: +90 (312) 490 40 50Fax: +90 (312) 490 41 42E-mail: [email protected]
Publisher: AVES Address: Büyükdere Cad., 105/9 34394 Mecidiyeköy, Şişli, İstanbul, TURKEYPhone: +90 212 217 17 00Fax: +90 212 217 22 92E-mail: [email protected] page: avesyayincilik.com

A-V
Turkish Thoracic Journal (Turk Thorac J) is the double-blind, peer-reviewed, open access, in-ternational publication organ of Turkish Thorac-ic Society. The journal is a quarterly publication, published on January, April, July, and October and its publication language is English.
The aim of the journal is to convey scientific developments and to create a dynamic discus-sion platform about pulmonary diseases. With this intent, the journal accepts articles from all related scientific areas that address adult and pediatric pulmonary diseases, as well as tho-racic imaging, environmental and occupational disorders, intensive care, sleep disorders and thoracic surgery. Clinical and research articles, reviews, statements of agreement or disagree-ment on controversial issues, national and in-ternational consensus reports, abstracts and comments of important international articles, interesting case reports, writings related to clinical and practical applications, letters to the editor, and editorials are accepted.
The editorial and publication processes of the journal are shaped in accordance with the guidelines of the International Council of Medi-cal Journal Editors (ICMJE), the World Associa-tion of Medical Editors (WAME), the Council of Science Editors (CSE), the Committee on Publi-cation Ethics (COPE), the European Association of Science Editors (EASE), and National Informa-tion Standards Organization (NISO). The journal conforms to the Principles of Transparency and Best Practice in Scholarly Publishing (doaj.org/bestpractice). Originality, high scientific quality, and citation potential are the most important criteria for a manuscript to be accepted for publication. Manuscripts submitted for evaluation should not have been previously presented or already published in an electronic or printed medium. The journal should be informed of manuscripts that have been submitted to another journal for evaluation and rejected for publication. The submission of previous reviewer reports will expedite the evaluation process. Manuscripts that have been presented in a meeting should be submitted with detailed information on the organization, including the name, date, and lo-cation of the organization. Manuscripts submitted to Turkish Thoracic Journal will go through a double-blind peer-re-view process. Each submission will be reviewed by at least two external, independent peer re-viewers who are experts in their fields in order to ensure an unbiased evaluation process. The editorial board will invite an external and inde-pendent editor to manage the evaluation pro-cesses of manuscripts submitted by editors or
by the editorial board members of the journal. The Editor in Chief is the final authority in the decision-making process for all submissions. An approval of research protocols by the Eth-ics Committee in accordance with international agreements (World Medical Association Decla-ration of Helsinki “Ethical Principles for Medical Research Involving Human Subjects,” amended in October 2013, www.wma.net) is required for experimental, clinical, and drug studies and for some case reports. If required, ethics commit-tee reports or an equivalent official document will be requested from the authors. For manu-scripts concerning experimental research on humans, a statement should be included that shows that written informed consent of pa-tients and volunteers was obtained following a detailed explanation of the procedures that they may undergo. For studies carried out on animals, the measures taken to prevent pain and suffering of the animals should be stated clearly. Information on patient consent, the name of the ethics committee, and the ethics committee approval number should also be stated in the Materials and Methods section of the manuscript. It is the authors’ responsibility to carefully protect the patients’ anonymity. For photographs that may reveal the identity of the patients, releases signed by the patient or their legal representative should be enclosed. All submissions are screened by a similarity de-tection software (iThenticate by CrossCheck). In the event of alleged or suspected research misconduct, e.g., plagiarism, citation manipu-lation, and data falsification/fabrication, the Editorial Board will follow and act in accordance with COPE guidelines. Each individual listed as an author should fulfil the authorship criteria recommended by the International Committee of Medical Journal Editors
(ICMJE - www.icmje.org). The ICMJE recom-mends that authorship be based on the follow-ing 4 criteria:1 Substantial contributions to the conception
or design of the work; or the acquisition, analysis, or interpretation of data for the work; AND
2 Drafting the work or revising it critically for important intellectual content; AND
3 Final approval of the version to be published; AND
4 Agreement to be accountable for all aspects of the work in ensuring that questions relat-ed to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
In addition to being accountable for the parts of the work he/she has done, an author should be able to identify which co-authors are respon-sible for specific other parts of the work. In addi-tion, authors should have confidence in the in-tegrity of the contributions of their co-authors. All those designated as authors should meet all four criteria for authorship, and all who meet the four criteria should be identified as authors. Those who do not meet all four criteria should be acknowledged in the title page of the manu-script. Turkish Thoracic Journal requires correspond-ing authors to submit a signed and scanned version of the authorship contribution form (available for download through www.turktho-racj.org) during the initial submission process in order to act appropriately on authorship rights and to prevent ghost or honorary authorship. If the editorial board suspects a case of “gift au-thorship,” the submission will be rejected with-out further review. As part of the submission of the manuscript, the corresponding author should also send a short statement declaring that he/she accepts to undertake all the respon-sibility for authorship during the submission and review stages of the manuscript. Turkish Thoracic Journal requires and encour-ages the authors and the individuals involved in the evaluation process of submitted manu-scripts to disclose any existing or potential con-flicts of interests, including financial, consultant, and institutional, that might lead to potential bias or a conflict of interest. Any financial grants or other support received for a submitted study from individuals or institutions should be dis-closed to the Editorial Board. To disclose a po-tential conflict of interest, the ICMJE Potential Conflict of Interest Disclosure Form should be filled in and submitted by all contributing au-thors. Cases of a potential conflict of interest of the editors, authors, or reviewers are resolved by the journal’s Editorial Board within the scope of COPE and ICMJE guidelines. The Editorial Board of the journal handles all appeal and complaint cases within the scope of COPE guidelines. In such cases, authors should get in direct contact with the editorial office regarding their appeals and complaints. When needed, an ombudsperson may be assigned to resolve cases that cannot be resolved internally. The Editor in Chief is the final authority in the decision-making process for all appeals and complaints. When submitting a manuscript to Turkish Tho-racic Journal, authors accept to assign the copy-right of their manuscript to Turkish Thoracic So-
INFORMATION FOR THE AUTHORS

A-VI
ciety. If rejected for publication, the copyright of the manuscript will be assigned back to the authors. Turkish Thoracic Journal requires each submission to be accompanied by a Copyright Transfer Form (available for download at www.turkthoracj.org). When using previously pub-lished content, including figures, tables, or any other material in both print and electronic for-mats, authors must obtain permission from the copyright holder. Legal, financial and criminal liabilities in this regard belong to the author(s). Statements or opinions expressed in the manu-scripts published in Turkish Thoracic Journal reflect the views of the author(s) and not the opinions of the editors, the editorial board, or the publisher; the editors, the editorial board, and the publisher disclaim any responsibility or liability for such materials. The final responsibility in regard to the published content rests with the authors. MANUSCRIPT PREPARATION The manuscripts should be prepared in accor-dance with ICMJE-Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals (updated in December 2017 - http://www.icmje.org/icmje-recommendations.pdf ). Authors are required to prepare manuscripts in accordance with the CONSORT guidelines for randomized research studies, STROBE guidelines for observational original research studies, STARD guidelines for studies on diagnostic accuracy, PRISMA guide-lines for systematic reviews and meta-analysis, ARRIVE guidelines for experimental animal studies, and TREND guidelines for non-random-ized public behaviour. Manuscripts can only be submitted through the journal’s online manuscript submission and evaluation system, available at www.turktho-racj.org. Manuscripts submitted via any other medium will not be evaluated. Manuscripts submitted to the journal will first go through a technical evaluation process where the editorial office staff will ensure that the manuscript has been prepared and submit-ted in accordance with the journal’s guidelines. Submissions that do not conform to the jour-nal’s guidelines will be returned to the submit-ting author with technical correction requests.
Authors are required to submit the following:• Copyright Transfer Form,• Author Contributions Form, and• ICMJE Potential Conflict of Interest Disclo-
sure Form (should be filled in by all contrib-uting authors)
during the initial submission. These forms are available for download at www.turkthoracj.org. Preparation of the ManuscriptTitle page: A separate title page should be submitted with all submissions and this page should include:• The full title of the manuscript as well as a short
title (running head) of no more than 50 characters,• Name(s), affiliations, and highest academic
degree(s) of the author(s),• Grant information and detailed information
on the other sources of support,• Name, address, telephone (including the mo-
bile phone number) and fax numbers, and email address of the corresponding author,
• Acknowledgment of the individuals who con-tributed to the preparation of the manuscript but who do not fulfill the authorship criteria.
Abstract: An English abstract should be submit-ted with all submissions except for Letters to the Editor. Submitting a Turkish abstract is not com-pulsory for international authors. The abstract of Original Articles should be structured with subheadings (Objective, Material and Methods, Results, and Conclusion). Please check Table 1 below for word count specifications. Keywords: Each submission must be accompa-nied by a minimum of three to a maximum of six keywords for subject indexing at the end of the abstract. The keywords should be listed in full without abbreviations. The keywords should be selected from the National Library of Medicine, Medical Subject Headings database (https://www.nlm.nih.gov/mesh/MBrowser.html). Manuscript TypesOriginal Articles: This is the most important type of article since it provides new informa-tion based on original research. The main text of original articles should be structured with In-troduction, Material and Methods, Results, and Discussion subheadings. Please check Table 1 for the limitations for Original Articles.
Statistical analysis to support conclusions is usu-ally necessary. Statistical analyses must be con-ducted in accordance with international statis-tical reporting standards (Altman DG, Gore SM, Gardner MJ, Pocock SJ. Statistical guidelines for contributors to medical journals. Br Med J 1983: 7; 1489-93). Information on statistical analyses should be provided with a separate subheading under the Materials and Methods section and the statistical software that was used during the process must be specified. Units should be prepared in accordance with the International System of Units (SI).
Editorial Comments: Editorial comments aim to provide a brief critical commentary by re-viewers with expertise or with high reputation in the topic of the research article published in the journal. Authors are selected and invited by the journal to provide such comments. Ab-stract, Keywords, and Tables, Figures, Images, and other media are not included. Review Articles: Reviews prepared by authors who have extensive knowledge on a particular field and whose scientific background has been translated into a high volume of publications with a high citation potential are welcomed. These authors may even be invited by the jour-nal. Reviews should describe, discuss, and eval-uate the current level of knowledge of a topic in clinical practice and should guide future stud-ies. The main text should contain Introduction, Clinical and Research Consequences, and Con-clusion sections. Please check Table 1 for the limitations for Review Articles. Case Reports: There is limited space for case reports in the journal and reports on rare cases or conditions that constitute challenges in diag-nosis and treatment, those offering new thera-pies or revealing knowledge not included in the literature, and interesting and educative case reports are accepted for publication. The text should include Introduction, Case Presenta-tion, and Discussion subheadings. Please check Table 1 for the limitations for Case Reports. Letters to the Editor: This type of manuscript discusses important parts, overlooked aspects, or lacking parts of a previously published ar-ticle. Articles on subjects within the scope of
Table 1. Limitations for each manuscript type
Type of manuscript Word limit Abstract word limit Reference limit Table limit Figure limitOriginal Article 3500 250 (Structured) 35 6 7 or total of 15 imagesReview Article 5000 250 50 6 10 or total of 20 imagesCase Report 1000 200 15 No tables 10 or total of 20 imagesLetter to the Editor 500 No abstract 5 No tables No media

A-VII
the journal that might attract the readers’ atten-tion, particularly educative cases, may also be submitted in the form of a “Letter to the Editor.” Readers can also present their comments on the published manuscripts in the form of a “Letter to the Editor.” Abstract, Keywords, and Tables, Figures, Images, and other media should not be included. The text should be unstructured. The manuscript that is being commented on must be properly cited within this manuscript.
TablesTables should be included in the main docu-ment, presented after the reference list, and they should be numbered consecutively in the order they are referred to within the main text. A de-scriptive title must be placed above the tables. Abbreviations used in the tables should be de-fined below the tables by footnotes (even if they are defined within the main text). Tables should be created using the “insert table” command of the word processing software and they should be arranged clearly to provide easy reading. Data presented in the tables should not be a repeti-tion of the data presented within the main text but should be supporting the main text.
Figures and Figure LegendsFigures, graphics, and photographs should be submitted as separate files (in TIFF or JPEG format) through the submission system. The files should not be embedded in a Word document or the main doc-ument. When there are figure subunits, the subunits should not be merged to form a single image. Each subunit should be submitted separately through the submission system. Images should not be labelled (a, b, c, etc.) to indicate figure subunits. Thick and thin arrows, arrowheads, stars, asterisks, and similar marks can be used on the images to support figure legends. Like the rest of the submission, the figures too should be blind. Any information within the im-ages that may indicate an individual or institution should be blinded. The minimum resolution of each submitted figure should be 300 DPI. To prevent de-lays in the evaluation process, all submitted figures should be clear in resolution and large in size (mini-mum dimensions: 100 × 100 mm). Figure legends should be listed at the end of the main document. All acronyms and abbreviations used in the manuscript should be defined at first use, both in the abstract and in the main text. The abbre-viation should be provided in parentheses fol-lowing the definition. When a drug, product, hardware, or software program is mentioned within the main text, product information, including the name of the product, the producer of the product, and city and the country of the company (including the state if in USA), should be provided in parenthe-
ses in the following format: “Discovery St PET/CT scanner (General Electric, Milwaukee, WI, USA)” All references, tables, and figures should be re-ferred to within the main text, and they should be numbered consecutively in the order they are referred to within the main text. Limitations, drawbacks, and the shortcomings of original articles should be mentioned in the Discus-sion section before the conclusion paragraph.
References
While citing publications, preference should be given to the latest, most up-to-date publica-tions. If an ahead-of-print publication is cited, the DOI number should be provided. Authors are responsible for the accuracy of references. Journal titles should be abbreviated in accor-dance with the journal abbreviations in Index Medicus/ MEDLINE/PubMed. When there are three or fewer authors, all authors should be listed. If there are four or more authors, the first three authors should be listed followed by “et al.” In the main text of the manuscript, refer-ences should be cited using Arabic numbers in parentheses. The reference styles for different types of publications are presented in the fol-lowing examples. Journal Article: Rankovic A, Rancic N, Jovanovic M, et al. Impact of imaging diagnostics on the budget - Are we spending too much? Vojnosa-nit Pregl 2013;70:709-11. Book Section: Suh KN, Keystone JS. Malaria and babesiosis. Gorbach SL, Barlett JG, Blacklow NR, editors. Infectious Diseases. Philadelphia: Lip-pincott Williams; 2004.p.2290-308. Books with a Single Author: Sweetman SC. Martindale the Complete Drug Reference. 34th ed. London: Pharmaceutical Press; 2005. Editor(s) as Author: Huizing EH, de Groot JAM, editors. Functional reconstructive nasal surgery. Stuttgart-New York: Thieme; 2003. Conference Proceedings: Bengisson S. So-themin BG. Enforcement of data protection, privacy and security in medical informatics. In: Lun KC, Degoulet P, Piemme TE, Rienhoff O, edi-tors. MEDINFO 92. Proceedings of the 7th World Congress on Medical Informatics; 1992 Sept 6-10; Geneva, Switzerland. Amsterdam: North-Holland; 1992. pp.1561-5. Scientific or Technical Report: Cusick M, Chew EY, Hoogwerf B, Agrón E, Wu L, Lindley A, et al. Early Treatment Diabetic Retinopathy Study Research Group. Risk factors for renal replacement therapy in the Early Treatment Diabetic Retinopathy Study (ETDRS), Early Treatment Diabetic Retinopathy Study Kidney Int: 2004. Report No: 26.
Thesis: Yılmaz B. Ankara Üniversitesindeki Öğrencilerin Beslenme Durumları, Fiziksel Ak-tiviteleri ve Beden Kitle İndeksleri Kan Lipidleri Arasındaki Ilişkiler. H.Ü. Sağlık Bilimleri En-stitüsü, Doktora Tezi. 2007. Manuscripts Accepted for Publication, Not Pub-lished Yet: Slots J. The microflora of black stain on human primary teeth. Scand J Dent Res. 1974. Epub Ahead of Print Articles: Cai L, Yeh BM, West-phalen AC, Roberts JP, Wang ZJ. Adult living donor liver imaging. Diagn Interv Radiol. 2016 Feb 24. doi: 10.5152/dir.2016.15323. [Epub ahead of print]. Manuscripts Published in Electronic Format: Morse SS. Factors in the emergence of infec-tious diseases. Emerg Infect Dis (serial online) 1995 Jan-Mar (cited 1996 June 5): 1(1): (24 screens). Available from: URL: http:/ www.cdc.gov/ncidodlElD/cid.htm. REVISIONSWhen submitting a revised version of a paper, the author must submit a detailed “Response to the reviewers” that states point by point how each issue raised by the reviewers has been covered and where it can be found (each re-viewer’s comment, followed by the author’s re-ply and line numbers where the changes have been made) as well as an annotated copy of the main document. Revised manuscripts must be submitted within 30 days from the date of the decision letter. If the revised version of the manuscript is not submitted within the allocat-ed time, the revision option may be cancelled. If the submitting author(s) believe that additional time is required, they should request this exten-sion before the initial 30-day period is over. Accepted manuscripts are copy-edited for gram-mar, punctuation, and format. Once the publica-tion process of a manuscript is completed, it is published online on the journal’s webpage as an ahead-of-print publication before it is included in its scheduled issue. A PDF proof of the accept-ed manuscript is sent to the corresponding au-thor and their publication approval is requested within 2 days of their receipt of the proof. Editors in Chief: Prof. Oğuz KILINÇProf. Metin AKGÜNAddress: Turan Güneş Bulvarı, Koyunlu Sitesi No: 175/19 Oran, Ankara, TURKEYPhone: +90 (312) 490 40 50Fax: +90 (312) 490 41 42E-mail: [email protected] Publisher: AVESAddress: Büyükdere Cad. 105/9 34394 Mecidi-yeköy, Şişli, İstanbul, TurkeyPhone: +90 212 217 17 00Fax: +90 212 217 22 92E-mail: [email protected]

A-VIII
CONTENTS
EditorialEssentials in the Comprehensive Management of Chronic Respiratory Diseases: Airway Clearance and VaccinationAslı Görek Dilektaşlı, Zeynep Pınar Önen; Bursa, Ankara, Turkey
Original ArticlesThe Efficacy of Flutter® and Active Cycle of Breathing Techniques in Patients with Bronchiectasis: A Prospective, Randomized, Comparative StudyBilge Üzmezoğlu, Gündeniz Altıay, Levent Özdemir, Hakan Tuna, Necdet Süt; Ankara, Edirne, Hatay, Turkey
Development of an Allergen-Exposure Avoidance Scale and Inhaler Use Scale for Patients with Asthma: A Reliability and Construct Validity StudyDöndü Şanlıtürk, Sultan Ayaz Alkaya; Tokat, Ankara, Turkey
Chest Diseases in Refugees Living in a Tent Camp and in Turkish Citizens Living in the District: Ceylanpınar ExperienceŞerif Kurtuluş, Zafer Hasan Ali Sak, Remziye Can; Şanlıurfa, Eskişehir, Turkey
Factors Affecting Influenza Vaccination Rates among Patients with Chronic Obstructive Pulmonary Disease in Rize, TurkeySongül Özyurt, Bilge Yılmaz Kara, Neslihan Özçelik, Ünal Şahin; Rize, Turkey
High-Frequency Jet Ventilation in Nonintubated PatientsAtefeh Abedini, Arda Kiani, Kimia Taghavi, Ali Khalili, Alireza Jahangiri Fard, Lida Fadaizadeh, Alireza Salimi, Tahereh Parsa, Akram Aarabi, Behrooz Farzanegan, Mahsa Pourabdollah Tootkaboni; Tehran, Iran
Violation of the Tobacco Control Law by Drivers in Vehicles in Two Streets in İzmir: A Descriptive StudyErdem Erkoyun, Mustafa Selahattin Alçiçek, Simge Selek; İzmir, Turkey
Rationale and Design of the Turkish Sleep Apnea Database - TURKAPNE: A National, Multicenter, Observational, Prospective Cohort StudyYüksel Peker, Özen K. Başoğlu, Hikmet Fırat, TURKAPNE Study Group; İstanbul, İzmir, Ankara, Turkey; Lund, Sweden; PA, USA
ReviewBronchoscopic Lung Volume Reduction: A 2018 Review and UpdateAşkın Gülşen; Borstel, Lübeck, Germany
Case ReportsA Rare Cause of Recurrent Spontaneous Pneumothorax: Birt-Hogg-Dube SyndromeEngin Karaman, Furkan Ufuk, Mahmut Demirci, Hüseyin Gökhan Yavaş; Denizli, Turkey
Delayed Diagnosis of Tuberculoma in a Child with Nephritis due to Systemic Lupus ErythematosusHeda Melinda Nataprawira, Gartika Sapartini, Ketut Indriani; Bandung, Indonesia
Letter to the EditorAuthors: Sapiens H, Consilius H, Laborem H, Mutuus H, Exercitationa H, Parasitorum H, Gloria Hİbrahim Onur Alıcı; İzmir, Turkey
Erratum
101
103
110
117
122
127
132
136
141
150
153
156158

Turk Thorac J 2018; 19(3): 101-2
Editorial
See Article: Üzmezoğlu B, Altıay G, Özdemir L, et al. The Efficacy of Flutter® and Active Cycle of Breathing Techniques in Patients with Bronchiectasis: A Prospective, Randomized, Comparative Study. Turk Thorac J 2018; 19(3): 103-9.
Özyurt S, Yılmaz Kara B, Özçelik N, et al. Factors Affecting Influenza Vaccination Rates among Patients with Chronic Obstructive Pulmonary Disease in Rize, Turkey. Turk Thorac J 2018; 19(3): 122-6
Essentials in the Comprehensive Management of Chronic Respiratory Diseases: Airway Clearance and Vaccination
Bronchiectasis is defined as an irreversible dilatation of a portion of the bronchial tree, with the destruction of elastic and muscular components of their walls, often caused by recurrent or severe infections [1]. This predisposes to reduction in the clearance of mucoid and mucopurulent secretions.
Chronic symptoms and recurrent exacerbations are explained by the vicious cycle hypothesis, with chronic bron-chial infection, impaired mucociliary clearance, and bronchial tissue damage being the key components of the dis-ease [2]. Mucociliary clearance is impaired by structural lung damage, airway dehydration, and excess mucus pro-duction. The main principles of bronchiectasis treatment are to alleviate acute and chronic bronchial infections and to improve the impaired mucociliary clearance in order to reduce pulmonary symptoms and prevent exacerbations [3]. Presumably, airway clearance techniques (ACTs) should be performed once or twice daily in patients with chronic cough or those with difficulty in expectorating sputum [2]. There are various ACTs, with oscillatory positive expiratory pressure (PEP) therapy being a common practice. Previous evidence has suggested that airway clearance with PEP therapy is beneficial compared with usual care [4]. However, current evidence for the choice of ACTs remains weak because existing studies in the literature are small scaled and poorly comparable owing to method-ological differences. Additionally, bronchiectasis is a common but orphan disease, and there are a limited number of original papers in the literature. In this issue of Turkish Thoracic Journal, Üzmezoğlu et al. [5] have reported that both oscillatory oscillatory PEP device, the Flutter®, and the active cycle of breathing techniques are associated with sig-nificant reductions in dyspnea in a 4-week parallel, randomized trial comparing two groups. Moreover, the authors have shown that the Flutter causes a more pronounced effect on the health-related quality of life and fatigue com-pared to active cycle of breathing techniques.
Patients with chronic respiratory diseases, such as chronic obstructive pulmonary disease and bronchiectasis devel-op frequent exacerbations, which are an important cause of reduced quality of life, morbidity, and mortality [6]. Main causes of exacerbations are of infectious origin. Vaccination against influenza can reduce lower respiratory tract infections, number of exacerbations, hospitalizations, and mortality in chronic obstructive pulmonary disease (COPD) patients, particularly in elderly group and patients with concomitant chronic cardiac comorbidities [7]. Pneumococcal vaccination has been shown to reduce community-acquired pneumonia in COPD patients with a severe airflow limitation (FEV1<40%) and below 65 years of age [8]. Therefore, protective strategies, such as routine vaccination against influenza and pneumococci, are directed towards the prevention of acute exacerbations of chronic respiratory diseases. Unfortunately, although risk groups are well-defined and reimbursed in Turkey, vacci-nation rates still remain low in these risk groups. In this issue of Turkish Thoracic Journal, Özyurt et al. [9] have reported considerably low rates of vaccination for both influenza and pneumococcus in Rize, Turkey. Their results are in accordance with those of other studies reporting low vaccination rates in COPD patients from Turkey [10, 11]. Further studies evaluating the main reasons underlying low vaccination rates in COPD patients in Turkey are warranted.
DOI: 10.5152/TurkThoracJ.2018.31818
Aslı Görek Dilektaşlı1 , Zeynep Pınar Önen2 1Department of Chest Diseases, Uludağ University School of Medicine, Bursa, Turkey2Department of Chest Diseases, Ankara University School of Medicine, Ankara, Turkey
Address for Correspondence: Aslı Görek Dilektaşlı, Department of Chest Diseases, Uludağ University School of Medicine, Bursa, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org 101
Cite this article as: Görek Dilektaşlı A, Önen ZP. Essentials in the Comprehensive Management of Chronic Respiratory Diseases: Airway Clearance and Vaccination. Turk Thorac J 2018; 19(3): 101-2

REFERENCES
1. Önen ZP, Gülbay BE, Şen E, et al. Analysis of the Factors Related
to Mortality in Patıents with Bronchiectasis. Respir Med 2007;101:1390-7. [CrossRef]
2. Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiartory Society guidelines fort he management of adult bronchiectasis. Eur Respir J 2017;50:1700629. [CrossRef]
3. Snijders D, Fernandez Dominguez B, Calgaro S, et al. Mucociliary clearance techniques for treating non-cystic fibro-sis bronchiectasis: Is there evidence? Int J Immunopathol Pharmacol 2015;28:150-9.
4. Lee AL, Burge AT, Holland AE. Positive expiratory pressure therapy versus other airway clearence techniques for bronchi-ectasis. Cochrane Database of Syst Rev 2017;9:CD011699.
5. Üzmezoğlu B, Altıay G, Özdemir L, et al. The efficacy of Flutter® and active cycle breathing techniques in patients with bronchiectasis: a prospective randomized, comparative study. Turk Thorac J 2018; 19(3): 103-9.
6. Yıldız OA, Önen ZP, Şen E, et al. Predictors of long-term sur-vival in patients with chronic obstructive pulmonary disease. Saudi Med J 2007;27:1866-72.
7. Huang CL, Nguyen PA, Kuo PL, et al. Influenza vaccination and reduction in risk of ischemic heart disease among chronic obstructive pulmonary elderly. Comput Methods Programs Biomed 2013;111:507-11. [CrossRef]
8. Alfageme I, Vazquez R, Reyes N, et al. Clinical efficacy of anti-pneumococcal vaccination in patients with COPD. Thorax 2006;61:189-95. [CrossRef]
9. Özyurt S, Kara BY, Özçelik N, Şahin Ü. Affecting influenza vac-cination rates among patients with chronic obstructive pulmo-nary diseases in Rize, Turkey. Turk Thorac J 2018; 19(3): 122-6.
10. Ciblak MA, Grip Platformu. Influenza vaccination rates in Turkey: Prevalence of risk groups, current vaccination status, factors influencing vaccine uptake and steps taken to increase vaccination rate. Vaccine 2013;31:518-23. [CrossRef]
11. Aka Aktürk Ü, Görek Dilektaşlı A, Şengül A, et al. Influenza and Pneumonia vaccination rates and factors affecting vaccination among patients with chronic obstructive pulmonary disease. Balkan Med J 2017;34:206-11. [CrossRef]
Turk Thorac J 2018; 19(3): 101-2
102

Turk Thorac J 2018; 19(3): 103-9
Original Article
The Efficacy of Flutter® and Active Cycle of Breathing Techniques in Patients with Bronchiectasis: A Prospective, Randomized, Comparative Study
INTRODUCTION
There are no definitive treatments of bronchiectasis. The objectives of treatment include achieving symptom control, preventing or reducing exacerbations, decelerating the progression of pulmonary injury, maintaining airway patency, and improving the quality of life, all of which are the factors to be accomplished merely by decreasing bronchial infection and inflammation and by increasing the mucociliary clearance [1]. Traditional physiotherapeutic methods used in patients with chronic pulmonary conditions such as bronchiectasis or cystic fibrosis increase the expectorated sputum volume as well as alveolar ventilation and decrease the frequency of infections. However, these conventional techniques have also been reported to result in temporary adverse effects on physiological parameters during the treatment phase and require the as-sistance of others [2]. In this regard, the Flutter® device represents an alternative to traditional physiotherapeutic modalities and has been increasingly used in the management of respiratory conditions characterized by chronic sputum production. Flutter® is a simple handheld device that allows removal of mucus from the airways using positive expiratory pressure (Figure 1) [3]. Active cycle of breathing techniques (ACBT) is a standard technique, and it bears some advantages. It is flex-ible, requires patient’s active participation, and requires neither the use of any specific devices nor any specific positioning. While breathing control prevents or diminishes airway narrowing, thoracic expansion exercises prevent deleterious effects of percussion (Figure 2) [2].
The objective of the present study was to compare the efficacy of home-based respiratory physiotherapy, either by means of the Flutter® device or by ACBT, on symptoms, sputum production, and perception of dyspnea, pulmonary functions, and health-related quality of life in patients with bronchiectasis. A study comparing autogenous drainage with Flutter® reported no differences in the amount of sputum produced by application of either of the two methods [4]; however, the Flutter® device was reported to be more effective in reducing viscoelasticity of the secretion. The positive expiratory pres-
DOI: 10.5152/TurkThoracJ.2018.17050
Bilge Üzmezoğlu1 , Gündeniz Altıay2 , Levent Özdemir3 , Hakan Tuna4 , Necdet Süt5
1Clinic of Occupational Diseases, Atatürk Chest Diseases and Thoracic Surgery Training and Research Hospital, Ankara, Turkey 2Department of Chest Diseases, Trakya University School of Medicine, Edirne, Turkey3Chest Diseases Service, Hatay Dörtyol State Hospital, Hatay, Turkey4Department of Physical Therapy and Rehabilitation, Trakya University School of Medicine, Edirne, Turkey5Department of Biostatistics and Medical Informatics, Trakya University School of Medicine, Edirne, Turkey
This study was presented in the European Respiratory Society (ERS) 2012 Annual Congress, September 1-5, 2012, Vienna, Austria.Address for Correspondence: Bilge Üzmezoğlu, Clinic of Occupational Diseases, Atatürk Chest Diseases and Thoracic Surgery Training and Research Hospital, Ankara, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
103
Cite this article as: Üzmezoğlu B, Altıay G, Özdemir L, et al. The Efficacy of Flutter® and Active Cycle of Breathing Techniques in Patients with Bronchiectasis: A Prospective, Randomized, Comparative Study. Turk Thorac J 2018; 19(3): 103-9.
OBJECTIVES: The objective of the study was to compare the efficacy of an oscillating positive expiratory device and the active cycle of breathing techniques (ACBT) in patients with bronchiectasis.
MATERIALS AND METHODS: A home-based study that lasted for 4 weeks was designed to compare the oscillating physiotherapy device Flutter® and the ACBT in 40 patients, who were randomly assigned into two groups containing 20 patients each. The effect of the two methods of physiotherapy on sputum production, pulmonary functions, and the quality of life was compared.
RESULTS: The results of the present study indicate that both the methods were associated with a reduced number of patients complain-ing of cough and fatigue and increased sputum production (p=0.000, p=0.004, and p=0.002, respectively). In addition, statistically significant reductions were determined by the Medical Research Council and Borg Dyspnea scores (p=0.001 and 0.002, respectively). The Flutter® device caused a more significant effect on the perception of dyspnea. Overall, there was an improvement in the physical sub-scale of the Short Form (SF)-36 Quality of Life Questionnaire scores of 36 patients who completed the study (p=0.001). During the physiotherapy period, no changes in pulmonary functions were observed. Exacerbations were recorded in 3 patients in the ACBT group and in 1 patient in the Flutter® group.
CONCLUSION: The Flutter® device and ACBT represent effective home-based physiotherapeutic methods. The Flutter® device appears to be more effective with regard to sputum production.
KEYWORDS: Bronchiectasis, pulmonary rehabilitation, oscillating physiotherapy device, active cycle of breathing techniques
Abstract
Received: 02.07.2017 Accepted: 29.01.2018 Available Online Date: 12.06.2018
An editorial comment on this article is available at page 101

sure was shown to be more effective than Flutter® in terms of preserving pulmonary function, hospital admissions, and an-tibiotic use in patients, who were followed up for 1 year [5]. Daily use of the Flutter® device at home was as effective as ACBT in patients with non-CF bronchiectasis, and it leads to higher levels of adherence by patients [3]. To our knowledge, there have not been many trials on evaluating effectiveness of home-based physiotherapy program. The aim of the study was to compare the efficacy of ACBT techniques with the Flutter® device in bronchiectasis patients.
MATERIALS AND METHODS
A prospective, randomized study was conducted to compare Flutter® and ACBT methods in patients with bronchiectasis. An approval by the Ethics Committee of the Trakya University School of Medicine, protocol no was 2009/153 and registered under the number 12/08, was obtained before commencing the study. A total of 40 patients, who were diagnosed with bronchi-ectasis and admitted to the Chest Diseases Department at the University Medical Faculty Hospital between December 2009 and March 2010 were included in this study if they complied with the inclusion criteria and met none of the exclusion crite-ria. The diagnosis of bronchiectasis was confirmed both clini-
cally and by HRCT. Twenty patients in each group, namely the ACBT and Flutter® groups, practiced home-based respiratory physiotherapy while continuing to receive their current treat-ment regimens. Patients were randomized into two separate study groups by a faculty member at the Department of Statis-tics of University using the MedCalc 11.5.1 package program. Figure 3 presents the flowchart for the study.
Inclusion criteria:
• Clinically stable patients• A diagnosis of bronchiectasis due to non-CF conditions in patients older than 18 years• Absence of acute and/or respiratory failure• No contraindication(s) for the physiotherapeutic method to be employedExclusion criteria:• A history of pneumothorax• Presence of cor pulmonale and/or heart failure• Presence of hemoptysis• Recent history of acute myocardial infarction• Presence of vertebral injury• Unstable intervertebral disc hernia and/or costal fracture• Severe osteoporosis • Respiratory distress requiring hospitalization
Patients were evaluated by a symptom assessment form, pulmonary function, and reversibility tests, the “Medical Re-search Council” scale, Borg Dyspnea Scale, and Short Form (SF)-36 Quality of Life Questionnaire. The assessments were performed at baseline and on days 10, 20, and 30.
Training on the Flutter® Device and ACBT Physiotherapy MethodAll patients received basic information and training on bron-chiectasis and respiratory physiotherapy on an individual ba-
Figure 2. The flowchart for performing an Active Cycle of Breathing Technique: BC, breathing control; TEE, thoracic expansion exercise; FET: forced expiration technique (http://bronchiectasis.com.au/physiotherapy/techniques/the-active-cycle-of-breathing-technique)
Figure 1. Parts of the Flutter device and the rate of oscillation (http://www.flutter.gen.tr/index.php?id=26)
Figure 3. The flowchart for the study
Patients diagnosed with bronchiectasis
n=40
Computer based randomization
ACBT n=20
ACBT training visits at baseline and 10,
20 and 30 days
3 patients with exacerbation
n=17
Flutter training visits at baseline and 10,
20 and 30 days
1 patients with exacerbation
n=19
Flutter n=20
Confirmation of the diagnosis
based on clinical findings and HRCT
Turk Thorac J 2018; 19(3): 103-9
104

sis. Following theoretical training, each patient in the ACBT group received practical training, individually.
The active cycle breathing chest physiotherapy technique with postural drainage consists of 3 steps (subjects were comfort-ably sitting in a standard chair): 1. Breathing control: The sub-ject breathes at a normal rate and depth using the lower chest. 2. By resting one hand on the epigastrium, allow the subject to breath in slowly and deeply using the lower chest (pause), then breathe out fully, but not forcefully. Repeat 2 to 3 times. Return to breathing control. 3. Sputum removal: The subject takes a slightly bigger-than-normal breath in, while keeping the mouth open and O shaped. The subject breathes out more forcefully by contracting the abdominal muscles while keeping the mouth and throat open. It should sound like a forced sigh as huffing (Figure 2) [6]. Return to breathing control till the patient is ready to begin another cycle. The patient is advised to start coughing out any sputum if necessary [7,8]. Each stan-dardized ACBT cycle lasted approximately for 2 min and was repeated for 15-20 min with postural drainage/gravity assisted drainage i.e., the use of specific positioning in which gravity enhances mucus transport from distal bronchi. The procedure was repeated twice daily with a minimum 6-h duration [9].
The training courses were planned and carried out with a specialist from the Department of Physical Therapy and Rehabilitation. After ascertaining that each patient fully un-derstood the instructions for the therapy, the physiotherapy sessions were commenced. Similarly, following the com-mencement of treatment, each patient received training on the use of the device in the Flutter® group, which would be practiced for 15-20 min twice daily. During each of the three follow-up visits after baseline, it was accessed whether the patients’ practice of the physiotherapeutic technique was performed properly i.e., as it was described during the train-ing sessions. The practice of physiotherapy was followed up by the Physiotherapy Practice Checklist, which included physiotherapy steps, the duration of physiotherapy, and how many times a day it was practiced. In case of inappropriate practices, training was repeated. For patients who could not attend the hospital visits, a telephone call was made or the patient was visited in his or her home to ascertain the proper use of the physiotherapeutic technique. An explanatory bro-chure was prepared and delivered to each patient for effec-tive home-based physiotherapy. Both therapy methods were performed twice daily by the patients.
Patient Assessment FormA “Bronchiectasis Patient Assessment Form” was made for all 40 study patients to collect and record information on personal data, demographic characteristics, past history, duration of disease, symptoms, follow-up of the changes in sputum production, and physical examination findings of the patients. The pulmonary function test (PFT) results, HRCT findings, the HRCT scores, Borg Dyspnea Scale, MRC Scale, and bronchodilator treatments received by the patients were recorded as well.
SymptomsCough, sputum, hemoptysis, wheezing, chest pain, fatigue, loss of appetite, sweating, and reflux were assessed before
and after physiotherapy, and they were recorded in the as-sessment form.
Changes in Sputum ProductionSputum production was evaluated in each patient before physiotherapy, and changes in sputum production were re-corded for each visit. A 4-category was used to determine the status of sputum production: 0, no sputum production; 1, reduced sputum production; 2, no change in sputum produc-tion; and 3, increased sputum production.
Pulmonary Function Tests (PFT)To assess the pulmonary functions, a Vmax 22 device (Sen-sormedics, USA) was used.
Dyspnea ScalesThe MRC and Modified Borg Dyspnea Scale were used. Scores before and after physiotherapy were recorded.
Short Form-36 Quality of Life QuestionnaireThis 36-item measure is divided into the following 8 sub-scales providing information on 36 items: physical function-ing (10 items), social functions (2 items), role limitations due to physical problems (4 items), role limitations due to emo-tional problems (3 items), general mental health (5 items), vi-tality and fatigue (4 items), pain (2 items), general health per-ception (5 items), and health transition (1 item). Items within subscales are summed up to provide a total score ranging from 0 (negative health) to 100 (positive health) [10,11]. SF-36 was completed by our patients both at the time-point when they provided informed consent and at the completion of visit 4. Assessments and scoring were performed at the end of the study period. Written informed consent was obtained from each patient after providing detailed information on the nature of the study. The study was supported by the Scien-tific Research Project Council (project no 2009/121, with the project approval date of October 21, 2009).
Statistical AnalysesFor the statistical analyses, Statistica 7.0 (Serial no: 31N6YUCV38) software pack was used. The difference be-tween the groups with regard to categorical variables was tested with Chi-square test, and nonparametric measure-ments were compared with the Mc Nemar test. The Wilcox-on paired two-sample test was used for the statistical anal-ysis of the change between the parameters. The difference in variables in pairwise group comparisons was assessed with the Bonferroni test. Data have been expressed as the mean±standard deviation, minimum, and maximum. The sta-tistical significance was set at a p-value of <0.05.
RESULTS
A total of 22 females (55%) and 18 males (45%) patients with a mean age of 54.18±11 were included in the study. Three patients in the ACBT group and 1 in the Flutter® group dis-continued participation due to exacerbations, while 17 and 19 patients in these two groups completed the study, respec-tively. The two groups were comparable with regard to demo-graphic characteristics, symptoms, sputum change, dyspnea scores, pulmonary function tests, and the SF-36 Quality of Life scores before physiotherapy (Table 1).
Üzmezoğlu et al. The Efficacy of Physiotherapy in Bronchiectasis
105

