tct recognition of vulnerable plaque guidelines
TRANSCRIPT

Total victims of new heart attacks in
2003
Will die before
reaching hospital.
>50%
Damaged Myocardi
um
Pre-Hospital Delay
10year mortality ticket issued on the way reaching hospital!
Future heart
failure…
Cardiology of Today CANNOT Reach >50% of Its Target Population
~ 500,000 in the USA

Everybody has atherosclerosis, the question is who has vulnerable plaque
Sudden Cardiac DeathAcute MI
VulnerablePlaque

Carl von Rokitansky (1804-1878)
Rokitansky gave early detailed descriptions of arterial disease. He
is alleged to have performed 30,000
autopsies.
Rokitansky in 1841 championed the Thrombogenic Theory. He proposed that the deposits observed in the inner layer of the arterial wall
derived primarily from fibrin and other blood elements rather than being the result of a purulent process. Subsequently, the atheroma resulted from the
degeneration of the fibrin and other blood proteins as a result of a preexisting crasis of the blood, and finally these deposits were modified toward a pulpy
mass containing cholesterol crystals and fatty globules. This theory came under attack by Virchow

First studies on inflammation of vessels, particularly phlebitis, Started at a time when Cruveilhier2had just stated: La phlebite domine toute la pathologie.3 First a great number of preparatory studies on fibrin, leukocytes, meta-morphosis of blood, published separately. …
Rudolf Virchow 1821-1902
The Father of Cellular Pathology
Virchow appreciates prior works.
Virchow presented his inflammatory theory. He utilized the name of "endarteritis deformans." By this he meant that the atheroma was a product of an inflammatory process within the intima with the fibrous thickening evolved as a consequence of a reactive fibrosis induced by proliferating connective tissue cells within the intima.

Olcott 1931 “plaque rupture”
Leary 1934 “rupture of atheromatous abscess”
Wartman 1938 “rupture-induced occlusion”
Horn 1940 “plaque fissure”
Helpern 1957 “plaque erosion”
Crawford 1961 “plaque thrombosis”
Gore 1963 “plaque ulceration”
Friedman 1964 “macrophage accumulation”
Byers 1964 “thrombogenic gruel”
Chapman 1966 “plaque rupture”
Plaque Fissure in Human Coronary Thrombosis (Abstract) Fed. Proc. 1964, 23, 443 Paris Constantinidis
“The destruction of the hyalinized wall separating lumen from the atheroma was almost always observed to be preceded by or associated with its invasion by lipid containing macrophages.”
Friedman and van den Bovenkamp 1965
Unheralded Pioneers

N Engl J Med 1999
“Atherosclerosis; an inflammatory disease”
Ross R.
Russell Ross
Atherosclerosis; arterial “Response to Injury”
N Engl J Med 1976 Aug 12;295(7):369-77 The pathogenesis of atherosclerosis (first of two parts).Ross R, Glomset JA.

James T. Willerson 1981N Engl J Med 1981 Mar 19;304(12):685-91
Plaque Thrombosis

Erling Falk Michael Davies
Autopsy Series
Thin Fibrous Cap + Large Lipid Core + Dense Macrophage
A culprit ruptured plaque
1981-1990
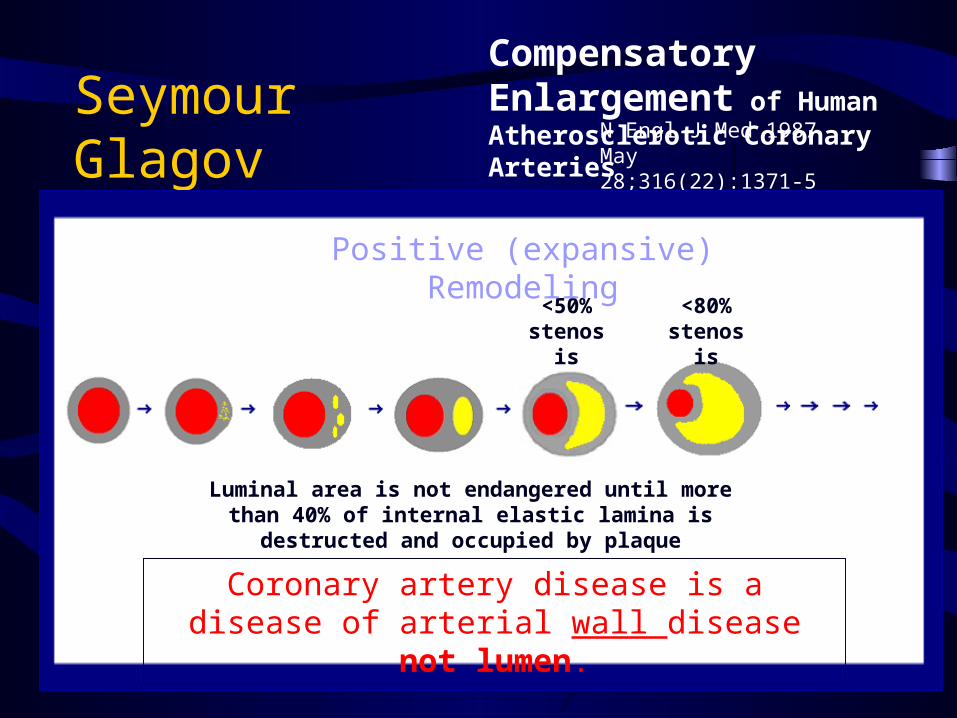
Seymour GlagovCompensatory Enlargement of Human Atherosclerotic Coronary Arteries N Engl J Med 1987 May
28;316(22):1371-5
<50% stenosis
Luminal area is not endangered until more than 40% of internal elastic lamina is destructed and occupied by plaque
Coronary artery disease is a disease of arterial wall disease not lumen.
Positive (expansive) Remodeling
<80% stenosis