After 4 weeks of physiotherapy, the change in symptoms were compared both in all of the study patients as well as between the groups. Physiotherapy was associated with a decrease in the number of patients who had cough, wheez-ing, and fatigue, as well as an increase in the number of
patients with improved appetite. A comparison between the groups demonstrated a significant reduction in the number of patients with cough in the ACBT group after physiother-apy, whereas a significant reduction was found in the num-ber of patients with fatigue in the Flutter® group. Wheezing was reduced in the ACBT group; however, no changes were observed in the Flutter® group. The decrease in wheezing was not significant (Table 2). A within- and between-group comparison of the sputum production and of the changes in sputum revealed that there were 23 patients with and 13 pa-tients without sputum production. Among all study patients, 4 patients, who could not produce sputum, started produc-tion, and 9 patients had increased sputum production with physiotherapy. Increased sputum production was detected in 4 patients in ACBT group and in 5 patients in the Flutter® group. In both groups, the increase in sputum production was statistically significant (Table 3). A comparison of the PFT before and after physiotherapy showed significant de-creases in both groups. Inter- and intra-group comparisons in terms of the change in the PFT before and after physio-therapy in the Flutter® and ACBT groups did not show any significant differences.
Comparison of dyspnea scores before and after physiother-apy revealed significant reductions in both dyspnea scale scores of all study patients (Table 4). In the Flutter® group, the scores of both MRC and Borg dyspnea scales demonstrat-ed significant decreases compared to baseline scores before physiotherapy (p=0.012 and p=0.006, respectively); howev-er, a significant decrease in the MRC was detected only in the ACBT group (p=0.021). A comparison of the dyspnea scale scores before and after physiotherapy showed no differences between the groups (Table 4).
A comparison of the SF-36 Quality of Life Questionnaire scores before and after physiotherapy demonstrated a sta-tistically significant improvement in physical function and physical role subscales, whereas the increase in physical
Table 1. Baseline patient characteristics
Characteristic ACBT n:20 Flutter® n:20
Age (years) mean SD 54.9±9.1 53.5±5.9
Female n, (%) 12(60) 10(50)
Smoking n, (%)
Nonsmoker 11(55) 11(55)
Ex 8(40) 9(45)
Smoker 1(5) 0(0)
Previous disease n, (%)
Measles 3(15) 3(15)
Pertussis 0 (0) 1 (5)
Pneumonia 3(15) 10(50)
Pleuritis 0 (0) 2(10)
Tuberculosis 7(35) 1 (5)
Measles and pneumonia 2(10) 2(10)
Tuberculosis and pneumonia 0 (0) 2(10)
No history 6(30) 2(10)
Symptoms n, (%)
Cough 17(85) 11(55)
Sputum 14(72) 12(60)
Wheezing 8(40) 8(40)
Chest pain 3(15) 2(10)
Fatigue 13(65) 13(65)
Loss of appetite 3(15) 2(10)
Sweating 2(10) 3(15)
Reflux 7(35) 7(35)
PFT mean SD
FVC (%) 67.8±18.6 62.0±16.7
FEV1 (%) 70.8±28.2 60.6±23.4
FEV1/FVC 82.1±12.8 77.6±12.0
PEF (%) 85.5±55.9 65.0±23.4
PFT: pulmonary function test; SD: standard deviation; FVC: forced vital capacity; FEV1:1 expiratory volume at 1 sec; PEF: peak expiratory flow
Table 2. Changes in symptoms after physiotherapy in study groups
ACBT (n:17) Flutter (n:19)
Before After Before After physiotherapy (n) physiotherapy (n) p physiotherapy (n) physiotherapy (n) p
Cough 14 4 *0.002 10 5 0.13
Wheezing 5 2 0.38 8 8 1.0
Fatigue 11 7 0.22 12 4 *0.021
Loss of appetite 3 1 0.50 2 0 -
ACBT: active cycle of breathing technique, *: p<0.05
Table 3. Distribution of patients with increased sputum after physiotherapy
ACBT (n:17) Flutter (n:19)
After After physiotherapy (n) p physiotherapy (n) p
Sputum 4 *0.004 5 *0.003 increase
ACBT: active cycle of breathing technique; *: p<0.05
Turk Thorac J 2018; 19(3): 103-9
106

status score was also significant (Table 4). Comparison of the subscales of general health, physical functions, physi-cal role, emotional role, social functions, pain, energy level,
and general mental health showed an improvement in the general health, physical function, physical role, emotional role, social function, pain, and energy in the Flutter® group; however, only the improvement in the emotional role and pain yielded in statistically significant results. A comparison between the groups before and after physiotherapy showed no differences in subscale scores other than those of general health and pain subscales. While there was no improve-ment after physiotherapy in the ACBT group with regard to physical assessments (physical functions, physical role, pain, and general health) and mental health (energy, social functions, emotional role, and mental health), patients in the Flutter® group had partial and statistically significant improvement in physical status. However, the comparison between the groups did not reveal statistically significant results (Table 5).
DISCUSSION
Our study, comparing two different physiotherapeutic tech-niques scheduled to be practiced at home, determined that both techniques were effective in removing phlegm. We eval-uated the changes in symptoms after the physiotherapy. Eval-uation of symptoms experienced on a daily or intermittent basis by the patients may provide a measure of the success of physiotherapy. A symptomatic improvement observed in both groups is supportive of the efficacy of the physiotherapy programs used in this study. However, this warrants further studies. One of the aim of the physiotherapy should include a reduction in the symptoms that influence the quality of life of the patients. The effects of respiratory physiotherapy modali-ties on the volume of sputum have been subject to previous research. Despite the use of a variety of techniques, many
Table 4. Changes in dyspnea and the SF-36 Quality of Life Questionnaire after physiotherapy as compared to baseline
Before After physiotherapy physiotherapy n:36 n:36 Mean±SD Mean±SD p
Dyspnea Score
MRC Score 1.8±1.1 1.3±1.1 *0.001
Borg Score 2.8±1.9 1.9±1.7 *0.002
SF-36 QoL Questionnaire
General health 36.2±24.9 37.9±24.5 0.45
Physical functioning 69.4±24.6 74.6±23.1 *0.031
Physical role 63.9±39.4 75.7±35.6 0.036
Emotional role 48.2±30.3 53.7±22.9 0.44
Social functioning 62.2±19.9 58.0±19.2 0.19
Pain 73.7±23.6 78.8±23.0 0.23
Vitality 49.6±20.8 45.7±19.2 043
Mental health 67.0±19.7 64.0±18.9 0.78
SF-36 Outcome Score
Physical state 43.5±10.4 46.6±10.8 *0.001 assessment
Mental state 42.0±9.8 39.9±10.1 0.63 assessment
MRC: Medical Research Council; SD: standard deviation; *: p<0.05
Table 5. The distribution and comparison of dyspnea score and the Quality of Life Questionnaire scores within and between the ACBT and Flutter® groups
ACBT (n:17) Flutter® (n:19)
After physiotherapy Mean±SD p1 After physiotherapy Mean±SD p1 p2
Dyspnea Score
MRC Score 1.1 ±1.1 *0.021 1.1±1.1 *0.006 0.97-
Borg Score 1.8±1.8 0.11 2.1±1.5 *0.012 0.39-
SF-36 QoL Questionnaire
General health 35.6±27.9 0.22 40.0±21.6 0.09 *0.048
Physical functioning 72.9±22.9 0.21 76.1±24.0 0.07 0.87
Physical role 76.5±25.8 0.16 75.0±43.3 0.12 0.81
Emotional role 47.1±26.5 0.64 56.7±17.9 *0.048 0.07
Social functioning 57.4±21.7 0.12 58.5±17.2 0.72 0.51
Pain 69.9±25.4 0.51 86.7±17.8 *0.005 *0.011
Vitality 42.4±21.9 0.28 48.7±16.4 0.95 0.13
Mental health 61.4±22.4 0.67 66.3±15.5 0.90 0.30
SF-36 Outcome Score
Physical state assessment 45.5±10.7 0.08 47.5±11.1 *0.005 0.28
Mental state assessment 38.4±11.2 0.26 39.9±8.3 0.43 0.16
ACBT: active cycle of breathing technique; SD: standard deviation; MRC: medical research council; SF: short form; p1: within group comparisons before and after physiotherapy in the ACBT and Flutter groups; p2: between-group comparisons for the change in scores after physiotherapy as compared to baseline *:p<0.05
Üzmezoğlu et al. The Efficacy of Physiotherapy in Bronchiectasis
107

studies found an increased sputum production as well as a positive effect on the airway clearance with the use of a single method or combined modalities [2,12-15]. Similarly, we also observed increased sputum production in our patient group. Recent studies have particularly focused on the comparative efficacy of ACBT and Flutter® in patients with cystic fibrosis (CF) or bronchiectasis. In one of these studies, no difference in the amount of daily sputum production could be detected, and no clear-cut data were provided concerning whether the intervention was carried out at home or at the hospital set-tings [3]. Similar to our study, ACBT and an oscillation device were compared in a study that lasted 3 days, and the device was found to be as effective as ACBT in terms of sputum pro-duction [16]. In another hospital-based study, the Flutter® device was reported to be superior for postural drainage with respect to the amount of sputum produced [17].
Since our study involved a relatively longer duration com-pared to previous studies i.e., 4 weeks, and the study design included a home-based therapy program, an objective as-sessment of the sputum volume could not be performed as opposed to other studies. This represents one potential limita-tion of our study. On the contrary, the intervention was per-formed in home settings in our study. Our findings not only are supportive of the efficacy of respiratory physiotherapy in bronchiectasis of non-CF origin but also have shown that the Flutter® device was as equally effective as ACBT. Further-more, the results support the notion that this approach may be as effective as a hospital-based intervention and feasible home settings. Studies examining the perception of dyspnea in patients with bronchiectasis are scarce in number. Dys-pnea occurring early in the course of the disease results in avoidance of physical activity because patients feel gradually more discouraged to be physically active with the presence of dyspnea. Thus, dyspnea represents an important symptom [18]. In one study, pulmonary rehabilitation was found to improve dyspneic symptoms in patients with chronic pul-monary disease [19]. In different studies utilizing the ACBT, ACBT-Postural Drainage (PD), and oscillation devices, no ef-fect of physiotherapy on dyspnea was observed [14,16]. In contrast, both techniques were associated with improved scores of both the MRC and Borg dyspnea scale of the pa-tients in our study. The improvement in dyspnea by the Flut-ter® device was detected not only during exercise but also at rest, suggesting that this technique is more efficacious. Since the clinical course of bronchiectasis may display significant variability, prediction of respiratory function abnormalities is not possible. Patients with airway obstruction comprise the majority of cases [20]. Also, the effect of physiotherapy on PFT is a matter of controversy. In studies utilizing oscillation devices and ACBT techniques, no change in PFTs have been reported [3,14,21], similar to our observations. This may be explained on the basis of the irreversible damage and bron-chial dilatation despite the achievement of effective airway clearance in bronchiectasis.
A reduced frequency of exacerbations by physiotherapy has previously been reported [22]. A smaller number of patients with exacerbations in the Flutter® group as compared to the ACBT group in our study suggest that colonization may be reduced via removal of secretions, leading to a decrease in
the risk of infective exacerbation episodes. However, because our study did not primarily target to assess the efficacy of physiotherapy on exacerbation frequency, further and longer-term studies would be warranted to reach more definite con-clusions on this subject. Studies examining the perception of dyspnea in patients with bronchiectasis are scarce in number. However, dyspnea occurring early in the course of the dis-ease results in the avoidance of physical activity because pa-tients gradually feel more discouraged to be physically active when affected by dyspnea. Thus, dyspnea represents an im-portant symptom [18]. In one study, pulmonary rehabilitation was found to improve dyspneic symptoms in patients with chronic pulmonary disease [19]. In different studies utilizing ACBT, ACBT-PD, and oscillation devices, no effect of physio-therapy on dyspnea was observed [14,16]. In contrast, both techniques were associated with improved MRC and Borg dyspnea scale scores of the study patients.
Bronchiectasis is associated with significant reductions in the quality of life as a result of the natural course of the disease leading to cough and production of purulent sputum, which may cause severe restrictions on social life. Studies examin-ing the effect of physiotherapy on the quality of life in pa-tients with bronchiectasis are very scarce in number, and only one study, which assessed the effect of the Flutter® and ACBT on the quality of life, is reported in the literature [3].
Previous studies examined the effect of the sputum volume and exercise capacity on the quality of life and found as-sociations between these factors. In our study, the effect of the quality of life on the exercise capacity was not evalu-ated, again representing a potential limitation for our study. Parameters such as dyspnea, exercise capacity, and sputum production may well be affected by increases or decreases in the quality of life in patients with bronchiectasis. Although physiotherapy was effective in improving the quality of life, the Flutter® device had even a more significant positive ef-fect on this parameter. This latter finding may be associated with the number of factors such as the ease of use, patient comfort, and better adherence to the therapy.
The limitations of our study are as follows: the patient num-ber was low; the amount of sputum was not measured by ob-jective methods; the following parameters, namely patients’ exercise capacity, exercise adherence, physical activity lev-els could not be compared; and there was no control group. Nevertheless, home-based physiotherapy during a follow-up period of 1 month in bronchiectasis patients revealed suc-cessful results. None of our patients presented with absentee-ism due to physiotherapy. A reduction in coughing, ease of sputum removal, decreased dyspnea perception, and perhaps an increase in the quality of life associated with the former are important results of our study in terms of demonstrating and supporting the success of physiotherapy.
Our results have demonstrated that physiotherapy represents an effective contribution to the management of patients with bronchiectasis. Higher efficacy of the Flutter® device in cer-tain parameters may be associated with its easy of use and the subsequent improvements in treatment compliance. Fur-ther studies are warranted to support these findings.
Turk Thorac J 2018; 19(3): 103-9
108

Ethics Committee Approval: Ethics committee approval was received for this study from the Ethics Committee of Trakya University School of Medicine (Approval Date: 25.06.2009; Approval No: 2009/153).
Informed Consent: Written informed consent was obtained from pa-tients who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - B.U., G.A.; Design - B.U., G.A.; Su-pervision - G.A., H.T.; Resource - B.U., L.O.; Materials -B.U., L.O., G.A. ; Data Collection and/or Processing - B.U.; Analysis and/or In-terpretation - B.U., N.S.; Literature Search - B.U., L.O.; Writing -B.U. ; Critical Reviews - G.A., H.T., L.O.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: This study has been provided by the scientific research projects at the Trakya University.
REFERENCES
1. Tsang KW, Bilton D. Clinical challenges in managing bronchi-ectasis. Respirology 2009;14:637-50. [CrossRef]
2. Savcı S, İnce D. The efficacy of different chest physiotherapy applications in patients with stable bronchiectasis. Respiratory Diseases (Stabil bronsektazili hastalarda farklı göğüs fizyotera-pisi uygulamalarının etkinliği. Solunum Hastalıkları) 2001;12:118-22.
3. Thompson CS, Harrison S, Ashley J, et al. Randomised crossover study of the Flutter® device and the active cycle of breathing technique in noncystic fibrosis bronchiectasis. Thorax 2002;57:446-8. [CrossRef]
4. App E, Kieselmann R, Reinhardt D, et al. Sputum Rheology Changes in Cystic Fibrosis Lung Disease Following Two Different Types of Physiotherapy: Flutter® vs Autogenic Drainage. Chest 1998;114:171-7. [CrossRef]
5. Mcllwaine PM, Wong LT, Peacock D, et al. Long-term compara-tive trial of positive expiratory pressure versus oscillating posi-tive expiratory pressure (flutter) physiotherapy in the treatment of cystic fibrosis. J Pediatr 2001;138:845-50. [CrossRef]
6. AbdelHalim HA, AboElNaga HH, Fathy KA. Comparison between active cycles of breathing with postural drainage ver-sus conventional chest physiotherapy in subjects with bronchi-ectasis, Egyptian J Chest Dis Tuberc 2016;65:157-65. [CrossRef]
7. Pryor JA, Webber BA, Hodson ME, et al. Evaluation of the forced expiration technique as an adjunct to postural drainage in treatment of cystic fibrosis, Br Med J 1979;2:417-8. [CrossRef]
8. AbdelHalim HA. Physiotherapy for Respiratory and Cardiac Problems. Pryor JA, Prasad SA, editors. Edinburgh, 1998.
9. Bipin P, Mohamed CK, Renuka DM, et al. Efficacy of active cycle of breathing technique and postural drainage in patients with bronchiectasis-A comparative study, IJMHS 2012;2:129-32.
10. Ware JE Jr, Sherbourne CD. The MOS 36-Item Short-Form Health Survey (SF-36): I. Conceptual framework and item selec-tion. Med Care 1992;30:473-83. [CrossRef]
11. Koçyiğit H, Aydemir Ö, Fişek G, et al. Reliability and Validity of the Turkish Version of Short Form-36 (SF-36) (Form-36 (KF-36)’nın Türkçe versiyonunun güvenilirliği ve geçerliliği). Drug and Treatmant Journal 1999;12:102-6.
12. Lee A, Button BM, Denehy L. Current Australian and New Zealand physiotherapy practice in the management of patients with bronchiectasis and chronic obstructive pulmonary disease. J Physiother 2008;36:46-58.
13. Pryor JA. Physiotherapy for airway clearance in adults. Eur Respir J 1999;14:1418-24. [CrossRef]
14. Eaton T, Young P, Zeng I, et al. A randomized evaluation of the acute efficacy, acceptability and tolerability of Flutter and active cycle of breathing with and without postural drainage in non-cystic fibrosis bronchiectasis. Chron Respir Dis 2007;4:23-30. [CrossRef]
15. Lee AL, Burge AT, Holland AE. Positive expiratory pressure therapy versus other airway clearance techniques for bronchi-ectasis. Cochrane Database Syst Rev 2017;9:CD011699. [CrossRef]
16. Patterson JE, Bradley JM, Hewitt O, et al. Airway Clearance in Bronchiectasis: A Randomized Crossover Trial of Active Cycle of Breathing Techniques versus Acapella. Respiration 2005;72:239-42. [CrossRef]
17. Konstan MW, Stern RC, Doershuk CF. Efficacy of the Flutter device for airway mucus clearance in patients with cystic fibro-sis. J Pediatr 1994;124:689-93. [CrossRef]
18. O’Donnell DE. Breathlessness in patients with chronic airflow limitation. Mechanisms and management. Chest 1994;106:904-12. [CrossRef]
19. Karapolat H, Gürgün A, Eyigör S, et al. The Effect of Short-Term Pulmonary Rehabilitation on Pulmonary Function Tests, Blood Gases, Functional Capacity, Dyspnea, Quality of Life and Psychological Symptoms in Chronic Pulmonary Diseases: A Retrospective Study (Kronik Pulmoner Hastalıklarda Kısa Dönem Pulmoner Rehabilitasyonun Pulmoner Fonksiyon Testleri, Kan Gazı, Fonksiyonel Kapasite, Dispne, Yasam Kalitesi ve Psikolojik Semptomlar Üzerine Etkisi: Retrospektif Çalışma) Turk J Phys Med Rehab 2010;56:6-10.
20. Koulouris NG, Retsou S, Kosmas E, et al. Tidal expiratory flow limitation, dyspnoea and exercise capacity in patients with bilateral bronchiectasis. Eur Respir J 2003;21:743-8. [CrossRef]
21. Murray MP, Pentland JL, Hill AT. A randomised crossover trial of chest physiotherapy in non-cystic fibrosis bronchiectasis. Eur Respir J 2009;34:1086-92. [CrossRef]
22. Lee AL, Cecins N, Hill CJ, et al. The effects of pulmonary reha-bilitation in patients with non-cystic fibrosis bronchiectasis: protocol for a randomised controlled trial. BMC Pulm Med 2010;10:5. [CrossRef]
Üzmezoğlu et al. The Efficacy of Physiotherapy in Bronchiectasis
109

Turk Thorac J 2018; 19(3): 110-6
Original Article
Development of an Allergen-Exposure Avoidance Scale and Inhaler Use Scale for Patients with Asthma: A Reliability and Construct Validity Study
INTRODUCTIONAsthma is a serious health problem that influences the quality of life and leads to disability and an increase in healthcare costs [1]. According to the Global Asthma Report (2014), as many as 334 million people have asthma worldwide [2]. The treatment goal is to control asthma by correctly using inhaler devices, identifying asthma triggers, and helping patients acquire avoidance behavior toward allergen exposure [3-5]. In order to achieve a behavior change in patients with asthma, we need to understand their knowledge levels, beliefs, attitudes, and learning styles [6].
The theory of planned behavior (TPB) is one of the most commonly used models to explain human behavior [7]. TPB provides guidelines to identify how willing the individual is to change his/her behavior, attitude toward the behavior, and /her motivation level; in other words, his/her intention. According to TPB, to exhibit a target behavior, first of all, the individual should have an intention (purpose for a behavior) to perform it. Further, the intention is influenced by three factors, which are attitude toward behavior (ATB), subjective norm (SN), and perceived behavioral control (PBC) [8]. ATB is a person’s favorable or unfavorable evaluation regarding a specific behavior while performing it. SN is the perceived social pressure to engage in a behavior. PBC is defined as the individual’s belief concerning how easy or difficult the behavior is [9,10]. Studies conducted using TPB have shown that the model is effective in planning personal interventions for factors affecting their behaviors [11,12].
New measurement tools should be developed to test the models used to improve the effectiveness of educational programs for patients in the healthcare field. After a literature search, no suitable measurement tool based on TPB can be found for patients with asthma. The present study aims to develop two Likert-type scales interrogating the beliefs of patients with asthma, their attitudes and perceptions toward inhaler use, and their avoidance behavior against allergen exposure, from a
DOI: 10.5152/TurkThoracJ.2018.17074
Döndü Şanlıtürk1 , Sultan Ayaz Alkaya2 1Department of Nursing, Gaziosmanpaşa University, Faculty of Health Sciences, Tokat, Tukey2Department of Nursing, Gazi University, Faculty of Health Sciences, Ankara, Turkey
This study was presented in the 1st International 2nd National Public Health Nursing Congress, April 23-26, 2018, Ankara, Turkey.
Address for Correspondence: Döndü Şanlıtürk, Department of Nursing, Gaziosmanpaşa University Faculty of Health Sciences, Tokat, Tukey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org 110
Cite this article as: Şanlıtürk D, Ayaz Alkaya S. Development of an Allergen-Exposure Avoidance Scale and Inhaler Use Scale for Patients with Asthma: A Reliability and Construct Validity Study. Turk Thorac J 2018; 19(3): 110-6.
OBJECTIVES: The present study aimed to evaluate the reliability of the allergen-exposure avoidance scale (AEAS) and inhaler use scale (IUS) in patients with asthma.
MATERIALS AND METHODS: The present study was performed as a methodological design. The study included 130 patients with asthma. Each scale of allergen-exposure avoidance and inhaler use comprised 13 items. Cronbach’s alpha and total item correlation were performed to calculate internal consistency of the scales, and the Kaiser-Meyer-Olkin, Bartlett’s, and exploratory factor analysis tests were performed to assess construct validity.
RESULTS: The Cronbach’s alpha coefficients were 0.724 for IUS and 0.624 for AEAS. After exploratory factor analysis, the factors with eigenvalues >1.00 in the analysis (eigenvalues for IUS were 3.790, 1.793, and 1.789 and for AEAS were 2.990, 2.195, and 1.291) were considered. In the results of the analysis, three factors emerged in parallel with the theoretical structure. These three factors explained 52.087% of the total variance in IUS (29.151%, 13.790%, and 9.145%, respectively) and 53.960% of the total variance in AEAS (24.916%, 18.289%, and 10.754%, respectively).
CONCLUSION: Inhaler use scale and AEAS were determined to be reliable and construct valid scales. They can be used to measure factors affecting the behavioral intentions toward individuals with asthma.
KEYWORDS: Planned behavior theory, asthma, validity, reliability, scale
Abstract
Received: 06.09.2017 Accepted: 15.01.2018 Available Online Date: 19.06.2018

broad perspective. The scales are considered to be used in clinical practices and researches, in developing educational plans, and in evaluating education outcomes.
The present study was planned to develop the allergen-exposure avoidance scale (AEAS) and the inhaler use scale (IUS) based on TPB for patients with asthma and to examine the reliability and construct validity of the scales.
MATERIALS AND METHODS
Study Design and ParticipantsThe present study was conducted using a methodological design. The study population comprised patients treated for asthma in chest clinics from two public hospitals. To deter-mine sample size for the reliability and construct validity of questionnaires, it is accepted that factor analysis requires a minimum of 5-10 times the number of items as there are subjects [13]. With regard to this criterion, the sample size of the present study was calculated as 130, which was 10 times the number of items. Inclusion criteria of the study were as follows: diagnosed with asthma, age 18 years or older, use of an inhaler, ability to communicate, and agreement to partici-pate in the study. Exclusion criteria were as follows: diag-nosed with any neuropsychiatric diseases, any disorders that affect human respiration (such as malignancy, cor pulmona-le, and sleep apnea), and having vision or hearing loss.
Data Collection InstrumentsFormulating items for the scalesThe items were created in accordance with the relevant lit-erature [5,12,14-16] and the manual of “Constructing scales based on the theory of planned behavior” [17]. When con-structing the scales, we created a pilot scale to measure atti-tudes. The pilot scale comprised 33 items, 17 of which were favorable and 16 were unfavorable. We showed attention to formulate items that assessed general intent (1 item) and its three components, which were ATB (8 items), SN (16 items), and PBC (8 items).
Content validityWe consulted five faculty members who were specialists in their field for the scales, to assess the items in terms of intel-ligibility and linguistic suitability. The opinions of these spe-cialists were evaluated based on the Davis technique. In accordance with these opinions obtained for the content validity, two 13-item attitude scales were derived from the 33-item pilot scale.
Inhaler use scale and allergen-exposure avoidance scale Inhaler use scale (Appendix 1) and allergen-exposure avoid-ance scale (Appendix 2) were developed within the frame of TPB for individuals with asthma, to measure the factors affecting behavioral intention. Each scale had three sub-groups, which were ATB, SN, and PBC. IUS comprised 13 items and AEAS comprised 12. Each item was rated on a 5-point Likert-type scale (strongly agree: 5, agree: 4, unde-cided: 3, disagree: 2, and strongly disagree: 1).
Of the 13 items included in IUS, the first item represented the general intent; items 3, 7, and 9 represented ATB; items 2, 4, 6, 8, 11, and 13 represented SN; and items 5, 10, and 12
represented PBC. Of the 12 items included in AEAS, the first item represented the general intent; items 3 and 8 repre-sented ATB; items 2, 4, 6, 7, 10, and 12 represented SN; and items 5, 9, and 11 represented PBC.
To obtain the scores for each scale, the subgroup scores were separately calculated by deriving the arithmetic mean of their related items. The subgroup scores were the sum of item scores for each subgroup divided by the number of items in the subgroup. Only item 7 in the ATB subgroup of IUS was negatively keyed and reverse-scored.
The score of item 1 that measured the general intent indi-cated behavioral intention. The minimum and maximum scores for each subgroup were 1 and 5, respectively. When the scales were evaluated, the item scores rated by the patients were calculated as explained above, and a decision was then taken on the effect level of the factors influencing the patients’ intent toward behavior. Accordingly, it was inferred that the higher the score on ATB, the more favorable the patient perceived the behavior; the higher the score on SN, the more environmental pressure the patient experienced to perform the target behavior; the higher the score on PBC, the more powerful the patient’s control was to perform the behavior; the higher the score on the general intent, the more willing the patient was to perform the behavior.
Data CollectionData were collected between June 13 and December 2, 2016. While filling in the data collection forms, the researcher read the statements in the scale to the patients and asked them to what extent they agreed or disagreed with the statement. It took approximately 10-15 minutes to fill in each scale.
Ethical ConsiderationEthics committee approval and institutional permission were obtained from the Ethic Committee of Gazi University to con-duct the study. After explaining the aim of the study and read-ing the informed consent to the patients who agreed to par-ticipate the study, we obtained their written and oral consents.
Statistical AnalysisData were analyzed using IBM Statistical Package for Social Science version 20.0 (IBM Corp.; Armonk, NY, USA) statisti-cal software program. Cronbach’s alpha and total item cor-relation were performed to calculate the internal consistency of the scales, and the Kaiser-Meyer-Olkin (KMO), Bartlett’s, and exploratory factor analysis (Principal Component Analysis) tests were performed to assess construct validity.
RESULTSThe mean patient age was 49.81±13.83 years. It was deter-mined that 46.9% of the patients were in the age range of 50-64 years; 52.3% were women, 36.2% were housewives, and 22.3% were farmers (Table 1).
Reliability of IUS and AEASInternal consistency analysisIn the present study conducted in patients with asthma (n=130), internal consistency of the scales was measured using Cronbach’s alpha coefficient. Cronbach’s alpha coef-ficients were 0.724 for IUS and 0.624 for AEAS.
Şanlıtürk and Ayaz Alkaya. Allergen-Exposure Avoidance Scale and Inhaler Use Scales’ Reliability and Construct Validity
111