Angiographic progression of coronary artery disease and the development of myocardial infarction.Ambrose JA, Tannenbaum MA, Alexopoulos D, Hjemdahl-Monsen CE, Leavy J, Weiss M, Borrico S, Gorlin R, Fuster V.
Department of Medicine, New York Cardiac Center, Mount Sinai Medical Center, New York 10029.
Simultaneously, Little et al, Haft et al reported that majority of culprit lesions are found on previously non-critical stenosis plaques.
Conclusion: “Myocardial infarction frequently develops from non-severe lesions.”
J Am Coll Cardiol 1988 Jul;12(1):56-62
Ambrose, Fuster, and colleagues
Angiographically Invisible Plaques

Falk E., Shak P.K., Fuster V. Circulation 1995
Non-stenotic (<75%) plaques cause about 80% of deadly MI

Macrophage- driven MMPs soften plaque cap and prompt it to rupture
P.K. Shah
Peter LibbyThe fate of
atherosclerosis and its thrombotic complication are governed by immune
system.
Goran Hanssonand others
Allard van der Wal
and others

•Eroded Plaque
Rupture-prone plaques are not the only type of vulnerable plaque
•Calcium Nodulevan der Wal - Netherlands
Renu Virmani -USA
Thiene - Italy
Kolodgie F., Burk A.P., Farb A., and Virmani R.
Muller JE, Abela GS, Nesto RW, Tofler GH.Triggers, acute risk factors and vulnerable plaques: the lexicon of a new frontier.J Am Coll Cardiol. 1994 Mar 1;23(3):809-13
James E. Muller 1994
Muller coined the term of “Vulnerable” Plaque
Muller likened Vulnerable Plaques to American nuclear missiles stored underground in Nevada desert where they could be vulnerable to Russians’ long-range missile attack!
“Vulnerable to disruption and thrombosis”

Vulnerable Plaque?
What is

Total victims of new heart attacks in
2003
Will die before
reaching hospital.
>50%
Damaged Myocardi
um
Pre-Hospital Delay
10year mortality ticket issued on the way reaching hospital!
Future heart
failure…
The major underlying cause of this long standing failure in cardiology.
~ 500,000 in the USA


Potential Underlying Cause of All (fatal and non-fatal) Heart Attacks(Sudden Cardiac Death + Acute Coronary Syndrome)
With Occlusive Thrombi
With Rupture
>70% Stenosis
With Significant Atherosclerosis or Ischemic Heart
<70% Stenosis
Without Significant Atherosclerosis or Atherosclerosis-Derived Myocardial Damage
Without Occlusive Thrombi
Without Rupture With Old Myocardial Damage
WithoutOld Myocardial Damage
Only Myocardial-Derived Factors(conductive disorders, …)
Erosion Calcified Nodule Others
With Critical Stenosis Without Critical Stenosis
With Expansive Remodeling
Without Expansive Remodeling

Ruptured Plaques (~70%)1. Stenotic (~20%)2. Non-stenotic (~50%)
Non-ruptured Plaques (~ 30%)1.Erosion (~20%)2.Calcified Nodule (~5%)3.Others / Unknown (~5%)
Plaque Pathology Responsible for Coronary Thrombotic Death
In summary:

Terminology:
Culprit Plaque: a Retrospective Terminology
Vulnerable Plaque: a Prospective Terminology

Different Types of Vulnerable Plaques Major Underlying Cause of
Acute Coronary Events
NormalRupture-prone
Fissured ErodedCritical Stenosis Hemorrhage
Naghavi et al, Cur Ath Rep 2001

Rupture-Prone Plaque
Vulnerable Plaque Naghavi et al, Cur Ath Rep 2001
Macrophage
Necrotic lipid core
Thin fibrous cap