Item total correlationIn the present study, when an item was removed from the scales, Cronbach’s alpha was recalculated, and the contribu-tion of the Cronbach’s alpha coefficients to the scale was revealed (Table 2,3). No item was excluded from IUS, because there was no item with an item total correlation <0.25 and negatively keyed [18]. However, 4 items (7, 9, 11, and 13) were found to have an item total correlation <0.25 in AEAS. We first excluded item 7, because of an increase in the Cronbach’s alpha value. Items 9, 11, and 13 were not excluded, because their exclusion did not affect much the Cronbach’s alpha value. After excluding item 7, the Cronbach’s alpha coefficient of AEAS was 0.659.
Validity of IUS and AEAS
Construct validity (factor analysis)The KMO values, which indicate whether the sample size is adequate for factor analysis, were 0.763 for IUS and 0.679 for AEAS. In addition, the Bartlett’s test value, which shows whether there is enough correlation among the study vari-ables to perform a factor analysis, was significant (p<0.001). As the required conditions were fulfilled to perform factor analysis, the results of the analysis were interpreted (Table 4).
We used exploratory factor analysis (principal component analysis) as the analysis method and considered the factors with eigenvalues >1.00 in the analysis (eigenvalues for IUS were 3.790, 1.793, and 1.789 and for AEAS were 2.990, 2.195, and 1.291).
In the results of the analysis, three factors emerged in parallel with the theoretical structure. These three factors explained 52.087% of the total variance in IUS (29.151%, 13.790%, and 9.145%, respectively) and 53.960% of the total variance in AEAS (24.916%, 18.289%, and 10.754%, respectively). When the contributions of the factors to the variance were
Table 1. Patient characteristics
Variable n %
Age (years)
18-39 32 24.6
40-49 21 16.2
50-64 61 46.9
65 and over 16 12.3
Gender
Female 68 52.3
Male 62 47.7
Employment status
Housewife 47 36.2
Farmer 29 22.3
Worker 26 20.0
Officer 13 10.0
Pensioner 12 9.2
Student 32 24.6
Table 2. IUS item total correlation and internal consistency analysis
Item total Cronbach’s alpha Item number correlation if item deleted
1 0.457 0.697
2 0.286 0.716
3 0.411 0.712
4 0.272 0.717
5 0.513 0.682
6 0.472 0.708
7 0.328 0.709
8 0.379 0.713
9 0.367 0.684
10 0.510 0.719
11 0.246 0.681
12 0.523 0.719
13 0.290 0.739
IUS: inhaler use scale
Table 3. AEAS item total correlation and internal consistency analysis
Item total Cronbach’s alpha Item number correlation if item deleted
1 0.366 0.586
2 0.311 0.609
3 0.343 0.607
4 0.240 0.609
5 0.419 0.570
6 0.275 0.609
7 -0.159 0.659
8 0.255 0.608
9 0.205 0.614
10 0.453 0.561
11 0.132 0.622
12 0.497 0.544
13 0.247 0.615
AEAS: allergen-exposure avoidance scale
Table 4. Kaiser-Meyer-Olkin and Bartlett’s test results
IUS AEAS
KMO
Measure of sampling 0.763 0.679 Adequacy
Bartlett’s test of Approximately 434.337 372.455 sphericity Chi-square
df 78 66
Significance <0.001 <0.001
KMO: Kaiser-Meyer-Olkin; IUS: inhaler use scale; AEAS: allergen-exposure avoidance scale
Turk Thorac J 2018; 19(3): 110-6
112

separately looked at, it was observed that the contribution decreased, and that the difference was too close as from fac-tor 3. Thus, it was revealed that there were three factors in parallel with the theoretical structure. The three factors that were revealed by performing factor rotation overlapped with the subgroups or were interrelated factors. Tables 5, 6 show the evaluation of statements, which were constructed in accordance with the model in the general intent item and in three subgroups, which constituted the intent, according to the subgroups, which were formed with the factor analysis.
Items 5, 10, and 12 representing PBC in IUS and AEAS were found in factor 2. Among the items representing SN in IUS, items 2, 4, and 6 were found in factor 3, and items 8, 11, and 13 were in factor 1. Among the items representing SN in AEAS, items 2, 4, 6, and 8 were found in factor 1, and items 11 and 13 were found in factor 3. Among the items repre-
senting ATB in IUS, item 3 was found in factor 3, item 7 was found in factor 2, and item 9 was found in factor 1. Among the items representing ATB in AEAS, item 3 was found in fac-tor 1 and item 9 was found in factor 3. Item 1 indicating the general intent was found in factor 1 for IUS and in factor 2 for AEAS.
DISCUSSIONAsthma is one of the commenest adulthood disease and is mostly affected by occupational conditions [18,19].
For patients with asthma to be able to change their behaviors, it is first necessary to intend to change the behavior. Intent shows the individual’s level of motivation toward achieving the target behavior. The stronger the individual’s intention to achieve the target behavior, the higher is the performance. It is not enough that only the intention exists for the target behavior to be exhibited. To perform the behavior depends on the individual’s attitude toward the behavior, the provi-sion of effective factors (such as money, time, skill, and social support), and PBC. In the present study, two scales were developed to identify the attitudes of patients with asthma toward inhaler use and allergen-exposure avoidance behav-iors.
According to the reliability analysis of IUS and AEAS, the Cronbach’s alpha values were 0.724 and 0.624, respectively. Literature states that Cronbach’s alpha coefficient ranges between 0 and 1, and when it is between 0.60 and 0.79 for a scale, the scale is considered as relatively reliable [20]. Hence, IUS and AEAS developed in the present study are relatively reliable. This result indicates that the items in each scale and data collected are reliable. In other words, as the homogeneity of the scale items is at an acceptable level, data collected with each scale will be interrelated, coherent, intelligible, adequate, and will have the quality to reveal the truth of the study.
As reliability is a measure of the consistency and a propor-tion of truth, it is important for all the items constituting a scale to have an enhancing effect on reliability [21]. Reliability analysis is used to determine each item’s power in terms of measuring what is wished to be measured using an instrument (such as intent, ATB, SN, and PBC) and to make the instrument more reliable using results [20,22]. Including or excluding an item is decided according to the results of this analysis. When an item is excluded from an instrument, if the recalculated Cronbach’s alpha coefficient value is lower than the Cronbach’s alpha coefficient value for the whole instrument, the item is considered to play a role in improving reliability, and it is included in the instrument. On the other hand, if the value is higher, then the item is exclud-ed from the instrument, because it adversely affects internal consistency [20-22]. If the correlation coefficient value is not negative and is >0.25 between the item excluded and total of the other items, it indicates that contribution of the con-cerned item to the whole instrument is high, and that the item should be included in the instrument [20,22]. When examining our study results in accordance with this informa-tion, we decided to exclude one item from AEAS. We con-cluded that the 13-item IUS and the 12-item AEAS were
Table 5. IUS exploratory factor analysis results
Component
Item number Factor 1 Factor 2 Factor 3
11 0.728
13 0.635
1 0.627
8 0.622
9 0.600
12 0.859
10 0.832
5 0.678
7 0.468
6 0.725
3 0.691
4 0.689
2 0.570
IUS: inhaler use scale
Table 6. AEAS exploratory factor analysis results
Component
Item number Factor 1 Factor 2 Factor 3
8 0.746
3 0.695
4 0.645
2 0.570
6 0.507
12 0.840
10 0.828
5 0.790
1 0.399
9 0.850
13 0.763
11 0.685
AEAS: Allergen-exposure avoidance scale.
Şanlıtürk and Ayaz Alkaya. Allergen-Exposure Avoidance Scale and Inhaler Use Scales’ Reliability and Construct Validity
113

reliable scales. The reliability of the scales developed in the present study is important in terms of determining the patient’s attitudes and beliefs to treatment and disease man-agement. It is believed that the scales will contribute to determining the positive or negative attitudes of patients with asthma toward inhaler use and avoidance of allergen expo-sure. Family plays a pivotal role in maintaining disease man-agement in asthma. In the present study, the social environ-ment (parents, siblings, spouses, and friends) on the scales developed is evaluated for the effect of the patient on exhib-iting the target behaviors. In the studies, it was found that there is a strong relationship between use of medication and advice of family and friends of patients with asthma, and that social support has positive effects on disease control and quality of life [23,24].
The KMO and Bartlett’s tests are used to evaluate the ade-quateness of sample size for factor analysis. In the present study, as the KMO and Bartlett’s test values were found to be >0.60, which is the lower limit, the sample size was consid-ered to be adequate for factor analysis. Thus, the factor analysis was performed to identify subgroups. Factor loads were examined to see which items loaded onto which fac-tors. According to literature, factor loads should be >0.30 [20-22]. In the present study, three factors were constructed in parallel with the theoretical structure at the end of the fac-tor rotation. It was revealed that these three factors over-lapped with the subgroups or were interrelated. Among the subgroups, which were intent and components of the intent (ATB, SN, and PBC), only PBC was found to load onto the same factor. The other subgroups loaded onto different fac-tors. It is considered that this situation results from the inter-related/interacting feature of the items in the subgroups owing to the general structure of the theory. The more the patients with asthma believe in the benefits of target behav-iors, the more they will increase their control over it. It is believed that determining the attitudes of the use of proper inhaler and avoidance of allergen exposure that cause attacks will lead to better results in disease control and treat-ment compliance in patients with asthma.
The attitudes of patients with asthma to disease and treat-ment are influencing treatment compliance. Patients with asthma think that they are cured when there are no symp-toms and cease treatment. Side effects of drugs and worry about addiction are the factors that reduce treatment compli-ance in patients with asthma [25]. For this reason, the atti-tudes of the patients need to be evaluated to increase treat-ment compliance.
Strength and limitationThis scale is the first reliable and construct valid instrument based on TPB for individuals with asthma. The limitation of this study is that the consistencies of IUS and AEAS over time have not been measured using the test-retest method and that the same test has not been administered to the same sample on different occasions. Further, we have not tested the cross-sectional construct, convergent, and discriminant validities and the screening accuracy and responsiveness of the ques-tionnaires.
To conclude, IUS and AEAS developed based on TPB are reliable and construct valid instruments to determine factors influencing behavioral intention of individuals with asthma. Depending on the study results, to assess the reliability of IUS and AEAS over time, it is recommended to conduct a test-retest study on the same group and to conduct validity studies in different patient groups.
Ethics Committee Approval: Ethics committee approval was received for this study from Gazi University Ethical Committee (Approval Date: 03.06.2016; Approval Number: 77082166-604.01.02)
Informed Consent: Written informed consent was obtained from the patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - D.Ş., S.A.A.; Design - D.Ş., S.A.A.; Supervision - S.A.A.; Resource - D.Ş.; Materials - D.Ş., S.A.A.; Data Collection and/or Processing - D.Ş.; Analysis and/or Interpretation - D.Ş., S.A.A.; Literature Search - D.Ş.; Writing - D.Ş., S.A.A.; Critical Reviews - D.Ş., S.A.A.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES1. To T, Stanojevic S, Moores G, et al. Global asthma prevalence
in adults: Findings from the cross-sectional world health survey. BMC Public Health 2012;12:2-8. [CrossRef]
2. The Global Asthma Report. 2014. Available from: http://www.globalasthmareport.org/about.php.
3. İbrahim M, Verma R, Garcia-Contreras L. Inhalation drug de-livery devices: Technology update. Medical Devices (Auckl) 2015;8:131-9.
4. Toumas-Shehata M, Price D, Basheti IA, Bosnic-Anticevich S. Exploring the role of quantitative feedback in inhaler tech-nique education: a cluster-randomised, two-arm, parallel-group, repeated-measures study. NPJ Prim Care Respir Med 2014;24:14071. [CrossRef]
5. Valizadeh L, Zarei S, Zamanazadeh V, et al. The effects of trig-gers’ modifying on adolescent self-efficacy with asthma: A ran-domized controlled clinical trial. J Caring Sci 2014;3:121-9.
6. Damon SA, Tardif RR. Asthma education: different viewpoints elicited by qualitative and quantitative methods. J Asthma 2015;52:314-7. [CrossRef]
7. Karayağız GM, Başbakkal Z. The planned behavior theory and breastfeeding behavior (Planlı davranış teorisi ve emzirme davranışı). Turk Clin J Nurs Sci 2013;5:28-40.
8. Bassett-Gunter RL, Levy-Milne R, Naylor PJ, et al. A compari-son of theory of planned behavior beliefs and healthy eating between couples without children and first-time parents. J Nutr Educ Behav 2015;47:216-24. [CrossRef]
9. Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes 1991; 50:179-211. [CrossRef]
10. Lapkin S, Levett-Jones T, Gilligan C. Using the theory of planned behavior to examine health professional students’ behavioural intentions in relation to medication safety and collaborative practice. Nurse Educ Today 2015;35:935-40. [CrossRef]
11. Pooreh S, Hosseini-Nodeh Z. Impact of education based on theory of planned behavior: An Investigation into hypertension-preventive self-care behaviors in Iranian girl adolescent. Iran J Public Health 2015;44:839-47.
Turk Thorac J 2018; 19(3): 110-6
114

12. Rashidian A, Russell I. General practitioners’ ıntentions and prescribing for asthma: Using the theory of planned behavior to explain guideline implementation. Int J Prev Med 2012;3:17-28.
13. Coşkun S, Bebiş H. Psychometric evaluation of a Turkish version of the e-health literacy scale (e-heals) in adolescent. Gulhane Med J 2015;57:378-84. [CrossRef]
14. Global Initiative for Astma (GINA). Global strategy for asthma management and prevention. Updated 2010, Chapter 1. Defini-tion and overview 2012;1-3.
15. Chiu KC, Boonsawat W, Cho SH, et al. Patients’ beliefs and behaviors related to treatment adherence in patients with asthma requiring maintenance treatment in Asia. J Asthma 2014;51:652-9. [CrossRef]
16. Dalcin Pde T, Grutcki DM, Laporte PL, et al. Factors related to the incorrect use of inhalers by asthma patients. J Bras Pneumol 2014;40:13-20. [CrossRef]
17. Ajzen I. Theory of Planned Behaviour Questionnaire. Mea-surement Instrument Database for the Social Science 2013. Retrieved from: http://www.midss.org/content/theory-planned-behaviour-questionnaire.
18. Bozkus F and Samur AA. The evaluation of asthmatic patients working in a textile factory. Duzce Medical Journal. 2014;16:41-4.
19. Hansen S, Probst-Hensch N, Keidel D, et al. Gender differences in adult-onset asthma: results from the Swiss SAPALDIA cohort study. Eur Respir J. 2015;46:1011-20. [CrossRef]
20. Alpar R. Applied statistics and examples with validity-reliabil-ity from sports, health and education sciences (Spor, sağlık ve eğitim bilimlerinden örneklerle uygulamalı istatistik ve geçerli-lik güvenirlik). 3rd ed. Ankara: Detay Yayıncılık 2014; 434-85.
21. Koçak C, Albayrak SA, Büyükkayacı Duman N. Developing an attitude scale for nurses in caregiving roles: Validity and reli-ability tests. Hemşirelikte Eğitim Araştırma Dergisi 2014; 11: 16
22. Güriş S, Astar M. SPSS ile istatistik (Statistics with SPSS). 2nd ed. İstanbul: Der Yayınları 2015; 415-7.
23. Rhee H, Belyea MJ, Brasch J. Family support and asthma out-comes in adolescents: Barriers to adherence as a mediator. J Adolesc Health 2010;47:472-8. [CrossRef]
24. Foster JM, Smith L, Bosnic-Anticevich SZ, et al. Identifying patient-specific beliefs and behaviours for conversations about adherence in asthma. Intern Med J 2012;42:136-44. [CrossRef]
25. Horne R, Price D, Cleland J, et al. Can asthma control be im-proved by understanding the patient’s perspective? BMC Pulm Med 2007;7:8. [CrossRef]
Şanlıtürk and Ayaz Alkaya. Allergen-Exposure Avoidance Scale and Inhaler Use Scales’ Reliability and Construct Validity
115
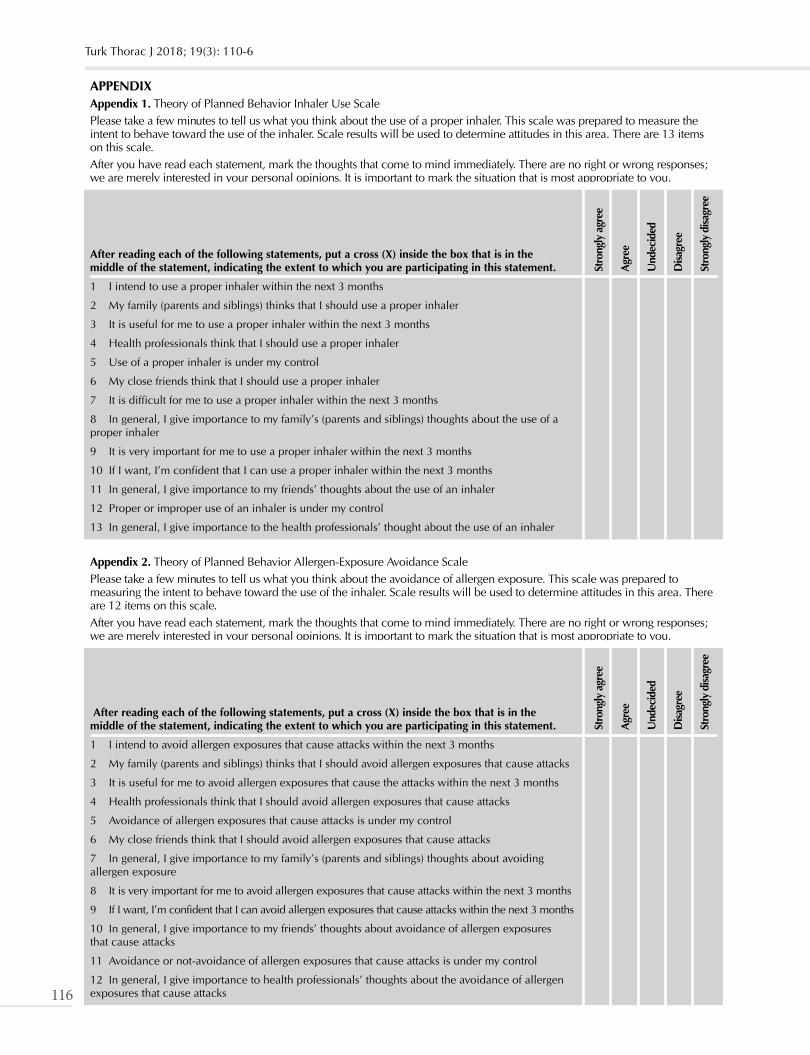
APPENDIXAppendix 1. Theory of Planned Behavior Inhaler Use ScalePlease take a few minutes to tell us what you think about the use of a proper inhaler. This scale was prepared to measure the intent to behave toward the use of the inhaler. Scale results will be used to determine attitudes in this area. There are 13 items on this scale.After you have read each statement, mark the thoughts that come to mind immediately. There are no right or wrong responses; we are merely interested in your personal opinions. It is important to mark the situation that is most appropriate to you.
After reading each of the following statements, put a cross (X) inside the box that is in the middle of the statement, indicating the extent to which you are participating in this statement.
1 I intend to use a proper inhaler within the next 3 months
2 My family (parents and siblings) thinks that I should use a proper inhaler
3 It is useful for me to use a proper inhaler within the next 3 months
4 Health professionals think that I should use a proper inhaler
5 Use of a proper inhaler is under my control
6 My close friends think that I should use a proper inhaler
7 It is difficult for me to use a proper inhaler within the next 3 months
8 In general, I give importance to my family’s (parents and siblings) thoughts about the use of a proper inhaler
9 It is very important for me to use a proper inhaler within the next 3 months
10 If I want, I’m confident that I can use a proper inhaler within the next 3 months
11 In general, I give importance to my friends’ thoughts about the use of an inhaler
12 Proper or improper use of an inhaler is under my control
13 In general, I give importance to the health professionals’ thought about the use of an inhaler
Stro
ngly
agr
ee
Agr
ee
Und
ecid
ed
Disa
gree
Stro
ngly
disa
gree
Appendix 2. Theory of Planned Behavior Allergen-Exposure Avoidance ScalePlease take a few minutes to tell us what you think about the avoidance of allergen exposure. This scale was prepared to measuring the intent to behave toward the use of the inhaler. Scale results will be used to determine attitudes in this area. There are 12 items on this scale.After you have read each statement, mark the thoughts that come to mind immediately. There are no right or wrong responses; we are merely interested in your personal opinions. It is important to mark the situation that is most appropriate to you.
After reading each of the following statements, put a cross (X) inside the box that is in the middle of the statement, indicating the extent to which you are participating in this statement.
1 I intend to avoid allergen exposures that cause attacks within the next 3 months
2 My family (parents and siblings) thinks that I should avoid allergen exposures that cause attacks
3 It is useful for me to avoid allergen exposures that cause the attacks within the next 3 months
4 Health professionals think that I should avoid allergen exposures that cause attacks
5 Avoidance of allergen exposures that cause attacks is under my control
6 My close friends think that I should avoid allergen exposures that cause attacks
7 In general, I give importance to my family’s (parents and siblings) thoughts about avoiding allergen exposure
8 It is very important for me to avoid allergen exposures that cause attacks within the next 3 months
9 If I want, I’m confident that I can avoid allergen exposures that cause attacks within the next 3 months
10 In general, I give importance to my friends’ thoughts about avoidance of allergen exposures that cause attacks
11 Avoidance or not-avoidance of allergen exposures that cause attacks is under my control
12 In general, I give importance to health professionals’ thoughts about the avoidance of allergen exposures that cause attacks
Stro
ngly
agr
ee
Agr
ee
Und
ecid
ed
Disa
gree
Stro
ngly
disa
gree
Turk Thorac J 2018; 19(3): 110-6
116

Turk Thorac J 2018; 19(3): 117-21
Original Article
Chest Diseases in Refugees Living in a Tent Camp and in Turkish Citizens Living in the District: Ceylanpınar Experience
INTRODUCTION
In recent years, the number of refugees has dramatically increased all over the world as a result of migration caused by wars. In fact, according to data by the United Nations, it is expected that the number of international immigrants in the world will reach 405 million by 2050, if migration continues to increase as rapidly as it has over the last 20 years [1].
The ongoing war in Syria over the last six years has caused 4 million people to emigrate. Turkey, being the neighboring na-tion, has opened its doors to immigrants owing to its geographical location and hosts the world’s largest refugee population, holding the first place among the most affected countries. Refugees who live in both in camps and in cities owing to refugee overburden have been taken under temporary protection by the Turkish Republic. In this context, health services, just as other services, are provided free of cost [2]. Despite the services offered, the fact that immigrants leave their homes, territories, and countries and settle in new places causes them to experience difficulties in adjustment [3]. However, challenging trans-portation to health institutions, poor nutrition, poor living conditions, language problems, low level of education, economic inadequacy, and lack of social security have negative effects on health [4]. Contagious diseases, vaccine preventable diseases (measles, tuberculosis, hepatitis, etc.), and psychiatric problems such as depression, anxiety disorders, burnout, sleep dis-orders, prolonged mourning, and post-traumatic stress disorder, play an important role among the health problems that are experienced by refugees [5,6]. Poor living conditions of asylum seekers cause unavailability of basic health needs. Moreover,
DOI: 10.5152/TurkThoracJ.2018.17070
Şerif Kurtuluş1 , Zafer Hasan Ali Sak2 , Remziye Can3 1Chest Diseases Clinic, Ceylanpınar State Hospital, Şanlıurfa, Turkey2Department of Chest Diseases, Harran University School of Medicine, Şanlıurfa, Turkey3Department of Nursing, Eskişehir Osmangazi University Faculty of Health Sciences, Eskişehir, Turkey
This study was presented in Turkish Thoracic Society 19th Annual Congress, April 06-10, 2016, Antalya, TurkeyAddress for Correspondence: Şerif Kurtuluş, Chest Diseases Clinic, Ceylanpınar State Hospital, Şanlıurfa, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
117
Cite this article as: Kurtuluş Ş, Sak ZHA, Can R. Chest Diseases in Refugees Living in a Tent Camp and in Turkish Citizens Living in the District: Ceylanpınar Experience. Turk Thorac J 2018; 19(3): 117-21.
OBJECTIVES: Displacement, for whatever reason, is an urgent situation that affects both the migrant and the migratory society in a holis-tic manner, and that especially hurts Middle Eastern societies. Studies show that health problems experienced as a result of immigration are important in terms of cost reduction and quality of life. This study aimed to investigate chest diseases (CD) among refugees living in a tent camp and Turkish citizens living in the district Şanlıurfa Ceylanpınar which is located in the South East of the Turkey.
MATERIALS AND METHODS: A retrospective registry-scan type study was performed between January 2015 and December 2015. The extent of this study is the citizens of Turkish Republic and refugees who applied to Şanlıurfa Ceylanpınar State Hospital CD Policlinic and Annex Building CD Policlinic and Emergency Polyclinic. The study has been divided into two groups as Refugees and Turkish citizens, the data of patients who were referred to the Chest Diseases Policlinic and Emergency Polyclinic for chest complaints were recorded. The diagnoses of chest diseases in both groups were compared. Patients who presented with a chest complaint but did not have any diagnosis were sent for further psychiatric evaluation with regard to anxiety. Tuberculosis, which is an important public health problem, was also studied in detail.
RESULTS: In total; 455,882patients were admitted to the Şanlıurfa Ceylanpınar State Hospital center and Annex Building Chest Diseases Policlinic and Emergency Polyclinic with chest complaints. Pneumonia, asthma, and chronic obstructive pulmonary disease were found to occur more frequently in refugees from the tent camp than in Turkish citizens. Anxiety was higher among Turkish Citizens in patients who had a chest complaint but did not receive any diagnosis.
CONCLUSION: Refugees living in tent camps and Turkish citizens living in the same area were found to have similar results in terms of respiratory diseases, including tuberculosis. Physiological and psychological effects of war were expected to be high in refugees be-cause they were affected by immigration; however, they were no different than the physiological and psychological effects noted in local people. These data suggest that the local people as well as current immigrants may be psychologically affected.
KEYWORDS: Migration, Syrian refugees, diagnosis rates, anxiety, tuberculosis
Abstract
Received: 30.08.2017 Accepted: 02.01.2018 Available Online Date: 12.06.2018

the threat of epidemic diseases increases, which poses a threat to the health of the local people. In addition, emerging health problems create a great pressure on the sector, and this causes the needs, demands, and costs to increase, and consequently, the number of personnel and institutions become insufficient [7]. For example, it was found that Syrian refugees resulted in an additional cost of 10% to the health sector in Jordan, and these services, which were provided free of cost, also in-creased workload in the healthcare sector and decreased the quality of services [8]. In Turkey, it is known that 953,466 op-erations were performed within the scope of the treatment of Syrian and Iraqi asylum seekers until the end of May 2017, and 1,143,393 inpatient services and 25,919,750 ambulatory care services were provided to them [9].
The aim of this study was to compare refugees living in tent camps and Turkish citizens living in the city, in terms of chest diseases.
MATERIALS AND METHODS
Ceylanpınar is a district in Şanlıurfa on Syrian border. The population of the town, which is 140 km away from the City Center, was 84,727 in the year 2015 [10]. The tent camp is 13 km away from Ceylanpınar. Refugees living in tent camps generally come from the Syrian cities of Idlip, Aleppo, and Haseke in general. There are fewer refugees from other parts of Syria and from countries such as Iraq and Palestine [2].
The Şanlıurfa Ceylanpınar State Hospital where the study was planned comprises two units viz., the Central Building and the Annex Building. The Central Building is located in dis-trict, and the Annex Building is located in the tent camp area. Health services at both the units are provided by the staff of Şanlıurfa Ceylanpınar State Hospital.
This is a retrospective registry-scan study executed between January1, 2015, and December 31, 2015, including Turk-ish citizens who applied to the Central Building of Şanlıurfa Ceylanpınar State Hospital Chest Diseases and Emergency Polyclinic with chest complaints and refugees who applied to the Department of Chest Diseases and Emergency Polyclinic of the Annex Building with chest complaints.
In the scope of the study, the diagnoses of the patients with chest complaints, who applied to both the Department of Chest Diseases and the emergency polyclinic, were recorded by querying the Hospital Information Management System. The diagnoses for chest diseases of both the groups were compared. The patients who applied with a chest complaint but did not receive any diagnosis, were consultated by the psychiatric in terms of anxiety. Tuberculosis, an important public health problem, was studied in detail.
The required approval was received from the Ethics Com-mittee fornon-interventional research at Harran University School of Medicine.
RESULTS
In total, 455,882 patients applied to the Department of Chest Diseases and Emergency Polyclinic in the Central Building and Annex Building of Şanlıurfa Ceylanpınar State Hospital (Table 1).
In total, 19,682 Turkish citizens applied to the Central Build-ing Chest Diseases Polyclinic. Chest pain (16%) was the most common chest symptom among Turkish citizens who applied to the Central Building Chest Diseases Polyclinic. The five most common diagnoses were asthma (13.5%), chronic ob-structive pulmonary disease (COPD) (9%), acute bronchitis (9%), pneumonia (6.7%), and seasonal allergic rhinitis (4%).
In total, 245,166 Turkish citizens applied to the Central Build-ing Emergency Polyclinic. The most common chest symptom among Turkish citizens who applied to the Central Building Emergency Polyclinic was chest pain with a rate of 1.5%, and the most common three diagnoses were acute upper re-spiratory tract infections (30.9%), myalgia (2.5%), and acute bronchitis (1.4%) (Table 1).
In total, 2,374Syrian refugees applied to the Annex Building Chest Diseases Polyclinic. Chest pain was the most common chest symptom with a rate of 11.5% among Syrian refugees who applied to the Annex Building Chest Diseases Polyclin-ic. The five most common diagnoses were asthma (18.7%), pneumonia (14.5%), COPD (10.6%), acute bronchitis (6.9%), and seasonal allergic rhinitis (2.4%).
In total, 188,660 refugees applied to the Annex Building Emergency Polyclinic. Chest pain (0.4%) was the most fre-quent chest symptom among refugees who applied to the An-nex Building Emergency Service polyclinic. The three most common diagnoses were acute upper respiratory tract infec-tions (28.7%), myalgia (6.3%), and acute bronchitis (2.6%) (Table 1).
The number of patients who applied to the Chest Diseases and Emergency Polyclinic with chest complaints in both units, but did not receive any diagnosis and whose anxiety was confirmed by the Psychiatric Department, was 1,958 (Table 2).
While the rate of anxiety was 1.6% for Turkish citizens that applied to the Central Building Chest Diseases Polyclinic, it was 0.49% for those that applied to the Central Building Emergency Polyclinic (Table 2).
While the rate of anxiety was 1.5% for refugees that ap-plied to the Annex Building Chest Diseases Polyclinic, it was 0.20% for those that applied to the Annex Building Emer-gency Polyclinic (Table 2).
Regarding tuberculosis, which is an important public health problem, three refugees living in a tent camp were diagnosed with Sputum ARB (+) pulmonary tuberculosis. Five of the Turkish citizens were diagnosed with pulmonary tuberculosis and five with non-pulmonary tuberculosis (Table 1). Two of the five were ARB (+) and the remaining were ARB (-). Two ARB (-) cases were disgnosed with tuberculosis via culture test and one via clinical-radiological method. Pulmoner tu-berculosis patients were isolated during the infection period, and those who had come in contact with the people who are exposed to infection of the patients who has pulmonary tuberculosis were screened through clinical and radiological evaluation and a PPD test. Throughout 2015, the PPD test was performed in a total of 318 people.
Turk Thorac J 2018; 19(3): 117-21
118
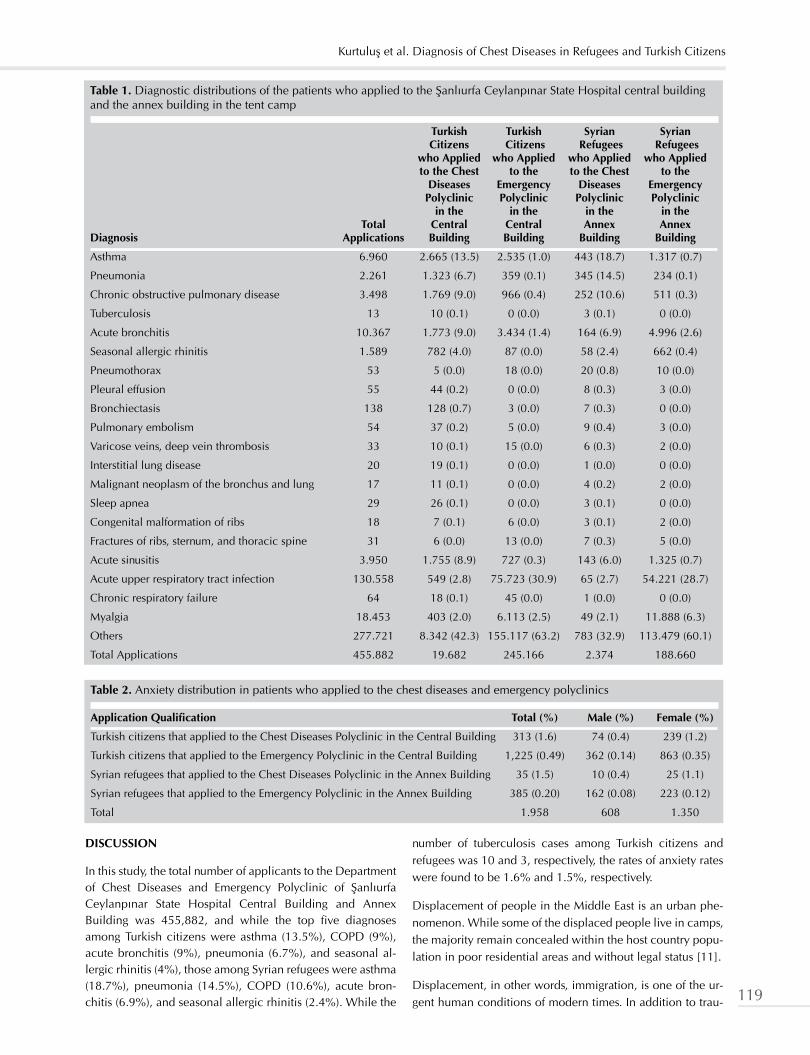
DISCUSSION
In this study, the total number of applicants to the Department of Chest Diseases and Emergency Polyclinic of Şanlıurfa Ceylanpınar State Hospital Central Building and Annex Building was 455,882, and while the top five diagnoses among Turkish citizens were asthma (13.5%), COPD (9%), acute bronchitis (9%), pneumonia (6.7%), and seasonal al-lergic rhinitis (4%), those among Syrian refugees were asthma (18.7%), pneumonia (14.5%), COPD (10.6%), acute bron-chitis (6.9%), and seasonal allergic rhinitis (2.4%). While the
number of tuberculosis cases among Turkish citizens and refugees was 10 and 3, respectively, the rates of anxiety rates were found to be 1.6% and 1.5%, respectively.
Displacement of people in the Middle East is an urban phe-nomenon. While some of the displaced people live in camps, the majority remain concealed within the host country popu-lation in poor residential areas and without legal status [11].
Displacement, in other words, immigration, is one of the ur-gent human conditions of modern times. In addition to trau-
Table 1. Diagnostic distributions of the patients who applied to the Şanlıurfa Ceylanpınar State Hospital central building and the annex building in the tent camp
Turkish Turkish Syrian Syrian Citizens Citizens Refugees Refugees who Applied who Applied who Applied who Applied to the Chest to the to the Chest to the Diseases Emergency Diseases Emergency Polyclinic Polyclinic Polyclinic Polyclinic in the in the in the in the Total Central Central Annex Annex Diagnosis Applications Building Building Building Building
Asthma 6.960 2.665 (13.5) 2.535 (1.0) 443 (18.7) 1.317 (0.7)
Pneumonia 2.261 1.323 (6.7) 359 (0.1) 345 (14.5) 234 (0.1)
Chronic obstructive pulmonary disease 3.498 1.769 (9.0) 966 (0.4) 252 (10.6) 511 (0.3)
Tuberculosis 13 10 (0.1) 0 (0.0) 3 (0.1) 0 (0.0)
Acute bronchitis 10.367 1.773 (9.0) 3.434 (1.4) 164 (6.9) 4.996 (2.6)
Seasonal allergic rhinitis 1.589 782 (4.0) 87 (0.0) 58 (2.4) 662 (0.4)
Pneumothorax 53 5 (0.0) 18 (0.0) 20 (0.8) 10 (0.0)
Pleural effusion 55 44 (0.2) 0 (0.0) 8 (0.3) 3 (0.0)
Bronchiectasis 138 128 (0.7) 3 (0.0) 7 (0.3) 0 (0.0)
Pulmonary embolism 54 37 (0.2) 5 (0.0) 9 (0.4) 3 (0.0)
Varicose veins, deep vein thrombosis 33 10 (0.1) 15 (0.0) 6 (0.3) 2 (0.0)
Interstitial lung disease 20 19 (0.1) 0 (0.0) 1 (0.0) 0 (0.0)
Malignant neoplasm of the bronchus and lung 17 11 (0.1) 0 (0.0) 4 (0.2) 2 (0.0)
Sleep apnea 29 26 (0.1) 0 (0.0) 3 (0.1) 0 (0.0)
Congenital malformation of ribs 18 7 (0.1) 6 (0.0) 3 (0.1) 2 (0.0)
Fractures of ribs, sternum, and thoracic spine 31 6 (0.0) 13 (0.0) 7 (0.3) 5 (0.0)
Acute sinusitis 3.950 1.755 (8.9) 727 (0.3) 143 (6.0) 1.325 (0.7)
Acute upper respiratory tract infection 130.558 549 (2.8) 75.723 (30.9) 65 (2.7) 54.221 (28.7)
Chronic respiratory failure 64 18 (0.1) 45 (0.0) 1 (0.0) 0 (0.0)
Myalgia 18.453 403 (2.0) 6.113 (2.5) 49 (2.1) 11.888 (6.3)
Others 277.721 8.342 (42.3) 155.117 (63.2) 783 (32.9) 113.479 (60.1)
Total Applications 455.882 19.682 245.166 2.374 188.660
Table 2. Anxiety distribution in patients who applied to the chest diseases and emergency polyclinics
Application Qualification Total (%) Male (%) Female (%)
Turkish citizens that applied to the Chest Diseases Polyclinic in the Central Building 313 (1.6) 74 (0.4) 239 (1.2)
Turkish citizens that applied to the Emergency Polyclinic in the Central Building 1,225 (0.49) 362 (0.14) 863 (0.35)
Syrian refugees that applied to the Chest Diseases Polyclinic in the Annex Building 35 (1.5) 10 (0.4) 25 (1.1)
Syrian refugees that applied to the Emergency Polyclinic in the Annex Building 385 (0.20) 162 (0.08) 223 (0.12)
Total 1.958 608 1.350
Kurtuluş et al. Diagnosis of Chest Diseases in Refugees and Turkish Citizens
119

matic events that may result in migration, illness, or death, lack of shelter, loss of living sources, poor nutrition, inade-quate hygiene, language problems, and inadequate access to health services lead to increased health problems, especially among individuals who experience forced migration [11,12]. One of these health problems is respiratory diseases [13,14]. Lung diseases, known as the cause of one in six deaths around the world, are one of the world’s most serious health problems because they decrease quality of life, increase the cost of care, and decrease productivity [15,16].
The data obtained from our study show that the rates of pneu-monia, asthma, and COPD among refugees living in tent camps are higher than those among Turkish citizens (Table 1). In a field research in which chronic diseases were also ex-amined among Syrian refugees using a questionnaire, it was reported that 7% of asylum seekers living in camps and 8% of the asylum seekers living outside camps had chronic dis-eases [17]. In our study, the rate of chronic bronchitis (COPD) among other chronic diseases was found to be 10.6% for refugees and 9% for Turkish citizens, which is remarkably high. The literature is insufficient in terms of the diagnosis that enables the comparison of the results obtained from our study. However, some studies with different methodologies show that respiratory diseases are a frequent problem in mi-grating communities and in immigrant-receiving communi-ties [13,14,18].
Psychological and physical violence during the pre-migra-tion period, genocide, witnessing the injury and death of relatives, destruction, plunder, child abduction, financial impossibilities, and trauma are circumstances that increase the risk of mental diseases. Moreover, legal barriers such as homelessness, anxiety about the future, and linguistic and cultural impediments pose a risk in terms of psychological problems that may also occur after migration [19]. Lebanon’s first large-scale psychiatric epidemiological study, which is a part of the Global Mental Health Research Initiative of the World Health Organization (WHO), has surprisingly shown that 49% of the population has experienced some sort of war-related trauma [20]. According to the study by Husain et al. [21], which was conducted in Sri Lanka during the post-war period, rate of anxiety was found to be 32.6%; in addi-tion, post-war post-traumatic stress syndrome, anxiety, and depression levels were also measured. In our study, the rate of anxiety was 1.7% among refugees. The results was ob-tained are lower than those in the literature, which can be explain by the inclusion of only the patients who applied to the Chest Diseases and Emergency Polyclinics. However, the rate of 1.7% is still remarkable for war- aggrieved patients. Even if our finding is lower than the study in the literature, it is enough to show that the refugees effects from the war [22,23]. The results obtained in our study show that the Turk-ish citizens that witness war and live in district close to the national border are also affected by war. This influence is higher than in the refugees coming from a war environment. In fact, the rate of anxiety detected among Turkish citizens was 2.09%. In both groups, anxiety was found to be more frequent in women than in men. Based on our subjective ob-servations, this can be explained by the fact that, in terms of protecting and maintaining the family, women are more sen-
sitive toward, migration, and the problems that accompany these circumstances. Anxiety levels were examined in a field research via questionnaire involving Syrian refugees in 2013, and anxiety was reported to be more frequent in women than in men [17]. This result is similar to our study.
According to World Health Organization (WHO) estimates, in 2015, 10.4 million new cases of tuberculosis were noted, and 1.8 million people lost their lives because of the disease. Although the number of new cases indicates that the inci-dence of tuberculosis decreases by 1.5% per year, it remains an important public health problem [24,25].
Societies experiencing migration are faced with several in-fectious diseases because they enter a new environment as well as they often live under bad conditions. The destruc-tion of health facilities and the difficulties in disease manage-ment because of the lack of medical personnel and due to increased need for drugs due to illness, and living outside the camp and indifferent refugees cannot get free drugs as ınability to achieve drugs, in the countries where they come from, and the physical, social, and psychological adaptation process in newly arrived societies are some of the main rea-sons of the emerging health problems. One of these health problems is tuberculosis, which is an important public health problem [24,26].
As per the 2012 WHO Global Tuberculosis Report, Syria’s goal for the prevention of tuberculosis was to decrease the preva-lence of tuberculosis from 85/100,000 in 1990 to 23/100,000 in 2011 [27]. As a matter of fact, in the 2014 tuberculosis re-port, it was seen that the rate decreased to 17/100,000. How-ever, the increase in conflicts in Syria has adversely affected diagnosis and treatment initiatives for tuberculosis in every area. The prevalence of tuberculosis in Syria was found to be 20/100,000 according to the data from the Global Tuberculo-sis Report in 2016. According to the same report, the preva-lence of tuberculosis in Turkey is 18/100,000 [24].
The prevalence of tuberculosis was found to be 18.7/100,000 in screening studies conducted on refugees in our country. This rate is the same as the prevalence in the Turkish society [28]. In our study, while the number of cases that was detected in Syr-ian refugees living in tent camps with a population of 19,948 [29] was three, this number was 10 in Turkish citizens living in this district with a population of 84,727 [10]. When the num-ber of cases which was investigated according to the popula-tion is proportioned, it is seen that there are similar proportions in refugees living in tent camps and in Turkish citizens living in this district. In addition, when the Global Tuberculosis Reports are examined, it is reported that the number of tuberculosis cases increased by years along with the war in Syria. It can be seen from our study that the number of cases of tuberculosis detected in refugees living in tent camps is lower than that in the country where they come from.
The results of our study show that there is no difference be-tween Syrian refugees and Turkish citizens, and at the same time, the refugees are in a better position in terms of tubercu-losis than in the countries they immigrate from. This can be explained by the lack of social and environmental problems brought by urbanization in the region where the study was
Turk Thorac J 2018; 19(3): 117-21
120

conducted, availability of unique social and environmental variables that are intertwined with nature, and adequacy of health services provided in the environments where access to health and other services is free of cost.
Regarding refugees and Turkish citizens, the similarity in the distribution of the applications to the Department of Chest Diseases and increase in infectious diseases such as tuber-culosis among refugees living in tent camps suggest that the quality of health services offered in the refugee tent camps are close to the ideal services. Contrary to the expectations that anxiety caused by war among refugees is higher than that among Turkish citizens, the fact that Turkish citizens have anxiety rates similar to refugees and are affected by war as much as the refugees are, suggests that the healthcare and psycho-social support offered to refugees in tent camps should also be given to Turkish citizens and that new regula-tions are required in public health policies. We believe that the data from our study will shed some light on this issue.
Ethics Committee Approval: Ethics committee approval was received for this study from Ethics Committee of Harran University (Approval Date: 06.10.2016).
Informed Consent: N/A
Peer-review: Externally peer-reviewed.
Author contributions: Concept - Ş.K., Z.H.A.S.; Design - Ş.K., Z.H.A.S., R.C.; Supervision - Ş.K., R.C.; Resource - Ş.K., Z.H.A.S., R.C.; Materials - Ş.K., Z.H.A.S., R.C.; Data Collection and/orProcess-ing - Ş.K., Z.H.A.S., R.C.; Analysis and/orInterpretation - Ş.K., R.C.; LiteratureSearch - Ş.K., Z.H.A.S., R.C.; Writing - Ş.K., Z.H.A.S., R.C.; Critical Reviews - Ş.K., Z.H.A.S., R.C.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has re-ceived no financial support.
REFERENCES
1. Turkey Immigration Report 2016 (Türkiye Göç Raporu 2016). http://www.goc.gov.tr/files/files/2016_goc_raporu_.pdf (Access: 23.05.2017)
2. United Nations High Commissioner for Refugees 2016.3. Ehntholt KA, Yule W. Practitioner review: assessment and treat-
ment of refugee children and adolescents who have experienced war-related trauma. J Child Psychol Psychiatry 2006;47:1197-210. [CrossRef]
4. Adanu RMK, Johnson TRB. Migration and women’shealth. Int J Gynaecol Obstet 2009;106:179-81. [CrossRef]
5. Eskiocak M. War And Health: Health Outcomes Of Hatay Civil War İn Syrian (There İs No Health Where There İs No Peace (Savaş ve Sağlık: Suriye İç Savaşının Hatay’daki Sağlık Sonuçları: Barışın Olmadığı Yerde Sağlık Olmaz) 2013;50-63.
6. Karadağ Ö, Altıntaş KH. Refugees and Health (Mülteciler ve Sağlık). TAF Preventive Medicine Bulletin 2010;9,55-62.
7. Department of Disaster and Emergency Management 2017 (Afet ve Acil Durum Yönetimi Başkanlığı 2017). https://www.afad.gov.tr/tr/2373/Suriyeli-Siginmacilara-YapilanYardimlar (Ac-cess: 11.06.2017)
8. Berti B.The Syrian Refugee Crisis: Regional and Human Security Implications. Strategic Assessment 2015;17:41-53.
9. Orhan O, Pirinçci F, Erkmen S, et al. The Situation of Syrian Refugees in the Neighboring Countries: Findings, Conclusions and Recommendations: 2014. Report Number: 189 (Suriye’ye Komşu Ülkelerde Suriyeli Mültecilerin Durumu Bulgular, Sonuçlar ve Öneriler: 2014. Rapor No:189)
10. http//:ceylanpinarkaymakamlik.gov.tr (Access: 15.07.2017) 11. Mowafi H. Conflict, displacement and health in the Middle
East. Glob Public Health 2011;6:5 472-8712. Peltokorpi V. İntercultural communication in foregien, subsidiar-
ies, the ınfluence Expatriates language and cultural competen-cies. SJM 2010;26:2 176-88
13. Çıtıl R, Eğri M. Migration and Infectious Diseases (Göçler ve En-feksiyon Hastalıkları). Türkiye Klinikleri J Public Health-Special Topics 2017;3:1 14-21
14. Amara AH, Aljunid SM. Noncommunicable diseases among urban refugees and asylum-seekers in developing countries: A Neglected Health Care Need. Global Health 2014;10:24. [CrossRef]
16. Pulmonary Health in Europe Facts and figures. Pulmonary health in Europe and better understanding of respiratory care (Avrupa’da Akciğer Sağlığı Gerçekler ve rakamlar. Avrupa’da Akciğer Sağlığı Avrupa’da akciğer sağlığı ve solunum bakımının daha iyi anlaşılması). 2013 http://www.europeanlung.org/as-sets/files/small_whitebooks/lung_health_in_europe_facts_and_figures_master_awturkish.pdf. (Access: 30.07.2017)
17. Department of Disaster and Emergency Management 2013 (Afet ve Acil Durum Yönetimi Başkanlığı 2013). https://www.afad.gov.tr/upload/Node/3925/xfiles/syrian-refugees-in-turkey 2013_baski_30_12_2013_tr.pdf https://www.afad.gov.tr/up-load/Node/3925/xfiles/syrian-refugees-in-turkey 2013_bas-ki_30_12_2013_tr.pdf (Access: 19.08.2017)
18. UNHCR Handbook for Emergencies. 3rd Edition. Geneva. 200719. Craıg T, Jajua PM, Warfa N. Mental Health Care Needs Of Refu-
gees. Psychiatry 2009; 8:9 351-420. Adams P. In Lebanon, mental health is on the mend. Lancet
Glob Health 2011;377:707-8. [CrossRef]21. Husain F, Anderson M, Lopes Cardozo B, et al. Prevalence of
war-related mental health conditions and association with displacement status in postwar Jaffna District Sri Lanka. JAMA 2011;306: 522-31. [CrossRef]
22. Önen C, Güneş G, Türeme A, et al. Depression and Anxiety Status in Syrians who Live in a Refugee Camp (Bir Mülteci Kampında Yaşayan Suriyelilerde Depresyon ve Anksiyete Du-rumu). ASOS Journal 2014;2:223-30. [CrossRef]
23. Bogic M, Njoku A, Priebes S, et al. Long-Term Mental Health of War-Refugees: A Systematic Literature Review. BMC, 2015:15-29
24. World HealthOrganization. Global tuberculosisreport 2016. http:// www.who.int/tb/publications/global_report/en/. (Access: 15.09. 2017)
25. European Centre for Disease Prevention and Control. 2015. WHO Regional Office for Europe. Tuberculosis surveillance and monitoring in Europe. https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/tuberculosis-surveillance-monitoring-Europe-.pdf (Access11.09.2017)
26. Balkan İ İ. Holistic Approach to Refugee Health. Mülteci Sağlığına Bütüncül Yaklaşım) SD Platform 2016;40:6-9.
27. World Health Organization: Global Tuberculosis Report 2012. http:// www.who.int/tb/publications/global_report/en/ (Access: 26.11. 2017)
28. Studies Directed at Syrian Guests (Suriyeli Misafirlere Yönelik Çalışmalar). The Data of Turkish Public Health Institution. (Türk Halk Sağlığı Kurumu Başkanlığı Verileri) https://www.saglik.gov.tr/TR,11062/turkiye-halk-sagligi-kurumu.html (Access: 15.11.2017)
29. https://www.afad.gov.tr/upload/Node/2374/files/22_11_2017_Suriye_GBM_Bilgi_Notu.pdf-(Access: 25.11.2017)
Kurtuluş et al. Diagnosis of Chest Diseases in Refugees and Turkish Citizens
121

Turk Thorac J 2018; 19(3): 122-6
Original Article
Factors Affecting Influenza Vaccination Rates among Patients with Chronic Obstructive Pulmonary Disease in Rize, Turkey
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) represents a major health challenge and is currently the fourth leading cause of death worldwide [1]. Acute excacerbations are the most common causes of death in COPD patients. . The con-nection between acute exacerbations of COPD (AECOPD) and morbidity and mortality has been disclosed [2]. Latest therapeutic and protective strategies are directed towards the prevention of AECOPD.
Approximately 70% of AECOPD cases are of infectious origin. Respiratory viruses are isolated in approximately 30% of cases [3,4]. Bacterial and viral co-infections may also occur with bacterial infections complicating an initial viral infec-tion. Both severity of COPD and not receiving influenza vaccination have been shown to be associated with a high risk of mortality [5]. As a result, influenza and pneumococcal infections are the most common causes of AECOPD [6]. Both influenza and pneumococcal vaccinations have been reported to decrease the incidence of lower respiratory tract infec-tions in the GOLD (Global Initiative for Chronic Obstructive Pulmonary Disease) 2017 guideline [7]. For this reason, vaccination is a cost-effective and life-saving approach. There are few studies that investigated the effects of influenza vaccination on AECOPD, but they have shown that influenza vaccination results in lower number of exacerbations than placebo use in vaccination [8]. No statistically significant effects on exacerbation have been shown with pneumococcal vaccination [9].
In this study, we aimed to assess the characteristics of COPD patients during 2014 vaccination season and its association with AECOPD in the following year in Rize, Turkey.
DOI: 10.5152/TurkThoracJ.2018.17075
Songül Özyurt, Bilge Yılmaz Kara, Neslihan Özçelik, Ünal ŞahinDepartment of Pulmonology, Recep Tayyip Erdoğan University School of Medicine, Rize, Turkey
Address for Correspondence: Bilge Yılmaz Kara, Department of Pulmonology, Recep Tayyip Erdoğan University School of Medicine, Rize, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
122
Cite this article as: Özyurt S, Yılmaz Kara B, Özçelik N, Şahin Ü. Factors Affecting Influenza Vaccination Rates among Patients with Chronic Obstructive Pulmonary Disease in Rize, Turkey. Turk Thorac J 2018; 19(3): 122-6.
OBJECTIVES: Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are major components of COPD-related so-cioeconomic burden. Upper or lower respiratory tract infections, usually caused by respiratory viruses or bacteria, are common causes of AECOPD. Vaccination aganist influenza virus and Streptoccus pneumoniae, the most prevalent agents, is recommended by COPD guidelines. The aims of this study were to determine the factors affecting vaccination among patients with COPD and to assess the effect of vaccination status on AECOPD.
MATERIALS AND METHODS: Patients with COPD were recruited from the outpatient clinic of a tertiary hospital between December 2014 and January 2015. Demographic data, vaccination status, and COPD-related hospital admissions triggered by tracheobronchial infections were evaluated.
RESULTS: In total, 108 patients were enrolled; 102 (94%) subjects were male, and 6 (6%) subjects were female; the mean age was 65.6 years. The number of patients who had received pneumococcal and influenza vaccinations were 8 (0.07%) and 36 (33.3%), respectively. There was no significant correlation between the level of education and vaccination status. No significant difference was found between two groups in terms of exacerbation frequency, hospitalization rates, mMRC scores, and COPD stages.
CONCLUSION: More efforts by both physicians and patients are needed to reach the ideal rates of vaccination for COPD.
KEYWORDS: Chronic obstructive pulmonary disease, influenza vaccination, pneumococcal vaccination
Abstract
Received: 26.09.2017 Accepted: 30.01.2018 Available Online Date: 12.06.2018
An editorial comment on this article is available at page 101

MATERIALS AND METHODS
Study PopulationA total of 108 patients with COPD were recruited from the outpatient clinic of a tertiary center in Rize province, Tur-key, between December 2014 and January 2015. All patients were residents of Rize, and they had been followed by pul-monary specialists for COPD.
Study DesignEducational status, residence information (urban/rural area), mMRC (modified Medical Research Council) dyspnea score and COPD stage according to GOLD guidelines, smoking habits, and co-morbidities were noted with the help of a questionnaire. History of an influenza vaccine shot during the previous year or a pneumococcal vaccine shot during the last five years, factors affecting the decision of being vaccinated or not (the source of information if vaccinated, the reason if not vaccinated), and the number of severe or mild AECOPD cases requiring hospital admission were en-quired and confirmed using the hospital’s computer record-ing system.
Exclusion CriteriaPatients previously diagnosed with obstructive pathologies such as asthma or bronchiectasis; patients with active cancer, chronic organ failure, uncontrolled hypertension, or diabetes mellitus; patients with a history of hospitalization during the study period, suffering from AECOPD, or unable to perform a pulmonary function test (PFT) for any reason during the data collection phase were excluded from the study. All patients provided written informed consent. The study was approved by the local ethics committee and was conducted in accor-dance with the Declaration of Helsinki.
Statistical AnalysisThe primary objective of the study was to determine the factors affecting influenza and pneumococcal vaccination among patients with COPD, and the secondary objective of the study was to show the relationship between vaccination and AECOPD rates in the following year.
IBM Statistical package for Social Sciences version 21.0 (IBM SPSS Corp.; Armonk, NY, USA) software was used for sta-tistical analysis. Parametric data were presented as mean ± standard deviation. Student’s t-test was used for parametric variables, and the Mann-Whitney U-test was used for non-parametric variables. Spearman test was used for correlation analysis. Yates correction chi-square test and Fisher’s exact test were used for the comparison of qualitative data. P-val-ues less than 0.05 were considered significant.
RESULTS
A total of 108 patients were included in the study. Their mean age was 65.6±9.7 years, and 94% were male. Among them, 63% resided in urban areas and the remaining 37% resided in rural areas. In addition to COPD, systemic hypertension was seen in 64.8% of the patients, congestive heart failure in 12%, and diabetes mellitus in 12%. According to the GOLD guideline, 33.3% of the patients were in group A, 22.2% were in group B, 17.6% were in group C, and 26.9% were in group D. The mean smoking rate was 48.5±31.6 packs per year. In total, 13% of the patients were illiterate, 64.8% were elementary school graduates, 9.3% were junior high school graduates, 6.5% were high school pass-outs, and 0.9% was university graduates. In the study population, only eight (7%) patients had pneumococcal vaccine shots and 36 (33.4%) had influenza vaccine shots. Vaccination was recommend-ed by physicians in 82.5% of the patients, by pharmacists in 15%, and by other sources (e.g., television or newspaper) in 2.5%. Among patients who did not receive vaccinations, 8.7% did not believe that vaccination was beneficial, where-as 88.4% reported that they did not receive vaccination be-cause it was not recommended by their physician (Table 1).
Demographic data comparing the influenza-vaccinated and non-vaccinated groups are presented in Table 2. Thirty-six of 108 patients (33.3%) had received influenza vaccination. There was no statistically significant difference between groups of patients who had and had not been vaccinated in terms of age, gender, co-morbidities, COPD stages, or smok-ing status. The rate of influenza vaccination was significantly higher in patients living in urban areas compared to those living in rural areas (p=0.024).
Table 1. Demographic data of all patients and study results
Parameters All patients (n=108)
Mean age (Years) 65.6± 9.7
Gender (M/F) 102 (94%)/6 (6%)
Place of residence (Urban/Rural) 68 (63%)/40 (37%)
Education level Illiterate 14 (13%)
Elementary school 70 (64.8%)
Junior high school 10 (9.3%)
High school 7 (6.5%)
University 1 (0.9%)
GOLD Stages A/B/C/D 36 (33.3%)/ 24 (22.2%)/ 19 (17.6%)/ 29 (26.9%)
Smoking history (packs/year) 48.5±31.6
Influenza vaccination Vaccinated 36 (33.4%)
Non-vaccinated 72 (66.6% )
Pneumococcal vaccination Vaccinated 8 (0.07 %)
Non-vaccinated 100 (99.3 %)
Source recommending vaccination Physician 33 (82.5%)
Pharmacist 6 (15%)
Other 1 (2.5%) (TV, newspaper etc.)
Reason for not being vaccinated Not recommended 61 (88.4%)
Do not believe 6 (8.7%) in the benefit
M: male; F: female; GOLD: Global Initiative for Chronic Obstructive Pulmonary Disease; TV: television. Data were presented as number and percentage.
Özyurt et al. Factors Affecting Influenza Vaccination among COPD Patients
123

Influenza-vaccinated patients had significantly lower post-bronchodilator FEV1, FEV1/FVC, and FVC values than non-vaccinated patients. No statistically significant difference was found between two groups in terms of frequency of exacerba-tions, rates of hospitalization, and mMRC scores (Table 3).
The rate of hospitalization positively correlated with GOLD stages, exacerbation number, and mMRC score and negatively correlated with pre- and post-bronchodilator FEV1 (liters, %)
and FVC (liters, %). There was no correlation between rates of hospitalization and vaccination as well as pre- and post- bronchodilator FEV1/FVC ratios (Table 4).
DISCUSSION
Although there is evidence that viral infections lead to exac-erbations of chronic airway diseases such as COPD [10,11], vaccination has not been proven to reduce mortality[12]. On the other hand, a systematic review that summarized the im-munogenicity, safety, efficacy, and effectiveness of influenza vaccination in patients with COPD found that six of seven studies indicated long-term benefits such as decreased num-ber of exacerbations, reduced number of hospitalizations, and decreased rates of all-cause and respiratory mortality [13]. In our study, we were not able to show the reduced number of exacerbations or rates of hospitalization in vac-cinated patients. Another study investigating etiologic agents causing AECOPD found Haemophilus influenzae, Moraxella catarrhalis, and rhinovirus as the most incident pathogens. Therefore, the vaccination spectrum for COPD should be more diverse to enclose other potential pathogens causing AECOPD [14], and new vaccines against these pathogens should be developed.
Educational status may influence vaccination awareness; in a study investigating the relationship between education level and preventive health care use, college attendance was found to be strongly associated with receiving influenza vac-cination in old age [15]. On the contrary, another study con-cluded that receiving vaccination was not related to the level of education but that the advice of health care professionals (particularly a doctor) led to high vaccination compliance [16]. Our findings showed that there was no relationship be-
Table 2. Demographic data of influenza-vaccinated and non-vaccinated patients
Influenza- Non- vaccinated vaccinated Parameters (n=36) (n=72) p
Age (years) 65.9±11.0 65.5±9.1 0.60
Gender (M/F) 34 (31%)/ 68 (63%)/ 0.98 2 (1%) 4 (3%)
Urban/Rural Residents 28 (77.8%)/ 40 (55.5%)/ 0.024 8 (22.2%) 32 (44.5%)
COPD Stages (A/B/C/D) 9/6/9/12 27/18/10/17 0.22
Co-morbidity (n, %) 14 (38.8%) 32 (44.4%) 0.68
Education level 0.29
• Illiterate 2 (5.6%) 12 (16.6%)
• Elementary school 28 (77.8%) 48 (66.7%)
• Junior high school 4 (11%) 6 (8.3%)
• High school 1 (2.8%) 6 (8.3%)
• University 1 (2.8%) 0 (0%)
Non-smoker (n, %) 2 (5.5%) 5 (7%)
Smoker (n, %) 2 (5.5%) 9 (12.5%) 0.49
Ex-smoker (n, %) 32 (89%) 58 (80.5%)
Smoking rate (packs/year) 47.15±33.0 51.19±28.9 0.27
Biomass (n, %) 1 (2.7%) 4 (5.5%) 0.66
Pneumococcal 5 (13.8%) 3 (4.1%) 0.11 vaccination (n, %)
M: male; F: female; COPD: chronic obstructive pulmonary disease Data were presented as number and percentage.
Table 4. Correlation analysis of hospitalization rates and GOLD stages, vaccination, exacerbation number, PFT parameters, and mMRC scores
Hospitalizations r p
GOLD stages +0.536 <0.001
Influenza vaccination +0.111 0.252
Pneumococcal vaccination +0.124 0.203
Number of exacerbations +0.467 <0.001
Pre-FEV1 /FVC ratio -0.128 0.199
Pre-FEV1 (L) -0.464 <0.001
Pre-FEV1 (%) -0.420 <0.001
Pre-FVC (L) -0.433 <0.001
Pre-FVC (%) -0.449 <0.001
Post-FEV1/FVC ratio -0.212 0.032
Post-FEV1 (L) -0.438 <0.001
Post-FEV1 (%) -0.449 <0.001
Post-FVC (L) -0.406 <0.001
Post-FVC (%) -0.459 <0.001
mMRC score +0.575 <0.001
GOLD: Global Initiative for Chronic Obstructive Pulmonary Disease; PFT: pulmonary function test; mMRC: modified Medical Research Council
Table 3. PFT results, mMRC scores, exacerbation numbers, and hospitalization rates of influenza-vaccinated and non-vaccinated patients
Influenza- Non- vaccinated vaccinated Parameters (n=36) (n=72) p
FEV1 (% pred) 51.9±15.9 62.6±23.1 0.02
FVC (% pred) 67.1±16.9 76.7±20.7 0.01
FEV1/FVC (%) 58.8±8.5 62.3±10.3 0.02
mMRC score 2.1±1.1 1.8±1.0 0.78
Number of exacerbations 5.5±5.8 5.1±4.7 0.89 Median: 4 Median: 4
Number of hospitalizations 0.9±1.9 0.8±2.0 0.25
M: male; F: female; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; mMRC: modified Medical Research Council; % pred: %predicted Data were presented as number and percentage.
Turk Thorac J 2018; 19(3): 122-6
124

tween the level of education and status for vaccination. The explanation of these conflicting results is that the relationship might be more complex and cannot be directly explained by the level of education or source of advice.
Patients tend to act in the direction of their physician’s sug-gestion, particularly when they have a chronic illness, which frequently exacerbates and forces the patients to seek a spe-cialist’s help. Most doctors have a tendency to closely deal with patients with advanced disease and frequent hospital-izations. Compared with mild disease, patients with more advanced disease stage may be more likely to seek vacci-nation because the consequences of influenza are more se-vere in such cases [17]. In our study, the negative correlation between PFT results and vaccination rates may reveal that “patients in danger” are those in an advanced stage based on doctors’ perspectives; PFT is not the only, but is still the best, indicator of severity. Further, the positive correlation with the mMRC score supports the idea that these patients suffer from more advanced disease. However, a change introduced in the 2010 NICE guideline is the new grading of COPD sever-ity, which is not based on the PFT alone. A full clinical assess-ment should include the severity of symptoms, frequency of exacerbations, and impact of disease on the functional and health status. All patients, regardless of their disease stage, should be recommended to receive influenza and pneumo-coccal vaccinations, body composition management, and pulmonary rehabilitation in addition to pharmacotherapy [18]. In our study, COPD staging was done according to the latest GOLD guidelines, but no statistically significant differ-ence between groups was demonstrated in terms of exacer-bation frequency or hospitalization rates.
Although Rize is a low-income province in Turkey, vacci-nation is paid by the health care system; hence, we do not believe that financial constrains are responsible for the low rate of vaccination in patients with COPD. Therefore, bet-ter understanding of factors affecting low compliance with vaccination at the individual level is crucial and should be elucidated in future studies [19].
In our study, low rates of both influenza and pneumococcal vaccinations in patients with COPD have been elucidated in Rize province. Similar studies have estimated vaccination rates from other parts of Turkey. Aktürk et al. reported a rate of 36.5% for influenza vaccination and 14.1% for pneumococ-cal vaccination [20]. A study investigating the gaps in using influenza vaccine pointed out that health care workers in low-income countries, such as India, believed that the influenza vaccine was harmful and hence was not prescribed. Other rea-sons cited by 1359 participants included unawareness about vaccine availability (32%), doubts about efficacy (18%), busy schedule (12%), fear of side effects (4%), and patients’ disbe-lief of being at risk group of influenza disease (6%) [21].
These results may be due to the lower vaccination rates in patients with COPD in Rize province than in similar subject groups in which a retrospective study design is used [22]. Moreover, beside the vaccination rates, other factors such as inhaler/systemic steroid usage, bacterial colonization of the lower respiratory tract, and antibiotic usage may be related
with the AECOPD frequency. In this regard, there is a need for prospective, randomized controlled trials involving more subjects.
The limitations of our study were as follows: 1. A comparison between males and females was not possible because most patients were male. 2. The sample size was small; therefore, the number of vaccinated subjects was not adequate to make a final decision about the effectiveness of vaccination. 3. Bacteriologic or viral isolation of agents responsible for AE-COPD was not possible due to financial or technical causes. 4. Since the number of pneumococcal vaccine recipients was low, the relevant data have not been discussed. 5. Data is missing about why doctors avoid prescription of pneumococ-cal or influenza vaccines.
In conclusion, tracheobronchial infections are one of the most common causes of acute attacks in patients with COPD, and vaccination against existing pathogens is essential. How-ever, vaccination rates are still low, and it should be empha-sized by physicians that all patients should be vaccinated.
Ethics Committee Approval: Ethics committee approval was ob-tained for this study from the Ethics Committee of Karadeniz Techni-cal University. (Approval Number: 2014/135)
Informed Consent: Written informed consent was obtained from all patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - S.Ö., Ü.Ş.; Design - S.Ö., Ü.Ş.; Su-pervision - S.Ö., Ü.Ş.; Resource - S.Ö., Ü.Ş. Materials - S.Ö., Ü.Ş.; Data Collection and/or Processing - S.Ö.; Analysis and/or Interpretation - B.Y.K., N.Ö.; Literature Search - B.Y.K.; Writing - B.Y.K., N.Ö.; Critical Reviews - B.Y.K., N.Ö.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has re-ceived no financial support.
REFERENCES
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Dis-ease Study 2010. Lancet 2012;380:2095-128. [CrossRef]
2. García-Sanz MT, Cánive-Gómez JC, Senín-Rial L,et al. One-year and long-term mortality in patients hospitalized for chron-ic obstructive pulmonary disease. J Thorac Dis 2017;9:636-45. [CrossRef]
3. Miravitlles M, Anzueto A. Role of infection in exacerbations of chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2015;21:278-83. [CrossRef]
4. Mohan A, Chandra S, Agarwal D, et al. Prevalence of viral infec-tion detected by PCR and RT-PCR in patients with acute exacer-bation of COPD: a systematic review. Respirology 2010;15:536-42. [CrossRef]
5. Montserrat-Capdevila J, Godoy P, et al. [Risk factors for mortality in patients with chronic obstructive pulmonary disease]. Aten Primaria 2015;47:498-504. [Article in Spanish] [CrossRef]
6. Sethi S. Murphy T. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med 2008;359:2355-65. [CrossRef]
Özyurt et al. Factors Affecting Influenza Vaccination among COPD Patients
125

7. GOLD (2017) Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. February. Available at: http://www.goldcopd.org.
8. Poole PJ, Chacko E, Wood-Baker R, et al. Influenza vaccine for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2006;1:CD002733. [CrossRef]
9. Walters JA, Smith S, Poole P,et al. Injectable vaccines for pre-venting pneumococcal infection in patients with chronic ob-structive pulmonary disease. Cochrane Database Syst Rev 2010;11:CD001390. [CrossRef]
10. Hershenson MB. Rhinovirus-Induced Exacerbations of Asthma and COPD, Scientifica (Cairo) 2013;2013:405876.
11. Koul PA., Khan UH., Asad R, et al. Contribution of influenza to acute exacerbations of chronic obstructive pulmonary disease in Kashmir, India, 2010-2012. Influenza Other Respir Viruses 2015;9:40-2. [CrossRef]
12. Joshi M, Chandra D, Mittadodla P, et al. The Impact of Vacci-nation on Influenza-Related Respiratory Failure and Mortality in Hospitalized Elderly Patients Over the 2013-2014 Season. Open Respir Med J 2015;9:9-14. [CrossRef]
13. Bekkat-Berkani R, Wilkinson T, Buchy P, et al. Seasonal influ-enza vaccination in patients with COPD: a systematic literature review. BMC Pulm Med 2017;17:79. [CrossRef]
14. Wilkinson TMA, Aris E, Bourne S, et al. A prospective, ob-servational cohort study of the seasonal dynamics of airway pathogens in the aetiology of exacerbations in COPD. Thorax 2017;72:919-27. [CrossRef]
15. Fletcher JM, Frisvold DE. Higher Education and Health Invest-ments: Does More Schooling Affect Preventive Health Care Use? J Hum Cap 2009 Summer; 3:144-76. [CrossRef]
16. Cimen P, Unlu M, Kirakli C, et al. Should Patients With COPD Be Vaccinated? Respir Care 2015;60:239-243. [CrossRef]
17. Mullahy J. It’ll only hurt a second? Microeconomic determinants of who gets flu shots. Health Econ 1999;8:9-24. [CrossRef]
18. Walker PP. Opportunistic case finding pivotal in diagnosing COPD. Practitioner 2010;254:19-20,23-4,2.
19. Gnatiuc L,Buist AS, Kato B, Janson C, Ait-Khaled NA, Nielsen R, et al. Gaps in using bronchodilators, inhaled corticosteroids and influenza vaccine among 23 high- and low-income sites. Int J Tuberc Lung Dis 2015;19:21-30. [CrossRef]
20. Aka Aktürk Ü, Görek Dilektaşlı A, Şengül A, Musaffa Salepçi B, Oktay N, Düger M, et al. Influenza and Pneumonia Vacci-nation Rates and Factors Affecting Vaccination among Patients with Chronic Obstructive Pulmonary Disease. Balkan Med J 2017;34:206-11. [CrossRef]
21. Bali NK, Ashraf M, Ahmad F, Khan UH, Widdowson MA, Lal RB, et al. Knowledge, attitude, and practices about the sea-sonal influenza vaccination among healthcare workers in Srinagar, India. Influenza Other Respir Viruses 2013;7:540-5. [CrossRef]
22. Santaularia J, Hou W, Perveen G, Welsh E, Faseru B. Prevalence of influenza vaccination and its association with health condi-tions and risk factors among Kansas adults in 2013: a crosssec-tional study. BMC Public Health 2016;16:185. [CrossRef]
Turk Thorac J 2018; 19(3): 122-6
126