Eroded Plaque
Vulnerable Plaque Naghavi et al, Cur Ath Rep 2001
Endothelial denudation
Proteoglycans
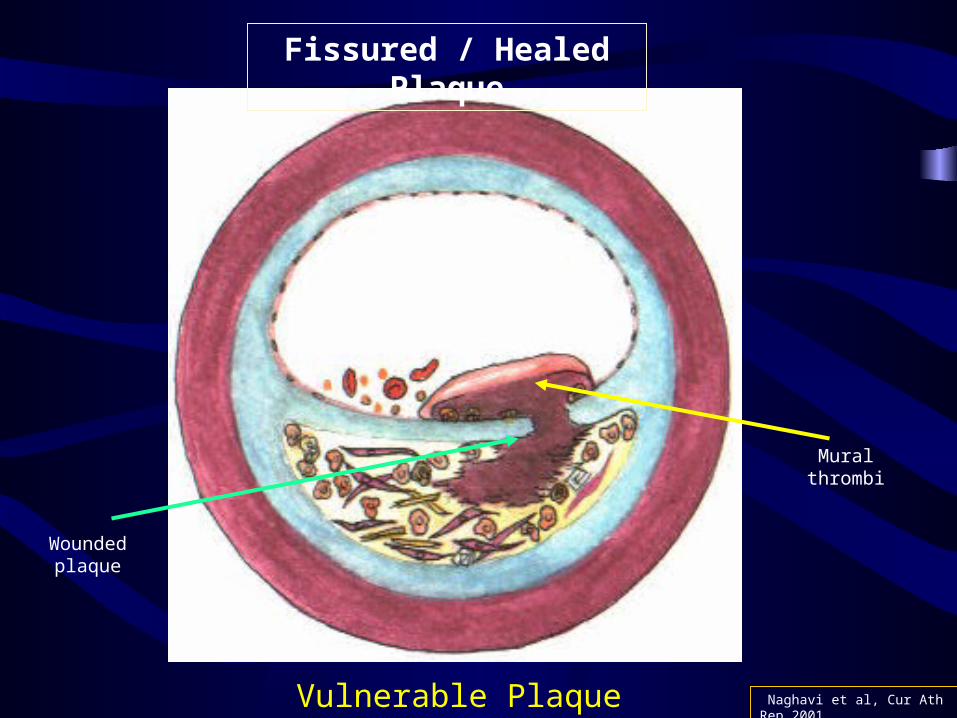
Fissured / Healed Plaque
Vulnerable Plaque Naghavi et al, Cur Ath Rep 2001
Mural thrombi
Wounded plaque

Plaque with a Intimal Calcified Nodule
Vulnerable Plaque Naghavi et al, Cur Ath Rep 2001
Calcified nodule

Intra-Plaque Hemorrhage with Intact Cap
Vulnerable Plaque Naghavi et al, Cur Ath Rep 2001
Leaking angiogenesis or rupture of
vasa vaserum

Critically Stenotic but Asymptomatic Plaque
Naghavi et al, Cur Ath Rep 2001Vulnerable Plaque
>75% lumina
narrowing

Different Types of Vulnerable Plaques Major Underlying Cause of
Acute Coronary Events
NormalRupture-prone
Fissured ErodedCritical Stenosis Hemorrhage
Naghavi et al, Cur Ath Rep 2001

Proposed Histopathological and Clinical Criteria for Definition of
Vulnerable Plaque Major Criteria:1. Active Inflammation (monocyte/
macrophage infiltration) 2. Thin Cap with Large Lipid Core 3. Endothelial Denudation with Superficial
Platelet Aggregation 4. Fissured / Wounded Plaque

Proposed Histopathological and Clinical Criteria for Definition of
Vulnerable Plaque Minor Criteria:1. Superficial Calcified nodule 2. Glistening Yellow 3. Intraplaque Hemorrhage 4. Critical Stenosis5. Positive Remodeling?

From “Vulnerable Plaque”
To “Vulnerable Patient”
A Call For New Definitions And Risk Assessment Strategies


Vulnerable Blood
Vulnerable Myocardium
Vulnerable Plaque
Vulnerable Patient

What is Vulnerable
Plaque?

A plaque with high likelihood of causing thrombus OR rapid progression.

What is Vulnerable
Blood?

A thrombogenic blood that exhibits increased coagulability or decreased endogenous thrombolytic activity.

What is Vulnerable
Myocardium?

A myocardium with electrical instability that has tendency to develop fatal arrhythmia upon ischemia.
Who is aVulnerable
Patient?

A patient with high likelihood of having an acute event:
-Sudden Cardiac Death-Myocardial Infarction-Acute Coronary Syndrome

In search of “vulnerable patient”

1,400,000 Annual Heart Attacks
140,000,000 Americans >35y
Home-Based Screening
Non-invasive Imaging
Office-Based Screening
Invasive 2-3 millions
40-50 millions
50-60 millions
Chol, CRP,Genetic
Screening,Age – Sex –
Family History
Calcium
MRI / MRA
Thermography, OCT,
Spectroscopy, …
CT-Angio