Turk Thorac J 2018; 19(3): 127-31
Original Article
High-Frequency Jet Ventilation in Nonintubated Patients
INTRODUCTION
Fiberoptic bronchoscopy has been widely utilized over the last years in pulmonary medicine for diagnosis and treatment of pulmonary diseases such as pleural tumors, tuberculosis, and lipoid pneumonia [1-3]. Qualified ventilation in sedated patients during bronchoscopy is an issue of utmost consequentiality. Nasal oxygen supply is adequate for maintaining conventional oxygen saturation (So2) of over 90% in mildly sedated patients. However, when deeper sedation is needed during the procedure, dropping oxygen (O2) and elevating carbon dioxide (CO2) pressures as well as acidemia and arrhythmia are the frequent quandaries faced. Different approaches have been introduced for ventilating deeply sedated patients [1]. Conventional mechanical ventilation (CMV) conventionally does not ameliorate O2 supplementation during bronchoscopy in sedated patients. Therefore, providing ventilation in this setting is vital.
High-frequency jet ventilation (HFJV) is an opportune technique that distributes a minuscule tidal volume with a fre-quency exceeding the physiologic level of the patient [3-5]. HFJV can be applied via supraglottic [such as laryngeal mask airway (LMA)], transtracheal, or subglottic approaches [6-9]. All of the three methods truncate the expiratory time and linearly increase the pulmonary capillary wedge pressure and greatest sanctioned working pressure.
The supraglottic HFJV provides the most rapid increase in airway pressure. Transtracheal HFJV approach provides the most consistent atmospheric pressure of the fraction of inspired oxygen (FiO2). However, both methods increase the peril
DOI: 10.5152/TurkThoracJ.2018.17025
Atefeh Abedini1 , Arda Kiani2 , Kimia Taghavi1 , Ali Khalili3, Alireza Jahangiri Fard4 , Lida Fadaizadeh5 , Alireza Salimi1 , Tahereh Parsa6 , Akram Aarabi4 , Behrooz Farzanegan2 , Mahsa Pourabdollah Tootkaboni1 1Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran2Tracheal Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran3Tobacco Prevention and Control Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran4Lung Transplantation Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran5Telemedicine Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran6Pediatric Respiratory Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Shahid Beheshti University of Medical Sciences, Tehran, Iran
Address for Correspondence: Arda Kiani, Tracheal Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases (NRITLD), Massih Daneshvari Hospital, Tehran, Iran E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
127
Cite this article as: Abedini A, Kiani A, Taghavi K, et al. High-Frequency Jet Ventilation in Nonintubated Patients. Turk Thorac J 2018; 19(3): 127-31.
OBJECTIVES: High-frequency jet ventilation (HFJV) is a convenient method for providing ventilation during fiberoptic bronchoscopy. We describe an incipient approach of high-frequency jet ventilation via the working channel of a flexible bronchoscope for nonintubated patients who suffer from hypoxemia during bronchoscopy. The aim of this study was to test the efficacy of this incipient approach and determine the possible complications related to it.
MATERIALS AND METHODS: Sixteen patients who had oxygen saturation below 70% that did not resolve with nasal oxygen for 20 s during interventional bronchoscopy were included in the study. High-frequency jet ventilation was administrated via the working chan-nel of a bronchoscope for 3 min. Arterial blood gas circumscriptions were compared before and after jet ventilation.
RESULTS: Oxygen saturation increased to >90% in all patients 30 s after jet ventilation. Mean arterial oxygen saturation pressure in-creased from 54.84 to 111.98 mmHg with jet ventilation (p=0.0001). Arterial carbon dioxide tension decreased after jet ventilation. The body mass index had no consequential effect on arterial carbon dioxide pressure after jet ventilation in our patients (p=0.1). Complica-tions such as pneumothorax and working channel damage were not observed.
CONCLUSION: High-frequency jet ventilation via the working channel of the bronchoscope is a novel method that can provide opti-mal ventilation with minimal complications to nonintubated patients suffering from hypoxemia during bronchoscopy. This method also reduces the duration of bronchoscopy procedures.
KEYWORDS: High-frequency jet ventilation, bronchoscopy, hypoxemia, ventilation, arterial oxygen, flexible bronchoscopy
Abstract
Received: 18.03.2017 Accepted: 10.04.2018

of blowing debris, barotrauma, and hypercapnia [5,6]. In comparison with these, complications are minimized with the subglottic approach. Furthermore, PAWP can be observed, and the distributed FiO2 can be determined. Recently, sub-glottic HFJV was utilized broadly via different bronchoscope channels. However, the working channel of the broncho-scope (utilized for suction, oxygen distribution, and local anesthesia administration) has not been applied before in any study.
We evaluated a novel technique in nonintubated sedated patients undergoing flexible bronchoscopy (HFJV via the working channel) in this study.
MATERIALS AND METHODS
Study Design This randomized clinical tribulation study was designed by an expert methodologist. The final study population was estimated to be 10-20 patients. The research project was approved by the ethics committee and review board of Shadid Behehti University of Medical Sciences (IR. SBMU. MSP. REC.1395.218), and ethical clearance conformed to the Declaration of Helsinki. To comply with health indemnifica-tion portability, the principle of secrecy of patient informa-tion was taken into consideration.
Study Population In total, 150 patients with asthmatic bronchitis and chronic bronchitis underwent interventional flexible fiberoptic bron-choscopy for diagnosis or treatment during April-August 2016. Patients signed apprised informed consents after the study procedure was explained to them. Intervention opera-tions were routine operative procedures, and none of them were set for clinical research.
Baseline demographic characteristics including age, gender, and body mass index (BMI) were recorded for further analy-sis. Ecumenical guidelines were utilized in determining the normality of limits [10]. After quantifying the blood pressure and performing electrocardiogram, patients underwent deep sedation using a resilient instauration short-half-life drug (propofol with an infusion rate of 50-75 µg/kg/min; mid-azolam: 0.02 mg/kg; and fentanyl: 1-2 µg/kg). Sedation status was monitored using a bispectral index of 60. All bronchos-copy operations were conducted using a conventional flexi-ble bronchoscope (BF-1T260, Olympus Tokyo, Japan). The outer and main diameters of the working channel were 5.9 and 2.8 mm, respectively, which comply with the national guidelines [10]. Vital signs and So
2 were monitored and CMV approaches were provided during the procedure.
Patients were further monitored using pulse oximetry for O2 saturation during the different prep times of each patient for approximately 30-60 min. If SpO2 decreased below 70% and did not resolve within 20 s of nasal oxygenation, the patient was recommended for study inclusion and HFJV administra-tion. The inclusion criterion was 70% O2 saturation for 20 s as the borderline (the greatest time of abiding the least satura-tion). The omission criteria included rigorous cardiac dis-eases and unstable hemodynamics. Arterial blood sample was accumulated to determine the arterial blood gas (ABG).
HFJV (Monsoon, Acutronic Medical Systems AG, Baar, Switzerland) was applied for 3 min via the working channel of the bronchoscope. HFJV was performed with the following parameters: inspiration time of 45%, driving pressure of 3 bar, peak pressure of 80 mbar, FiO2 of 30%-100%, and fre-quency (ventilator rate) of 250/min. After applying HFJV for 3 min to obtain an incremented SpO2 to 90%, second arte-rial blood sampling was performed, and the bronchoscopy procedure was commenced (Figure 1,2). The arterial blood
Figure 1. Non-intubated sedated patient under HFJV during bronchoscopy with a flexible fiberoptic bronchoscope via the working channel
Figure 2. Jet ventilator catheter
Turk Thorac J 2018; 19(3): 127-31
128

pH was compared in two blood samples. The estimated ven-tilation efficacy and the availability of oxygen was obtained by comparing the partial pressure of carbon dioxide (PaCO2) (mmHg) and the arterial partial pressure of oxygen (PaO2) (mmHg) in two samples. The design of the current study is shown on Figure 3.
Statistical AnalysisData were statistically analyzed using paired t-test and ANOVA using (SPSS) Statistical Package for Social Sciences version 22.0 (IBM Corp.; Armonk, NY, USA). Statistical analyses were conducted following international statistical
standards. The perpetual analysis of variables such as age, gender, and BMI were presented as frequency and percent-age and mean (±standard deviation) or median (minimum-maximum). Categorical variables were expressed as frequen-cies and percentages. The variables for between-group differ-ences of the mean were calculated using Student’s t-test with significance set at p<0.05. Different parameter correlations were resolved using one-way ANOVA correlation coefficient.
RESULTS
Demographics AnalysisThe normality of variables was obtained using Kolmogorov-Smirnov test. Sixteen patients [10 males (62.5%) and 6 females (37.5%)] met the inclusion criteria. The patients’ age range was 37-75 years, with a mean age of 56±9.95 years. BMI of patients was in the range of 20.8-41 kg/m2, with a mean of 31.6±5.5 kg/m2. Two (12.5%) patients showed mun-dane BMI; 3 (18.8%) patients were inordinately corpulent and 11 (68.8%) were exorbitantly corpulent, according to International World Health Organization (Table 1).
Clinical AnalysisHigh-frequency jet ventilation increased SpO2 to more than 95% in less than 30 s in all 16 patients. The analysis of two ABG samples showed that mean PaCO2 decreased from 59.3±6.7 to 52.6±8.09 mmHg after 3 min of jet ventilation. Paired t-test showed that PaCO2 decreased significantly by applying HFJV (p=0.001). Arterial pH also increased from 7.29±0.03 to 7.30±0.04 after jet ventilation. However, these changes were not significant according to the paired t-test analysis (p=0.08). Mean PaO2 was 54.84 mmHg (PaO2/FiO2 ratio<300) before jet ventilation and increased significantly to 111.98 mmHg (P/F ratio~575) with HFJV. (p=0.0001). Partial pressure of carbon dioxide (PCO2) was 53.2±0.9 mmHg in patients with mundane BMI and 52.3±12.1 mmHg in inordi-nately corpulent patients. Despite our prospects, no significant differences were observed in PCO2 in individuals with different BMI status on the basis of one-way ANOVA p=0.1) (Table 2).
Post-procedure RecoveryLeak test was conducted after each procedure to estimate the possible complications associated with HFJV such as tearing of the working channel of the fiberoptic bronchoscope. However, no positive test was reported. To check for pneumothorax as
Table 1. Baseline demographic characteristics and BMI
Parameters Values
Age (year) (mean±SD) 56±9.95
Gender (M/F) 10/6
Body mass index (kg/m2) 31.6±5.5
Cause of intervention procedure
Asthmatic bronchitis, no. (%) 7 (44)
Chronic bronchitis, no. (%) 9 (66)
BMI NL (%) 12.5
Overweight (%) 18.8
Obese (%) 68.8
BMI: body mass index; SD: standard deviation
Figure 4. HFJV connected to the working channel of a flexible fiberoptic bronchoscope
Figure 3. Design of current randomized clinical tribulation study
150 patients were referred with asthmatic bronchitis and chronic bronchitis diagnosis
during April-August 2016
3 patients were excluded from the study due to
rigorous cardiac diseases and unstable hemodynamics
First arterial blood sample was accumulated to figure arterial blood gases (ABG)
Approval diagnostic or treatment interventional flexible fiber optic
bronchoscopy was operated
HFJV was applied for 3 minutes through the bronchoscope working channel with Inspiration Time (IT): 45%, Driving pressure: 3 bar, Peak pressure: 80 mbar, FiO2: 30-100%,
Frequency (Ventilator rate): 250/min
After stabilizing patients SpO2 to 90%, second arterial blood sampling was performed and the
bronchoscopy procedure was commenced
Sixteen patients (10 men and 6 women)
consummated the inclusion criteria
19 patients were recognized as HFJV necessity case due to SpO2 70% under for
twenty seconds or above
Abedini et al. Bronchoscopy High-Frequency Jet Ventilation
129

another complication of HFJV, we performed chest radiogra-phy after the procedure and every 2 h twice. No pneumotho-rax or other complications attributable to HFJV were observed.
DISCUSSION
High-frequency jet ventilation has been applied during interventional bronchoscopy since 1977. The variable methods of HFJV and the associated complications have been studied. Veres et al. [11] studied HFJV via LMA and achieved qualified ventilation during the procedure. However, they reported mild hypercapnia due to hypoven-tilation as the most mundane minor unpropitious effect of LMA-HFJV. They also reported that the LMA-HFJV tech-nique resulted in the extension of the bronchoscopy dura-tion due to removal of the bronchoscope and application of the ventilation mask when hypoxemia occurred. In an ear-lier study, Fernandez-Bustamante et al. [12] applied inter-ventional rigid bronchoscopy connected to a transvector for ventilation; they reported hypercapnia, hypoxemia, and transient hemodynamic changes as the most common com-plications of this HFJV technique. HFJV has been increas-ingly utilized using nasotracheal or tracheal catheters via the lateral port of the rigid bronchoscope, via the transtra-cheal route, or by moving the catheter in the bronchoscope [13-21]. Hautmann et al. [19] studied HFJV using a tra-cheal catheter; they achieved adequate gas exchange dur-ing the bronchoscopy procedure and observed no hypoxia and hypotension. However, hypercapnia was the most com-mon complication during their approach.
The current study aimed to introduce a novel HFJV method to achieve optimal ventilation support and mitigate compli-cations during bronchoscopy. We delivered HFJV via the working channel of a flexible fiberoptic bronchoscope to nonintubated sedated patients who suffer from hypoxemia.
To designate a borderline hypoxemia index, the following study design was evaluated: SpO2 below 75% is the border-line of rigorous hypoxemia and SpO2 of 65% and below is the index value at which the patient will lose consciousness. Jet ventilation should never be resumed until the airway is open. Considering that mucus clogged the airway in most of our patients, conventional ventilations were applied at the maximum time to open the airway felicitously. Given that vital organs such as the encephalon have 20 s worth of oxy-gen storage capacity, 70% O2 saturation for 20 s was desig-nated as the borderline inclusion criterion (the maximum time of abiding the minimum saturation).
Considering the lack of access to capnography, we analyzed ABGs before and after jet ventilation to evaluate ventilation efficacy and possible ventilator setting adjustment needed. PaCO2 was found to be significantly reduced in our study after jet ventilation (p=0.001), whereas PaO2 significantly increased (p=0.0001). The congruous results favor the effi-cacy of the current incipient approach, which provides con-gruous ventilation to patients during bronchoscopy.
A P/F ratio<300 is equivalent to a partial pressure of oxygen (pO2) <60 mmHg; a P/F ratio<250 is equivalent to a pO2<50 mm Hg; and a P/F ratio<200 is equivalent to a pO2<40 mm Hg on room air. The P/F ratio significantly increased after HFJV (p=0.0001). Arterial pH additionally increased after jet ventilation, but the incrimination was not paramount after 3 min in our patients (p=0.08). However, given that most of our patients had chronic respiratory acidosis due to asthmatic bronchitis and chronic bronchitis, the arterial pH results might have been affected.
Generally, PCO2 reflects the exchange of this gas through the lungs to the outside air. Some degrees of pulmonary diseases with hyperventilation cause pH elevation. Pulmonary edema and acute asthmatic attacks affect lung capacity for freely exchanging CO2 across the alveolar membrane, thus, leading to high PCO2 levels.
Additionally, decreased pH is related to ventilation failure and severe degrees of pulmonary diseases. Overweight indi-viduals who are hyperventilating will breathe more rapidly and deeply and will blow off more CO2, thus, leading to low PCO2 levels. We hypothesized that HFJV will lead to increased pH in overweight individuals with high BMI. Despite our prospects, differences in PCO2 value after HFJV in the three variable BMI groups showed no significant differ-ences (p=0.1).
Prolonged foreign bodies result in granulation formation in the field of bronchoscopy. Recently, we utilized HFJV for clearing the bronchoscopy field when perpetuated peregrine body predisposed the field to bleeding during procedures. The current method was used as an auxiliary method in extracting the peregrine bodies. In pediatric patients, HFJV was applied with caution and with low jet ventilation pres-sure.
The issue of retracting the bronchoscope in hypoxemia dura-tion was resolved by the current approach, and the proce-dure was diverted. The whole procedure duration was mini-
Table 2. ABG changes after HFJV analysis using paired t-test
Arterial blood Before jet Post jet gas levels ventilation ventilation P
pH (mean±SD) 7.29±0.03 7.30±0.04 0.08
PaCO2 mmHg (kPa) 59.3±6.7 52.6±8.1 0.001 (mean±SD)
HCO3 (mmol/L)
PaO2 mmHg (kPa) 54.84 111.98 <0.001 (three digit enough)
PaO2/FiO2 ratio <300 ~575 <0.001
PaCO2 (kPa/mmHg)
NL 50.9±1.02 53.2±0.0 0.1 (ANOVA)
Overweight 49.1±8.6 52.3±12.1
Obese
ANOVA: analysis of variance; pH: power of hydrogen; PaO2: partial pressure of oxygen in the alveoli (mmHg); PaCO2: partial pressure of carbon dioxide in arterial blood (mmHg); Std. Deviation: standard deviation
Turk Thorac J 2018; 19(3): 127-31
130

mized, and the operator working field was not restricted. Our procedures were conducted using a flexible bronchoscope with a working channel diameter of 2.8 mm (Figure 4). We have applied this method in over 100 recent procedures; the reports and results of these procedures will be presented soon. No damages were observed in the bronchoscope with a working channel diameter of 2.8 mm. We also tried venti-lation using a bronchoscope with a 2 mm working channel. However, the use of a smaller working channel diameter (<2.8 mm) led to high airway pressure and limited the venti-lation. Thus, we do not recommend using HFJV through a working channel with <2.8 mm diameter. Jet ventilation was also ineffective in the working channel when there were too many secretions because this method blew the secretions into the airways and disturbed the ventilation method. Considering that the maximum time of tolerating the mini-mum saturation of oxygen was selected as the inclusion cri-teria in the current study, only 16 patients fulfilled the sug-gested index. A small study group in the current study may have affected our results. Further studies with higher sample sizes are required to offer enough data to confirm the effi-cacy of the current approach.
The use of HFJV in the working channel of a flexible bron-choscope is suggested to be an effective ventilation tech-nique. This method delivers an open field for intervention tools and provides adequate gas exchange without increas-ing the risk of barotrauma.
Ethics Committee Approval: Ethics committee approval was received for this study from the Ethics Committee of Shadid Behehti University of Medical Sciences (IR. SBMU. MSP. REC.1395.218).
Informed Consent: Written informed consent was obtained from all the patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - A.A., A.K.; Design - A.A., A.K., L.F., A.S., T.P.; Supervision - A.A., A.K.; Resource - A.A., A.K., M.P.T.; Materials - A.A., A.K., A.K.; Data Collection and/or Processing - A.A., A.K., K.T.; Analysis and/or Interpretation - A.A., B.F., M.P.T.; Literature Search - A.A., A.K., K.T.; Writing - A.A., A.K., K.T.; Critical Reviews - A.A., A.K., K.T., A.K., A.J.F., L.F., A.S., T.P., A.A., B.F., M.P.T.
Acknowledgements: The authors would like to thank all the hospital cooperators for their favor in conducting current study.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
1. Karapolat S. Leiomyoma: an unusual pleural tumor: letters to the editor (Leiomyoma: Nadir bir plevral tumor: Editore mektup). Turk Thorac J 2008;16:193-4.
2. Nezhad ZD, Farnia P, Sheikholslami FM, etal. Prevalence of non-tuberculosis mycobacteria in patients referring to myco-bacteriology research center of iran. Sci J Kurdistan Univ Med Sci 2014;19:31-9.
3. Nasiri MJ, Varahram M, Shams M, etal. Osteoarticular Tubercu-losis in Iran, 2002 to 2011. Advances in Research. 2014;2:509-14. [CrossRef]
4. Shokouhi S, Niyati R, Darazam I, et al. Resolution of Chest X-ray opacities in patients with ventilator-associated pneumonia. Infect Disord Drug Targets 2018;18:23-8. [CrossRef]
5. Fahimi F, Kobarfard F, Salamzadeh J, et al. The Bioavailability of Salbutamol in Urine via Volumatic and Nonvolumatic Valved Holding Chambers. World Allergy Organ J. 2011;4:179-83. [CrossRef]
6. Jamaati H, Kahkouee S, Farrokhpour M, etal . Endogenous lipoid pneumonia associated with rheumatoid arthritis, Tuberculosis and cytomegalovirus infection. Paripex. Indian Journal of Re-search 2017:6:1-9.
7. Malekmohammad M, Sharif-Kashani B, Monjazebi F, etal. Intermit-tent intravenous administration of Iloprost in patients with idiopathic pulmonary arterial hypertension. IJCA 2016;2:114-8. [CrossRef]
8. Saghebi S, Zangi M, Tajali T, et al. The role of T-tubes in the management of airway stenosis. Eur J Cardiothorac Surg 2012;43:934-9. [CrossRef]
9. Eslami-Behroozi M, Pazhoohan S, Aref E, et al. Bronchocon-striction Induces Structural and Functional Airway Alterations in Non-sensitized Rats. Lung 2017;195:167-71. [CrossRef]
10. Schneider M, Probst R. High frequency jet ventilation via a tracheoscope for endobronchial laser surgery. Can J Anaesth 1990;37:372-6. [CrossRef]
11. Veres J, Slavei K, Errhalt P, etal. The Veres adapter: clinical experience with a new device for jet ventilation via a laryn-geal mask airway during flexible bronchoscopy. Anesth Analg 2011;112:597-600. [CrossRef]
12. Fernandez-Bustamante A, Ibanez V, Alfaro JJ, et al. High-fre-quency jet ventilation in interventional bronchoscopy: factors with predictive value on high-frequency jet ventilation compli-cations. J Clin Anesth 2006;18:349-56. [CrossRef]
13. Fadaizadeh L, Hosseini MS. Laryngeal mask airway in interven-tional bronchoscopy for tracheal lesions. Acta Anaesthesiol Tai-wan 2013;51:137. [CrossRef]
14. Hashemian S, Jamaati H, Fakharian A, et al. 428: Non Invasive Ventilation in Acute Respiratory Failure of Myasthenia Gravis Tients J Crit Care Med 2013;41:103. [CrossRef]
15. Sadeghi S, Fakharian A, Nasri P, etal. Comparison of Comfort and Effectiveness of Total Face Mask and Oronasal Mask in Noninvasive Positive Pressure Ventilation in Patients with Acute Respiratory Failure: A Clinical Trial. Can Respir J 2017;2017:1-6. [CrossRef]
16. Fadaizadeh L, Hoseini MS, Bagheri M. Anaesthesia Manage-ment During Interventional Bronchoscopic Procedures: Laryn-geal Mask Airway or Rigid Bronchoscope. Turk J Anaesthesiol Reanim 2014;42:302-7. [CrossRef]
17. Bourgain JL, Desruennes E, Fischler M, etal. Transtracheal high frequency jet ventilation for endoscopic airway surgery: a mul-ticentre study. Br J Anaesth 2001;87:870-5. [CrossRef]
18. Aminde LN, Atem JA, Kengne AP, et al. Body mass index-mea-sured adiposity and population attributability of associated fac-tors: a population-based study from Buea, Cameroon. BMC Obes 2017; 4:1-11. [CrossRef]
19. Hautmann H, Gamarra F, Henke M, et al. High frequency jet ventilation in interventional fiberoptic bronchoscopy. Anesth Analg 2000;90:1436-40. [CrossRef]
20. Unzueta MC, Casas I, Merten A, et al. Endobronchial high-fre-quency jet ventilation for endobronchial laser surgery: an alter-native approach. Anesth Analg 2003;96:298-300. [CrossRef]
21. Ayuso MA, Luis M, Sala X, et al. Comparative study of high-frequency jet ventilation in 4 types of patients undergoing laryn-geal microsurgery. Rev Esp Anestesiol Reanim 1997;44:7-12.
Abedini et al. Bronchoscopy High-Frequency Jet Ventilation
131

INTRODUCTION
Tobacco smoking is a widely known hazard to human health. Doll and Hill’s milestone work on the health hazards of tobacco smoking in a huge pile of literature suggested its effects on morbidity and mortality, and developing countries share more burden [1]. As literature accrued on its hazardous effects, governments felt more responsible to restrict its use in the community. In 2003, another international achievement was accomplished. World Health Assembly accepted the Framework Convention on Tobacco Control (FCTC) by consensus [2]. This is a set of policy options developed to decrease the smoking rates and alleviate its health burden in the community.
Ministry of Health, Turkey, immediately signed the FCTC in 2004, and in the same year, the Grand National Assembly of Turkey accepted the convention [3]. The acceptance of FCTC in Turkey expanded the smoking ban and accelerated political action to lower the smoking cases in the community.
In Turkey, the first Global Adult Tobacco Survey (GATS) was conducted in 2008 and the second one was conducted in 2012. The law against tobacco products was passed in 1996 and was called the Legislation on the Prevention and Control of Harms of Tobacco Products No. 4207 (in short, Law no. 4207). It was amended in 2008 to be in line with FCTC. After a decrease in the smoking prevalence was observed in GATS 2012 (from 31.2% to 27.1%), the coverage of smoking ban was expanded in 2013. This latest amendment banned smoking for all drivers in all kinds of vehicles, including private cars [4].
Only observing the law violation rate is a method that has been used in the literature. There is another study that assessed the violation of Law no. 4207 in restaurants in Istanbul in the years 2013 and 2014 [5]. Previously, Öztürk et al. [6] published a study by observing taxis in Ankara and found the prevalence of law violation to be 1.3%. In Ireland, where all cars were observed, the violation prevalence was 1.4% [7]. To our knowledge, no studies have observed all drivers and violation rates in Turkey.
Address for Correspondence: Erdem Erkoyun, Department of Public Health, Dokuz Eylül University School of Medicine, İzmir, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
132
Turk Thorac J 2018; 19(3): 132-5
Original Article
Violation of the Tobacco Control Law by Drivers in Vehicles in Two Streets in İzmir: A Descriptive Study
DOI: 10.5152/TurkThoracJ.2018.17077
Erdem Erkoyun1, Mustafa Selahattin Alçiçek2, Simge Selek2
1Department of Public Health, Dokuz Eylül University School of Medicine, İzmir, Turkey2Medical Student, Dokuz Eylül University School of Medicine, İzmir, Turkey
Cite this article as: Erkoyun E, Alçiçek MS, Selek S. Violation of the Tobacco Control Law by Drivers in Vehicles in Two Streets in İzmir: A Descriptive Study. Turk Thorac J 2018; 19(3): 132-5.
OBJECTIVES: After signing and approving the Framework Convention on Tobacco Control (FCTC), Turkey amended laws on tobacco control in 2008 and also expanded the smoking ban in 2013 to include drivers in all vehicles. Four years later, this amendment does not seem as effective. The aim of this study was to observe violation of the law by the drivers and to analyze the association between gender of the driver, type of the vehicle, approximate age group definition of the passenger (either child or adult), and the law violation in two streets in Konak district, İzmir, Turkey.
MATERIALS AND METHODS: In this cross-sectional study, two observer teams were located in two different busy streets on the same afternoon and they collected data on the violation of the law, gender of the driver, approximate age group definition of the passengers (either adult or child), and type of the vehicle (special, taxi, or other commercial). Logistic regression for the violation of the law was conducted.
RESULTS: Law violation prevalence is 7.2%. In univariate analysis, the gender of the driver and having at least one child as a passenger were associated with the violation of the law. In multivariate analysis, not having children increases (OR: 8.4) the risk of the violation of the law.
CONCLUSION: The violation of the law was high, but the drivers seemed to be aware of the harms of smoking by looking at the in-creased risk of the violation in vehicles, in which no child was carried as passengers.
KEYWORDS: Tobacco smoking, smoking ban, violation of tobacco control law
Abstract
Received: 22.09.2017 Accepted: 20.03.2018

In Östergötland, Sweden, Johansson et al. [8] found that parenthood had an effect on the smoking behavior. Adults without children more commonly smoked inside the house than those with children.
The aim of this study was to determine the prevalence of violation of Law no. 4207 and to analyze the effect of the gender of the driver and having at least one child passenger or any other passenger in the car on the violation of this law in two streets in the Konak district of İzmir province.
MATERIALS AND METHODS
The violation of Law no. 4207 by the drivers was observed at two locations simultaneously in the Konak district of İzmir on a Thursday afternoon of August 10, 2017. İzmir is a highly urbanized city. It is the third largest city of Turkey and also has several heavy industrial facilities. The headquarters of the municipality and local government are located in the Konak district. The international harbor of the city is also located in Konak. Car traffic is usually busy on both weekdays and weekends. Two observation points were selected as appro-priate for monitoring the drivers’ actions in Konak. These streets were selected for the convenience of observers. These streets were Talatpaşa and İnönü. Both streets are busy during the day time. Two teams composed of five people each were located on the two streets. Two observers from each team observed the vehicles and dictated the features about the driver, vehicle, and the presence of a passenger. The other team members took notes on a structured sheet. All decisions were subjective and instant and were made by observer teams separately.
On the basis of GATS 2008 and 2012 results, smoking preva-lence was accepted as 30% among adults [9]. Then, at an incidental time, a chance to encounter a person smoking was thought to be 5%. Sample size was calculated with this prevalence and 1% deviation. With a 95% confidence level and 80% power, the minimum sample size was 1,822.
The dependent variable of this study was the violation of Law no. 4207. According to this law, smoking is prohibited for all the drivers. In taxis and other public vehicles, smoking is pro-hibited for the passengers and drivers. Therefore, the violation of the law was defined as either a driver smoking in the vehicle or at least one passenger smoking in a taxi or any other public vehicle.
The drivers’ gender, existence of a passenger in the vehicle, and the make of the vehicle were noted. The gender of any smoking passenger was recorded separately. The approxi-mate age group definition of the passengers was classified as either child or adult. Vehicles were classified as private cars, taxis, or other commercial vehicles. Other commercial groups composed of vehicles, other than taxis, that were in use for transporting goods or people.
Ethical board approval was not obtained for this study. The reason behind this idea was that the subject for this research was protected by a law, which is the highest regulation after the Constitution in Turkey. In a similar study in Ankara, researchers also did not have ethical approval [6]. A direct
contact with the participants was not possible because all the participants of this study were in vehicles. Informed consent was not been taken.
Statistical AnalysisThe percentages of variables were shown. The association between independent and dependent variables was analyzed using the chi-square test. Analysis with the logistic regression model was conducted with independent variables, which were found to be significantly associated with the dependent vari-able. A P value less than 0.05 was accepted as significant. Statistical analyses were performed using SPSS (Statistical Package for the Social Sciences) version 15.0 (SPSS Inc.; Chicago, IL, USA).
RESULTS
In this study, 1,189 drivers and vehicles were observed. Only 153 (12.9%) of all the drivers were female. Almost half of the vehicles had passengers (47.5%). In 101 vehicles, at least one of the passenger was thought to be a child. In total, 473 (39.8%) were commercial vehicles, and of these, 165 (13.9%) were taxis. Law no. 4027 had been violated in 86 vehicles (7.2%). Among all the observations, in eight vehicles (0.7%), the passenger and driver were found to be smoking (Table 1).
In the chi-square analysis, the existence of at least one pas-senger in the vehicle (p=0.275) and classification of the vehicle (p=0.16) were not found to be associated with the violation of Law no. 4207. Male drivers (p=0.043) and driv-ers who did not have at least one child as a passenger (p=0.011) were found to be associated with the violation of the Law no. 4207 (Table 1).
Male drivers violated the law 2.4 times [95% confidence interval (CI), 1.0-6.2] more than female drivers when adjust-ed for having at least one child as a passenger but this asso-ciation was not significant. Not having at least one child passenger was significantly associated with an 8.4 times increased risk of the law violation relative to the existence of a child in the car (95% CI, 1.2-60.9) (Table 2).
DISCUSSION
This cross-sectional observational study shows that the viola-tion of Law no. 4207 prevalence is high and not having at least a child passenger in the vehicle significantly increases risk of law violation. This association persists after adjusting for the gender of the driver, which suggests that drivers are sensitive to the health of the children they have as passen-gers. This may also suggest that some smokers acknowledge the harms of cigarette smoking, but they endanger their health when they do not have children as passengers.
Tobacco smoking is a highly addictive behavior, and the tobacco industry plays a critical and powerful role to keep the revenue high [10,11]. In 2008, all political parties in the Grand National Assembly supported the expansion of the smoking ban [4]. The support for the comprehensive bans was 95.5% in GATS 2012 in all participants and 86.9% in smokers. After the latest amendment about smoking ban, which has been published in the Official Journal mass media, by looking at the results of this study, we can say that the clause that bans
Erkoyun et al. Violation of Tobacco Law by Drivers in İzmir
133

smoking in the driver’s place does not have practical implica-tions. There may be a divergence between the rhetoric and behavior in the community. This may also be the result of a quantitative study design where the participant may make claims about the intention of the interviewer.
A study in Ankara found a lower prevalence of the law viola-tion [9]. They focused only on commercial taxis. According to their findings, the presence of a child is not protective against smoking in taxis. Smoking ban in taxis is an older regulation than smoking ban for all drivers. Maybe the regulation for taxis has been acknowledged more widely by the community. Smoking prevalence in Ireland is quite low compared with the observation of our study (1.4%), although the study was con-ducted before smoking was banned in vehicles for drivers.
In a commentary, Elbek et al. [4] suggested that ministries other than the Ministry of Health did not meet their legal liabilities about the law. Prior to 1996, in Turkey, traveling by commercial bus lines was hard because of commuter smok-
ing in the buses. After the first ban came into agenda, the public generally acknowledged the rule of law. There may be some ways to increase obedience to this latest regulation. The results of this study may be used to choose target popula-tions for health promotion.
All of our observations are based on the subjective decisions of observers, where decisions were made on an individual basis. We did not conduct a pre-trial consistency analysis between the two teams on the same street simultaneously. A bias caused by inconsistency is not likely because the teams observed a restricted and definite set of variables. Children older than 15 years may have been misclassified as adults. The estimated minimum sample size was not reached. This may explain the higher prevalence of violation than expect-ed. Among all these limitations, this study has some strengths. All observations were made during the day time. Missing a smoking driver or passenger was not likely. Also, people who acted as observers and those who collected data were differ-ent. The positions that were chosen for observation were convenient for observation. We did not calculate missing vehicles, but we claim that their rate is low.
In conclusion, the law violation prevalence was found to be high on the two busy streets in Konak, and not having chil-dren as a passenger in the vehicle was found to be associated with the violation of law in the vehicles. The adverse effects of second-hand smoking on children can be considered to reach target audience.
Ethics Committee Approval: N/A
Informed Consent: N/A
Peer-review: Externally peer-reviewed.
Author contributions: Concept - E.E., M.S.A., S.S..; Design - E.E., M.S.A., S.S.; Supervision - E.E.; Resource - M.S.A., S.S.; Materials - M.S.A., S.S.; Data Collection and/or Processing - E.E., M.S.A., S.S.; Analysis and/or Interpretation - E.E.; Literature Search - E.E.; Writing - E.E., M.S.A., S.S.; Critical Reviews - E.E., M.S.A., S.S.
Acknowledgements: We would like to thank to our fellows for their contribution on study design, data collection and analysis; namely Sümeyye Tereci, Selen Toy, Halil Said Kaçmaz, Fatma Karakoç, Büşra Nur Bacık Göksu , Fevzi Kolay, Talha Özüdoğru, Enes Gidirişlioğlu (sixth grade medical students) and Hasan Koç (MD, resident of pub-lic health).
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
1. Ezzati M, Lopez AD. Measuring the accumulated hazards of smoking: global and regional estimates for 2000. Tob Control 2003 Mar;12:79-85.
2. Roemer R, Taylor A, Lariviere J. Origins of the WHO Frame-work Convention on Tobacco Control. Am J Public Health 2005;95:936-8. [CrossRef]
3. Bilir N. Level of Tobacco Control in Turkey (Türkiye tütün kon-trolünde dünyanın neresinde?). Turk Thorac J 2009;10:31-4.
Table 1. Characteristics of the driver, passenger, and vehicle and their association with violation of law
Violation
Yes No Total
Characteristic n % n % n %
Driver
Gender
Male 81 7.8 955 92.2 1.036 100.0
Female 5 3.3 148 96.7 153 100.0
Chi-square=4.114, p=0.043
Chi-square=0.659, p=0.719
Having passenger
Absent 50 8.0 574 92.0 624 100.0
Present 36 6.4 529 93.6 565 100.0
Chi-square=1.190, p=0.175
Having child passenger
Absent 85 7.8 1.003 92.2 1.088 100.0
Present 1 1.0 100 99.0 101 100.0
Chi-square=6.411, p=0.011
Vehicle classification
Special 44 6.1 672 93.9 716 100.0
Taxi 13 7.9 152 92.1 165 100.0
Other 29 9.4 279 90.6 308 100.0 commercial
Chi-square=3.552, p=0.160
Table 2. Logistic regression of violation of Law no. 4207
Variable B p OR (95% CI)
Male (ref*: Female) 0.909 0.053 2.5 (1.0-6.2)
Not having child passenger 2.126 0.036 8.4 (1.2-60.9) (ref*: presence)
*: category
Turk Thorac J 2018; 19(3): 132-5
134

4. Elbek O, Kılınç O, Ayfer Aytemur Z, et al. Tobacco Control in Turkey. Turk Thorac J 2015;16,141-50.
5. Ay P, Evrengil E, Guner M, et al. Noncompliance to smoke-free law: which hospitality premises are more prone? Public Health 2016;141:1-6.
6. Öztürk B, Kosku H, Guven İ, et al. A Study Examining Compli-ance with the Anti-Tobacco Law Nb. 4207 Inside Taxis. Turk Thorac J 2017;18:88-93.
7. Gilroy I, Donnelly N, Matthews W, et al. Smoking in vehicles is lower than mobile telephone use while driving, but is socially patterned. Ir Med J 2013;106:118-20.
8. Johansson A, Halling A, Hermansson G, et al. Assessment of Smoking Behaviors in the Home and Their Influence on Chil-dren's Passive Smoking: Development of a Questionnaire. Ann Epidemiol 2005;15:453-9. [CrossRef]
9. Public Health Institution of Turkey. Global Adult Tobacco Sur-vey Turkey 2012. Int: 2014. Report No: 948.
10. Hatsukami DK, Stead LF, Gupta PC. Tobacco addiction. Lancet 2008;371:2027-38. [CrossRef]
11. Lee S, Ling PM, Glantz SA. The vector of the tobacco epidemic: tobacco industry practices in low and middle-income countries. Cancer Causes Control 2012;23:117-29. [CrossRef]
Erkoyun et al. Violation of Tobacco Law by Drivers in İzmir
135

INTRODUCTION
Obstructive sleep apnea (OSA) is a chronic disorder characterized by repeated upper-airway collapse during sleep, result-ing in intermittent hypoxia, fragmented sleep, fluctuations in blood pressure, and increased sympathetic nervous system activity [1]. In the early 1990s in the USA, population studies found OSA-defined by an apnea-hypopnea index (AHI) higher than five events per hour-in 9% of women and 24% of men, respectively [2]. Later reports demonstrated an increased prevalence (17% of middle-aged women and 34% of men), which was primarily attributed to increased body mass index (BMI) in general populations over the last decades [3]. Remarkably, on the basis of the recent hypopnea definitions of the American Academy of Sleep Medicine (AASM) [4], the largest European epidemiologic study to date (the HypnoLaus Study) showed that 61% of women and 84% of men had OSA based on the polysomnographic AHI cut-off level of five events/h in an unselected general cohort of 2121 adults [5]. The authors concluded that the prevalence of OSA was highly dependent on technical procedures, that is, nasal cannulas recording more subtle breathing variations as hypopneas as well as applying the latest hypopnea definitions, which are more liberal compared with the earlier ones (3% desaturations instead of 4% desaturations, and/or arousals). To date, there is no data regarding the prevalence of OSA in Turkey based on sleep recordings. However, the largest questionnaire-based Turkish Adult Population Epidemiology of Sleep (TAPES) study [6], including a nationwide representative sample of 5021 participants, suggested the prevalence of OSA at 13.7% on the basis of the Berlin questionnaire [7], and excessive daytime sleepiness (EDS) 5.4% on the basis of the Epworth Sleepiness Scale (ESS) [8].
Accumulated research data suggest that OSA with concomitant EDS is associated with neurocognitive dysfunction and reduced quality of life [9] as well as with increased risk for traffic accidents [10]. It may also lead to cardiovascular dis-eases (CVD) including systemic hypertension, coronary artery disease (CAD), cardiac failure, arrhythmias, and stroke [11,12]. The first choice of treatment for OSA is positive airway pressure (PAP), which is efficient in reducing EDS and
Address for Correspondence: Yüksel Peker, Department of Pulmonary Medicine, Marmara University School of Medicine, Pendik Training and Research Hospital, Sleep Medicine Center, İstanbul, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
136
Turk Thorac J 2018; 19(3): 136-40
Original Article
Rationale and Design of the Turkish Sleep Apnea Database - TURKAPNE: A National, Multicenter, Observational, Prospective Cohort Study
DOI: 10.5152/TurkThoracJ.2018.18097
Yüksel Peker1,2,3 , Özen K. Başoğlu4 , Hikmet Fırat5 , and the TURKAPNE Study Group*1Department of Pulmonary Medicine, Marmara University School of Medicine, İstanbul, Turkey2Department of Clinical Sciences, Respiratory Medicine and Allergology, Faculty of Medicine, Lund University, Lund, Sweden3Division of Pulmonary, Allergy, and Critical Care Medicine, University of Pittsburgh School of Medicine, Pittsburgh, PA, USA4Department of Pulmonary Medicine, Ege University School of Medicine, İzmir, Turkey5Clinic of Chest Diseases and Sleep Center, Dışkapı Yıldırım Beyazıt Training and Research Hospital, Ankara, Turkey
Cite this article as: Peker Y, Başoğlu ÖK, Fırat H, TURKAPNE Study Group. Rationale and Design of the Turkish Sleep Apnea Database - TURKAPNE: A National, Multicenter, Observational, Prospective Cohort Study. Turk Thorac J 2018; 19(3): 136-40.
OBJECTIVES: The primary aim of The Turkish Sleep Apnea Database (TURKAPNE) study is to generate a cross-sectional nationwide database for defining the clinical and polysomnographic characteristics of the patients with obstructive sleep apnea (OSA) in Turkey.
MATERIALS AND METHODS: In this ongoing project, all consecutive adults with suspected OSA are recruited from the sleep centers of the university and research hospitals in Turkey. Information on anthropometric data, educational status, driving license, smoking habits, alcohol use, comorbidities, drug use, questionnaires, polysomnographic, and/or cardiorespiratory polygraphic findings are recorded in a systematized Web-based report form. Blood glucose, lipids and other biochemical markers, lung function, and echocardiography measurements are optionally included. Follow-up data regarding treatment modality and compliance is assessed. Cross-sectional and longitudinal associations between OSA phenotypes and metabolic, pulmonary, and cardiovascular comorbidities as well as traffic ac-cidents, and the impact of treatment will be further explored. We target a total sample of 10,000 participants.
RESULTS: The study was registered with ClinicalTrials.gov (NCT02784977) in May 2016 and the first patient was recruited in October 2017. A total of 1911 participants from 19 centers have been enrolled in the study by May 31, 2018.
CONCLUSION: The TURKAPNE study will contribute to a better understanding of the health-related burden of OSA phenotypes and its association with the comorbidities and adverse outcomes, including traffic accidents in Turkey. The results may also contribute to a more personalized approach and better management of varying OSA phenotypes with concomitant disorders.
KEYWORDS: Obstructive sleep apnea, clinical registry, quality of care
Abstract
Received: 10.06.2018 Accepted: 02.07.2018

improving the quality of life [9]. However, as the majority of the patients with CVD do not report EDS, adherence to PAP treatment in the recent randomized controlled trials has been challenging [13,14]. Clinical phenotypes of OSA have been demonstrated to differ on the basis of anatomical [15] or physiological [16] features or a mixture of both [17]. The degree of EDS, gender differences in the presentation of symptoms, and comorbid conditions may considerably vary [18]. Moreover, among individuals who otherwise had nor-mal total AHI values [19], OSA during rapid eye movement (REM) sleep has been shown to be associated with hyperten-sion, indicating that this subgroup of patients deserves atten-tion with regard to CVD outcomes [20].
With the identification of OSA as a health burden, there has been a continuous increase in the referrals to sleep centers worldwide, and numerous clinical and research protocols have been initiated to better understand the outcomes of the diagnostic and treatment procedures for the patients with OSA. In this context, the European Sleep Apnea Database (ESADA) is the largest ongoing project to date that has already recruited an enormous cohort of patients referred to sleep centers in Europe [21] for the evaluation of suspected OSA, and several reports have been published for cross-sec-tional and longitudinal associations of OSA with different clinical phenotypes and comorbidities [18,22-28]. The majority of the patients in the ESADA cohort were diagnosed with home sleep testing (cardiorespiratory polygraphy), and it has been emphasized that as compared with patients inves-tigated using polysomnography [26], the individuals investi-gated using polygraphy are likely to have a 30% lower AHI on average.
In Turkey, the clinical management and initiation of treat-ment of the patients with OSA rely on in-hospital polysom-nography investigations, but not much is known regarding the cross-sectional and longitudinal outcomes of the patients with OSA nationwide. One single-center, retro-spective study has demonstrated gender differences in symptoms and polysomnographic features of the patients with OSA [29], and two single-center studies prospectively addressed the compliance with PAP treatment [30,31]. However, to date, there has been a lack of collaborative national network for answering the challenging research questions regarding the OSA phenotypes and metabolic and CVD outcomes as well as traffic accidents and the impact of treatment.
ObjectivesThe main aim of the The Turkish Sleep Apnea Database (TURKAPNE) study is to generate a cross-sectional nation-wide database for defining clinical and polysomnographic characteristics of the patients with OSA in Turkey. The pri-mary outcomes will be the prevalence and incidence of metabolic, pulmonary, and CVD in OSA phenotypes. The association of the OSA severity indices such as AHI and oxygen desaturation index (ODI) during REM sleep and non-REM sleep with diabetes mellitus and CVD will be explored. Secondary outcomes will include gender differences in clini-cal symptoms, comorbidities, and polysomnographic fea-tures as well as association with traffic accidents. Moreover,
adherence to PAP treatment will be evaluated. The incidence of CVD and mortality will be further addressed as long-term outcomes.
MATERIALS AND METHODS
The Study DesignThe TURKAPNE study is a national, multicenter, observa-tional, prospective cohort study, which was initiated in October 2017. The study duration for the primary outcomes is estimated to be 3 years for the first results with goal to include at least 10,000 participants during a total follow-up period of at least 10 years for all secondary outcomes. Additional subprotocols will be developed when necessary, especially in collaboration with national researchers within the other disease groups associated with OSA.
The Study PopulationThe inclusion and exclusion criteria are shown in Table 1, and the study protocol is outlined in Figure 1. All patients are recruited from the sleep centers of the university and research hospitals in Turkey. For acquiring full cross-sectional sample, patients are included irrespective of concomitant medication and degree of sleepiness as well as comorbidity, except the conditions summarized in the exclusion criteria. Information on anthropometric data, educational status, driv-ing license, smoking habits, alcohol use, comorbidities, drug use, questionnaires, polysomnographic, and/or cardiorespi-ratory polygraphic findings are recorded in a systematized web-based report form. For supervising the data collection and analysis and for resolving any practical issues associated with the study, a scientific core committee was formed (YP, OKB, HF), and additionally, different joint scientific working-groups comprising representatives from the different partici-pating centers are being formed for coordinating and direct-
Figure 1. Outline of the Turkish Sleep Apnea Database (TURKAPNE) study protocolOSA: obstructive sleep apnea; PAP: positive airway pressure
Patients referred to sleep centre with suspected OSA from October 2017
Sleep study conducted
No OSA
No treatment
Treatment T0Outcome Follow-up 1Outcome Follow-up 2,3...
Weight reduction
Intraoral device
Surgery PAP treatment
OSA
ExcludedIf no need for sleep study
Peker et al. The Turkish Sleep Apnea Database
137

ing all scientific issues associated with the ongoing protocols for the primary and secondary outcomes.
Ethical ConsiderationsPatients with suspected OSA who are referred to the partici-pating sleep centers are invited to participate in the study. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the Ethics Committee of the Medical Faculty of the Marmara University, Istanbul (approval nr: 09.2016.311). All patients provided written informed consent. The study was registered with the ClinicalTrials.gov (NCT02784977).
Data Collection and Data Quality AssuranceThe TURKAPNE project uses a specifically designed web-based data collection system constructed for transferring data to the central database www.turkapne.org at a server hosted by Hetzner Online GmbH localized in Jestetten, Germany. Each center is provided with a personal login to a clinical report format (CRF) module containing seven predefined submodules for recording data. Each sleep center has com-
plete access to stored data on its own participants. The regis-try of the participants is coded and the identity of the patients is kept at the reporting sleep center and secured with a writ-ten participant identity log. A detailed protocol describing the methods for data sampling, calculation, and reporting has been distributed to all participating sleep centers. Data quality and completeness will be randomly checked by an independent study monitor with full access to the complete database. The TURKAPNE web report format will be open for new and specific CRF modules for specific sub-studies for specific patient groups, such as diabetes mellitus, pulmonary diseases, CVDs, and neurological disorders as well as for health economy evaluations that may be introduced by the participating sleep centers within the TURKAPNE network.
Database
Anthropometric data, comorbidities, and concomitant medicationMandatory variables for each entry include information on age at diagnosis, sex, marital and educational status, driving license, smoking and alcohol habits, height, weight, circum-ference of the neck, waist and hip, heart rate, and systolic and diastolic blood pressure, and menstrual/menopausal status in women. A medical history including comorbidities as well as information on all ongoing medications is assessed. If taken, blood tests including blood glucose, lipids and other biochemical markers as well as lung function tests and echocardiography measurements are optionally includ-ed. Other biomarkers of interest, if already taken, can be optionally entered.
Questionnaires, excessive daytime sleepinessMarital status, educational status, information on driving license, estimated driving distance (km/yr), accident history during the last three years, smoking habits, and alcohol use
Table 1. Eligibility criteria for the Turkish Sleep Apnea Database (TURKAPNE) study
Inclusion criteria
Consecutive adult patients undergoing sleep study for suspicion of obstructive sleep apnea Ability to read and speak
Signed informed consent
Exclusion criteria
Subjects who use positive airway pressure
Subjects with limited life expectancy due to advanced renal disease or uncontrolled malignancies Subjects with alcohol dependency
Figure 2. JDistribution of the enrolled cases per participating center as on May 31, 2018
Dicle U
nivers
ity, D
iyarb
akır
2402302202102001901801701601501401301201101009080706050403020100
Namık
Kemal
Univers
ity, T
ekird
ağ
Bezmial
em V
akif
Univers
ity, İ
stanb
ul
Pamuk
kale
Univers
ity, D
enizl
i
Ege U
nivers
ity, İ
zmir
Sürey
yapa
şa H
ospit
al, İs
tanbu
l
Balıke
sir U
nivers
ity, B
alıke
sir
Osman
gazi
Univers
ity, E
skişe
hir
Atatür
k Univ
ersity
, Erzu
rum
Afyon
Kocate
pe U
nivers
ity, A
fyon
Adana
Baş
kent
Univers
ity, A
dana
İstan
bul B
aşke
nt Univ
ersity
, İsta
nbul
Uludağ
Univ
ersity
, Bur
sa
Dışkap
ı Yıld
ırım B
eyaz
ıt Hos
pital,
Ank
ara
Derinc
e Hos
pital,
Koc
aeli
Acıbad
em U
nivers
ity, A
taken
t Hos
pital,
İstan
bul
Dokuz
Eylül
Univ
ersity
, İzm
ir
İstanb
ul Univ
ersity,
Cerr
ahpa
şa M
edica
l Sch
ool, İ
stanb
ul
Marm
ara U
nivers
ity, D
ept. o
f Pulm
onolo
gy M
ed., İ
stanb
ul
Turk Thorac J 2018; 19(3): 136-40
138

are included in the modules. Self-reported sleep latency and sleep duration as well as the ESS questionnaire containing eight questions for addressing the chance of dozing-off under eight different scenarios in the past month [8] are also included. For further evaluating and validating the OSA phe-notypes in the Turkish sleep clinic cohorts, a more detailed questionnaire containing 16 questions related to symptoms associated with OSA with rating scores 1 (never), 2 (some-times), 3 (often), 4 (very often) is optionally added. The data-base will be expanded for other already validated specific questionnaires when necessary.
Polygraphic and polysomnographic findingsIn cases with diagnostic cardiorespiratory polygraphy data, information regarding the number of channels used, esti-mated sleep time, AHI, ODI (3%), average and minimum oxygen saturation time spent on supine position, and supine-AHI are documented. In clinical routines and as presently required by the Turkish Ministry of Labor and Social Security, an overnight polysomnography is obligatory when a PAP device is prescribed. Polysomnography data contain total sleep time, wake after sleep onset, sleep efficiency, sleep latency, REM latency, sleep stages, arousal index, periodic limb movement index, and AHI, ODI (3%), average and minimum oxygen saturation levels, time spent below 90% oxygen saturation, and heart rate as well as the distribution of the respiratory indices during supine/non-supine position and during the REM and non-REM sleep stages. Sleep stages as well as respiratory parameters are scored in accordance with the criteria of the AASM from 2012 [4]; apnea was defined as a reduction in airflow of at least 90% for at least 10 s, and hypopnea was defined as a reduction in airflow of at least 30% accompanied by at least a 3% desaturation in the preceding 30 s, and a reduction in chest wall movement and/or arousal. AHI is referred to as the average number of apneas and hypopneas per hour of sleep, and OSA is defined as an AHI of at least five events/h, and the severity of OSA is categorized as mild (AHI 5.0–14.9 events/h), moderate (AHI 15.0–29.9 events/h), or severe (AHI 30.0 events/h). Before the analysis of the primary and secondary outcomes, sepa-rate definitions of clusters and phenotypes will be carried out accordingly by the TURKAPNE scientific working-groups.
Follow-up data regarding treatment modality and complianceIn cases with PAP treatment, the values at the PAP-titration night, PAP modality (i.e., fixed PAP, automatic PAP, bi-level PAP, adaptive servoventilator), and the applied pressure levels will be documented. Compliance data will be downloaded from the devices at follow-ups in accordance with each sleep center’s clinical routines.
Statistical AnalysisStandard statistical analysis will be performed using the IBM Statistical Package for the Social Sciences version 22.0 for Windows software (IBM SPSS Corp.; Armonk, NY, USA). For comparison between multiple groups, one-way analysis of variance will be applied for continuous variables and Pearson Chi-square test will be performed for percentages. For com-parison between subgroups, posthoc Bonferroni analysis will be performed where equal variances are found, and Games
Howell analysis will be used where there is no equal variance. Regression analysis will be used for determining the relation-ship between OSA phenotypes and the outcome variables. All odds ratios will be presented with their 95% confidence inter-vals. All statistical tests will be two-sided, and p-values less than 0.05 will be considered statistically significant. Specific power estimates will be performed for each protocol before data analysis and the publication of the results.
RESULTS
The first patient was recruited in October 2017. A total of 25 sleep centers are presently registered as participating centers, of which 19 have actively entered a minimum of 30 patients by May 31, 2018 as required for the present paper; 1911 patients were entered into the database by May 31, 2018. The distribution of the enrolled cases per participating center is illustrated in Figure 2.
DISCUSSION
Obstructive sleep apnea is a frequently occurring condition with serious adverse outcomes, and the management of these high-risk individuals is presently not optimal either globally or in Turkey. The primary aim of the TURKAPNE study is to generate a cross-sectional nationwide database for defining clinical and polysomnographic characteristics of the patients with OSA. When completed, the project will con-tribute to a better understanding of the health burden of OSA phenotypes and its association with the comorbidities and adverse outcomes, including traffic accidents in Turkey. The results may also contribute to a more personalized approach and better management of varying OSA phenotypes with concomitant disorders.
*TURKAPNE Study Group
Ahmet Ursavaş, Aylin Özsancak Uğurlu , Baran Balcan , Buğra Kerget , Demet İlhan Algın , Derya Karadeniz , Dursun Dursunoğlu , Ersin Günay , Fuat Erel , Gökhan Kırbaş , Gülçin Benbir Şenel , Gülgün Çetintaş Afşar , Gülin Melikoğlu, Hadice Selimoğlu Şen , Hamza Ogun , İbrahim Öztura , Mehmet Ali Habesoğlu , Mehmet Karadağ, Mehmet Sezai Taşbakan , Melike Banu Yüceege , Metin Akgün , Muhammed Emin Akkoyunlu , Murat Aksu, Nejat Altıntaş , Neşe Dursunoğlu , Nurhan Sarıoğlu , Oğuz Osman Erdinç , Oya İtil, Özgür Bilgin Topçuoğlu , Pınar Bekdik Şirinocak , Sema Saraç , Sevgi Ferik , Sibel Pekcan, Süreyya Yılmaz , Yıldız Kaya , Zahide Yılmaz
Ethics Committee Approval: Ethics committee approval was re-ceived for this study from the ethics committee of Medical Faculty of the Marmara University, İstanbul (approval no: 09.2016.311).
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Conception – Y.P., O.K.B., H.F.; Design - Y.P., O.K.B., H.F.; Supervision – Y.P; Funding – Y.P., O.K.B., H.F.; Materials
Peker et al. The Turkish Sleep Apnea Database
139

– Y.P., O.K.B., H.F., T.S.G.; Data Collection and/or Processing – Y.P., O.K.B., H.F., T.S.G.; Analysis and/or Interpretation - Y.P., O.K.B., H.F.; Literature Review - Y.P., O.K.B.; Writer – Y.P.; Critical Review - Y.P., O.K.B., H.F., T.S.G.
Acknowledgements: The authors thank Ömer Şeker and Onur Sönmez from the MedTurca Company for the formation, infrastruc-ture, and technical support of the TURKAPNE database, and The Turkish Thoracic Society for sponsoring the initial phase of the proj-ect.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The foundation and infrastructure of the data-base was supported by grants from the Turkish Thoracic Society with no influence on the design of the study, the analysis of the data, the data collection, drafting of the manuscript, or the decision to pub-lish.
REFERENCES
1. Young T, Palta M, Dempsey J, et al. Burden of sleep apnea: ratio-nale, design, and major findings of the Wisconsin Sleep Cohort study. WMJ 2009;108:246-9.
2. Young T, Palta M, Dempsey J, et al. The occurrence of sleep-disordered breathing among middle-aged adults. New England J Med 1993;328:1230-5. [CrossRef]
3. Peppard PE, Young T, Barnet JH, et al. Increased prevalence of sleep- disordered breathing in adults. Am J Epidemiol 2013;177:1006-14. [CrossRef]
4. Berry RB, Budhiraja R, Gottlieb DJ, et al. Rules for scoring re-spiratory events in sleep: update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the Sleep Apnea Definitions Task Force of the American Academy of Sleep Medicine. J Clin Sleep Med 2012;8:597-619.
5. Heinzer R, Vat S, Marques-Vidal P, et al. Prevalence of sleep-disordered breathing in the general population: the HypnoLaus study. Lancet Respir Med 2015;3:310-8. [CrossRef]
6. Demir A, Ardic S, Firat H, et al. Prevalence of sleep disorders in the Turkish adult population epidemiology of sleep study. Sleep and Biological Rhythms 2015;13:298-308. [CrossRef]
7. Netzer NC, Stoohs RA, Netzer CM, et al. Using the Berlin Ques-tionnaire to identify patients at risk for the sleep apnea syn-drome. Ann Intern Med 1999;131:485-91. [CrossRef]
8. Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep 1991;14:540-5. [CrossRef]
9. Engleman HM, Martin SE, Kingshott RN, et al. Randomised placebo controlled trial of daytime function after continuous positive airway pressure (CPAP) therapy for the sleep apnoea/hypopnoea syndrome. Thorax 1998;53:341-5. [CrossRef]
10. McNicholas WT, Rodenstein D. Sleep apnoea and driving risk: the need for regulation. Eur Respir Rev 2015;24:602-6. [CrossRef]
11. Javaheri S, Barbe F, Campos-Rodriguez F, et al. Sleep Apnea: Types, Mechanisms, and Clinical Cardiovascular Consequenc-es. J Am Coll Cardiol 2017;69:841-58. [CrossRef]
12. Celen YT, Peker Y. Cardiovascular consequences of sleep ap-nea: I -epidemiology. Anadolu Kardiyol Derg 2010;10:75-80. [CrossRef]
13. Peker Y, Glantz H, Eulenburg C, et al. Effect of Positive Airway Pressure on Cardiovascular Outcomes in Coronary Artery Dis-ease Patients with Nonsleepy Obstructive Sleep Apnea. The RICCADSA Randomized Controlled Trial. Am J Respir Crit Care Med 2016;194:613-20. [CrossRef]
14. McEvoy RD, Antic NA, Heeley E, et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. New Engl J Med 2016;375:919-31. [CrossRef]
15. Lee RW, Sutherland K, Chan AS, et al. Relationship between surface facial dimensions and upper airway structures in ob-structive sleep apnea. Sleep 2010;33:1249-54. [CrossRef]
16. Eckert DJ, White DP, Jordan AS, et al. Defining phenotypic causes of obstructive sleep apnea. Identification of novel thera-peutic targets. Am J Respir Crit Care Med 2013;188:996-1004. [CrossRef]
17. Owens RL, Edwards BA, Eckert DJ, et al. An integrative model of physiological traits can be used to predict obstructive sleep apnea and response to non positive airway pressure therapy. Sleep 2015;38:961-70. [CrossRef]
18. Saaresranta T, Hedner J, Bonsignore MR, et al. Clinical Pheno-types and Comorbidity in European Sleep Apnoea Patients. PloS One 2016;11:e0163439. [CrossRef]
19. Mokhlesi B, Finn LA, Hagen EW, et al. Obstructive sleep apnea during REM sleep and hypertension. results of the Wisconsin Sleep Cohort. Am J Respir Crit Care Med 2014;190:1158-67. [CrossRef]
20. Peker Y. REM sleep: a nightmare for patients with obstructive sleep apnea? Am J Respir Crit Care Med 2014;190:1088-90. [CrossRef]
21. Hedner J, Grote L, Bonsignore M, et al. The European Sleep Ap-noea Database (ESADA): report from 22 European sleep labora-tories. Eur Respir J 2011;38:635-42. [CrossRef]
22. Kent BD, Grote L, Bonsignore MR, et al. Sleep apnoea sever-ity independently predicts glycaemic health in nondiabetic subjects: the ESADA study. European Respir J 2014;44:130-9. [CrossRef]
23. Kent BD, Grote L, Ryan S, et al. Diabetes mellitus prevalence and control in sleep-disordered breathing: the European Sleep Apnea Cohort (ESADA) study. Chest 2014;146:982-90. [CrossRef]
24. Karimi M, Hedner J, Lombardi C, et al. Driving habits and risk factors for traffic accidents among sleep apnea patients--a Eu-ropean multi-centre cohort study. J Sleep Res 2014;23:689-99. [CrossRef]
25. Tkacova R, McNicholas WT, Javorsky M, et al. Nocturnal inter-mittent hypoxia predicts prevalent hypertension in the European Sleep Apnoea Database cohort study. Eur Respir J 2014;44:931-41. [CrossRef]
26. Escourrou P, Grote L, Penzel T, et al. The diagnostic method has a strong influence on classification of obstructive sleep apnea. J Sleep Res 2015;24:730-8. [CrossRef]
27. Marrone O, Battaglia S, Steiropoulos P, et al. Chronic kidney disease in European patients with obstructive sleep apnea: the ESADA cohort study. J Sleep Res 2016;25:739-45. [CrossRef]
28. Basoglu OK, Zou D, Tasbakan MS, et al. Change in weight and central obesity by positive airway pressure treatment in obstruc-tive sleep apnea patients: longitudinal data from the ESADA co-hort. J Sleep Res 2018:e12705. [CrossRef]
29. Basoglu OK, Tasbakan MS. Gender differences in clinical and polysomnographic features of obstructive sleep apnea: a clinical study of 2827 patients. Sleep Breath 2018;22:241-9. [CrossRef]
30. Salepci B, Caglayan B, Kiral N, et al. CPAP adherence of patients with obstructive sleep apnea. Respir Care 2013;58:1467-73. [CrossRef]
31. Sarac S, Afsar GC, Oruc O, et al. Impact of Patient Education on Compliance with Positive Airway Pressure Treatment in Obstructive Sleep Apnea. Med Sci Monit 2017;23:1792-9. [CrossRef]
Turk Thorac J 2018; 19(3): 136-40
140

Turk Thorac J 2018; 19(3): 141-9
Review
Bronchoscopic Lung Volume Reduction: A 2018 Review and Update
INTRODUCTION
Chronic obstructive pulmonary disease (COPD) is characterized by irreversible airway obstruction with persistent respira-tory symptoms and is a relatively treatable disease. Emphysema is one of the most common chronic and progressive conditions associated with COPD. Pathophysiologically, it includes the destruction of the lung parenchyma via chronic inflammation, followed by the permanent enlargement of the terminal bronchioles, dynamic hyperinflation, and loss of elastic recoil, air trapping, and reduced exercise capacity [1]. In addition, there is an increase in residual volume (RV) due to thoracic compression and dysfunction of the respiratory muscles in patients with COPD [2]. Smoking is still the most common cause, and dust exposure and alpha-1 antitrypsin deficiency are also known to be associated with its pathogenesis [3].
At present, standard treatment options include smoking cessation, bronchodilation, mucolytic agents, phosphodiesterase 4 inhibitors, respiratory rehabilitation, and nutritional support, vaccination against influenza and pneumococcus, and long-term oxygen therapy [4]. These treatments help to increase the exercise capacity of patients and decrease symptom exacerbation. However, they do not cure the pathophysiology of the disease or prevent disease progression. In the last decade, in addition to lung volume reduction surgeries (LVRSs), bronchoscopic lung volume reduction (BLVR) has expanded the treatment spectrum of patients with end-stage emphysema [5,6]. These treatments include valve, coil, thermal vapor ablation (TVA), bio-lung volume reduction (BioLVR), targeted lung denervation (TLD), and airway bypass stent (ABS).
Lung volume reduction surgeries is based on the principle of resecting damaged lung parenchyma and reducing hyper-inflation in selected patients with heterogeneous emphysema with upper lobe predominance. Patients are often selected for surgery in accordance with the National Emphysema Treatment Trial (NETT) criteria [5]. Patients with hypercapnic respiratory failure, which is defined as an arterial partial pressure of carbon dioxide (PaCO2) >60 mmHg, and oxygen therapy requirement during rest are not recommended for surgery. LVRS can reportedly improve exercise capacity, lung
DOI: 10.5152/TurkThoracJ.2018.18044
Aşkın Gülşen 1,2 1Division of Clinical and Molecular Allergology, Research Center Borstel, Airway Research, Center North (ARCN), Member of the German Center for Lung Research, Borstel, Germany2Interdisciplinary Allergy Outpatient Clinic, Department of Pneumology, University of Lübeck, Germany
Address for Correspondence: Aşkın Gülşen, Division of Clinical and Molecular Allergology, Research Center Borstel, Airway Research, Center North (ARCN), Member of the German Center for Lung Research, Borstel; Interdisciplinary Allergy Outpatient Clinic, Department of Pneumology, University of Lübeck, Germany E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org
141
Cite this article as: Gülşen A. Bronchoscopic Lung Volume Reduction: A 2018 Review and Update. Turk Thorac J 2018; 19(3): 141-9.
Bronchoscopic lung volume reduction (BLVR) procedure has expanded the treatment spectrum of patients with end-stage emphysema. These treatments include valve, coil, thermal vapor ablation, bio-lung volume reduction, targeted lung denervation, and airway bypass stent. This short review provides an up-to-date information on BLVR treatments, their clinical benefits, and an overview of complications. BLVR treatments generally affect dyspnea by reducing hyperinflation and residual volume (RV). Benefits of treatment are associated with improvement in lung function parameters (forced expiration volume in the first second, total lung capacity, RV, and 6-minute walking test) and quality of life. Serious potential pulmonary complications, such as pneumothorax, pneumonia, respiratory failure, and chronic obstructive pulmonary disease exacerbation, may also occur after BLVR treatment. In addition to these, low-cost BLVR methods, such as autologous blood and fibrin glue, are in the developmental stage. Bronchoscopic lung volume reduction treatments are a promis-ing method with positive results for patients with severe emphysema. The widespread use of these techniques, inadequate selection of patients, and non-critical and, therefore, unsuccessful use of BLVR in non-specialist centers lead to a false negative impression of the effectiveness of these techniques. In addition to these considerations, it is obvious that these treatments, which are quite expensive, are burdening social health systems. The reduction of costs or the development of lower-cost treatment methods is important for the future and for the availability of treatments.
KEYWORDS: Emphysema, bronchoscopic, lung volume reduction, valve, procedures, coil
Abstract
Received: 28.03.2018 Accepted: 11.06.2018

function, and quality of life, especially in patients with upper lobe emphysema [5]. However, patient selection is limited due to high postoperative non-fatal pulmonary complica-tions and short-term mortality of 6.9% [5]. In addition to medical treatment and surgery, BLVR treatments, especially in specific types of patients, have reportedly yielded promising short- to medium-term results [6-10]. After these results, the BLVR treatment methods (valve and coil) were introduced into the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017 guideline [4]. The guideline states that LVRS or BLVR treatments can be considered only in a refrac-tory situation to optimal medical treatment. However, it has been reported that patients who are not eligible for both treatment methods may be candidates for lung transplanta-tion if their forced expiration volume in the first second (FEV1) values are <25% [4].
This short review provides an up-to-date information on BLVR treatments, their clinical benefits, and an overview of compli-cations. All bronchoscopic approaches are presented here.
BRONCHOSCOPIC APPROACH TO LUNG VOLUME REDUCTION
Owing to the high complication rate and risk of mortality observed during the NETT trial, in recent years, less invasive
emphysema treatment procedures and bronchoscopic approaches have been developed [5]. These methods have been proven effective and safe in the short- to medium-term clinical trials [6-10]. Studies investigating long-term results are ongoing. The indications, effect mechanisms, outcomes, and complication rates of these BLVR treatment modalities are discussed further below.
COMMON INDICATIONS
Patients tend to exhibit the same typical indications, with some variation in minor details. In general, they include evi-dence of emphysema diagnosed via computed tomography, post-bronchodilator FEV1 <15%-50% predicted, RV >175%, total lung capacity (TLC) >100%, 6-minute walking test (6MWT) >150 m, pulmonary hypertension not present, PaCO2 <50-55 mmHg, and cessation of smoking >2 months prior [6]. Table 1 shows the generally accepted indications pertaining to all BLVR techniques.
MECHANISM
BLVR treatments generally affect dyspnea by reducing hyper-inflation and RV. Individually, they have different mechanisms of action and are not suitable for every patient. Endobronchial valves (EBVs) reduce air trapping, coils improve the elastic
Table 1. General inclusion criteria in the literature
FEV1 RV TLC PAB, PaCO2 6MWT mMRC DLCO Smoking Methods % pred % pred % pred mmHg mmHg m p % cessation
Valves13-20 15-50 >175 >100 <50 <60 100-500 >2 - >6 Months
Coils24-33 15-45 >175 >100 <50 <55 150-450 - - >8 Weeks
TVA37-39 20-45 >150 >100 <35 <55 >140 - >20 >4 Months
>200*
BioLVR40,41 <50 >150 >100 <25 <65 >150 - 20-60 >4 Months
TLD42,43 30-60 - - <25 <60 - - - >6 Months
ABS44-45 <50 >180 - <25 <50 - >2 >15 >8 Weeks
TVA: thermal vapor ablation; LVR: lung volume reduction; TLD: targeted lung denervation; ABS: airway bypass stent; FEV1: forced expiration volume in the 1 s; RV: residual volume; TLC: total lung capacity; PAB: pulmonary arterial pressure; PaCO2: arterial partial pressure of carbon dioxide; 6MWT: 6-minute walking test; mMRC: Modified British Medical Research Council; DLCO: diffusing capacity for carbon monoxide; *: preferably
Table 2. Mechanism of the BLVR procedures
Valve13-20 Coil24-33 TVA37-39 ABS42,43 TLD44,45
Mechanism Reducing airway Improvement of Local inflammatory Blocking Airway Reduction of Trapping elastic recoil reactions bronchoconstriction
Reversibility Yes Partial No Partial No
Dependence of Yes No No Yes No collateral ventilation
Type of Emphysema Heterogeneous Heterogeneous Heterogeneous, Homogeneous Heterogeneous or homogeneous only upper lobe or homogeneous
Possible relevant Pneumothorax, COPD Local and systemic Exacerbation, Exacerbation, complications Dislocation, or Exacerbation, inflammatory pneumothorax, Procedure related migration of Valve Pneumonia reactions, Pneumonia hemoptysis or Pneumonitis
BLVR: bronchoscopic lung volume reduction; TVA: thermal vapor ablation; LVR: lung volume reduction; TLD: targeted lung denervation; ABS: airway bypass stent
Turk Thorac J 2018; 19(3): 141-9
142

recoil of the lungs, BioLVR and TVA create a local inflamma-tory reaction, ABS blocks the airway, and TLD reduces bron-choconstriction through innervation (Table 2) [6].
Endobronchial Valves ImplantationEndobronchial valves (Spiration, Inc., Redmond, WA, USA) are inserted bronchoscopically into the targeted segmental or subsegmental bronchi. With regard to blocking, they only allow a unidirectional flow of air during expiration, so that the treated lung section is vented, and the following atelec-tasis formation achieves the desired volume-reducing effect. The procedure can be performed under mild sedation as a standard bronchoscopic intervention. Patients with collateral ventilation or parenchymal connections in the relevant lung lobe are not suitable for this procedure. If collateral ventila-tion (short-circuit connection) is present, the desired atelec-tasis does not occur in the targeted lobe after valve insertion. With planned valve therapy, the likelihood of a good response to therapy by computed tomographic analysis may indicate completeness of interlobar fissures, and/or the direct determination of collateral ventilation with the Chartis sys-tem can be estimated during bronchoscopy [11,12].
Bronchoscopic valve application aims to achieve targeted lobar volume reduction (TLVR) in patients with severe emphysema and is considered an efficacy parameter. In this respect, a quantitative multidetector computed tomography scan is used to calculate and analyze efficacy, and currently, a 350 mL reduction is considered indicative of a favorable response [13]. Nevertheless, the importance of TLVR after valve implantation is unclear.
Several randomized controlled trials have confirmed the effi-cacy of EBV treatment [13-20]. Efficacy has been assessed via changes in lung function parameters, exercise tests, and health-related quality of life questionnaires, such as the St. George’s Respiratory Questionnaire (SGRQ) [20], and significant improvements have been reported. Studies conducted from 2010 to 2017 collectively indicate that the mean FEV1 increas-es to 77.5 mL (34.5-140 mL) and 13.7% (4.3%-20.7%), the mean RV decreases to 440 mL (200-680 mL), and the mean 6MWT increases to 40.8 m (9.3-91.0 m) (Table 3) [13-20].
In the previous studies, the mean survival after EBV treatment was 51 (46.5-56.3) months, and the death rate was 27% (9/33 patients) in the longest follow-up study. The causes of death reported were cancer, myocardial infarction, and end-stage respiratory failure [15]. Another interesting study has reported the 10-year survival results of patients with EBV treatment between 2002 and 2004. In that study, 19 patients were examined, and 40% of patients with atelectasis and 14% of patients without atelectasis were alive. In addition, attention has been drawn to the future development of col-lateral ventilation in patients and, if necessary, the replace-ment of EBVs [21].
Notably, however, EBV treatment is also associated with some risk. Data related to complications in published studies include COPD exacerbation rates of 9.3%-64.0%, pneumo-nia rates of up to 11.7%, pneumothorax rates of 4.2%-29.2%, valve migration and replacement rates of 1.5%-20.0%, and mortality rates of up to 8%. Another less frequent and important complication is granulation formation around the valves and associated EBV dislocation (Table 3) [13-20].
Table 3. Overview of principal BLVR-Valve Studies
Follow-up Δ RV Δ 6MWT Δ SGRQ TLVR Study / Author Year n time, M Δ FEV1 L m point mL
Sciurba et al. [14] 2010 220 6 +34.5 mL, +4.3% * +9.3 -2.8 *
Herth et al. [15] 2012 111 12 +15.0% * +22% -5.0 *
Davey et al. [16] 2015 25 6 +60 mL, +8.7% -0.26 +25.0 -4.4 *
Valipour et al. [17] 2016 43 3 +100 mL -0.42 +22.6 -8.6 -1195
Klooster et al. [18] 2017 64 12 +17.0% -0.68 +61.0 -11.0 *
Fiorelli et al. [19] 2017 33 60 +17.0% -39% +91.0 -17.0 *
Kemp et al. [20] 2017 65 6 +140 mL, +20.7% -0.66 +36.2 -7.2 *
Welling et al. [13] 2018 318 6 +53.4 mL -0.20 * -4.3 -463
Overview of Complications
Study / Author Year n Follow-up, M Pneumonia COPD Exc. PNX Valve EMR Death
Sciurba et al. [14] 2010 220 6 3.2% 9.3% 4.2% * 0.9%
Herth et al. [15] 2012 111 12 11.7% 42.3% 8.0% * 5.4%
Davey et al. [16] 2015 25 6 8.0% 64.0% 8.0% 20.0% 8.0%
Valipour et al. [17] 2016 43 3 0 16.3% 25.6% 7.0% 0
Klooster et al. [18] 2017 64 12 8.0% 14.0% 22.0% 17.0% 3.0%
Fiorelli et al. [19] 2017 33 60 3.0% * 6.0% 5.0% 0
Kemp et al. [20] 2017 65 6 4.6% 4.6% 29.2% 1.5% 1.5%
n: patient population; M: month; TLVR: target lobar volume reduction; SGRQ: St George’s Respiratory Questionnaire total score; COPD: chronic obstructive pulmonary disease; Exc: Exacerbation; PNX: pneumothorax; EMR: Expectoration, migration, and replacement; FEV1: forced expiration volume in the 1 s; Δ: change; *: no data
Gülşen A. Review of Bronchoscopic Lung Volume Reduction Procedures
143

Finally, the EBV procedure is relatively expensive. Depending on the relevant agreements with local commercial and social health systems, the cost of the Chartis catheter and the deliv-ery system for a single procedure range from €8,200 to €9,200. This does not include any costs associated with the actual performance of the operation itself or the manage-ment of any complications should they arise. It is a current challenge for both healthcare systems and valve manufactur-ing companies to make this treatment more accessible in developing countries [22].
Endobronchial Coil ImplantationCoil treatment (PneumRx, Inc., Mountain View, CA, USA) has been developed for patients with interlobar collateral ventilation in the years following EBV therapy. A pilot study of 22 BLVR operations published by Herth et al. [23] in 2010 was successful, and the treatment was reported to be more useful in heterogeneous emphysema.
Over the years, there have been improvements in procedures and techniques, and it is generally considered acceptable practice for a patient to undergo bronchoscopic placement of 8-14 coils (mean number of 10 coils) in one lung under gen-eral anesthesia and fluoroscopy [24,25]. Depending on the anatomical length of the subsegment, 100, 125, and 150 mm coils are preferred. In general, each subsegment has 1 coil implant, with an average of 10 coils per lobe. Although the middle lobe and lingual segment are generally not preferred for treatment, it is necessary for the patient to have intact parenchymal tissue in unintended lung areas. Emphysema in patients is confirmed via high-resolution computed tomogra-phy (HRCT), with the required lung function parameters of FEV1 15%-45%, RV >175%, TLC >100%, and 6MWT 150-450 m. The treatment method is not recommended for patients who are active smokers or patients with paraseptal emphysema, pulmonary arterial pressure (PAP) >50 mmHg, bronchiectasis, lung cancer, or bullous lesions >4 cm. It is also not recommended for patients undergoing anticoagulation therapy, though in such cases, the treatment may be feasible in conjunction with the implantation of left atrial appendage occlusion and subsequent anticoagulation reduction.
The principle of the coils is simple. The implanted wire spirals collect the diseased lung tissue, creating more space for less diseased tissue in the surrounding region. This enhances the capacity for respiratory function, the natural elasticity of the lung improves, and the lungs can stretch and contract better during the breathing process. As a result, this alleviates respira-tory distress in patients. Studies conducted from 2012 to 2018 indicate that the average FEV1 increases to 130 mL (90-200 mL) and 12.1% (7%-14%), the average RV decreases to 420 mL (310-510 mL) and 16.5% (14.5%-22.0%), and the mean 6MWT increases to 47 m (14.6-84.0 m) (Table 4) [24-33].
Complications may also ensue immediately or after treat-ment using this treatment method. The complication rates in published studies include COPD exacerbation of 41.0% (10.8%-87.0%), pneumonia of 14.8% (0%-46.0%), pneumo-thorax of 5.7% (0%-11.6%), and mortality of 3.3% (0%-8%). Another less frequent complication is pleuritic chest pain and hemoptysis after treatment (Table 4) [24-33].
The total costs for 1 year are $53,521 for BLVR coil treatment and $5912 for follow-up patients only [30]. Based on one preliminary study (REVOLENS) of patients with severe emphysema followed up for 6 months, the initial cost of BLVR coil treatment appears to be high, but it seems that large-scale studies are needed to determine its long-term cost and effectiveness [30].
Thermal Vapor AblationIn addition to coils and EBVs, other endoscopic options for reducing lung volume have been developed. Bronchoscopic TVA (Uptake Medical Corporation, Seattle, WA, USA) is one of the techniques. It delivers thermal energy directly to the airways via a bronchoscope through heated water vapor. It induces an inflammatory reaction by instilling water vapor into the destroyed lung parenchyma. The local inflammatory reaction leads to fibrosis and scarring after approximately 8-12 weeks and thus to the desired lung volume reduction. This irreversible procedure is only preferred in patients with upper lobe emphysema, regardless of collateral ventilation [34,35]. The instillation of a hot water vapor at 75°C occurs via a special balloon catheter, with which the lung area to be treated is occluded. The vapor dose is calculated based on the mass of the lung tissue to be treated, and the average vapor dose is 10 cal/g alveolar tissue. This makes the targeted treatment of the area selected based on the HRCT possible. The heterogeneity index (HI) was identified as a predictor of an excellent outcome following bronchoscopic TVA. Patients with heterogeneous disease with an HI >1.2 and patients with COPD GOLD IV had greater improvements in FEV1 and 6MWT in recent studies [34,35].
The criteria in defining patients who can be treated in prin-ciple are (1) upper lobe dominant emphysema determined via HRCT; (2) ages between 40 and 75 years; (3) FEV1 between 15% and 45% predicted; (4) RV >150% predicted, ly >200; (5) TLC >100% predicted; (6) diffusing capacity of the lungs for carbon monoxide (DLCO) >20% predicted; (7) 6MWT >140 m; (8) PaCO2 <55 mmHg and partial arterial oxygen pressure >45 mm Hg; and (9) non-smoker for ≥4 months. Bronchoscopic TVA treatment is not recommended for patients with (1) known α-1-antitrypsin deficiency, asth-ma, or bronchiectasis; (2) bulla >1/3 lobe of the lung; (3) history of thoracotomy; (4) left ventricular ejection fraction ≤40%; or (5) pulmonary hypertension (mean pulmonary artery pressure ≥35 mmHg) [36].
There are fewer published TVA studies than published studies pertaining to coils and EBVs. Two major TVA studies con-ducted from 2012 to 2016 showed reduced hyperinflation and dyspnea and improvement of exercise tolerance and health-related quality of life. The first study was an uncon-trolled follow-up study in which unilateral bronchoscopic thermoablation with a vapor dose of 10 cal/g was performed in 44 patients with an HI of >1.2. After 6 months of treat-ment, there was a 48% decrease in lobar lung volume and a significant improvement in lung function parameters and quality of life. There were also significant improvements in FEV1 (0.14±0.16 L), RV (-0.40±0.71 L), 6MWT (46.5±67.1 m), and SGRQ (-14±15.1 points) at a 6-month interval. A GOLD IV subgroup shows greater improvements than GOLD III [37]. The second study was the first randomized con-
Turk Thorac J 2018; 19(3): 141-9
144

trolled trial of TVA treatment (n=46) versus medical manage-ment (n=24) and reported mean relative improvements of 14.7% (7.8%-21.5%) and 0.13 L (0.063-0.198 L) in FEV1, -9.7 points (-15.7 to -3.7 points) in SGRQ, and 30.5 m (1.5-62.4 m) in 6MWT at a 6-month follow-up [38].
The most common complication in the first few weeks was an excessive inflammatory response characterized by respi-ratory symptoms, such as dyspnea, cough, fever, and mild hemoptysis [39]. The most common complications in the following period were pneumonia (18%-23%) and COPD exacerbation (9%-24%) (Table 5). Therefore, consistent inpa-tient follow-up and concomitant prophylactic antibiotic and anti-inflammatory therapy are required. The severity of the local inflammatory response correlates with the good response to thermoablation and better result [34]. More effective TVA is associated with more pronounced inflamma-tion. In addition, there appears to be a correlation between the volume of the treated lung lobe and the extent of the inflammatory response. Patients with a treated lung volume of >1700 mL had to be re-hospitalized more frequently dur-ing the course of the disease due to a pronounced local inflammatory response. However, 6 months after TVA, this patient population exhibited the greatest benefit from TVA.
Bio-Lung Volume ReductionBioLVR or polymeric LVR is a method of bronchoscopic instil-lation of hydrogel into the target lobe that is intended to block lung tissue in patients with advanced emphysema. AeriSeal (Aeris Therapeutics, Inc., Woburn, MA, USA) is a foam-like liquid medium used in bronchioles and alveoli with 10 mL (low dose) or 20 mL (high dose) for each part. The application of the polymer foam is an irreversible BLVR procedure. Bronchoscopically applied polymer resin causes fibrosis in the targeted pulmonary parenchyma. A subsequent inflammatory reaction functions to decrease the tissue in the target regions and reduce volume. In the first study, which included 14 patients and was published in 2011, a positive therapeutic effect was apparent but so were complications, mainly due to inflammatory processes [40]. The results reported included an FEV1 increase of +15.9% predicted, a 6MWT increase of 28.7 m, RV/TLC change of -7.4% predicted, forced vital capacity (FVC) increase of 24.1% predicted, DLCO change of +9.3%, and SGRQ score change of -9.9 points [40].
In the “ASPIRE” study conducted in 2014, BioLVR using hydrogel was compared with medical therapy and has since been abandoned due to increased adverse events and an unacceptable complication rate resulting in patients with
Table 4. Overview of principal BLVR-Coil Studies
Author Year n Follow-up, M Δ FEV1 Δ RV Δ 6MWT Δ SGRQ
Slebos et al. [24] 2012 16 6 +14.9% -11.4% +84.4 m -14.9
Shah et al. [25] 2013 23 3 +14.1% -0.51 L +51.1 m -8.6
Klooster et al. [26] 2014 10 6 +0.11 L -22.0% +61.0 m -15.0
Deslee et al. [27] 2014 34 12 +16.0% -13.75% +51.4 m -11.1
Hartman et al. [28] 2014 35 12 +0.20 L -21% +31.0 m -4.2 27 24 - 0.05 L -10% -12.0 m -8.0 22 36 - 0.04 L -2% -31.5 m -7.2
Zoumot et al. [29] 2015 35 12 + 8.9% -0.32 L +34.1 m -6.1
Deslee et al. [30] 2016 50 12 + 0.09 L -0.52 L +9% -11.1
Sciurba et al. [31] 2016 158 12 + 7.0% -0.31 L +14.6 m -8.9
Gülsen et al. [32] 2017 40 6 +0.15 L -14.5% +48.0 m -10.4
Simon et al. [33] 2018 33 3 +0.10 L -0.44 L +48.0 m *
Overview of Complications
Author Year n Follow-up, M Pnx COPD Exc. Pneumonia Death
Slebos et al. [24] 2012 16 6 0 87.0% 18.7% 0
Shah et al. [25] 2013 23 3 8.6% 17.0% 0 0
Klooster et al. [26] 2014 10 6 10% 70.0% 0 0
Deslee et al. [27] 2014 34 12 11.6% 33.0% 23.3% 0
Hartman et al. [28] 2014 35 12 6.0% 51.0% 46.0% 3% 27 24 0 37.0% 7.0% 8% 22 36 0 36.0% 5.0% 6%
Zoumot et al. [29] 2015 84 12 9.6% 10.8% 2.4% -
Deslee et al. [30] 2016 50 12 2.0% 26.0% 18.0% 8%
Sciurba et al. [31] 2016 158 12 9.7% 27.7% 20.0% 6.5%
Gülsen et al. [32] 2017 40 6 0 41.4% 17.0% 2%
Simon et al. [33] 2018 33 3 0 46.3% 5.6% 0
n: patient population; COPD: Chronic obstructive pulmonary disease; FEV1: forced expiration volume in the 1 s; Δ: change; M: month; SGRQ: St George’s Respiratory Questionnaire total score
Gülşen A. Review of Bronchoscopic Lung Volume Reduction Procedures
145

BioLVR requiring more hospitalization [41]. The clinical method it entails is currently not recommended.
Targeted Lung DenervationTargeted Lung Denervation is the most recently developed novel therapeutic COPD treatment. Technically, it is not a vol-ume reduction procedure; rather, its aims are ablation of para-sympathetic nerves innervating the basal lung and the reduc-tion of bronchoconstriction. Its effects are similar to those of anticholinergic drugs. It is performed via a double-cooled radiofrequency catheter (Holaira, Minneapolis, MN, USA). Radiofrequency (15-20 W) is applied to the target lung and 8 points. The cooler is also used in order to prevent the resulting heat from affecting the inner surface of the airway. It is usually applied bilaterally and step by step. Slebos et al. [42] con-ducted an initial pilot study in 2015 and reported that 20 W is more successful than 15 W. Patients receiving TLD incorporat-ing 20 W reported an increase of 11.6% in FEV1, an increase of 6.8 min in submaximal cycle endurance, and a decrease of 11.1 points in SGRQ score. The most frequent adverse event at a 1-year follow-up was COPD exacerbation (59%). Gastritis (18%), respiratory inflammation (18%), and anaphylactic reac-tion (5%) were also observed. Non-serious complications, such as bronchial perforation, ulceration, and stenosis, may also rarely occur depending on the procedure. In another study, the anti-inflammatory effects of TLD were reported, and it was asserted that further research is needed [43].
The major criteria in defining patients who can be treated in principle are (1) age ≥40 years; (2) COPD with FEV1/FVC <70% and FEV1 between 30% and 60% predicted; (3) posi-tive relative change in FEV1 >15% following inhalation of ipratropium; (4) non-smoking for ≥6 months; (5) smoking history of at least 10 pack-years; and (6) PaCO2 <60 mmHg, PaO2 >55 mmHg, and PAP <25 mmHg [42]. The first pro-spective randomized controlled trial of lung denervation (“AIRFLOW-1”, NCT02058459) is still ongoing. TLD is not yet used in routine clinical practice.
Airway Bypass StentABS (Broncus Technologies, Inc., Mountain View, CA, USA) is only recommended for patients with severe homogeneous
emphysema. In this method, extra-anatomical transitions are made from the airway walls to the lung parenchyma to release the trapped air. A small drug (paclitaxel)-eluting stent is inserted into each drilled hole so that bypass occlusion is avoided. The intention is to bypass small collapsed airways. However, studies and data on this treatment method are lim-ited, and this BLVR technique is still in the trial phase.
In a small study reported by Choong et al. [44] in 2009, ABS improved pulmonary function parameters and reduced respi-ratory distress. However, no statistically significant results were obtained. In 2011, the “EASE” study involving 315 patients with severe homogeneous emphysema was reported [45]. Patients were randomly assigned to the ABS group (n=208) or the control group (n=107), followed by 1, 3, 6, and 12 months of respiratory function parameter assessment, 6MWT, and SGRQ. There was no statistically significant dif-ference between the two groups detected in their study. Compared with baseline, there was an increase of 12% in FEV1 and 1 point in the modified British Medical Research Council scale 6 months after the procedure. Therefore, it was reported that ABS is effective in the short term. Loss of effi-cacy over time is thought to be due to factors involving mucus plugs and granuloma formation. For this reason, it has been stated that further research is required in order to opti-mize the treatment method, and it is currently not one of the preferred BLVR treatments in practice.
Bronchoscopic Lung Volume Reduction Using Autologous Blood and Fibrin GlueA pilot study reported in 2016 assessed the efficacy and safety of BLVR using low-cost agents including autologous blood (n=7) and fibrin glue (n=8) [46]. On week 12 after the proce-dure, the autologous blood group exhibited an 8% FEV1 increase and a 16 m 6MWT increase, whereas the fibrin glue group exhibited a 17% FEV1 increase and a 96 m 6MWT increase. One patient in the autologous blood group had pneumonia in the first 10 days after the procedure, and one patient in the fibrin glue group had exhibited COPD exacerba-tion at 12 weeks follow-up, and mortality was not reported. The method was shown to constitute an effective and safe treatment, with good cost effectiveness for patients with severe
Table 5. Overview of principal Termal Vapor Ablation Studies
Follow-up, Δ FEV1 Δ RV Δ 6MWT Δ SGRQ TLVR Author Year n M mL mL m point mL
Herth et al. [37] 2012 22 12 +64£ -270£ +10.9£ 9.4£ -735£
22 12 +108† -335† +25.6† -12.7† -772†
Gompelmann et al. [35] 2014 44 6 +141 -406 * * -716
Gompelmann et al. [39] 2016 35 12 +65 -108 6.2 -12.1 *
Herth et al. [38] 2016 45 6 +130 -302 30.5 -9.7 *
Overview of Complications
Author Year n Follow-up, Pneumonia or COPD M pneumonitis Exc. PNX SAEs Death
Gompelmann et al. [39] 2016 35 12 23.0% 9.0% 3.0% 26.0% 3.0%
Herth et al. [38] 2016 45 6 18.0% 24.0% 2.0% 36.0% 2.0%
SAEs: serious adverse events; *: COPD Gold III patients; £: COPD Gold III patients; †: COPD GOLD IV patients; n: patient population; M: month; TLVR: target lobar volume reduction; FEV1: forced expiration volume in the 1 s; Δ: change; 6MWT: 6-minute walking test
Turk Thorac J 2018; 19(3): 141-9
146

emphysema. This biological lung volume reduction treatment is very promising in terms of its low-cost. Notably, however, the very small sample size and short follow-up detract from the power of the study. There is a need for long-term studies of cost, effectiveness, and safety in relation to this method.
REVERSIBILITY OF ALL BRONCHOSCOPIC LUNG VOLUME REDUCTION PROCEDURES
Reversibility of treatments and informing patients in this regard is a very important issue. EBV treatments are gener-ally considered reversible, whereas TLD and TVA are irre-versible. The coil procedure is regarded as partially revers-ible. Only three studies in the literature describe the removal of the coils. In a small case series (n=3) of patients with pleuritic pain, the coils could be removed within 4 weeks after implantation [47]. In another study, persistent thoracic pain was reported after treatment, and two coils were removed after 10 months [48]. Gülşen et al. [32] removed and replaced the coil in 10% of the patients during the pro-cedure. Thus, the literature suggests that the removal of the coils is generally only possible during the procedure and in the following few months, and that it is not possible to remove all coils.
BENEFITS OF BRONCHOSCOPIC LUNG VOLUME REDUCTION METHODS
With regard to the benefits of treatment, EBV is associated with average increases of 77.5 mL (34.5-140.0 mL) in FEV1 and 40.8 m (9.3-91.0 m) in 6MWT and an average reduction of 440 mL (200-680 mL) in RV. Coil therapy reportedly results in average increases of 130 mL (90-200 mL) in FEV1 and 47.0 m (14.6-84.0 m) in 6MWT and an average reduc-tion of 420 mL (310-510 mL) in RV. TVA treatment results in average increases of 101 mL (64-141 mL) in FEV1 and 18.3 m (6.2-30.5 m) in 6MWT and an average reduction of 284 mL (108-406 mL) in RV (Table 6).
COMPLICATIONS OF BRONCHOSCOPIC LUNG VOLUME REDUCTION TREATMENT AT A GLANCE
Serious potential pulmonary complications are associated with BLVR treatment methods. The complications of EBV treatments most commonly reported in the literature are COPD exacerbation (25.0%; 4.6%-64.0%) and pneumotho-
rax (14.7%; 4.2%-29.2%). In this treatment method, valve migration is reportedly seen in approximately 10.1% (1.5%-20.0%) of the patients. Coil treatments are most commonly associated with COPD exacerbation (41.0%; 10.8%-87.0%), pneumonia (14.8%; 0%-46.0%), and pneumothorax (5.7%; 0%-11.6%). In TVA treatments, the most common complica-tions are pneumonia (21.0%; 18.0%-23%) and COPD exac-erbation (16.5%; 9.0%-24.0%). The mortality rates are reportedly 2.6%, 3.3%, and 2.5%, respectively (Table 6).
POST-TREATMENT OF ACUTE INFLAMMATORY RESPONSE
Bronchoscopic Lung Volume Reduction treatments generally induce an acute inflammatory response (fever, dyspnea, cough, chest pain, and/or elevated inflammatory markers) after treatment. The authors generally recommend and administer steroid and prophylactic antibiotic therapy for 7 days to reduce inflammation. In addition, it is advisable to monitor patients in the hospital for at least 1 night and administer prophylactic non-steroidal anti-inflammatory drugs and stress ulcer prophylaxis for 3 days after treatment [49,50]. Although there is no general consensus on the appli-cation of prophylactic antibiotics, they are commonly used by the authors due to the high risk of COPD exacerbation and pneumonia. Pneumococcal and influenza vaccines are an overlooked but absolutely necessary consideration in these patients.
ONGOING AND FUTURE STUDIES
There are many future studies of BLVR techniques planned. The most interesting are the “BREATHE-NL” study in which a 5-year efficacy and benefit of EBV treatments was planned, the “LVRC-Micro Study” in which changes in the microbi-ome of the lungs will be observed after BLVR coil treatment, the study of sleep quality in coil therapy, the 3-year effects of TLD treatment, the “AIRFLOW-1 Study” to investigate the 3-year effects and benefits of TLD treatment, and the “BLOOD-VALVES Study” to compare EBV with low-cost autologous blood (Figure 1).
CONCLUSION
BLVR treatments are a promising method with positive results for patients with severe emphysema. Optimal patient and method selection for BLVR treatments and implementation in
Table 6. Overview of benefits of all BLVR techniques in the literature
Technique Δ FEV mL Δ FEV % pred. Δ RV mL Δ RV % pred. Δ 6MWT m
Valve 77.5 (34.5-140) 13.7 (4.3-20.7) 440 (200-680) - 40.8 (9.3-91.0)
Coil 130 (90.0-200) 12.1 (7.0-14.0) 420 (310-510) 16.5 (14.5-22.0%) 47.0 (14.6-84.0)
TVA 101 (64.0-141) - 284 (108-406) - 18.3 (6.2-30.5)
Overview of all mean complication rates
Technique Pneumonia COPD Exacerbation PNX Migration and replacement Death
Valve 6.4 (0-11.7) 25.0 (4.6-64.0) 14.7 (4.2-29.2) 10.1 (1.5-20.0) 2.6 (0-8.6)
Coil 14.8 (0-46.0) 41.0 (10.8-87.0) 5.7 (0-11.6) - 3.3 (0-8.0)
TVA 21.0 (18-23.0) 16.5 (9.0-24.0) 2.5 (2-3.0) - 2.5 (2-3.0)
Data of benefits are shown mean (min-max)/Data of complications are shown mean % (min-max)COPD: chronic obstructive pulmonary disease; FEV: forced expiration volume; Δ: change; M: month; PNX: pneumothorax; 6MWT: 6-minute walking test
Gülşen A. Review of Bronchoscopic Lung Volume Reduction Procedures
147

experienced centers are very important. However, it is neces-sary to be prepared for potential complications. The wide-spread use of these techniques, inadequate selection of patients, and non-critical and therefore, unsuccessful use of BLVR in non-specialist centers lead to a false negative impression of the effectiveness of these techniques. In addi-tion to these considerations, it is obvious that these treat-ments, which are quite expensive, are burdening social health systems. The reduction of costs or the development of lower-cost treatment methods is important for the future and for the availability of treatments. Therefore, BLVR in patients with severe emphysema will be a treatment of choice in the near future once clinical trials show the ongoing long-term effectiveness of the procedures.
Peer-review: Externally peer-reviewed.
Conflict of Interest: The author have no conflicts of interest to declare.
Financial Disclosure: The author declared that this study has received no financial support.
REFERENCES
1. Holloway RA, Donnelly LE. Immunopathogenesis of chronic ob-structive pulmonary disease. Curr Opin Pulm Med 2013;19:95-102. [CrossRef]
2. O'Donnell DE, Webb KA. The major limitation to exercise per-formance in COPD is dynamic hyperinflation. J Appl Physiol (1985) 2008;105: 753-5. [CrossRef]
3. Kemp SV, Polkey MI, Shah PL. The epidemiology, etiology, clini-cal features, and natural history of emphysema. Thorac Surg Clin 2009;19:149-58. [CrossRef]
4. Global Initiative for Chronic Obstructive Lung Disease. Glob-al strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease 2017. Access: http://www.goldcopd.org/.
5. Criner GJ, Cordova F, Sternberg AL, et al. The National Em-physema Treatment Trial (NETT) Part II: Lessons learned about lung volume reduction surgery. Am J Respir Crit Care Med 2011;184:881-93. [CrossRef]
6. Herth FJ, Slebos DJ, Criner GJ, et al. Endoscopic Lung Volume Reduction: An Expert Panel Recommendation - Update 2017. Respiration 2017;94:380-8. [CrossRef]
7. Ramaswamy A, Puchalski J. Bronchoscopic lung volume reduc-tion: recent updates. J Thorac Dis.2018;10(4):2519-27. [CrossRef]
8. Choi M, Lee WS, Lee M, Jeon K, Sheen S, Jheon S, Kim YS. Effectiveness of bronchoscopic lung volume reduction using unilateral endobronchial valve: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis.2015;10:703-10.
9. Snell G, Herth FJ, Hopkins P, Baker KM, Witt C, Gotfried MH, Vali-pour A, Wagner M, Stanzel F, Egan JJ, Kesten S, Ernst A. Bronchoscop-ic thermal vapour ablation therapy in the management of heteroge-neous emphysema. Eur Respir J.2012;39(6):1326-33. [CrossRef]
10. Gompelmann D, Eberhardt R, Herth FJ. Novel Endoscopic Ap-proaches to Treating Chronic Obstructive Pulmonary Disease and Emphysema. Semin Respir Crit Care Med.2015;36(4):609-15. [CrossRef]
11. Gompelmann D, Eberhardt R, Slebos DJ, et al. Diagnostic per-formance comparison of the Chartis System and high-resolution computerized tomography fissure analysis for planning endo-scopic lung volume reduction. Respirology 2014;19:524-30. [CrossRef]
12. Reymond E, Jankowski A, Pison C, et al. Prediction of lobar col-lateral ventilation in 25 patients with severe emphysema by fis-sure analysis with CT. AJR Am J Roentgenol 2013; 201: 571-5. [CrossRef]
13. Welling JBA, Hartman JE, van Rikxoort EM, et al. Minimal important difference of target lobar volume reduction after endobronchial valve treatment for emphysema. Respirology 2018;23:306-10. [CrossRef]
14. Sciurba FC, Ernst A, Herth FJ, et al. VENT Study Research Group A randomized study of endobronchial valves for advanced em-physema. N Engl J Med 2010;363:1233-44. [CrossRef]
15. Herth FJ, Noppen M, Valipour A, et al. International VENT Study Group. Efficacy predictors of lung volume reduction with Zeph-yr valves in a European cohort. Eur Respir J 2012;39:1334-42. [CrossRef]
16. Davey C, Zoumot Z, Jordan S, et al. Bronchoscopic lung vol-ume reduction with endobronchial valves for patients with heterogeneous emphysema and intact interlobar fissures (the BeLieVeR- HIFi study): a randomised controlled trial. Lancet 2015;386:1066-73. [CrossRef]
17. Valipour A, Slebos DJ, Herth F, et al. IMPACT Study Team Endo-bronchial valve therapy in patients with homogeneous emphy-sema. Results from the IMPACT Study. Am J Respir Crit Care Med 2016;194:1073-82. [CrossRef]
18. Klooster K, Hartman JE, Ten Hacken NH, et al. One-Year Fol-low-Up after Endobronchial Valve Treatment in Patients with Emphysema without Collateral Ventilation Treated in the STEL-VIO Trial. Respiration 2017;93:112-21. [CrossRef]
19. Fiorelli A, Santoriello C, De Felice A, et al. Bronchoscopic lung volume reduction with endobronchial valves for heterogeneous emphysema: long-term results. J Vis Surg 2017;3:170. [CrossRef]
Figure 1. Ongoing randomized clinical trials of bronchoscopic lung volume reduction therapies
Turk Thorac J 2018; 19(3): 141-9
148

20. Kemp SV, Slebos DJ, Kirk A, et al.; TRANSFORM Study Team. A Multicenter Randomized Controlled Trial of Zephyr Endo-bronchial Valve Treatment in Heterogeneous Emphysema (TRANSFORM). Am J Respir Crit Care Med 2017;196:1535-43. [CrossRef]
21. Garner J, Kemp SV, Toma TP, et al. Survival after Endobronchial Valve Placement for Emphysema: A 10-Year Follow-up Study. Am J Respir Crit Care Med 2016;194:519-21. [CrossRef]
22. Jarad N. Clinical review: Endobronchial valve treatment for em-physema. Chron Respir Dis 2016;13:173-88. [CrossRef]
23. Herth FJ, Eberhard R, Gompelmann D, et al. Bronchoscopic lung volume reduction with a dedicated coil: a clinical pilot study. Ther Adv Respir Dis 2010;4:225-31. [CrossRef]
24. Slebos DJ, Klooster K, Ernst A, et al. Bronchoscopic lung volume reduction coil treatment of patients with severe heterogeneous emphysema. Chest 2012;142: 574-82. [CrossRef]
25. Shah PL, Zoumot Z, Singh S, et al. Endobronchial coils for the treatment of severe emphysema with hyperinflation (RESET): a randomised controlled trial. Lancet Respir Med 2013;1:233-40. [CrossRef]
26. Klooster K, Ten Hacken NH, Franz I, et al. Lung volume reduc-tion coil treatment in chronic obstructive pulmonary disease pa-tients with homogeneous emphysema: a prospective feasibility trial. Respiration 2014;88:116-25. [CrossRef]
27. Deslee G, Klooster K, Hetzel M, et al. Lung volume reduction coil treatment for patients with severe emphysema: a European multicentre trial. Thorax 2014;69:980-6. [CrossRef]
28. Hartman JE, Klooster K, Gortzak K, et al. Long-term follow-up after bronchoscopic lung volume reduction treatment with coils in patients with severe emphysema. Respirology 2015;20: 319-26. [CrossRef]
29. Zoumot Z, Kemp SV, Singh S, et al. Endobronchial coils for se-vere emphysema are effective up to 12 months following treat-ment: medium term and cross-over results from a randomized controlled trial. PLoS One 2015;10:e0122656.
30. Deslée G, Mal H, Dutau H, et al.; REVOLENS Study Group. Lung Volume Reduction Coil Treatment vs Usual Care in Pa-tients With Severe Emphysema: The REVOLENS Randomized Clinical Trial. JAMA 2016;315:175-84. [CrossRef]
31. Sciurba FC, Criner GJ, Strange C, et al. RENEW Study Research Group. Effect of Endobronchial Coils vs Usual Care on Exer-cise Tolerance in Patients With Severe Emphysema: The RE-NEW Randomized Clinical Trial. JAMA. 2016;315:2178-89. [CrossRef]
32. Gulsen A, Sever F, Girgin P, et al. Evaluation of bronchoscopic lung volume reduction coil treatment results in patients with severe emphysema. Clin Respir J 2017;11:585-92. [CrossRef]
33. Simon M, Harbaum L, Oqueka T, et al. Endoscopic lung volume reduction coil treatment in patients with very low FEV1: an observational study. Ther Adv Respir Dis 2018;12:1753466618760133. [CrossRef]
34. Gompelmann D, Eberhardt R, Ernst A, et al.: The localized in-flammatory response to bronchoscopic thermal vapor ablation in patients with emphysema. Respiration 2013; 86:324-31. [CrossRef]
35. Gompelmann D, Eberhardt R, Herth FJ. Technology update: bronchoscopic thermal vapor ablation for managing severe em-physema. Med Devices (Auckl) 2014;7:335-41. [CrossRef]
36. Snell GI, Hopkins P, Westall G, et al. A feasibility and safety study of bronchoscopic thermal vapor ablation: a novel emphy-sema therapy. Ann Thorac Surg 2009;88:1993-8. [CrossRef]
37. Herth FJ, Ernst A, Baker KM, et al. Characterization of outcomes 1 year after endoscopic thermal vapor ablation for patients with heterogeneous emphysema. Int J Chron Obstruct Pulmon Dis 2012;7:397-405.
38. Herth FJ, Valipour A, Shah PL, et al. Segmental volume reduc-tion using thermal vapour ablation in patients with severe em-physema: 6-month results of the multicentre, parallel-group, open-label, randomised controlled STEP-UP trial. Lancet Respir Med 2016;4:185-93. [CrossRef]
39. Gompelmann D, Eberhardt R, Schuhmann M, et al. Lung Vol-ume Reduction with Vapor Ablation in the Presence of Incom-plete Fissures: 12-Month Results from the STEP-UP Randomized Controlled Study. Respiration 2016;92:397-403. [CrossRef]
40. Herth FJ, Gompelmann D, Stanzel F, et al. Treatment of advanced emphysema with emphysematous lung sealant (AeriSeal®). Res-piration 2011;82:36-45. [CrossRef]
41. Come C, Abu-Hijleh M, Berkowitz D, et al. Results of the AS-PIRE endoscopic lung volume reduction trial at study termina-tion. Eur Respir J 2014; 44:3717.
42. Slebos DJ, Klooster K, Koegelenberg CF, et al. Targeted lung de-nervation for moderate to severe COPD: a pilot study. Thorax 2015;70:411-9. [CrossRef]
43. Kistemaker LE, Slebos DJ, Meurs H, et al. Anti-inflammatory ef-fects of targeted lung denervation in patients with COPD. Eur Respir J 2015;46:1489-92. [CrossRef]
44. Choong CK, Cardoso PF, Sybrecht GW, et al. Airway bypass treatment of severe homogeneous emphysema: taking advan-tage of collateral ventilation. Thorac Surg Clin 2009;19:239-45. [CrossRef]
45. Shah PL, Slebos DJ, Cardoso PF, et al. Bronchoscopic lung-vol-ume reduction with Exhale airway stents for emphysema(EASE trial): randomised, sham-controlled, multicentre trial. Lancet 2011;378:997-1005. [CrossRef]
46. Bakeer M, Abdelgawad TT, El-Metwaly R, et al. Low cost biolog-ical lung volume reduction therapy for advanced emphysema. Int J Chron Obstruct Pulmon Dis 2016;11:1793-800. [CrossRef]
47. Hetzel M, Bartscher E, Merk T, et al. Reversibilitat der Implanta-tion von RePneu Coils. In: Poster session (67/ P314) presented at the 54th Annual meeting of the Pneumologie. Hannover, Ger-many, 2013.
48. Dutau H, Bourru D, Guinde J, et al. Successful Late Removal of Endobronchial Coils. Chest 2016;150:143-5. [CrossRef]
49. Herth FJ, Eberhardt R, Ingenito EP, et al. Assessment of a novel lung sealant for performing endoscopic volume reduction ther-apy in patients with advanced emphysema. Expert Rev Med De-vices 2011;8:307-12. [CrossRef]
50. Kramer MR, Refaely Y, Maimon N, et al. Bilateral endoscopic sealant lung volume reduction therapy for advanced emphy-sema. Chest 2012;142:1111-7. [CrossRef]
Gülşen A. Review of Bronchoscopic Lung Volume Reduction Procedures
149

Turk Thorac J 2018; 19(3): 150-2
Case Report
A Rare Cause of Recurrent Spontaneous Pneumothorax: Birt-Hogg-Dube Syndrome
INTRODUCTION
Spontaneous pneumothorax can be classified as primary or secondary depending on the presence or absence of an underlying lung disease, such as cystic lung diseases. Birt-Hogg-Dube (BHD) syndrome is an autosomal dominant disorder characterized by the development of cutaneous lesions, renal tumors and lung cysts. In cases with BHD syndrome, the frequency of recurrent pneumothorax is increased due to presence of multiple lung cysts [1]. Herein, we report a case of a 34-year-old woman with BHD syndrome who admitted to the emergency department with complaints of dyspnea and chest pain due to pneumothorax. We present imaging findings and associated conditions in BHD syndrome.
CASE PRESENTATION
A 34-year-old female patient was admitted to the emergency department with sudden onset of breathlessness and left-sided chest pain. The patient had complaints for 6 hours. The patient was a non-smoker. She had a history of spontaneous pneumothorax five years ago and a diagnosis of prolactin secreting pituitary adenoma for three years. Her family history revealed that the patient’s mother had a history of pneumothorax, and her aunt had cystic lung disease. Physical examination revealed breath sounds were reduced over the left side. Papular skin lesions involv-ing the nose, face and chest wall were detected. She was afebrile and her blood pressure was normal. Chest x-ray showed suspicious focal pneumothorax on the left side. Computed tomography (CT) of the chest was obtained. Chest CT confirmed a loculated pneumothorax on the left side. Bilateral multiple lung cysts various in size and shape, predominantly located in the basal regions were evident (Figure 1). A chest tube was inserted into the left side and the pneumothorax improved immediately. The patient was diagnosed as BHD syndrome because of the presence of lung cysts and skin lesions, and her history suggestive of BHD syndrome. Contrast-enhanced CT of the abdomen was performed to investigate the presence of renal lesions. Abdominal CT scan showed a contrast-enhancing mass in the upper pole of the right kidney (Figure 2). Biopsy of the dermatologic lesions showed trichodiscoma and BHD syndrome diagnosis was confirmed by the identification of a mutation in the folliculin gene, encoded by FLCN. The patient underwent laparoscopic partial nephrectomy and the lesion was diagnosed as renal cell carcinoma with oncocytic and chromophobe components. No recurrence was detected at a 9-month follow-up period. The patient’s written informed consent for publication was obtained.
DISCUSSION
Birt-Hogg-Dube syndrome commonly presents with the clinical triad of skin lesions, pulmonary cysts with an increased risk of pneumothorax, and renal neoplasms. The syndrome is an autosomal dominant disorder arising from germline mutations
DOI: 10.5152/TurkThoracJ.2018.17045
Engin Karaman , Furkan Ufuk , Mahmut Demirci , Hüseyin Gökhan Yavaş Department of Radiology, Pamukkale University School of Medicine, Denizli, Turkey
Address for Correspondence: Furkan Ufuk, Department of Radiology, Pamukkale University School of Medicine, Denizli, TurkeyE-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org 150
Cite this article as: Karaman E, Ufuk F, Demirci M, Yavaş HG. A Rare Cause of Recurrent Spontaneous Pneumothorax: Birt-Hogg-Dube Syndrome. Turk Thorac J 2018; 19(3): 150-2.
Birt-Hogg-Dube (BHD) syndrome is an unusual disorder characterized by the triad of cutaneous lesions, renal tumors and lung cysts. In cases with BHD syndrome, the frequency of recurrent pneumothorax is increased due to presence of multiple lung cysts. It is important to evaluate the BHD syndrome in differential diagnosis of recurrent pneumothorax especially with multiple lung cysts predominating in the lung base. In these patients, the presence of accompanying kidney and other tumors should be investigated. Herein, we report a case of BHD syndrome presenting with recurrent pneumothorax.
KEYWORDS: Birt-Hogg-Dube syndrome, cystic lung disease, pneumothorax, pituitary adenoma
Abstract
Received: 05.06.2017 Accepted: 16.09.2017

in the folliculin (FLCN) gene. The FLCN gene is expressed in skin, nephrons, and type 1 pneumocytes. Its functions are not well-known, although it is reported as a tumor suppressor gene elsewhere [2,3]. Since it is a very rare disorder the diagnosis of BHD syndrome can frequently be delayed. The skin manifes-tations of BHD include fibrofolliculomas, trichodiscomas, and acrochordons. Renal findings can range from benign cysts to malignant tumors, and are often multiple and bilateral [1,3]. The risk of renal cancer is estimated to be seven times higher in patients with BHD syndrome and the prevalence of kidney lesions and lung cysts are about 34% and 84%, respective-ly [3]. Patients with BHD syndrome should be informed the increased incidence of kidney tumors and should be recom-mended yearly abdominal ultrasound or CT scan screening. Kunogi et al. [4] showed that none of the 21 patients in their study had skin or renal lesions. Therefore, BHD syndrome can-not be excluded simply because there are no kidney or skin lesions. Family history, bilateral, multiple lung cysts in the basal regions of the lung, and skin and renal lesions are typical for BHD syndrome, as in our patient.
Thyroid nodules, parotid oncocytoma, colonic polyposis, an-giolipoma, parathyroid adenoma, flecked chorioretinopathy, neurothekeoma, meningioma, breast cancer, tonsil cancer, colorectal cancer, sarcoma, lung cancer, melanoma, basal cell carcinoma, and squamous cell carcinoma have been reported to be associated with BHD syndrome in case reports and case series [5-7]. However, these relations are not clear. Interest-ingly, a prolactin secreting pituitary adenoma was present in our case (Figure 3). To the best of our knowledge, there are no reports about an association between BHD syndrome and prolactin secreting pituitary adenoma in the literature yet. This association could be coincidental. Additional studies and re-ports that investigate this relationship is required.
Spontaneous pneumothorax is a possible clinical manifesta-tion of BHD syndrome, with a high risk of recurrence. The risk of pneumothorax is estimated to be 50 times higher in patients with BHD syndrome. First presentation of a BHD pa-tient may be with spontaneous pneumothorax [4]. Cysts in BHD syndrome are usually well defined, thin walled, mainly
Figure 1. a,b. (a) Axial CT image of patient demonstrates a limited pneumothorax in the left lung, (b) coronal reformatted CT scan of patient shows bilateral, multiple thin walled cysts, especially in the lower lobes
a
b
Figure 2. Abdominal CT shows a well-defined, hypodense mass (white arrows) in the upper pole of the right kidney
Figure 3. Sagittal post-gadolinium T1-weighted pituitary magnetic resonance image shows hypointense, well-defined pituitary adenoma (white arrow)
Karaman et al. Spontaneous Pneumothorax in a patient with Birt-Hogg-Dube Syndrome
151

oval and lentiform shaped, usually multiple and bilaterally lo-cated and distributed among the lower zone and subpleural regions, as in our case [1].
The differential diagnosis of multiple pulmonary cysts includes centrilobular emphysema, lymphangioleiomyomatosis, pul-monary Langerhans cell histiocytosis, lymphocytic interstitial pneumonitis, and neurofibromatosis type 1. Centrilobular em-physema occurs in upper lobes of smokers, and has no dis-cernable walls. Lymphangioleiomyomatosis is characterized by multiple thin walled, multiple, round, well circumscribed cysts, which are distributed diffusely throughout the lungs in reproductive women. Langerhans cell histiocytosis may pres-ent with a combination of both nodules and bizarre shaped cysts, and it tends to spare lung bases and costophrenic angles. A few scattered perivascular lung cysts associated with ground-glass opacities, centrilobular nodules and septal thickening are seen in lymphocytic interstitial pneumonitis, which is usually related with other autoimmune and connective tissue diseas-es. Multiple lung cysts may also be seen in neurofibramatosis type 1, which has characteristic skin lesions [1,5,7]. BHD syn-drome is a rare genetic disorder with an increased risk of renal tumors. The prompt and accurate diagnosis is necessary for appropriate management of patients and genetic counseling. Presence of recurrent pneumothorax in a patient with typical skin lesions should raise the suspicion of BHD syndrome, and CT of the chest and abdomen should be performed to rule out lung cysts and renal lesions. In addition, BHD syndrome and pituitary adenoma was evident in our case. Therefore, we think that BHD syndrome and pituitary adenoma may exist together. Additional studies and reports are needed to show this possible relationship.
Informed Consent: Written informed consent was obtained from the patient who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - E.K., H.G.Y., M.D.; Design - E.K., H.G.Y., M.D.; Supervision - F.U.; Resource - E.K., H.G.Y., M.D.; Ma-terials - E.K., H.G.Y., M.D.; Data Collection and/or Processing - E.K., H.G.Y., M.D.; Analysis and/or Interpretation - F.U.; Literature Search - F.U.; Writing - E.K., F.U.; Critical Reviews - F.U.
Conflict of Interest: The authors have no conflicts of interest to de-clare.
Financial Disclosure: The authors declared that this study has re-ceived no financial support.
REFERENCES
1. Burkett A, Coffey N, Tomiak E, et al. Recurrent spontaneous pneumothoraces and bullous emphysema. A novel mutation causing Birt-Hogg-Dube syndrome. Respir Med Case Rep 2016;19:106-8.
2. Noppen M, De Keukeleire T. Pneumothorax. Respiration 2008;76:121-7. [CrossRef]
3. Toro JR, Wei MH, Glenn GM, et al. BHD mutations, clinical and molecular genetic investigations of Birt-Hogg-Dubé syndrome: a new series of 50 families and a review of published reports. J Med Genet 2008;45:321-31. [CrossRef]
4. Kunogi M, Akiyoshi T, Gunji Y, et al. Mutation analysis of the Birt-Hogg-Dubé gene in patients with multiple lung cysts. Am J Respir Crit Care Med 2009;179:A4398.
5. Maffe A, Toschi B, Circo G, et al. Constitutional FLCN muta-tions in patients with suspected Birt-Hogg-Dube syndrome ascertained for non-cutaneous manifestations. Clin Genet 2011;79:345-54. [CrossRef]
6. Chung JY, Ramos-Caro FA, Beers B, et al. Multiple lipomas, angiolipomas, and parathyroid adenomas in a patient with Birt-Hogg-Dube syndrome. Int J Dermatol 1996;35:365-7. [CrossRef]
7. Gupta N, Sunwoo BY, Kotloff RM. Birt-Hogg-Dubé Syndrome. Clin Chest Med 2016;37:475-86.[CrossRef]
Turk Thorac J 2018; 19(3): 150-2
152
Turk Thorac J 2018; 19(3): 153-5
Case Report
Delayed Diagnosis of Tuberculoma in a Child with Nephritis due to Systemic Lupus Erythematosus
INTRODUCTION
Infection, particularly tuberculosis (TB), is a major cause of morbidity and mortality in patients with systemic lupus ery-thematosus (SLE) in TB endemic areas. The prevalence of TB infection in patients with SLE is 18% [1]. Clinical manifes-tation of TB infection in an immunocompromised patient is absent, or unusual symptoms may appear. Supporting inves-tigation may give vague results because of atypical and reduced inflammatory responses. Infections can progress rapidly, so time is limited for accurate diagnosis and management of the patient [2].
We present the case of a patient with SLE who commenced on immunosuppressive therapy and had tuberculoma on the occipital lobe of the brain.
CASE PRESENTATIONA 13-year-old girl was diagnosed with SLE one year before. She was brought to the outpatient clinic with signs and symptoms of alopecia, arthralgia, and malar rash, and laboratory findings documented positive results of serum antinu-clear antibody and anti-double-stranded deoxyribonucleic acid antibody. During follow-up, we identified hypertension and proteinuria suggesting nephritis due to SLE. Intravenous (IV) high dose methylprednisolone and cyclophosphamide were commenced. She visited the outpatient immunology clinic regularly during follow up. No TB symptoms were iden-tified, and she did not report having close contact with adult TB.
On the fifth cycle of IV cyclophosphamide, she complained of severe headache and experienced focal seizure. Neurological examination including cranial nerve examination, funduscopy, and physiological reflexes were normal. We did not find any pathological reflexes. No lymphadenopathy or manifestation of active SLE was observed. Cardiovascular system examination was within normal limit except for high blood pressure (130/90 mmHg). Body temperature was within normal limit. There was no liver or spleen enlargement. The respiratory system and gastrointestinal system were normal. Laboratory findings showed low hemoglobin level (8.3 mg/dL), high leukocyte count (23.8109/L) with 87% neutrophils, and lymphopenia and platelet count was within normal limit. Peripheral blood smear showed an anisochro-
DOI: 10.5152/TurkThoracJ.2018.17033
Heda Melinda Nataprawira1 , Gartika Sapartini2, Ketut Indriani3 1Division of Respirology, Department of Child Health, Padjadjaran University School of Medicine, Hasan Sadikin General Hospital, Bandung, Indonesia2Division of Allergy and Immunology, Padjadjaran University School of Medicine, Hasan Sadikin General Hospital, Bandung, Indonesia3Department of Child Health, Padjadjaran University School of Medicine, Hasan Sadikin General Hospital, Bandung, Indonesia
Address for Correspondence: Heda Melinda Nataprawira, Division of Respirology, Department of Child Health, Padjadjaran University School of Medicine, Hasan Sadikin General Hospital, Bandung, Indonesia E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org 153
Cite this article as: Nataprawira HM, Sapartini G, Indriani K. Delayed Diagnosis of Tuberculoma in a Child with Nephritis due to Systemic Lupus Erythematosus. Turk Thorac J 2018; 19(3): 153-5.
Tuberculoma is one of the manifestations of tuberculosis infection in the central nervous system. Even though its prevalence is only 1%, the mortality rate is high. Clinical presentation in immunocompromised patients with tuberculoma maybe different, thus making the diagnosis difficult. We present the case of a 13-year-old girl who was admitted for routine intravenous administration of cyclophospha-mide and steroid therapy for nephritis due to systemic lupus erythematosus. She experienced severe headache and focal seizure on the second day of hospitalization. Neurology examination did not show any abnormalities. The Xpert MTB/RIF from the cerebrospinal fluid and sputum yielded negative results. Computed tomography scan and magnetic resonance imaging showed tuberculoma with caseous necrosisaround the fibrous capsule in the right occipital lobe of the brain. Electroencephalography showed no abnormalities. Clinical improvement was seen after 3weeks of treatment; however, antituberculosis drug-induced hepatotoxicity occurred.
KEYWORDS: Tuberculoma, systemic lupus erythematosus, child
Abstract
Received: 04.05.2017 Accepted: 18.12.2017 Available Online Date: 19.06.2018

mic anemia, with leukocyte shift to the left, hypersegmented, and granular toxic. C-reactive protein was 35.8 mg/L. Electrolyte levels were within normal limits. Urinalysis showed proteinuria and glucosuria. Serum liver, renal func-tion, and blood glucose were within normal limits. Blood culture was sterile. Chest X-ray appeared normal.
She underwent head computed tomography (CT) scan with contrast and revealed meningeal enhancement at the tento-rium cerebelli bilateral fissure, posterior interhemispheric fissure, corticalsulci, and bilateral occipital lobes suggesting
meningitis. Single ring-enhancing lesion size was 15 mm in the subcortical on the right occipital lobes with perifocal edema suggesting tuberculoma (Figure 1).
Cerebrospinal fluid (CSF) analysis showed clear liquid with normal cell count, protein level was normal, and CSF-to-serum glucose ratio was normal. Fungal, bacterial, and Mycobacterium tuberculosis cultures from the CSF yielded negative results. Sputum culture was sterile. Gene Xpert MTB/RIF from sputum and CSF were also negative. She was initially treated with broad spectrum IV antibiotic cefotaxi-me. She started antituberculous therapy (ATT) with isoniazid (INH), rifampicin (RIF), ethambutol (EMB), and pyrazinamide (PZA) daily and steroid (methylprednisolone). However, her seizures did not subside, so electroencephalography was conducted, resulting in cortical hypofunction with no epilep-tiform wave. Phenobarbital was commenced for focal sei-zure. She also experienced severe headache, so morphine was given orally. After 2 weeks without clinical improve-ment, head magnetic resonance imaging (MRI) with contrast was performed. MRI resulted in tuberculoma size of 25 mm with caseous necrosis surrounded by fibrous capsule and perifocal edema at the subcortical right occipital lobes (Figure 2).After approximately 1.5 months of therapy with ATT, the patient complained of feeling nauseous and yellow-ish in the sclera. Laboratory examination was performed and found an increased total serum bilirubin, which was 2 times than normal and normal serum liver enzymes. INH, RIF, and PZA were stopped and switched with EMB and streptomycin. Clinical improvement was seen during follow up. There was no headache or episode of seizure after 1 month of therapy with ATT. We obtained written permission from the parents to submit this case to a scientific journal.
DISCUSSIONTuberculoma occurs when tubercles in the brain develop without rupturing into the subarachnoid space [3]. Lesions are mostly intraparenchymal, and any part of the central nervous system may be involved and may be solitary or mul-tiple. It may develop with or without tuberculous meningitis [4]. Our patient had a single lesion in the right occipital lobe with caseous necrosis surrounded by fibrous capsule. Tuberculomas, brain abscess, neurocysticercosis, and neo-plasms are considered as differential diagnosis [5]. Based on history of immunosuppression condition, insidious onset, head CT scan, and MRI result, our patient was considered to have TB infection as the most likely diagnosis. However, we did not find any suggested TB signs and symptoms or neuro-logical deficit. Moreover, chest X-ray did not suggest TB, and based on our supported investigation, acid-fast bacilli bacte-ria were not found.
Clinical presentation of tuberculomas depends on their loca-tions. The predilection site is usually at the frontal and pari-etal lobes. The clinical manifestations may be similar with space occupying lesions such as headache, vomiting, drows-iness, focal neurological signs, seizures, papilloedema, and fever. CSF analysis usually shows non-specific result, and cultures may fail to detect MTB [6]. Neuroimaging examina-tion assists clinicians in diagnosing tuberculoma. The radio-logical imaging characteristic determines whether the granu-
Figure 1. Head CT scan. The image shows a single ring-enhancing lesion at the occipital lobe with a size of 15 mm
Figure 2. MRI with contrast. This image shows a tuberculoma size of 25 mm with caseous necrosis surrounded by fibrous capsule and perifocal edema at the subcortical right occipital lobes
Turk Thorac J 2018; 19(3): 153-5
154

loma is non-caseating, caseating with a solid center, or caseating with a liquid center. CT scan and MRI are useful and important non-invasive techniques for the diagnosis of tuberculoma [7]. The prevalence of TB infection in a patient with SLE ranges from 3.6% to 13%, and the mortality rate from TB in SLE ranges from 0% to 31%. The increased risk of TB infection in a patient with SLE is caused by decreased immune function and immunosuppressive effects of medica-tions to treat the disease [1].
In this patient, we conducted Xpert MTB/RIF twice from the sputum and once from the CSF to ensure the diagnosis, but the results were negative. Xpert MTB/RIF is the newest diag-nostic examination for TB infection recommended by the World Health Organization since 2013 in children [7]. Xpert MTB/RIF compared with culture has a sensitivity of 62% and specificity of 98%for TB detection in children [8]. The prob-lem in our diagnosis for TB was due to the negative result of our supporting investigation.
This patient also experienced antituberculosis drug-induced hepatotoxicity. INH, RIF, and PZA were stopped, and ATT was switched to EMB and streptomycin that were less hepa-totoxic. Regular laboratory check-up in patients with ATT drugs is important, even though they are asymptomatic. After 2 months of therapy, this patient clinically showed improve-ment, and her body weight increased.
In conclusion, clinical presentation of tuberculosis infection in immunocompromised patient could be not obvious so clinician should made careful decision on diagnosis and treatment. In addition, once we commenced antituberculosis drug, close monitoring of side effect was needed.
Informed Consent: Informed consent was obtained from parents of the patient who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - H.M.D., G.I., K.I., Design - H.M.D., K.I.; Supervision - H.M.D., G.I., K.I.; Resource - H.M.D., G.I., K.I.; Materials - H.M.D., G.I., K.I.; Data Collection and/or Processing - H.M.D., K.I.; Analysis and/or Interpretation - H.M.D., G.I., K.I.; Literature Search - H.M.D., K.I.; Writing - H.M.D., G.I., K.I.; Critical Reviews - H.M.D., G.I., K.I.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: The authors declared that the study has received no financial support.
REFERENCES1. Chu AD, Polesky AH, Bhatia G, et al. Active and latent tubercu-
losis in patients with systemic lupus erythematosus living in the United States. J Clin Rheumatol 2009;15:226-9. [CrossRef]
2. Fishman JA. Infections in immunocompromised hosts and organ transplant recipients: essentials. Liver Transpl 2011;17:34-7. [CrossRef]
3. Rock RB, Olin M, Baker CA, et al. Central nervous system tuber-culosis: pathogenesis and clinical aspects. Clin Microbiol Rev 2008;21:243-61. [CrossRef]
4. Chatterjee S. Brain tuberculomas, tubercular meningitis, and post-tubercular hydrocephalus in children. J Pediatr Neurosci. 2011;6:96-100. [CrossRef]
5. Mukherjee S, Das R, Begum S. Tuberculoma of the brain-a diagnostic dilemma: magnetic resonance spectroscopy a new ray of hope. J Assoc Chest Physicians 2015;3:3-8. [CrossRef]
6. Ahluwalia VV, Sagar GD, Singh T, et al. MRI spectrum of CNS tuberculosis. J Indian Acad Clin Med 2013;14:83-90.
7. WHO. Guidance for national tuberculosis programmes on the management of tuberculosis in children: World Health Organization; 2014.
8. Detjen AK, DiNardo AR, Leyden J, et al. Xpert MTB/RIF assay for the diagnosis of pulmonary tuberculosis in children: a systematic review and meta-analysis. Lancet Respir Med. 2015;3:451-61. [CrossRef]
Nataprawira et al. Tuberculoma in a Child with SLE-Nephritis
155

Turk Thorac J 2018; 19(3): 156-7
Letter to the Editor
Authors: Sapiens H, Consilius H, Laborem H, Mutuus H, Exercitationa H, Parasitorum H, Gloria H
Dear Editor,
Besides its professional satisfaction, being a journal author brings several academic, social, and financial implications. Real scientific authorship requires substantial efforts while conducting it along with a responsibility of the content. Therefore, an authorship should be clearly differentiated from other kinds of contribution. This issue has always been a problem for several investigators [1,2].
In order to “review best practice and ethical standards in the conduct and reporting of research and other material pub-lished in medical journals,” International Committee of Medical Journal Editors (ICMJE) has developed some recommen-dations [3]. This article contains a dedicated section on the authorship that delineates the importance of authorship, gives a brief definition of “the author,” and allocates the roles of other kinds of contribution. About being an author, ICMJE recommends the following four distinct criteria:
1. Substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work;
2. Drafting the work or revising it critically for important intellectual content;
3. Final approval of the version to be published; and
4. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
These statements are widely accepted worldwide; there is a substantial number of journals using these recommendations which are either members of ICMJE or are voluntarily using them without membership (http://www.icmje.org/journals-following-the-icmje-recommendations). However, the journals and the editors are notably not responsible for deciding which individual should be designated as an author. It is the responsibility of the conductors of the study to decide whether a colleague is an author or not. The individuals who do not meet ALL four criteria should be listed in the Acknowledgements section. The ICMJE recommendations give some examples regarding such contributions as acquisi-tion of funding; general supervision of a research group or general administrative support; and writing assistance, techni-cal editing, language editing, and proofreading.
In the following section, I would like to define the main features of an author and then provide additional examples of pseudo-authors who should be better pronounced in the Acknowledgement sections.
The intelligence, design, and performance are the main ontological requirements of a study, just as mind, form, and matter are in Aristotle’s hylomorphism. Thus, we may stratify the body of a study as establishing the main hypothesis (Homo sapiens; wise, rational, and philosophical), defining the methodology (Homo consilius; planner and designer) and accord-
DOI: 10.5152/TurkThoracJ.2018.18032
İbrahim Onur Alıcı Department of Pulmonology, Health Sciences University, Dr. Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital, İzmir, Turkey
Address for Correspondence: İbrahim Onur Alıcı, Department of Pulmonology, Health Sciences University, Dr. Suat Seren Chest Diseases and Thoracic Surgery Training and Research Hospital, İzmir, Turkey E-mail: [email protected]©Copyright 2018 by Turkish Thoracic Society - Available online at www.turkthoracj.org 156
Cite this article as: Alıcı İO. Authors: Sapiens H, Consilius H, Laborem H, Mutuus H, Exercitationa H, Parasitorum H, Gloria H. Turk Thorac J 2018; 19(3): 156-7
Received: 05.03.2018 Accepted: 20.05.2018

ingly intervening (Homo laborem; labor, effort, and work), which is followed by data acquisition, analysis, and discus-sion in the light of existing literature to decide whether the hypothesis is approved or not. Interpretation and discussion of the results by comparing with the data in the literature, which should be named “writing of a manuscript,” is the effort that gives the core of philosophy behind the study. Thus, the manuscript should be written, reviewed, and approved only by the designers and performers of the study, and not by a third-party individual. This ensures the authorship, which gives desired academic, social, and financial advantages. These advantages are not only personal, but are also institu-tional and national. On behalf of Homo Sapiens, Homo Consilius, and Homo Laborem, I would like to provide some examples of those “honorary” and “ghost” authors [2].
Homo MutuusThere may be a relation of mutual benefit between several investigators in a clinic or institution. Two colleagues may become an author in each other’s studies to increase the number of their studies without any remarkable effort.
Homo ExercitationaThe data that comes from a routine practice of a colleague may not make him or her an author. For example, in a study on a multidisciplinary subject (i.e., lung cancer) which was planned and conducted by a pulmonologist; a thoracic sur-geon, a radiologist, or a pathologist may appear as an author, although he or she did not fulfill the ICMJE criteria and instead only performed routine practice on the patients involved in the study.
Homo Parasitorum Most embarrassingly, there may be some individuals who were not involved in any step of the investigation, but gath-ered an authorship by being a friend, using the power of chair, paramedical memberships, and so on.
Homo Gloria Some investigators try to benefit from the glory of their respectable colleagues. Being an author also entails taking full responsibility of the study; in this case, the venerable col-league is mentioned as an author although he or she does not entirely know the study.
Homo DecipiusAs is easily noted, Homo Decipius is not written as an author in the title. The reason is clear; he or she had a substantial effort in data acquisition, analysis, or interpretation of the
study, but could not have the opportunity to be an author; instead, he or she was only exploited.
These points do not mean that a lower number of authors is better. The number of authors increases as the science becomes more complex [4]. Alternatively, pseudo-authorship is the main problem that should be resolved. Departments of medical ethics within government or universities and nation-al scientific societies are somewhat responsible for a possible correction. There are specific working groups within nation-al scientific societies which comprise countless bright minds with a deep knowledge and experience in their fields and scientific methodology. A comprehensive discussion in a multidisciplinary assembly would easily result in a hypothe-sis in their field. Also, regarding the institutional nature of the working groups, a dedicated investigator should ensure the worthiness of an authorship. In addition, continuing educa-tional programs may be implemented for post-graduation investigators.
In conclusion, the establishment of such scientific working groups should be encouraged not only at the national level, but also at an institutional level. Moreover, a nationwide update on medical and professional ethics is urgently required for raising the scientific reputation of the country to the desired level.
Peer-review: Externally peer-reviewed.
Acknowledgements: The author would like to thank to Prof. Yücel Demiral, MD, PhD for his guidance.
Conflict of Interest: The author have no conflicts of interest to declare.
Financial Disclosure: The author declared that this study has received no financial support.
REFERENCES1. van Loon AJ. Pseudo-authorship. Nature 1997;389:11. [CrossRef]2. Flanagin A, Carey LA, Fontanarosa PB, et al. Prevalence of Articles
With Honorary Authors and Ghost Authors in Peer-Reviewed Medical Journals. JAMA 1998;280:222-4. [CrossRef]
3. Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals (Updated December 2017). International Committee of Medical Journal Editors, 2017.
4. Weeks WB, Wallace AE, Kimberly BC. Changes in authorship pat-terns in prestigious US medical journals. Soc Sci Med 2004;59:1949-54. [CrossRef]
Alıcı İ.O. The Turkish Sleep Apnea Database
157

Turk Thorac J 2018; 19(3): 158
158
DOI: 10.5152/TurkThoracJ.2018.110718
Metin Akgün ve Begüm Ergan tarafından hazırlanan ve Turkish Thoracic Journal Nisan 2018 sayısında yayınlanan “Silicosis in Turkey: Is it an Endless Nightmare or is There Still Hope?” (Turk Thorac J 2018; 19: 89-93 DOI: 10.5152/TurkThoracJ.2018.040189) başlıklı yazıda yer alan Figür 1’de ve alt yazısında yazım hatası tespit edilmiştir. Dergi editörlüğüne iletilen talep sonrasında ilgili hatalar düzenlenmiştir. Yazının güncel versiyonuna https://doi.org/10.5152/TurkThoracJ.2018.040189 adresinden ulaşılabilmektedir.
In the article by Metin Akgün and Begüm Ergan, entitled “Silicosis in Turkey: Is It an Endless Nightmare?” that was published in the April 2018 issue of Turkish Thoracic Journal (Turkish Thorac J 2018; 19: 89-93 DOI: 10.5152 / TurkThoracJ.2018.040189), typing errors were detected in Figure 1 and in its footnote. These errors were since corrected. The up-to-date version of the articles is available at https://doi.org/10.5152/TurkThoracJ.2018.040189.
DOI: 10.5152/TurkThoracJ.2018.120718
Mohammadreza Masjedi ve ark.ları tarafından hazırlanan ve Turkish Thoracic Journal Nisan 2018 sayısında yayınlanan “Assessing the Prevalence and Incidence of Asthma and Chronic Obstructive Pulmonary Disease in the Eastern Mediterranean Region” (Turk Thorac J 2018; 19: 56-60 DOI: 10.5152/TurkThoracJ.2018.17051) başlıklı yazının içeriğinde ve yazarların kurum bilgilerinde yazım hataları tespit edilmiştir. Dergi editörlüğüne iletilen talep sonrasında ilgili hatalar düzenlenmiştir. Yazının güncel versiyonuna https://doi.org/10.5152/TurkThoracJ.2018.17051 adresinden ulaşılabilmektedir.
In the article by Masjedi et al., entitled “Assessing the Prevalence and Incidence of Asthma and Chronic Obstructive Pulmonary Disease in the Eastern Mediterranean Region” that was published in the April 2018 issue of Turkish Thoracic Journal (Turk Thorac J 2018; 19: 56-60 DOI: 10.5152/TurkThoracJ.2018.17051), typing errors were detected in the main text and in the authors’ instituions. These errors were since corrected. The up-to-date version of the articles is available at https://doi.org/10.5152/TurkThoracJ.2018.17051.
ERRATUM